2199 optimal field arrangements for stage i nonsmall cell lung cancer
TRANSCRIPT

380 I. J. Radiation Oncology l Biology 0 Physics Volume 45, Number 3 Supplement 1999
with irradiation alone or those treated with p-interferon and irradiation. Although there was a trend towards increased toxicity in the p-interferon group this could be attributed to poor tolerance of unacceptable treatment volumes in the patients who experienced toxicity. The survival outcome for patients receiving radiation alone is surprising, at 10.9 months it is very similar to the result we obtained in the standard arm of RTOG 88-08 (11.4 months), with patients KPS <70 and less than 5 % weight loss.
2 i 98 INVOLVED FIELD RADIOTHERAPY ALONE FOR EARLY STAGE NON-SMALL CELL LUNG CANCER
Cheung PC’, Brundage MD’, Dixon P’: Youssef YM’, Zhou S’, Mackillop WJ’
The Radiation Oncology Research Unit, Kingston Regional Cancer Centre, Kingston General Hospital, Queen’s University, Kingston, ON, Canada’; Princess Margaret Hospital, University Health Network, University of Toronto, Toronto, ON, Canada’
Purpose: To audit the policy at the Kingston Regional Cancer Centre in treating early stage non-small cell lung cancer (NSCLC) with radiotherapy alone directed at the primary tumour without elective irradiation of uninvolved nodal areas.
Materials and Methods: One hundred and two patients were identified as having early stage (Tl-4, NO-l, MO) NSCLC treated with involved field radiotherapy alone between 1986 and 1995. Charts and simulator films were retrieved and pertinent data were extracted and analyzed. Potential prognostic factors, such as tumour volume and size of field margins, were sought and analyzed with respect to effect on outcomes. Univariate analyses were performed using the log rank test, and multivariate analyses were performed using Cox’s method of proportional hazards.
Results: Median age of the population was 71.5 years. Ninety-eight percent of patients had ECOG performance status of 0 or 1. Most patients (76.5%) were not surgical candidates because of medical co-morbidities or old age. Ninety-three percent of patients had CT of the thorax as part of initial staging, while mediastinoscopy was performed in 16.7%. Ninety-five percent of patients were treated with an intended (policy) dose of 5000-5250 cGy in 20 fractions over 4 weeks. All patients were treated with megavoltage photons. Actuarial overall survival was 37.3% at 3 years and 16.2% at 5 years. Median survival was 24 months. Actuarial cause specific survival was 46.0% at 3 years and 26.9% at 5 years. Actuarial recurrence free survival was 25.1% at 3 years and 14.0% at 5 years. The actuarial risk of recurrence was 67.1% at 3 years and 73.9% at 5 years. Of those who recurred, >60% had a local component of failure at initial relapse, while about one-third had a distant component. Forty-nine percent of initial relapses were isolated local failures, while isolated regional nodal failures at initial relapse occurred in only 6.6% of recurrences. Univariate and multivariate analyses found neither tumour volume nor size of field margins to be significant predictors of outcome. Patients with tumours 5 10 cm3 had 3 and 5 year survivals of 33.3% and 14.3% respectively, compared with 21.7% and 13.0% respectively for those with tumours >50 cm3. Patients with minimum lateral margins between 0.5 and 1.5 cm had 3 and 5 year survivals of 33.3% and 16.7% respectively, compared with 25.0% and 12.5% respectively for those with lateral margins greater than 2.5 cm. There were no treatment interruptions due to acute toxicity and no treatment related deaths. Pneumonitis was documented in 4.9% of patients, while lung fibrosis causing increased shortness of breath was reported in 2.9% of patients.
Conclusion: Radiotherapy alone can cure a small but significant proportion of patients with early stage NSCLC. There is a high recurrence rate, with a significant proportion failing locally at initial relapse. Efforts should be made to increase local control with the use of altered fractionation/dose escalation or combined modality with chemotherapy. Elective nodal irradiation will not impact significantly on outcome until there is better local control of the primary tumour.
2 199 OPTIMAL FIELD ARRANGEMENTS FOR STAGE I NONSMALL CELL LUNG CANCER
Das SK, Sibley GS, Munley MT, Marks LB
Duke University Medical Center, Durham, NC, USA
Purpose: Patients with medically inoperable nonsmall cell lung cancer (NSCLC) typically have very poor pulmonary function, which makes optimization of the treatment plan essential to sparing functional lung tissue. 3D treatment planning allows sophisticated methods to be used to compare various treatment plans. The purpose of this paper is to determine “optimal” treatment plans for specific tumor locations, evaluated by dosimetric endpoints.
