abc’s of pediatric adjusting modifications for the pediatric patient stephanie c. o’neill, dc,...
TRANSCRIPT
ABC’s Of Pediatric Adjusting
Modifications for the Pediatric Patient
Stephanie C. O’Neill, DC, DICCP
“Wellness Care”
Fysh recommends spinal check-ups– for school-aged children, at least every 3 months– for pre-school children, at least every 2 months– for infants in the first 2 years of life, at least every
month
Determining Visit Frequency
Several things should be taken into account:
History• physical, chemical, and/or mental trauma will increase the
likelihood s/he will require a higher frequency
Examination findings
Lifestyle, activity and stress levels
Joan Fallon
The Child Patient: A Matrix for Chiropractic Care– published as a supplement to JCCP
(Vol. 6, No. 3)
– www.icapediatrics.com
Overview
Assessing the pediatric patient
Unique features of the pediatric spine
Adapting your technique
Comfort and Safety
Newborn Evaluation
Where do you start?
Newborn Evaluation
Reverse Fencer Maneuver– Heel swing– Acetabular pump
Supine Leg Check Instrumentation - atlas fossa reading Posture analysis Static Palpation Motion palpation
McMullen Reverse Fencer
<6 months old less accurate once the child gains strength and control of
the cervical spine musculature
McMullen M. Assessing Upper Cervical Subluxations in Infants Under Six Months- Utilizing the Reverse Fencer Response. ICA International Review of Chiropractic. March/April;1990,39-41.
Reverse Fencer- Part 1
Heel swing: Hold infant upside down, making sure to have
a solid grip on their ankles Release one foot slowly, watch the child‘s head
turn to that side Repeat on other side
WARNING!
Before you suspend a child by their legs you must rule out hip instability.
Congenital Hip Dysplasia
Reverse Fencer- Part 1
Heel swing (cont‘d):
Compare motion from side to side– restricted? twitching?
What if...?
Child arches backwards (opisthotonis) meningeal tension
What do you do? Adjust them...
– upper C spine, occiput, sacrum
“He‘s so strong, he can hold his head up already...”
Infant pulls away when you hold them against your shoulder
Only comfortable in the “football hold”
Problems breastfeeding/sleeping
Etc…
Reverse Fencer-Part 2
Acetabular pump: Infant supine, apply pressure along the shaft of
the femur into the acetabular fossa Compare the resistance on each side
The “spongy“ side is said to be the side of atlas laterality
Interpreting your findings...
“a negative response (heel swing) indicates a subluxation complex between the atlas-axis or atlas-occ. on that side“
Interpreting your findings...
Differentiating b/w atlas and occ.
Dr. McMullen suggests that you look at the Acetabular Pump findings– spongy side=atlas laterality– even=occiput
Supine Leg Check
Lay the infant supine Gently straighten the legs
– make sure that the head is in a neutral position
Compare medial malleoli, fat folds at the knee, etc.
Long leg side is “said to be“ the
side of atlas laterality...
Prone Leg Check – Older Child
Instrumentation
DP nervoscope & newborns?– can‘t sit up– lots of skin
– accuracy? size of probes patient relaxation
Old enough to sit still...
Advances in Instrumentation
www.titronics.com
Atlas fossa reading
DT-25 is used to measure atlas fossa temperatures– hold 1/4“ away from the skin – repeat 3x each side
Remember to take into consideration the way the child was being held, sitting in the sun in the car seat, etc.
Atlas fossa reading
The cold side is “said to be“ the side of atlas laterality...
More likely, it tells us there is an imbalance
What if…?
Atlas fossa: R 85 L86 No other findings in the cervical spine
_ _ _ _ _ _
What if…?
