acupuncture treatment for parkinson s disease · researchers would accept the acupuncture therapy...
TRANSCRIPT

See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/261706011
Acupuncture Treatment For Parkinson’s Disease
Chapter · July 2012
DOI: 10.1007/978-1-4614-3357-6_7
CITATIONS
5
READS
3,204
Some of the authors of this publication are also working on these related projects:
Treatment strategy for elderly patients View project
All content following this page was uploaded by Tetsuya Asakawa on 18 April 2014.
The user has requested enhancement of the downloaded file.

215Y. Xia et al. (eds.), Current Research in Acupuncture, DOI 10.1007/978-1-4614-3357-6_7, © Springer Science+Business Media New York 2013
Abstract Acupuncture is widely accepted as an alternative therapy for Parkinson’s disease (PD) in East Asia. The aim of this chapter is to review the current progress of the clinical and experimental acupuncture studies. A number of clinical studies in China and Korea proved that the ef fi cacy of acupuncture lies in improving the motor impair-ments and complications of PD and reducing the long-term medical side effects; how-ever, certain problems in the study design possibly exaggerated the ef fi cacy of acupuncture and crippled the power of these evidences. More strictly designed clinical studies following the principles of randomization, control, double blindedness, and placebo are needed, to furnish powerful evidence in order to verify the ef fi cacy of acupuncture. Several bench studies have tried to clarify the proposed mechanisms of acupuncture therapy like delaying the dopamine (DA) neuron depletion, improving the dopaminergic (DA-ergic) system in the PD state, neuroprotective effects, amelioration of the motor control network in the basal ganglia, and to attenuate the oxidative stress in PD state. The limited present-day bench studies still have not been able to provide suf fi cient evidence for revealing the secrets of acupuncture. At the end of this chapter, a new experimental strategy has been introduced. On combining the basis of the traditional acupuncture theory with the observation that the stimulation of the somatosensory pathways affects the cerebral DA level, a modi fi ed electroacupuncture method—the
T. Asakawa (*) Department of Neurosurgery , Hamamatsu University School of Medicine , Handayama, 1-20-1 , Higashi-ku, Hamamatsu-city, Shizuoka 431-3192 , Japan e-mail: [email protected]
Y. Xia (*) Department of Neurosurgery , The University of Texas Medical School at Houston, Houston , TX 77030 , USA
The University of Texas Graduate School of Biomedical Sciences at Houston , Houston , TX 77030 , USA
Yale University School of Medicine, New Haven, CT 06520, USA e-mail: [email protected]
Chapter 7 Acupuncture Treatment for Parkinson’s Disease
Tetsuya Asakawa and Ying Xia

216 T. Asakawa and Y. Xia
so-called super fi cial electrical stimulation (SES), is proposed. We hope that general PD researchers would accept the acupuncture therapy to a greater extent in the future.
Keywords Parkinson’s disease • Acupuncture • Acupoint • Dopamine neuron • Degeneration • Neuroprotection • Deep brain stimulation • Motor control network • Basal ganglia
7.1 Introduction
Parkinson’s disease (PD), fi rst reported by James Parkinson in 1817, is a neurode-generative disorder that results from a progressive degeneration of striatum-projecting dopamine (DA) neurons in the substantia nigra pars compacta (SNpc) manifesting as static tremor, rigidity, bradykinesia, gait dysfunction, and postural instability (Hirsch et al. 1988 ; Przedborski 2005 ; Parkinson 2002 ) . PD is classi fi ed as the sec-ond most common neurodegenerative disease following the Alzheimer’s disease (AD), with a lifetime risk of 2 % (Schapira 2009 ) . The pathogenesis involved in PD onset is still unclear. However, it is generally accepted by most of the authors that the probable mechanisms lie in the genetic factors and environmental toxins (George et al. 2009 ; Schapira 2009 ) (Fig. 7.1 .)
At present, there is no satisfactory therapy for PD. The available traditional treat-ment options include medical and surgical therapies. The medical therapies at hand
Fig. 7.1 The possible mechanisms involved in the PD pathogenesis

2177 Acupuncture Treatment for Parkinson’s Disease
include: (1) Administration of levodopa ( l -dopa), which is the most useful drug for idiopathic PD; (2) Direct agonists of DA-ergic receptors administration, such as selective D
2 receptor agonists like bromocriptine; D
1 - and D
2 -receptor agonists like
pergolide; (3) Administration of monoamine oxidase-B (MAO-B) inhibitors such as rasagiline and selegiline, which were reported to possess additional neuroprotective and anti-apoptotic effects (Lam et al. 2008 ; Palhagen et al. 2006 ) ; (4) Other medications such as amantadine, anticholinergic medications (artane), etc., are known to ef fi cacious as well. The main mechanism of the drug therapy is correction of the abnormal catecholamine metabolism and enhancing the DA-ergic effects on the pre/postsynaptic structures. The most commonly used neurosurgical treatments include primitive surgical ablation (pallidotomy or thalamotomy) and high-frequency deep brain stimulation (DBS) of certain structures such as subthalamic nucleus (STN). The exact mechanisms of surgical ablation and DBS are still unclear. STN plays a critical role in the basal ganglia and thalamocortical circuitry (Fig. 7.2 .). Anatomically, it acts as an input and output station for basal ganglia. The STN receives g -aminobutyric acid (GABA)-ergic input from the external segment of the globus pallidum (GPe) and sends the excitatory glutamatergic output to GPe, substantia nigra pars reticulate (SNpr), and the internal segment of the globus pal-lidum (GPi). In PD state, the overactive STN inhibits the thalamus through the hyperdirect and indirect pathways that are regarded as the key elements of motor control network in the basal ganglia. Then, the outputs from the thalamus become inhibitory, thus causing motor impairments. It is hypothesized that unilateral surgi-cal ablations break the circuits, while DBS corrects the overactive state of STN in PD patients. In early studies, high-frequency stimulations of the STN reportedly
Cx
STN GPe
GPi/SNr
Th
Str
hyperdirectpathway
(glu)
(glu)
(glu)
(glu)
(GABA)
(GABA)
(GABA)
(GABA)
(GABA)
indirect pathway
direct pathway
Fig. 7.2 The motor control network in basal ganglia (Nambu et al. 2002 )

218 T. Asakawa and Y. Xia
caused inhibition of the STN itself or of the GPi and SNr. The inhibition caused by high-frequency stimulations seemed to be in reasonable accordance with Alexander–DeLong diagram. Recently, Hashimoto et al. and Nambu et al. have shown that high-frequency STN stimulation does not simply inhibit the GPi, but rather excites or causes an excitation–inhibition–excitation pattern in the GPi (Alexander et al. 1986, 1990 ; Fang et al. 2006a ; Hashimoto et al. 2003 ; Nambu et al. 2002 ) .
Recently, newer therapies such as stem cell transplantation and gene therapy have been developed. Stem cell transplantation is also considered as a promising new therapy for PD. The research on stem cell transplantation as a prospective PD therapy has boomed with the introduction of induced pleuripotent stem (iPS) cells, and has also successfully resolved the issue regarding the supply of stem cells. Some groups have reportedly succeeded in inducing the embryonic stem cells (ES cells) into DA neurons in vitro with a high success rate (Kim et al. 2002 ) . However, the main dif fi culties lie with increasing the life of the induced neurons and reducing the cancerous trend in vivo. Stem cell transplantation still has a long way to go to mature into an established therapy that could be effectively used for the cure of patients. Gene therapy is another upcoming strategy, albeit only a few genes includ-ing a -synuclein (PARK1) and Parkin (PARK2) have been deeply investigated in the animal PD models (George et al. 2009 ) . With the increasing knowledge of the vital genes involved in the neurodegenerative process, gene therapy has also developed considerably. An important aspect of gene therapy is increasing the gene expression of certain neurotrophic factors. It has been reported that a reduction in certain neu-rotrophic factors can possibly cause DA neuron degeneration. Some authors found that the administration of brain-derived neurotrophic factor (BDNF) was bene fi cial for the survival of the DA neurons and protected them from injury by neurotoxins, both, in vivo and in vitro (Frim et al. 1994 ; Shults et al. 1995 ; Spina et al. 1992 ; Liang et al. 2002 ) . The Glial cell line-derived neurotrophic factor (GDNF) is another important neuroprotective factor reported to increase the survival rate of a DA neuron in a neurotoxic environment (Burke et al. 1998 ; Clarkson et al. 1999 ) . However, different clinical trials using the same protocol of intra-putamen infusion of GDNF got inconsistent results, which indicates the need for veri fi cation of the ef fi cacy of GDNF therapy (Lang et al. 2006 ; Gill et al. 2003 ; Slevin et al. 2005 ) . Another nota-ble observation of gene therapy is the increase in GABA-ergic effects in STN with an increased expression of GABA-ergic genes. Multiple evidences have indicated that increased GABA-ergic effects in STN can bring about an improvement in the symptoms of Parkinson’s disease (Kaplitt et al. 2007 ; Levy et al. 2001 ; Windels et al. 2005 ; Feigin et al. 2007 ) . It was observed that with the transfer of glutamic acid decarboxylase (GAD) gene by adeno-associated virus (AAV) into the STN of patients with Parkinson’s disease, the symptoms of these patients improved with an associated upregulation of GABA expression in STN (Kaplitt et al. 2007 ) . Based on the excitatory/inhibitory mechanisms involved in the basal ganglia (Nambu et al. 2002 ) , microinjection of a drug or drug combination at the stations of the motor control network is potentially a new therapy, e.g., using GABA agonist or/and glutamate inhibitor at STN, GPi, or striatum; or using GABA inhibitor or/and glutamate agonist at the thalamus and GPe. There are several other therapies under development

2197 Acupuncture Treatment for Parkinson’s Disease
including anti-oxidant treatment, neuroprotective treatment, and metal dysregulation treatment such as improvement of the metal-associated protein (Ferritin), metal chelation therapies, and metal protein attenuating compounds (MPAC) (George et al. 2009 ) . The ef fi cacy and safety of these therapies is arguable and therefore needs to be veri fi ed by more clinical and bench investigations.
However, there are several limitations to the above strategies that make PD an intractable disease. (1) The limitation of the symptomatic therapy : Except some uncertain neuroprotective roles of the neurotrophic factors and the stem cell transplanta-tion, both mature medical and surgical strategies, nowadays, are chie fl y symptomatic therapies and have a little ef fi cacy on stopping the neurodegenerative process (Hilker et al. 2003, 2005 ) . (2) The long-term ef fi cacy is unfavorable : The most effective therapy till now, i.e., l -dopa administration, is well known for its “wearing off” phenomenon, which means the ef fi cacy of l -dopa weakens with the progression of PD and the dose of l -dopa has to be increased in order to maintain the same ef fi cacy, however, along with the side effects. The long-term ef fi cacy of DBS is also controversial. Though many reports suggest that DBS is a bene fi cial long-term treatment (Kleiner-Fisman et al. 2003 ; Krack et al. 2003 ) , yet the battery life of the stimulator and its side-effects have to be taken into account. (3) Cost and risk associated with the surgical therapies are the limitations that signi fi cantly affect a patient’s selection of surgical treatment as the preferred modality, especially, in a developing country which lacks a good health insurance system. (4) In advanced-stage PD patients, as the disease symptoms progress along with the accumulation of motor side-effects of l -dopa, the motor impairments get further complicated, intractable and sometimes, incurable.
In view of the above limitations, to maintain a good motor function and long-term medical ef fi cacy, most of the patients undergo comprehensive treatments (e.g., l -dopa plus MAO-B inhibitor, l -dopa plus DBS, etc.), which are analogous to the drug cocktail therapy of AIDS. In this context, some alternative therapies are being adopted. It was reported that 40 % of the PD patients in the USA and 38.7 % in the UK underwent complementary and alternative medical therapies, of which 7–10 % patients had selected acupuncture (Rajendran et al. 2001 ; Ferry et al. 2002 ; Lam et al. 2008 ) . Indeed, acupuncture is widely used as an adjuvant in the treatment of PD in East Asia including China, Japan, Korea, and Singapore. It is thought to bene fi t by improving the symptoms and complications of PD.
7.2 Clinical Application of Acupuncture in PD
Substantial evidence suggests that acupuncture can stimulate peripheral nerves (Zhou et al. 2010 ) and thus generate neural signals to regulate the activities of neu-rotransmitter systems, including the synthesis and release of dopamine system, in the central nervous system (Wen et al. 2010a, b ) . Therefore, acupuncture is broadly used in the treatment of neurological diseases (Xia et al. 2010 ) such as stroke (Guo et al. 2010 ) and other cardiovascular disorders (Kang and Xia 2010a, b ) in clinical settings, especially in oriental countries.

220 T. Asakawa and Y. Xia
PD had been reported in an ancient classic of traditional Chinese medicine (TCM)—The Yellow Emperor’s Inner Classic (Huangdi Neijing), nearly 2,000 years ago. It was believed that the tremor was derived from the “liver dysfunction” according to the TCM theory, and the stiffness was caused by the over strong element, “wind.” In the current TCM theory, the pathogenesis of PD lies in the weakness of “qi and blood,” insuf fi ciency of the “liver” and “kidney” (in the TCM theory) and inner movements of wind and phlegm. Acupuncture use in the treatment of PD has a long history in the East Asian countries of China, Japan, Korea, and Singapore. Liu, in 1974, fi rst reported the application of acupuncture in central nervous system disorders, including PD (Liu and Sadove 1974 ) .
The various styles of acupuncture involved in treating PD include scalp acupuncture, body acupuncture, electroacupuncture (EA), alternative acupuncture, and combina-tion therapy. A typical acupuncture operator always learns the techniques from a predecessor teacher or from the classics of TCM and then gathers experience by treating patients. The traditional pattern and practice of the acupuncture have lead to a lack of objective standard in diagnosis and therapy. The selection of therapy styles usually depends upon the operator’s experience (sometimes arbitrary prefer-ence) rather than an objective standard, which is considered as a drawback of all traditional medicines.
Compared to the diseases such as stroke (and its sequelae) (Guo et al. 2010 ) , spinal injury, and Bell’s palsy for which acupuncture is more widely used, acupuncture is always selected as a complementary therapy in most of the PD cases to optimize the ef fi cacy/dose of DA-ergic treatments, to reduce the side-effects, or to improve the motor de fi cits. Currently, there is no report available that suggests adoption of acupuncture as an independent main therapy for PD in the clinical practice. Although most authors of the traditional medicine from China and Korea believe in the ef fi cacy of acupuncture, some authors consider the role of acupuncture in treatment of movement disorders, especially PD, as quite a limited one (Shulman et al. 2002 ; Lam et al. 2008 ; Lee et al. 2008 ; Cristian et al. 2005 ) . In the following sections, we try to provide an objective overview on these studies, rather than drawing a conclu-sion for disputation.
7.2.1 Scalp Acupuncture
With regard to the acupuncture treatment for PD, the scalp acupuncture is undividedly accepted to hold the highest status. It is a common belief of many Chinese investiga-tors that scalp acupuncture can achieve much better results more swiftly when compared to other routes. There are two methods to stimulate the scalp acupoints. One is to insert and operate the needles manually and another is to use electroacu-puncture (EA). As manual acupuncture relies more on the therapists’ experience, therefore, EA stimulation has become much more popular in the recent years (EA is discussed in Sect. 7.2.3 ).

