a local approach to regional care collaborative organizations (rccos): an overview of region 7...
TRANSCRIPT

A Local Approach to Regional Care Collaborative Organizations (RCCOs):
An Overview of Region 7
Michael AllenAspenPointe Health Network
January 29, 2013

Summary
• Statewide RCCO Pilots Overview• Community Care (Region 7) Approach• Areas of Focus• Healthcare Reform• Predicting the Future• Questions

My goals – you will have…
1. Understanding of Statewide Regional Care Collaborative Organization (RCCO) concept
2. Understanding of Region 7 approach
3. Awareness of broad Healthcare Reform concepts
4. Grasp of a model for embracing Healthcare Reform

Medical Home Key Principles
• Personal Physician• Physician directed care teams• Whole person orientation• Quality and Safety• Enhanced access

Medical Home Standards
• Enhance Access/Continuity• Patients have access to culturally and linguistically appropriate
routine/urgent care and clinical advice during and after office hours • Patients may select a clinician• The focus is on team-based care with trained staff
• Identify/Manage Patient Populations• The practice collects demographic and clinical data for population
management• The practice assesses and documents patient risk factors• The practice identifies patients for proactive and point-of-care reminders

Medical Home Standards (cont.)• Plan/Manage Care
• The practice identifies patients with specific conditions, including high-risk or complex care needs and conditions related to health behaviors, mental health or substance abuse problems
• Care management emphasizes:• Pre-visit planning• Assessing patient progress toward treatment goals• Addressing patient barriers to treatment goals
• Provide Self-Care Support/Community Resources• The practice assesses patient/family self-management abilities• The practice works with patient/family to develop a self-care plan and provide
tools and resources, including community resources
• Track/Coordinate Care• The practice tracks, follows-up on and coordinates tests, referrals and care at
other facilities (e.g., hospitals)• The practice follows up with discharged patients

What are the RCCO Pilots?
Title: Regional Care Collaborative Organizations for the Accountable Care Collaborative Program
Funder: Colorado Department of Health Care Policy and Financing
Shift from a volume-driven, fee-for-service model to a coordinated outcomes-based system that will control costs in a responsible manner.
The program will not take over the management of any of the Department’s behavioral health care, which will remain with the behavioral health managed care organizations.

RCCO Goals & Objectives
Goals:
1. To improve health outcomes of Medicaid Clients through a coordinated, client/family-centered system that proactively addresses clients’ health needs
2. To control costs by reducing avoidable, duplicative, variable and inappropriate use of health care resources.
Program Objectives:
3. Expand access to comprehensive primary care.
4. Provide a focal point of care/Medical Home for all Members including coordinated and integrated access to other services.
5. Ensure a positive Member and provider experience and promote Member and provider Engagement.
6. Effectively apply an unprecedented level of statewide data and analytics functionality to support transparent, secure data-sharing and enable the near-real-time monitoring and measurement of health care costs and outcomes.

RCCO Outcome Measures
• Reduce Emergency Department Visits• Reduce Imaging• Reduce Hospital Readmissions• Reduce Costs

State Medicaid Pilot Parameters• Initial Phase: July 2011-June 2012
• Limited Pilot Area (Focus Community)• Limited Primary Care Medical Providers• 6,300 clients July 1, 2011 • 8,900 clients August 1, 2011• 17,200 clients December 1, 2011
• Expansion Phase: July 2012-June 2016• Expand to Full Pilot Area• Expand Primary Care Medical Providers• Expand to 60,000+ clients (Currently 40,000+)

No Referral Required• Emergency Care• EPSDT Screenings• Emergency and non-emergency transportation• Anesthesiology Services• Dental Services• Vision Services• Family Planning Services• Behavioral Health Services• Home and Community-Based Waiver Services as defined in the State
Plan that the Department has submitted to the Centers for Medicare and Medicaid Services
• Obstetrical Care• Primary care from a primary care physician, other than the Member’s
PCMP, if the Member’s PCMP is unavailable to see the Member