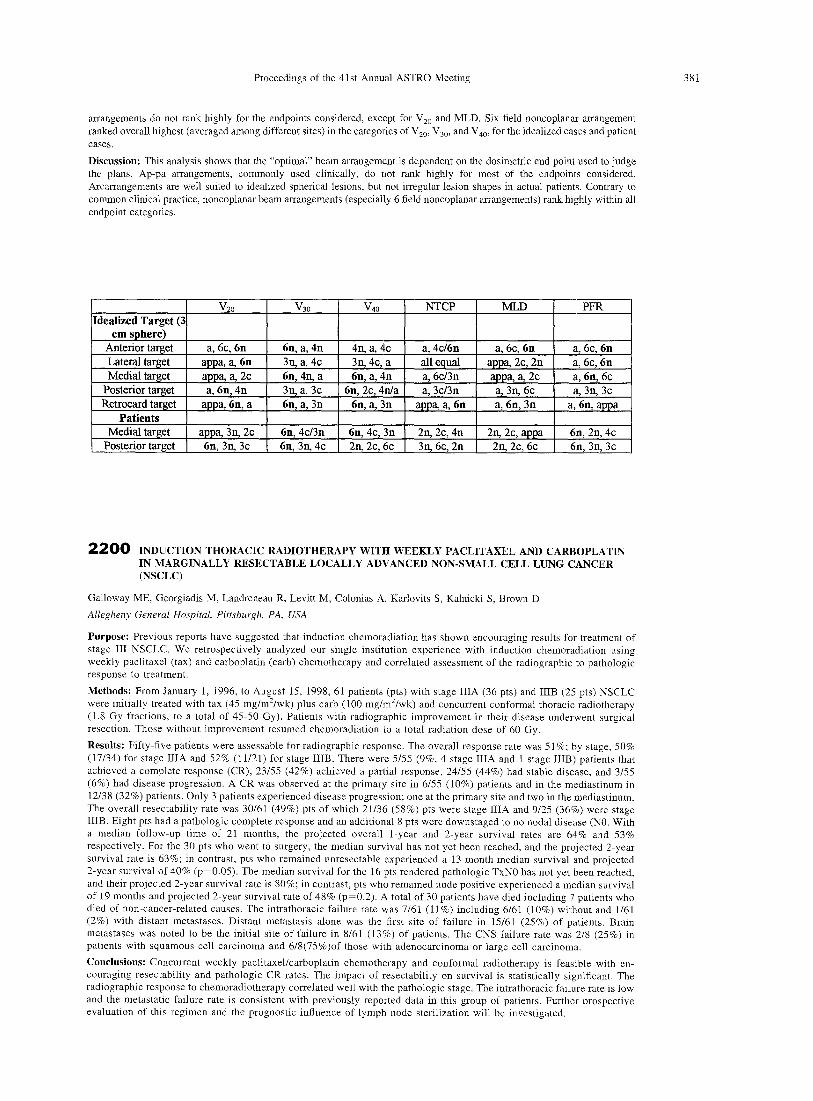
Methods: Coplanar, noncoplanar, ap-pa, and 180” arc arrangements were simulated on idealized 3-cm spherical targets within the lung for 4 different locations (medial. anterior, posterior, and retrocardiac). An optimization program was used to determine the beam geometry (orientations) for the coplanar and noncoplanar arrangements; the program sought to minimize lung dose while maximizing target coverage. Using a prescription dose of 70 Gy, the 10 different beam arrangements (4 coplanar, 4 noncoplanar, ap-pa, arc) were compared using the endpoints of lung volume > 20 Gy (V,,), > 30 Gy (V,,), > 40 Gy (V,,), normal tissue complication probabilily (NTCP, Kutcher), mean lung dose (MLD), and percent lung function reduction (PFR). PFR is the weighted sum of predicted percent reduction in regional lung function based on dose response curves from our clinical studies. This dosimetric study was repeated in 6 patients with medically inoperable stage I NSCLC irradiated at our institution (three had medial lesions, and three had posterior lesions). Results: The Table shows the three “best” arrangements for each endpoint, for the idealized 3-cm spherical lesion and the patients (a = arc, c = coplanar, n = noncoplanar). Where equivalent, the simplest arrangement was chosen. The beam arrangement rankings of the idealized and patient cases agree, with the exception of arc arrangements. While arc arrangements are well suited to idealized spherical lesions, they are not so for the irregular lesion shapes in the actual patients. Ap-pa
Proceedings of the 41 st Annual ASTRO Meeting 381
arrangements do not rank highly for the endpoints considered, except for V,, and MLD. Six field noncoplanar arrangement ranked overall highest (averaged among different sites) in the categories of V,,, V,,, and V,,, for the idealized casles and patient cases.
