a prospective cohort study of intake of calcium, vitamin d...
TRANSCRIPT

Vol. 7, 221-225. March 1998 Cancer Epidemiology, Biomarkers & Prevention 22/
A Prospective Cohort Study of Intake of Calcium, Vitamin D, and Other
Micronutrients in Relation to Incidence of Rectal Cancer among
Postmenopausal Women’
Wei Zheng,2 Kristin E. Anderson, Lawrence H. Kushi,Thomas A. Sellers, Jessica Greenstein, Ching-Ping Hong,James R. Cerhan, Roberd M. Bostick, andAaron R. Folsom
Division of Epidemiology. School of Public Health. University of Minnesota.
Minneapolis. Minnesota 55454-1015 [W. Z., K. E. A., L. H. K., T. A. S., J. G.,
C-P. H., A. R. F.]; Department of Preventive Medicine and EnvironmentalHealth, College of Medicine, University of Iowa, Iowa City. Iowa 52242
[J. R. C.]; and Division of Public Health Sciences-Epidemiology, The BowmanGray School of Medicine, Wake Forest University, Winston-Salem, North
Carolina 27157 [R. M. B.]
Abstract
To investigate whether high intakes of calcium and othermicronutrients (carotene, retinol, and vitamins C, D, andE) are related to reduced risks of rectal cancer, weanalyzed data from a large cohort study ofpostmenopausal Iowa women who responded to a mailedsurvey in 1986. After 9 years of follow-up, 144 incidentrectal cancer cases were ascertained among the 34,702women at risk. Intake levels of micronutrients at baselinewere derived from self-reported data on vitaminsupplements and dietary intake of 127 foods included in asemiquantitative food frequency questionnaire. Afteradjustment for total energy intake and other potentialconfounding factors, a dose-response inverse associationwas observed between total calcium intake and the risk ofrectal cancer: adjusted relative risks (RRs) were 1.00,0.90, and 0.59 (trend test, P = 0.02) from the lowest tothe highest calcium intake tertiles. High intakes of dietaryand supplement calcium were both related to a slightlyreduced risk of rectal cancer, but neither of the trendtests was statistically significant. Reduced risks of rectalcancer were also observed for high intake of carotene andvitamins A, C, and D, although none of the associationswere statistically significant. For vitamin D, the adjustedRRs were 1.00, 0.71, and 0.76 (trend test, P 0.20) forincreasing intake tertiles. Compared with women whoconsumed low levels of both total calcium and vitamin D,those in the highest intake group of both nutrients wereat a 45% reduced risk of rectal cancer (RR, 0.55; 95%confidence interval, 0.32-0.93). This study supports thehypothesis that high intake of calcium and possibly other
Received 7/24/97: revised 12/5/97; accepted 12/I 1/97.The costs of publication of this article were defrayed in part by the payment of
page charges. This article must therefore be hereby marked adi’ertiserne,tt inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
I This study was supported by Grant ROl CA39742 from the National Cancer
Institute.
2 To whom requests for reprints should be addressed. at 15 Richland Medical
Park. Suite 310. University of South Carolina. Columbia, SC 29203.
micronutrients may be beneficial in the prevention ofrectal cancer.
Introduction
Calcium and a number of micronutrients have been hypothe-sized to have potential beneficial effects in the prevention of
colorectal cancer ( 1 ), the second most common malignancy inthe United States ( 1 ). Experimental studies in rodents have
shown that calcium administration ameliorates the proliferation
of colonic epithelial cells (2, 3) and reduces the occurrence ofchemically induced tumors (2, 3). This cancer-inhibitory effectis believed to be due to the ability of this mineral to bindsecondary bile acids and ionized fatty acids in the colonic
lumen to reduce their toxic effects on epithelial cells (2, 3). Invitro studies have also suggested that calcium may act directly
on colonic epithelial cells by regulating the cell cycle andinducing terminal differentiation (2, 3).
The absorption of calcium in the gastrointestinal tract andcell uptake of this mineral depend on adequate vitamin D.
Vitamin D can also induce differentiation of colonic mucosa,
and this function may be mediated through the vitamin Dreceptor (3-8). It has been demonstrated in animal studies thatadministration of vitamin D inhibits proliferation of colonic
epithelial cells and reduces the occurrence of chemically in-
duced colon tumors (3-8). Other micronutrients may also pro-tect against colorectal cancer. Carotenoids and vitamins C andE are antioxidants that quench free radicals and reduce oxida-
tive damage to DNA and other molecules (9). It has beendemonstrated in a number of animal studies that increasing
intake of these micronutrients reduces the risk of experimentaltumors in different organs, including the large bowel (9).