Colorado RCCO Regions

A Local Approach• Community Health Partnership is the Regional Care
Collaborative Organization (RCCO) for El Paso, Teller, Elbert and Park Counties.
• Primary partners in the RCCO pilot include:
• Contractors in the RCCO pilot include:

Community Care Medicaid Pilot• Initial Phase: July 2011-June 2012
• Primary Care Medical Providers• Peak Vista• CSHP
• Colorado Springs is Focus Community
• Expansion Phase: July 2012-June 2016• Primary Care Medical Providers
• Peak Vista, CSHP, private providers
• El Paso, Teller, Park and Elbert Counties

Primary Care Medical Providers
• Peak Vista• Mountain View Medical Group
• Colorado Community Clinic
• Dr. Charles L. Johnson• Dr. Margot A. Williams
• Prairie View Family Care• Colorado Springs Health Partners
• Rocky Mountain Health Care Services
• Summit Medical Clinic• Sunrise Health Care

Key Requirements/Expectations
A focus group of Medicaid members was conducted.
What do you care about or need (for healthcare)?• Quality care and compassion from providers at all points of access
(staff, doctor, nurse, billing, pharmacy, etc.)• A doctor who knows them and their family• Greater access to providers in a timely manner• Care coordination among providers• Better customer service from office staff; respect and accountability• Help with health education for wellness• Help navigating the system

Key Requirements/Expectations
CHP member physicians and physician practice leaders were asked what they required and expected from a RCCO:
• More efficiency in reimbursement from Medicaid • Increase in payment rates (to at least cover the cost of care)• Reduce “fragmentation” of access and scarcity in availability of
certain services. Need help in getting patients connected with the care they need.
• Improvement in patient “compliance”; i.e. follow through with provider’s instructions, showing up for appointments, etc.

Community Care Areas of Focus
• Practice Support• Care Coordination• Access to Services• Member and Provider Satisfaction
• Service Center• Responsibilities• Role of Service Coordinators

Practice Support
• Training and assistance with MedicaidMedicaid Provider ApplicationMedicaid policies and proceduresMember eligibility and enrollmentBenefit informationClaims and billingOther aspects being a Medicaid provider
• Newsletters• Website links & information• Orientation for new providers• Personal provider visits, building relationships & identifying support needs

Practice Support
Provide resources and support for the following:
Clinical Tools• Huddles• Workflow Assessment• Registry• Team Based Care• Best Practices
Client Materials• Community Care Basic Resource Directory

Practice Support
Operational Practice SupportModel for ImprovementAIM Statement WorksheetPDSA WorksheetConducting Effective MeetingsWorkflow AssessmentDemand and CapacityPhone Demand and TackingAppointment DemandLEAN ToolsPatient Cycle Times

Care Coordination Goals
Improve health outcomes of Medicaid members through a coordinated, client/family-centered system that proactively addresses clients’ health
Control costs by reducing avoidable, duplicative, variable and inappropriate use of health care resources

Care Coordination Model
The coordinated, client/family-centered system of care is provided through the PCMP who delivers the majority of comprehensive primary, preventative, and sick medical care in accordance with medical home principals:
• Site specific care coordination• Case management• Best practices• Practice support – tools and resources• Referrals to non-PCMP providers• Disease Management

Care Coordination Overview
• Patient Navigation• Case Management• Disease Management

Patient Navigation
Patient navigation is a process by which an individual – a patient navigator – guides patients through their care and around barriers.
Barriers to quality care that may be addressed by the patient navigator include:
EconomicLanguage & cultureCommunicationHealth care systemTransportationBias based on culture/race/ageFear

Role of Patient Navigator• Link between the member & access to community resource helping
overcome social & economic barriers to care
• Observe the living environment, assessing additional needs, and offering support to the patient
• Helping members understand and access what services are available; including public assistance, housing, nutrition, and child care
• Work closely with providers, the care team, and health educators
providing clients with resources improving health outcomes and increase the client’s ability managing health issues effectively
~ All patients are eligible for patient navigation ~

