acute lymphoblastic leukemia maggie davis hovda 5/26/2009
TRANSCRIPT
Acute Lymphoblastic LeukemiaMaggie Davis Hovda
5/26/2009

Definition
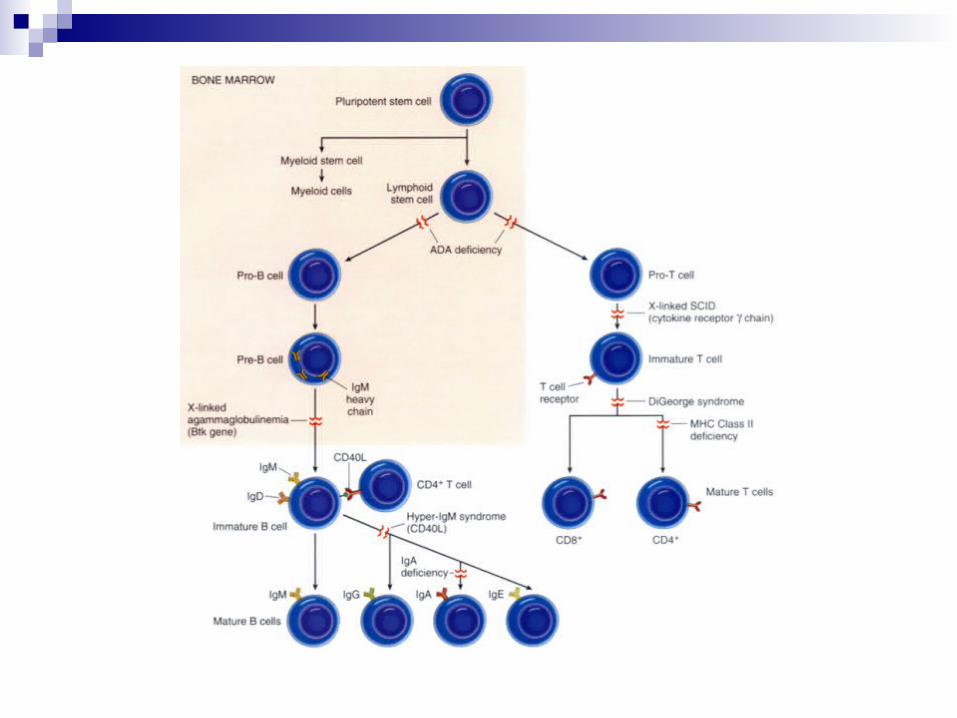
Neoplastic disease which results from a mutation in a single lymphoid progenitor cell at one of several discrete stages of development
B Cell or T Cell

Epidemiology
Most common childhood acute leukemia, ~80%
Incidence in adults ~20% Bimodal distribution of occurrence:
Peak at age 2-5Second increased incidence after age 50
Pathogenesis
Acquired Genetic Change in Chromosome Change in number, ie ploidy Change in structure
Translocations (most common) Inversions Deletions Point mutations Amplifications
Changes in normal means of cell differentiation, proliferation, and survival

Mechanisms of Leukemia Induction
1 – Activation of a proto-oncogene OR creation of a fusion gene with oncogenic properties
- Ph Chromosome t(9;22)
2 – Loss or inactivation of ≥ 1 tumor suppressor gene
- p53 (p16 mutation)

Etiology
Unknown ? Genetic Predisposition
Increased incidence amongst monozygotic and dizygotic twins Down Syndrome Disorder with chromosomal fragility:
Fanconi’s anemia Bloom Syndrome Ataxia-Telangiectasia
? Infections HTLV1 in T cell leukemia/lymphoma EBV in mature B cell ALL HIV in lymphoproliferative DO
Presentation
Nonspecific Symptoms Fatigue/decreased energy Fever Easy bruising Bleeding Dyspnea Dizziness Infection
Joint, extremity pains CNS involvement

Clinical Presentation
Physical Exam Pallor Ecchymoses Petechiae LAD Hepatosplenomegaly
Lab Abnormalities anemia wbc vary
0.1 (20-40%) - >100 k (10-16%)
Platelets – usually ↓ ↑ LD, uric acid CXR: eval for thymic mass CSF to eval for
involvement

Diagnosis
MorphologicFrench American British Classification
L1: small uniform blasts (pediatric ALL) L2: larger, more variable sized blasts (adult ALL) L3: uniform cells with basophilic and sometimes
vacuolated cytoplasm (mature B cell ALL)

Immunophenotyping
From: Jabbour, E. et al. Adult Acute Lymphoblastic Leukemia. Mayo Clinic Proc. 2005;80(11):1517-1527

Cytogenetic Abnormalities
From: Jabbour, E. et al. Adult Acute Lymphoblastic Leukemia. Mayo Clinic Proc. 2005;80(11):1517-1527

Classification of ALL
Immunologic Subtype
% of cases FAB Subtype Cytogenetic Abnormalities
Pre-B ALL 75 L1, L2 t(9;22), t(4;11), t(1;19)
T cell ALL 20 L1, L2 14q11 or 7q34
B cell ALL 5 L3 t(8;14), t(8;22), t(2;8)
From: Harrison’s Principles of Internal Medicine, 16th ed. 2005. Chapter 97, Malignancies of lymphoid cells.

Differential Diagnosis
ITP Aplastic Anemia Infectious mononucleosis Rheumatoid Arthritis Rheumatic Fever Collagen Vascular Disease
Treatment
1 – Remission Induction 2 – Intensification (Consolidation) Therapy 3 – Maintenance Therapy 4 – CNS Prophylaxis 5 – Allogeneic Stem Cell Transplant

Treatment
Remission Induction Goals: restore normal hematopoiesis, induce a
complete remission rapidly in order to prevent resistance to drugs
Standard induction regimen 4 or 5 drugs: vincristine, prednisone, anthracycline, L-
asparaginase, +/- cyclophosphamide
Intensification High doses of multiple agents not used during
induction or re-administration of the induction regimen

Treatment
Maintenance Therapy Daily po 6MP, weekly MTX, monthly pulses of
vincristine and prednisone for 2-3 yrs
CNS Prophylaxis Given during induction and intensification Intrathecal: MTX, Cytarabine, corticosteroids Systemic: high dose mtx, cytarabine, L-asparaginase +/- Cranial Irradiation
Treatment
Stem Cell Transplant Done during first CR Indications:
Ph Chromosome t(4;11) mutation Poor initial response to induction therapy
Other Adolescents benefit significantly from pediatric ALL
regimens vs. adult regimens

Relapse & Prognosis
Relapse Most occur during treatment or within the first 2 years Bone Marrow is the most common site Poor prognostic factors in patients previously treated:
Relapse on therapy Short initial remission after intense therapy T-cell immunophenotype Ph Chromosome Circulating blasts High leukocyte count at relapse
Prognosis
Overall better in children than in adults In adults, worse outcomes with:
Increasing age, >60 Increased wbc count at presentation
Sources
Jabbour, E. et al. Adult Acute Lymphoblastic Leukemia. Mayo Clinic Proc. 2005;80(11):1517-1527
Xavier, T. Chemotherapy of acute leukemia in adults. Expert Opin. Pharmacother. (2009) 10(2):221-237
Williams Hematology, 6th ed. 2001. Chapter 97, Acute Lymphoblastic Leukemia.
Harrison’s Principles of Internal Medicine, 16th ed. 2005. Chapter 97, Malignancies of lymphoid cells.