addressing plantar fasciitis - basi pilates · addressing plantar fasciitis with pilates ... , her...
TRANSCRIPT

AddressingPlantarFasciitiswithPilates
JennaLamornaMcCabe
16December2016Wimbledon,UK,2016

2
Abstract
ThispaperisabouttheuseofPilatestoaddressplantarfasciitis.Statisticsshow
thatbetween4%and7%ofpeopleintheworldhaveheelpainatanygiventime
andabout80%ofthesecasesareduetoplantarfasciitis1.Inflammationand
painfromthisconditioncanbesosevereitinhibitsday-to-dayactivityduetothe
inabilitytowalknormally.Thiscasestudylooksata50year-old,activeandfit
womanwhohasrecentlystartedsufferingwithplantarfasciitisinherleftheel.
Asaresult,herbodyhasasevereleft/rightimbalanceandhasstartedto
compensateforthepainwithnewmusclepatterns.Sheis12sessionsintoa20
sessionPilatesplan,advisedbyherdoctor.Withthecorrectfocus,Pilatescan
helphersignificantly.
1Beeson,P.“PlantarFasciopathy:revisitingtheriskfactors.”FootandAnkleSurgery.September2014.20:160-5

3
Tableofcontents
AnatomicalDescription 4
Introduction:SufferingPlantarFasciitis 8
CaseStudy:TheClient 9
ConditioningProgramme 11
Conclusion 13
Bibliography 14

4
AnatomicalDescription
PlantarFasciitisisinflammationoffascia–athick,white,fibrousbandoftissue,
fascia(orapneurosis),whichoriginatesatthemedialtubercleofthecalcaneus
(heel)andrunsforwardtoinsertintothedeep,shorttransverseligamentsofthe
metatarsalheads,dividinginto5digitalbandsatthemetatarsophalangeal
joints2.Thesebandseachextenddownthefivedistalphalanges,straddlingthe
flexortendons.
Theplantarfasciastretchesalongthesoleofthefoot,supportingthearchand
protectingthesolefrominjury3.Onthebottomofthefoottherearetwomajor
ligaments:thelongplantarligamentandshortplantarligament.Theligament
generallyreferredtoasthe‘plantarfascia’or‘fascia’isthelongplantar.When
theplantarfasciaisoverlystretched,tinytearscanoccuronthesurfaceofthe
muscle,causinginflammationandpain,whichisoftenfeltintheheeland/orthe
soleofthefoot4.Ahealthyplantarfascialigamentisstrongandsupportsthearch
withenoughelasticitytobeartheimpactofthespringinyourwalk.
2 Williams,P.L.,Warwick,R.Gray’sAnatomy.Philadelphia:WBSaunder;1980.36:612-6133“PlantarFasciaAnatomy.”DocPods.DocpodsPtyLtd,Web.Copyright2016.http://www.docpods.com/plantar-fascia-anatomy4Beeson,P.“PlantarFasciopathy:revisitingtheriskfactors.”FootandAnkleSurgery.September2014.20:160-5
5
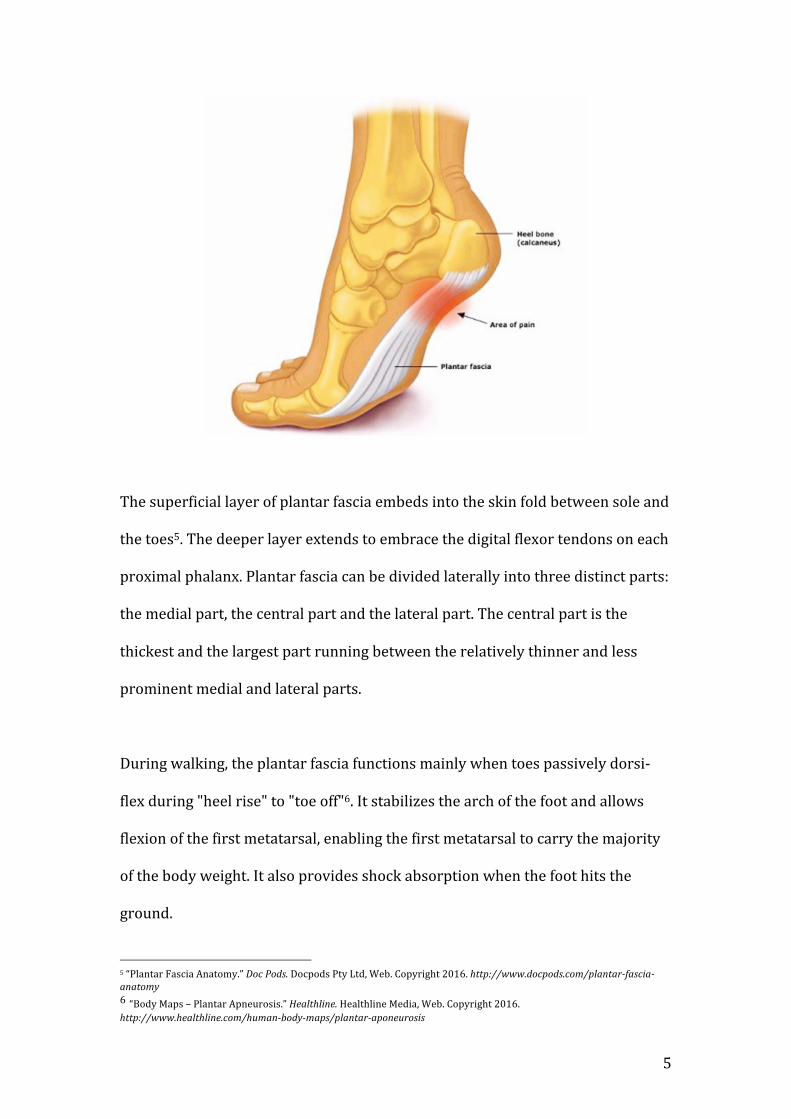
Thesuperficiallayerofplantarfasciaembedsintotheskinfoldbetweensoleand
thetoes5.Thedeeperlayerextendstoembracethedigitalflexortendonsoneach
proximalphalanx.Plantarfasciacanbedividedlaterallyintothreedistinctparts:
themedialpart,thecentralpartandthelateralpart.Thecentralpartisthe
thickestandthelargestpartrunningbetweentherelativelythinnerandless
prominentmedialandlateralparts.
Duringwalking,theplantarfasciafunctionsmainlywhentoespassivelydorsi-
flexduring"heelrise"to"toeoff"6.Itstabilizesthearchofthefootandallows
flexionofthefirstmetatarsal,enablingthefirstmetatarsaltocarrythemajority
ofthebodyweight.Italsoprovidesshockabsorptionwhenthefoothitsthe
ground.
5“PlantarFasciaAnatomy.”DocPods.DocpodsPtyLtd,Web.Copyright2016.http://www.docpods.com/plantar-fascia-anatomy6“BodyMaps–PlantarApneurosis.”Healthline.HealthlineMedia,Web.Copyright2016.http://www.healthline.com/human-body-maps/plantar-aponeurosis

