a manual therapy and exercise approach to breast cancer
TRANSCRIPT

2014 Annual Breast Cancer Rehabilitation
Healthcare Provider Event
A Manual Therapy and Exercise Approach to Breast Cancer Rehabilitation Course
November 7th and 8th, 2014
Mercer University, Atlanta, GA
Sponsored By:
TurningPoint’s Edith Van Riper-Haase Breast Cancer
Rehabiltation Advocacy Fund
thevisualab.com
Presentations are
Available on TurningPoint’s Website:
myturningpoint.org
Click on Course Link
www.oncologypt.org itsthejourney.org

A Manual Therapy and Exercise Approach to Breast Cancer Rehabilitation Course
Lymphedema:
Physiology, Risk Factors and Early Detection
Cathy Furbish, PT, DPT, CLT
This Presentation is available on TurningPoint’s Website:
myturningpoint.org
From Homepage Click on Course Link

Lymphedema is Likely
the Most Feared
Survivorship Issue…

What is the Lymphatic System?

The Lymphatic System The lymphatic system is a
complex network of lymphoid organs (thymus, tonsils, spleen),lymph nodes, lymph ducts, lymphatic tissues, lymph capillaries and lymph vessels
The system produces and transports lymph fluid from tissues to the circulatory system
The lymphatic system is a major component of the immune system

Interstitial Fluid / Lymph Fluid
Interstitial fluid is a clear fluid
Circulates through your tissues to cleanse them and keep them firm, and then drains away through the lymphatic system.

Purpose of the Lymphatic System
The lymph system is a one-way drainage route designed to rid the tissues of unwanted material and excess fluid.
An essential function of the system is to transport proteins too large to re-enter the blood vessels directly.

Functions of the Lymphatic System Components
Lymph Formation
initial lymphatics
Lymph Transport
lymph collectors – superficial / deep
Lymph Concentration and Filtration
lymph nodes

Microcirculation / Lymph Formation

Lymph Transport

Lymphatic Anatomy


Lymphangion Subject to stretch reflex
Filling triggers contraction
Longitudinal muscle opens valve
Turbulence passively closes valve on relaxation
Responds to internal and external pressure changes

LymphangionRate of contraction affected by
External forces (pressure changes)
Respiration
Movement
Arterial pulsation
Internal forces
Filling of lymphangion
Greater volume of fluid transported = faster rate of contraction
Under influence of autonomic nervous system

Lymph Vessels Lymph vessels collect lymph fluid and carry it to
the lymph node
Series of lymphangia make up the lymph vessel Lymphatic vessels (lymphatics) start in the
superficial fatty tissue Become progressively larger closer to the trunk
and are located near the veins. Lymphatic vessels resemble veins in structure
except that lymphatics: have thinner walls. contain more valves to prevent retrograde flow
(‘backflow’) have well developed muscular walls contain lymph nodes located at certain intervals along
their course.

Deep lymphatic system Within the body the
lymphatic vessels (lymphatics) become progressively larger
Lymphatics are located near the veins.


Lymph System Lymph pumps (lymphangions) are able to accommodate
their activity to the lymphatic load (need)
Highest possible lymphatic output = “transport capacity”
Lymph collects at the cisterna chyli and fluid travels up the main lymph trunk into the venous system
Each day approximately 2L of lymph fluid (containing essential proteins and immune cells) empties into the blood circulation

Lymph NodesFiltration and Concentration
Vary in size between .2 to 3.0 cm
600-700 in adult
Grouped in clusters or chains along the lymph collectors
Do not regenerate
Arranged sequentially along lymph path Function is to filter out and trap bacteria,
viruses, cancer cells, and other unwanted substances, and to make sure they are safely eliminated from the body.
Reabsorb ~ 40% of H2O from lymph fluid and returns it to the venous system
Store Inert Particles

Lymph NodesImmune Function
Debris and Bacteria are then phagocytosed by immune cells such as macrophages
Cancer cells are attacked by specific cellular elements like T-cells