Case Management
Case management is provided for clients who require extensive use of resources and/or who may require help navigating the system to facilitate appropriate delivery of care and services.
Clients are selected for case management when a high-risk criterion is present (but not limited to the following):• Low functional status or cognitive deficit• Mental illness or substance use disorder• Repeated emergency department visits and/or hospitalization• History of traumatic brain injury or stroke• Psychosocial concerns

Case Management (cont.)
Role of Case ManagerConduct assessment of client’s health and psychosocial needs
(including health literacy status and deficits)
Planning with client, family, or caregiver to maximize health care responses, quality, and cost-effectiveness
Facilitate communication and coordination between members of the health care team
Educate client, family, or caregiver and care team about treatment options, community resources, psychosocial concerns

Disease Management
Disease Management is a system of coordinated health care interventions and communications for populations with conditions in which patient self-care efforts are significant.
Clients are selected for disease management when one of the following chronic conditions is present:• Asthma• Diabetes• Cardiovascular Disease• Depression
Evidence-based Clinical Guidelines are followed for Disease Management
Member Access to Services
• MOU with PCMPs defines access & availability requirements
• Monitoring will be done using: “Secret Shoppers”Patient Satisfaction SurveysFocus GroupsGrievance Tracking

Assessing Member and Provider Satisfaction
• Performance Improvement Advisory Committee
• Member Satisfaction Surveys
• Provider Satisfaction Surveys

Service Center Description• A “one-stop-shop” Service Center with a dedicated
helpline/call center (toll-free number)
• Staffed by Service Center Coordinators who are trained in customer service
• Representatives available 8am-5pm, Monday – Friday

Service Center (cont.)
Overall responsibilities:
Provider network management; maintain adequate provider network (PCMPs and
specialists), ensure access, provider recruitment, training and support
Manage Complaint, Grievance and Appeal processes
Communication with members and providers; member handbook; content for website; provider directory, member letters, provider surveys
Educate providers on the RCCO, its role in the Colorado Medicaid system, SDAC, enrollment broker, UM contractor, etc.
Linkage with community partners
Data management; maintenance of IT system, import and export data from SDAC and other Medicaid partners; data queries, reporting and analysis

Service Center (cont.)
Role of Service Coordinators
Member assistance with choice of PCMP
Provide education to PCMPs on referral process
Support PCMP in finding specialist or other provider in Network
Troubleshoot issues or problems for members or providers
Assistance navigating health care system including barriers to care
Member advocacy including access to Medicaid Ombudsman
Support member use of the Medicaid 24-hour Nurse Advice Line

Service Center (cont.)
Role of Service Coordinators
Maintain directory of community resources
Coordinate care members receive in other RCCOs
Collaborate with behavioral health organizations and other community providers
Assist PCMP in care coordination not provided in practice setting
Assist providers with Colorado Medicaid eligibility, enrollment, benefit packages, UM, claims and billing, etc.
Collect and enter data not contained in Medicaid claims
Record member disenrollment

How Are We Doing?

Enrollment by Eligibility TypeJanuary 2013 RCCO 7 Roster, by Eligibility Type
Eligibility Description December December January JanuaryCategory Roster Roster Roster Roster
Member Percentage Member PercentageCount of Total Count of Total
Unknown No Category Listed 1,007 2.8% 356 0.9%AFDC/CWPA Aid to Families Dep. Child - Adult 12,223 33.5% 12,259 32.0%AFDC/CWPC Aid to Families Dep. Child - Child 13,549 37.1% 15,748 41.1%AND/AB-SSI Aid to Needy, Disabled, and Blind 3,670 10.1% 3,733 9.7%AWDC Adults without Dep. Children 1,226 3.4% 1,150 3.0%BC CHLD Baby Care Children 2,257 6.2% 2,392 6.2%BC WOMEN Baby Care Mother 330 0.9% 342 0.9%BUYIN CBWD Buy-in: Children with Disabilities 4 0.0% 4 0.0%BUYIN WAWD Buy-in: Working Adult Disabled 4 0.0% 7 0.0%CHP PLUS Child Health Plan Plus 105 0.3% 148 0.4%FOST Care Foster Care 1,471 4.0% 1,533 4.0%LI PRENATL Prenatal State Only 1 0.0% 1 0.0%NCRA Non-Citizen Refugee Assistance 0 0.0% 0 0.0%OAP-A 65 years or older 286 0.8% 291 0.8%OAP-B-SSI 60-64 years old 349 1.0% 367 1.0%OAP-STATE Old Age Pension 13 0.0% 9 0.0%QI Qualified Insured 1 0.0% 1 0.0%QMB ONLY Qualified Medicare Beneficiary 10 0.0% 10 0.0%SLMB Specified Low-Income Medicare Beneficiaries 1 0.0% 1 0.0%Grand Total: 36,507 100.0% 38,352 100.0%