Despite evidence from animal studies and in vitro exper-iments, the potential benefits of calcium, vitamin D, and other
micronutrients on colorectal cancer have not been clearly dem-onstrated in humans (1-3, 10-17). Most previous epidemiologystudies were case-control studies, and many of them had a smallsample size and/or incomplete data on dietary and supplementalsources of calcium and vitamins ( 1-3). Cohort studies have
been few, and results from them are inconsistent (1, 1 1-17). Inthe Iowa Women’s Health Study, comprehensive information
on usual diet and food supplements was obtained from 41,836women ages 55-69 years in 1986. High intakes ofcalcium andvitamins D and E were previously suggested in this cohort to be
related to a reduced risk of colon cancer ( 1 1 , 12). In this report,we evaluate the association of these nutrients with the incidenceof rectal cancer.
Materials and Methods
Detailed descriptions of the cohort study have been published
elsewhere (18-20). Briefly, 41,836 Iowa women ages 55-69
on November 29, 2018. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

222 Calcium, Vitamins, and Rectal Cancers
3 The abbreviations used are: RR, relative risk; Cl, confidence interval.
years who completed a mailed questionnaire in January 1986were followed for mortality and cancer incidence. Vital statusfor cohort members was determined through computer linkage
of participant identifiers with Iowa death certificates and the Na-
tional Death Index and through mailed follow-up questionnaires in1987, 1989, and 1992. On the basis of our follow-up surveys, it is
estimated that the out-migration rate among cohort members was
less than 1% annually. Information on cancer diagnosis was ob-tamed through the State Health Registry of Iowa, part of theSurveillance, Epidemiology, and End Results Program of the Na-tional Cancer Institute (21). Through December 31, 1994 (9 yearsof follow-up), 41 13 women developed at least one new primarycancer. Among them, 157 were cancer of the rectum (International
Classification of Diseases-Oncology, code = 154), accounting for24.7% of cancers of the large intestine (22).
A self-administered questionnaire was used in the 1986baseline survey to obtain information on diet and other major
risk factors for cancer. Diet was assessed using a semiquanti-
tative food frequency questionnaire almost identical to that usedin the 1984 Nurses’ Health Study (23). Usual intakes of specifiedportions of I 27 food items were ascertained. A separate section onvitamin and mineral supplements was included in the question-
naire to obtain information on intake of calcium; vitamins A, C, D,and E; and multivitamins. The validity and reliability of the FoodFrequency Questionnaire in our study population have been re-ported elsewhere (23). The Pearson’s correlation coefficients ofnutrient intake from the frequency questionnaire with those from
five 24-h dietary recalls are 0.67 for calcium, 0.5 1 for vitamin D,
0.60 for vitamin A, 0.82 for vitamin C, and 0.62 for vitamin E.Nutrient intake was estimated using the nutrient database devel-oped for the Nurses’ Health Study (23).
We excluded from the analyses women who reported at
baseline a history of cancer, including melanoma (n 3830),those who left 30 or more blanks on the dietary questionnaire(n 2782), those who were determined to have extreme totalenergy intake (<600 or �5000 kcallday; n = 538), and thosewho were not postmenopausal (n 569). A total of565 womenhad two or more exclusions. After these exclusions, 34,702
cohort members, including 144 who developed rectal cancer,remained for the analyses.
