a review on the impact of p-glycoprotein on the penetration of drugs into the brain. focus on...
TRANSCRIPT

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 1/13
REVIEW
A review on the impact of P-glycoprotein on the
penetration of drugs into the brain.
Focus on psychotropic drugs
Kristian Linnet ⁎, Thomas Broeng Ejsing
The Department of Forensic Chemistry, Institute of Forensic Medicine, University of Copenhagen, Frederik V ’s Vej 11,2100 Copenhagen, Denmark
Received 19 December 2006; received in revised form 15 May 2007; accepted 19 June 2007
Abstract
In recent years there has been increasing focus on the role of the drug transporter P-glycoprotein(P-gp) with regardto drug penetration into thebrain. Studies using mice devoid of functional P-gphave revealed that P-gp at theblood–brain barrier (BBB) canexerta profound effecton theabilityof some drugs to enter the brain, e.g. cardiovascular drugs (digoxin, quinidine), opioids
(morphine, loperamide, methadone), HIV protease inhibitors, the new generation of anti-histamines, and some antidepressants and antipsychotics. Among the latter group, risperidone isstrongly influenced having about 10 times higher cerebral concentration in P-gp knock-out micethan in control mice. Taking into account that polytherapy is commonplace in psychiatry,theoretically there is a risk of drug–drug interactions with regard to P-gp at the BBB. Here wereview the evidence for a role of P-gp with regard to psychoactive drugs from in vitro studies andexperiments in knock-out mice devoid of functional P-gp. Moreover, the evidence for significantdrug–drug interactions involving psychotropic drugs in rodents is considered. Clinical observa-tions suggesting a role for P-gp in relation to drug–drug interactions at the BBB are sparse, and adefinite conclusion awaits further studies. Also, the possible clinical relevance of P-gp geneticpolymorphisms is questionable, and more investigations are needed on this subject.© 2007 Elsevier B.V. and ECNP. All rights reserved.
KEYWORDS
P-glycoprotein;Psychotropic drugs;Blood–brain barrier;Mdr1a/1b knock-out mice;Drug–drug interactions
1. Introduction
The blood–brain barrier (BBB) is a major impediment to theentry of many therapeutic drugs into thebrain, andduring thelast decadeit hasbecome clear that multispecific, xenobiotictransporters play an important role at the BBB. With the
sequencing of the human genome, it has been estimated thatapproximately 500–1200 genes code for transport proteins(Sakaeda et al., 2003). At present, messenger RNA (mRNA)from 15 of these drug transporters has been found at the BBB.They belong to the following subfamilies: the multidrugresistance protein (MDR), the multidrug resistance-associat-ed protein (MRP), the organic anion transporter (OAT), theorganic anion transporting polypeptide (OATP), the organiccation transporter (OCT), the concentrative nucleoside
⁎ Corresponding author. Tel.: +45 3532 6100; fax: +45 3532 6085.E-mail address: [email protected] (K. Linnet).
0924-977X/$ – see front matter © 2007 Elsevier B.V. and ECNP. All rights reserved.doi:10.1016/j.euroneuro.2007.06.003
www.e l sev i e r .com/ locate /eu roneu ro
European Neuropsychopharmacology (2008) 18, 157–169

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 2/13
transporter (CNT), and the equilibrative nucleoside trans-porter (ENT) (Bauer et al., 2005). P-glycoprotein (P-gp),which belongs to the MDR family, was one of the first of theseproteins that was identified at the BBB, and thus the bulk of studies concerning drug efflux from the brain deal with P-gp.During the last decade it has been shown that P-gp exerts animportant influence on the brain concentrations of somedrugs (Lin and Yamazaki, 2003). Experiments in mice lackingfunctional P-gp at the BBB have revealed drasticallyenhanced brain levels (20 times or higher than those of thecontrol animals) of e.g. theanthelmintic drug ivermectin, thecardiac glycoside digoxin and the HIV protease inhibitornelfinavir (Schinkel et al., 1994; Choo et al., 2000; Mayeret al., 1996). Likewise, in a number of cases concerning Colliedogs devoid of functional P-gp severe signs of neurologicalsymptoms were reported after treatment with the chemo-therapeutic agent vincristine and the antidiarrheal agentloperamide (Mealey et al., 2003; Hugnet et al., 1996). P-gp atthe BBB may in particular influence the effect of psychotropicdrugs. Moreover, there is a possibility of drug–drug interac-tions with regard to P-gp. Here, we review the evidence of
drug–
drug interactions involving primarily psychotropic drugsand P-gp at the BBB on the basis of in vitro studies, animalexperiments, and observations in humans. Additionally,pharmacogenetic aspects in relation to P-gp are considered.
2. General properties of P-gp
2.1. Structure and function
P-gp is located mainly in theplasma membrane whereit activelyextrudes drugsfrom thecell. It was originally discovered in 1976in drug-resistant ovary cells from Chinese hamsters (Juliano andLing, 1976). Humans possess one gene (originally named MDR1
but today also denoted as ABCB1) encoding drug transporting P-gp whereasrodents havetwo (mdr1a andmdr1b). Thecombinedtissue distribution of these two genes in rodents roughlycoincides with that of the single MDR1 in humans, indicatingthat mdr1a and mdr1b together fulfil the same function as thehuman MDR1 (Bosch and Croop, 1998). Species variation withrespect to P-gp exists. Cutler et al. (2006) found about similarbehaviour of P-gp in mice and rats in relation to the potent P-gpinhibitor GF120918 (Elacridar) but not in guinea pigs. The latterspecies required about ten times higher concentration of GF120918 than rats and mice for a similar degree of inhibition.Murakami et al. (2000) compared BBB permeability in mice andrats for a range of compounds, including typical P-gp substrates
such as quinidine, and found similar values. Generally, thefunctional consequences of species variation may vary fromcompound to compound (Yamazaki et al., 2001). Furtherstudies, however, are needed on this aspect.
The human P-gp consists of approximately 1280 aminoacids and weighs around 170 kDa (Sharom, 1997; Schinkel,1999). It contains two homologous, but not identical, partsjoined together by a short linker region (Bosch and Croop,1998). Each part comprises six transmembrane α-helices andan ATP-binding site (Fig. 1). The 12 transmembrane segmentsfold together to form a barrel-like structure that traversesthe plasma membrane. The two ATP-binding sites are locatedat the cytoplasmic site, and hydrolysis of ATP provides theenergy necessary for drug transport (Schinkel, 1997).
The exact mechanism of drug transport has not beenelucidated yet, but increasing amounts of evidence suggestthat P-gp recognizes its substrates in the plasma membrane(Chen et al., 2001; Shapiro and Ling, 1998; Lugo and Sharom,2005; Loo and Clarke, 2005). P-gp is able to recognize andtransport an impressive array of substrates ranging in sizefromapproximately 250 Da (cimetidine) to more than 1850 Da(gramicidin D) (Schinkel, 1999). These substrates include awidevariety of chemotherapeutic agents of natural origin suchas anthracyclines (doxorubicin), vinca alkaloids (vinblastine),epipodophyllotoxins (etoposide), and taxanes (paclitaxel)(Kim, 2002). P-gp substrates also include drugs and pesticidessuch as the immunosuppressive agents cyclosporine A (CsA)and FK506 (Saeki et al., 1993), cardiac glycosides such asdigoxin (Begley, 2004), antipsychotics and antidepressants likerisperidone, nortriptyline, and citalopram (Uhr et al., 2000;Uhr and Grauer, 2003; Ejsing and Linnet, 2005; Ejsing et al.,2005), HIV protease inhibitors (Choo et al., 2000; Begley,2004), and the anthelmintic pesticide ivermectin (Begley,2004). P-gp substrates may act as competitive inhibitors of P-gp, e.g. the drugs cyclosporine A and verapamil (Saeki et al.,
1993; Ford and Hait, 1990), which have been used as P-gpinhibitors since the early eighties.Many drugs are racemates and the question of stereoselec-
tivity of transport mediated by P-gp thus is of relevance. Arecent study by Miura et al. (2007) showed that thepharmacokinetics of fexofenadine, a probe substrate for P-gp,displays stereoselectivity. Apparently, P-gp has higher affinityfor S(+)-fexofenadine than for R(−)-fenadine resulting in higheroral and renal clearance of the S(+)-form. Similarly, a study byBertilsson et al. (1991) on the relationship between plasma andcerebrospinalfluidconcentrations of the enantiomers of (E)-10-OH-nortriptyline showed that the (−)-enantiomer was moreeffectively transported out from the CNS than the (+)-enantiomer. Studies on methadone pharmacokinetics also
suggests stereoselectivity with regard to P-gp mediatedtransport (see later).
2.2. Tissue distribution of P-gp
At the interface between the blood and the central nervoussystem P-gp is present in the microvessels and the choroidplexus. In the former, P-gp is found at the luminal membraneof the endothelial cells lining the capillaries (Tanaka et al.,1994; Beaulieu et al., 1997; Virginento et al., 2002) (Fig. 2A).
Figure 1 Two-dimensional representation of human P-gp. The12 Transmembrane segments fold together to form a threedimensional barrel-structure in the membrane. N-linked glyco-sylation trees that are found in the first extracellular loop. TheATP binding domains are shown with circles. Modified fromSchinkel et al. (1999).
158 K. Linnet, T.B. Ejsing

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 3/13
Here it excretes compounds into the blood, thus preventinge.g. drugs from gaining access to the brain. In the choroidplexus, P-gp is located at the apical surface of the epitheliacells that constitute the ventricular exposed surface of theplexus (Fig. 2B) (Rao et al., 1999; Warren et al., 2000).Furthermore, P-gp is expressed at the blood–spinal cordbarrier (Sugawara et al., 1990).
Apart from the central nervous system, P-gp is also foundin the heart, lungs, pancreas, and other organs including theapical surface of the columnar epithelial cells of theintestines. This is the major uptake place for drugs into thebody, and several studies have proved that P-gp activelysecretes drugs into the intestinal lumen (Mayer et al., 1996;Sparreboom et al., 1997; Van Asperen et al., 2000). Likewise,P-gp is positioned at the major exit routesof the body, namelythe biliary epithelial cells, and proximal renal tubules(Cordon-Cardo et al., 1990). P-gp is also located in theplacenta (Young et al., 2003).