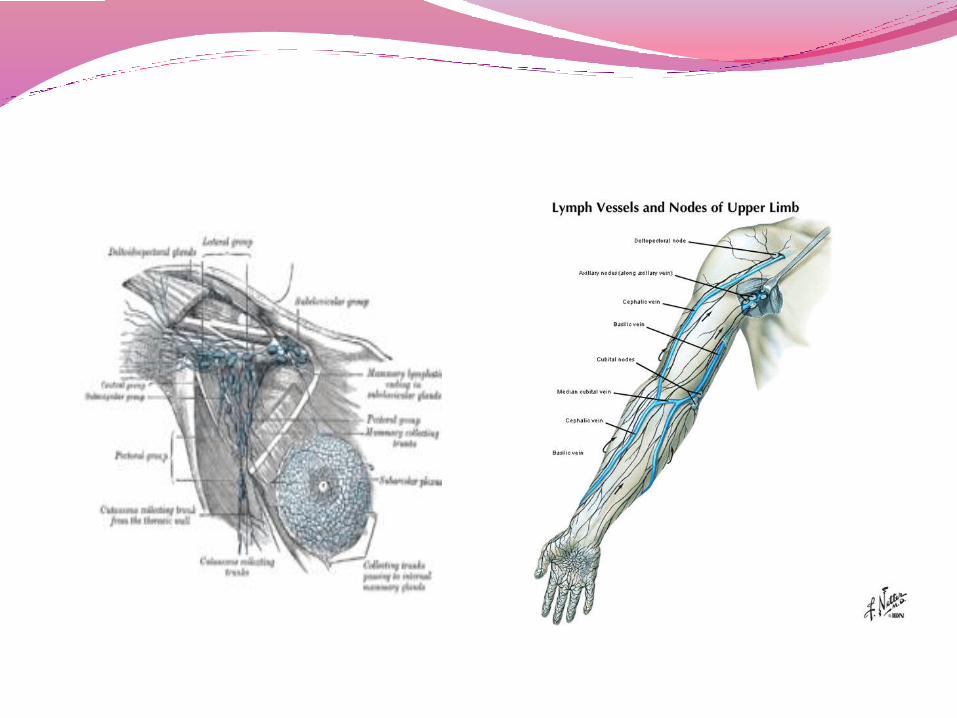
Axillary Lymph Nodes
Located between pectoral and latissimus muscles on the thorax
20-30 per side

Node (Cluster) Placement Head and neck
Supraclavicular fossae
Axillae
Medial cubital fossae
Inguinal fossae
Popliteal fossae
Lumbosacral
About 600 in body
About 160 in head & neck

Direction Of Lymph Flow

Lymphatic Anastomoses

Upper extremity lymphatics

What is Lymphedema?

Lymphedema
Lymphedema is the result of damaged or blocked lymphatic vessels caused by surgery, radiation therapy, injury, limb paralysis, infection, or an inflammatory condition.
Surgery combined with radiation therapy for breast cancer is the most common cause of arm lymphedema for women in the United States

Lymphedema If lymph flow is disrupted, protein rich fluid accumulates
in the tissues
The ground substance (interstitium) swells
As in any chronic inflammatory process:
Monocytes migrate into the area
Monocytes develop into macrophages and multiply
Macrophages produce cytokines
Cytokines induce fibroblasts and proliferate
This increases formation of connective tissue
Some fibroblasts develop into adipose tissue

Lymphedema may be acute or chronic, transient or progressive.
Most often it is seen in the clinic as a chronic, progressive condition. If left untreated it may evolve into a permanent disfiguring condition which is manageable but irreversible.

LymphedemaLymphedema while most commonly found in the arm, may also occur in the trunk, abdomen or breast, resulting from poor or abnormal flow of lymph from tissues to the blood circulation.

Incidence of lymphedema?