6
Asyoucanseeintheimageabove,theplantarfasciaisenclosedbetweena
numberofkeymuscles,whichactontheankleandfoot.Thetibialisposterior
(whichconnectsthelowerleg–andspecificallytheperoneuslongusand
peroneusbrevis-tothearchandundersideofthefoot)andtibialisanterior
(whichrunsacrossthetibia,fibulaandankletothemedialarchofthefoot)are
theclosesttwomajormusclesneighbouringtheplantarfasciawhichenable
dorsiflexion,plantarflexionandinversionofthefoot.

7
Otherimportantmusclesthatwillimpact,orbeaffectedbythemovementofthe
plantarfasciainclude:
- Theextensordigitoriumlongus,whichrunsdownthefibulaandattaches
tothetopofthefourouterdistalphalanges.
- Thegastrocnemius(prominentcalfmuscle),whichconnectsfromthe
lowerfemurtothecalcaneus(heel)viatheAchillestendon.
- Thesoleus,whichrunsdownthebackofthetibiabelowthe
gastrocnemiusintothecalcaneusviatheAchillestendon.
- Thepernoealslongusandbrevisasmentionedabove,whichoriginateat
thefibulaandinsertviathetibialisposteriorintotheundersideofthe
foot.
Itisimportanttobeawareofhowthesemusclesareconnectedandfunctionin
relationtotheplantarfasciawhenaddressinganissue/injuryandtheresulting
compensationsofthistoo.
Movementsofankle-footjointandtheprimarymusclesthatproducethese
movements7:
Joint Movement PrimaryMover
Ankle-foot Dorsiflexion Tibialisanterior,extensordigitoriumlongus
Ankle-foot Plantarflexion Gastrocnemius,soleus
Ankle-foot Inversion Tibialisanterior,tibialisposterior
Ankle-foot Eversion Peroneuslongus,peroneusbrevis
7Isacowitz,Rael.StudyGuide:ComprehensiveCourse.CostaMesa,California:BodyArtsandScienceInternational,2013.