2217 Acupuncture Treatment for Parkinson’s Disease
The acupoints are selected based on the theory of differential symptoms (Bian-Zheng-Shi-Zhi) of TCM. Stimulation of the scalp acupoints has an overall effect of “calming the liver wind” that is believed to bene fi t the symptoms of tremor and stiffness. The so-called Chorea-Tremor controlling area (CTCA)— fi rst described by Dr. Sunfa Jiao in 1975, is regarded as the most important scalp acupoint for treating the extra pyramidal disorders including PD (Wang 2000 ) . Jiao de fi ned several scalp acupuncture controlling areas according to the cortex area extension line and clinical experience. The most important areas are the sensory controlling area (SCA), motor controlling area (MCA), and the CTCA (Fig. 7.3 ). It has been widely reported that stimulation of the CTCA improves the tremor and involuntary movements of the contralateral limbs (Shi et al. 2002 ; Wang 2000 ; Yu 1994 ) . Acupuncture at the CTCA along with other acupoints can achieve a better ef fi cacy. Shi reported that stimulating the CTCA together with SCA would bene fi t the sensory impairments, whereas stimu-lating the CTCA with MCA would improve the motor impairments (Shi et al. 2002 ) .
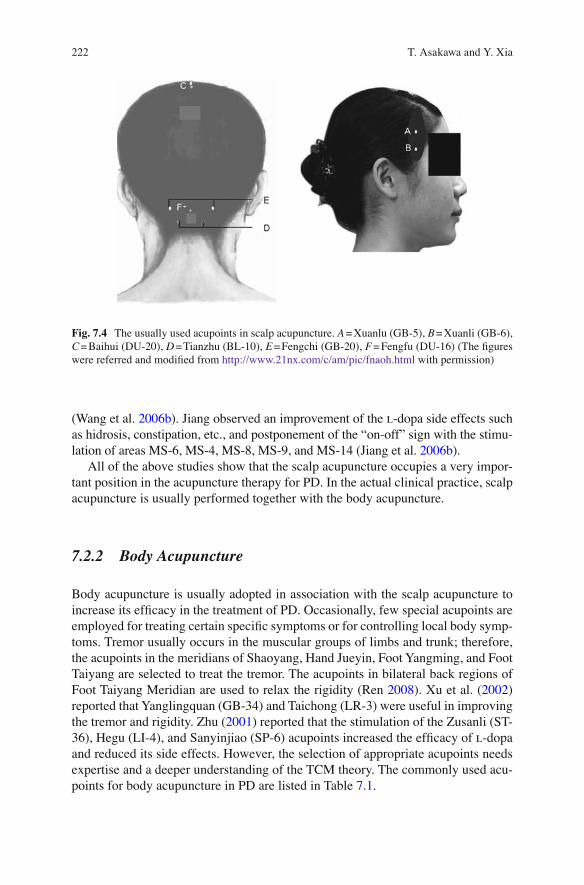
Other commonly used acupoints are shown in the Fig. 7.4 . Xi et al. ( 1996 ) , reported an improvement in the tremor myoelectric potential by electrical stimulation at the acupoint Baihui (DU-20) in Parkinson’s patients. Wang et al. reported that EA at the acupoints Xuanli (GB-6), Xuanlu (GB-5), Fengfu (DU-16), Tianzhu (BL-10), and Fengchi (GB-20) signi fi cantly improved the electromyography (EMG) ( Wang et al. 2003 ) , superoxide dismutase (SOD), and lipid peroxides (LPO) in the PD patients
Fig. 7.3 The Chorea-Tremor controlling area de fi ned by Dr Jiao Sunfa. A line depicts the sensory controlling area (SCA), which is at 2 cm posterior to the middle line of the skull. B line depicts the motor controlling area (MCA), which is at 0.5 cm posterior to the middle line of the skull and is considered as an extension line of the precentral gyrus. C line depicts the location of the Chorea-Tremor controlling area (CTCA), which is at 1.5 cm anterior to the B line (The fi gure was referred and modi fi ed from http://yibian.hopto.org/shu/?sid=8162 with permission)
222 T. Asakawa and Y. Xia
(Wang et al. 2006b ) . Jiang observed an improvement of the l -dopa side effects such as hidrosis, constipation, etc., and postponement of the “on-off” sign with the stimu-lation of areas MS-6, MS-4, MS-8, MS-9, and MS-14 (Jiang et al. 2006b ).
All of the above studies show that the scalp acupuncture occupies a very impor-tant position in the acupuncture therapy for PD. In the actual clinical practice, scalp acupuncture is usually performed together with the body acupuncture.
7.2.2 Body Acupuncture
Body acupuncture is usually adopted in association with the scalp acupuncture to increase its ef fi cacy in the treatment of PD. Occasionally, few special acupoints are employed for treating certain speci fi c symptoms or for controlling local body symp-toms. Tremor usually occurs in the muscular groups of limbs and trunk; therefore, the acupoints in the meridians of Shaoyang, Hand Jueyin, Foot Yangming, and Foot Taiyang are selected to treat the tremor. The acupoints in bilateral back regions of Foot Taiyang Meridian are used to relax the rigidity (Ren 2008 ) . Xu et al. ( 2002 ) reported that Yanglingquan (GB-34) and Taichong (LR-3) were useful in improving the tremor and rigidity. Zhu ( 2001 ) reported that the stimulation of the Zusanli (ST-36), Hegu (LI-4), and Sanyinjiao (SP-6) acupoints increased the ef fi cacy of l -dopa and reduced its side effects. However, the selection of appropriate acupoints needs expertise and a deeper understanding of the TCM theory. The commonly used acu-points for body acupuncture in PD are listed in Table 7.1 .
Fig. 7.4 The usually used acupoints in scalp acupuncture. A = Xuanlu (GB-5), B = Xuanli (GB-6), C = Baihui (DU-20), D = Tianzhu (BL-10), E = Fengchi (GB-20), F = Fengfu (DU-16) (The fi gures were referred and modi fi ed from http://www.21nx.com/c/am/pic/fnaoh.html with permission)

2237 Acupuncture Treatment for Parkinson’s Disease
7.2.3 Electroacupuncture
Recently, EA has become the most extensively used method in the treatment of PD via acupuncture and has a strong potential to replace the traditional manual acupuncture. EA stimulation is easier to manipulate than traditional manual acu-puncture. The parameter setting is relatively more objective and relies less on experience. Another advantage of EA, as accepted by many Chinese authors, is its safety. It is believed that EA causes less injury and side effects, thereby, increasing the level of its acceptability among the patients.
In contrast to the treatments with objective parameters setting such as DBS, there are great variations in the parameters selected by different therapists. The parameter setting relies on both, the experience of the therapist and the patient’s subjective experience. Nowadays, these have become more uniform as most of the investiga-tors have come to adopt the stimulation conditions listed in Table 7.2 (Jiang et al. 2006b ; Wang et al. 2003, 2006b ; Xi et al. 1996 ) .
7.2.4 Other Alternative Therapies Related to Acupuncture
In addition to typical acupuncture, some Chinese investigators selected other alternative therapies related to the classical acupuncture. Xu et al. ( 2002 ) injected Mailuoning , a mixture of several Chinese medicines, at Zusanli (ZT-36) and Yanglingquan (GB-34) acupoints in 23 PD patients. They got a total effectivity rate
Table 7.1 Commonly used acupoints for body acupuncture in the treatment of PD overviewed and summarized from the works of Ren ( 2008 ) , Lam et al. ( 2008 ) and Shulman et al. ( 2002 ) .
Meridians and collaterals Acupoints
Lung meridian of hand Taiyin (LU) Chize (LU-5) Large intestine meridian of hand Yangming (LI) Hegu (LI-4), Yangxi (LI-5), Quchi (LI-11),
Jianyu (LI-15) Stomach meridian of foot Yangming (ST) Zusanli (ST-36), Fenglong (ST-40), Jiexi (ST-41) Spleen meridian of foot Taiyin (SP) Sanyinjiao (SP-6), Yinlingquan (SP-9), Heart meridian of hand Shaoyin (HT) Shaohai (HT-3), Small intestine meridian of hand Taiyang (SI) Yanglao (SI-6), Jianzhen (SI-9), Bladder meridian of foot Taiyang (BL) Yuzhen (BL-9), Chengfu (BL-36), Weizhong
(BL-40), Kunlun (BL60) Kidney meridian of foot Shaoyin (KI) Taixi (KI-3), Dazhong (KI-4), Yingu (KI-10) Pericardium meridian of hand Jueyin (PC) Quze (PC-3), Neiguan (PC-6), Daling (PC-7) Triple energizer meridian of hand Shaoyang
(TE) Yangchi (TE-4), Jianliao (TE-14),
Gallbladder meridian of foot Shaoyang (GB) Huantiao (GB-30), Yanglingquan (GB-34) Liver meridian of foot Jueyin (LR) Taichong (LR-3), Zhongfeng (LR-4), Meridians of hand Shaoyang (SJ) Waiguan (SJ-5) Du channel (DU) Yaoyangguan (DU-3), Xuanshu (DU-5),
Jizhong (DU-6), Lingtai (DU-10), (DU-17), Extra points Jiaji (EX-B-2)

224 T. Asakawa and Y. Xia
of 65 % from the injection of these acupoints. They also found that the acupoints’ injection brought about an alteration in the monoamine neurotransmitters in the cerebrospinal fl uid (CSF); however, these variations were not signi fi cantly corre-lated to the ef fi cacy. Zhang et al. ( 2005 ) performed herbs-partitioned moxibustion at the Shenque (CV-8) in 54 PD patients who were undergoing the classical medicine treatment, and compared them to 36 PD control patients who received only classical medicine. They found that there were signi fi cant improvements in PD rating scales in the patients of treatment group than the controls (those who only received classi-cal medicine treatment). Therefore, they concluded that herbs-partitioned moxibus-tion was an effective therapy for PD. Huang ( 2000a, b ) performed eye acupuncture, which is a special method of acupuncture that stimulates certain areas around the eyes, on 45 patients (37 primary PD cases and 8 Parkinsonism cases). She compared the scores of the Chinese PD rating scales before and after eye acupuncture, and found signi fi cant improvements in 40 cases. She also found a better ef fi cacy in the early-stage PD patients (Huang 2000a ) . There are several other alternative methods to stimulate the acupoints such as, bloodletting therapy (Wang 2000 ) ; stimulation of the special areas in ear—presumably the same as those used for brain mapping (Su 2002 ) ; acupuncture based on the theory of strengthening the body by corresponding the Taiji structure in man and the universe (Qi and Wang 2007 ; Wu 2002 ) ; and stimulation of the acupoints by Dianxue, which is a special method to hit speci fi c acupoints (Wu et al. 1996 ; Dai 2004 ) .
The methods described above are the “alternative” therapies in the acupuncture, which in itself is considered as an “alternative” therapy for PD. Such treatments rely to a great extent on experience and lack suf fi cient objectivity that could verify their ef fi cacy. If an investigator wants to evaluate a new therapy, he must provide enough believable evidence to prove the ef fi cacy and safety. This issue is discussed in the Sect. 7.2.6 .
7.2.5 Combination Therapy
The l -dopa administration is still regarded as the most effective therapy for PD. It is for this reason that all the other therapies are based on their effects on l -dopa whether they prolong the effective period of l -dopa, reduce its dose, increase its
Table 7.2 Commonly adopted EA stimulation conditions by the Chinese therapeutists
Parameters Data
Depth from the skin 30–40 mm Frequency 2–100 Hz Current intensity Top strength endured by the patient Wave Pattern Condensation wave or disperse-dense wave Time of one therapy Stimulation for 30 min, retaining the needle for 60 min,
one therapy per day Time of the whole course 30 days (consecutive or consecutive 5 days with a 2-day
interval on the weekends) Diameter and material of the needle 0.3–0.4 mm, stainless steel

2257 Acupuncture Treatment for Parkinson’s Disease
ef fi cacy, abate the side effects, or ameliorate the complications and rehabilitation in the advanced-stage PD cases. Except a few studies, which adopted acupuncture as a temporary monotherapy for a limited experimental period in order to clarify the acupunctural mechanism (Wang et al. 2000 ) , we did not fi nd a single report in the available English and Chinese literature that adopted acupuncture as a unique main treatment even in the early-stage mild PD patients in the actual clinical practice. This shows that acupuncture is chie fl y used as an alternative treatment for PD. The meaning of “combination therapy” in this section refers to the combination of different styles of therapies offered in TCM.
Most of the acupuncture therapists adopt the combination therapy in real-time clinical practice. The commonest combination is the scalp acupuncture plus body acupuncture. First, the area for scalp acupuncture is selected, which is almost always CTCA (the most important area) although the MCA and SCA are also considered as per the symptoms. Next, the acupoints for the body acupuncture are selected. Since each individual PD patient is different from another, the acupoint selection also presents a great individuality. All the acupoints must be selected based on the theory of differentiate symptoms in the TCM. Therefore, the step of acupoint selection is of vital importance and needs an in-depth understanding of the TCM theory along with an excellent experience in acupuncture. The most commonly used acupoints for body acupuncture are listed in the Table 7.1 .
Another widely used combination is the acupuncture and TCM. Liu and Li ( 2001 ) compared the ef fi cacy of the acupuncture therapy with the surgical therapy via ventral pallidotomy. They performed scalp acupuncture at CTCA and MS6, and administrated a mixture of several Chinese medicines including Tianma (rhizome-gastrodiae), Gouteng (uncaria), Zhenzhumu (mother of pearl), and Jiangcan (cicada) in the TCM group. They found that both the therapies signi fi cantly improved the PD symptoms. The effects of surgical operation presented sooner but were accompa-nied with severe side effects as well. In contrast, the onset of the effects in the TCM group was late but associated with fewer side effects. Zhu ( 2001 ) used scalp acu-puncture at CTCA combined with several Chinese herbal medicines for PD patients who were receiving normal l -dopa therapy. They found that in comparison with the patients receiving regular treatment with l -dopa, the patients receiving a lower dose of l -dopa plus acupuncture and Chinese herbal medicines achieved the same ef fi cacy. Li and Yang ( 2005 ) treated PD with comprehensive therapies. Fifty- fi ve patients were divided into two groups at random. The control group underwent only l -dopa administration and the treatment group additionally underwent the compre-hensive treatments, including both body and scalp acupuncture, and the Chinese medicine (i.e., pills of six ingredients with rehmannia plus Zuogui pills). He did not fi nd any signi fi cant difference in the total scores on the PD rating scale between the two groups after treatment. The treatment group got the same ef fi cacy as the control group; however, the dose of l -dopa in the treatment group was signi fi cantly lower than that of control group.
The reports above indicate that the combination therapy is a successful strategy for acupunctural treatment of PD. More and more western clinicians have now accepted acupuncture as one of the plausible options in treating the intractable,