Discussion: This analysis shows that the “optimal” beam arrangement is dependent on the dosimetric end point used to judge the plans. Ap-pa arrangements, commonly used clinically, do not rank highly for most of the endpoints considered. Arcarrangements are well suited to idealized spherical lesions, but not irregular lesion shapes in actual patients. Contrary to common clinical practice, noncoplanar beam arrangements (especially 6 field noncoplanar arrangements) rank highly within all endpoint categories.
2200 INDUCTION THORACIC RADIOTHERAPY WITH WEEKLY PACLITAXEL AND CARBOPLATIN IN MARGINALLY RESECTABLE LOCALLY ADVANCED NON-SMALL CELL LUNG CANCER (NSCLC)
Galloway ME, Georgiadis M, Landreneau R, Levitt M, Colonias A, Karlovits S, Kalnicki S, Brown D
Allegheny General Hospital, Pittsburgh, PA, USA
Purpose: Previous reports have suggested that induction chemoradiation has shown encouraging results for treatment of stage III NSCLC. We retrospectively analyzed our single institution experience with induction chemoradiation using weekly paclitaxel (tax) and carboplatin (carb) chemotherapy and correlated assessment of the radiographic to pathologic response to treatment.
Methods: From January 1, 1996, to August 15, 1998, 61 patients (pts) with stage IIIA (36 pts) and IIIB (25 pts) NSCLC were initially treated with tax (45 mg/m’/wk) plus carb (100 mglm*/wk) and concurrent conformal thoracic radiotherapy (1.8 Gy fractions, to a total of 45-50 Gy). Patients with radiographic improvement in their disease underwent surgical resection. Those without improvement resumed chemoradiation to a total radiation dose of 60 Gy.
Results: Fifty-five patients were assessable for radiographic response. The overall response rate was 5 1 lo; by stage, 50% (17/34) for stage IIIA and 52% (1 l/21) for stage IIIB. There were 5/55 (9%, 4 stage IIIA and 1 stage IIIB) patients that achieved a complete response (CR), 23155 (42%) achieved a partial response, 24/55 (44%) had stable disease, and 3/55 (6%) had disease progression. A CR was observed at the primary site in 6/55 (10%) patients and in the mediastinum in 12138 (32%) patients. Only 3 patients experienced disease progression: one at the primary site and two in the mediastinum. The overall resectability rate was 30161 (49%) pts of which 21136 (58%) pts were stage IIIA and 9/25 (36%) were stage IIIB. Eight pts had a pathologic complete response and an additional 8 pts were downstaged to no nodal disease (NO. With a median follow-up time of 21 months, the projected overall l-year and 2.year survival rates are 64% and 53% respectively. For the 30 pts who went to surgery, the median survival has not yet been reached, and the projected 2.year survival rate is 63%; in contrast; pts who remained unresectable experienced a 13 month median survival and projected 2-year survival of 40% (p=O.O5). The median survival for the 16 pts rendered pathologic TxNO has not yet been reached, and their projected 2-year survival rate is 80%; in contrast, pts who remained node positive experienced a median sui-viva1 of 19 months and projected 2-year survival rate of 48% (p=O.2). A total of 30 patients have died including 7 patients who died of non-cancer-related causes. The intrathoracic failure rate was 7/61 (11%) including 6/61 (10%) without and 1161 (2%) with distant metastases. Distant metastasis alone was the first site of failure in 15/61 (25%) of patients. Brain metastases was noted to be the initial site of failure in S/61 (13%) of patients. The CNS failure rate was 2/S (25%) in patients with squamous cell carcinoma and 6/8(75%)of those with adenocarcinoma or large cell carcinoma.
Conclusions: Concurrent weekly paclitaxebcarboplatin chemotherapy and conformal radiotherapy is feasible with en- couraging resectability and pathologic CR rates. The impact of resectability on survival is statistically significant, The radiographic response to chemoradiotherapy correlated well with the pathologic stage. The intrathoracic failure rate is low and the metastatic failure rate is consistent with previously reported data in this group of patients. Further prospective evaluation of this regimen and the prognostic influence of lymph node sterilization will be investigated.