Incidence of Lymphedema Estimates of the incidence of lymphedema following
breast surgery varies from 6 to 30%
Improvements in surgical and radiation therapy techniques have reduced the prevalence to around 20%
Hayes, 2012
Petrek JA, 2001

Incidence of Lymphedema survey of 1,151 women treated with surgery and
post-op radiation for breast cancer
23% of subjects reported lymphedema in the first 2 years post treatment
45% reported lymphedema by 15 or more years post treatment.
Erickson VS et al: J Natl Cancer Inst 93(2) 96-111 (2001)

Onset is not usually immediate, but typically 6 months to 3 years post treatment
77% of women who develop lymphedema have onset within 3 yrs post surgery
The remaining women developed lymphedema at a rate of almost 1% per year
Petrek JA et al. Cancer 2001 Sep;92(6):1368-77
Typical Time for Onset of Lymphedema

How can the transport capacity of the lymph system be
affected in breast cancer ?

Normal Lymph Function
TIME
VOLUME
Functional Reserve = Safety Valve Function
Capacity is 10 x normal volume in healthy person
Normal Volume of Lymph Fluid Leaving Upper Extremity
Transport Capacity = Maximal Volume of Lymph Fluid Normal System Can Deal With

Lymph System Compromised
TIME
VOLUME
Functional Reserve Decreased = Safety Valve Lower
Normal Volume Lymph Fluid Leaving Upper Extremity
Normal Transport Capacity
Gradually Reduced Transport Capacity After Breast Cancer

Lymph System Insufficiency
TIME
VOLUME
Visible Swelling
•Volume of Lymph Fluid Increases Beyond Reserve Capacity
•Due to Increased Arterial Flow from Infection, Inflammation, Burn AND/ORDecreasing Transport Capacity
Gradually Reduced Transport Capacity After Breast Cancer

Treatment Factors The most important factor that predisposes a patient to
the occurrence of lymphedema is axillary lymph node dissection
The incidence of lymphedema increases with the number of nodes removed

Determination of Axillary Node
Status
Axillary Node Dissection
10 – 30 nodes removed usually through same incision as mastectomy, separate incision for lumpectomy
pathological examination to determine if cancer cells
Sentinel Node Biopsy
Less invasive determination of axillary node status

Sentinel Node Biopsy
Radioactive tracer +/- blue dye injected into tumor
Wait 45 min – 6 hours
Scan or Geiger counter to determine location of ‘sentinel node(s)’
Small incision to remove SN
If positive, further axillary node dissection
If negative, assume all nodes are negative and avoid further node removal

Radiation and Lymphedema Radiation therapy delays normal growth of
lymphatics into tissues repairing after surgery and inhibits normal lymphatic proliferative response to inflammation
Lymph node fibrosis occurs with radiation and decreases the filtering function of the nodes which deters the immune response
Radiation therapy blocks or compresses lymph vessels through radiation fibrosis
Herd-Smith et al: Cancer 92(7) 1783-1787, 2001

Radiation Therapy
Radiation therapy improves survival for women with breast cancer whether treated with a lumpectomy or mastectomy.

Treatment Factors
Lymphedema is found to only have a prevalence of 6 % in women who do not receive radiation therapy.
Herd-Smith et al: Cancer 92(7) 1783-1787, 2001

Development of arm lymphedema after breast surgery is a function of Extent of axillary node
removal(0-18%)
Radiation therapy (9-44%)
Herd-Smith et al: Cancer 92(7) 1783-1787, 2001
Treatment Factors

Patient Factors
Increased Body Mass Index (BMI)
increases the incidence of lymphedema
Ozaslan C et al: Am J. Surg. 187; 1069-72, 2004

Patient Factors: Ethnicity 494 women: 271 White and 223 Black with
DCIS –Stage III-A breast cancer
Circumferential measures for 50 months following diagnosis
Factors associated with breast cancer
Younger age of onset
Obesity
More than 10 lymph nodes removed
Black women had a higher prevalence of lymphedema (28% vs. 21%) race as an independent variable was not associated with lymphedema

Patient FactorsPatient factors that are unrelated to the development of lymphedema:
Age
Drug/chemotherapy
Menopausal status
Pathological status/tumor size
Medical co-morbidities such as DM, CHF, hypertension and autoimmune diseases
Vocation/Avocation