RRs3 were used to measure the strength of associationbetween exposures and cancer incidence. Proportional hazards
regression (the Cox model) was used to control for potentialconfounders and to derive adjusted RRs and 95% CIs (24). RRswere adjusted for the following independent risk factors thatwere correlated with one or more dietary variables: age (con-
tinuous variable), smoking status (never, former, or current)and pack-years of cigarette smoking (continuous variable), and
hormone replacement therapy (never or ever). Meat and fiberintakes, which are risk factors for colorectal cancer reported in
other studies ( 1),were not found to be related to the risk in thisstudy population and thus not were included in the model as
confounding variables. Dietary factors were adjusted also fortotal energy intake using the residual method to evaluate the
independent association of a specific nutrient or mineral and toreduce potential variations that may have arisen from over- orunder-reporting of food consumption (25). In some analyses,
adjustments were done for additional variables, body massindex, alcohol consumption, fat and protein intake, and physical
activity using tertile variables. A trend test for a dose-responserelationship across levels of each dietary variable was per-
Table I RRs of rectal cancer for selected variables, from the Iowa Women’s
Health Study. 1986-1993
No. of No. of Age-adjusted RR
person-yr cases” (95% CI)
Age at baseline (yrs)
55-59 107,377 38 1.00”
60-64 104,081 52 1.41 (0.93-2.15)
�65 81,632 54 1.87 (1.24-2.84)
P for trend < 0.01
Education
Less than high school 52,758 29 1.00
High school graduate 123,784 59 0.91 (0.58-1.42)
More than high school graduate 1 15,982 56 0.92 (0.59-1.44)
P for trend = 0.70
Pack-yrs of smoking
Never 192,062 87 1.00
<30 pack-yr 54,287 27 1.16 (0.75-1.79)
�30 pack-yr 40,695 26 1 .49 (0.96-2.31)
P for trend = 0.08
Hormone replacement therapy
Never 179,130 99 1.00
<5 years 79,408 32 0.72 (0.48-1.07)
�5 years 31,946 12 0.67 (0.37-1.23)
P for trend = 0.20
Total energy intake (tertiles. kcal/day)
<1499.1 97,428 54 1.00
1499.1-1970.3 97,675 42 0.78 (0.52-1.17)
�1940.4 97,987 48 0.89 (0.60-1.32)
P for trend = 0.56
Total fat intake (tertiles. g/day)
<54.6 97.319 51 1.00
54.6-75.9 97,506 50 0.93 (0.60-1.43)
�76.0 98,266 43 0.73 (0.38-1.38)
P for trend = 0.33
Total fruit and vegetable intake (tertile. servings/week)
<33.5 96,744 50 1.00
33.5-48.5 98,806 44 0.85 (0.56-1.28)
�48.6 97,540 50 0.97 (0.62-1.51)
P for trend = 0.87
“ May not add up to 144 cases due to missing values.
“ Unadjusted RR.
formed by treating each ordinal-score variable (with values of1, 2, and 3) as a continuous variable in proportional hazardsregression after adjustment for potential confounders.
Results
The associations between rectal cancer incidence and ma-jor risk factors reported in other studies were examined in this
cohort (Table 1). Age was positively related to the risk of rectalcancer. The risks were also elevated among women who were
heavy smokers. There was a suggestive inverse association withduration of hormone replacement therapy, although it was notstatistically significant. No apparent association was observed
between rectal cancer and intake levels of total energy, total fat,and total fruits and vegetables. The associations of these van-ables with calcium intake, the variable of primary interest in
this paper, are presented in the Appendix. Only a few of thevariables were confounders, because they were related to bothrectal cancer risk and calcium intake. Other suspected etiolog-
ical factors, including physical inactivity, alcohol drinking,
body weight, use of nonsteroidal anti-inflammatory drugs, andmeat and fiber intake, were not found to be associated withrectal cancer risk (data not shown).
Table 2 presents the associations of rectal cancer withintake levels of calcium and vitamins from both diet and sup-
on November 29, 2018. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 223
Table 2 RRs of rectal cancer by intake levels of selected micronutrients,
from the Iowa Women’s Health Study, 1986-1993
Intake level (tertiles)”P for trend
Low Intermediate High
Calcium
No. of cases 56 52 36
RR” 1 .00 0.90 0.59 0.02
95% CI 0.61-1.33 0.37-0.94
Vitamin D
No. of cases 56 41 47
RR 1.00 0.71 0.76 0.20
95% CI 0.47-1.08 0.50-1.16
Vitamin A
No. of cases 54 48 42
RR 1.00 0.87 0.76 0.22
95% CI 0.58-1.29 0.49-1.18
Retinol
No. of cases 47 55 42
RR 1.00 1.16 0.84 0.44
95% CI 0.78-1.72 0.55-1.30
Carotene
No. of cases 49 50 45
RR 1.00 0.96 0.80 0.31
95% CI 0.62-1.49 0.52-1.23
Vitamin C
No. of cases 55 41 48
RR 1.00 0.72 0.84 0.40
95% CI 0.48-1.10 0.56-1.26
Vitamin E
No. of cases 52 49 43
RR 1.00 1.00 0.93 0.73
95% CI 0.67-1.51 0.59-1.44
a Subjects were categorized according to the tertile distribution of all cohort
members at risk. The cutoff points were <800.8 and >1278.7 for calcium
(mg/day), <224.1 and >475.5 for vitamin D (lU/day), <9555.8 and >16119.5
for vitamin A (lU/day), <2099.5 and >5673. 1 for retinol (lU/day), <5539. 1 and> 10649.5 for carotene (lU/day), < 144.6 and >261 .7 for vitamin C (mg/day). and
<7.0 and >18.3 for vitamin E (mg/day).
b Adjusted for age, smoking status. pack-years of smoking. use of hormone
replacement therapy, and total energy intake.
plements. After adjustment for age, smoking, hormone replace-ment therapy, and total energy intake, calcium intake wasinversely related to the risk of rectal cancer (trend test, P0.02); the RR was 0.59 (95% CI, 0.37-0.94) for the highestintake tertile compared with the lowest intake tertile. The re-sults were essentially unchanged after additional adjustment forintake of animal fat and protein, alcohol consumption, physical
activity, and body mass index. The risks were about 20-30%reduced among women who consumed a high level of carotene
or vitamin D, A, or C, but none of the RRs or trend testsapproached standard statistical significance level (P < 0.05).