20,525
18,892
Adults vs. Children
Adults
Children

Capitation Count
Jul 11
Aug 11
Sep 11
Oct 11
Nov 11
Dec 11
Jan 12
Feb 12
Mar 12
Apr 12
May 12
Jun 12
Jul 12
Aug 12
Sep 12
Oct 12
Nov 12
Dec 12
0 5,000 10,000 15,000 20,000 25,000 30,000 35,000 40,000
6,226
7,422
7,713
8,154
8,580
13,499
16,827
17,788
18,293
19,097
18,700
19,432
21,494
20,946
21,594
24,881
31,110
34,740

Service Center Calls & Contacts
Mar-2012
Apr-2012
May-2012
Jun-2012
Jul-2012
Aug-2012
Sep-2012
Oct-2012
Nov-2012
Dec-2012
0 50 100 150 200 250 300 350 400 450
245
129
95
422
383
388
238
288
213
308
Inbound Calls

Dashboard Overview

Key Performance Indicators
-35.0% -30.0% -25.0% -20.0% -15.0% -10.0% -5.0% 0.0%
-10.3%
-16.5%
-14.1%
-31.4%
-30.8%
30 Day Readmits
July 2011-Aug 2012
July 2011-July 2012
July 2011-June 2012
July 2011-May 2012
July 2011-Apr 2012
-16.0% -14.0% -12.0% -10.0% -8.0% -6.0% -4.0% -2.0% 0.0%
-15.0%
-11.4%
-13.9%
-1.6%
-9.4%
High Cost Imaging
July 2011-Aug 2012
July 2011-July 2012
July 2011-June 2012
July 2011-May 2012
July 2011-Apr 2012

Key Performance Indicators
0.0% 5.0% 10.0% 15.0% 20.0% 25.0% 30.0% 35.0%
20.9%
28.1%
26.0%
33.2%
31.9%
Emergency Room Visits
July 2011-Aug 2012
July 2011-July 2012
July 2011-June 2012
July 2011-May 2012
July 2011-Apr 2012

Population Risk Data
Through October 25,710 Members
Through November 32,177 Members
Through October 25,710 Members
Through November 32,177 Members
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
51.58% 54.95%
8.64% 11.30%
4.69%3.80%
8.65% 7.51%
8.03%10.08%
4.19%6.49%
10.01%9.03%
7.67%8.30%
14.09%12.34%
19.50%18.74%
10.72% 9.04%
41.01%38.25%
0.89% 0.75%
10.35% 9.41%
Risk Group Percentage vs. Total Cost Percentage
6 - Malignancies & Catastrophic
5.5 - Dominant Chronic
5.0 - Moderate Chronic
4 - Minor Chronic
3 - Significant Acute
2 - Pregnancy/Delivery
1 - Healthy & Non Users

Healthcare Reform

The Basics
• The Move Towards Health Reform Started Before The ACA Was Passed in Washington• The cost of health care was going up at a rate that
cannot be sustained• The number of uninsured was rising at a rapid rate• Health outcomes were not what they should be• The delivery of care was fragmented• Payment to providers not aligned to do the right things

The “Triple Aim”
IMPROVED POPULATION HEALTH
IMPROVED PATIENT
EXPERIENCE
DECREASED PER CAPITA COSTS
Highly Integrated Delivery System
Risk-adjusted, Performance-based Global
Payments
Fully Engaged, Informed, and Empowered Consumers and
Businesses Partners
Access to Timely,
Accurate Data