8
Introduction:SufferingPlantarFasciitis
Statisticsshowthatbetween4%and7%ofpeopleintheworldhaveheelpainat
anygiventimeandabout80%ofthesecasesareduetoplantarfasciitis8.It
becomesmorecommonwithageanditisunclearifonesexismoreaffectedthan
theother.
Thosesufferingwithplantarfasciitiswilloftenfeelthemostseverepainduring
thefirststepsoftheday,orafterthefoothasbeenrested.Bendingthefootand
toesupwards,puttingweightontheheelandexposingthesole/heeltoimpact
canintensifypain.Irritantsofplantarfasciitisarecitedaslongperiodsof
standing,supinationofthefootduetomisalignment,increasedorintensified
impactexercise,orobesity.
Symptomsofplantarfasciitisarecitedas:inflammation,tightcalves,the
shortenedplantarfasciaprotrudingthesolewhenyoustretchit(i.e.during
dorsiflexion)duetotension,anatomicalfoot-anklealignmentproblemsdueto
compensation,alackofstrengthinsupporting/neighboringmusclesanda
‘handedness’imbalance,whichfavoursthedominantsideofthebody.
Adoctor,orthopedicfootspecialist,podiatristorchiropodistmustclearclients
toundertakePilatesbeforestartingacourseofsessions.
8Beeson,P.“PlantarFasciopathy:revisitingtheriskfactors.”FootandAnkleSurgery.September2014.20:160-5

9
CaseStudy:TheClient
Aliceisa50year-old‘stayathome’mumoffourchildrenwhoseagesnowrange
between17and26.Shepracticesyogaandisakeenrunner.Althoughshehas
alwaysbeenactivewiththechildrenandwalkingherdog,shehasrecently
startedrunninganincreasedamounttotrainforamarathon.Shehassuffered
withpatellainjuries/irritationonherlefthandsideinpreviousyearsonafew
occasions,buthasalwaysmanagedthisseeingaphysiotherapist.Around4
monthsago,theonsetofplantarfasciitisinherleftfootforcedhertoseek
medicalhelpasthepainbecamesoseverethatshecouldnolongerwalkaround
withoutextremediscomfort.Shewasclearedandadvisedtostartundertaking
PilatesinlateSeptemberwhenshewasreferredtothestudio.Wearenow12
sessionsinandshehasmadehugeprogressintermsofre-balancingherbody.Of
herlowerlimbs,herleftsideisstrong(andclearlytakesthebruntofimpact
whenrunningandwalking)whilstherrightsideisveryweakthroughthefoot-
ankle,kneeandevenhip.Shehasaslightanteriorpelvictiltandishavingto
consciouslyworkonherpelvicengagementtore-alignthis.Hertransverse
abdominusrequiressomeextraattention,butotherwisehertrunkstabilization
andoblique/rectusabdominusstrengthisgood.Shecarriesverylittleexcess
weight;sheisgenerallyflexibleandisincrediblyfitasidefromhercurrent
plantarfasciitisissue.Herlumbarspinearticulationislimitedbutshehasno
lowerbackpain.Therestofherspinearticulateswellandherupperbodyis
strong.Intermsofherlowerextremity,heradductorsareweakandneedtobe
trainedtoengage(forexampleduringpelviccurlsandanyexerciseswithlegson
tabletop).Hercalvesareverytightonbothlegs,butmoresotheleft.Herleft
footalsohasquiteaseveresupinationduringmovement.Shecurrentlydirects

10
moreweightthanusualintotheballofherleftfoottocompensateforthepainin
herheel,whichhasstartedtoslightlyliftherlefthipupwards,andthisneedsto
beobservedcloselyduringsessionstoensureincorrectmusclepatternsarenot
adapted.
AconditioningprogrammeusingtheBASIBlockSystemisbeingusedtowork
withAlice’sbodyholistically.ThetenBASIprinciplesofawareness,balance,
breath,concentration,centre,control,efficiency,flow,precision
andharmonyarebeingutilizedandAliceisparticularlyreceptiveto
concentration,control,breathandflow.Shedoes,however,understandan
increasedneedforprecisionandbalance(inparticular)tocorrectherissue.
HercurrentsessionsfollowtheBASIblocksystemandfocusonexerciseswithin
eachblockthatwillalsotargetherissueareasof:
- Foot-anklealignment(leftsupination),strengthandstretching
- Encouragementofperonealengagementontheleft
- Encouragementofadductorengagementonbothlegs
- Calf,archoffootandAchillesstretching
- Rebalancingoflowerextremities(leftdominant)
- Realignmentofslightlefthipcompensation
- Correctionofanteriortiltandencouragementofpelvicengagement
- Transverseabdominusstrengthening
- Increasinglumbarspinearticulation