About 48% of women reported taking calcium supple-
ments regularly at the baseline survey. Additional analyseswere performed to assess the calcium-cancer association by
intake sources of this mineral. After adjusting for confoundingvariables, the RRs were 1.00, 0.84, and 0.57 with increasing
intake tertiles of dietary calcium (trend test, P = 0.10). Theadjusted RRs were 1.00, 0.94, and 0.72 with increasing intake
tertiles of dairy products (trend test, P = 0.17), the major foodsource of dietary calcium. The strengths of the associations
were attenuated slightly for both total calcium intake (RR, 0.64;
95% CI, 0.39-1.06 for the uppermost tertile) and dairy productintake (RR, 0.84; 95% CI, 0.51-1.37 for the uppermost tertile)when these two variables were included in the same model.
Compared to women who reported never taking calcium sup-
plements, those who took calcium supplements regularly wereat about 25% reduced risk of rectal cancer (RR, 0.76; 95% CI,
0.54-1.07). The risk, however, was not reduced further withincreasing supplement dose (P for trend, 0. 17). No apparent
association was observed between rectal cancer and any of thevitamins stratified by intake sources. For example, the adjusted
RRs were 1.00, 1.13, and 0.91 (P for trend, 0.70) with increasingintake tertiles of dietary vitamin D and 1.00, 0.87, and 0.95 (P fortrend, 0.80) with increasing tertiles of vitamin D supplements.
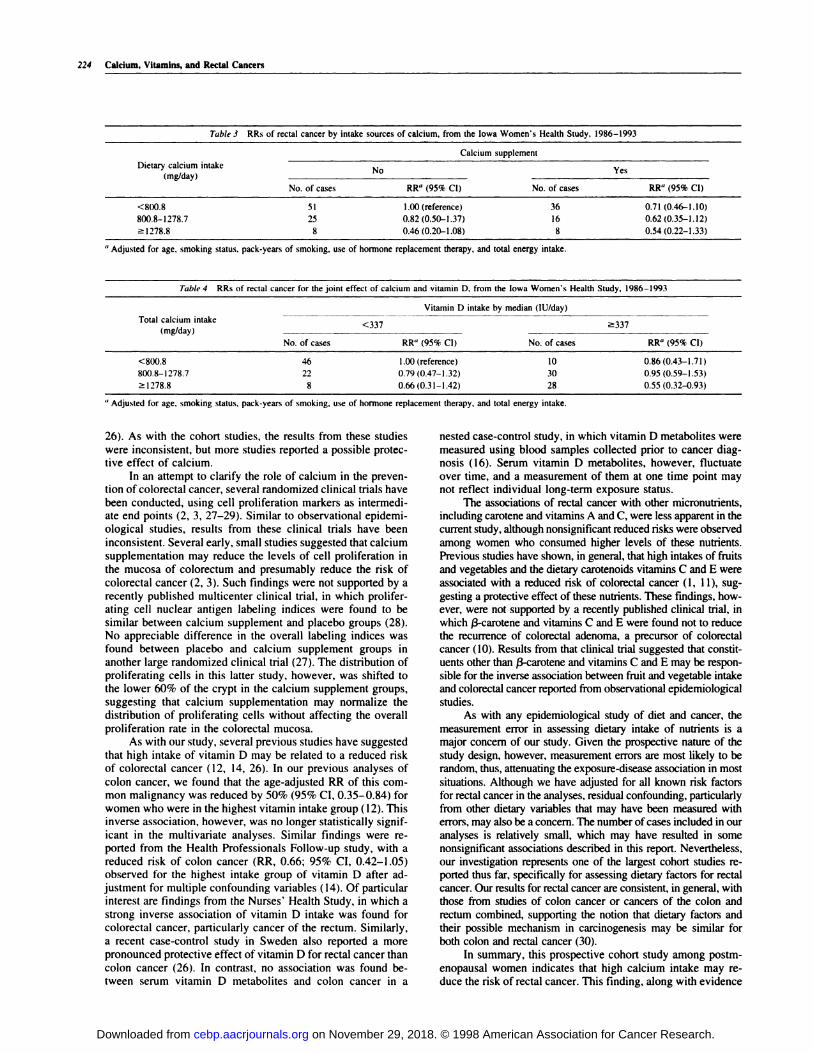
To assess possible independent associations of dietary and
supplemental calcium with rectal cancer risk, a stratified anal-ysis was performed (Table 3). The risks of rectal cancer werereduced with increasing intakes of dietary calcium in both
calcium supplement and nonsupplement groups. Calcium sup-plements also appeared to reduce the rectal cancer risk, but the
pattern was less consistent. The small number of cancer casesprecluded detailed analyses of supplement dose in relation torectal cancer risk.