Some Things Happening Now…
• Consumer driven care/consumer involvement• More people will have coverage• Integrated Care: Healthcare Homes• Regionalization of Healthcare delivery
• Medical Neighborhoods• Accountable Care Organizations
• Data and research-driven solutions• Payment Reform
• Pay for better health outcomes not amount of services• Resurgence of managed care and other payment methodologies
• Technology-driven healthcare is increasing at a rapid rate• Health Information Exchange• Health Information Technology

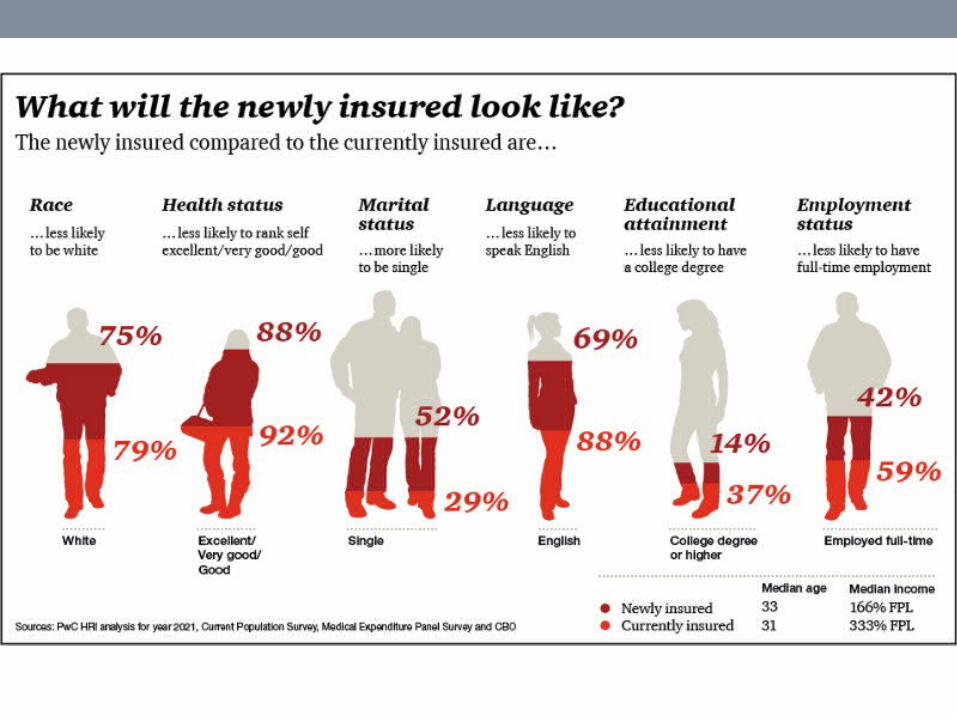
Healthcare Coverage
• Expansion of Medicaid• Creates Health Insurance Exchanges (HIX)• Plans are expanding into new markets and getting bigger• The number of uninsured in Colorado will drop from 800,000
to less than 200,000• Benefits are not determined yet, but parity will be a factor

Who Will Have Health Coverage in July 2014?% Gross Yearly Income
Family Size
25% 50% 75% 81% 100% 133% 175% 200% 250% 300%
1 $2,793 $5,585 $8,378 $9,048 $11,170 $14,856 $19,548 $22,340 $27,925 $33,510
2 $3,783 $7,565 $11,348 $12,255 $15,130 $20,123 $26,478 $30,260 $37,825 $45,390
3 $4,773 $9,545 $14,318 $15,463 $19,090 $25,390 $33,408 $38,180 $47,725 $57,270
4 $5,763 $11,525 $17,288 $18,671 $23,050 $30,657 $40,338 $46,100 $57,625 $69,150
5 $6,753 $13,505 $20,258 $21,878 $27,010 $35,923 $47,268 $54,020 $67,525 $81,030
6 $7,743 $15,485 $23,228 $25,086 $30,970 $41,190 $54,198 $61,940 $77,425 $92,910
7 $8,733 $17,465 $26,198 $28,293 $34,930 $46,457 $61,128 $69,860 $87,325 $104,79
8 $9,723 $19,445 $29,168 $31,501 $38,890 $51,724 $68,058 $77,780 $97,225 $116,67

