3.2 dr. jeffrey da sp.jp - ace inhibitor dan arb pada gagal jantung
TRANSCRIPT

ACE Inhibitors and ARBs
in Heart Failure

In the United States:
• HF incidence increases with age
• >650,000 new HF cases diagnosed annually
• >1 million hospitalizations annually
• Absolute mortality rates for HF: 50% within 5 years of diagnosis
structural or functional impairments that leads to alteration of ventricular filling or contraction
inadequate cardiac output to maintain metabolic requirements

Myocardial injury
Cardiac function
Activation of SNS, RAAS, endothelin,
AVP, inflammatory cytokines,
oxidative stress
Acute
(adaptive) Hypertrophy,
remodeling,
apoptosis

Neurohormonal model
1980s-2000s
Hemodynamic model
1950s-1980s
Reduced contractility
Pump dysfunction
Treatment:
Positive inotropic drugs
Vasodilators
Conventional drugs
Diuretics
Digitalis
Progressive remodeling &
impaired myocard function
Treatment:
Neurohormone blockers:
ACE inhibitors, ARBs
β-blockers
Conventional drugs
Diuretics
Digitalis

Jessup, M. et al. N Engl J Med 2003;348:2007-2018

Weber K. N Engl J Med 2001;345:1689-1697

GFR
Proteinuria
Aldosterone release
Glomerular sclerosis
Atherosclerosis
Vasoconstriction
Vascular hypertrophy
Endothelial dysfunction
LV hypertrophy
Fibrosis
Remodeling
Apoptosis
Stroke
DEATH
Hypertension
Heart failure
MI
Renal failure
AT1 receptors

Angiotensinogen
Angiotensin I
Angiotensin II
AT1R AT2R
Renin
ACE Non-ACE pathways ACE
inhibitor
AT1
receptor
blocker
Bradykinin
Nitric oxide
Inactive
peptides
CV protection Vasodilatation Anti fibrosis Anti growth
Vasoconstriction Proatherosclerosis Proinflammation Prothrombosis

ACE
inhibitors
Vasodilatory
effects
Plaque
stabilization
Regression of
LV hypertrophy
Regression of VSMC
proliferation
↓ Formation of
superoxide anions

Ris
k C
ontinuum
CONSENSUS
SOLVD Rx
V-HeFT II
SAVE, AIRE, TRACE
SOLVD Prevention
Class IV cardiac failure, low EF
Class II-III cardiac failure, EF <35%
Cardiac failure post-infarct ± cardiac failure,
EF<35-40%
Class I, EF <35%
Size of Population Affected
Smoking, Dyslipidemia, Hypertension, Diabetes CV Risk Factors
Vascular disease, LVEF >40% TIA Stroke
CAB
GC
PAD
Diabetes
+ 1 CV
risk
factor
Angina PCI CABG MI
EUROPA
HOPE


SOLVD Investigators N Engl J Med 1991;325:293-302
0
10
20
30
40
50
0 6 12 18 24 30 36 42 48
Placebo
Enalapril
Follow-up (months)
Mortality (%)
Risk reduction 16%
p=0.0036

Mortality 26%
Readmission for CHF 27%
Reinfarction 20%
Yancy CW, et al. Circulation 2013;128:000-000.
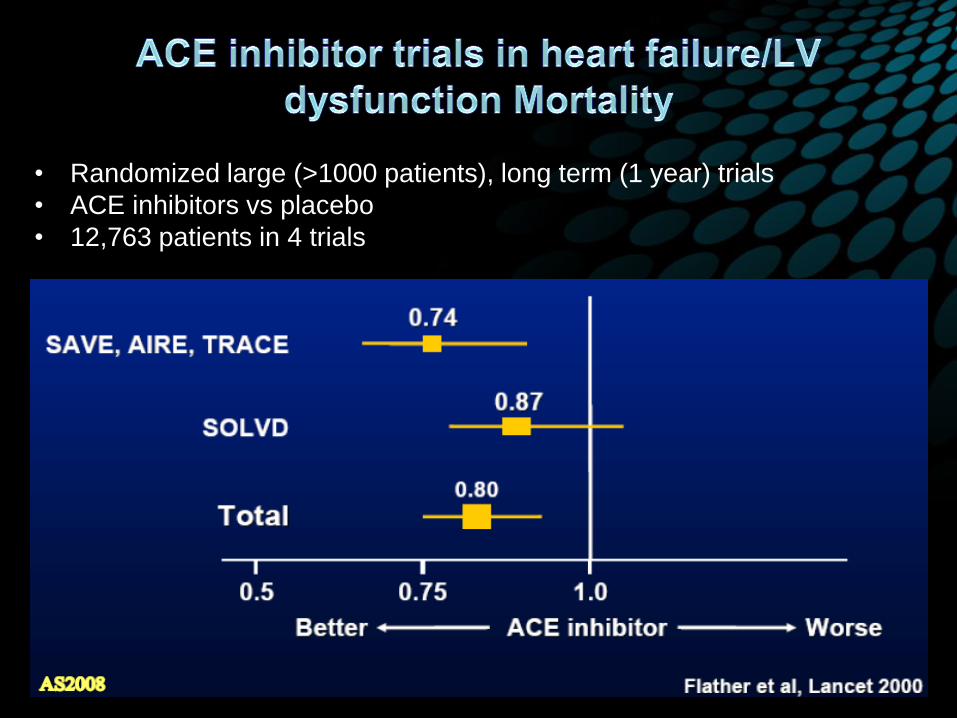
• Randomized large (>1000 patients), long term (1 year) trials
• ACE inhibitors vs placebo
• 12,763 patients in 4 trials