Because vitamin D is involved in the absorption of calcium,
we explored the potential interaction of these two compounds in
the prevention of rectal cancer. Cohort members were stratified
according to the median intake level of vitamin D and then furthergrouped by tertile intake levels oftotal calcium (Table 4). Women
who consumed the highest levels of both calcium and vitamin Dhad the lowest risk of developing rectal cancer (RR, 0.55; 95% CI,
0.32-0.93), but the potential interaction was not statistically sig-
nificant on a multiplicative scale.
Discussion
This prospective cohort study found that postmenopausal
women who consumed levels of calcium in the upper tertile hada reduced risk of developing rectal cancer in the subsequent 9
years. Our data also suggested that high intakes of carotene andvitamins D, A, and C may be related to a decreased risk of rectal
cancer, but the associations were not statistically significantwith this number of cases.
Although in vitro and animal studies have consistently
demonstrated the beneficial effect of calcium in the preventionof colorectal tumors, results from epidemiological studies have
been inconsistent. We previously reported from the Iowa Wom-
en’s Health Study that high calcium intake was associated witha 50% lower risk of colon cancer after adjustment for age ( 12).This inverse association persisted after adjustment for addi-tional variables, but the trend test was no longer statisticallysignificant. Similar findings were reported in the Health Pro-fessionals Follow-up Study with multiple adjustment substan-
tially attenuating the inverse association between calcium andcolon cancer (14). In the Nurses’ Health Study, a nonsignificantreduced risk of colorectal cancer was found to be associated
with high intake of dietary calcium ( I 3). Of note is that theinverse association was more pronounced for rectal cancer, but
the results were based on a small number of cases. Likewise, astronger inverse association of calcium intake from unfer-mented dairy products was found with rectal cancer than withcancers of the colon and rectum combined in the Netherlands
Cohort Study (15). In that study, however, no statisticallysignificant association was observed between colorectal cancerand total dietary calcium (15). Perhaps the strongest associationbetween calcium intake and colorectal cancer was reported
from an early study in the Western Electric Cohort, in which a70% reduction in risk was found among high calcium consum-ers (17). In addition to the cohort studies described above, manycase-control studies have also been conducted to assess theassociation between calcium intake and colorectal cancer ( 1,
on November 29, 2018. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
224 Calcium, Vitamins, and Rectal Cancers
Table 3 RRs of rectal cancer by intake sources of calcium, from the Iowa Women’s Health Study, 1986-1993
Calcium supplement
Dietary calcium intakeNo Yes
(mg/day)
No. of cases RR� (95% CI) No. of cases RR� (95% CI)
<800.8 51 1.00 (reference) 36 0.71 (0.46-1.10)
800.8-1278.7 25 0.82 (0.50-1.37) 16 0.62 (0.35-1.12)
�l278.8 8 0.46 (0.20-1.08) 8 0.54 (0.22-1.33)
a Adjusted for age, smoking status. pack-years of smoking. use of hormone replacement therapy, and total energy intake.
Table 4 RRs of rectal cancer for the joint effect of calcium and vitamin D, from the Iowa Women’s Health Study. 1986-1993
Vitamin D intake by median (lU/day)
Total calcium intake <337 >337
(mg/day) -
No. of cases RR� (95% CI) No. of cases RR� (95% CI)
<800.8 46 1.00 (reference) 10 0.86(0.43-1.71)
800.8-1278.7 22 0.79 (0.47-1.32) 30 0.95 (0.59-1.53)
�l278.8 8 0.66 (0.31-1.42) 28 0.55 (0.32-0.93)
a Adjusted for age. smoking status, pack-years of smoking. use of hormone replacement therapy, and total energy intake.
26). As with the cohort studies, the results from these studies
were inconsistent, but more studies reported a possible protec-tive effect of calcium.