3. In vitro studies on drug/P-gp relations
Several psychoactive drugs have been shown to be substratesand/or inhibitors of human P-gp in vitro. One principle of assessing interaction between a drug and P-gp is to measureP-gp mediated ATP-ase activity (Boulton et al., 2002). P-gpprovides active transport by hydrolysis of ATP. The majority of drugs that stimulate the ATP-ase activity of P-gp are alsotransported by the protein. Thus, measurement of the ATP-ase activity in vitro can be used to identify P-gp substrates. Inthis way risperidone and quetiapine have been identified asgood P-gp substrates comparable to the potent competitiveinhibitor and model compound verapamil (Table 1) (Boultonet al., 2002; Ejsing et al., 2005). The main metabolite of risperidone, 9-OH-risperidone, and the antipsychotic drugs
olanzapine and chlorpromazine are intermediate substrates(Boulton et al., 2002; Ejsing et al., 2005), whereas clozapine,haloperidol and nortriptyline were poor substrates with K mvalues that were 10-fold higher than that of verapamil(Boulton et al., 2002; Ejsing et al., 2006).
In another in vitro model, El Ela et al. (2004) measured theP-gp mediated efflux of 14 psychoactive compounds across ahuman colon adenocarcinoma (Caco-2) cell monolayer. Theyclassified six of these drugs as P-gp substrates: amisulpride,demethyl-clozapine, domperidone, flupentixol, fluphen-azine, and fluvoxamine. The drugs not found to be P-gpsubstrates included quetiapine, olanzapine, clozapine, andhaloperidol. This contrasts somewhat with the results of
Boulton et al. (2002), who identified quetiapine andolanzapine as substrates. P-gp is thought to recognize itssubstrates in the plasma membrane, and one reason for thedifferences may therefore be the membrane composition, asthe Caco-2 cells are of human origin, whereas the membranefractions used in the ATP-ase assay were from insect cells.Several studies have shown that the membrane compositioncan influence the substrate specificity of P-gp (Germannet al., 1990; Romsicki and Sharom, 1999; Riou et al., 2003),and thus caution is needed when comparing results fromdifferent cell and membrane systems (Weiss et al., 2003).
Permeation studies in primary porcine brain microvesselendothelial cells showed that P-gp influenced the penetra-tion of amisulpride through the monolayer, whereas cloza-
pine and N -desmethylclozapine were not transported(Härtter et al., 2003). The results were supported by Caco-2 cell transport studies. Using monolayers of bovine brain
microvessel endothelial cells, Rochat et al.(1999) did notfindany interaction between P-gp and citalopram. However, invivo studies in mice have later verified that citalopram is aP-gp substrate (see later).
As P-gp is one of the important proteins involved inmultidrug resistance of tumours, extensive research has beenundertaken to find drugs that can reverse the resistance. Inthis process numerous psychotropic drugs have beenscreened, and some exhibited a high inhibitory potential.Among these are the antidepressants sertraline and parox-etine, both of which inhibited the uptake of calcein-acetoxymethylester (calcein-AM) in a porcine cell line trans-fected with human P-gp (Weiss et al., 2003). The IC50 (the
concentration leading to half maximum inhibition of thecalcein AM transport) was 29.8μM for paroxetine and 31.8 forsertraline, which is comparable to the value of the efficientP-gp inhibitor quinidine (33.8 μM) but still higher than that of verapamil (18.9 μM). Szabó et al. (1999) tested the effect of psychotropic drugs on cellular uptakeof the model compoundrhodamine 123 in cell lines transfected with human P-gp anduptake of daunorubicin in tumour cell lines selected for P-gpmediated resistance. They found that the tricyclic antide-pressant amitriptyline as well as fluphenazine and haloper-idol were good inhibitors comparable to the powerful P-gpinhibitor cyclosporine A. Moreover, they found that theremaining drugs (maprotiline, trimipramine, desipramine,imipramine and doxepin) all to a greater or lesser extent
Figure 2 P-gp at the blood–central nervous system barrier.A: The BBB barrier (modified from Schinkel et al. (1999)). B: Thechoroid plexus.
159A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 4/13
increased the cellular uptake of daunorubicin. Finally,Ibrahim et al. (2000) examined the effect of 33 drugs andmetabolites on the cellular uptake of the P-gp substraterhodamine 123 in human Caco-2 cells. Among the drugswere several psychoactive drugs, and especially amitripty-line, chlorpromazine, pimozide and protriptyline displayeda high degree of P-gp inhibition, reaching at least 80%inhibition. They also found haloperidol, trimipramine,
clozapine, and desipramine to be intermediate inhibitorsdisplaying 20–60% inhibition. Some drugs, such as nortrip-tyline, chlorazepate, triazolam, and estazolam displayed noinhibitory effect at all.
Interaction between P-gp and nutritional components isalso a subject of interest. The active components of St.John’s wort hypericin and hyperforin are able to inhibit P-gpin vitro (Wang et al., 2004a). More important, however, isthe induction effect of St. John’s wort (see later). Anothernutritional component of interest is grape fruit juice.Generally, effects of grapefruit juice have been ascribed toinhibition of the CYP3A4 enzyme. However, grapefruit juicecomponents are also able to inhibit P-gp as demonstrated byin vitro studies (Wang et al., 2001).
The in vitro study results suggest generally that somepsychotropic drugs can exert an important effect with regardto drug uptake in the brain. However, two factors ought to bekept in mind. First, the inhibitory effect of most of the drugsare only manifest when the concentration is in themicromolar range, which is larger than the serum levelstypically observed during therapeutic conditions (Ibrahimet al., 2000). Moreover, studies in cell lines easily lead to
exaggerated expectations regarding the effects in vivo, ascell lines, chosen for their resistance to P-gp substrates,often express amounts of P-gp that by far exceeds thoseobserved in vivo (Litman et al., 2001), thereby overshadow-ing other factors that may influence drug distribution. Polliet al. (2001) concluded that some in vitro techniques werereliable for high affinity- and others for low-affinity drugswith respect to P-gp. Thus, when several in vitro techniquesare applied on the same drugs, discrepant results areobtained in some cases. Accordingly, in vitro studies mayprovide an indication on the relationship to P-gp, but in vivotechniques as described in the following more clearly revealthe functional consequences (with reservations for possiblespecies variation).
Table 1 Psychotropic drugs identified in vitro as substrates/inhibitors for P-gp
In vitro interaction principle References
Amisulpride Microvessel permeation Härtter et al. (2003)Caco-2 cell transport Härtter et al. (2003)
El Ela et al. (2004)Schmitt et al. (2006)
Chlorpromazine Rhodamine 123 uptake in human Caco-2 cells Ibrahim et al. (2000)ATP-ase Boulton et al. (2002)
Clozapine Rhodamine 123 uptake in human Caco-2 cells Ibrahim et al. (2000)ATP-ase Boulton et al. (2002)
Demethyl-clozapine Caco-2 cell transport Boulton et al. (2002)Desipramine Rhodamine 123 uptake in human Caco-2 cells Ibrahim et al. (2000)
Rhodamine123/daunorubicin cellular uptake Szabó et al. (1999)Domperidone Caco-2 cell transport El Ela et al. (2004)Doxepin Rhodamine123/daunorubicin cellular uptake Szabó et al. (1999)Fluphenazine Rhodamine123/daunorubicin cellular uptake Szabó et al. (1999)
Caco-2 cell transport El Ela et al. (2004)Flupentixol Caco-2 cell transport El Ela et al. (2004)Fluvoxamine Caco-2 cell transport El Ela et al. (2004)Haloperidol Rhodamine123/daunorubicin cellular uptake Szabó et al. (1999)
Rhodamine 123 uptake in human Caco-2 cells Ibrahim et al. (2000)ATP-ase Boulton et al. (2002)Imipramine Rhodamine123/daunorubicin cellular uptake Szabó et al. (1999)Maprotiline Rhodamine123/daunorubicin cellular uptake Szabó et al. (1999)Nortriptyline ATP-ase Ejsing et al. (2005)Olanzapine ATP-ase Boulton et al. (2002)Paroxetine Calcein AM transport Weiss et al. (2003)Pimozide Rhodamine 123 uptake in human Caco-2 cells Ibrahim et al. (2000)Protriptyline Rhodamine 123 uptake in human Caco-2 cells Ibrahim et al. (2000)Quetiapine ATP-ase Boulton et al. (2002)Risperidone ATP-ase Boulton et al. (2002)
Ejsing et al. (2005)9-HO-Risperidone ATP-ase Ejsing et al. (2005)Sertraline Calcein AM transport Weiss et al. (2003)
Trimipramine Rhodamine 123 uptake in human Caco-2 cells Ibrahim et al. (2000)Rhodamine123/daunorubicin cellular uptake Szabó et al. (1999)
160 K. Linnet, T.B. Ejsing

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 5/13
4. Distribution of drugs over the blood–brainbarrier in knock-out mice versus control mice
A simple method to estimate the influence of P-gp on thedistribution of drugs over the BBB is to compare brainconcentrations in P-gp knock-out (KO) and wild-type (WT)mice. At present three targeted KO mice strains areavailable: the mdr1a (abcb1a) (−/−) KO mice (Schinkelet al., 1994), the mdr1b (abcb1b) (−/−) KO mice (Schinkelet al., 1997) and the mdr1a/mdr1b (−/−) double KO mice(Schinkel et al., 1997). It is now well established that onlymdr1a P-gp is expressed at the BBB and not mdr1b P-gp(Barrand et al., 1995; Regina et al., 1998; Demeule et al.,2001). Thus the mdr1a and the mdr1a/1b (−/−) KO miceshould be equally good models for the absence of P-gp at theBBB. P-gp KO mice are phenotypically normal, but are moresensitive towards the toxicity of P-gp substrates (Schinkel,1997).
Numerous drugs have been screened in KO mice, and quitedramatic differences between KO and WT mice have beenobserved for some drugs. These include nelfinavir, digoxin,
ivermectin, the antiarrhythmic drugs amiodarone, quinidineand verapamil (Kusuhara et al., 1997; Dagenais et al., 2001;Doran et al., 2005) as well as methadone (Wang et al., 2004b)and the chemotherapeutic agent vinblastine (Van Asperenet al., 1996). All these drugs had brain concentrations in theKO-mice that were at least 10 times larger than thoseobserved in WT mice. Several psychotropic drugs have beenscreened in KO mice, and they generally showed smallerdifferences between KO and WT mice (Tables 2 and 3).Table 2 gives the brain–serum and in some instances thebrain–kidney ratios for a number of psychotropic drugs afteracute administration (for amitriptyline also after repeateddosing). The KO/WT ratios of brain–serum ratios show thatthe absence of P-gp has a rather moderate effect on most
drugs with ratios below 3. The only exceptions arerisperidone, 9-OH-risperidone, the hydroxylated amitripty-line metabolites and E-10-OH-nortriptyline. As the brainconcentrations have been normalized against the serum orkidney concentration, elevated serum concentrations fol-lowing decreased P-gp efflux in the intestines, liver andkidneys can be ignored. In a few cases, however, the brain–serum ratios were not available. Instead the brain(KO mice)–
brain(WT mice) concentration ratios are given along with theplasma–plasma ratios (Table 3). Again, the effect was quitemoderate.
