3. central line associated blood stream infection
TRANSCRIPT

Central Line Associated Blood Stream Infection
(CLABSI)
Continuing Education

Introduction According to the National Health Safety Network (NHSN), a
central venous catheter or central line is “an intravascular catheter that :o Terminates at or close to the heart or o Is in one of the great vessels which is used for infusion, withdrawal of
blood or hemodynamic monitoring”. The great vessels include the
o Aorta o Pulmonary artery o Superior and inferior vena cava o Brachiocephalic veinso Internal jugular veinso Subclavian veinso External iliac veinso Common iliac veinso Femoral veins,o And in neonates, the umbilical artery/vein.

Introduction Cont. Venous access is one of the most basic yet critical components of
patient care both in hospital and ambulatory settings. It is estimated that almost 300 million catheters are used each
year and nearly 3 million are central venous catheters (CVCs), otherwise known as central lines.
They play an integral role in modern health care allowing for the administration of IV fluids, medications, blood products, parenteral nutrition as well as hemodialysis access and hemodynamic monitoring.
For as long as patients have had CVC’s, infections have occurred.o Central Venous Catheters are the most frequent cause of healthcare
associated bloodstream infection. o An estimated 41,000 central line associated bloodstream infections occur in
U.S. Hospitals each year, causing prolonged hospital stays, increased costs, and risk of mortality.
o Estimated costs for one central line infection ranges from $6,000 to $30,000.
o Of all patients diagnosed with a central line infection, one in four will die.

Definition of CLABSI
Definition One Central line-associated
bloodstream infections (CLABSI) is a term used by US Centers for Disease Control and Prevention’s (CDC’s) National Healthcare Safety Network (NHSN)
Refers to a primary blood stream infection in a patient that had a central line within the 48 hour period before the development of the blood stream infection and is not related to an infection at another site.
Its definition is more practical for surveillance.
Definition Two Catheter related
bloodstream infection (CRBSI) is a more clinical definition that requires specific lab testing to identify the catheter as the source for the bloodstream infection and is not typically used for surveillance purposes.
There are 2 terms to describe intravascular catheter related infections and are often used interchangeably even though their meanings differ.
How it relates to you National estimates of CLABSI rates are available through CDC’s NHSN, a
surveillance system of healthcare associated infections and are available on the CDC’s website.
Recent acute rates range from 1.2 to 2.1 per 1000 catheter days. The unit of measurement for these infections is based on the concept of
"catheter days." This combines the number of large vein catheters in use with the number of days they are being used. o For example, if in one particular month there were 12 cases of central
line associated bloodstream infections, the number of cases would be 12 for that month.
o We want to be able to understand that number as a proportion of the total number of days that patients had central lines. Thus, if 25 patients had central lines during that month and, for purposes of example, each kept their line for 3 days, the number of catheter days would be 25 x 3 = 75 for that particular month. The CLABSI Rate per 1,000 catheter days then would be 12/75 x 1000 = 160.
Even though the overall risk for central line related infections in the home setting are low when compared to the inpatient setting, it is important to understand the significant cost and human suffering related to this preventable problem.
Currently home health companies are not required to report incidences of catheter related infections but are estimated to range from 0.24 to 0.45 per 1000 catheter days.

Risk Factors for CLABSI Risk factors for CLABSI can be either Intrinsic or
Extrinsic. Age, gender, and underlying health conditions are
all examples of Intrinsic factors. CLABSI rates are higher among children,
particularly neonates, and highest in Pediatric ICU’s, Adult Burn, trauma and critical care units.
Hematological and Immunological deficient patients have higher risk of CLABSI as well as underlying gastrointestinal and cardiac diseases.
Female gender has lower incidences of CLABSI.