In an attempt to clarify the role of calcium in the preven-tion of colorectal cancer, several randomized clinical trials have
been conducted, using cell proliferation markers as intermedi-ate end points (2, 3, 27-29). Similar to observational epidemi-ological studies, results from these clinical trials have beeninconsistent. Several early, small studies suggested that calciumsupplementation may reduce the levels of cell proliferation in
the mucosa of colorectum and presumably reduce the risk of
colorectal cancer (2, 3). Such findings were not supported by arecently published multicenter clinical trial, in which prolifer-ating cell nuclear antigen labeling indices were found to besimilar between calcium supplement and placebo groups (28).No appreciable difference in the overall labeling indices wasfound between placebo and calcium supplement groups in
another large randomized clinical trial (27). The distribution ofproliferating cells in this latter study, however, was shifted to
the lower 60% of the crypt in the calcium supplement groups,suggesting that calcium supplementation may normalize the
distribution of proliferating cells without affecting the overallproliferation rate in the colorectal mucosa.
As with our study, several previous studies have suggestedthat high intake of vitamin D may be related to a reduced riskof colorectal cancer (12, 14, 26). In our previous analyses of
colon cancer, we found that the age-adjusted RR of this com-mon malignancy was reduced by 50% (95% CI, 0.35-0.84) for
women who were in the highest vitamin intake group (12). Thisinverse association, however, was no longer statistically signif-icant in the multivaniate analyses. Similar findings were re-
ported from the Health Professionals Follow-up study, with areduced risk of colon cancer (RR, 0.66; 95% CI, 0.42-1.05)observed for the highest intake group of vitamin D after ad-
justment for multiple confounding variables (14). Of particularinterest are findings from the Nurses’ Health Study, in which astrong inverse association of vitamin D intake was found forcolorectal cancer, particularly cancer of the rectum. Similarly,
a recent case-control study in Sweden also reported a morepronounced protective effect of vitamin D for rectal cancer than
colon cancer (26). In contrast, no association was found be-tween serum vitamin D metabolites and colon cancer in a
nested case-control study, in which vitamin D metabolites were
measured using blood samples collected prior to cancer diag-nosis (16). Serum vitamin D metabolites, however, fluctuateover time, and a measurement of them at one time point maynot reflect individual long-term exposure status.
The associations of rectal cancer with other micronutnients,including carotene and vitamins A and C, were less apparent in thecurrent study, although nonsignificant reduced risks were observed
among women who consumed higher levels of these nutrients.Previous studies have shown, in general, that high intakes of fruits
and vegetables and the dietary carotenoids vitamins C and E wereassociated with a reduced risk of colorectal cancer (1, 11), sug-
gesting a protective effect of these nutrients. These findings, how-
ever, were not supported by a recently published clinical trial, inwhich f3-carotene and vitamins C and E were found not to reduce
the recurrence of colorectal adenoma, a precursor of colorectalcancer (10). Results from that clinical trial suggested that constit-uents other than �3-carotene and vitamins C and E may be respon-sible for the inverse association between fruit and vegetable intake
and colorectal cancer reported from observational epidemiologicalstudies.
As with any epidemiological study of diet and cancer, the
measurement error in assessing dietary intake of nutrients is amajor concern of our study. Given the prospective nature of the
study design, however, measurement errors are most likely to berandom, thus, attenuating the exposure-disease association in most
situations. Although we have adjusted for all known risk factorsfor rectal cancer in the analyses, residual confounding, particularly
from other dietary variables that may have been measured witherrors, may also be a concern. The number of cases included in our
analyses is relatively small, which may have resulted in somenonsignificant associations described in this report. Nevertheless,
our investigation represents one of the largest cohort studies re-ported thus far, specifically for assessing dietary factors for rectal
cancer. Our results for rectal cancer are consistent, in general, withthose from studies of colon cancer or cancers of the colon andrectum combined, supporting the notion that dietary factors and
their possible mechanism in carcinogenesis may be similar forboth colon and rectal cancer (30).
In summary, this prospective cohort study among postm-
enopausal women indicates that high calcium intake may re-duce the risk of rectal cancer. This finding, along with evidence
on November 29, 2018. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer EpIdemiology, Biomarkers & Prevention 225
accumulated from numerous in vitro, animal, and epidemiolog-
ical investigations, suggests that increasing dietary intake of
calcium may be beneficial in the prevention of rectal cancer.
Acknowledgments
We thank Pat Thomas for technical assistance.