226 T. Asakawa and Y. Xia
advanced-stage PD patients, as it is indeed a prickly endeavor to choose an effective method that can bring further improvements. For some terminal stage PD patients, on whom all the classical therapies have been exhausted, acupuncture might be the last ray of hope, at least in bringing psychological comfort to the patient and his family.
7.2.6 Comments
7.2.6.1 Factors that In fl uence the Acupuncture Ef fi cacy
Most of the current studies focus on the validation of the ef fi cacy of acupuncture as an alternative therapy for PD. There is no enough information yet on the ef fi cacy of acupuncture in different conditions (e.g., during the different EA parameters, selec-tion of the patients, acupoints selection, and so on), which is necessary to delineate the factors that might in fl uence the ef fi cacy of acupuncture. Here, we try to sum-marize the in fl uence factors based on data currently available in the literature.
(a) Stage of the patients: Several studies have reported that acupuncture has a better ef fi cacy in early-stage PD than the advanced stage (Ma 1999 ; Wang 2000 ; Jiang et al. 2006b ; Liu and Ren 1993 ) . This tendency shows a trend comparable to other therapies such as DBS and Medical.
(b) Clinical subtype of PD: A good ef fi cacy was observed in the younger patients with chief symptoms of tremor or rigidity and who had lesser complications. Poor ef fi cacy was noted in those who were old, suffered from more complica-tions, and those who had Parkinsonism (Liu and Ren 1993 ) ; however, as per the results obtained by Wang, there was no signi fi cant difference among the patients based on their presenting symptoms (Wang 2000 ) . The con fl ictive results make it dif fi cult to draw any conclusions. Further studies are therefore required to shed more light on this issue.
(c) Protocol of acupuncture: Since PD is a progressive disease with a long course, protocol selection is crucial for improving the ef fi cacy. Xi and Cai ( 1995 ) pro-posed a long protocol which involved acupuncture every 2 days for a minimum of 60 days. Zhang and Han ( 1996 ) observed an improvement in symptoms after a continuous acupuncture q.d. for 40 days. Wang believed that the protocol should be prolonged to 2–3 years (Wang 2000 ) . Though the discrepancy on the length of course of acupuncture among different authors is large, all the authors agree on one fact that the onset of the effects of acupuncture is extremely slow and that it should be continued for a long time to keep the ef fi cacy up.
(d) Choosing the acupoints: As we have discussed several times in the previous sec-tions, the selection of acupoints is extremely dif fi cult and equally crucial. In some English studies performed by non-Chinese investigators, they made strict trial designs but still got negative results on the acupuncture ef fi cacy which were largely different from the results obtained by the Chinese investigators (Cristian et al. 2005 ; Shulman et al. 2002 ) . Besides the study design (see next section),

2277 Acupuncture Treatment for Parkinson’s Disease
we also found that the acupoints selected in these studies were quite different from those used in Chinese/Korean reports. Thus, the selection of acupoints should be considered quite seriously when designing an acupuncture study.
7.2.6.2 Problems with the Experimental Design of the Studies Evaluating the Ef fi cacy/Safety of Acupuncture
Evaluation of a new therapy is practiced through evidence-based medicine. Strong evidence should be gathered based on the following principles: (1) randomization; (2) control; (3) double blinding; and (4) placebo. For making a reasonable statistical deduction the following additional conditions must be achieved: (5) enough sample size; (6) appropriate statistical method; (7) repeatability, and (8) full introduction about the adverse events and the patients who cannot fi nish the trial.
Notwithstanding the legends of acupuncture being mysterious and charming, it must be subjected to the same objective evaluation standards as all other medical treat-ments. If not, any conclusion made on the acupuncture ef fi cacy would be dubious.
As with other alternative therapies based on the TCM, the ef fi cacy of acupuncture was sometimes overestimated or exaggerated by some improperly conducted studies, which raised a question not only on the acupuncture therapy but also on the validity of TCM. What is worse is that the data reported by some Chinese/Korean investigators are possibly losing the trust of many investigators on grounds of “high publication bias” (Moher et al. 2003 ; Vickers et al. 1998 ) .
Lee et al. ( 2008 ) searched the keywords “acupuncture and Parkinson disease” through main English/Chinese/Korean electronic database in the USA, UK, Korea, and China within 1 year. They found that only 11 of the 103 studies were random-ized controlled trials (RCTs) with subjective outcome measure. Only 1 of these 11 studies described a double-blinded method (Cristian et al. 2005 ) , and only 2 of these described the patient blinding (Lee et al. 2008 ) . Interestingly, the double-blinded study by Cristian and another rigorous study by Shulman failed to prove the ef fi cacy of acupuncture, albeit the negative results maybe a consequence of erroneous selection of the acupoints (see Sect. 7.2.6.1 ) (Cristian et al. 2005 ; Shulman et al. 2002 ) . Lee et al. ( 2009 ) searched the same keywords through ten Korean electronic databases; only one study from South Korea proved that the constitutional acupuncture is more effective than standard acupuncture based on Uni fi ed PD rating scale (UPDRS) and freezing gate; however, no further evidence was found to prove the ef fi cacy of acupuncture. Lam et al. ( 2008 ) searched the cross-referenced data on acupuncture therapy in PD both as MeSH and as text words in English/Chinese through several electronic databases. Only 10 of the 784 studies could be de fi ned as rigorous RCTs studies. Although, nine of the ten studies suggested a “signi fi cant” ef fi cacy of acupuncture in treating PD, Lam pointed out there was insuf fi cient evidence to support this conclusion due to certain method-ological fl aws in the studies. It is true that, so far, we have not been able to fi nd a well-designed study that provides formidable positive results on acupuncture ef fi cacy in treating PD.

228 T. Asakawa and Y. Xia
A recently performed systematic review on various Chinese studies evaluating the potency of acupuncture treatment in PD, reached at an analogous conclusion. Yang et al. ( 2010 ) analyzed 832 cases from 13 randomized clinical studies. Although many authors found that the ef fi cacy of medication plus acupuncture was far better than that of medication alone, however, the shortcomings in the designs of several studies weakened this conclusion.
The main problems in the experimental design of the acupuncture studies in treating PD are listed as below:
1. Absence of or incorrect usage of blinding methods is considered to be the most commonly recurring problem with the experimental design. Most of the authors use some subjective rating scales, such as UPDRS and Webster rating scale to evaluate the PD status. If there is no “blinding” applied to the observers, there is an increased possibility of occurrence of observational bias. The patients tend to report a positive variation under the in fl uence of psychological suggestion in the absence of blinding known as the “placebo effect.” Some studies tried to demonstrate the acupuncture ef fi cacy by comparing acupuncture plus drug therapy with drugs only (i.e., C + A vs. C, C = classical therapy; A = acupuncture). If double blinding is not employed, it is quite natural to get the results in the form of C + A > C, which is possibly attributable to the placebo effect and/or observational bias. The ef fi cacy of A is thereby overestimated. In this regard, to exclude the so-called placebo effect, the study design of C + A vs. C should be ameliorated by C + A vs. C + P (P = placebo acupuncture, which might be a false acupuncture or an inef-fective acupuncture, such as using a false needle, or inserting the needle to a non-acupoint area). However, achieving full double blinding in physical therapies is deemed to be dif fi cult (Lam et al. 2008 ) . Only under one circumstance is the single-blinded-patients-design acceptable, that is, if the evaluating index is objec-tive and is not affected by the inklings of the observer. Several methods were adopted to perform the single-blinded trials, for instance, by use of gauze to prevent the patients from seeing the acupuncture procedure; sham device, placebo needles, and inserting the needles into the blank areas with respect to the acupoints were also used for patient blinding (Cristian et al. 2005 ; Hammerschlag 1998 ; McManus et al. 2007 ; Park et al. 2002 ) .
2. Inadequate randomization and too small sample sizes are other big issues asso-ciated with the trial design. It is a tendency of the investigators to select milder cases for the treatment group, whereas severer cases for the control group. Inadequate randomization will cause such a selection bias, which can confound the results and overestimate the ef fi cacy. However, to perform complete ran-domization one needs enough sample size to maintain a baseline balance between the treatment and the control groups. Too small a sample size will lead to a difference at the baseline before even giving the treatments, which leaves the data after treatments incomparable. In terms of statistical analysis, too small size will lead type II error.
3. Insuf fi cient account of the adverse events and the dropouts or withdrawal reduce the reliability of the whole study. Though acupuncture seems to be safe (Jiang