When considering the displayed results of cerebral drugconcentrations in KO-mice, it should be noted that acute
drug administration experiments form the basis. In theclinical situation, chronic administration is of primaryrelevance. Grauer and Uhr (2004) studied the distributionof amitriptyline and its metabolites in KO- and control miceafter administration for 10 days. Somewhat surprisingly, onlythe metabolites and not amitriptyline itself had significantlyhigher cerebral concentrations in KO-mice than in controls(Table 2). Partial saturation of P-gp may play a role for thisunexpected result, but further studies on the conditionsduring chronic dosing would be desirable.
With regard to antiepileptic drugs (not included in Tables 2and 3), the absence of P-gp had a limited effect. Drugs suchas phenytoin, phenobarbital, lamotrigine, topiramate andcarbamazepine had ratios between 1 and 1.8 (Doran et al.,
2005; Sills et al., 2002). Finally, P-gp is of importance forseveral opioids. Methadone has more than 10 times higherbrain concentration in KO-mice than in controls (R-metha-done 15- and S-methadone 23-fold) (Wang et al., 2004b). Formorphine, the influence is smaller, amounting to a factor 1.7(Doran et al., 2005). The peripherally acting opioid,loperamide, on the other hand, has a ratio of 65 (Kalvasset al., 2004).
The in vitro studies above suggested that psychotropicdrugs were good P-gp substrates and inhibitors. The data inTables 2 and 3, however, show that although P-gp influencesthe brain penetration of many psychotropic drugs andmetabolites in KO mice, the effect is rather limited in mostcases. One factor that may affect the ratios is other transportproteins at the BBB. It has previously been shown that at theBBB of mdr1a KO mice the mRNA level of Breast CancerResistance Protein (BCRP), which is an ABC transporter thathas overlapping substrate specificities with P-gp (Litman etal., 2001), is threefold higher than that of the WT mice. Thesubstrate specificity of BCRP with regard to psychotropicdrugs has not been examined, and thus it is difficult estimate
the significance of the increased expression of BCRP.Additionally, when interpreting the mice results, the possi-bility of species variation should be kept in mind.
Although not in focus here, it should be briefly mentionedthat also endogenous compounds are transported by P-gp.The steroids corticosterone, cortisol and aldosterone havebeen shown to attain higher cerebral concentrations in KO-mice than in controls (Uhr et al., 2002). Further, a role for P-gp concerning transport of β-amyloid out of the CNS has beensuggested (Kandimalla et al., 2005, Thuerauf and Fromm,2006). Thus, the level of P-gp expression might hypotheti-cally play a role for development of Alzheimer’s disease.
5. Drug–
drug interaction experimentsin relation to P-gp in rats and mice
The large number of psychoactive drugs that are substrates of P-gp could potentially be involved in a significant number of drug–druginteractions regarding P-gp. Because of overlappingsubstrate specificities between CYP3A4 and P-glycoprotein,many drug interactions may involve both CYP3A4 and P-glycoprotein. Therefore, it is important to distinguish CYP3A4-mediated from P-glycoprotein-mediated inhibition in order tomake appropriate interpretation of drug interaction data. Thefollowing studies all use brain–serum or dialysate–serumratios, and thus there should be accounted for potential
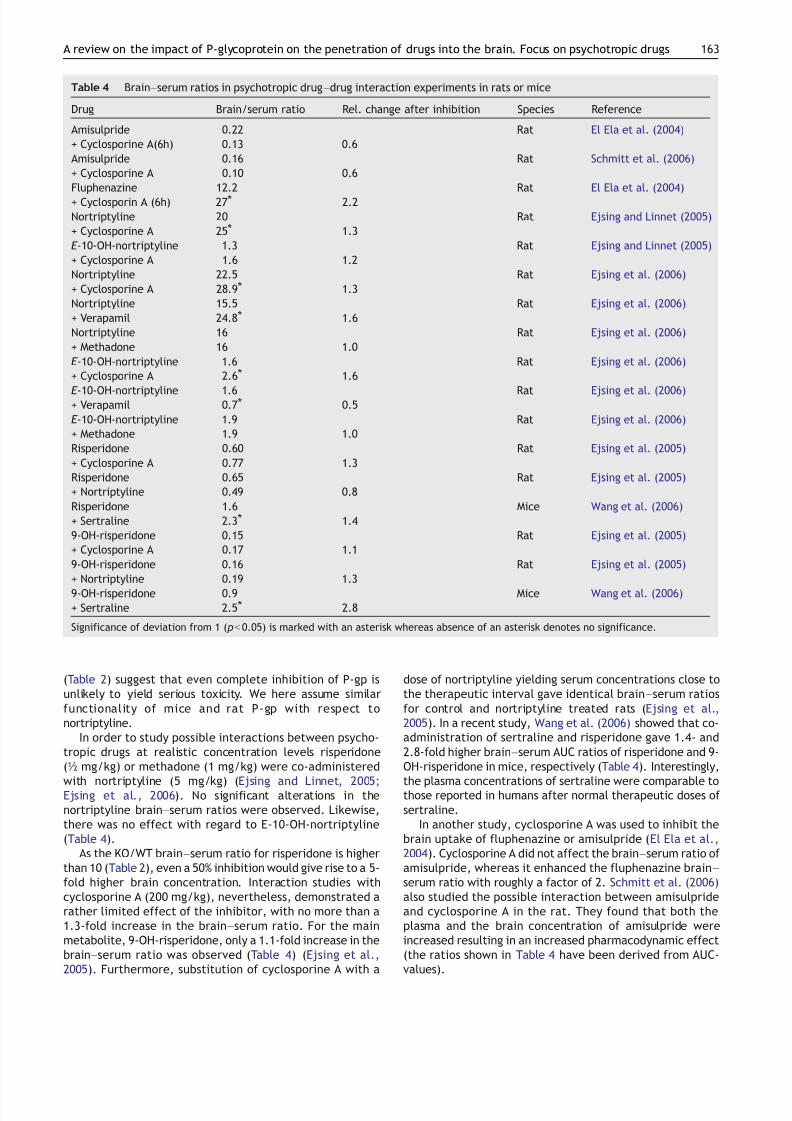
metabolic effects influencing the serum levels. Numerousinteraction studies with chemosensitizers and chemothera-peuticagents in rats and mice havebeenmade, and these showthat significant increases of drug brain levels can occur (Chooet al., 2000; Cisternino et al., 2004). One of the earlychemosensitizers, cyclosporine A (Ford and Hait, 1990), hasalso been used in studies including psychotropic drugs. Co-treatment of rats with nortriptyline in different doses andcyclosporine A (200 mg/kg, i.p.) increased the nortriptylinebrain–serum ratios with roughly 25% for nortriptyline and 30%for the major metabolite, E-10-OH-nortriptyline (Table 4)(Ejsing and Linnet, 2005). Taking into account that thetherapeutic interval in humans covers plasma concentrationsfrom 190 to 570 nM (Task Force on the Use of Laboratory Tests
161A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 6/13
in Psychiatry, 1985) (i.e. a variation corresponding to a factorof three),an increase of about1.25 for the brain–serumratiois
not dramatic. Substitution of cyclosporine A with verapamil
(50 mg/kg) led to a 60% increase in brain–serum ratios of nortriptyline (Table 4) (Ejsing et al., 2006). Likewise, the
abovementionedKO/WT nortriptyline ratios of 1.6, 1.8and 2.6
Table 3 Brain–brain (cbrain, KO mice/cbrain, WT mice) ratio of psychotropic drugs and metabolites screened in KO mice
Drug Ratiobrain Ratioplasma Mice type Reference
Citalopram 3.0⁎ 0.9 Mdr1a Uhr and Grauer (2003)Doxepin 1.2⁎ 1.1 Mdr1a/1b Uhr et al. (2003)Mirtazapine 1.3 1.3 Mdr1a/1b Uhr et al. (2003)Paroxetine 2.1⁎ 1.4 Mdr1a/1b Uhr et al. (2003)Trimipramine 1.2⁎ 0.9 Mdr1a Uhr and Grauer (2003)Desmethyl-trimipramine 1.5⁎ 1.2 Mdr1a Uhr and Grauer (2003)Venlafaxine 2.3⁎ 1.3⁎ Mdr1a/1b Uhr and Grauer (2003)
⁎: pb0.05. No asterisk denotes no significant difference.