Appendix
Distribution of calcium intake levels by selected variables, from th
Women’s Health Study, 1986-1993e Iowa
Calcium intake level
(tertile, mg/day)”
<800.8 800.8-1278.7 a 1278.8
Age at baseline
55-59 32.8 32.5 34.6
60-64 33.6 33.4 33.0
a65 33.6 34.4 32.1
Education
Less than high school 39.3 32.3 28.4
High school graduate 36.3 33.5 30.2
More than high school graduate 27.5 33.6 38.9
Pack-yr of smoking
Never 32.2 33.9 34.0
<30 pack-yrs 30.7 33.0 36.3
a30 pack-yrs 38.5 32.0 29.6
Hormone replacement therapy
Never 35.7 33.4 30.9
<5 years 29.9 33.2 37.0
as years 28.7 33.1 38.3
Total energy intake (tertile, kcallday)
<1499.1 52.2 29.3 18.5
1499.1-1970.3 33.5 37.0 29.6
a1940.4 14.3 33.7 52.0
Total fat intake (tertile, g/day)
<54.6 46.2 31.1 22.7
54.6-75.9 34.2 34.6 31.2
a76.O 19.6 34.4 46.0
Total fruit and vegetable intake
(tertile, servings/week)
<33.5 48.5 31.0 20.5
33.5-48.5 33.1 35.0 31.0
a48.6 18.5 34.0 47.5
a Percentage by row.
References
1. Schottenfeld, D., and Winawer, S. J. Cancers of the large intestine. In: D.Schottenfeld and J. F. Fraumeni, Jr. (eds.), Cancer Epidemiology and Prevention,2nd Ed, pp. 813-840. New York: W. B. Saunders Co., 1996.
2. Lipkin, M., and Newmark, H. Calcium and the prevention of colon cancer. I.
Cell. Biochem. Suppl., 22: 65-73, 1995.
3. Kleibeuker, J. H., van der Meer, R., and de Vries, E. G. E. Calcium andvitamin D: possible protective agents against colorectal cancer? Eur. J. Cancer,
31A: 1081-1084, 1995.
4. Norman, A. W. The vitamin D endocrine system: manipulation of structure-
function relationships to provide opportunities for development of new cancer
chemopreventive and immunosuppressive agents. J. Cell. Biochem. Suppl., 22:
218-225, 1995.
5. Sitrin, M. D., Halline, A. 0., Abrabams, C., and Brasitus, T. A. Dietary
calcium and vitamin D modulate 1,2-dimethylhydrazine-induced colonic carci.
nogenesis in the rat. Cancer Res., 51: 5608-5613, 1991.
6. Cross, H. S., Pavelka, M., Slavik, J., and Peterlik, M. Growth control of humancolon cancer cells by vitamin D and calcium in vitro. J. Nail. Cancer Inst., 84:
1355-1357. 1992.
7. Thao, X.. and Felman, D. Regulation of vitamin D receptor abundance and
responsiveness during differentiation of HT-29 human colon cancer cells. Endo-
crinology, 132: 1808-1814, 1993.
8. Shabahang, M., Buras, R. R., Davoodi, F., Schumaker, L. M., Nauta, R. J.,Uskokovic, M. R., Brenner, R. I. V., and Evans, S. R. Growth inhibition of HT-29
human colon cancer cells by analogues of I ,25..dihydroxyvitamin D3. Cancer
Res., 54: 4057-4064, 1994.
9. Gerster, H. )3-carotene, vitamin E, and vitamin C in different stages ofexperimental carcinogenesis. Eur. J. Clin. Nutr., 49: 155-168. 1995.
10. Greenberg, E. R., Baron, J. A., Tosteson, T. D., Freeman, D. H., Jr., Beck,
G. J., Bond, J. H., Colacchio T. A., Coller, iA., Frankl, D. H., and Haile, R. W.A clinical trial of antioxidant vitamins to prevent colorectal adenoma. N. EngI.
J. Med., 331: 141-147, 1994.
II. Bostick. R. M., Porter, J. D., McKenzie, D. R., Sellers, T. A.. Kushi, L. H.,
Steinmetz, K. A.. and Folsom, A. R. Reduced risk of colon cancer with high intake
of vitamin E: the Iowa Women’s Health Study. Cancer Rca.. 53: 4230-4237, 993.
12. Bostick, R. M., Potter, J. D., Sellers, T. A., McKenzie, D. R., Kushi, L. H.,
and Folsom, A. R. Relation of calcium, vitamin D, and dairy food intake to
incidence of colon cancer among older women. Am. J. Epidemiol.. 137: 1302-
1317, 1993.
13. Martinez, M. E, Giovannucci, E L, Colditz, G. A., Stampfer, M. J., Hunter,
D. J., Speizer, F. E., Wing, A., and Willett, W. C. Calcium, vitamin D, and theoccurrence of colorectal cancer among women. J. NatI. Cancer Inst., 88: 1375-1382,
1996.
14. Kearney. J., Giovannucci, E., Rimm, E. B., Ascherio, A.. Stampfer, M. J.,
Colditz, 0. A., Wing, A., Kampman, E., and Willett, W. C. Calcium, vitamin D,
and dairy foods and the occurrence of colon cancer in men. Am. J. Epidemiol.,
143: 907-917, 1996.