Predictors of Lymphedema after Breast Cancer Surgery
Assessed 94 patients with lymphedema and 94 controls without lymphedema
Patients with lymphedema :
BMI over 25,
axillary radiation
more nodes removed than controls
Swenson KK et al: Oncol Nurs Forum. 36 (185-93 (2009

Risk Factors:
Radiation
Axillary Node Dissection
Petrek analyzed 15 other potential predictive factors and
only 2 were statistically significantly associated in
lymphedema:
Arm infection/injury Weight gain since operation
Herd-Smith et al: Cancer 92(7) 1783, 2001 ; Petrek JA et al. Cancer Sep;92(6):1368, 2001.
Lymphedema Risk Factors

Predictors of Lymphedema after Breast Cancer Surgery Axillary Node Dissection
Odds of swelling increases by 4% for every node removed
Axillary Radiation * Arm infection/injury Weight gain since surgery
Petrek JA et al, 2001; Paskett et al, 2007
Gur A et al 2009

Risk of Developing Lymphedemaa Meta-Analysis
Articles 1950-2008
Excluded articles without a control group
Lymphedema measured by circumference, water displacement, impedance, self-report
Treatment factors included type of surgery, extent of lymph node dissection, radiation therapy, chemotherapy, presence of positive nodes
Tsai, R et al: Ann Surg Oncol Apr.14, 2009

Risk of Developing Lymphedemaa Meta-AnalysisSUMMARY: Mastectomy increased risk of lymphedema compared with lumpectomy.
AXILLARY DISSECTION HAS MORE THAN A 3-fold INCREASED RISK COMPARED WITH NO DISSECTION. AND compared with SNB risk was similar.
Overall subjects who had received any radiation were at significantly increased risk of developing lymphedema. Among subjects that rec’d RT, those who had the axilla radiated had increased risk for developing lymphedema
There was NO association between chemotherapy and lymphedemaTsai, R et al: Ann Surg Oncol Apr.14, 2009

How can risk of getting lymphedema be reduced?

Myths and Realities
“ The inability to identify reliably the factors that cause lymphedema fosters fear and frustration in patients with breast cancer.”
American Cancer Society Lymphedema Workshop 1998

Myths and Realities
“Many of the patient education materials in current use continue to promulgate behaviors and modifications emanating from an unsubstantiated, empirically derived conception of the physical forces that govern the progression of lymphedema.”
Rockson, S. Cancer 83:2814-2816, 1998

Clinical Factors “ ‘ Do’s and Don'ts’ have not changed
appreciably in several generations of cancer therapy and unfortunately, few objective data have been accumulated to validate the recommendations.”
Rockson, S.Cancer 83:2814-2816, 1998

The Origin of Lymphedema “DO’s and DON’T”sNelson,P: Geriatrics 21:62 1966
Avoid cuts, scratches, pinpricks, hangnails
Do not dig in the garden or work with thorny plants
Do not reach into a hot oven Do not permit injections,
blood specimens or blood pressure readings in your arm
Wear rubber gloves when washing dishes or cleaning house
Use a thimble when sewing Apply lanolin based hand
cream frequently Contact your doctor if your
arm appears red, warm or swollen

The Myths That Women were Told about Lymphedema…
2010 American Cancer Society Website: “Avoid vigorous, repeated activities, heavy lifting, or pulling. Use your unaffected arm or both arms as much as possible to carry heavy packages, groceries, handbags, or children.”
Don’t do overhead activities
Don’t lift over 5 pounds
Don’t weight train
Avoid air travel

Risk Reduction Strategies? Many primary prevention strategies make sense- avoid
sunburn, infection, trauma
Other strategies such as avoidance of exercise and repetitive UE use may have potentially negative consequences
Exercise may reduce risk of recurrence
Clinical trials suggest that exercise may protect against lymphedema
Quality of life

Lymphedema and Air Travel
Air travel is thought to contribute to lymphedema due to the lowered cabin pressure exerting less atmospheric pressure on the limb.
The addition of minimal movement while sitting in cramped seats may decrease the muscle pump contributing to the obstruction of lymphatic drainage

Lymphedema and Air Travel There are only four published studies on air travel and
lymphedema
One study by Ward is a single case study that examines the impact of multiple flights (21) over a years period of time. The subject a breast cancer survivor with established lymphedema performed self-impedance measures before and after flights. The impedance measures fluctuated over time and gradually worsened Ward L et al Lymphology 42 (3) 139-145, 2009
Graham reported in a retrospective study of 287 breast cancer survivors that there were no cases of permanent new or permanent increased swelling after flying and nine cases of temporary swelling Graham PH Breast 11, 66-71 (2002)

Lymphedema and Air Travel
A study on air travel and the appearance or exacerbation of lymphedema.
The study was a retrospective, self-report questionnaire that indicated that 5% of women who traveled developed arm lymphedema. 27 of 490 women
Casley-Smith J. Aviat Space Environ Med(67) 52-6 (1996)

Air Travel and lymphedema 72 “at risk” women 60 from Canada and 12 from Australia
attending a dragon boat race in Australia. (5 women or 7% had lymphedema at the onset)
Measured 2 weeks before flight and 6 weeks after flight using a bioimpedance device
95% of the women had no change in impedance measures indicating air travel did not cause increase in extracellular fluid.
Worsening of lymphedema in 2 of the 5 women with pre-existing lymphedema and 2 new cases (all from Canada)

Air Travel and lymphedema Overall the number of studies is low
The incidence of lymphedema associated with air travel is low
The majority of women who got lymphedema had axillary dissection, took long haul flights
Each woman at risk for lymphedema must be evaluated individually. The relative risk for getting lymphedema with air travel is low; however, the patient’s extent of treatment, whether or not they had axillary radiation, number of nodes removed, BMI, length of flight should be taken into consideration
The prophylactic wearing of a compression garment for women without lymphedema is unlikely to be advantageous. (Graham found an increased swelling with prophylactic sleeve on short flights)

Lymph System Insufficiency
Surgery and radiation may decrease the lymph flow capacity of the upper extremity, the axilla is like a kink in a garden hose
Triggers that increase fluid volume in arm may act as triggers to lymphedema: infection inflammation heat decreased atmospheric pressure
Fluid volume that exceeds maximal capacity results in visible swelling

Reducing Risk of Lymphedema…Truths
Early Physical Therapy
Exercise – aerobic and strength to maximize lymph flow
Avoid infection
Avoid inflammation
Avoid excessive weight gain

Managing/Preventing lymphedema
Weight loss, whether through reduced calorie intake or increased exercisedemonstrated that weight loss reduced lymphedema volumes regardless of the method used to achieve wt loss.
Shaw,C et al: Cancer 28 (2007)

MYTH: Exercise Causes Lymphedema
REALITY
Exercise encourages skeletal muscle contraction to help pump lymph and promote drainage

Lymphedema and Exercise
No form of physical activity has been associated with lymphedema in the literature.
Harris (2000) dragon boat paddling
Ahmed (2006) weight training
Cheema (2006) weight training
Courneya (2007) aerobic exercise
Lane (2005) resistance training & dragon boat paddling
McKenzie (2003) resistance training and arm ergometer

Weight Training and Exercise for Women with
Lymphedema: Randomized Controlled Trial
Women with unilateral stable lymphedema
Groups balanced for potential confounding factors, such as age, surgical history, radiation,
obesity, etc.
•2x/wk x 90 min x 1 year
•Community YMCA
•Supervised x 13 weeks
•Progressed weight when 10 reps achieved
•No upper limit on weight
Weight Training Group
(n=71)
• Instructed to maintain current fitness activitiesControl Group
(n=71)
Schmitz , 2009
REALITY

Results:
No significant difference in arm or hand swelling at 1 year
Decreased number of flare-ups of lymphedema in weight lifting group
Decreased number and severity of symptoms in weight lifting group
Significant increase in upper and lower body strength in weight lifting group
No upper limit for amount of weight

Early Physical Therapy Decreases Risk of Lymphedema in Women with Breast CancerLocomba, MT et al. , British Medical Journal, February, 2010
Results: 1. At 12 month follow -up the incidence of lymphedema was significantly lower in the physical therapy group at 7% (4 women) compared to 25% in the control group (14 women)2. Women in the control group developed lymphedema more quickly after surgery3. The study is the first demonstrate the relationship between axillary cording and subsequent development of lymphedema.

Reducing Our Risk of Lymphedema: Summary of the Scientific Evidence
Approach should be based on individual risk of lymphedema Education re: early signs and symptoms of lymphedema to
facilitate early intervention Baseline measures of upper extremity volume (ideally pre-op) to
allow early detection (Gergich, 2008)
Lifestyle Advice: Exercise Regularly- include stretching, strengthening and aerobic activity Maintain your ideal body mass index (19 - 22)
Understand Potential Triggers Avoid injury, sprains and strains – lift within your capacity, work up weights gradually Avoid infection – gloves when gardening, extra care for cuts and burns, caution with
heat/sun Take a compression sleeve with you for long trips so that you can initiate treatment at the
first sign of swelling, including while flying

What are the signs and symptoms of lymphedema ?

Signs and symptoms of Arm or Hand Lymphedema
Feeling of tightness, fullness, tingling or heaviness
Rings, watch or bracelet becomes tight
Arm may swell during the day and diminish or disappear overnight
Decreased visibility of the veins in the back of the hand
Greater roundness or fullness of the elbow, wrist or forearm

Common Symptoms of trunk/ breast Lymphedema
Trunk
Vise-like pressure around the lower rib cage or thorax
Waistband on clothing feels tighter at the end of the day
Breast
Feeling of fullness, tenderness, pain, heat in the breast tissue
Vise-like pressure around the chest or thorax
Bra feels tighter more uncomfortable at the end of the day


Lymphedema Screening Stemmer’s Sign: Negative if you can pick up the skin on
dorsum of the first bone (proximal phalanx) of the index finger.
Knuckle Check: Make two fists. Check between knuckles for diminished space between knuckles.
Forearm Tissue (Ulnar/Radius interstitial tissue)
Boney contours of elbow
Observe Arms outstretched (Abduction)

Lymphedema



Stout Gergich, N.L., Pfalzer , N. L., McGarvey, C., Springer, B., Gerber, L. H. and Soballe, P. (2008), Preoperative assessment enables the early diagnosis and successful treatment of lymphedema. Cancer, 112: 2809–2819.
Pre-Operative Assessment of Breast Cancer Patients by Physical Therapists Improves Lymphedema Diagnosis and treatment
All study participants were monitored pre-op and at one month post-surgery and at three-month intervals thereafter for one year even if they exhibited no swelling. Using both the pre- and post-operative assessments enabled investigators to diagnose lymphedema before it became visible
The authors demonstrated the effectiveness of a surveillance program to successfully detect and treat lymphedema
detection and management of lymphedema at early stages may prevent the condition from progressing
Once lymphedema was diagnosed it was managed using a light-grade compression sleeve and gauntlet for daily wear for 4 to 6 weeks and then PRN.

2014 American Cancer Society Website Try to get to / stay at a healthy weight
Try to avoid infection
Try to avoid constriction
Exercise
Use your arm as normally as you can, once you have healed from surgery or radiation
Exercise regularly, but do not overtire your arm
Avoid vigorous, repetitive activity
Avoid heavy lifting or pulling

Summary 1. Risk factors for lymphedema are number of nodes removed and
radiation
2. Increased fluid load may trigger lymphedema, but does not CAUSE it
3. Early physical therapy may reduce lymphedema risk
4. Early identification and management is key to controlling lymphedema
5. Exercise is not only safe, but important to risk reduction and treatment of lymphedema
6. While no one wants lymphedema, we can control it
