adolescent substance abuse & co-occuring mental … · substance abuse antisocial behavior ......
TRANSCRIPT

Adolescent Substance Use Disorder & Co-occurring Mental
Illness or Visa Versa
R. Joffree Barrnett, M.D.
2015

Goals
Provide an overview of adolescent development, mental illness and substance use disorders
Discuss the neurobiology of mental illness and substance use disorder using the example of dopamine (DA)
Review the extent of the disorders and clinical course
Review best practices of treatment for co-occurring disorders
Discuss barriers to recovery

Overview of Illness and Brain Maturation

Defining Substance Use Disorders (SUD)2-3 = Mild, 4-5 = Moderate, 6-7 = Severe
• The substance is often taken in larger amounts or over a longer period than was intended.• There is a persistent desire or unsuccessful effort to cut down or control use of the
substance.• A great deal of time is spent in activities necessary to obtain the substance, use the
substance, or recover from its effects.• Craving, or a strong desire or urge to use the substance.• Recurrent use of the substance resulting in a failure to fulfill major role obligations at work,
school, or home.• Continued use of the substance despite having persistent or recurrent social or interpersonal
problems caused or exacerbated by the effects of its use.• Important social, occupational, or recreational activities are given up or reduced because of
use of the substance.• Recurrent use of the substance in situations in which it is physically hazardous.• Use of the substance is continued despite knowledge of having a persistent or recurrent
physical or psychological problem that is likely to have been caused or exacerbated by the substance.
• Tolerance, as defined by either of the following:a. Need markedly increased amounts of substance to achieve intoxication or desired effect.
• b. A markedly diminished effect with continued use of the same amount of the substance.• Withdrawal, as manifested by either of the following:
a. The characteristic withdrawal syndrome for that substance (as specified in the DSM 5)b. The substance (or other substance) is taken to relieve or avoid withdrawal symptoms.

Onset of Substance Use in Childhood and Adolescence

Mental Illness in Adolescents
Rules of Thumb I• The overall rate is similar to adults in a 6 month
period. Close to 20-25% (1 in 4-5)have a diagnosable condition.
• If you require a criteria of “clinical significant dysfunction” the rate drops to 16-18%.
• In prepubertal disorders males predominate (3:1) and exhibit primarily “behavioral” disorders.
• In adolescence rates of mental illness in males and females become more equal; rates of mood and substance use increase.
Mental Illness in Adolescents Interacts With Normal Brain Development
Rules of Thumb II• The brain develops over the first two plus
decades and influences the manifestations of mental illness.
• Thinking capacity: organization, planning and the use of logic is not fully developed until after puberty.
• Language (the ability to express thinking/perceptual capacity) also varies as a function of development.

Brain Development

Milestones in Adolescent Development
• Physical maturity• Sense of identity (self, body, normality)• Transition from family to peer relations• Growth of social skills• Growing sexual interest and identification• Improved mood modulation• Improved impulse control• Maturation of morality• Improved abstract thinking

Risk Factors
• Poor self control
• Aggressive behavior in childhood
• Lack of parental supervision, support or mentoring
• Poor social skills
• Drug experimentation
• Availability of drugs at school
• Community poverty/poor cohesion
• Learning problems
Protective Factors• Good self-control (impulses and
mood)• Parental monitoring and
support/mentoring• Good social skills, positive
relationships• Good academic
function/Intelligence• School drug education/anti-drug
policies• Neighborhood
pride/cohesiveness• Spirituality
The Overall Product of Development is a Capacity for Resilience: Living in the World

Life Course and Risk Factors in Children
& Adolescents
Mother’s HealthPregnancy ProblemExposure to Drugs& Heavy Metals(Brain Damage)
PovertyNeighborhood CohesionParentingTemperamentEarly AggressionParental Mental IllnessAbuse or Neglect
Peers / GangsSubstance AbuseAntisocial Behavior
Birth Puberty
Childhood Adolescence
Adulthood