Atlas fossa: R 85 L86 No other findings in the cervical spine
S A C R U M
Posture analysis
Head tilt Head rotation High shoulder Scoliosis High ilium Genu varus and valgum Internal & extenal foot rotation
Normal Development
Normal evolution from bowlegs to knock-knees to normal valgus
2 years 3 years 5 years
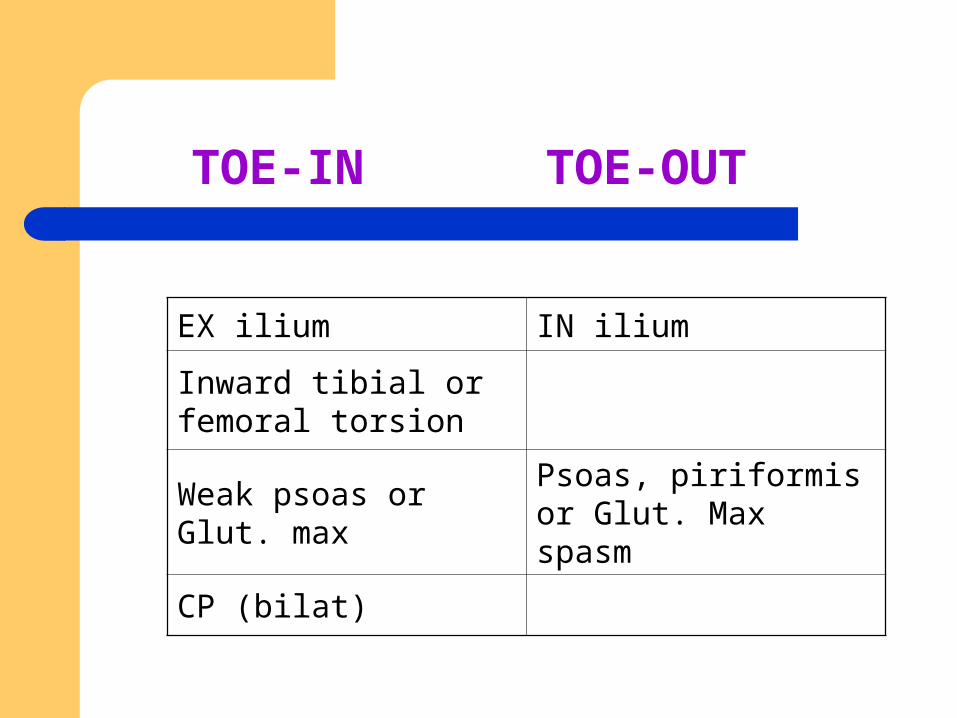
TOE-IN TOE-OUT
EX ilium IN ilium
Inward tibial or femoral torsion
Weak psoas or Glut. max
Psoas, piriformis or Glut. Max spasm
CP (bilat)
Static Palpation
Taut and tender fibers Muscle spasm
– common with congenital torticollis
Sudoriferous changes – stickiness/dryness
Temperature
Pay attention to the child!
They’ll let you know…– squirming– fussiness– clutching at your hand– etc.
Clinical Note
Just because it sticks out doesn‘t mean it‘s subluxated!
For Example
L1 is often prominant in infants (similar to the adult‘s T4) but it is not always fixed
You must evaluate the motion, feel for springiness, T&T fibers, sudoriferous changes, instumentation findings, etc.
Motion palpation
Similar to adults but much more subtle– ligament laxity, cartilagenous vertebrae
Be creative!
Gross Range of Motion
Can be evaluated by “playing“ with them– Can they bend in half forward?– Can they bend ear to foot equally on both sides?– Can they cross shoulder to opposite foot
comfortably?
Remember, newborns should be flexible!
Sacrum and Pelvis
Gluteal Cleft Deviation Sacral Dimples Dangling legs Gluteal Folds
Gluteal Cleft Check
Pinch cheeks togetherCleft should be midline
Gluteal Cleft Deviation
If it deviates...
may either be to the side of posterior-inferior sacroiliac subluxation (P-R, PI-R, P-L, PI-L) or to the side of anterior-inferior sacral movement at the lumbosacral junction
(Fysh, 2002)
Sacral Dimples
Asymmetry (with fixation of SI joints) suggests pelvic misalignment
Palpate S2 to PSIS
Other things to note...