2297 Acupuncture Treatment for Parkinson’s Disease
et al. 2006b ; Wang et al. 2006b ) , it is not a totally harmless therapy. Minor adverse effects such as stabbing pain, bleeding, and hematoma have been reported, along with some potentially serious side effects like infection and pneumothorax (Lam et al. 2008 ; Yamashita et al. 1998 ; Odsberg et al. 2001 ; White et al. 2001 ; White and Ernst 2001 ) .
4. Other methodological weaknesses, such as inappropriate statistical analysis, inadequate control group setting, etc., might occur and can reduce the worthiness of the study.
For obtaining powerful evidence on the ef fi cacy and safety of acupuncture therapy in PD, well-designed studies with less methodological fl aws are of great desidera-tum. According to the guidelines for clinical trials of acupuncture (Birch 2004 ; MacPherson et al. 2002a, b ) , a perfect study for evaluating the ef fi cacy and safety of acupuncture in treating PD should be a large, double-blinded (or single-blinded to patients with an objective evaluating criterion), rigorously randomized, and placebo-controlled study. Detailed recording of the adverse events and correct selection of statistical methods should be seriously taken into account. Long-term, multicentric, and multinational large clinical trials should be designed and performed to obtain formidable evidence for verifying the ef fi cacy and safety of acupuncture in treating PD.
7.3 Potential Mechanisms of Acupuncture Therapy for PD
The mechanisms of acupuncture treatment for PD are still unclear at present. Although there are numerous clinical reports from China and Korea that have claimed its ef fi cacy and safety, the studies aiming to uncover its mechanism are relatively few. We found several reports regarding the bench studies for the mecha-nisms of acupuncture on PD. It is dif fi cult, however, to make solid conclusions from these studies because of limited size of samples, lack of repeatability, or problem-atic experimental design (see Sect. 7.2.6.2 ). Owing to these drawbacks, more in-depth studies are needed to validate the potential mechanisms summarized below based on the current studies.
7.3.1 Delaying the Progress of DA Neuron Degeneration by Neuroprotective Effects
The most important causative factor of PD is the progressive degeneration of the DA neurons in SNpc, which “triggers” the successive pathophysiology. “To arrest” the DA neuron degeneration is, hence, the best strategy for treating PD. Unfortunately, even the most effective therapies including l -dopa administration and STN-DBS cannot contribute much to this effect (see Sect. 7.1 ).
230 T. Asakawa and Y. Xia
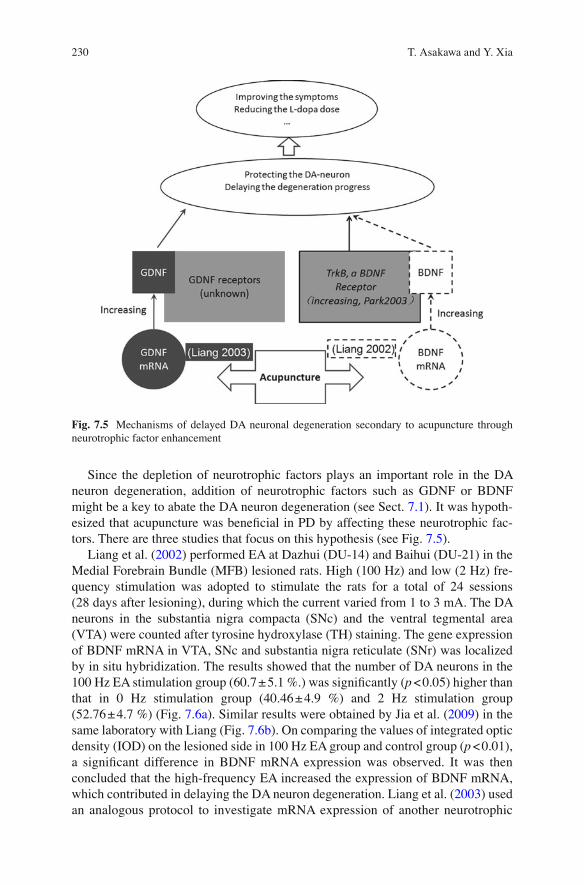
Since the depletion of neurotrophic factors plays an important role in the DA neuron degeneration, addition of neurotrophic factors such as GDNF or BDNF might be a key to abate the DA neuron degeneration (see Sect. 7.1 ). It was hypoth-esized that acupuncture was bene fi cial in PD by affecting these neurotrophic fac-tors. There are three studies that focus on this hypothesis (see Fig. 7.5 ).
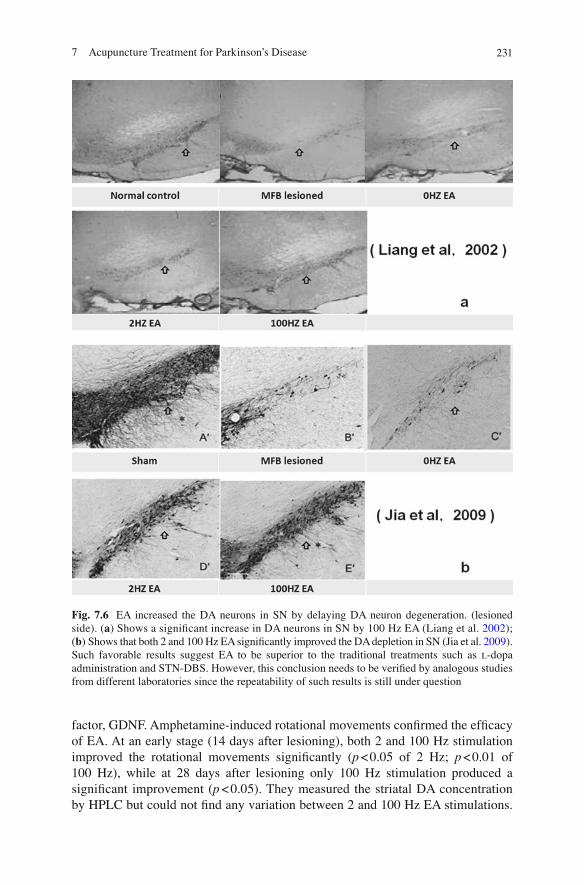
Liang et al. ( 2002 ) performed EA at Dazhui (DU-14) and Baihui (DU-21) in the Medial Forebrain Bundle (MFB) lesioned rats. High (100 Hz) and low (2 Hz) fre-quency stimulation was adopted to stimulate the rats for a total of 24 sessions (28 days after lesioning), during which the current varied from 1 to 3 mA. The DA neurons in the substantia nigra compacta (SNc) and the ventral tegmental area (VTA) were counted after tyrosine hydroxylase (TH) staining. The gene expression of BDNF mRNA in VTA, SNc and substantia nigra reticulate (SNr) was localized by in situ hybridization. The results showed that the number of DA neurons in the 100 Hz EA stimulation group (60.7 ± 5.1 %.) was signi fi cantly ( p < 0.05) higher than that in 0 Hz stimulation group (40.46 ± 4.9 %) and 2 Hz stimulation group (52.76 ± 4.7 %) (Fig. 7.6a ). Similar results were obtained by Jia et al. ( 2009 ) in the same laboratory with Liang (Fig. 7.6b ). On comparing the values of integrated optic density (IOD) on the lesioned side in 100 Hz EA group and control group ( p < 0.01), a signi fi cant difference in BDNF mRNA expression was observed. It was then concluded that the high-frequency EA increased the expression of BDNF mRNA, which contributed in delaying the DA neuron degeneration. Liang et al. ( 2003 ) used an analogous protocol to investigate mRNA expression of another neurotrophic
Fig. 7.5 Mechanisms of delayed DA neuronal degeneration secondary to acupuncture through neurotrophic factor enhancement
2317 Acupuncture Treatment for Parkinson’s Disease
factor, GDNF. Amphetamine-induced rotational movements con fi rmed the ef fi cacy of EA. At an early stage (14 days after lesioning), both 2 and 100 Hz stimulation improved the rotational movements signi fi cantly ( p < 0.05 of 2 Hz; p < 0.01 of 100 Hz), while at 28 days after lesioning only 100 Hz stimulation produced a signi fi cant improvement ( p < 0.05). They measured the striatal DA concentration by HPLC but could not fi nd any variation between 2 and 100 Hz EA stimulations.
Fig. 7.6 EA increased the DA neurons in SN by delaying DA neuron degeneration. (lesioned side). ( a ) Shows a signi fi cant increase in DA neurons in SN by 100 Hz EA (Liang et al. 2002 ) ; ( b ) Shows that both 2 and 100 Hz EA signi fi cantly improved the DA depletion in SN (Jia et al. 2009 ) . Such favorable results suggest EA to be superior to the traditional treatments such as l -dopa administration and STN-DBS. However, this conclusion needs to be veri fi ed by analogous studies from different laboratories since the repeatability of such results is still under question
232 T. Asakawa and Y. Xia
The expression of GDNF mRNA was evaluated by in situ hybridization and calculation of the GDNF-positive cells. Interestingly, 2 Hz EA improved GDNF mRNA expression on the unlesioned side in SN and VTA, while 100 Hz improved that on both lesioned and unlesioned sides. Both of Liang’s studies suggested that EA manifests a neuro-protective effect against the degeneration of DA neurons by activating endogenous neurotrophic factors such as BDNF and GDNF. The increased expression of BDNF mRNA and GDNG mRNA after EA may be a plausible mechanism of action of acupuncture (Liang et al. 2002, 2003 ) .
Park et al. ( 2003 ) performed acupunctures at two groups of acupoints in the striatal-lesioned rats. Acu1, which included Yanglingquan (GB-34) and Taichong (LR-3), was set as an effective acupuncture for PD; Acu2, which included Hegu (LI-4) and Quchi (LI-11)—the acupoints for gastrointestinal functions, was set as an ineffective acu-puncture. Five groups of rats were investigated at random. (1) Acu1 on 6-OHDA lesioned models was set as the effective treatment group; (2) Acu2 on 6-OHDA lesioned models was set as noneffective treatment group; (3) control group was the 6-OHDA lesioned rats that underwent no acupuncture; (4) Acu1 was performed on some sham operated rats, which was set as SAcu1 group. Sham group underwent only sham opera-tion and did not receive any acupuncture. Acupunctures were performed for 13 con-secutive days with each treatment lasting for 60 s. Apomorphine-induced rotational movements were used to evaluate the motor status. The DA neurons in the SN were calculated after the TH staining 2 weeks after lesioning. In addition, trkB (regarded as a high-af fi nity receptor for BDNF) was evaluated by counting the trkB-positive cells in SN after immunohistochemistry speci fi c for the tyrosine kinase (trkB) receptor. The results showed that the number of DA neurons on the lesioned SN side in the Acu1 group (78.6 %) was signi fi cantly higher ( p < 0.01) than the numbers in the control (45.7 %) and Acu2 (58.8 %) groups; the trkB-positive cells in Acu1 group (56.8 ± 4.4) were signi fi cantly higher than the contralateral part of the same group ( p < 0.01) and ipsilateral part of the control group ( p < 0.05). The data indicated that acupuncture at Yanglingquan and Taichong signi fi cantly reduced the DA neurons degeneration, which was possibly caused by the activation of the BDNF through increasing BDNF receptor (trkB) expression (Park et al. 2003 ) .
Several Chinese (Ma and Wang 2001 ; Ma et al. 2003 b ; Chen et al. 2010 ; Wang et al. 2010 ; Zhao et al. 2010 ) and Korean authors (Joh et al. 2010 ; Hong et al. 2010 ; Jeon et al. 2008 ) reported similar results. Kim et al. ( 2005 ) performed acupuncture at Zusanli (ST-36) in striatal PD rat models. They found that the Zusanli acupunc-ture could improve the behavioral test and TH staining in SN. They, therefore, concluded that acupuncture at the ST-36 is a useful strategy for treating PD. Jeon et al. ( 2008 ) investigated whether acupuncture alters protein expression in the SN to favor attenuation of neuronal degeneration in C57BL/6 mice treated with MPTP (30 mg/kg/day). They performed EA at Yanglingquan (GB-34), observed an improvement in the behavioral impairment and reduction in tyrosine TH-positive DA neurodegeneration. Moreover, the levels of cyclophilin A (CypA), which is a neuroprotective agent, were unchanged by MPTP treatment but were increased in MPTP-EA mice. All these studies showed positive results in demonstrating the neu-roprotective effects of acupuncture. These studies followed the randomized-control
2337 Acupuncture Treatment for Parkinson’s Disease
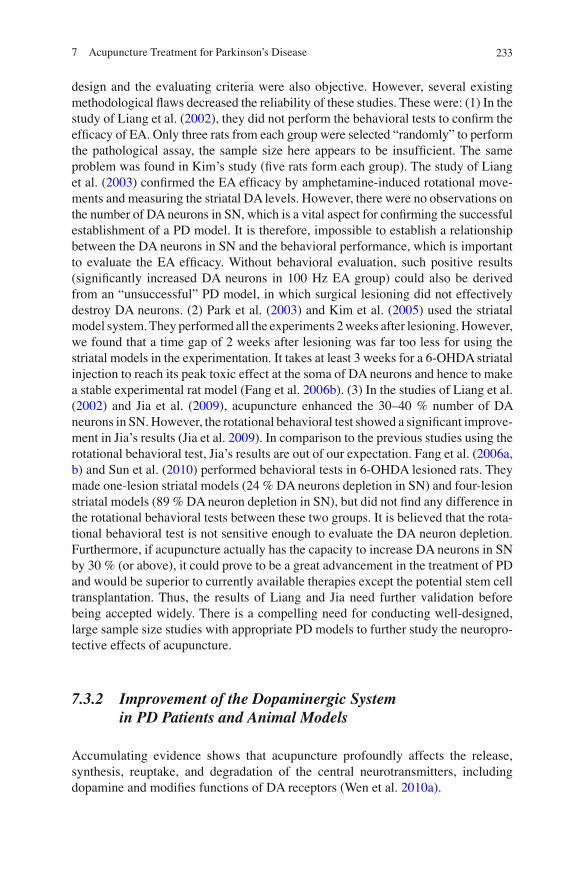
design and the evaluating criteria were also objective. However, several existing methodological fl aws decreased the reliability of these studies. These were: (1) In the study of Liang et al. ( 2002 ) , they did not perform the behavioral tests to con fi rm the ef fi cacy of EA. Only three rats from each group were selected “randomly” to perform the pathological assay, the sample size here appears to be insuf fi cient. The same problem was found in Kim’s study ( fi ve rats form each group). The study of Liang et al. ( 2003 ) con fi rmed the EA ef fi cacy by amphetamine-induced rotational move-ments and measuring the striatal DA levels. However, there were no observations on the number of DA neurons in SN, which is a vital aspect for con fi rming the successful establishment of a PD model. It is therefore, impossible to establish a relationship between the DA neurons in SN and the behavioral performance, which is important to evaluate the EA ef fi cacy. Without behavioral evaluation, such positive results (signi fi cantly increased DA neurons in 100 Hz EA group) could also be derived from an “unsuccessful” PD model, in which surgical lesioning did not effectively destroy DA neurons. (2) Park et al. ( 2003 ) and Kim et al. ( 2005 ) used the striatal model system. They performed all the experiments 2 weeks after lesioning. However, we found that a time gap of 2 weeks after lesioning was far too less for using the striatal models in the experimentation. It takes at least 3 weeks for a 6-OHDA striatal injection to reach its peak toxic effect at the soma of DA neurons and hence to make a stable experimental rat model (Fang et al. 2006b ) . (3) In the studies of Liang et al. ( 2002 ) and Jia et al. ( 2009 ) , acupuncture enhanced the 30–40 % number of DA neurons in SN. However, the rotational behavioral test showed a signi fi cant improve-ment in Jia’s results (Jia et al. 2009 ) . In comparison to the previous studies using the rotational behavioral test, Jia’s results are out of our expectation. Fang et al. ( 2006a, b ) and Sun et al. ( 2010 ) performed behavioral tests in 6-OHDA lesioned rats. They made one-lesion striatal models (24 % DA neurons depletion in SN) and four-lesion striatal models (89 % DA neuron depletion in SN), but did not fi nd any difference in the rotational behavioral tests between these two groups. It is believed that the rota-tional behavioral test is not sensitive enough to evaluate the DA neuron depletion. Furthermore, if acupuncture actually has the capacity to increase DA neurons in SN by 30 % (or above), it could prove to be a great advancement in the treatment of PD and would be superior to currently available therapies except the potential stem cell transplantation. Thus, the results of Liang and Jia need further validation before being accepted widely. There is a compelling need for conducting well-designed, large sample size studies with appropriate PD models to further study the neuropro-tective effects of acupuncture.
7.3.2 Improvement of the Dopaminergic System in PD Patients and Animal Models
Accumulating evidence shows that acupuncture profoundly affects the release, synthesis, reuptake, and degradation of the central neurotransmitters, including dopamine and modi fi es functions of DA receptors (Wen et al. 2010a ) .

234 T. Asakawa and Y. Xia
Wang et al. ( 2009 ) found that the expression of TH mRNA and dopamine transport (DAT) mRNA in the SN of 6-OHDA-treated rats was upregulated upon treatment with electroacupuncture at “Baihui” (GV-20)-through-“Taiyang” (EX-NH-5), when given in two courses (one course = once per day for 6 days). This fi nding suggests that EA attenutes neuronal degeneration, thus increasing DA neurons in SN.
Some authors believe that acupuncture improves the DA-ergic system by reduc-ing the neuronal degeneration in PD state, as DA neuron degeneration is the pathog-nomonic dysfunction of the DA-ergic system seen in PD. If acupuncture contributes to the reduction of DA neuronal depletion (see Sect. 7.3.1 ), it is reasonable to con-clude that the DA-ergic system can consequently be improved. Furthermore, other researchers have reported that peripheral electrical stimulation of certain parts of the animal body surface directly affected the cerebral DA levels (see Sect. 7.4 ).
7.3.2.1 Acupuncture Increases DA in the Brain
Sundry reports by Chinese investigators have indicated that acupuncture application at certain acupoints increases the cerebral DA level. Other investigators unrelated to TCM and acupuncture have also accounted that peripheral electrical stimulation in fl uenced the cerebral DA levels (see Sect. 7.4 ). Thus, it is accepted that stimula-tion of certain parts of the body will affect the DA levels in the brain, albeit the exact mechanisms and processes are still unclear. It also remains unfathomed as to whether these observations are attained by the direct effects of acupuncture, or due to sec-ondary variations through an increase in the number of DA neurons. In this section, we list only some of these Chinese reports; we will discuss the peripheral electrical stimulation in the next section.
Xu et al. ( 2002 ) performed acupuncture at Yanglingquan (GB-34), Neiguan (PC-6), Taichong (LR-3), and Baihui (DU-21) in PD patients and measured the con-centrations of DA, noradrenalin (NA), and 5-HT in the patients’ CSF by HPLC-EC. They reported that the levels of DA and NA in the effective acupuncture patients were signi fi cantly increased ( p < 0.001), but 5-HT levels showed no change. Zhu et al. ( 1996 ) performed acupuncture at Baihui (DU-21) in 1-methyl 4-phenyl 1,2,3,6-tetrahydropyridine (MPTP) treated mice. They measured DA and its metabo-lite, dihydroxyphenylacetic acid (DOPAC) in the caudate nucleus, and mesencepha-lon by HPLC-EC. They found that acupuncture signi fi cantly increased DA in the caudate nucleus and mesencephalon and normalized the increased DOPAC/DA ratio in the PD state. Wang et al. ( 2006a ) performed acupuncture at the Baihui (DU-21), Fengfu (DU-16) of the lesioned side, and bilateral Yanglingquan (LR-3) in the striatal PD rat models. Apomorphine-induced rotational movements were used to con fi rm the successful establishment of the PD models and the acupuncture ef fi cacy. The striatal DA and its metabolites DOPAC and homovanillic acid (HVA) were measured by HPLC-EC. They found that acupuncture at the above acupoints signi fi cantly increased the behavioral performance as well as the striatal DA, DOPAC, and HAV levels.
Yin et al. ( 2009 ) found that the application of EA (frequency from 2 to 100 Hz, voltage from 2 to 4 V) at Hegu (LI-4) and Taichong (LV-3) increased the expression

2357 Acupuncture Treatment for Parkinson’s Disease
of protein kinase A (PKA), and cAMP response element binding protein (CREB1) in the SNc of MPTP-treated mice. Since PKA and CREB1 play important roles in maintaining the DA balance, it is possible that they are also involved in the DA changes seen after acupuncture treatment in the PD animals.
It was also found that DA neuron depletion results in insuf fi cient DA in the audi-tory conduction pathway, which leads to abnormal auditory brainstem responses (ABRs). Prolongation of latencies (wave III or V) and interpeak latencies (IPLs; I–III, I–V, and III–V IPL) are regarded as the characteristic abnormalities in PD. Such abnormalities can be improved by the administration of l -dopa; thus, ABRs can be employed as indirect, yet objective evidence to assess the cerebral DA levels (O’Donnell et al. 1987 ; Kodama et al. 1999 ) . Wang et al. ( 2000 ) studied the ABRs in the PD patients and observed the abnormalities including prolonged latencies of wave V and interpeak latencies of I–V, III–V IPL. All these patients were then subjected to the experimental single acupuncture treatment. The results showed that the ef fi cacy of acupuncture was remarkable and there was a signi fi cant positive correla-tion between the ABRs and Webster rating scores. It was therefore concluded that acupuncture improves the cerebral DA and activates the DA neurons.
7.3.2.2 Acupuncture Activates the Dopamine Transport
Zhang et al. ( 2006 ) investigated the expression and activity of DAT affected by EA (frequency from 2 to 100 Hz, voltage from 2 to 4 V) in MPTP-treated mice by immu-nohistochemistry staining. They found that after stimulating the Hegu (LI-4) and Taichong (LR-3) acupoints for three courses (7 days, 20 min/day), the number of cells with DAT-positive expression signi fi cantly increased (24.67 ± 13.01) in the treatment group (vs. 2.33 ± 3.22 in the control group) along with the integral optical density (26088.88 ± 4498.05 in the treatment group vs. 15248.27 ± 4195.38 in the control group) in SNc. This fi nding demonstrated that the activation of DAT could be an important mechanism of action underlying the acupuncture treatment for PD.
Jiang et al. ( 2006a ) studied the changes in DAT in the striatum by conducting single photon emission computer tomography (SPECT) in fi ve PD patients. All the patients underwent electro-scalp acupuncture (ESA) for 6 weeks at MS6, MS4, MS8, MS9, and MS14 (hemi-PD patients received hemi-ESA; bilateral PD patients received bilateral ESA). The ESA parameters were the same as described in Table 7.2 . SPECT scans were performed before and after ESA treatment in each case. They used 99m Tc-TRODAT as the tracer agent for DAT (125 mCi, i.v). Regions of interest (ROI) were set as bilateral striatum (ST) and unilateral occipital lobe (OC). The ratio of radioactivity in the ST to OC was regarded as an index of DAT density or functional state. The results showed that bilateral ST/OC improved after ESA, but not signi fi cantly ( p > 0.05). It was concluded that the ESA was instrumental in activating bilateral striatal DAT or decreasing the loss of DAT (Fig. 7.7 ). Later works from this lab using the same experimental system showed that patients who received l -dopa and complementary acupuncture had increased regional cerebral blood fl ow (rCBF) in the following areas on the affected side after ESA: frontal lobe,