Mental Illness in Adolescence: Environmental Influences
Rules of Thumb III• The younger the individual the more dependent
and influenced by the environment.• Only the extremes of abnormal parenting are
associated with mental illness in children. Not so with substance use
• In adolescence peers and social environments have a stronger influence
• Adverse events and trauma affect brain circuits and increase the vulnerability to disorders through the HPA axis
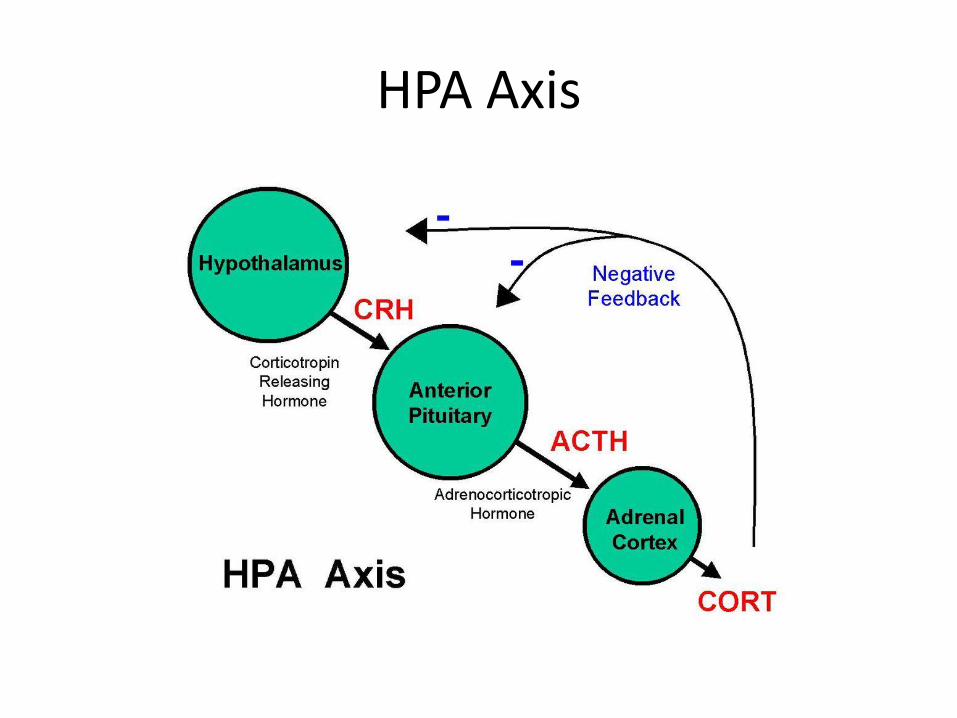
HPA Axis

Mental Illness in Adolescence
Rules of Thumb IV• Mental illness is a disorder of central nervous
system function manifested as emotions thoughts and behaviors.
• The earlier the onset of illness (disruption in brain development) the worse the prognosis.
• General or specific CNS impairments increase the probability of mental illness.
• Two of more diagnoses is almost as common as a single diagnosis
Mental Illness in Adolescence: Genetics
• Genes have an influence but interact with the environment to produce a new biological level of function. Genes are turned on and off (capacities and deficits)
• We inherit a vulnerability for a particular illness that then is triggered following interaction with the environment
• There are probably critical periods for normative function in brain development
• Differences in genetic makeup affect responses to treatment