Dangling legs– ilium rotation
Gluteal fold observation– sacral tilts
Older Babies and Toddlers
As they start to be mobile, you have to become more creative...
– Do they have to be on a table to get adjusted?
– Follow them as they crawl, play, etc.
Toddlers & School Aged Kids
“Flying Airplane”– Child lays on their tummy
(table, dad’s lap, your lap…)– Have them hold their arms out like wings
– You lift both legs and go through motion palpation of lumbars ~> thoracics
Toddlers
Want to be in control of their world– important to respect their need for autonomy but
you also have to maintain control of the interaction
Give them choices between 2 acceptible options“Do you want to lay on your front or on your back?“
NOT “Do you want to get adjusted?“
Unique Features…
Unique Features…
Anatomy Biomechanics
MacGregor, 2000
Anatomy
Underdeveloped cervical lordosis Low vertebral height Horizontal facets (until age 10) Undeveloped uncinates (until age 7)
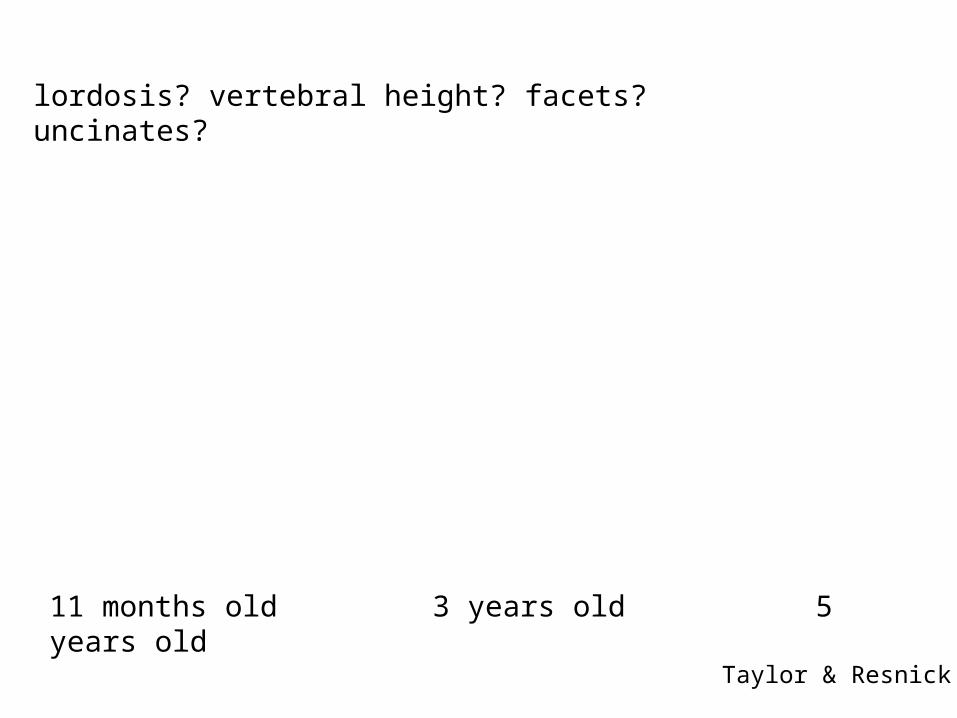
11 months old 3 years old 5 years old
Taylor & Resnick
lordosis? vertebral height? facets? uncinates?
Biomechanics
Large head Weak muscles Spine is more flexible
MVA injuries
How will this affect your adjustment?

Joint End Play
Determined by the degree of flexibility and elasticity of a joint
Increased in children
Some say that…“Spinal adjusting in the pediatric spine should be performed at a point somewhat before the end of the passive range is reached.”