236 T. Asakawa and Y. Xia
occipital lobe, basal ganglion, and cerebellum when compared to the baseline, but there were no observed changes in the basal ganglia DAT levels. Treatment with l -dopa alone did not change rCBF but it did increase the basal ganglia DAT activity (Huang et al. 2010 ) .
In this section, we have summarized several Chinese studies, which reported that the acupuncture improved the DA-ergic system including the DA concentrations in CSF, striatum, auditory conduction pathway, and the DAT. No study was found to be successful in analyzing the relationship between acupuncture and the changes in DA receptors, which is another important element of the DA-ergic system.
Fig. 7.7 SPECT images of striatal DAT before and after ESA in a hemisection of the brain of a PD patient. Left arrow indicates contralateral side to the abnormal limbs. Right arrow indicates the ipsilateral side to the abnormal limbs in each image. The SPECT imaging showed ESA increased the bilateral striatal DAT though the increase was not signi fi cant ( p > 0.05) (Jiang et al. 2006a )

2377 Acupuncture Treatment for Parkinson’s Disease
7.3.3 Acupuncture Improvement of the Motor Control Network in the Basal Ganglia
As a consequence of DA neuron depletion, the abnormal state of the motor controlling network (Fig. 7.2 .) is regarded as an important pathological element of PD (Hashimoto et al. 2003 ; Nambu et al. 2002 ) . Some studies reported that acupuncture has a direct contribution to correct the basal ganglia circuit.
Liang et al. ( 2003 ) reported that EA balances the activity of each nucleus in the basal ganglia circuit. Jia et al. ( 2009 ) performed the same EA procedure as Liang ( Liang et al. 2002 ) and con fi rmed the successful establishment of PD rat models and the ef fi cacy of EA by rotational behavioral test. The ventral midbrain glutamate decarboxylase-67 (GAD 67) mRNA was evaluated by real-time quantitative RT-PCR; substance P (SP) and enkephalin (ENK) of ventral midbrain and globus pallidus (GP) was measured by a radioimmunoassay (RIA) test. The results showed that 100 Hz EA normalized the SP, which is decreased in PD ( p < 0.05) and decreased the GAD 67 mRNA level in the midbrain ( p < 0.01), however it did not affect the ENK in GP. These data suggest that high-frequency EA stimulation results in neu-ropeptide normalization in the basal ganglia circuit. EA appears to normalize the MFB lesion-induced variations in GAD 67 mRNA expression in the ventral midbrain, thereby, affecting the inhibitory GABA transmission and counteracting the overactive output structures of the basal ganglia in PD. In a recent study by the same group, Jia investigated the GABA content of midbrain in the MFB transected rat models during effective EA (100 Hz) and ineffective EA (2 Hz) at Dazhui (DU-14) and Baihui (DU-21) by HPLC. He found that the effective EA improved the GABA content in the midbrain but had no effect on the GABA content of the globus pallidus, which indicated that the effective EA improved the motor controlling network by increasing the GABA-ergic inhibition in the output structure of basal ganglia (Jia et al. 2010 ) . These processes might share the same mechanisms as the surgical therapies including STN-DBS and microinjection.
7.3.4 Acupuncture Attenuation of Oxidative Stress in PD State
Ever since Przedborski fi rst reported in 1992 that oxy-radicals play a role in the MPTP-induced neurotoxicity, the oxidative stress has been largely accepted as a pathogenic factor in PD. It is believed that increased SOD and decreased LPO activities act as protective factors that confer resistance to oxidative stress and oxidative damage in the PD state (Przedborski et al. 1992 ; Verma and Nehru 2009 ; Jenner and Olanow 1996 ; Reynolds et al. 2007 ) .
Zhang et al. ( 1997 ) performed scalp acupuncture at CTCA and Baihui (DU-21) in MPTP-treated C57 mouse models. The activities of superoxide dismutase (T-SOD), glutathione peroxidase (GSH-PX), and catalase (CAT), and the levels of malondial-dehyde (MDA) were measured. The results suggested that the scalp acupuncture

238 T. Asakawa and Y. Xia
increased the antioxidase activities in the caudate nucleus and mesencephalon and normalized the overactive lipid peroxidation. Yuan et al. ( 2010 ) evaluated the expression of SOD, GSH-PX, and MDA in 6-OHDA lesioned rats. They got similar results as obtained in the mice. Acupuncture signi fi cantly raised the effect of SOD and GSH-PX, and attenuated the expression of MDA.
Dong et al. ( 2001 ) investigated the blood LPO and SOD levels in the 57 PD patients who underwent acupuncture treatment. The acupoints included MS6, Waiguan (TE-5), Hegu (LI-4), Yanglingquan (GB-34), Taichong (LR-3), and Zusanli (ST-36). Three courses of acupuncture were given with each course comprising of acupuncture given once daily for ten sessions. The plasma LPO and SOD of red blood cells were then measured. The results showed that the acupuncture signi fi cantly improved SOD levels in the senior (over 60 years, p < 0.05) and female cases ( p < 0.01). There was an improving trend of SOD seen in the early-stage PD patients (onset within 3 years, p » 0.05). Wang et al. ( 2006b ) performed ESA at the Xuanli (GB-5), Xuanlu (GB-6), Fengfu (DU-16), Tianzhu (BL-10), and Fengchi (GB-20) in the 37 PD patients who received normal l -dopa administration. The other 39 control patients received l -dopa treatment only. The SOD and LPO levels of all the cases were investigated before and after ESA. The results showed that acupuncture signi fi cantly improved the scores on the rating scale ( p < 0.01). SOD in the treatment group was signi fi cantly increased while the LPO was decreased ( p < 0.01).
Above two bench studies and the two clinical studies showed that acupuncture increased the SOD while decreased the LPO, which is suggestive of a possible mechanism of acupuncture action underlying the DA neuroprotection from oxida-tive stress and oxidative damage.
7.3.5 Other Possible Mechanisms Involved in the Acupuncture Treatment of PD
We introduced the most widely investigated mechanisms of acupuncture involved in treating PD in the previous sections. As with other neurological diseases, many interactive factors and processes might be involved thereby making these mecha-nisms complicated. In this section, we list other possible mechanisms that need to undergo further investigation.
7.3.5.1 Regulation of Endogenous Opioids and Their Receptors
Endogenous opioid peptides (EOP) produce a myriad of physiological functions in the central nervous system by binding with different opioid receptors, including m , d , and k -opioid receptors (MOR, DOR, and KOR) (Wen et al. 2010b ) . The DOR and its endogenous ligands (e.g., enkephalins) are widely expressed in the basal ganglia, STN, striatum, GP, and SNr (Abou-Khalil et al. 1984 ; Aubert et al. 2007 ;
2397 Acupuncture Treatment for Parkinson’s Disease
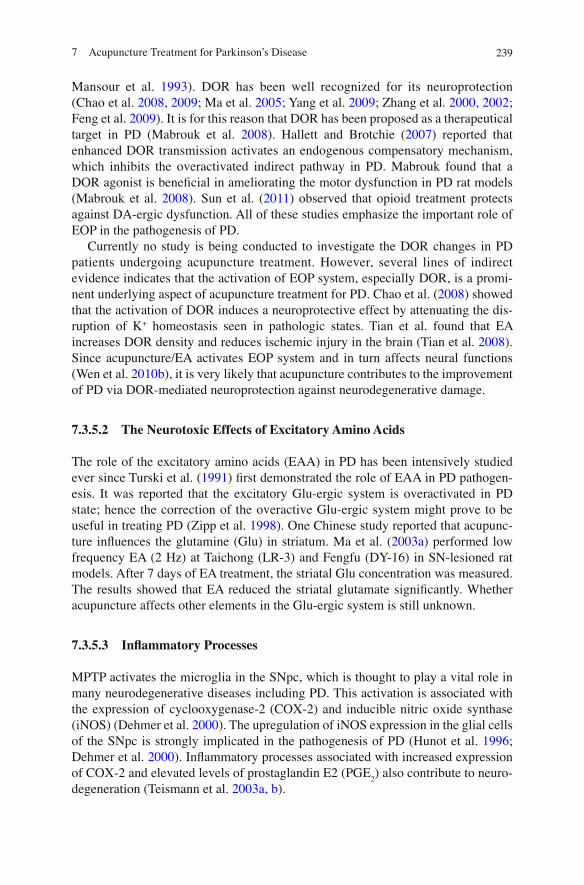
Mansour et al. 1993 ) . DOR has been well recognized for its neuroprotection (Chao et al. 2008, 2009 ; Ma et al. 2005 ; Yang et al. 2009 ; Zhang et al. 2000, 2002 ; Feng et al. 2009 ) . It is for this reason that DOR has been proposed as a therapeutical target in PD (Mabrouk et al. 2008 ) . Hallett and Brotchie ( 2007 ) reported that enhanced DOR transmission activates an endogenous compensatory mechanism, which inhibits the overactivated indirect pathway in PD. Mabrouk found that a DOR agonist is bene fi cial in ameliorating the motor dysfunction in PD rat models (Mabrouk et al. 2008 ) . Sun et al. ( 2011 ) observed that opioid treatment protects against DA-ergic dysfunction. All of these studies emphasize the important role of EOP in the pathogenesis of PD.
Currently no study is being conducted to investigate the DOR changes in PD patients undergoing acupuncture treatment. However, several lines of indirect evidence indicates that the activation of EOP system, especially DOR, is a promi-nent underlying aspect of acupuncture treatment for PD. Chao et al. ( 2008 ) showed that the activation of DOR induces a neuroprotective effect by attenuating the dis-ruption of K + homeostasis seen in pathologic states. Tian et al. found that EA increases DOR density and reduces ischemic injury in the brain (Tian et al. 2008 ) . Since acupuncture/EA activates EOP system and in turn affects neural functions (Wen et al. 2010b ) , it is very likely that acupuncture contributes to the improvement of PD via DOR-mediated neuroprotection against neurodegenerative damage.
7.3.5.2 The Neurotoxic Effects of Excitatory Amino Acids
The role of the excitatory amino acids (EAA) in PD has been intensively studied ever since Turski et al. ( 1991 ) fi rst demonstrated the role of EAA in PD pathogen-esis. It was reported that the excitatory Glu-ergic system is overactivated in PD state; hence the correction of the overactive Glu-ergic system might prove to be useful in treating PD (Zipp et al. 1998 ) . One Chinese study reported that acupunc-ture in fl uences the glutamine (Glu) in striatum. Ma et al. ( 2003 a ) performed low frequency EA (2 Hz) at Taichong (LR-3) and Fengfu (DY-16) in SN-lesioned rat models. After 7 days of EA treatment, the striatal Glu concentration was measured. The results showed that EA reduced the striatal glutamate signi fi cantly. Whether acupuncture affects other elements in the Glu-ergic system is still unknown.
7.3.5.3 In fl ammatory Processes
MPTP activates the microglia in the SNpc, which is thought to play a vital role in many neurodegenerative diseases including PD. This activation is associated with the expression of cyclooxygenase-2 (COX-2) and inducible nitric oxide synthase (iNOS) (Dehmer et al. 2000 ) . The upregulation of iNOS expression in the glial cells of the SNpc is strongly implicated in the pathogenesis of PD (Hunot et al. 1996 ; Dehmer et al. 2000 ) . In fl ammatory processes associated with increased expression of COX-2 and elevated levels of prostaglandin E2 (PGE
2 ) also contribute to neuro-
degeneration (Teismann et al. 2003a, b ) .

240 T. Asakawa and Y. Xia
Kang et al. ( 2007 ) performed acupuncture at Yanglingquan (GB-34) and Taichong (LR-3) in MPTP-treated C57BL/6 mice. In accordance with the previous studies, acu-puncture generated a neuroprotective effect in the SN and ST at 1, 3, and 7 days after MPTP injection. The increasing expression of COX2 and iNOS on the days 1, 3, and 7 was down-regulated. The remaining striatal DA in the acupuncture group was mea-sured and found to be 78 % at the seventh day compared to that of 46 % in the control group. Therefore, it was concluded that acupuncture could be used as a neuroprotective intervention for inhibiting microglial activation and in fl ammatory processes in PD.
7.3.5.4 Acupuncture Induces Peripheral Improvements in PD
Besides affecting the central nervous system, acupuncture also contributes to the amelioration of the peripheral abnormalities caused by PD.
Several Chinese clinical studies have reported that ESA stimulation improves the abnormal tremor myoelectric potential. Xi et al. ( 1996 ) , Huang ( 2000b ) , and Wang et al. ( 2003 ) compared the electromyography (EMG) before and after the effective ESA stimulation. The acupoints selected were as follows: Xi used Baihui (DU-21); Huang used bilateral CTCA and MCA; Wang selected Fengchi (GB-20), Xuanli (GB-6), Qianding (GV-21), and Xuanlu (GB-5). In all these studies, the selected patients suffered from a serious tremor. It was observed that after ESA stimulation, the tremor symptoms in each of the three studies signi fi cantly improved ( p < 0.05). After stimulation, in 39 % (Xi), 25.8 % (Huang), and 79 % (Wang) patients’ abnormal tremor myoelectric potential disappeared; in 33 % (Xi), 51.6 % (Huang), and 21 % (Wang) improvement was obtained, which was de fi ned as a 50 % reduction in the frequency and swing range; while there were 28 % (Xi), 22.6 % (Huang), and 0 % (Wang) who did not improve. The improvements in EMG coincided with the varia-tions of the tremor symptoms. It was concluded that ESA was bene fi cial in correct-ing the abnormal myoelectric potential in PD state. EMG can be employed as an effective objective index for evaluating the tremor in PD.
7.3.6 Comments
In this section, we summarized the potential mechanisms of the acupuncture treat-ment in PD. The most important mechanism is the reduction of the DA neuron degeneration by increasing some neurotrophic factors, which is quite superior to the classic treatments including l -dopa administration and DBS. Though many studies from China and Korea published rather excellent results showing signi fi cant improvements of the DA neurons in SN the weaknesses in the experimental design and the lack of peer con fi rmation of these results in other laboratories reduced the reliability of such reports.
We believe that the mechanics of acupuncture involve many complex factors and processes rather than a single mechanism. It is reasonable to believe that acupuncture can potentially affect different aspects of the pathogenesis of PD. Uncovering the secret of these mechanisms still has a long way to go.