Table 2 Brain–serum ratios of psychotropic drugs and metabolites in either knock-out (KO) or wild-type (WT) mice
Drug KO WT KO/WT Mouse type Reference
Amitriptyline - - ∼1.9 ⁎ Mdr1a Uhr et al. (2000)Amitriptyline (chronic dosing) 13.3 10.3 1.3 Mdr1a/1b Grauer and Uhr (2004)E-10-OH-amitriptyline - - ∼3.2⁎ Mdr1a Uhr et al. (2000)E-10-OH-amitriptyline 2.2 1.6 1.4 Mdr1a/1b Grauer and Uhr (2004)Z-10-OH-amitriptyline - - ∼4.5⁎ Mdr1a Uhr et al. (2000)Z-10-OH-amitriptyline 7.4 1.5 4.9⁎ Mdr1a/1b Grauer and Uhr (2004)Buspirone 2.0 1.6 1.3⁎ Mdr1a/1b Doran et al. (2005)Chlorpromazine 29 23 1.3⁎ Mdr1a/1b Doran et al. (2005)Citalopram 9.7 5.1 1.9⁎ Mdr1a/1b Doran et al. (2005)Clozapine 6.6 4.1 1.6⁎ Mdr1a/1b Doran et al. (2005)Diazepam 2.3 2.0 1.2⁎ Mdr1a/1b Doran et al. (2005)Fluoxetine - - ∼1.1 Mdr1a Uhr et al. (2000)Fluoxetine 18 12 1.5⁎ Mdr1a/1b Doran et al. (2005)Norfluoxetine - - ∼1.1 Mdr1a Uhr et al. (2000)Fluvoxamine 14 6.1 2.3⁎ Mdr1a/1b Doran et al. (2005)Haloperidol 18 13 1.4⁎ Mdr1a/1b Doran et al. (2005)Meprobamate 0.70 0.42 1.7⁎ Mdr1a/1b Doran et al. (2005)Midazolam 0.24 0.23 1.0 Mdr1a/1b Doran et al. (2005)
Nortriptyline 20 11 1.8⁎
Mdr1a/1b Doran et al. (2005)- - ∼2.5⁎ Mdr1a Uhr et al. (2000)
30 18 1.6⁎ Mdr1a Ejsing et al. (2006)E-10-OH-nortriptyline - - ∼2.9 ⁎ Mdr1a Uhr et al. (2000)
3.1 0.48 6.4⁎ Mdr1a Ejsing et al. (2006)Z-10-OH-nortriptyline - - ∼2.4⁎ Mdr1a Uhr et al. (2000)Demethyl-nortriptyline 13 8.5 1.5⁎ Mdr1a Ejsing et al. (2006)Olanzapine 2.0 0.9 2.6⁎ Mdr1a Wang et al. (2004c)Paroxetine 7.1 3.3 2.2⁎ Mdr1a/1b Doran et al. (2005)Risperidone 8.0 0.78 10⁎ Mdr1a/1b Doran et al. (2005)
∼5.8 ∼0.4 12⁎ Mdr1a/1b Wang et al. (2004d)5.6 0.4 14⁎ Mdr1a Ejsing et al. (2005)
9-OH-risperidone 1.0 0.060 17⁎ Mdr1a/1b Doran et al. (2005)∼2.9 ∼0.1 29⁎ Mdr1a/1b Wang et al. (2004d)
3.2 0.26 12⁎ Mdr1a Ejsing et al. (2005)Sertraline 27 24 1.1 Mdr1a/1b Doran et al. (2005)Sulpiride 0.15 0.078 1.9⁎ Mdr1a/1b Doran et al. (2005)Trazodone 0.54 0.61 0.9 Mdr1a/1b Doran et al. (2005)Venlafaxine 7.7 4.2 1.8⁎ Mdr1a/1b Doran et al. (2005)Zolpidem 0.40 0.29 1.4⁎ Mdr1a/1b Doran et al. (2005)
Significance of deviation from 1 ( pb0.05) is marked with an asterisk whereas absence of an asterisk denotes no significance. Results basedon brain–kidney ratios are shown in italics.-: no brain–serum values were available.∼: In the article the ratio was given graphically.
162 K. Linnet, T.B. Ejsing
7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 7/13
(Table 2) suggest that even complete inhibition of P-gp isunlikely to yield serious toxicity. We here assume similarfunctionality of mice and rat P-gp with respect tonortriptyline.
In order to study possible interactions between psycho-tropic drugs at realistic concentration levels risperidone(½ mg/kg) or methadone (1 mg/kg) were co-administered
with nortriptyline (5 mg/kg) (Ejsing and Linnet, 2005;Ejsing et al., 2006). No significant alterations in thenortriptyline brain–serum ratios were observed. Likewise,there was no effect with regard to E-10-OH-nortriptyline(Table 4).
As the KO/WT brain–serum ratio for risperidone is higherthan 10 (Table 2), even a 50% inhibition would give rise to a 5-fold higher brain concentration. Interaction studies withcyclosporine A (200 mg/kg), nevertheless, demonstrated arather limited effect of the inhibitor, with no more than a1.3-fold increase in the brain–serum ratio. For the mainmetabolite, 9-OH-risperidone, only a 1.1-fold increase in thebrain–serum ratio was observed (Table 4) (Ejsing et al.,2005). Furthermore, substitution of cyclosporine A with a
dose of nortriptyline yielding serum concentrations close tothe therapeutic interval gave identical brain–serum ratiosfor control and nortriptyline treated rats (Ejsing et al.,2005). In a recent study, Wang et al. (2006) showed that co-administration of sertraline and risperidone gave 1.4- and2.8-fold higher brain–serum AUC ratios of risperidone and 9-OH-risperidone in mice, respectively (Table 4). Interestingly,
the plasma concentrations of sertraline were comparable tothose reported in humans after normal therapeutic doses of sertraline.
In another study, cyclosporine A was used to inhibit thebrain uptake of fluphenazine or amisulpride (El Ela et al.,2004). Cyclosporine A did not affect the brain–serum ratio of amisulpride, whereas it enhanced the fluphenazine brain–serum ratio with roughly a factor of 2. Schmitt et al. (2006)also studied the possible interaction between amisulprideand cyclosporine A in the rat. They found that both theplasma and the brain concentration of amisulpride wereincreased resulting in an increased pharmacodynamic effect(the ratios shown in Table 4 have been derived from AUC-values).
Table 4 Brain–serum ratios in psychotropic drug–drug interaction experiments in rats or mice
Drug Brain/serum ratio Rel. change after inhibition Species Reference
Amisulpride 0.22 Rat El Ela et al. (2004)+ Cyclosporine A(6h) 0.13 0.6Amisulpride 0.16 Rat Schmitt et al. (2006)+ Cyclosporine A 0.10 0.6Fluphenazine 12.2 Rat El Ela et al. (2004)+ Cyclosporin A (6h) 27⁎ 2.2Nortriptyline 20 Rat Ejsing and Linnet (2005)+ Cyclosporine A 25⁎ 1.3E-10-OH-nortriptyline 1.3 Rat Ejsing and Linnet (2005)+ Cyclosporine A 1.6 1.2Nortriptyline 22.5 Rat Ejsing et al. (2006)+ Cyclosporine A 28.9⁎ 1.3Nortriptyline 15.5 Rat Ejsing et al. (2006)+ Verapamil 24.8⁎ 1.6Nortriptyline 16 Rat Ejsing et al. (2006)+ Methadone 16 1.0E-10-OH-nortriptyline 1.6 Rat Ejsing et al. (2006)+ Cyclosporine A 2.6⁎ 1.6
E-10-OH-nortriptyline 1.6 Rat Ejsing et al. (2006)+ Verapamil 0.7⁎ 0.5E-10-OH-nortriptyline 1.9 Rat Ejsing et al. (2006)+ Methadone 1.9 1.0Risperidone 0.60 Rat Ejsing et al. (2005)+ Cyclosporine A 0.77 1.3Risperidone 0.65 Rat Ejsing et al. (2005)+ Nortriptyline 0.49 0.8Risperidone 1.6 Mice Wang et al. (2006)+ Sertraline 2.3⁎ 1.49-OH-risperidone 0.15 Rat Ejsing et al. (2005)+ Cyclosporine A 0.17 1.19-OH-risperidone 0.16 Rat Ejsing et al. (2005)+ Nortriptyline 0.19 1.3
9-OH-risperidone 0.9 Mice Wang et al. (2006)+ Sertraline 2.5⁎ 2.8
Significance of deviation from 1 ( pb0.05) is marked with an asterisk whereas absence of an asterisk denotes no significance.
163A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 8/13
A number of antiepileptic drugs have been studied bymicrodialysis experiments in rats by Potschka and co-work-ers. They found that local administration of verapamil led toa 1.25-fold increase in the dialysate–plasma ratio of carbamazepine (Potschka et al., 2001) and a 1.8-foldincrease for phenytoin (Potschka and Löscher, 2001).Subsequent studies showed that verapamil gave between1.5- and 2-fold increases in the dialysate–plasma ratios of lamotrigine, felbamate and phenobarbital (Potschka et al.,2002), whereas no effect was observed for levitiracetam(Potschka et al., 2004). Under normal conditions P-gp is notexpressed in neurons (Volk et al., 2004), but recently somestudies have shown that neurons in the rat hippocampusbegin to express P-gp after a chemically induced statusepilepticus (Lazarowski et al., 2004b; Volk et al., 2004).Neuronal P-gp expression in epileptic patients has also beenreported (Lazarowski et al., 2004a; Volk et al., 2004). Takingthe above-mentioned results into account, P-gp could beinvolved in drug-refractory epilepsy (Sisodiya et al., 2002).Interestingly, a recent study has shown that local adminis-tration (microdialysis) of verapamil and i.p. administration
of oxcarbazepine can decrease the number of pilocarpineinduced limbic seizures in rats (Clinckers et al., 2005).Inhibition of P-gp has also been tested with regard to
analgesic drugs. Methadone is a good P-gp substrate in mice, asmentioned above. In a study, where rats were pretreated withthe powerful P-gp inhibitor valspodar 30 min prior tomethadone administration, a threefold increase in the anti-nociceptive effect was observed. After 20 min the methadonebrain–plasma ratios were five times higher in the valspodartreated group than in the control group (Rodriguez et al.,2004). Likewise, theP-gpinhibitor elacridar (GF120918) gaveathreefold increasein the brain–serum ratios of morphine, and,as it also was the case formethadone, a twofold increase in theantinociceptive effect was observed (Letrent et al., 1999). In
contrast, valspodar had no effect on the brain penetration of the opioid oxycodone (Boström et al., 2005).
6. Relevance in humans of P-gp in relation toCNS effects of drugs
6.1. Interactions
The experimental findings of the interaction studies de-scribed above clearly support the notion that P-gp plays animportant role in brain uptake of drugs. The results also pointto the potential risk of neurotoxicity when potent P-gp
inhibitors are co-administered. A good example is the studyby Sadeque et al. (2000). They treated healthy volunteerswith the antidiarrhoeal agent loperamide (16 mg, oral) withor without co-administration of quinidine (600 mg, oral).When loperamide was administered alone, no adverse effectswere observed. Contrary to this, serious respiratory depres-sion occurred when the drug was given with quinidine, whichwas ascribed to inhibition of P-gp. In another study, however,also performed on healthy volunteers, quinidine (800 mg/kg,oral) did not enhance the central nervous effects of morphine(7.5 mg, infusion) (Skarke et al., 2003). Kharasch et al. (2004)found that quinidine enhanced the effects of orally admin-istered methadone but not of methadone given by theintravenous route. Since the plasma concentration of
methadone given orally was increased by quinidine, it wasconcluded that quinidine enhanced the absorption of methadone by inhibition of intestinal P-gp, but that quinidinein the administered dose did not inhibit P-gp at the BBB. Anadditional contributing factor might be inhibition of CYP2D6by quinidine, since CYP2D6 is involved in the metabolism of methadone (Eap et al., 2001).
Recently, an interaction between colchicine and verapa-mil with regard to P-gp at the BBB was proposed, based on acase report (Tröger et al., 2005). In this case the drugcombination resulted in enhanced neurotoxicity of colchi-cine in the form of tetraparesis.