Motion
Joints of Lushka/Uncovertebral Joints– begin to develop between 6-9 years of age
(are complete at age 18)
Function: guide the coupled motion of rotation and lateral
flexion, limiting side bending
Pediatric Technique
Chiropractic Care for the Pediatric Patient, Fysh
Adjusting Considerations
Minimize excessive range of motion/forces Reduce depth of thrust
C-spine: lat bend and minimum rotation (30 degrees)
Sometimes, pre-stress can effect a correction...
Specificity
Contact Points
Pediatric vertebrae are much smaller– cervical spine of a newborn is <2 inches in length
High degree of specificity is required
Pad of the finger-tip or thumb tip
Occiput
Findings Fixation between Co/C1* Increased tension in suboccipital muscles
– unilateral/bilateral
*If significantly fixed, infant may become irritable even with light palpation
Occiput (AS)
Correction Light cephalad traction with the fingertips When released, infant becomes relaxed & may even
fall asleep
Atlas
Findings Fixation at C1
We’ll add… T&T Instrumentation Etc.
Atlas
Correction Place lateral tip of the index finger against the
prominent C1 transverse Laterally bend to the side of contact until end-range A quick, light, low-amplitude thrust is delivered to the
tip of the C1 transverse toward the neutral position
*Not uncommon for a young baby to cry 15-20 seconds(stimulate Moro response)
Pediatric Drop Piece
Clinical Note
Compared with C1, rotation of C2-C7 is significantly reduced
C1/C2 40 degrees
C2/C3 3 degrees
C7/T1 2 degrees
Therefore, C2 and C7 are prone to subluxation with end-range rotation of the head
C2 – C7
Findings Muscle spasm – usually side of spinous process
deviation Fixation – spinous does not move away with lateral
bend
C2 – C7
Correction Tip of index finger on articular pillar Rotate head 25-30 degrees Laterally bend the neck over contact finger If no release is felt, apply a light thrust
Thoracic Spine – Infant & Child
Prone thoracic adjusting
If the child will not lie quietly in the prone position (lifting head, extending trunk)…
Move infant to edge of the table, supporting the legs over the edge
Doctor can flex the abdomen over the table’s edge to induce a normal thoracic curve
Infant upright, chest to chest with doctor or parent Infant lying prone on top of parent
Thoracics
Correction
DTH - thumbs on either side of the spinous process
Anterior adjusting– Not recommended for children under 3 years of age– Flexible rib cage
L1 – L3
Sagittal plane, facet joints
Correction Contact mammillary process with a light thumb
contact P-A, I-S thrust
L4 – L5
Correction Contact the spinous process (side of spinous
rotation) with a light thumb contact Apply light pressure over the contralateral
mammilary process (stabilization) Thrust toward the spinous process
*Side Posture: infants >12 months
Sacro-iliac
Correction Prone or side posture
– Light adjustive thrust– Direction appropriate to correct PI, AS, In or Ex
References
Anrig & Plaugher. Pediatric Chiropractic. Baltimore, MD: Lippincott Williams & Wilkins, 1998.
Anrig-Howe C. Scientific Ramifications for Providing Pre-natal and Neonate Chiropractic Care. The American Chiropractor, 1993; May/June: 20-26.
Fallon. Textbook on Chiropractic and Pregnancy. Arlington, VA: International Chiropractors Association, 1994.
Forrester J. Chiropractic Management of Third Trimester In-utero Constraint. Canadian Chiropractor, 1997; 2(3): 8-13.
Fysh. Chiropractic Care for the Pediatric Patient. Arlington VA: ICACCP, 2002. Kunau P. Application of the Webster In-utero Constraint Technique: A Case
Series. Journal of Clinical Chiropractic Pediatrics, 1998; 3(1): 211-6. McMullen M. Assessing upper Cervical Subluxations in Infants Under Six
Months. ICA International Review of Chiropractic, 1990; March/April: 39-41 Pistoles R. The Webster Technique: A Chiropractic Technique with Obstetric
Implications. JMPT, 2002; 25(6). Webster L. Chiropractic Care During Pregnancy. Today’s Chiropractic, 1982;
Sept/Oct: 20-22.