Randomized comparison of low dose (2.5-5mg/d) and
high dose lisinopril (32.5-35mg/d)
8% lower risk of death (p= 0.01)
15% lower risk of death or hospitalization for heart
failure (p=0.001)
greater risk of hypotension, renal insufficiency and
hyperkalemia with high dose
Packer et al. Circulation. 1999;100:2312-2318.
The Assessment of Treatment with
Lisinopril and Survival (ATLAS)

Yancy CW, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure : A Report of the American College of
Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013; 128:000-000.
McMurray JJV, et al. ESC Guidelines for
the diagnosis and treatment of acute and
chronic heart failure 2012. The Task Force
for the Diagnosis and Treatment of Acute
and Chronic Heart Failure 2012 of the
European Society of Cardiology. European
heart Journal 2012; 33:1787-1847

Adverse effects :
• Hypotension
• Hyperkalemia
• Renal dysfunction
• Dry cough
• Angioedema
ACE
inhibitors
Initial doses Target doses
Captopril
Ramipril
Trandolapril
Enalapril
Fosinopril
Lisinopril
Quinapril
Perindopril
6,25 mg t.i.d
2,5 mg o.d.
1 mg o.d.
2,5 mg b.i.d.
10 mg o.d.
2,5-5 mg o.d.
5 mg b.i.d.
2 mg o.d.
50 mg t.i.d.
10 mg o.d.
4 mg o.d.
10-20 mg
b.i.d.
40 mg o.d.
20-40 mg o.d.
20 mg b.i.d.
8-16 mg o.d.

ACE Inhibitor intolerant?
Angiotensin Receptor
Blockers (ARBs)
Alternative agents
Additional therapy

More complete inhibition of RAAS
Retard bradykinine degradation

• ELITE II
• OPTIMAAL
• RESOLVD
• VALHEFT
• VALIANT
• CHARM

0 100 200 300 400 500 600 700
Days of Follow-up
0.0
0.2
0.4
0.6
0.8
1.0
Pro
ba
bili
ty o
f S
urv
iva
l
Losartan (N=1578) 280 Events
Captopril (N=1574) 250 Events
Captopril/Losartan Hazard Ratio (95% C.I.):
0.88 (0.75, 1.05) P=0.16
Primary Endpoint:
All-Cause Mortality


McKelvie RS et al. Circulation. 1999;100:1056-1064.
35
30
25
20
15
10
5
0
-5
17 Weeks 43 Weeks 0 Weeks
**
End Diastolic
Volume
(mL)
Candesartan
Candesartan + enalapril
Enalapril
*
*
* P <0.01 compared with 0 weeks.
**P <0.05 compared with enalapril.


Captopril
0
0.05
0.1
0.15
0.2
0.25
0.3
0 6 12 18 24 30 36
Pro
bab
ilit
y o
f E
ven
t
Mortality by treatment
Pfeffer, McMurray, Velazquez, et al. N Engl J Med 2003;349
Months
Valsartan vs. Captopril: HR = 1.00; P = 0.982
Valsartan + Captopril vs. Captopril: HR = 0.98; P = 0.726
Valsartan
Valsartan + Captopril

CHARM Added
CHARM Preserved
3 component trials comparing candesartan to placebo in patients with symptomatic heart failure
CHARM Alternative
n=2028
LVEF 40% ACE inhibitor
intolerant
n=2548
LVEF 40% ACE inhibitor
treated
n=3025
LVEF >40% ACE inhibitor
treated/not treated
Primary outcome for Overall Programme: All-cause death
Primary outcome for each trial: CV death or CHF hospitalisation

0 1 2 3 years 0
10
20
30
40
50
Placebo
Candesartan
%
HR 0.77 (95% CI 0.67-0.89), p=0.0004
Adjusted HR 0.70, p<0.0001
3.5
406 (40.0%)
334 (33.0%)
CV mortality HR 0.85 (95% CI 0.71-1.02 Adjusted HR 0.80 (95% CI 0.66-0.97) p=0.02
MI HR 1.52 (95% CI 1.06-2.18)
Primary Outcome:
CV death or CHF hospitalization

0 1 2 3 years 0
10
20
30
40
50
Placebo
Candesartan
3.5
HR 0.85 (95% CI 0.75-0.96), p=0.011
Adjusted HR 0.85, p=0.010
483 (37.9%)
538 (42.3%)
%
CV mortality : HR 0.84 (95% CI 0.72-0.98) p=0.02 Covariate Adjusted HR p=0.021
MI : Not reported
Primary Outcome:
CV death or CHF hospitalization

0 1 2 3 years Number at risk
Candesartan 1514 1458 1377 833 182
Placebo 1509 1441 1359 824 195
3.5 0
10
20
30 Placebo
Candesartan
5
15
25
HR 0.89 (95% CI 0.77-1.03), p=0.118
Adjusted HR 0.86, p=0.051
%
366 (24.3%)
333 (22.0%)
Primary Outcome:
CV death or CHF hospitalization



Yancy CW, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure : A Report of the American College of
Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013; 128:000-000.
McMurray JJV, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012. The Task Force for the Diagnosis
and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. European heart Journal 2012; 33:1787-1847

Yancy CW, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure : A Report of the American College of
Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013; 128:000-000.
McMurray JJV, et al. ESC Guidelines
for the diagnosis and treatment of
acute and chronic heart failure 2012.
The Task Force for the Diagnosis
and Treatment of Acute and Chronic
Heart Failure 2012 of the European
Society of Cardiology.
European heart Journal 2012;
33:1787-1847

ARBs Initial doses Target doses
Candesartan
Irbesartan
Losartan
Valsartan
Telmisartan
4 mg o.d.
75-150 mg o.d.
12,5-50 mg o.d.
20-40 mg b.i.d.
40 mg o.d.
32 mg o.d.
300 mg o.d.
150 mg o.d.
160 mg b.i.d.
80 mg o.d.
Adverse effects:
• Hypotension
• Hyperkalemia
• Renal dysfunction
• More AE when
combined to
ACEIs

One strategy to manage heart failure is RAS blockade with ACE inhibitors or ARBS.
ACE inhibitors are beneficial in all stages of heart failure and remain to be the first-line therapy
ARBs are alternative agents for heart failure in patients who are ACE inhibitors intolerant.
Combination therapy of ACE inhibitors and ARBs reduce morbidity in heart failure patients, with more adverse effects.


CHARM Added
CHARM Preserved
3 component trials comparing candesartan to placebo in patients with symptomatic heart failure
CHARM Alternative
n=2028
LVEF 40% ACE inhibitor
intolerant
n=2548
LVEF 40% ACE inhibitor
treated
n=3025
LVEF >40% ACE inhibitor
treated/not treated
Primary outcome for Overall Programme: All-cause death
Primary outcome for each trial: CV death or CHF hospitalisation


Trial Agent Target
Doses
Population Findings
CONSENSUS I
(n: 253)
Enalapril
(vs. placebo)
20 mg bid NYHA class
IV
•40% RRR of all-cause
mortality at 6 months
•50% RRR of deaths from
progressive heart failure
SOLVD Treatment
Trial
(n: 2569)
Enalapril
(vs. placebo)
10 mg bid NYHA
classes II-IV,
EF ≤35%
•16% decrease in 3.5-year
mortality
•26% decrease in death or
hospitalization for CHF
SOLVD
Prevention Trial
(n: 4228)
Enalapril
(vs. placebo)
10 mg bid NYHA class I,
EF ≤35%
•20% decrease in death or
hospitalization for CHF
•Non significant mortality
trend favoring enalapril
ATLAS
(n: 3164)
Lisinopril low dose
(2,5-5 mg)
vs. high
dose (32,5-
35 mg)
NYHA III-IV
or class II
with
exacerbation
in prior 6
months
•8% mortality reduction in
high-dose group
•24% RRR of
hospitalization for HF

ACEIs ARBs
• RESOLVD
• ELITE II
• CHARM-Programme
• VALHEFT
• OPTIMAAL

Telmisartan 80mg added to ramipril 10mg: as effective as ramipril alone
Composite CV risk = cardiovascular mortality + non-fatal myocardial infarction + hospitalisation for congestive heart failure + non-fatal stroke
Reduction in composite CV risk
The ONTARGET Investigators. N Engl J Med 2008;358:1547–1559

ACE Inhibitors Β-blockers
ARBs



RESOLVD : Neurohormones
McKelvie RS et al. Circulation. 1999;100:1056-1064.
10
17 Weeks 43 Weeks
BNP
(pmol/mL)
0 Weeks
*† * †
Candesartan
Candesartan + enalapril
Enalapril
5
0
-5
-10
*P <0.01 compared with 0 weeks. †P <0.01 compared with enalapril.

RESOLVD : Ventricular Function
McKelvie RS et al. Circulation. 1999;100:1056-1064.
35
30
25
20
15
10
5
0
-5
17 Weeks 43 Weeks 0 Weeks
**
End Diastolic
Volume
(mL)
Candesartan
Candesartan + enalapril
Enalapril
*
*
* P <0.01 compared with 0 weeks.
**P <0.05 compared with enalapril.