As previously mentioned, P-gp and CYP3A4 have a strikingsubstrate overlap (Fromm, 2004). Since the brain concentra-tions are not readily available in humans, CNS effects willoften be ascribed solely to metabolic interactions involvingthe CYP enzymes, even though CNS adverse effects couldarise from the combination of drug–drug interactions inrelation to CYP enzymes and with regard to P-gp at the BBB.An example is the interaction between risperidone and theHIV protease inhibitor ritonavir. Following concomitant
administration of the drugs, extrapyramidal symptoms(Kelly et al., 2002) and reversible coma (Jover et al., 2002)have been reported. These effects were ascribed tometabolic interactions, but as ritonavir is a good P-gpinhibitor in vitro (Drewe et al., 1999; Van der Sandt et al.,2001) and can inhibit P-gp at the renal tubules in humans(Ding et al., 2004), inhibition of P-gp at the BBB might also beinvolved. Although the reported cases point to drug–druginteractions with regard to P-gp at the BBB, it should be keptin mind that few reports exist for these relatively widelyused drugs. Thus, further systematic research is needed todelineate the interaction potential in a clinical context.
As mentioned previously, interaction between P-gp andnutritional components takes place. Ingestion of a single dose
of St. John’s wort increased the maximum plasma concentra-tion of the P-gp model compound fexofenadine by 45%,whereas long-term treatment caused a 35% decrease due toinduction (Wang et al., 2002). Specific interactions between P-gpandSt.John’s wortcomponentswith regard to psychotropicdrugs at the BBB have apparently not been assessed. However,the well-known inducing effect of St. John’s wort with regardto CYP3A4will influence the effect of manypsychotropic drugsvia a decrease of the plasma concentration.
6.2. Pharmacogenomics
Recently, attention has been directed towards the pharmaco-
genomicsof P-gp. As manycentral nervous system-active drugsare P-gp substrates, differences in P-gp expression at the BBBcould, at least in part, be of importance for inter-individualvariation in response and the occurrence of side effects atidentical plasma concentrations. More than 50 single nucleo-tide polymorphisms (SNPs) have been detected in the humanMDR1 gene (Marzolini et al., 2004, Kimchi-Sarfaty et al.,2007). SNPs in exon 21 and 26 have been associated withdifferences in P-gp expression and function in humans(Sakaeda et al., 2003). The majority of SNP related reportsfocus on the silent C3435T SNP of exon 26. This SNP has beenassociated with both increased and decreased expression of P-gp in the intestines and with changes in serum levels of digoxinand fexofenadine (Hoffmeyer et al., 2000; Kurata et al., 2002;
164 K. Linnet, T.B. Ejsing

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 9/13
Nakamura et al., 2002). With regard to the effect of theC3435T SNP on P-gp at the BBB few studies are available.Roberts et al. (2002) genotyped a number of depressedpatients for the C3435T SNP and randomized them to eithernortriptyline or fluoxetine treatment. Fifty-four of thenortriptyline treated patients completed the 6-week trial,and among these patients no difference in nortriptyline serumlevels between C/C, C/T, and TT genotypes were found. Theydid, however, observe that there was an increased frequencyof postural hypotension for the patients homozygous for T. Noassociation between any of the genotypes and posturalhypotension was apparent for the 72 fluoxetine treatedpatients that completed the trial. In a similar study Laikaet al. (2006) found no correlation between the G2677T/A SNPsand the therapeutic outcome and occurrence of side effects indepressed inpatients treated with amitriptyline.DeLucaetal.(2003) investigated the involvement of the C3435T SNP inantidepressant-induced mania in depressed patients. Thestudy included 55 patients treated with fluoxetine, fluvox-amine, sertraline, imipramine, moclobemide, venlafaxine,paroxetine, nefazodone or combination therapy with fluox-
etine/fluvoxamine. They found no association, but the largenumber of different drugs included in the study is a problem.Thus, further studies are needed to clarify the possibleinfluence of the C3435T SNP at the BBB on the effects of psychotropic drugs.
Apart from antidepressants and antipsychotics a numberof studies have focused on the possible association betweenthe C3435T SNP and drug-resistant epilepsy. Siddiqui et al.(2003) genotyped 200 patients with drug-resistant epilepsy aswell as 115 patients with drug-sensitive epilepsy. Theyreported that patients with drug-resistant epilepsy weremore likely to have the CC genotype than the TT genotype.Using identical inclusion criteria, Tan et al.(2004) studied 401cases of drug-resistant epilepsy and 208 drug responsive
epileptics. In contrast to Siddique andco-workers, they foundno association between the C3435T SNP and lack of responseto antiepileptic treatment. Likewise, Sills et al. (2005) andKim et al. (2006) did not find any correlation between C3435Tand multidrug resistance in patients with epilepsy. Finally,Zimprich et al. (2004) studied patients that were homozygousfor either of two haplotypes. One haplotype (called TTT)included a thymine at positions 1236, 2677, and 3435,whereas the other haplotype (CGC) had cytosine at positions1236 and 3435 and guanine at position 2677. They reported acorrelation between the CGC haplotype and treatmentfailure. A discussion of possible confounders and problemswith data analysis in these studies has been presented by Ott
(2004).Hestatesthatduetothelowsamplesizeandlowpriorprobability of true association, the simplest and mostplausible explanation is that the significant results are falsepositive findings.
Finally, no correlation between C3435Tand central nervoussystem effects of loperamide treatment in healthy volunteerswas found (Pauli-Magnus et al., 2003). In another study,Brunner et al. (2005) measured the brain uptake of 11C-verapamil by PET (positron emission tomography) in 20volunteers. Ten of these had the abovementioned TTThaplotype whereas the remainders had the CGC haplotype. Inthis study no difference between the two groups wasobserved.
The importance of SNPs has also been investigated inrelationtoP-gp’sroleintheplacenta. Hitzletal.(2004) found
that the polymorphisms C3435Tand G2677Twere associatedwith lower P-gp expression in the placenta. Rahi et al. (inpress) studied placental transport of the antipsychoticquetiapine, and observed that C3435Twas associated with ahigh placental transfer value. However, there was nocorrelation between P-gp expression levels and quetiapinetransfer suggesting that further studies are needed on thisissue.
Generally, the majority of studies concerning the effect of P-gp polymorphisms on adverse effects or brain penetrationof drugs do not show any significant effects. A loss of functionmutation could, however, have quite drastic effects, asseveral examples from Collie dogs devoid in functional P-gphave shown. When these Collie dogs are treated withstandard doses of loperamide they are subject to severeneurotoxic effects, including mydriasis, ataxia, prostrationand disorientation (Hugnet et al., 1996; Sartor et al., 2004).Likewise, the antiparasitic drug ivermectin gives rise toneurotoxicity when dogs are treated for e.g. mite infections(Mealey et al., 2004). No loss-of-function mutations havebeen described for MDR1 in humans (Eichelbaum et al.,
2004). However, recently, Kimchi-Sarfaty et al. (2007) havesuggested that silent SNPs in P-gp may be associated withchanged folding patterns of the protein resulting in changedfunctionality. Further studies are needed on the significanceof this finding (Komar, 2007). Currently, it seems that geneticpolymorphisms in the MDR1 gene are not of importance inthe context of mono- or polypharmacy with psychoactivedrugs.
7. Conclusion
The various in vitro studies give an indication of whichpsychoactive drugs are substrates of P-gp. An impression of
the functional significance can be gained by KO mice studies,although some reservation should be taken with regard topossible species variation. For antidepressants that are P-gpsubstrates the brain concentrations in KO mice are up toabout 2.5 times higher than in control mice. With regard toantipsychotics P-gp exerts a moderate influence in mostcases, except for risperidone and its active metabolite,which both have a more than 10-fold higher brain concen-tration in KO mice than in control mice. However, in humans,no loss-of-function mutation in P-gp has hitherto beendiscovered. Animal experiments show that drug–drug inter-actions of psychotropic drugs in relation to P-gp may occur,but when considering the relatively low impact of P-gpabsence in KO mice in relation to most psychotropic drugs,the possible clinical effects are probably limited in mostcases. Yet, for a drug like risperidone important effectscannot be excluded.
Role of the funding source
There was no specific funding for this work.
Contributors
Kristian Linnet planned the structure of the review. Thomas B.Ejsing made the first draft of the ms. including one table. Kristian
165A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 10/13
Linnet produced the rest of the tables and re-wrote the ms. Bothauthors contributed to the literaturesearch.Both authors approvedthe final ms.
Conflicts of interest
Kristian Linnet has not had any financial, personal or otherrelationships that have influenced the work. Thomas B. Ejsing has
not had any financial, personal or other relationships that haveinfluenced the work.
Acknowledgements
We thank the reviewers for helpful suggestions that have improvedthe present work.
References
Barrand, M.A., Robertson, K.J., von Weikersthal, S.F., 1995.Comparisons of P-glycoprotein expression in isolated rat brainmicrovessels and in primary cultures of endothelial cells derivedfrom microvasculature of rat brain, epididymal fat pad and from
aorta. FEBS Lett. 374, 179–
183.Bauer, B., Hartz, A.M.S., Fricker, G., Miller, D.S., 2005. Modulation of P-glycoprotein transport function at the blood–brain barrier.Exp. Biol. Med. 230, 118–127.
Beaulieu, E., Demeule, M., Ghitescu, L., Béliveau, R., 1997.P-glycoprotein is strongly expressed in the luminal membranesof the endothelium of blood vessels in the brain. Biochem. J.326, 539–544.
Begley, D.J., 2004. ABC transporters and the blood–brain barrier(review). Curr. Pharm. Des. 10, 1295–1312.
Bertilsson, Otani, K., Dahl, M.L., Nordin, C., Åberg-Wistedt, A.,1991. Stereoselective efflux of (E)-10-hydroxynortriptylineenantiomers from the cerebrospinal fluid of depressed patients.Pharmacol. Toxicol. 68, 100–103.
Bosch, I., Croop, J.M., 1998. P-glycoprotein structure and evolu-
tionary homologies (review). Cytotechnology 27, 1–
30.Boström, E., Simonsson, U.S.H., Hammarlund-Udenaes, M., 2005.Oxycodone pharmacokinetics and pharmacodynamics in the ratin the presence of the P-glycoprotein inhibitor PSC833. J. Pharm.Sci. 94, 1060–1066.
Boulton, D.W., DeVane, C.L., Liston, H.L., Markowitz, J.S., 2002. Invitro P-glycoprotein affinity for atypical and conventionalantipsychotics. Life Sci. 71, 163–169.
Brunner, M., Langer, O., Sunder-Plassmann, R., Dobrozensky, G.,Müller, U., Wadsak, W., Krcal, A., Karch, R., Mannhalter, C.,Dudczak, R., Kletter, K., Steiner, I., Baumgartner, C., Müller, M.,2005. Influence of functional haplotypes in the drug transportergene ABCB1 on central nervous system drug distribution inhumans. Clin. Pharmacol. Ther. 78, 182–190.