Risk Factors for CLABSI Cont.
Extrinsic factors are potentially modifiable. They include prolonged hospital stay prior to insertion of
CVC, multiple catheters, multi-lumen catheters, duration of catheter, TPN administration, CVC site, and catheter type.
Femoral and internal jugular access sites have higher CLABSI rates than subclavian sites in adult patients.
Non tunneled CVC’s account for the majority of CLABSIs. Tunneled catheters and peripherally inserted central
catheters (PICC) have a lower rate of infection than non tunneled. Implanted ports have the lowest infection rates.
Insertion procedure of central venous catheter plays a large role in development of CLABSI.
Lack of maximum sterile barriers (cap, mask, sterile gloves, sterile gown and full sterile drape) all increase risk as well as insertion in an ICU or emergency department.
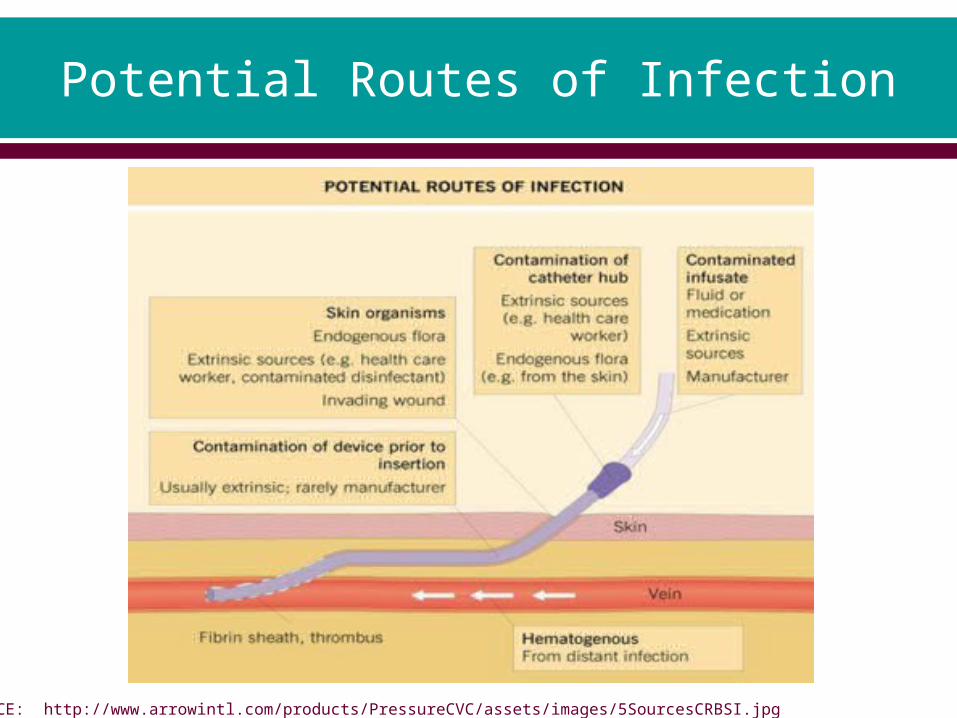
Potential Routes of Infection
REFERENCE: http://www.arrowintl.com/products/PressureCVC/assets/images/5SourcesCRBSI.jpg

Pathogenesis of CLABSI
CLABSI can be prevented through proper insertion techniques, management of the CVC while in place, and removal as soon as the catheter is no longer necessary.
CVCs can be contaminated with microorganisms via 2 major routes, extra-luminal and intra-luminal.
Extra luminal catheter infections typically occur within the first week of placement.
The patient’s skin is considered the primary source of contamination but can also include the healthcare provider’s hands.
During catheter insertion, organisms attach to the catheter as it passes through the epidermis.
Attention to strict skin antisepsis and hand hygiene is likely the most important intervention in preventing catheter associated infection.

Pathogenesis of CLABSI
Intra luminal infections occur when microorganisms directly enter the internal catheter during manipulation of the IV system such as accessing or connecting injection caps, tubing, or syringes to the catheter.
Additionally, direct contamination from patient’s skin or own body fluids can occur.
Less commonly, catheters become seeded from a secondary site of infection such as a UTI or pneumonia.
Rarely, contamination of infusate such as IV fluid or medication can be the source of infection.

Pathogenesis of CLABSI Cont.
Within minutes of venous access device insertion into the bloodstream, the patient’s body reacts to the presence of a foreign body and the damage to the endothelial lining of the vein.
A fibrin layer or sheath begins to form on the catheter surface.o Within 24 hours, a layer of platelets and white blood cells are trapped in
the fibrin layer. o A thrombus may eventually form.
Like the fibrin layer, biofilm formation begins at the same time.o Microorganisms introduced through the skin during venipuncture and
infusions colonize and interact with the fibrin. o Some bacteria produce an extracellular polysaccharide known as slime,
which protects the bacteria from antibiotics. o Bacteria from the biofilm that detach from either the internal or external
catheter surface can lead to a catheter associated bloodstream infection. o It can also result in a serious focal infection such as endocarditis. o Once a biofilm is formed, eradication is difficult thus elimination of
microbial entry is paramount to prevention.

Pathogenesis of CLABSI Cont.
REFERENCE: http://www.cathflo.com/media/Pharmacy_Sell_Sheet_12.6.pdf

Coagulase negative staphylococci, staphylococcal aureus, aerobic gram negative bacilli and Candida albicans most commonly cause catheter related bloodstream infections.
In most cases of non-tunneled CVC related bacteremia or fungemia, the catheter should be removed.
For management of tunneled CVCs and implanted ports, the decision to remove the device should be based on the o severity of the illness, o presence of complications such as endocarditis, tunnel
infection, septic thrombosis or metastatic seeding.
Pathogens in CLABSI

Prevention of CLABSI Safe and reliable venous access is an important
issue in daily practice to prevent CLABSI. In the acute care setting “bundles” or groups of
evidenced-based interventions have been created for patients with central lines.
Conceived by the Institute for Healthcare Improvement (IHI) these “bundles” result in better outcomes than when implemented individually.
While there are no evidence-based “bundles” specific to the homecare setting we must utilize the standards provided and adapt to them to the homecare setting.

Prevention of CLABSI Cont.
The key components of the IHI Bundle are:o Hand hygiene
• http://www.ihi.org/knowledge/Pages/Changes/HandHygiene.aspx
o Maximum barrier Precautions upon Insertion• http
://www.ihi.org/knowledge/Pages/Changes/MaximalBarrierPrecautionsUponInsertion.aspx
o Chlorhexidine Skin Antisepsis• http://www.ihi.org/knowledge/Pages/Changes/ChlorhexidineSk
inAntisepsis.aspxo Optimal Catheter Site selection, with avoidance in femoral
vein for Central Venous Access in adult patients• http://www.ihi.org/knowledge/Pages/Changes/OptimalCatheter
SiteSelectionwithAvoidanceofFemoralVeinforCentralVenousAccessinAdultPatients.aspx
o Daily review of Line Necessity with prompt removal of Unnecessary Lines• http://www.ihi.org/knowledge/Pages/Changes/DailyReviewofLi
neNecessitywithPromptRemovalofUnnecessaryLines.aspx

Prevention of CLABSI Cont.
Since implementing the 5 elements in the Central Line Bundle which was created in the 1990’s, hospitals across the nation have seen results in lowering the incidence of central line infections.
The CDC’s recommendations for Vascular catheter-related infection prevention provides further measures but are not limited to:o Dressing change frequency o Catheter replacemento Antisepsis of injection ports o Catheter selection o Prophylactic antimicrobialso Education.
Conclusion Infections in the acute and home setting are
preventable. As a healthcare provider and role model, we must be
knowledgeable about infection transmission. We must hold the highest standards and adhere to
and educate infection prevention interventions such as hand hygiene, aseptic technique and infusion-related care.
It is our responsibility to ensure our patients receive the best care determined by evidence-based research.
Tools to reduce and eliminate infections have been provided to us. It is our role to utilize these tools to improve our patients’ outcomes.
References Joint Commission.org: Preventing Central Line-Associated Bloodstream Infections: A
Global Challenge, A Global Perspective http://www.jointcommission.org/preventing_clabsi/
Gorski, L. Home Healthcare Nurse: 2010(28) 221-229
NHIA.org: CVAD guidelines for Home Infusion 2011(17)29-36
Poole, S. NHIA.org: Central Line Infection: Improving Our Surveillance, Treatment and Prevention in the Home Setting 2009(15)31-35
CDC: 2011 Guidelines for the Prevention of Intravascular Catheter Related Infections http://www.cdc.gov/hicpac/bsi/bsi-guidelines-2011.html
IHI: Implement the Central Line Bundle http://www.ihi.org/knowledge/Pages/Changes/ImplementtheCentralLineBundle.aspx
Seigel, M, Kramer-Cain, J. Advance For Nurses: Vascular Catheter-Associated Infections. Learn what measures can and should be taken. http://nursing.advanceweb.com/Article/Vascular-Catheter-Associated-Infections-2.aspx