2417 Acupuncture Treatment for Parkinson’s Disease
7.4 Prospective Strategy: DBS vs. Modi fi ed Electroacupuncture
DBS has been widely accepted as a mainstream surgical therapy since Benabid initially reported it 11 years ago (Benabid et al. 2000 ) . However, DBS is an invasive procedure with a high surgical risk. The limitation of the battery life of the stimulator embedded under the skin forces the patients to make a tough decision either to undergo another surgical operation to change the battery or adopt a palliative pattern by reducing the stimulation current to save the battery. In some developing countries without a perfect health insurance system, DBS is an extremely expensive operation. In addition to the cost, due to the above fl aws of DBS many PD clinicians today hope to fi nd a new effective procedure that is less invasive and can be performed by electri-cally stimulating certain easily accessible super fi cial structures (Xia et al. 2010 ) .
Acupuncture proves to be an exactly such procedure ideal for PD, conducted by stimulating the acupoints on the body surface. However, EA is not so popular other than the Asian countries and is effectively practiced by those who can really under-stand the theory of TCM. The dif fi cult theories of TCM hinder the understanding and acceptance of acupuncture. In this section, we would like to suggest a new elec-trical stimulation strategy, which is a modi fi ed EA mainly based on the conventional medical theory but closely related to the TCM theory, which we will refer to as the super fi cial electrical stimulation (SES). We hope that this would come across as an appropriate and acceptable alternative to the general PD investigators.
Several reports, other than those studies based on the acupoints stimulation, have demonstrated that peripheral electrical stimulation can in fl uence the cerebral DA release. There is enough evidence on the direct interaction between the somatosen-sory system and motor system both in the PD patients and animal models. Back in 1977, Nieoullon fi rst demonstrated that electrical stimulation of the forepaw caused an increased DA release in ipsilateral basal ganglia in the animals (Nieoullon et al. 1977 ) . Rothblat and Schneider ( 1993 ) later pointed out that sensory stimulus affected the spontaneous activity of caudate nucleus units, which re fl ects the overall motor condition of the animal. Schultz found that peripheral noxious stimulation in fl uenced the mesencephalic DA neurons by depressing or activating them (Schultz and Romo 1987 ) . Inoue et al. ( 2004 ) performed sensory stimulation at the forepaw in six normal cats. [ 11 C]-raclopride positron emission tomography (PET) was used to detect the functional status of D
2 -like receptor, which is commonly employed as an indirect
index for evaluating DA release during the stimulation. The results showed that the sensory stimulation obviously in fl uenced the endogenous DA release in the contral-ateral nucleus accumbens and striatum (Fig. 7.8 ). Fuentes et al. ( 2009 ) lately proposed a new spinal cord electrical stimulation method for the treatment of PD. Dorsal column stimulation (DCS) was performed on acute MPTP-treated mice and chronic 6-OHDA treated rats. The motor impairments in the mice and rats were seen to improve signi fi cantly, especially, the initiation of the locomotion.
All of the fi ndings above suggest that stimulating certain peripheral “stations” in speci fi c somatosensory pathways will affect the cerebral DA release, which can

242 T. Asakawa and Y. Xia
possibly be bene fi cial in improving the PD symptoms. The anatomical connections of somatosensory pathways, including the distribution on the body surface, are not fully understood. Inoue’s data suggested the possible anatomical pathways exist between the mesencephalic DA-ergic nuclei and the sensory system causing the observed modulation of DA release in the basal ganglia. One plausible connection is from the sensory areas in the neocortex contralateral to the stimulation side projects back into the ipsilateral striatum. One such pathway is the sensory area of the neo-cortex that projects back into the ipsilateral striatum. This connection activates the ipsilateral DA release from mesencephalic DA-ergic nuclei. Another possible ana-tomical connection could be the projecting fi bers between the nuclei intralaminares thalami and the SNpc through the striatum on contralateral side. In addition, there is another potential pathway between the VTA and the mesencephalic central gray, which is innervated collaterally by the spinothalamic tract. (Inoue et al. 2004 ) . The dorsal column in the spinal cord is believed to act as a connecting “station” in a certain somatosensory pathway. Stimulation of the dorsal column is thought to recruit brain-stem arousal systems, leading to suf fi cient cortical and striatal desynchronization required for the voluntary initiation of movements (Fanselow et al. 2000 ; Fuentes et al. 2009 ) . These fi ndings also provide enough clues for establishing the SES approach. In our future studies, we will try to fi nd such “special” somatosensory pathways and the related peripheral “stations” which may prove to be advantageous in improving locomotion in the PD animal models and patients by SES.
7.4.1 Animal Model Selection
Rodent animals (rat and mouse), cats, and non-human primate animals (rhesus monkey or cynomolgus monkey) are most commonly recruited for setting up of PD models. Because of a difference in DA metabolic enzyme systems, the selective DA
Fig. 7.8 The striatal D2-like receptor activity affected by contralateral forepaw electrical stimulation. Parametric images of binding potential (BP) in coregistered MRI; Left image : The electrical stimu-lation in the left paw decreased the BP value in the right basal ganglia. Right image : The electrical stimulation in the right paw decreased the BP value in the left basal ganglia. Center image : A parametric image of BP without stimulation. The BP value is shown in the color bar . Rt: The right side of the cat brain (Inoue et al. 2004 ) .

2437 Acupuncture Treatment for Parkinson’s Disease
neuron neurotoxins are different among different animals. Mouse, cat, and non-human primate animal PD models are usually established by MPTP adminis-tration, while the rat and pig PD models are set up by 6-OHDA injection, or surgical lesioning (such as MFB transection). Ideal animal models for SES studies should not only closely imitate the symptoms but also the natural process of PD in a human being. Hence, chronic–low dose–toxin administration in an aged animal seems to be a reasonable approach for theoretically establishing the PD model, yet it is rarely adopted considering its experimental ef fi ciency and cost.
The following factors have to be contemplated upon while selecting an appropriate PD model for SES studies:
1. MPTP administration is quite dangerous for the experimenters and requires expertise along with a good ventilation system. For safety reasons, rats might be a better choice for a larger sample required in the early stage of the study; while MPTP-treated monkey models are good for the terminal animal experiments before applying certain new therapies or new medicines to human beings.
2. A monkey model can imitate all the symptoms observed in humans, whereas it is dif fi cult to produce certain symptoms such as tremor and gesture failure in the non-primates animals.
3. For functional imaging studies such as PET and SPECT, the brain size is of vital importance in differentiating the variations in tiny structures. Too small brain will cause a large bias in the data acquisition, absorption correction, image recon-struction, and statistical analysis. Mouse model is not good for such imaging studies for SES.
4. The compliance to the behavioral tests. The behavioral evaluation techniques in rodent animals and monkeys are mature and reliable, and they are thought to have good compliance with the task training.
We therefore selected rat and monkey models after minutely considering the above factors. Rat models were used during the early stage of the study, to detect the appropriate stimulating points. Monkey models were selected for the advanced stage, when the experimental system has been established and the ef fi cacy has been con fi rmed. Monkey models also proved to be a good choice for carrying out the functional imaging studies before planning a human study.
Among the rat models, we had MFB-lesioned models (complete kill model), SN-lesioned models, and striatal models. In our previous studies, we found that the D
2 -like receptor in MFB-lesioned rats was upregulated during early stages after
lesioning (4 weeks after lesioning), then down-regulated in the later stages (6 months after lesioning), which is close to the dynamic changes of D
2 -like receptor seen in
the PD patients (Sun et al. 2010 ) . We, hence, believe that MFB-lesioned models are better than striatal and SN-lesioned for the initiation of SES study.
7.4.2 Behavioral Assessments
Behavioral tests have come to play increasingly important roles in designing experi-mental PD studies. Behavioral tasks are always used for verifying the success of

244 T. Asakawa and Y. Xia
establishing an animal model, or assessing the ef fi cacy of a new therapy. An ideal behavioral test should have the following features: (1) objectivity and repeatability; (2) quantitative; (3) representativeness; (4) operability; and (5) sensitivity.
For SES study, we have to detect the appropriate stimulation targets fi rst; thus, symptoms that are easily observed should be taken into account. The initiation time of the stepping test in rats and tremor termination in the monkeys are appropriate for target selection.
When optimizing the targets to be stimulation, more behavioral tests should be tried, including the stepping test (Nikkhah et al. 1993 ; Fang et al. 2006b ) , Rotarod test (Rozas et al. 1997 ; Fang et al. 2006b ) , and amphetamine-induced rotational movement in rats and the food-reaching test (FRT) in the monkeys (unpublished data). We also considered developing a new behavioral test appropriate for SES ef fi cacy assessment in the study.
7.4.3 Exploring the Appropriate Super fi cial Targets for SES
This is the most important procedure of the whole study. Just like it has been described in the former sections, SES is different yet in a way related, to the tradi-tional EA. The target identi fi cation for SES can be performed by either of the two approaches: First is by following the potential somatosensory pathways: fi nd and stimulate the important peripheral “stations” through the pathway; and second is by following the theory of TCM—stimulating the various acupoints. Conversely, we can track all the acupoints with good ef fi cacy, comprehensively analyze them, and fi nd new peripheral distributions of their associated somatosensory pathways.
7.4.4 Adjusting the Parameters for Stimulation
The selection of stimulation parameters is another critical issue in SES. First, while detecting the stimulating targets, we must decide on a “potentially” effective stimu-lating condition, which is decided based on the experiences of the previous studies, such as high stimulating frequency (over 100 Hz) and strong current intensity (1–2 mA). After the stimulating targets are set, we should compare the different conditions of stimulation: (1) low frequency vs. high-frequency stimulation; (2) the appropriate current intensity; and (3) stimulations using different wave patterns, such as rectangular wave in DBS or disperse-dense wave in EA.
7.4.5 Ef fi cacy Evaluation Using Molecular Imaging Approaches
In the traditional animal experiments, animals sometimes had to be killed to perform a pathological assay. We cannot compare the index such as the DA neurons in SN

2457 Acupuncture Treatment for Parkinson’s Disease
before and after treatment using one rat. An alternative method is to set several parallel control/Sham groups. However, if the sample size is not large enough, the conclusions can be distorted by individual differences (selection bias). Molecular imaging methods can absolve these limitations.
With the development of new tracers, PET scan is beginning to be used in the evaluation of certain new therapies. PET is a noninvasive method and exempts the need to sacri fi ce the animals; the biggest advantage of PET, however, lies in the fact that it can quantitatively or semiquantitatively detect the dynamic real-time variations in certain substances/indices in a living animal, or during certain treatments such as DBS or acupuncture. Variations in different indices induced by a treatment can be dynamically evaluated by using multiple tracers in the same animal. Such features are appropriate for evaluating SES, since the dynamic changes in the DA-ergic system induced by SES in vivo are critical for evaluation of the SES ef fi cacy.
The available tracers commonly used for current PET studies on PD are listed in Table 7.3 .
7.5 Concluding Remarks
In this chapter, we have summarized the clinical applications of acupuncture in PD treatment by reviewing the current studies from all over the world and have also tried to fi nd clues on the potential mechanisms from the limited information available. A number of studies from China and Korea have reported positive ef fi cacy and fewer side effects of acupuncture in PD treatment. Several studies focusing on the different aspects of the potential mechanisms involved in the acupuncture are being conducted. If such effects of acupuncture are rigorously validated, acupuncture can be intro-duced to the mainstream academia for a commonly used alternative therapy for PD.
Like with other alternative therapies, the ef fi cacy and safety of acupuncture have not been strictly veri fi ed. Due to methodological weaknesses, the observations and results thus obtained have overestimated the treatment ef fi cacy and concealed the possible adverse events, which reduces the reliability of these studies. This is a major reason for the unacceptability of some of the alternative therapies. What is worse is that not only is the therapy itself under doubt, but it has also prejudiced the
Table 7.3 Currently available PET tracers for PD
Radionuclide Tracers Function
11 C 11 C-dopa Presynaptic DA synthesis PE2I DAT 11 C-CFT DAT 11 C-raclopride DA D
2 like receptor
11 C-SCH23390 DA D 1 like receptor
18 F FDG Glucose metabolism FLT Cell proliferation
15 O H 2 O Regional cerebral blood fl ow

246 T. Asakawa and Y. Xia
viewpoint of the involved researchers against the whole TCM theory system, including those from its motherland. An illustration of this fact is that despite so many Chinese/Korean studies on PD, which have proved the ef fi cacy of acupuncture (essentially, a kind of peripheral stimulation), it has still not stepped into the view of mainstream PD academia, as the PD clinicians are still pondering to fi nd a noninvasive new electrical stimulation method for PD, and have not yet accepted acupuncture as an option. It is for this reason that TCM today faces an awkward stand even in China. Hence, we wish to raise this interest and bring forth the need for well-designed, rigorous clinical and experimental studies to provide formidable scienti fi c evidence validating the ef fi cacy and safety of acupuncture in the treatment of PD.
At fag end of this chapter, a modi fi ed EA method conceived from the combination of the theories of western medicine and TCM, called SES, has been suggested. In future, we will concentrate on developing this new therapy, which we believe would be accepted by most PD researchers including the general medical investigators.
Acknowledgments TA was supported by Japan Society for the Promotion of Science (Grant-in-Aid for Young Scientists, Type B, #20791025 and Grant-in-Aid for Scienti fi c Research General, #24592157). YX was supported by the National Institutes of Health (AT-004422 and HD-034852) and the Vivian L. Smith Neurologic Foundation.
References
Abou-Khalil B, Young AB, Penney JB (1984) Evidence for the presynaptic localization of opiate binding sites on striatal efferent fi bers. Brain Res 323 (1):21–29
Alexander GE, Crutcher MD, DeLong MR (1990) Basal ganglia-thalamocortical circuits: parallel sub-strates for motor, oculomotor, “prefrontal” and “limbic” functions. Prog Brain Res 85:119–146
Alexander GE, DeLong MR, Strick PL (1986) Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annu Rev Neurosci 9:357–381
Aubert I, Guigoni C, Li Q, Dovero S, Bioulac BH, Gross CE, Crossman AR, Bloch B, Bezard E (2007) Enhanced preproenkephalin-B-derived opioid transmission in striatum and subthalamic nucleus converges upon globus pallidus internalis in L-3,4-dihydroxyphenylalanine-induced dyskinesia. Biol Psychiatry 61 (7):836–844
Benabid AL, Koudsie A, Benazzouz A, Fraix V, Ashraf A, Le Bas JF, Chabardes S, Pollak P (2000) Subthalamic stimulation for Parkinson’s disease. Arch Med Res 31 (3):282–289
Birch S (2004) Clinical research on acupuncture. Part 2. Controlled clinical trials, an overview of their methods. J Altern Complement Med 10 (3):481–498
Burke RE, Antonelli M, Sulzer D (1998) Glial cell line-derived neurotrophic growth factor inhibits apoptotic death of postnatal substantia nigra dopamine neurons in primary culture. J Neurochem 71 (2):517–525
Chao D, Balboni G, Lazarus LH, Salvadori S, Xia Y (2009) Na+ mechanism of delta-opioid receptor induced protection from anoxic K+ leakage in the cortex. Cell Mol Life Sci 66 (6):1105–1115
Chao D, Bazzy-Asaad A, Balboni G, Salvadori S, Xia Y (2008) Activation of DOR attenuates anoxic K+ derangement via inhibition of Na+ entry in mouse cortex. Cereb Cortex 18 (9):2217–2227
Chen L, LI J, Li X, Chen B, Mo L (2010) Tendons acupuncture points Yanglingquan substantia nigra in Parkinson’s mouse model of TH expression. Guiding Journal of Traditional Chinese Medicine and Pharmacology 16 (11):67–68 (in Chinese)
Clarkson ED, Edwards-Prasad J, Freed CR, Prasad KN (1999) Immortalized dopamine neurons: A model to study neurotoxicity and neuroprotection. Proc Soc Exp Biol Med 222 (2):157–163