15. Kampman, E.. Goldbohm, A., van den Brandt, P. A., and van’t Veer, P.
Fermented dairy products. calcium. and colorectal cancer in the Netherlands
Cohort Study. Cancer Res., 54: 3 186-3190, 1994.
16. Braun, M. M., Helzlsouer, K. J., Hollis, B. W., and Comstock, G. W. Coloncancer and serum vitamin D metabolite levels 10-17 years prior to diagnosis.Am. J. Epidemiol., 142: 608-61 1, 1995.
17. Garland, C., Shekelle, R., Barrett-Conner, E.. Criqui, M. H., Rossof, A. H.,
and Oglesby, P. Dietary vitamin D and calcium and risk of colorectal cancer: a19-year prospective study in men. Lancet. I: 307-309. 1985.
18. Kushi, L. H., Sellers, T. A., Potter, J. D., Nelson, C. L., Munger, R. G., Kaye,S. A., and Folsom, A. R. Dietary fat and postmenopausal breast cancer. J. NatI.
Cancer Inst., 84: 1092-1099, 1992.
19. Folsom, A. R., Kaye, S. A., Sellers, T. A., Hong. C. P., Cerhan, J. R. Potter.
J. D., and Prineas, R. J. Body fat distribution and 5-year risk of death in older
women. J. Am. Med. Assoc., 269: 483-487, 1993.
20. Bisgard, K. M., Folsom, A. R., Hong, C-P., and Sellers, T. A. Mortality and
cancer rates in nonrespondents to a prospective study of older women: 5-yearfollow-up. Am. J. Epidemiol., 139: 990-1000, 1994.
21. Kosary, C. L. Ries, L. A. G., Miller, B. A., Hankey, B. F., Harras. A., andEdwards, B. K. (eds.) SEER Cancer Statistics Review, 1973-1992: Tables and
Graphs. National Cancer Institute. NIH PubI. No. 96-2789. Bethesda, MD:National Cancer Institute, 1995.
22. Percy, C., Van Holten, V., and Muir, C. International Class of Diseases for
Oncology, 2nd Ed. Geneva: WHO, 1990.
23. Munger, R. G., Folsom, A. R., Kushi, L. H., Kaye, S. A., and Sellers, T. A.
Dietary assessment of older Iowa women with a food frequency questionnaire:nutrient intake, reproducibility, and comparison with 24-hour dietary recall in-
terviews. Am. J. Epidemiol.. 136: 192-200, 1992.
24. Cox, D. R. Regression models and life-tables. J. R. Stat. Soc. Ser. B, 34:187-220, 1972.
25. Willett, W. C. Nutritional Epidemiology. New York: Oxford University
Press, 1990.
26. Pritchard, R. S., Baron, J. A., and Gerhardsson de Verdier. M. Dietary
calcium, vitamin D, and the risk of colorectal cancer in Stockholm, Sweden.Cancer Epidemiol. Biomark. Prey., 5: 897-900, 1996.
27. Bostick, R. M., Fosdick, L., Wood, J. R., Grambsch, P., Grandits, G. A.,
Lillemoe, T. J., Louis, T. A., and Potter, J. D. Calcium and colorectal epithelial
cell proliferation in sporadic adenoma patients: a randomized, double-blinded,
placebo-controlled clinical trial. J. NatI. Cancer Inst., 87: 1307-1315. 1995.
28. Baron, J. A., Tosteson, T. D.. Wargovich, M. J., Sandier, R., Mandel, J.,Bond, J., Haile, R.. Summers, R., van Stolk, R., Rothstein, R., and Weiss, J.Calcium supplementation and rectal mucosal proliferation: a randomized con-
trolled trial. J. NatI. Cancer Inst., 87: 1303-1307, 1995.
29. Cats, A., Kleibeuker, H., van der Meer, R., Kuipers, F., Sluiter. W. J..
Hardonk, M. J.. Oremus. E. T., Mulder, N. H., and de Vries, E. 0. Randomized,double-blinded, placebo-controlled intervention study with supplemental calcium
in families with hereditary nonpolyposis colorectal cancer. J. NatI. Cancer Inst..87: 598-603, 1995.
30. Potter, J. D. Nutrition and colorectal cancer. Cancer Causes Control, 7:
127-146, 1996.
on November 29, 2018. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1998;7:221-225. Cancer Epidemiol Biomarkers Prev W Zheng, K E Anderson, L H Kushi, et al. among postmenopausal women.other micronutrients in relation to incidence of rectal cancer A prospective cohort study of intake of calcium, vitamin D, and
Updated version
http://cebp.aacrjournals.org/content/7/3/221
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/7/3/221To request permission to re-use all or part of this article, use this link
on November 29, 2018. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from