Chen, Y., Pant, A.C., Simon, S.M., 2001. P-glycoprotein does not
reduce substrate concentration from the extracellular leaflet of the plasma membrane in living cells. Cancer Res. 61, 7763–7769.Choo, E.F., Leake, B., Wandel, C., Imamura, H., Wood, A.J.J.,
Wilkinson, G.R., Kim, R.B., 2000. Pharmacological inhibition of P-glycoprotein transport enhances the distribution of HIV-1protease inhibitors into brain and testes. Drug Metab. Dispos.28, 655–660.
Cisternino, S., Rousselle, C., Debray, M., Scherrmann, J.M., 2004. In
situ transport of vinblastine and selected P-glycoprotein sub-strates: implications for drug–drug interactions at the mouseblood–brain barrier. Pharm. Res. 21, 1382–1389.
Clinckers, R., Smolders, I., Meurs, A., Ebinger, G., Michotte, Y.,2005. Quantitative in vivo microdialysis study on the influence of multidrug transporters on the blood–brain barrier passage of oxcarbazepine: concomitant use of hippocampal monoamines as
pharmacodynamic markers for the anticonvulsant activity.J. Pharmacol. Exp. Ther. 31, 725–731.
Cordon-Cardo, C., O’Brien, J.P., Boccia, J., Casals, D., Bertino, J.R.,Melamed, M.R., 1990. Expression of the multidrug resistancegene product (P-glycoprotein) in human normal and tumortissues. J. Histochem. Cytochem. 38, 1277–1287.
Cutler, L., Hoves, C., Deeks, N.J., Buck, T.L., Jeffrey, P., 2006.Development of a P-glycoprotein knockout model in rodents todefine species differences in its functional effect at the blood–brain barrier. J. Pharm. Sci. 95, 1944–1953.
Dagenais, C., Zong, J., Ducharme, J., Pollack, G.M., 2001. Effect of mdr1a P-glycoprotein gene disruption, gender, and substrateconcentration on brain uptake of selected compounds. Pharm.Res. 19, 957–963.
De Luca, V., Mundo, E.,Trakalo,J., Wong, G.W.H.,Kennedy, J.L., 2003.Investigation of polymorphism in the MDR1 gene and antidepres-sant-induced mania. Pharmacogenomics J. 3, 297–299.
Demeule, M., Labelle, M., Régina, A., Berthelet, F., Béliveau, R.,2001. Isolation of endothelial cells from brain, lung, and kidney:expression of the multidrug resistance O-glycoprotein isoforms.Biochem. Biophys. Res. Commun. 281, 827–834.
Ding, R., Tayrouz, Y., Riedel, K.D., Burhenne, J., Weiss, J., Mikos,G., Haefeli, W., 2004. Substantial pharmacokinetic interaction
between digoxin and ritonavir in healthy volunteers. Clin.Pharmacol. Ther. 76, 73–84.Doran, A., Obach, R.S., Smith, B.J., Hosea, N.A., Becker, S., et al.,
2005. The impact of P-glycoprotein on the disposition of drugstargeted for indications of the central nervous system: evalua-tion using the mdr1a/1b knockout mouse model. Drug Metab.Dispos. 33, 165–174.
Drewe, J., Gutmann, H., Fricker, G., Török, M., Beglinger, C.,Huwyler, J., 1999. HIV protease inhibitor ritonavir: a more potentinhibitor of P-glycoprotein than the cyclosporine Analog SDZ PSC833. Biochem. Pharmacol. 57, 1147–1152.
Eap,C.B.,Broly, F., Mino, A.,Hammig, R.,Deglon, J.J., Uehlinger, C.,Meili, D., Chevalley, A.F., Bertschy, G., Zullino, D., Kosel, M.,Preisig, M., Baumann, P., 2001. Cytochrome P450 2D6 genotypeand methadone steady-state concentrations. J. Clin. Psycho-
pharmacol. 21, 229–
234.Eichelbaum, M., Fromm, M.F., Schwab, M., 2004. Clinical aspects of the MDR1 (ABCB1) gene polymorphism (review). Ther. DrugMonit. 26, 180–185.
Ejsing, T.B., Linnet, K., 2005. Influence of P-glycoprotein inhibition onthe distribution of the tricyclic antidepressant nortriptyline overthe blood–brain barrier. Hum. Psychopharmacol. 20, 149–153.
Ejsing, T.B., Pedersen, A.D., Linnet, K., 2005. P-glycoproteininteraction with risperidone and 9-OH-risperidone studied invitro, in knock-out mice and in drug–drug interaction experi-ments. Hum. Psychopharmacol. 20, 493–500.
Ejsing, T.B., Hasselstrøm, J., Linnet, K., 2006. The influence of P-glycoprotein on cerebral and hepatic concentrations of nortrip-tyline. Drug Metab. Drug Interac. 21, 139–162.
El Ela, A.A., Härtter, S., Schmitt, U., Hiemke, C., Spahn-Langguth,
H., Langguth, P., 2004. Identification of P-glycoprotein substratesand inhibitors among psychoactive compounds — implications forpharmacokinetics of selected substrates. J. Pharm. Pharmacol.56, 967–975.
Ford,J.M.,Hait, W.N.,1990. Pharmacologyof drugsthat alter multidrugresistance in cancer (review). Pharmacol. Rev. 42, S155–S199.
Fromm, M.F., 2004. Importance of P-glycoprotein at blood–tissuebarriers. Trends Pharmacol. Sci. 25, 423–429.
Germann, U., Willingham, M.C., Pastan, I., Gottesman, M.M., 1990.Expression of the human multidrug transporter in insect cells by arecombinant baculovirus. Biochemistry 29, 2295–2303.
Grauer, M.T., Uhr, M., 2004. P-glycoprotein reduces the ability of amitriptyline metabolites to cross the blood–brain barrier in miceafter a 10-day administrationof amitriptyline. J. Psychopharmacol.18, 66–74.
166 K. Linnet, T.B. Ejsing
7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 11/13
Hitzl, M., Schaeffeler, E., Hocher, B., Slowinski, T., Halle, H.,Eichelbaum, M., Kaufmann, P., Fritz, P., Fromm, M.F., Schwab, M.,2004. Variable expression of P-glycoprotein in the human placentaand ist association with mutations of the multidrug resistance 1gene (MDR1. Pharmacogenetics 14, 309–318.
Hoffmeyer, S., Burk, O., von Rischter, O., Arnold, H.P., Brockmöller,J., Johne, A., Cascorbi, I., Gerloff, T., Roots, I., Eichelbaum, M.,Brinkmann, U., 2000. Functional polymophisms of the humanmultidrug-resistance gene: multiple sequence variations andcorrelation of one allele with P-glycoprotein expression andactivity in vivo. Proc. Natl. Acad. Sci. U. S. A. 97, 3473–3478.
Hugnet, C., Cadore, J.L., Buronfosse, F., Pineau, X., Mathet, T.,Berny, P.J., 1996. Loperamide poisoning in the dog. Vet. Hum.Toxicol. 38, 31–33.
Härtter, S., Hüwel, S., Lohmann, T., El Ala, A.A., Langguth, P.,Hiemke, C., Galla, H.J., 2003. How does the benzamideantipsychotic amisulpride get into the brain? — an in vitro
approach comparing amisulpride with clozapine. Neuropsycho-pharmacology 28, 1916–1922.
Ibrahim, S., Peggins, J., Knapton, A., Licht, T., Aszalos, A., 2000.Influence of antipsychotic, antiemetic, and Ca2+ channel blockerdrugs on the cellular accumulation of the anticancer drugdaunorubicin: P-glycoprotein modulation. J. Pharmacol. Exp.
Ther. 295, 1276–
1283.Jover, F., Cuadrado, J.M., Andreu, L., Merino, J., 2002. Reversiblecoma caused by risperidone–ritonavir interaction. Clin. Neuro-pharmacol. 25, 251–253.
Juliano, R.L., Ling, V., 1976. A surface glycoprotein modulating drugpermeability in Chinese hamster ovary cell mutants. Biochim.Biophys. Acta 455, 152–162.
Kalvass, J.C., Graff, C.L., Pollack, G.M., 2004. Use of loperamide asa phenotypic probe of mdr1a status in CF-1 mice. Pharm. Res. 21,1867–1870.
Kandimalla, K.K.,Curran, G.L., Holasek, S.S., Gilles, E.J., Wengenack,T.M., Poduslo, J.F., 2005. Pharmacokinetic analysis of the blood–brainbarrier transport of 125I-amyloid beta protein 40 in wild-typeand Alzheimer’s disease transgenic mice (APP,PS1) and its implica-tions for amyloid plaque formation. J. Pharmacol. Exp. Ther. 313,
1370–
1378.Kelly, D.V., Béïque, L.C.,Bowmer, M.I.,2002. Extrapyramidal symptomswith ritonavir/indinavir plus risperidone. Ann. Pharmacother. 36,827–830.
Kharasch, E.D., Hoffer, C., Whittington, D., 2004. The effect of quinidine, used as a probe for the involvement of P-glycoprotein,on the intestinal absorption and pharmacodynamics of metha-done. Br. J. Clin. Pharmacol. 57, 600–610.
Kimchi-Sarfaty, C., Oh, J.M., Kim, I.-W., Sauna, Z.E., Calcagno, A.M.,Ambudkar, S.V., Gottesman, M.M., 2007. A “silent” polymorphismin the MDR1 gene changes substrate specificity. Science 315,525–528.
Kim, R.B., 2002. Drugs as P-glycoprotein substrates, inhibitors, andinducers (review). Drug Metab. Rev. 34, 47–54.
Kim, D.W., Kim, M., Lee, S.K., Kang, R., Lee, S.Y., 2006. Lack of
association between C3435Tnucleotide MDR1 genetic polymorphismand multidrug-resistant epilepsy. Seizure 5, 344–347.Komar, A.A., 2007. SNPs, silent but not invisible. Science 315,
466–467.Kurata, Y., Ieri, I., Kimura, M., Morita, T., Irie, S., Urae, A., Ohdo, S.,
Ohtani, H., Sawada, Y., Higuchi, S., Otsubo, K., 2002. Role of human MDR1 gene polymorphism in bioavailability and interac-tion of digoxin, a substrate of P-glycoprotein. Clin. Pharmacol.Ther. 72, 209–219.