2477 Acupuncture Treatment for Parkinson’s Disease
Cristian A, Katz M, Cutrone E, Walker RH (2005) Evaluation of acupuncture in the treatment of Parkinson’s disease: a double-blind pilot study. Mov Disord 20 (9):1185–1188
Dai LJ (2004) The progress of treating Parkinson’s disease by acupuncture. Yunnan Journal of Traditional Chinese Medicine and Materia Medica 25 (5):48–49 (in Chinese)
Dehmer T, Lindenau J, Haid S, Dichgans J, Schulz JB (2000) De fi ciency of inducible nitric oxide synthase protects against MPTP toxicity in vivo. J Neurochem 74 (5):2213–2216
Dong XT, Wang SK, Ren XQ, Yu MJ, Yang JH, Liu AH, Liu JY, Chen GP, Wang YJ (2001) Effects of Acupuncture Treatment on Blood LPO and SOD Contents in Parkinsonism Patients. Acupuncture Research 26 (1):28–30 (in Chinese with English abstract)
Fang X, Sugiyama K, Akamine S, Namba H (2006a) Improvements in motor behavioral tests during deep brain stimulation of the subthalamic nucleus in rats with different degrees of unilateral parkinsonism. Brain Res 1120 (1):202–210
Fang X, Sugiyama K, Akamine S, Namba H (2006b) The stepping test and its learning process in different degrees of unilateral striatal lesions by 6-hydroxydopamine in rats. Neurosci Res 55 (4):403–409
Fanselow EE, Reid AP, Nicolelis MA (2000) Reduction of pentylenetetrazole-induced seizure activity in awake rats by seizure-triggered trigeminal nerve stimulation. J Neurosci 20 (21):8160–8168
Feigin A, Kaplitt MG, Tang C, Lin T, Mattis P, Dhawan V, During MJ, Eidelberg D (2007) Modulation of metabolic brain networks after subthalamic gene therapy for Parkinson’s disease. Proc Natl Acad Sci U S A 104 (49):19559–19564
Feng Y, Chao D, He X, Yang Y, Kang X, Lazarus LH, Xia Y (2009) A novel insight into neuropro-tection against hypoxic/ischemic stress. Sheng Li Xue Bao 61 (6):585–592
Ferry P, Johnson M, Wallis P (2002) Use of complementary therapies and non-prescribed medication in patients with Parkinson’s disease. Postgrad Med J 78 (924):612–614
Frim DM, Uhler TA, Galpern WR, Beal MF, Breake fi eld XO, Isacson O (1994) Implanted fi broblasts genetically engineered to produce brain-derived neurotrophic factor prevent 1-methyl-4-phenylpyridinium toxicity to dopaminergic neurons in the rat. Proc Natl Acad Sci U S A 91 (11):5104–5108
Fuentes R, Petersson P, Siesser WB, Caron MG, Nicolelis MA (2009) Spinal cord stimulation restores locomotion in animal models of Parkinson’s disease. Science 323 (5921):1578–1582
George JL, Mok S, Moses D, Wilkins S, Bush AI, Cherny RA, Finkelstein DI (2009) Targeting the progression of Parkinson’s disease. Curr Neuropharmacol 7 (1):9–36
Gill SS, Patel NK, Hotton GR, O’Sullivan K, McCarter R, Bunnage M, Brooks DJ, Svendsen CN, Heywood P (2003) Direct brain infusion of glial cell line-derived neurotrophic factor in Parkinson disease. Nat Med 9 (5):589–595
Guo JC, Cheng JS, Xia Y (2010) Acupuncture therapy for stroke. In: Acupuncture Therapy for Neurological Diseases: A Neurobiological View. Heidelberg, London, New York, Beijing, pp 226–262
Hallett PJ, Brotchie JM (2007) Striatal delta opioid receptor binding in experimental models of Parkinson’s disease and dyskinesia. Mov Disord 22 (1):28–40
Hammerschlag R (1998) Methodological and ethical issues in clinical trials of acupuncture. Journal of Alternative and Complementary Medicine 4 (2):159–171
Hashimoto T, Elder CM, Okun MS, Patrick SK, Vitek JL (2003) Stimulation of the subthalamic nucleus changes the fi ring pattern of pallidal neurons. J Neurosci 23 (5):1916–1923
Hilker R, Portman AT, Voges J, Staal MJ, Burghaus L, van Laar T, Koulousakis A, Maguire RP, Pruim J, de Jong BM, Herholz K, Sturm V, Heiss WD, Leenders KL (2005) Disease progression continues in patients with advanced Parkinson’s disease and effective subthalamic nucleus stimulation. J Neurol Neurosurg Psychiatry 76 (9):1217–1221
Hilker R, Voges J, Ghaemi M, Lehrke R, Rudolf J, Koulousakis A, Herholz K, Wienhard K, Sturm V, Heiss WD (2003) Deep brain stimulation of the subthalamic nucleus does not increase the striatal dopamine concentration in parkinsonian humans. Mov Disord 18 (1):41–48
Hirsch E, Graybiel AM, Agid YA (1988) Melanized dopaminergic neurons are differentially sus-ceptible to degeneration in Parkinson’s disease. Nature 334 (6180):345–348

248 T. Asakawa and Y. Xia
Hong MS, Park HK, Yang JS, Park HJ, Kim ST, Kim SN, Park JY, Song JY, Jo DJ, Park SW, HwanYun D, Ban JY, Chung JH (2010) Gene expression pro fi le of acupuncture treatment in 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine-induced Parkinson’s disease model. Neurol Res 32 Suppl 1:74–78
Huang WY (2000a) Eye acupuncture in 45 Parkinsonian Patients, a clinical report. Shanghai Journal of Acupuncture and Moxibustion 19 (4):20 (in Chinese)
Huang WY (2000b) In fl uence of electric stimulation of scalp acupuncture on electromyogram in tremor pattern of Parkinson’s disease. Acta Universitatis Traditionis Medicalis Sinensis Pharmacologiaeque Shanghai 14 (3):38–39 (in Chinese)
Huang Y, Jiang X, Zhuo Y, Wik G (2010) Complementary acupuncture in Parkinson’s disease: a spect study. Int J Neurosci 120 (2):150–154
Hunot S, Boissiere F, Faucheux B, Brugg B, Mouatt-Prigent A, Agid Y, Hirsch EC (1996) Nitric oxide synthase and neuronal vulnerability in Parkinson’s disease. Neuroscience 72 (2):355–363
Inoue M, Katsumi Y, Hayashi T, Mukai T, Ishizu K, Hashikawa K, Saji H, Fukuyama H (2004) Sensory stimulation accelerates dopamine release in the basal ganglia. Brain Res 1026 (2):179–184
Jenner P, Olanow CW (1996) Oxidative stress and the pathogenesis of Parkinson’s disease. Neurology 47 (6 Suppl 3):S161–170
Jeon S, Kim YJ, Kim ST, Moon W, Chae Y, Kang M, Chung MY, Lee H, Hong MS, Chung JH, Joh TH, Park HJ (2008) Proteomic analysis of the neuroprotective mechanisms of acupuncture treat-ment in a Parkinson’s disease mouse model. Proteomics 8 (22):4822–4832
Jia J, Li B, Sun ZL, Yu F, Wang X, Wang XM (2010) Electro-acupuncture stimulation acts on the basal ganglia output pathway to ameliorate motor impairment in Parkinsonian model rats. Behav Neurosci 124 (2):305–310
Jia J, Sun Z, Li B, Pan Y, Wang H, Wang X, Yu F, Liu L, Zhang L (2009) Electro-acupuncture stimulation improves motor disorders in Parkinsonian rats. Behav Brain Res 205 (1):214–218
Jiang XM, Huang Y, Li DJ, Tang AW, Wang SX, Zhuo Y, Li QS, Chen J, Gao YP (2006a) [Effect of electro-scalp acupuncture on cerebral dopamine transporter in the striatum area of the patient of Parkinson’s disease by means of single photon emission computer tomography]. Zhongguo Zhen Jiu 26 (6):427–430 (in Chinese with English abstract)
Jiang XM, Huang Y, Zhuo Y, Gao YP (2006b) [Therapeutic effect of scalp electroacupuncture on Parkinson disease]. Nan Fang Yi Ke Da Xue Xue Bao 26 (1):114–116 (in Chinese with English abstract)
Joh TH, Park HJ, Kim SN, Lee H (2010) Recent development of acupuncture on Parkinson’s disease. Neurol Res 32 Suppl 1:5–9
Kang JM, Park HJ, Choi YG, Choe IH, Park JH, Kim YS, Lim S (2007) Acupuncture inhibits microglial activation and in fl ammatory events in the MPTP-induced mouse model. Brain Res 1131 (1):211–219
Kang XZ, Xia Y (2010a) Acupuncture therapy for hypertension and hypotension. In: Acupuncture Therapy for Neurological Diseases: A Neurobiological View. Springer-Tsinghua Press, Heidelberg, London, New York, Beijing, pp 289–325
Kang XZ, Xia Y (2010b) Effects of Acupuncture on Arrhythmia and Other Cardiac Diseases. In: Acupuncture Therapy for Neurological Diseases: A Neurobiological View. Springer-Tsinghua Press, Heidelberg, London, New York, Beijing, pp 263–288
Kaplitt MG, Feigin A, Tang C, Fitzsimons HL, Mattis P, Lawlor PA, Bland RJ, Young D, Strybing K, Eidelberg D, During MJ (2007) Safety and tolerability of gene therapy with an adeno-associated virus (AAV) borne GAD gene for Parkinson’s disease: an open label, phase I trial. Lancet 369 (9579):2097–2105
Kim JH, Auerbach JM, Rodriguez-Gomez JA, Velasco I, Gavin D, Lumelsky N, Lee SH, Nguyen J, Sanchez-Pernaute R, Bankiewicz K, McKay R (2002) Dopamine neurons derived from embry-onic stem cells function in an animal model of Parkinson’s disease. Nature 418 (6893):50–56
Kim YK, Lim HH, Song YK, Lee HH, Lim S, Han SM, Kim CJ (2005) Effect of acupuncture on 6-hydroxydopamine-induced nigrostratal dopaminergic neuronal cell death in rats. Neurosci Lett 384 (1–2):133–138

2497 Acupuncture Treatment for Parkinson’s Disease
Kleiner-Fisman G, Fisman DN, Sime E, Saint-Cyr JA, Lozano AM, Lang AE (2003) Long-term follow up of bilateral deep brain stimulation of the subthalamic nucleus in patients with advanced Parkinson disease. J Neurosurg 99 (3):489–495
Kodama Y, Ieda T, Hirayama M, Koike Y, Ito H, Sobue G (1999) Auditory brainstem responses in patients with autonomic failure with Parkinson’s disease and multiple system atrophy. J Auton Nerv Syst 77 (2–3):184–189
Krack P, Batir A, Van Blercom N, Chabardes S, Fraix V, Ardouin C, Koudsie A, Limousin PD, Benazzouz A, LeBas JF, Benabid AL, Pollak P (2003) Five-year follow-up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson’s disease. N Engl J Med 349 (20):1925–1934
Lam YC, Kum WF, Durairajan SS, Lu JH, Man SC, Xu M, Zhang XF, Huang XZ, Li M (2008) Ef fi cacy and safety of acupuncture for idiopathic Parkinson’s disease: a systematic review. J Altern Complement Med 14 (6):663–671
Lang AE, Gill S, Patel NK, Lozano A, Nutt JG, Penn R, Brooks DJ, Hotton G, Moro E, Heywood P, Brodsky MA, Burchiel K, Kelly P, Dalvi A, Scott B, Stacy M, Turner D, Wooten VG, Elias WJ, Laws ER, Dhawan V, Stoessl AJ, Matcham J, Coffey RJ, Traub M (2006) Randomized con-trolled trial of intraputamenal glial cell line-derived neurotrophic factor infusion in Parkinson disease. Ann Neurol 59 (3):459–466
Lee MS, Shin BC, Choi SM, Kim JY (2009) Randomized clinical trials of constitutional acupuncture: a systematic review. Evid Based Complement Alternat Med 6 Suppl 1:59–64
Lee MS, Shin BC, Kong JC, Ernst E (2008) Effectiveness of acupuncture for Parkinson’s disease: a systematic review. Mov Disord 23 (11):1505–1515
Levy R, Lang AE, Dostrovsky JO, Pahapill P, Romas J, Saint-Cyr J, Hutchison WD, Lozano AM (2001) Lidocaine and muscimol microinjections in subthalamic nucleus reverse Parkinsonian symptoms. Brain 124 (Pt 10):2105–2118
Li ZT, Yang WB (2005) Treatment of Parkinson’s disease mainly by comprehensive therapy: A Clinical Observation of 30 Cases. Journal of New Chinese Medicine 37 (10):52–54 (in Chinese)
Liang XB, Liu XY, Li FQ, Luo Y, Lu J, Zhang WM, Wang XM, Han JS (2002) Long-term high-frequency electro-acupuncture stimulation prevents neuronal degeneration and up-regulates BDNF mRNA in the substantia nigra and ventral tegmental area following medial forebrain bundle axotomy. Brain Res Mol Brain Res 108 (1–2):51–59
Liang XB, Luo Y, Liu XY, Lu J, Li FQ, Wang Q, Wang XM, Han JS (2003) Electro-acupuncture improves behavior and upregulates GDNF mRNA in MFB transected rats. Neuroreport 14 (8):1177–1181
Liu JY, Ren XQ (1993) The observation of the ef fi ciency in the 159 Parkinson’s disease cases treated by acupuncture. Journal of Clinical Acupuncture and Moxibustion 9 (5):10–11 (in Chinese)
Liu TH, Sadove MS (1974) Scalp needle therapy--acupuncture treatment for central nervous system disorders. Am J Chin Med (Gard City N Y) 2 (3):261–269
Liu YTS, Z.D., Li SJ (2001) Contrast study of microelectrode guided post - ventrual pallidotomy and Chinese medicine for treatment in Parkinson disease. Chinese Journal of Stereotactic and Functional Neurosurgery 14 (3):731 (in Chinese)
Ma J (1999) The theories of the Parkinson’s disease in traditional Chinese medicine. Journal of Hubei College of Traditional Chinese Medicine 1 (1):62–63 (in Chinese)
Ma J, Tian Q, Wang YC, Wang H (2003a) In fl uence of electroacupuncture on the content of glu-tamine in striatum of Parkinson’s disease rats. Shanghai Journal of Acupuncture and Moxibustion 22 (1):36 (in Chinese)
Ma J, Wang H (2001) Effect of electroacupuncture on TH content in mesencephalic substantia nigra of PD rats. Acupuncture Research 26 (4):288–291 (in Chinese with English abstract)
Ma J, Wang YC, Gan SY (2003b) In fl uence of electroacupuncture at Fengfu point and Taichong point on apoptosis of black substance neuron of PD rats. Hubei Journal of Traditional Chinese Medicine 25 (11):5–6 (in Chinese)
Ma MC, Qian H, Ghassemi F, Zhao P, Xia Y (2005) Oxygen-sensitive {delta}-opioid receptor-regulated survival and death signals: novel insights into neuronal preconditioning and protection. J Biol Chem 280 (16):16208–16218
250 T. Asakawa and Y. Xia
Mabrouk OS, Volta M, Marti M, Morari M (2008) Stimulation of delta opioid receptors located in substantia nigra reticulata but not globus pallidus or striatum restores motor activity in 6-hydroxydopamine lesioned rats: new insights into the role of delta receptors in parkinsonism. J Neurochem 107 (6):1647–1659
MacPherson H, White A, Cummings M, Jobst K, Rose K, Niemtzow R (2002a) Standards for reporting interventions in controlled trials of acupuncture: The STRICTA recommendations.STandards for Reporting Interventions in Controlled Trails of Acupuncture. Acupunct Med 20 (1):22–25
MacPherson H, White A, Cummings M, Jobst KA, Rose K, Niemtzow RC (2002b) Standards for Reporting Interventions in Controlled Trials of Acupuncture: the STRICTA recommendations. J Altern Complement Med 8 (1):85–89
Mansour A, Thompson RC, Akil H, Watson SJ (1993) Delta opioid receptor mRNA distribution in the brain: comparison to delta receptor binding and proenkephalin mRNA. J Chem Neuroanat 6 (6):351–362
McManus CA, Kaptchuk TJ, Schnyer RN, Goldman R, Kerr CE, Nguyen LT, Stason WB (2007) Experiences of acupuncturists in a placebo-controlled, randomized clinical trial. J Altern Complement Med 13 (5):533–538
Moher D, Pham B, Lawson ML, Klassen TP (2003) The inclusion of reports of randomised trials pub-lished in languages other than English in systematic reviews. Health Technol Assess 7 (41):1–90
Nambu A, Tokuno H, Takada M (2002) Functional signi fi cance of the cortico-subthalamo-pallidal ‘hyperdirect’ pathway. Neurosci Res 43 (2):111–117
Nieoullon A, Cheramy A, Glowinski J (1977) Nigral and striatal dopamine release under sensory stimuli. Nature 269 (5626):340–342
Nikkhah G, Duan WM, Knappe U, Jodicke A, Bjorklund A (1993) Restoration of complex senso-rimotor behavior and skilled forelimb use by a modi fi ed nigral cell suspension transplantation approach in the rat Parkinson model. Neuroscience 56 (1):33–43
O’Donnell BF, Squires NK, Martz MJ, Chen JR, Phay AJ (1987) Evoked potential changes and neuropsychological performance in Parkinson’s disease. Biol Psychol 24 (1):23–37
Odsberg A, Schill U, Haker E (2001) Acupuncture treatment: side effects and complications reported by Swedish physiotherapists. Complement Ther Med 9 (1):17–20
Palhagen S, Heinonen E, Hagglund J, Kaugesaar T, Maki-Ikola O, Palm R (2006) Selegiline slows the progression of the symptoms of Parkinson disease. Neurology 66 (8):1200–1206
Park HJ, Lim S, Joo WS, Yin CS, Lee HS, Lee HJ, Seo JC, Leem K, Son YS, Kim YJ, Kim CJ, Kim YS, Chung JH (2003) Acupuncture prevents 6-hydroxydopamine-induced neuronal death in the nigrostriatal dopaminergic system in the rat Parkinson’s disease model. Exp Neurol 180 (1):93–98
Park J, White A, Stevinson C, Ernst E, James M (2002) Validating a new non-penetrating sham acupuncture device: two randomised controlled trials. Acupunct Med 20 (4):168–174
Parkinson J (2002) An essay on the shaking palsy. 1817. J Neuropsychiatry Clin Neurosci 14 (2):223–236; discussion 222
Przedborski S (2005) Pathogenesis of nigral cell death in Parkinson’s disease. Parkinsonism Relat Disord 11 Suppl 1:S3–7
Przedborski S, Kostic V, Jackson-Lewis V, Naini AB, Simonetti S, Fahn S, Carlson E, Epstein CJ, Cadet JL (1992) Transgenic mice with increased Cu/Zn-superoxide dismutase activity are resistant to N-methyl-4-phenyl-1,2,3,6-tetrahydropyridine-induced neurotoxicity. J Neurosci 12 (5):1658–1667
Qi XJ, Wang S (2007) The progress in the clinical researches of the acupuncture therapy on Parkinson’s disease. Journal of Clinical Acupuncture and Moxibustion 23 (7):68–69 (in Chinese)
Rajendran PR, Thompson RE, Reich SG (2001) The use of alternative therapies by patients with Parkinson’s disease. Neurology 57 (5):790–794
Ren XM (2008) Fifty cases of Parkinson’s disease treated by acupuncture combined with madopar. J Tradit Chin Med 28 (4):255–257
Reynolds A, Laurie C, Mosley RL, Gendelman HE (2007) Oxidative stress and the pathogenesis of neurodegenerative disorders. Int Rev Neurobiol 82:297–325