11
ConditioningProgramme
Note:repsshouldbeslow,controlledandchoreographedwithbreathing
BASIBlock Apparatus Exercise(s) NotesWarm-up Mat/
Cadillacbed
Pelviccurl,Spinetwistsupine,Chestlift,Chestliftwithrotation6repseach
Checkpressingequallythroughthefeet,watchkneesdon’textend
outwards,kneesandanklestogetherandlevelinSpinesupine
twist
Footwork Reformer3red
Parallelheels,paralleltoes,V-positiontoes,OpenV-position
heels,OpenV-position
toes,Calfraises,Prances,
Prehensile(ifcomfortable),Singlelegheels,Singlelegtoes6-8repseach
Watchfootalignment(especiallyleftsupination)andweight
placement,ensurecorrectflexionineachposition,checkfoot-ankle-
knee-hipalignment,engageadductorsandhipadductors
whenkneesexternallyrotated,incalfraises,usethefullrangeof
anklemotionthroughthesubtalarjoint,inprehensilewrapthefeetandreachtheheelsunderthebar,
insinglelegmaintainpelvicstabilityandcorrectfoot-ankle-knee-hipalignment-especiallyon
weakerleg
Abdominalwork
Reformer1red+1blue
Hundred,Co-ordination8repseach
Pelvic-lumbarstabilisation,usedeepabdominalstoliftheadandchest,neckinlinewithspine–notension,imprintlowerback,adductorsactivated,kneesandanklesgluedtogetheruntilstrongandpreciseopen-closeinco-
ordination
Hipwork Cadillac2yellow
Frog,Hipcircles(down,up),
Walking,Bicycle10repseach
Encourageequalandlevelmovementthroughbothhipsandlegs–watchingdominantvsweak
side,watchlefthipraising,lengthenthroughleftside,ensurepelvisremainsstableandsacrum
onthebed
Spinalarticulation
Cadillac1red
Monkey,Tower
prep/Tower6-8repseach
Watchfootalignmentindorsi/plantarflexionthroughout,
controlwithtransverseabdominals

12
Stretching Reformer1red
Standinglunge6-8repseach
side
Guidepelvicmovementalonghorizontallinefromposteriortoanterior,hipslevel,knees/anklesalignedwithhip,dorsiflexfootonsupportinglegwheninhamstringstretch-watchingsupination,
long,flatspine
FullBodyIntegration
Reformer1red+1blue
Stomachmassageround
back10-12reps
Ccurvespine&neck,shouldersabovehips,watchfootalignmentindorsi/plantarflexionatstraight
leg
Armwork Wundachair
1/2or2/2triceps
3/2or3/3backwardfacingdips
Tricepsseated,Backwardfacing
dips2xsetsof8-10
each
Longspine,trunkengagementandstabilisation,engagelegsandankles-feet,kneestogether,wideandstablescapuli,elbowparallel
Legwork Wundachair0/2
Legpressstanding12-15reps
Strongplantarflexion,pressthroughallmetatarsalsequally,ensurefoot-ankle-knee-hip
alignment,pullupthroughcore
Lateralflexion&rotation
Wundachair
0/2or0/1
Sideover8-10repseach
side
Legsandpelvisstable,anchorfootofthestraightlegonthefloor,lengthenequallythroughhiponeachside,workincoronalplane
only
Backextension
Wundachair
2/2or1/2
Basicswan Trunkstabilisation,abdominalengagement,legsengagedandparalleltofloor,kneesandfeet
gluedtogether,feetstrongplantarflexion,pressintopedaltowiden
shouldersaslift
Conclusion
ThisprogramshouldsignificantlyimprovethestrengthandalignmentofAlice’s
lowerextremities–especiallythefoot-anklearea-throughaspecificfocuson
recruitmentofthemajorlegmuscles(quadriceps,hamstringsand

13
gastrocnemius)aswellasspecificsmallermusclesinandaroundthesubtalar
joint.Itisalwaysimportanttoworktowardsbalancedmovementacrossthe
wholebody,despitespecificareaissuesandinadditiontothis,breathingand
mind/bodyawarenessshouldbeencouraged.Tailoredsessionswillensure
optimalimprovementinAlice’sconditionandthiswillalsobeverymuch
dependentonstrongobservationandattentiontodetailbytheinstructorwithin
thesessions.

14
Bibliography
Beeson,P.“PlantarFasciopathy:revisitingtheriskfactors.”FootandAnkleSurgery.September2014.20:160-5
“BodyMaps–PlantarApneurosis.”Healthline.HealthlineMedia,Web.Copyright
2016.http://www.healthline.com/human-body-maps/plantar-aponeurosis
Isacowitz,Rael.Pilates:SecondEdition.USA:HumanKinetics,2014.
Isacowitz,Rael.StudyGuide:ComprehensiveCourse.CostaMesa,California:BodyArtsandScienceInternational,2013.
“PlantarFasciaAnatomy.”DocPods.DocpodsPtyLtd,Web.Copyright2016.
http://www.docpods.com/plantar-fascia-anatomy
Patterson,J.TeachingPilatesforPosturalInjuriesandFaults:APracticalGuide.Oxford,UK:Butterworth-Heinemann,2010.
Williams,P.L.,Warwick,R.Gray’sAnatomy.Philadelphia:WBSaunder;1980.
36:612-613