Concordance Rates of Mental Illness in Twins vs. rates in the General Population
• Monozygotic Twins:
– Schizophrenia 35-50%
– Major Depression 59%
– Bipolar Disorder 74-80%
• General population
– Schizophrenia 1%
– Major Depression 5%
– Bipolar Disorder 1.5%
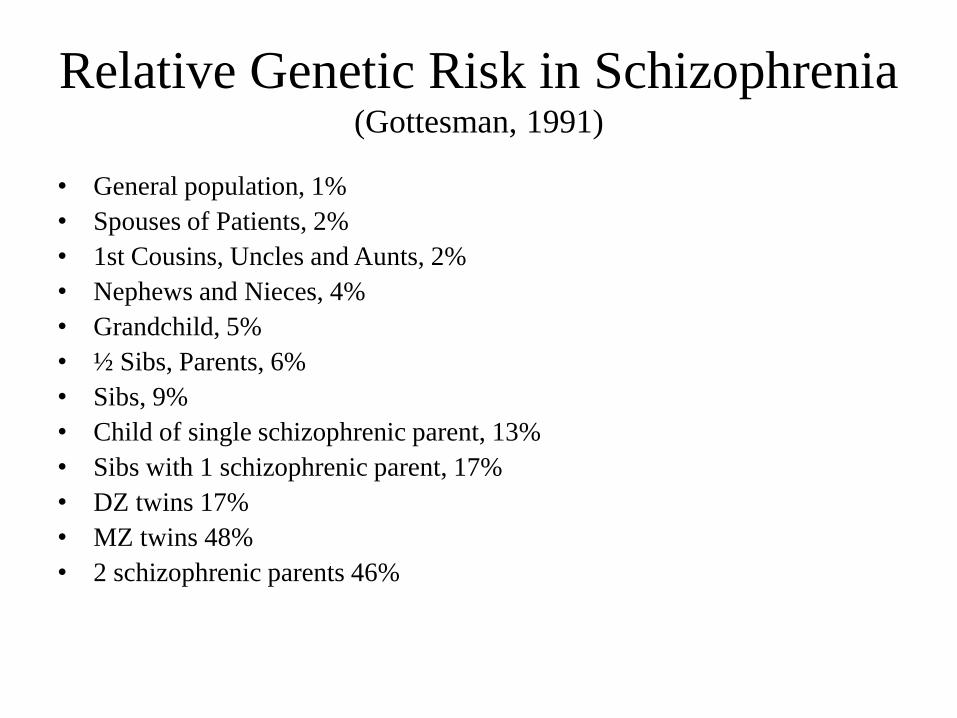
Relative Genetic Risk in Schizophrenia (Gottesman, 1991)
• General population, 1%
• Spouses of Patients, 2%
• 1st Cousins, Uncles and Aunts, 2%
• Nephews and Nieces, 4%
• Grandchild, 5%
• ½ Sibs, Parents, 6%
• Sibs, 9%
• Child of single schizophrenic parent, 13%
• Sibs with 1 schizophrenic parent, 17%
• DZ twins 17%
• MZ twins 48%
• 2 schizophrenic parents 46%
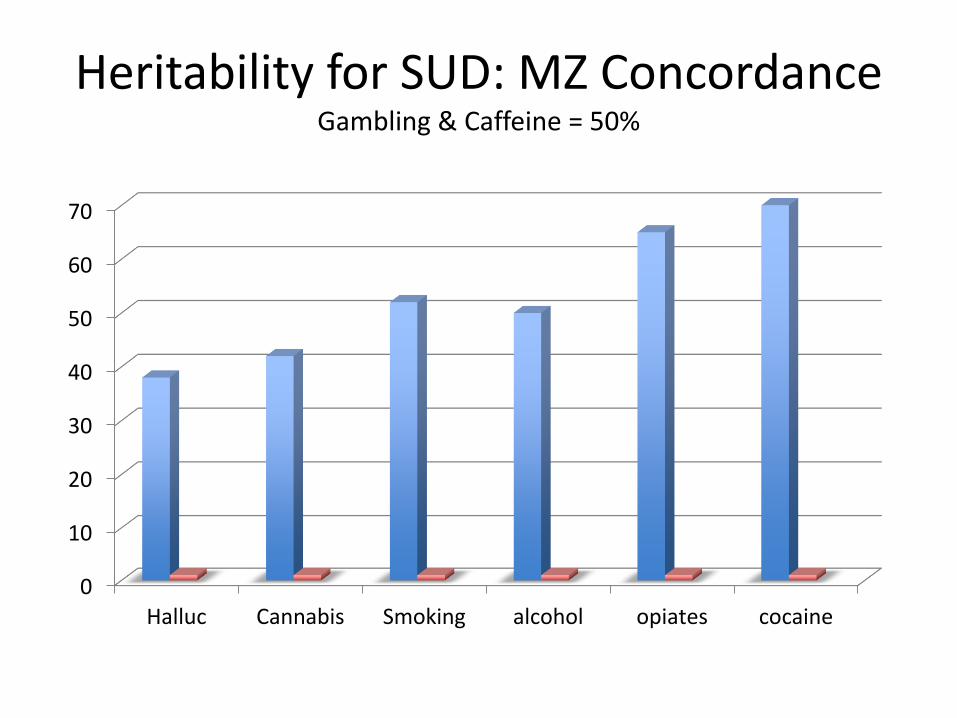
Heritability for SUD: MZ ConcordanceGambling & Caffeine = 50%
0
10
20
30
40
50
60
70
Halluc Cannabis Smoking alcohol opiates cocaine

Genetics
• Genes and the environment interact
• Genes can make an individual more vulnerable to an external influence
• External influences can turn on or off gene expressions (cell function)

Catechol-O-Methyltransferase: COMT Metabolizes Catecholamine Neurotransmitters (Dopamine, Norepinephrine etc.)

Genetics and Pleasure With Marijuana: Val158Met polymorphism
• Methionine (Met) vs. Valine (Val)
• Val is 4x more metabolic than Met
• Val/Val, Val/Met, Met/Met
• Met/Met experiences more pleasure from less stimulating events than Val/Val
• Thus Val/Val>> (more potent) Met/Met Thus higher 500% higher risk of Cannabis use.