2517 Acupuncture Treatment for Parkinson’s Disease
Rothblat DS, Schneider JS (1993) Response of caudate neurons to stimulation of intrinsic and peripheral afferents in normal, symptomatic, and recovered MPTP-treated cats. J Neurosci 13 (10):4372–4378
Rozas G, Guerra MJ, Labandeira-Garcia JL (1997) An automated rotarod method for quantitative drug-free evaluation of overall motor de fi cits in rat models of parkinsonism. Brain Res Brain Res Protoc 2 (1):75–84
Schapira AH (2009) Neurobiology and treatment of Parkinson’s disease. Trends Pharmacol Sci 30 (1):41–47
Schultz W, Romo R (1987) Responses of nigrostriatal dopamine neurons to high-intensity somatosensory stimulation in the anesthetized monkey. J Neurophysiol 57 (1):201–217
Shi Y, Liu HR, Wu HG (2002) The clinical study of the mechanism of acupuncture therapy for Parkinson’s disease. Chinese Journal of Clinical Rehabilitation 6 (December):3598–3599 (in Chinese with English abstract)
Shulman LM, Wen X, Weiner WJ, Bateman D, Minagar A, Duncan R, Konefal J (2002) Acupuncture therapy for the symptoms of Parkinson’s disease. Mov Disord 17 (4):799–802
Shults CW, Kimber T, Altar CA (1995) BDNF attenuates the effects of intrastriatal injection of 6-hydroxydopamine. Neuroreport 6 (8):1109–1112
Slevin JT, Gerhardt GA, Smith CD, Gash DM, Kryscio R, Young B (2005) Improvement of bilateral motor functions in patients with Parkinson disease through the unilateral intraputaminal infusion of glial cell line-derived neurotrophic factor. J Neurosurg 102 (2):216–222
Spina MB, Squinto SP, Miller J, Lindsay RM, Hyman C (1992) Brain-derived neurotrophic factor protects dopamine neurons against 6-hydroxydopamine and N-methyl-4-phenylpyridinium ion toxicity: involvement of the glutathione system. J Neurochem 59 (1):99–106
Su EL (2002) The clinical application and experience of scalp acupuncture at the specia areas of head imitating the viscus mapping in the tongue. Liaoning Journal of Traditional Chinese Medicine 29 (5):289–290 (in Chinese with English abstract)
Sun W, Sugiyama K, Fang X, Yamaguchi H, Akamine S, Magata Y, Namba H (2010) Different striatal D2-like receptor function in an early stage after unilateral striatal lesion and medial forebrain bundle lesion in rats. Brain Res 1317:227–235
Sun YM, Hoang T, Neubauer JA, Walters AS (2011) Opioids protect against substantia nigra cell degeneration under conditions of iron deprivation: a mechanism of possible relevance to the Restless Legs Syndrome (RLS) and Parkinson’s disease. J Neurol Sci 304 (1–2):93–101
Teismann P, Tieu K, Choi DK, Wu DC, Naini A, Hunot S, Vila M, Jackson-Lewis V, Przedborski S (2003a) Cyclooxygenase-2 is instrumental in Parkinson’s disease neurodegeneration. Proc Natl Acad Sci U S A 100 (9):5473–5478
Teismann P, Vila M, Choi DK, Tieu K, Wu DC, Jackson-Lewis V, Przedborski S (2003b) COX-2 and neurodegeneration in Parkinson’s disease. Ann N Y Acad Sci 991:272–277
Tian XS, Zhou F, Yang R, Xia Y, Wu GC, Guo JC (2008) Electro-acupuncture protects the brain against ischemic injury via up-regulation of delta-opioid receptors. J Chin Integr Med 6:632–638 (in Chinese with English abstract)
Turski L, Bressler K, Rettig KJ, Loschmann PA, Wachtel H (1991) Protection of substantia nigra from MPP + neurotoxicity by N-methyl-D-aspartate antagonists. Nature 349 (6308):414–418
Verma R, Nehru B (2009) Effect of centrophenoxine against rotenone-induced oxidative stress in an animal model of Parkinson’s disease. Neurochem Int 55 (6):369–375
Vickers A, Goyal N, Harland R, Rees R (1998) Do certain countries produce only positive results? A systematic review of controlled trials. Control Clin Trials 19 (2):159–166
Wang LL (2000) Acupuncture therapy of Parkinson’s disease. Modern Rehabilitation 4 (March):346–348 (in Chinese)
Wang LL, Chong HE, Liu YG, Zhu LL (2000) Effects of acupuncture on brain stem evoked poten-tial with Parkinson’s disease. J Nanjing Tradit Chin Med Univ 16 (4):229–231 (in Chinese with English abstract)
Wang Q, Chen XH, Tang CZ, Yang JJ, Xian ZH (2006a) The Effect of Acupuncture on the Content of Dopamine, HVA and DOPAC in Striate Body of Rats with Parkinson’s Disease. Chinese Journal of Integrative Medicine on Cardio/Cerebrovascular Disease 4 (6):92–93 (in Chinese)

252 T. Asakawa and Y. Xia
Wang S, Cai YY, Shang YJ, Jin-rong L (2006b) [Effects of head point-through-point electroacupuncture on SOD and LPO in the patient of Parkinson’s disease]. Zhongguo Zhen Jiu 26 (4):240–242 (in Chinese with English abstract)
Wang S, Qi XJ, Han D (2009) [Effect of electroacupuncture scalp point-through-point therapy on the expression of tyrosine hydroxylase and dopamine transporter mRNAs in substantia nigra of Parkinson’s disease model rats]. Zhongguo Zhen Jiu 29 (5):391–394 (in Chinese with English abstract)
Wang S, Zhou ZK, Hu BC (2003) Clinical study on head point-through-point electroacupuncture for treatment of Parkinson’s disease. Zhongguo Zhen Jiu 23 (3):129–131 (in Chinese with English abstract)
Wang YC, Cheng YH, Ma J, Gan SY, Wang SJ, Zhou H, Du YJ, Yang M, Shen F (2010) [Effects of electroacupuncture on the expression of GDNF and Ret in Parkinson’s disease model rats]. Zhongguo Zhen Jiu 30 (9):739–743 (in Chinese with English abstract)
Wen GQ, He XZ, Lu Y, Xia Y (2010a) Effect of acupuncture on neurotransmitters/modulators. In: Acupuncture Therapy for Neurological Diseases: A Neurobiological View. Springer-Tsinghua Press, Heidelberg, London, New York, Beijing,, pp 120–142
Wen GQ, Yang YL, Xia Y (2010b) Acupuncture-induced activation of endogenous opioid system. In: Acupuncture Therapy for Neurological Diseases: A Neurobiological View. Springer-Tsinghua Press, Heidelberg, London, New York, Beijing,, pp 104–119
White A, Ernst E (2001) Adverse events associated with acupuncture reported in 2000. Acupunct Med 19 (2):136–137
White A, Hayhoe S, Hart A, Ernst E (2001) Survey of adverse events following acupuncture (SAFA): a prospective study of 32,000 consultations. Acupunct Med 19 (2):84–92
Windels F, Carcenac C, Poupard A, Savasta M (2005) Pallidal origin of GABA release within the substantia nigra pars reticulata during high-frequency stimulation of the subthalamic nucleus. J Neurosci 25 (20):5079–5086
Wu Q (2002) Refractory senile diseases and the needling method of strengthening the body resno-scope and correspondance of Taiji structure in man and universe. Tianjin Journal of Traditional Chinese Medicine 19 (2):63–66 (in Chinese)
Wu WG, Li CB, Sun P (1996) Treating the Parkinson’s disease by hitting the acupoints. Journal of Clinical Acupuncture and Moxibustion 12 (4):39–40 (in Chinese)
Xi GF, Cai DH (1995) The analysis of the clinical ef fi cacy in the Parkinson’s disease cases treated by acupuncture and traditional Chinese medicine. Shanghai Journal of Acupuncture and Moxibustion 14 (6):243 (in Chinese)
Xi GF, Cai DH, Chen GM, Yu AZ (1996) The in fl uence of the tremor myoelectricpotential by electrical stimulation at the scalp acupoints in Parkinson’s Patients. Shanghai Journal of Acupuncture and Moxibustion 15 (3):5–6 (in Chinese)
Xia Y, Cao XD, Wu GC, Cheng JS (2010) Acupuncture Therapy for Neurological Diseases: A Neurobiological View (Research Monograph). Springer-Tsinghua Press, Heidelberg, London, New York, Beijing,
Xu B, Ma C, Chen GZ (2002) Clinical Observation on Regulative Action of Acupuncture on Monoamine Neurotransmitters in Cerebrospinal Fluid in the Patient of Parkinson Disease. Zhongguo Zhen Jiu 22 (3):183–185 (in Chinese with English abstract)
Yamashita H, Tsukayama H, Tanno Y, Nishijo K (1998) Adverse events related to acupuncture. JAMA 280 (18):1563–1564
Yang L, Du Y, Xiong J, Liu J, Wang Y, Li Y, Li L (2010) Acupuncture treatment for Parkinson disease: A systematic review. Chinese Journal of Evidence-Based Medicine 10 (6):711–716 (in Chinese with English abstract)
Yang Y, Xia X, Zhang Y, Wang Q, Li L, Luo G, Xia Y (2009) delta-Opioid receptor activation attenuates oxidative injury in the ischemic rat brain. BMC Biol 7:55
Yin H, Tang Y, Chen J, Yu S (2009) Increased expression of PKA and CREB1 in substantia nigra of Parkinson’s disease mice by electroacupuncture therapy. Chinese Journal of Gerontology 29 (3):263–264 (in Chinese with English abstract)

2537 Acupuncture Treatment for Parkinson’s Disease
Yu ZQ (1994) Using the scalp plus Siguan acupunture to treat Parkinson’s disease. Journal of Zhejiang University of Traditional Chinese Medicine 031 (6):45 (in Chinese)
Yuan H, Liu P, Zheng C, Wang X, Zhang Z, Li C, Jiao S, Bai L, Liang L (2010) The possible mechanism of oxidative stress on acupuncture treatment in the rat of Parkinson’s disease. Chinese Journal of Health Care and Medcine 12 (1):45–47 (in Chinese with English abstract)
Zhang J, Gibney GT, Zhao P, Xia Y (2002) Neuroprotective role of delta-opioid receptors in cortical neurons. Am J Physiol Cell Physiol 282 (6):C1225–1234
Zhang J, Haddad GG, Xia Y (2000) delta-, but not mu- and kappa-, opioid receptor activation pro-tects neocortical neurons from glutamate-induced excitotoxic injury. Brain Res 885 (2):143–153
Zhang JF, Sun GS, Zhao GH (2005) [Observation on therapeutic effect of herbs-partitioned moxi-bustion on Parkinson disease of 54 cases]. Zhongguo Zhen Jiu 25 (9):610–612 (in Chinese with English abstract)
Zhang L, Tang Y, Yu S (2006) Increased expression of dopamine transporter in Parkinson’s Disease mice substantia nigra by electroacupuncture therapy. Journal of Chengdu University of Traditional Chinese Medicine 29 (3):30–33 (in Chinese with English abstract)
Zhang L, Xi GF, He BM (1997) Effects of the cerebral antioxidase by scalp-acupuncture and tra-ditional Chinese medicine in Parkinsonian mouse models. Shanghai Journal of Acupuncture and Moxibustion 16 (6):32–33 (in Chinese)
Zhang NZ, Han XH (1996) The observation of the clinical ef fi ciency in the 35 cases of Parkinson’s disease treated by scalp and body acupuncture. Zhongguo Zhen Jiu 15 (2):5 (in Chinese with English abstract)
Zhao Y, Sun Z, Huang L, Li H (2010) Impact of acupuncture and moxibustion on behaviors and apoptosis in rats with Parkinson’s disease. World Journal of Integrated Tradititional and Western Medicine 5 (3):209–211 (in Chinese with English abstract)
Zhou F, Huang DK, Xia Y (2010) Neuroanatomic basis of acupuncture points. In: Acupuncture Therapy for Neurological Diseases: A Neurobiological View. Springer-Tsinghua Press, Heidelberg, London, New York, Beijing,, pp 32–80
Zhu WX, Xi GF, Ju JH (1996) The effect of the cerebral dopamine in the Parkinson’s disease mouse models treated by acupuncture combined with traditional Chinese medicines. Acupuncture Research 21 (4):46–48 (in Chinese)
Zhu Z (2001) Observation of the rehabilitation ef fi ciency by therapy of acupuncture with Chinese medicine in Parkinson’s disease. Modern Rehabilitation 5 (11):125 (in Chinese)
Zipp F, Demisch L, Derouiche A, Fischer PA (1998) Glutamine synthetase activity in patients with Parkinson’s disease. Acta Neurol Scand 97 (5):300–302
View publication statsView publication stats