Kusuhara, H., Suzuki, H., Terasaki, T., Kakee, A., Lemaire, M.,Sugiyama, Y., 1997.P-glycoprotein mediatesthe efflux of quinidineacross the blood–brain barrier. J. Pharmacol. Exp. Ther. 283,574–580.
Laika, B., Leucht, S., Steimer, W., 2006. ABCB1 (P-glycoprotein/MDR1) gene G2677T/A sequence variation (polymorphism): lack
of association with side effects and therapeutic response indepressed inpatients treated with amitriptyline. Clin. Chem. 52,893–895.
Lazarowski, A., Massaro, M., Schteinschnaider, A., Intruvini, S.,Sevlever, G., Rabinowicz, A., 2004a. Neuronal MDR1 geneexpression and persistent low levels of anticonvulsants in achild with refractory epilepsy. Ther. Drug Monit. 26, 44–46.
Lazarowski, A., Ramos, A.J., Garcia-Rivello, H., Brusco, A., Girardi,E., 2004b. Neuronal and glial expression of the multidrugresistance gene product in an experimental epilepsy model.Cell. Mol. Neurobiol. 24, 77–85.
Letrent, S.P., Pollack, G.M., Brouwer, K.R., Brouwer, K.L.R.,1999. Effects of a potent and specific P-glycoprotein inhibitoron the blood–brain barrier distribution and antinociceptiveeffect of morphine in the rat. Drug Metab. Dispos. 27,827–834.
Lin, J.H., Yamazaki, M., 2003. Role of P-glycoprotein in pharmaco-kinetics — clinical implications. Clin. Pharmacokinet. 42, 59–98.
Litman, T., Druley, T.E., Stein, W.D., Bates, S.E., 2001. From MDR toMXR: new understanding of multidrug resistance systems, theirproperties and clinical significance (Review). Cell. Mol. Life Sci.58, 931–959.
Loo, T.W., Clarke, D.M., 2005. Do drug substrates enter the common
drug-binding pocket of P-glycoprotein through “
gates”
. Biochem.Biophys. Res. Commun. 329, 419–422.Lugo, M.R., Sharom, F.J., 2005. Interaction of LDS-751 with P-
glycoprotein and mapping of the location of the R drug bindingsite. Biochemistry 44, 643–655.
Marzolini, C., Paus, E., Buclin, T., Kim, R.B., 2004. Polymorphisms inhuman MDR1 (P-glycoprotein): recent advances and clinicalrelevance (review). Clin. Pharmacol. Ther. 75, 13–33.
Mayer, U., Wagenaar, E., Beijnen, J.H., Smit, J.W., Meijer, D.K.F.,van Asperen, J., Borst, P., Schinkel, A.H., 1996. Substantialexcretion of digoxin via the intestinal mucosa and prevention of long-term digoxin accumulation in the brain by the mdr1a P-glycoprotein. Br. J. Pharmacol. 119, 1038–1044.
Mealey, K.L., Northrup, N.C., Bentjen, S.A., 2003. Increased toxicityof P-glycoprotein-substrate chemotherapeutic agents in a dog
with the MDR1 deletion mutation associated with ivermectinsensitivity. J. Am. Vet. Med. Assoc. 223, 1453–1455.Mealey, K.L., Bentjen, S.A., Gay, J.M., Cantor, G.H., 2004.
Ivermectin sensitivity in collies is associated with a deletionmutation of the mdr1 gene. Pharmacogenetics 11, 727–733.
Miura, M., Uno, T., Tateishi, T., Suzuki, T., 2007. Pharmacokinetics of fexofenadine enantiomers in healthy subjects. Chirality 19,223–227.
Murakami, H., Takanaga, H., Matsuo, H., Ohtani, H., Sawada, Y.,2000. Comparison of blood–brain barrier permeability in miceand rats using in situ brain perfusion technique. Am. J. Physiol,Heart Circ. Physiol. 279, H1022–H1028.
Nakamura, T., Sakaeda, T., Horinouchi, M., Tamura, T., Aoyama, N.,Shirakawa, T., Matsuo, M., Kasuga, M., Okumura, K., 2002. Effectof the mutation (C3435T) at exon 26 of the MDR1 gene on
expression level of MDR1 messenger ribonucleic acid in duodenalenterocytes of healthy Japanese subjects. Clin. Pharmacol. Ther.71, 297–303.
Ott, J., 2004. Association of genetic loci. Neurology 63, 955–958.Pauli-Magnus, C., Feiner, J., Brett, C., Lin, E., Kroetz, D.L., 2003. No
effect of MDR1 C3435T variant loperamide disposition andcentral nervous system effects. Clin. Pharmacol. Ther. 74,487–498.
Polli, J.W., Wring, S.A., Humphreys, J.E., Huang, L., Morgan, J.B.,Webster, L.O., Serabjit-Singh, C.S., 2001. Rational use of in vitroP-glycoprotein assays in drug discovery. J. Pharmacol. Exp. Ther.299, 620–628.
Potschka, H., Löscher, W., 2001. In vivo evidence for P-glycoprotein-mediated transport of phenytoin at the blood–brain barrier of rats. Epilepsia 42, 1231–1240.
167A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 12/13
Potschka, H., Fedrowitz, M., Löscher, W., 2001. P-glycoproteinand multidrug resistance-associated protein are involved inthe regulation of extracellular levels of the major antiepi-leptic drug carbamazepine in the brain. NeuroReport 12,3557–3560.
Potschka, H., Fedrowitz, M., Löscher, W., 2002. P-glycoprotein-mediated efflux of phenobarbital, lamotrigine, and felbamate atthe blood–brain barrier: evidence from microdialysis experi-ments in rats. Neurosci. Lett. 327, 173–176.
Potschka, H., Baltes, S., Löscher, W., 2004. Inhibition of multidrugtransporters by verapamil or probenicid does not alter blood–
brain barrier penetration of levetiracetam in rats. Epilepsy Res.58, 85–91.
Rahi, M., Heikkinen, T., Hartter, S., Hakkola, J., Hakala, K., Waller-man, O., Wadelius, M., Wadelius, C., Laine, K., in press. Placentaltransfer of quetiapine in relation to P-glycoprotein activity.J. Psychopharmacol. (Electronic publication ahead of print).
Rao, V.V., Dahlheimer, J.L., Bardgett, M.E., Snyder, A.Z., Finch, R.A.,Sartorelli, A.C., Piwnica-Worms, D., 1999. Choroid plexus epithe-lial expression of MDR1 P-glycoprotein and multidrug resistance-associated protein contribute to the blood-cerebrospinal-fluiddrug-permeability barrier. Proc. Natl. Acad. Sci. U. S. A. 96,3900–3905.
Regina, A., Koman, A., Piciotti, M., El Hafny, B., Center, M.S.,Bergmann, R., Couraud, P.O., Roux, F., 1998. Mrp1 multidrugresistance-associated protein and P-glycoprotein expression inrat brain microvessels endothelial cells. J. Neurochem. 71,705–715.
Riou, M., Guégnard, F., le Vern, Y., Kerboeuf, D., 2003. Modulation of the multidrug resistance (MDR) system in the nematode Haemo-
chus contortus by changing cholesterol content: effects onresistance to anthelmintics. J. Antimicrob. Chemother. 52,180–187.
Roberts, R.L., Joyce, P.R., Mulder, R.T., Begg, E.J., Kennedy, M.A.,2002. A common P-glycoprotein polymorphism is associated withnortriptyline-induced postural hypotension in patients treatedfor major depression. Pharmacogenomics J. 2, 191–196.
Rochat, B., Baumann, P., Audus, K.L., 1999. Transport mechanisms
for the antidepressant citalopram in brain microvessel endothe-lium. Brain Res. 831, 229–236.Rodriguez, M., Ortega, I., Soengas, I., Suarez, E., Lukas, J.C., Calvo,
R., 2004. Effect of P-glycoprotein inhibition on methadoneanalgesia and brain distribution in the rat. J. Pharm. Pharmacol.56, 367–374.
Romsicki, Y., Sharom, F.J., 1999. The membrane lipid environmentmodulates drug interactions with the P-glycoprotein multidrugtransporter. Biochemistry 38, 6887–6896.
Sadeque, A.J.M., Wandel, C., He, H., Shah, S., Wood, A.J.J., 2000.Increased drug delivery to the brain by P-glycoprotein inhibition.Clin. Pharmacol. Ther. 68, 231–237.
Saeki, T., Ueda, K., Tanigawara, Y., Hori, R., Komano, T., 1993. P-glycoprotein transports cyclosporine A and FK506. J. Biol. Chem.268, 6077–6080.
Sakaeda, T., Nakamura, T., Okumura, K., 2003. Pharmacogenetics of MDR1 and its impact on the pharmacokinetics and pharmacody-namics of drugs (Review). Pharmacogenomics 4, 397–410.
Sartor, L.L., Bentjen, S.A., Trepanier, L., Mealey, K.L., 2004.Loperamide toxicity in a Collie with the MDR1 mutationassociated with ivermectin sensitivity. J. Vet. Intern. Med. 18,117–118.
Schinkel, A.H., 1997. The physiological function of drug-transportingP-glycoproteins (Review). Semin. Cancer Biol. 8, 161–170.
Schinkel, A.H., 1999. P-glycoprotein, a gatekeeper in the blood–brain barrier (Review). Adv. Drug Deliv. Rev. 36, 179–194.
Schinkel, A.H., Smit, J.J.M., Beijnen, J.H., Wagenaar, E., vanDeemter, L., Mol, C.A.A.M., van der Valk, M.A., Robanus-Maandag, E.C., te Riele, H.P.J., Berns, A.J.M., Borst, P., 1994.Disruption of the mouse mdr1a P-glycoprotein gene leads to a
deficiency in the blood–brain barrier and to increased sensitivityto drugs. Cell 77, 491–502.
Schinkel, A.H., Mayer, U., Wagenaar, E., Mol, C.A.A.M., vanDeemter, L., Smit, J.J.M., van der Valk, M.A., Voordouw, A.C.,Spits, H., van Tellingen, O., Zijlmans, J.M., Fibbe, W.E., Borst, P.,1997. Normal viability and altered pharmacokinetics in micelacking mdr1-type (drug-transporting) P-glycoproteins. Proc.Natl. Acad. Sci. U. S. A. 94, 4028–4033.
Schmitt, U., Abou El-Ela, A., Guo, L.J., et al., 2006. Cyclosporine A(CsA) affects the pharmacodynamics and pharmacokinetics of theatypical antipsychotic amisulpride probably via inhibition of P-glycoprotein (P-gp). J. Neural Transm. 113, 787–801.