Who Needs to Integrate Care?
• Various “Health” Systems• Substance Use Disorder/Mental Health• Physical Health• Criminal Justice• Public Health• Human/Social Services• Hospitals
• Think beyond our usual borders• Align and become comfortable with unusual partners• Think big and beyond ourselves• Health Homes and Medical Neighborhoods (ACO)

Integration Must Balance Four Areas
Integrated Delivery System
CLINICAL
FINANCIAL
DATA
OPERATIONAL

Some Broad Definitions
• Clinical: Types of services that work and show evidence of health improvement in each setting: (E.g. screening, assessment, prevention, treatment, recovery)
• Operational: How the work is carried out functionally at the location: (E.g. practice design, policies, rules and regulations, health records, collaboration with other entities, health exchange, tele-health, staff and patient interface, and facilities)
• Financial: What benefits are covered, understanding cost, payment models, partnerships, getting paid to do the right thing!
• Data: Both business and patient outcomes, knowing what are the right things to measure, how you are going to measure it, implementation, and use of information.

Value Creation
› Have we improved the quality of care and health status of populations being served through redesigning our clinical processes, utilizing best practices and measuring outcomes?
› Have we improved service to customers by providing choices and partnerships in clinical decisions?
› Have we improved access to care and services and encouraged the delivery of the most appropriate care at the most appropriate time at the most appropriate site?
› Have we reduced unit costs by redesigning core business processes and improving operating efficiencies across the delivery system?

Considerations for Health Policy
• Focus on the overall health care needs of Consumers and Their Families
• Promote population Health,
• Reduce Disparities, and Address Chronic Illness
• Standardize Quality and Outcome Measures for Use in Research and Practice
• Use Data Driven Decision Making,
• Promote Collaboration and Co-location
• Redesign Financing, the Regulatory Environment and Contracting Methods

Considerations (continued)• Invest in Training and communication
• Workforce Development
• Use of technology to deliver services
• Health Information Exchange (between providers and consumers)
• Benefit acquisition
• Screening, patient education, prevention and early intervention
• Focus on providing care that has the highest probability of best outcomes
• Right Place, Right Time, Right Service, Right Cost

Current Areas to Consider• The legislature will decide this year on Medicaid Expansion• The Exchange Board will be determining coverage for behavioral health
• The state is working on changes to rules and regulations to streamline, and hopefully address integrated care.
• The State is currently preparing for payment reform demonstration(s) to model integrated care.
• The State is waiting to hear on the SIM Grant that has a priority of integrating physical and behavioral health.
• All Payer Claims Data Base• What can you do to help Colorado and your organization to get ready for the future?

Healthcare Reform
Prepared by Dale Jarvis and Associates for the National Council, May 19, 2011

Predicting the Future…
• New models for care coordination for high-cost patients
• Increasing Medicaid rolls• More localized health care• Industry consolidation• Reduced hospital readmissions• Pay-for-performance and other financing realignments

A Model for Readiness
EducationHow will
Healthcare Reform change What we do and How we do it?
Readiness Assessment
What Gaps exist between What Is and Where We
Need to Be?
Planning & Design
What are our Redesign Priorities/Strategic
Initiatives (Who, What, When)?
Internal Work Using Rapid
Cycle Improvement (RCI) Project
Methods
Evaluation Are we
achieving our desired
objectives?
Plan Do Study
What’s our Next Phase of Redesign Priorities/Strategic
Initiatives?
Yes? No?
No or “Not Quite”
Act
External Work Relationship building and
Influencing Policy Makers and
Funders
Yes
Prepared by Dale Jarvis and Associates for the National Council, May 19, 2011

Contact Information
Community Health Partnership
P.O. Box 249 Colorado Springs, CO, 80901
Street Address: 722 S. Wahsatch Street
(719) 632-5094
Community Care Service Center
Local: (719) 314-2560
Toll Free: (866) 938-5091