Neurobiology of Substance Use and the Dopamine Neurotransmitter
System

Brain Circuits related to Substance UseInhibition, Reward, Motivation/Drive & Learning/Memory

Legend for the above Slide
• The areas depicted contain the circuits that underlie feelings of reward, learning and memory, motivation and drive, and inhibitory control. Each of these brain areas and the behaviors they control must be considered when developing strategies to treat drug addiction.
• Key:
• PFC – prefrontal cortex;
• ACG – anterior cingulate gyrus;
• OFC – orbitofrontal cortex;
• SCC – subcallosal cortex;
• NAc – nucleus accumbens;
• VP – ventral pallidum;
• Hipp – hippocampus;
• Amyg – amygdala.

Neurotransmitters and Substance Use
• Brain Neurotransmitters– Glutamate
– Gama-aminobutyric acid (GABA)
– Dopamine (DA)
– Opoid receptors (endorphins)
– Nicotine receptors
– Cannabinoid receptors
• Networks of each effect reward, motivation, conditioning & impulse control
• Clinical Relevance:
Acute: (intoxication, withdrawal manifestations)
Chronic: (emotional and cognitive function)

Dopamine & the Reward/Pleasure Circuits
• Cocaine and methamphetamine, are among the most addictive substances known and directly increase Dopamine levels.
• Heroin and nicotine cause increases in dopamine levels by indirect mechanisms.
• Conversely, drugs that reduce dopamine levels can cause anhedonia• Many types of pleasurable experiences (e.g. sex, food, gambling) will
increase dopamine release but not as much as cocaine.• Direct electrical stimulation of dopamine pathways in animals creates
repetitive behaviors to obtain it.• Dopamine neurons in the ventral tegmental area and substantia nigra are
strongly activated by rewarding events.• However, reward (repetition/seeking) does not equal pleasure. There is a
difference between wanting & liking

Drug Effects on DA: blue-amphetamine,
red-cocaine, green-nicotine, purple-morphineLeft: % baseline release
0
200
400
600
800
1000
1200
0hr 1hr 2hr 3hr 4hr 5hr
Series 1
Series 2
Series 3
Series 4

Dopamine Pathways: 1) nigrostriatal 2) mesolimbic

Cocaine and Dopamine

From Biological to Clinical: Dopamine (DA)
• DA increases pursuit of rewards• Psychomotor Stimulants: Cocaine, Ecstacy
(MDNA), Amphetamine, Methylphenidate (Ritalin), Metamphetamine (Ice) all increase DA
• High doses cause psychosis which are treated by antipsychotics which reduce DA
• DA effects: mood (euphoria & aggression), reinforcement, conditioning, attention, motivation
• Illnesses linked to DA are ADHD, Psychoses, SUD

Biological to Clinical: Progression of Use
• DA release increases reward seeking• DA metabolism produces impulse for more• Regular/Chronic use produces changes in neuron
internal and neuronal circuit function that diminish actual function
• User no longer experiences pleasure or reward but continues compulsively
• Impairment of mesolimbic circuit increases drug seeking behavior to exclusion of others and limits impulse controlling influence
• Many of diagnostic behavior criteria are displayed

From Biological to Clinical
• Cocaine intoxication:
• >Heart rate & blood pressure, Chest pain, heart arrhythmias, perspiration/chills, nausea/vomiting, psychomotor agitation or retardation, dyskinesia, dystonia, seizure and coma (all Sympathomimetic overload effects)
• Cocaine Withdrawal:• Fatigue, hypersomnia, psychomotor retardation,
depression (all DA depletion)

Co-occurrence/Comorbidity

Relationship Between Psychiatric Disorders and SUD
Age 0 5 10 15 20
Gene/Env Stress/HPA Function Brain development
Family School Peers Work
Substance Use Disorders
Poor Temperament ADHD (30-50%) Conduct Disorder (50-80%)
Bipolar Disorder (15-30%) early onset less likely
Depression (15-30%), ½ before, ½ after
Anxiety Disorders (20-40%)

Lifetime Occurrence of MI & SUD in
Adolescence: % of TotalMerikongas et al, 2010
Age 13-14 15-16 17-18 Severe
Any Depression 8.4 12.6 15.4 8.7
Bipolar 1.9 3.1 4.3 2.6
Any Anxiety 31.4 32.1 32.3 8.3
ADHD 8.8 8.6 9.0 4.2
ODD 12.0 12.6 13.6 6.5
CD 4.4 7.5 9.6 2.2
Alcohol 1.3 6.5 14.5 -
Drug 3.4 2.8 3.0 -
Eating Disorder 2.4 2.8 3.0 -

Progression of Onset of Adolescent MI & SUD

Comorbidity Merikongas et al 2010

Numbers of Initiates of Drug use in the Last Year Among People Aged 12 or Older: 2014

Past Year Marijuana Initiates 2002-2014

Past Year Heroin Initiates 2002-2014

Past-Year Initiation of Substance Use Among Adolescents Aged 12–17 in New Hampshire, by
Substance of Abuse (2009–2013)
Among adolescents in New Hampshire, 12.9% initiated alcohol use (i.e., used it for the first time) within the year prior to being surveyed, and 6.5% initiated marijuana use within the year prior to being surveyed.
• Cigarettes : 5.3%• Alcohol: 12.9% • Marijuana: 6.5% • Nonmedical Use of Psychotherapeutics: 3.1%
Source: SAMHSA, Center for Behavioral Health Statistics and Quality, National Survey on Drug Use and Health, 2009 to 2013.

NH Data for 2012-2013
• New Hampshire’s percentage of alcohol dependence or abuse among individuals aged 12 or older (82,000) was similar to the national percentage in 2012–2013.
• NH= 7.6%• US= 6.7%• Drug use or dependence in individuals aged 12 or
older (37,000):• NH = 2.9%• US = 2.7%

NH Individuals 12 and Older Receiving SUD Treatment
• In a single-day count in 2013, 6,702 individuals in New Hampshire were enrolled in substance use treatment—an increase from 5,107 individuals in 2009.
• In New Hampshire, among individuals aged 12 or older with alcohol dependence or abuse, about 7,000 individuals (8.0% of total; 85000) per year in 2009–2013 received treatment for their alcohol use within the year prior to being surveyed.
• In New Hampshire, among individuals aged 12 or older with illicit drug dependence or abuse, about 6,000 individuals (16.4% of total;36500) per year in 2009–2013 received treatment for their illicit drug use within the year prior to being surveyed.

Education vs. Exposure
• 80% of youths are exposed to educational/preventive messages
• 12.1% (about 1 in 8) of youths 12-17 are approached by someone selling substances

Assessment &Treatment of Co-occurring Disorders

Common Drugs & Street Names
• Anabolic Steroids Roids, Juice• Bath Salts Bloom, Cloud Nine, Vanilla Sky, White
Lightning• Cocaine Coke, Coca, C, Snow, Flake, Blow, Bump,
Candy, Charlie, Rock, Toot• Cough and Cold Medicines Robotripping, Robo, Tussin,
Triple C, Dex, Skittles, Candy, Velvet, Drank• Heroin Smack, Junk, H, Black tar, Ska, Horse• Inhalants Laughing Gas, Snappers, Poppers, Whippets,
Bold• Marijuana Pot, Grass, Herb, Weed, Mary Jane, Reefer,
Skunk• MDMA (Ecstasy or Molly) E, XTC, X, Adam, Hug, Beans,
Clarity, Love Drug•
• Methamphetamine (Meth) Speed, Chalk, Tina, Ice, Crystal, Crank, Glass, Fire, Go Fast
• Prescription Depressant Medications Barbs, Reds, Red birds, Phennies, Tooies, Yellows, Yellow jackets; Candy, Downers, Sleeping pills, Tranks; A-minus, Zombie pills
• Prescription Drugs Oxy, Percs, Vikes, Barbs, Reds, Candy, Tranks, Speed
• Prescription Pain Medications (Opioids) Hillbilly heroin, Oxy, OC, Oxycotton, Percs, Happy pills, Vikes
• Prescription Stimulant Medications (Amphetamines) Skippy, the Smart drug, Vitamin R, Bennies, Black beauties, Roses, Hearts, Speed, Uppers
• Salvia Salvia divinorum, Shepherdess's Herb, Maria Pastora, Sally-D, Ska Pastora
• Spice K2, Fake Weed, Yucatan Fire, Skunk, Moon Rocks• Tobacco, Nicotine, & E-Cigarettes Smokes, Cigs, Chew,
Dip, Snuff•

Goals of Intervention
• Relieve suffering
• Facilitate personal change
• Reduction of harm
• Maintain abstinence
• Prevent or reduce relapse
• Facilitate reintegration into normative activity
• Return to developmental trajectory

Assessment and Diagnosis
• Screening instruments for MI & SUD (CRAFFT @ceasar-boston.org; MI instruments @aacap.org)
• Include multiple sources of information besides the adolescent: parents (family), Pediatrician, School, Legal, Child protection
• Delineate risk factors and strengths• Organize categorically (by diagnosis/problem)• Prioritize by severity and acuity (suicidal vs.
withdrawal)• Enlist partners in a treatment plan, interventions and
ongoing monitoring

Interventions: Overview• Interpersonal
– Cognitive behavioral therapy
– Motivational enhancement
– Contingency management
– Collaborative Problem Solving
– Family therapy
– Group therapy
• Psychopharmacology
• adjunct, limited uses in SUD except withdrawal
• May be co-primary in MI
• 12 Step programs
• Derivations of 12 Step interventions (Rational recovery etc.)
• Court ordered and monitored (drug courts)
• Varied intensity and frequency (inpatient, residential, intensive outpatient, outpatient clinic)
• Integration, maintenance and relapse prevention
• Integrated/combined treatment yields best outcomes
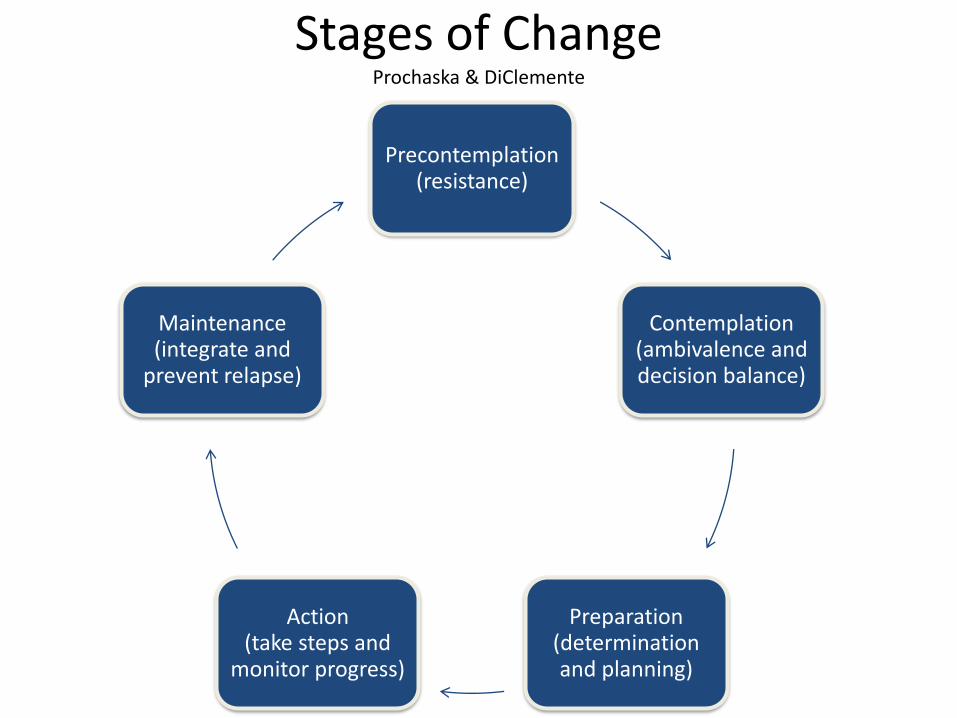
Stages of ChangeProchaska & DiClemente
Precontemplation (resistance)
Contemplation (ambivalence and decision balance)
Preparation (determination and planning)
Action (take steps and
monitor progress)
Maintenance (integrate and
prevent relapse)

Motivational InterviewingMiller & Rollnick
• Client centered, directive method for enhancing intrinsic motivation to change by exploring and resolving ambivalence
• Elements: Conversation about change, collaborative, evocative (clients motivation and commitment), honors autonomy
• Mixed research results in adolescence but mostly positive• Can be used as a brief, adjunct or ongoing behavior change
intervention• Different variations: Motivational Enhancement Therapy,
Dual Diagnosis Motivational Interviewing, Compliance Therapy

Cognitive Behavioral Therapy (CBT)Beck
EventsThoughts Emotions
Behavior & Skills to Manage

Variations of CBT
• Beckian• Metacognitive• REBT• CBT for SUD• Trauma focused CBT• DBT• Acceptance and Commitment Therapy (ACT)• Schema focused• Compassionate mind CBT

Differences
CBT• Problem focused
• Formulation led
• Schema
• Expert-led
• How?
• Thoughts/feelings/behavior
• Change a function of client
• Psychological/medical
MI• Focus on strengths
• Target-behavior led
• Values (of client)
• Expert-trap
• Why? (ambivalence focus)
• Values-dissonance-behavior
• Change a function of relationship
• Humanistic-psychological

Similarities between CBT & MI
• Neither grounded in theory
• Emerged from phenomenological research
– Beck: cognitive distortion
– Miller: Client centered expression of values
– Both have a strong evidence base and culture of evaluation
– Viewed as best practices with extensive research base

Perceived Risk of Harm and Drug Use

Contingency Management
• Based on operant conditioning and social learning theory
• Utilizes rewards and reinforcement for positive behavior
• Long used in Schools and Parent Effectiveness Training (PBIS, IOD at UNH)
• Primarily adjunct
• Assumes impaired or lack of motivation

Collaborative Problem SolvingRoss Greene; Livesinthebalance.org
• Assumes individual Would if they could
• Identifies areas of skill deficits
• Promotes skill development through an empathic relationship
• Once relationship established initiates supported problem solving

12 Step Programs
AA, Originally developed for Alcohol in 1930s
Now adapted to all SUD, Obesity, Gambling etc. and family members of (Al-anon)
Free, widely available and no waiting list
Utilizes mentoring, peer support and group participation
Employs use of a “higher power" and development of spirituality
Highly flexible regarding the definition of “higher power” and spiritual belief and practice
Research supports AA as a “best practice” for SUD

12 Step Alternatives
• Abstinence and 12 Step programs aren’t the only remedies for SUDs. Self-Management and Recovery Training (SMART Recovery) is another treatment option that concentrates on four main principles, which are:
• Creating and sustaining motivation
• Managing urges to use
• Controlling thoughts, emotions, and actions
• Living a well-rounded life

12 Step Alternatives
• Rational Recovery, which centers on a singular approach to recovery
• Utilizes the Addictive Voice Recognition Technique.
• Constantly battling internal urges to relapse into substance use
• The program allows participants to consider themselves fully recovered on day one and to operate with that mindset moving forward.

Supportive Education and Employment
• What do you do after?
• Best practice for adults with SMI
• Client centered support to pursue personal goals
• Renew (J. Malloy, Institute on Disabilities, UNH)

Sample Risk Management Plan:
Adolescent that threatened to
Bomb School with Co-occurring
Disorders
Risk factor Intervention Who’s responsible
Abuse history Trauma Focused CBT Ind., Fam., Rxist
Bullied at School Anti-bullying school plan Ind., Fam., School, Rxist
Depressed w. sui/homi id Prevent-Medication/CBT Ind., Fam., Rxist, ? Hosp.
Mixed use in withdrawal SUD Rx Ind., Fam., Rxist ? Rehab.
Antisocial peer group Alternative
social/recreational
Ind., Fam., School, Rxist

Integrating Treatment Priorities By Severity of Co-occurring Disorders
Problem Severity1. Drug withdrawal &
homicidal/suicidal ideas
2. Depression & PTSD
3. SUD
4. Legal charges
5. Peer conflict and poor role models
6. Integration & maintenance
Intervention Sequence1. Hospitalize begin individual
and family Rx
2. Medication and CBT
3. MET/family Rx/SUD Rx/drug testing/CM
4. Coordinate with court
5. School and family help with social conflicts/CPS
6. Supportive education and employment

Importance of Combined Treatment
• Treating addictive disorders and co-occurring mental health disorders at the same time is important for several reasons:
• Integrated recovery plans are designed to overcome the negative side effects of mental health disorders, such as a reduced attention span, a low level of motivation, and a fear of socializing with others.
• Medication therapy is more effective when your pharmacological plan addresses your mental health disorder as well as your substance abuse disorder.
• In co-occurring disorder’s treatment, the traditional hesitations about prescribing psychotherapeutic medications are no longer an issue.
• Group therapy for people with co-occurring disorders offers a stronger support network for individuals who are struggling with mental illness as well as addiction.
• Treating addiction and a mental health disorder at the same time helps rehab clients address their unique relapse triggers, such as depression, mood swings or panic attacks.

Barriers for Clients, Families and Professionals

Stigma
• SU is considered a moral failure.
• MI elicits fear frustration and condemnation
• The above leads to estrangement and marginalization of affected individuals
• Non affected individuals design and implement discriminatory policy and interventions
• Failure to adequately address these illnesses increases the burden and cost to society
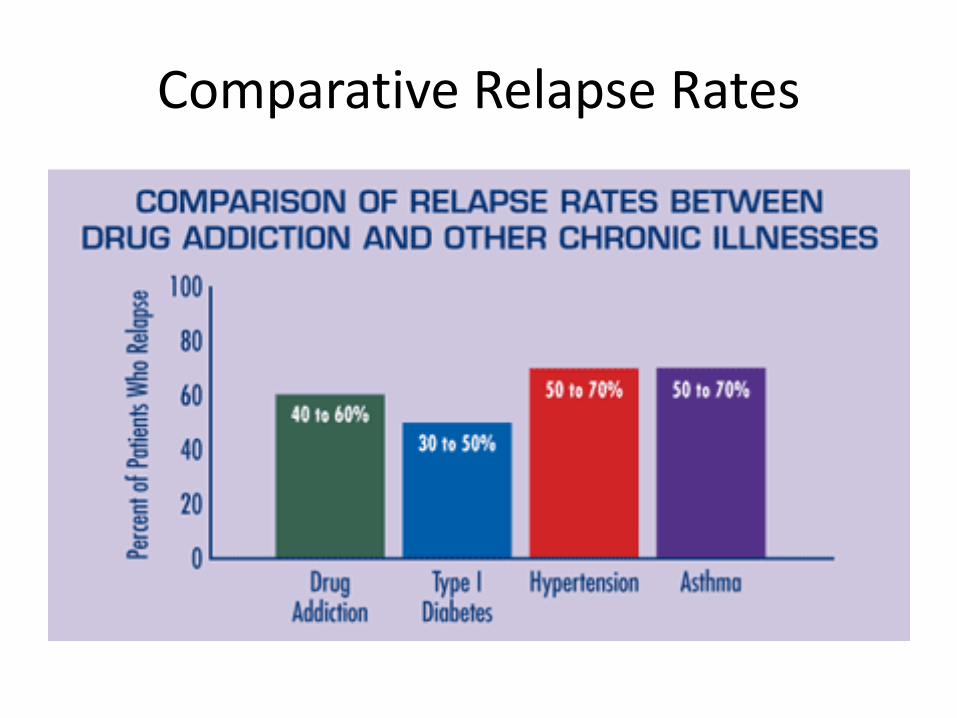
Comparative Relapse Rates

Important Changes Need to be Made in the Current System of Care
• Welcoming clients with co-occurring disorders into substance abuse treatment instead of excluding them because of a psychiatric condition
• Giving the addictive disorder and the co-occurring psychiatric disorder the same level of attention and care during the rehabilitation process
• Addressing both the mental illness and the substance use disorder as chronic, relapsing conditions that require long-term support
• Ensuring that care is provided by a treatment team that’s trained in addressing co-occurring disorders
• Assessing each client for mental health disorders as early in the rehabilitation process as possible so treatment can begin promptly
• Treating all clients with dignity and respect, even if they are in the midst of a mental health crisis or acutely intoxicated.

Columnar Organization of the System of Care
0123456789
10

Insurance/Funding & Managed Care:
• Actuarial vs. epidemiological approach• Reimbursement drives treatment interventions• Review standards/criteria are legal terms of art based
on contract law not scientific/clinical understanding of disease
• Parity of MH benefits• Behavioral Health carve outs• Separation of MI & SUD management and
reimbursement• Do not focus on prevention or maintenance of recovery
Research to Practice/Education and Implementation
• Scientific understanding and advances precede practice changes by 5-10 years
• Research defined “Best Practices” require costly training and supervision of fidelity to the treatment model is an additional cost
• Use of modern technology is only just beginning to be utilized in training and supervision and costs to create and maintain.
• There is little immediate incentive for infrastructural or practice pattern change

Access to Assessment and TreatmentParity for Nature of Disability
• Wait lists are long just for general MH practitioners
• ERs respond to crises but connection to aftercare is poor
• Specialists are few and far between• Full integration the vertical and horizontal aspects
of treatment is lacking – Hospital/rehab-residential/IOP-Outpatient– School/pediatrician/family/therapist
• Supportive services are lacking

Past-Year Depression Treatment Among Adolescents Aged 12–17 with Major Depressive Episode (MDE) in New Hampshire
(2009–2013)
• New Hampshire’s percentage of treatment for depression among adolescents with MDE was higher than the national percentage in 2009–2013.
• 47.1% Received Treatment for Depression (approximately 5,000 individuals per year in 2009-2013 within the year prior to the survey)
• 52.9% Did Not Receive Treatment for Depression • Source: SAMHSA, Center for Behavioral Health
Statistics and Quality, National Survey on Drug Use and Health, 2009 to 2013.

Additional Resources
• National Alliance on Mental Illness (nami.org, naminh.org)
• National Institute on Drug Abuse (NIDA)• Substance Abuse Mental Health Services
Administration (SAMHSA)• dualdiagnosis.org• Aacap.org (American Academy of Child and
Adolescent Psychiatry)• Psychiatry.org (American Psychiatry Association)• APA.org (American Psychological Association)• AAP.org (American Academy of Pediatrics)• Healthychildren.org (designed by AAP)