Shapiro,A.B.,Ling,V., 1998. Transport of LDS-751 fromthe cytoplasmicleaflet of the plasma membrane by the rhodamine-123-selectivesite of P-glycoprotein. Eur. J. Biochem. 254, 181–188.
Sharom, F.J., 1997. The P-glycoprotein efflux pump: how does ittransport drugs? (Review). J. Membr. Biol. 160, 161–175.
Siddiqui, A., Kerb, R., Weale, M.E., Brinkmann, U., Smith, A.,Goldstein, D.B., Wood, N.W., Sisodya, S.M., 2003. Association of multidrug resistance in epilepsy with a polymorphism in the drug-transporter gene ABCB1. N. Engl. J. Med. 348, 1442–1448.
Sills, G.J., Kwan, P., Butler, E., de Lange, E.C.M., van den Berg, D.J.,Brodie, M.J., 2002. P-glycoprotein-mediated efflux of antiepi-
leptic drugs: preliminary studies in mdr1a knockout mice.Epilepsy Behav. 3, 427–432.Sills, G.J., Mohanraj, R., Butler, E., McCrindle, S., Collier, L., Wilson,
E.A., Brodie, M.J., 2005. Lack of association between the C3435TPolymorphism in the human multidrug resistance (MDR1) geneand response to antiepileptic drug treatment. Epilepsia 46,643–647.
Sisodiya, S.M., Lin, W.R., Harding, B.N., Squier, M.V., Thom, M., 2002.Drug resistance in epilepsy: expression of drug resistance proteinsin common causes of refractory epilepsy. Brain 125, 22–31.
Skarke, C., Jarrar, M., Erb, K., Schmidt, H., Geisslinger, G., Lötsch,J., 2003. Respiratory and miotic effects of morphine in healthyvolunteers when P-glycoprotein is blocked by quinidine. Clin.Pharmacol. Ther. 74, 303–311.
Sparreboom, A., Van Asperen, J., Mayer, U., Schinkel, A.H., Smit,
J.W., Meijer, D.K.F., Borst, P., Nooijen, W.J., Beijnen, J.H., VanTellingen, O., 1997. Limited oral bioavailability and activeepithelial excretion of paclitaxel (Taxol) caused by P-glycopro-tein in the intestine. Proc. Natl. Acad. Sci. U. S. A. 94,2031–2035.
Sugawara, I., Hamada, H., Tsuruo, T., Mori, S., 1990. Specializedlocalization of P-glycoprotein recognized by MRK 16 monoclonalantibody in endothelial cells of the brain and the spinal cord.Jpn. J. Cancer Res. 81, 727–730.
Szabó, D., Szabó Jr., G., Ocsovszki, I., Aszalos, A., Molnár, J., 1999.Anti-psychotic drugs reverse multidrug resistance of tumor celllines and human AML cells ex-vivo. Cancer Lett. 139, 115–119.
Tan, N.C.K., Heron, S.E., Scheffer, I.E., Pelekanos, J.T., McMahon, J.M.,Vears, D.F., Mulley, J.C., Berkovic, S.F., 2004. Failure to confirmassociation of a polymorphism in ABCB1 with multidrug-resistant
epilepsy. Neurology 63, 1090–
1092.Tanaka, Y., Abe, Y., Tsugu, A., Takamiya, Y., Akatsuka, A., Tsuruo, T.,Yamazaki, H., Ueyama, Y., Sato, O., Tamaoki, N., Nakamura, M.,1994. Ultrastructural localization of P-glycoprotein on capillaryendothelial cells in human gliomas. Virchows Arch. 425, 133–138.
Task Force on the Use of Laboratory Tests in Psychiatry, 1985.Tricyclic antidepressants — blood level measurements andclinical outcome: an APA task force report. Am. J. Psychiatry142, 155–162.
Thuerauf, N., Fromm, M.F., 2006. The role of the transporter P-glycoprotein for disposition and effects of centrally acting drugsand for the pathogenesis of CNS diseases. Eur. Arch. PsychiatryClin. Neurosci. 256, 281–286.
Tröger, U., Lins, H., Scherrmann, J.M., Wallesch, C.W., Bode-Böger,S.M., 2005. Tetraparesis associated with colchicines is probably
168 K. Linnet, T.B. Ejsing

7/27/2019 A Review on the Impact of P-Glycoprotein on the Penetration of Drugs Into the Brain. Focus on Psychotropic Drugs
http://slidepdf.com/reader/full/a-review-on-the-impact-of-p-glycoprotein-on-the-penetration-of-drugs-into-the 13/13
due to inhibition by verapamil of the P-glycoprotein efflux pumpin the blood–brain barrier. BMJ 331, 613.
Uhr, M., Grauer, M.T., 2003. abcb1ab P-glycoprotein is involved inuptake of citalopram and trimipramine into the brain of mice.J. Psychiatr. Res. 37, 179–185.
Uhr, M., Steckler, T., Yassouridis, A., Holsboer, F., 2000. Penetration of amitriptyline, butnot of fluoxetine, into brain is enhancedin micewith blood–brain barrier deficiency due to Mdr1a P-glycoproteingene disruption. Neuropsychopharmacology 22, 380–387.
Uhr, M., Holsboer, F., Müller, M.B., 2002. Penetration of endogenoussteroid hormones corticosterone, cortisol, aldosterone andprogesterone into the brain is enhanced in mice deficient forboth mdr1a and mdr1b P-glycoproteins. J. Neuroendocrinol. 14,753–759.
Uhr, M., Grauer, M.T., Holsboer, F., 2003. Differential enhancementof antidepressant penetration into the brain in mice withabcb1ab (mdr1ab) P-glycoprotein gene disruption. Biol. Psychi-atry 54, 840–846.
Van Asperen, J., Schinkel, A.H., Beijnen, J.H., Nooijen, W.J., Borst,P., van Tellingen, O., 1996. Altered pharmacokinetics of vinblastine in Mdr1a P-glycoprotein-deficient mice. J. Natl.Cancer Inst. 88, 994–999.
Van Asperen,J., vanTellingen, O.,Beijnen, J.H., 2000.The roleof mdr1a
P-glycoprotein in the biliary and intestinal secretion of doxorubicinand vinblastine in mice. Drug Metab. Dispos. 28, 264–267.Van der Sandt, I.C.J., Vos, C.M.P., Nabulsi, L., Blom-Roosemalen,
M.C.M., Voorwinden, H.H. , de Boer, A.G., Breimer, D.D., 2001.Assessment of active transport of HIV protease inhibitors invarious cell lines and the in vitro blood–brain barrier. AIDS 15,483–491.
Virginento, D., Robertson, D., Errede, M., Benagiano, V., Girolamo,F., Maiorano, E., Roncali, L., Bertossi, M., 2002. Expression of P-glycoprotein in human cerebral cortex microvessels. J. Histo-chem. Cytochem. 50, 1671–1676.
Volk, H.A., Burkhardt, K., Potschka, H., Chen, J., Becker, A.,Löscher, W., 2004. Neuronal expression of the drug effluxtransporter P-glycoprotein in the rat hippocampus after limbicseizures. Neuroscience 123, 751–759.
Wang, E.J., Casciano, C.N., Clement, R.P., Johnson, W.W., 2001.Inhibition of P-glycoprotein transport function by grapefruit juicepsoralen. Pharm. Res. 18, 432–438.
Wang, Z., Hamman, M.A., Huang, S.M., Lesko, L.J., Hall, S.D., 2002.Effect of St John’s wort on the pharmacokinetics of fexofena-dine. Clin. Pharmacol. Ther. 71, 414–420.
Wang, E.-J., Barecki-Roach, M., Johnson, W.W., 2004a. Quantitativecharacterization of direct P-glycoprotein inhibition by St John’swort constituents hypericin and hyperforin. J. Pharm. Pharma-col. 56, 123–128.
Wang, J.S., Ruan, Y., Taylor, R.M., Donovan, J.L., Markowitz, J.S.,DeVane, C.L., 2004b. Brain penetration of methadone (R)- and(S)-enantiomers is greatly increased by P-glycoprotein deficiencyin the blood–brain barrier of Abcb1a gene knockout mice.Psychopharmacology (Berl) 173, 132–138.
Wang, J.S., Taylor, R., Ruan, Y., Donovan, J.L., Markowitz, J.S.,DeVane, C.L., 2004c. Olanzapine penetration into brain is greaterin transgenic Abcb1a P-glycoprotein deficient mice than FVB1(wild-type) animals. Neuropsychopharmacology 29, 551–557.
Wang, J.S., Ruan, Y., Taylor, R.M., Donovan, J.L., Markowitz, J.S.,DeVane, C.L., 2004d. The brain entry of risperidone and 9-hydroxyrisperidone is greatly limited by P-glycoprotein. Int. J.Neuropsychopharmacol. 7, 415–419.
Wang,J.S., DeVane, C.L., Gibson,B.B.,Donovan, J.L., Markowitz,J.S.,Zhu, H.J., 2006. Population pharmacokinetic analysis of drug–druginteractions among risperidone, buprion, and sertraline in CF1mice. Psychopharmacology (Berl) 183, 490–499.
Warren, K.E., Patel, M.C., McCully, C.M., Montuenga, L.M., Balis, F.M.,2000. Effect of P-glycoprotein modulation with cyclosprin A on
cerebrospinal fluid penetration of doxorubicin in non-humanprimates. Cancer Chemother. Pharmacol. 45, 207–212.Weiss, J., Dormann, S.M., Martin-Facklam, M., Kerpen, C.J., Ketabi-
Kiyanvash, N., Haefeli, W.E., 2003. Inhibition of P-glycoprotein bynewer antidepressants. J. Pharmacol. Exp. Ther. 305, 197–204.
Yamazaki, M., Neway, W.E., Ohe, T., Chen, I.-W., Rowe, J.F.,Hochman, J.H., Chiba, M., Lin, J.H., 2001. In vitro substrateidentification studies for P-glycoprotein-mediated transport:species difference and predictability of in vivo results.J. Pharmacol. Exp. Ther. 296, 723–735.
Young, A.M., Allen, C.E., Audus, K.L., 2003. Efflux transporters of the human placenta. Adv. Drug Deliv. Rev. 55, 125–132.
Zimprich, F., Sunder-Plassmann, R., Stogmann, E., Gleiss, A., Dal-Bianco, A., Zimprich, A., Plumer, S., Baumgartner, C., Mannhal-ter, C., 2004. Association of an ABCB1 gene haplotype with
pharmacoresistance in temporal lobe epilepsy. Neurology 63,1087–1089.
169A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs