2.10.2009ellyte.ppt1 disturbances of water & electrolyte metabolism part 1 – water &...
TRANSCRIPT

2.10.2009 ellyte.ppt 1
DISTURBANCES OF WATER &DISTURBANCES OF WATER & ELEELECCTROLYTTROLYTE METABOLISME METABOLISM
PART 1 PART 1 – – WWAATER &TER & SOD SODIUMIUM
LLECECTURETURE FROM FROM PATPATHHOOPHPHYYSSIOLIOLOOGGYY
schoschool ol yeayear 2009r 2009/2010/2010
OLIVER RÁCZ OLIVER RÁCZ ININSTSTITUTE OFITUTE OF PAT PATHHOOPHPHYYSSIOLIOLOOGGY,Y,
MEDICAL SCHOOL,MEDICAL SCHOOL, UPJŠ KOŠICE UPJŠ KOŠICE

2.10.2009 ellyte.ppt 2
IIoonn Amount in Amount in bodybody
PlaPlassmama
mmol/lmmol/l
CellsCells
mmol/lmmol/lSodSodiumium, Na, Na++ 92 g92 g
4 mol4 mol141141 1010
Potassium, KPotassium, K++ 100-140 g100-140 g
2,5-3,5 mo2,5-3,5 moll44 155155
Calcium, CaCalcium, Ca2+2+ 1200 g1200 g
30 m30 mooll2,52,5 < 0,001< 0,001
(uneven(uneven in in organellesorganelles))
Magnesium, MgMagnesium, Mg2+2+ 26,5 g26,5 g
1,1 mo1,1 moll11 1515
ChloridChloride, Cle, Cl-- 50 g50 g
1,4 m1,4 mooll103103 88
PhosphatePhosphate(a(ass phphososphphororusus))
775 g775 g
25 m25 mooll11 6565

2.10.2009 ellyte.ppt 3
SodSodiumium – k – kitcitchheenn s saltalt in our dietin our diet
EuropeEurope 10 – 12 g10 – 12 g/d/d 230 – 276 mmol/d 230 – 276 mmol/d RecommendedRecommended 2 – 7 2 – 7 46 – 161 46 – 161 HypertonicHypertonicss << 3,5 3,5 80 80 StrictStrict vegetari vegetariaannss 0,75 0,75 17 17
Ca & Mg dCa & Mg deficieficiency is frequentency is frequent!!
Mg: 300 – 350 mg/d = 12-14 mmol/dmore in puberty, gravidity, lactation& physical exerciseUSA: 143 – 266 mg/d
Ca: 800 mg/d = 20 mmol/dthe same for chidren and younggravidity & lactation – 1200 mg/d!

2.10.2009 ellyte.ppt 4
DISTRIBUTION OF WATER IN HUMAN BODY
CompartmentCompartment Volume, Volume, litreslitres
% of body % of body massmass
% of total % of total waterwater
ICS*ICS* 2828 4040 6767
ECSECS 1414 2020 3333
ISFISF 1111 15,715,7 2626
IVFIVF 33 4,34,3 77
SUMMASUMMA 4242 6060 100100
*1014 cells
Third space! small virtual volume, dynamicexchange – important in pathological conditions
2.10.2009 ellyte.ppt 5
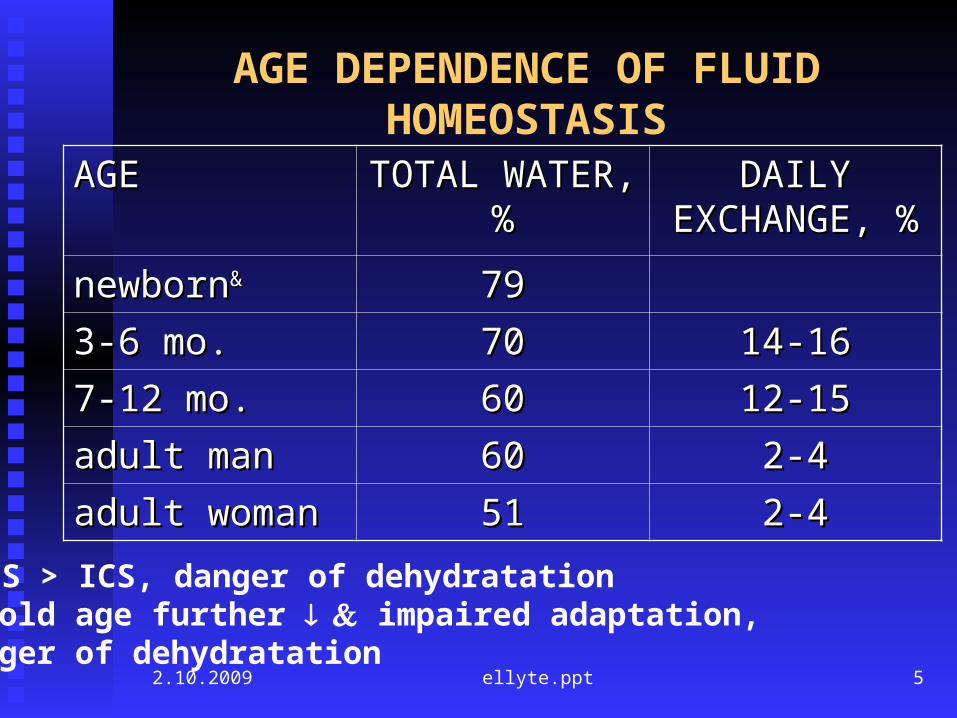
AGE DEPENDENCE OF FLUID HOMEOSTASIS
AGEAGE TOTALTOTAL WWAATERTER, , %%
DAILY DAILY EEXCHAXCHANNGEGE, %, %
nnewbornewborn&& 7979
3-6 m3-6 mo.o. 7070 14-1614-16
7-12 m7-12 moo.. 6060 12-1512-15
adult manadult man 6060 2-42-4
adult womanadult woman 5151 2-42-4
& ECS > ICS, danger of dehydratationIn old age further impaired adaptation, danger of dehydratation

2.10.2009 ellyte.ppt 6
BALANCE & DYNAMICS
intakeintake = = outputoutput++ 1,2 – 1,2 – 1,5 beverage1,5 beverage
++ 1,0 1,0 foodfood
++ 0,3 – 0,5 metaboli0,3 – 0,5 metabolissmm
– – 1,0 – 2,0 urine1,0 – 2,0 urine
– – 0,6 – 0,8 perspirat0,6 – 0,8 perspiratiionon
– – 0,4 – 0,50,4 – 0,5 respirationrespiration
– – 0,10,1 sto stoooll
2,5 – 3,0 lit2,5 – 3,0 liteerrs/days/day
KKIIDNEYSDNEYS = 180 l/d = 180 l/d GITGIT = 8,2 l/d = 8,2 l/d
ssaallivaiva 1,51,5 stomachstomach 2,52,5 panpanccreasreas 0,70,7 bibillee 0,50,5 gutsguts 3,03,0
THIRDTHIRD SSPPACEACE

volume 5 l= 25 5,0/l= 25 5,0/l= 3 0,6/l= 53 10,6/l
Volume change (water loss)
Canges in concentration of solutes without change of the amount!
Compensatory mechanismsretention or excretion of ions adjustment of concentations
OSMOLALITOSMOLALITYY && OSMOTIC GAPOSMOTIC GAP
Osmolality = 2*[Na] + [glucose] + [urea]

Volume 5 4 l= 25 5,0 6,25/l= 25 5,0 6,25/l= 3 0,6 0,75/l= 53 10 13,25/l
Volume change (water loss)
Canges in concentration of solutes without change of the amount!
Compensatory mechanismsretention or excretion of ions adjustment of concentations
OSMOLALITOSMOLALITYY && OSMOTIC GAPOSMOTIC GAP
Osmolality = 2*[Na] + [glucose] + [urea]

Volume 5 4 l= 25 5,0 6,25/l= 25 5,0 6,25/l= 3 0,6 0,75/l= 53 10 13,25/l
Volume change (water loss)
Canges in concentration of solutes without change of the amount!
Compensatory mechanismsretention or excretion of ions adjustment of concentations
OSMOLALITOSMOLALITYY && OSMOTIC GAPOSMOTIC GAP
Osmolality = 2*[Na] + [glucose] + [urea]

Loss of isotonic fluid
Reduction of ECS, thirstno change of ICSnormal plasma sodium

Loss of hypotonic fluid
Reduction of ECS.Hypernatremia compensated through water shift from ICSShrinkage of cells

Salt loss
Hyponatremia compensated through water shift from ECSinto ICS, Reduction of ECS, swelling (oedema) of cells

2.10.2009 ellyte.ppt 13
DISTURBANCES OF THE SYSTEDISTURBANCES OF THE SYSTEMM
No pureNo pure form formss – – loss of water, salt...loss of water, salt...
ImmediateImmediate reactionreaction of comof compenpenssaatory systemstory systems
ECS ECS is in contact both with external environment is in contact both with external environment aand withnd with ICS ICS
ICS ICS is in contact only withis in contact only with ECS ECS
Plasmatic concentrations are not amounts and does Plasmatic concentrations are not amounts and does not inform on dynamics of compoundsnot inform on dynamics of compounds

2.10.2009 ellyte.ppt 14
POSSIBLE CAUSES AND POSSIBLE CAUSES AND MECHANISMSMECHANISMS
ExtrExtreeme me deviations of external environmentdeviations of external environment
DehydratDehydratationation from insufficient water intakefrom insufficient water intake
Disturbances caused by damaged function of effector Disturbances caused by damaged function of effector systemssystems ( (kidneyskidneys, GIT, , GIT, eettc.c.))
DiarrhoeaDiarrhoea, , vomitusvomitus, , kidney diseaseskidney diseases
Disturbances caused byDisturbances caused by erroneouserroneous regul regulationation (CNS, (CNS, ADH, aldosterADH, aldosteroonnee))
Diabetes insipidus, Conn sy., SIADHDiabetes insipidus, Conn sy., SIADH
Heart failure & RAA activationHeart failure & RAA activation

2.10.2009 ellyte.ppt 15
DECREASED WATER INTAKEDECREASED WATER INTAKE
1 – 2 d1 – 2 daysays: hypero: hyperossmotic hypovolmotic hypovoleemiamia
thirthirsstt, , compensated throughcompensated through ADH/RA ADH/RAAA Pespiratio insensibilis 5 ml/hoPespiratio insensibilis 5 ml/hourur
fever and in hot environment In old people and kidney diseases the
concentrating capacity od kidneys is decreased Later: exsicosis, dehydratation, > 20 % death

2.10.2009 ellyte.ppt 16
WATER DEFICIENCY WATER DEFICIENCY – – REDUCTION OF REDUCTION OF ECECSS
CausesCauses Insufficient fluid intakeInsufficient fluid intake Inability to drinkInability to drink ((loss of consciousnessloss of consciousness)) Losses throughLosses through GIT GIT ((diarrhoe, vomitusdiarrhoe, vomitus)) Losses through kidneysLosses through kidneys
((diuretidiureticscs, osmotic diur, osmotic diuresisesis, , kideny diseaseskideny diseases, , m. Addisonm. Addison))
Losses through skinLosses through skin ((increased sweatingincreased sweating, , burnsburns)) Displacement intoDisplacement into t third hird pplacelace (ileus, ascites)(ileus, ascites) Blood lossBlood loss (?) (?)
SymptomsSymptoms: hypoten: hypotensionsion, tachy, tachyccardia, ardia, dry skindry skin, , thirstthirst, , oligoliguuria ria && decreased sodium excretiondecreased sodium excretion, , increase of increase of hematohematoccritrit

2.10.2009 ellyte.ppt 17
WATER RWATER RETENETENTIONTION – ECS – ECS EXPANSION EXPANSION
CausesCausesIncreasedIncreased fluid intakefluid intake
Increased intake &Increased intake & disturbed disturbed regulregulatatiionon – SIADH – SIADHkidney failurekidney failurenenephphrotic sy.rotic sy.heart failureheart failureliver cirrhosisliver cirrhosis
SymptomsSymptoms:: OeOeddeemmaa. .

2.10.2009 ellyte.ppt 18
HHypernatrypernatraaeemimiaa >150 / 160 mmol/l>150 / 160 mmol/l
Low osmolality of urineLow osmolality of urine – diabetes insipidus – diabetes insipidusOsmolalitOsmolalityy of urineof urine pla plassmmaa – osmotic diur – osmotic diuresisesis
(diabetes mellitus)(diabetes mellitus)OsmolalitOsmolality of uriney of urine > pla > plassmmaa – dehydrat – dehydratationation
diarrhoea, vomitus sweatingdiarrhoea, vomitus sweatingConn syndrConn syndroommee (hyperaldo (hyperaldossteroniteronissm) m)
hypernatrhypernatreemia, hypokalmia, hypokaleemiamia

2.10.2009 ellyte.ppt 19
HHyponatryponatraaeemimiaa <130 / 120 mmol/l<130 / 120 mmol/l
Plasma oPlasma osmolalitsmolalityy highhigh hypergly hyperglycecemia ?!mia ?!Plasma oPlasma osmolalitsmolalityy lowlow
Na Na in urinein urine > 20 mmol/l > 20 mmol/l && hypovol hypovoleemiamiam. Addison, diuretim. Addison, diureticscssalt losing salt losing nenephphritisritis
Na Na inin urineurine << 20 mmol/l 20 mmol/l && hypovol hypovoleemiamiadiarrhoea, vomitus, sweating with diarrhoea, vomitus, sweating with inadequate fluid replacementinadequate fluid replacement
Na Na inin urineurine << 20 mmol/l 20 mmol/l && oedemaoedemaheart failure,heart failure, cir cirrrhhosis,osis, ne nephphrotic sy.rotic sy.SIADHSIADH

2.10.2009 ellyte.ppt 20
DISTURBANCES OF ADH SECRETION DISTURBANCES OF ADH SECRETION AND EFFECTSAND EFFECTS – – I.I.
Diabetes insipidus, neurogenDiabetes insipidus, neurogenicic (AD) (AD)AVP gene mutationAVP gene mutation
Acquired formsAcquired forms – – damage ofdamage of hypot hypothhalamualamussCCompletomplete & partial formse & partial forms
Diabetes insipidus, renDiabetes insipidus, renaal (X-l (X-related &related & AR) AR)Receptor Receptor (X) (X) or water channel protein (AR)or water channel protein (AR) gene mutationsgene mutations
AcquiredAcquired – – kidney diseaseskidney diseases

2.10.2009 ellyte.ppt 21
DISTURBANCES OF ADH SECRETION DISTURBANCES OF ADH SECRETION AND EFFECTSAND EFFECTS – – IIII..
SIADH – inadeSIADH – inadequatequate se seccrretion ofetion of ADH ( ADH (lack of suspensionlack of suspension))ExpanExpanssiion of on of ECSECShyponatrhyponatreemia, hypoosmolalitmia, hypoosmolalityyHigh urineHigh urine osmolalit osmolality &y & high high Na Na in urinein urine IncreasedIncreased ANP ANPRenRenaal l && endo endoccrinrinee func functtiions ions inntacttact
Hereditary forms and stressHereditary forms and stress ??!! ??!!

2.10.2009 ellyte.ppt 22
DISTURBANCES OF WATER &DISTURBANCES OF WATER & ELEELECCTROLYTTROLYTE METABOLISME METABOLISM
PART PART 22 – POTASSIUM– POTASSIUM
LLECECTURETURE FROM FROM PATPATHHOOPHPHYYSSIOLIOLOOGGYY
schoschool ol yeayear 2009r 2009/2010/2010
OLIVER RÁCZ OLIVER RÁCZ ININSTSTITUTE OFITUTE OF PAT PATHHOOPHPHYYSSIOLIOLOOGGY,Y,
MEDICAL SCHOOL,MEDICAL SCHOOL, UPJŠ KOŠICE UPJŠ KOŠICE

2.10.2009 ellyte.ppt 23
POTASSIUM HOMEOSTASIS
Serum concentration: Serum concentration: 3,8 – 5,5 mmol/l3,8 – 5,5 mmol/l** Total amount depends on muscle massTotal amount depends on muscle mass
(young > old;(young > old; mman > woman > womenen) )
37 – 52 mmol/kg 37 – 52 mmol/kg body massbody mass IntakeIntake: : 2-6 g/d2-6 g/d = 50-150 mmol/d= 50-150 mmol/d Excretion through kidneysExcretion through kidneys 10 – 20 mmol/d 10 – 20 mmol/d
(0,4 – 0,8 g/d). (0,4 – 0,8 g/d). Inverse association with Na excretionInverse association with Na excretion GIT GIT excretion iexcretion iss important in kidney failure important in kidney failure a andnd inin
patpathhologicologicalal conditionsconditions ( (diarrhoeadiarrhoea))
*Depends on method. Preanalytic errors - hemolysis!

2.10.2009 ellyte.ppt 24
FUNCTIONS OF POTASSIUM & INTERPRETATION OF RESULTS
FunctionsFunctions intraceintracelllullulaar osmotic r osmotic pressurepressure resting & action resting & action potenpotenttiiaal l enzenzyymme activitye activity, proteosynt, proteosynthesishesis
ProblProbleemmss: :
1.1. assesment of cell homeostasis from extraassesment of cell homeostasis from extracecelllullulaar r cconcentroncentrationation
2.2. pHpH changes changes: : exchangeexchange H H//K K betweenbetween EC ECFF/IC/ICFF
2.10.2009 ellyte.ppt 25
INTERNAL & EXTERNAL BALANCE
acidosis: Hacidosis: H++ enters the cells, K enters the cells, K+ + out into ECFout into ECF alkalalkalosisosis: : HH++ into into ECFECF, K, K+ + enters the cellsenters the cells KK++ entry into cellsentry into cells: in: inssululiinn (together with glucose) (together with glucose), ,
aldosteraldosteroonnee, adrenaline, adrenaline rapid cellular proliferatiom (treatmentrapid cellular proliferatiom (treatment of of perniciperniciousous ana anaeemia mia
with with BB1212 vitamin vitamin cell necrosis, hemolysiscell necrosis, hemolysis (crush sy, (crush sy, malignanciesmalignancies), ), KK++ intinto o
ECFECF
kidney or GIT retentionkidney or GIT retention//losseslosses, parenter, parenteraal l intakeintake dietary dietary deficideficiency/excess as an additional factorency/excess as an additional factor
internal – ECF/ICF
external – ECF/environment
2.10.2009 ellyte.ppt 26
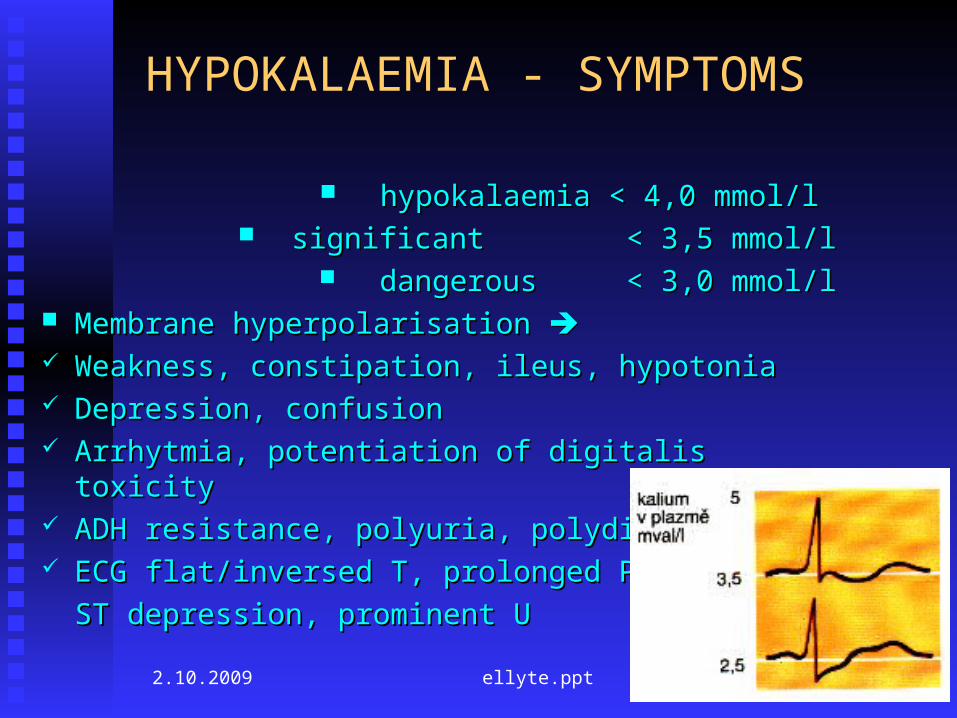
HYPOKALAEMIA - SYMPTOMS
hypokalaemiahypokalaemia < 4,0 mmol/l < 4,0 mmol/l significantsignificant < 3,5 mmol/l < 3,5 mmol/l dangerousdangerous < 3,0 mmol/l < 3,0 mmol/l
Membrane hMembrane hyperpolariyperpolarisationsation Weakness, constipation, ileus, hypotoniaWeakness, constipation, ileus, hypotonia Depression, confusionDepression, confusion Arrhytmia, potentiation of digitalis toxicityArrhytmia, potentiation of digitalis toxicity ADH resistance, pADH resistance, polyuria, polydipsiaolyuria, polydipsia EECCG G flat/inversedflat/inversed T T, prolonged PR, prolonged PR, ,
STST depression depression, , prominent prominent UU

2.10.2009 ellyte.ppt 27
HYPOKALAEMIA - CAUSES
Disorders of externalDisorders of external b baalancelance GIT – diarrhoea, vomitus, tumors of colon, rectum, GIT – diarrhoea, vomitus, tumors of colon, rectum,
pancreaspancreas KidneysKidneys - - diuretics, polyuric stage of renal failure, diuretics, polyuric stage of renal failure,
hereditary tubulopathieshereditary tubulopathies,, PrimPrimaary ry && secondary hyperaldosteronism, abuse of secondary hyperaldosteronism, abuse of
liquoriceliquorice, , Cushing, ectopic ACTH productionCushing, ectopic ACTH production
Glycyrrhiza glabra. GlycyrrhizinGlycyrrhiza glabra. Glycyrrhizin, a sweet substance, a sweet substanceWeakWeak ccortiorticcomimetic omimetic && fitoestrog fitoestrogeenn effect effect Component of herb teas, nonalcoholic drinks and beerComponent of herb teas, nonalcoholic drinks and beer

2.10.2009 ellyte.ppt 28
HYPOKALAEMIA - CAUSES
Disorders ofDisorders of intern internalal b baalancelance Treatment of Treatment of diabetic hyperglydiabetic hyperglycaecaemimiaa with with ininssululiin n
((KK+ + entry into cells together with glucoseentry into cells together with glucose)) AlkalosisAlkalosis Rapid cellular proliferationRapid cellular proliferation Familiar hypokalaemic periodic paralysis (hereditary) Familiar hypokalaemic periodic paralysis (hereditary)

2.10.2009 ellyte.ppt 29
HYPERKALAEMIA - SYMPTOMS hyperkalaemiahyperkalaemia < < 55,5 mmol/l,5 mmol/l
significantsignificant < < 66,5 mmol/l,5 mmol/l dangerousdangerous < < 77,5 mmol/l,5 mmol/l
Low resting potential, short cardiac action potential, Low resting potential, short cardiac action potential, increased speed of repolarization increased speed of repolarization
Can kill without warningCan kill without warning Ventricular fibrillation and cardiac arrest may be the first Ventricular fibrillation and cardiac arrest may be the first
signs! (if you do not check K & ECG)signs! (if you do not check K & ECG) EECG: abnormal/absent P; broad QRS, CG: abnormal/absent P; broad QRS,
peaked Tpeaked T,, ST depressionST depression

2.10.2009 ellyte.ppt 30
HYPERKALAEMIA - CAUSES
Disorders ofDisorders of extern externalal b baalancelance Decreased excretion.Decreased excretion. UnderUnder GFR 15 ml/min GFR 15 ml/min alwaysalways. .
AAnnuuriria: Ka: K increaseincrease 1 mmol/l d1 mmol/l dailyaily
In mild impairment of kidney function only when other In mild impairment of kidney function only when other factors are presentfactors are present
Increased intake (infusions, NaCl substitution) only in the Increased intake (infusions, NaCl substitution) only in the case of impaired kidney functioncase of impaired kidney function
m. Addison, adrenogenitm. Addison, adrenogenitaal sy., inhibl sy., inhibiitortors ofs of angioten angiotensinsin cconvertonvertinging enz enzyymmee

2.10.2009 ellyte.ppt 31
HYPERKALAEMIA - CAUSES
Disorders ofDisorders of intern internalal b baalancelance AAcidcidosisosis Cell necrosis - rhabodmyolysis, burns, cytostatic treatment Cell necrosis - rhabodmyolysis, burns, cytostatic treatment
of malignanaciesof malignanacies Digitalis overdosisDigitalis overdosis Hyperkalaemic periodic paralysis (hereditary)Hyperkalaemic periodic paralysis (hereditary) Malignant hypertermia (hereditary)Malignant hypertermia (hereditary)

2.10.2009 ellyte.ppt 32
DISTURBANCES OF WATER &DISTURBANCES OF WATER & ELEELECCTROLYTTROLYTE METABOLISME METABOLISM
PART PART 33 – CALCIUM– CALCIUM & & MAGNESIUM MAGNESIUM
LLECECTURETURE FROM FROM PATPATHHOOPHPHYYSSIOLIOLOOGGYY
schoschool ol yeayear 2009r 2009/2010/2010
OLIVER RÁCZ OLIVER RÁCZ ININSTSTITUTE OFITUTE OF PAT PATHHOOPHPHYYSSIOLIOLOOGGY,Y,
MEDICAL SCHOOL,MEDICAL SCHOOL, UPJŠ KOŠICE UPJŠ KOŠICE

2.10.2009 ellyte.ppt 33
CALCIUM
Total body Total body 1200 g 1200 g 30 mol30 mol ECFECF 0,9 g 0,9 g 22,5 mmol22,5 mmol PlasmaPlasma 0,36 g 0,36 g 9,0 mmol 9,0 mmol Bone / ECF exchange Bone / ECF exchange 500 mmol/d500 mmol/d Daily losses Daily losses 25 mmol/d (1g)25 mmol/d (1g)
urineurine 6 mmol (240 GF – 234 reabsorbtion)6 mmol (240 GF – 234 reabsorbtion) faeces 19 mmol (+25 food, 12 in, + 6 secr.)faeces 19 mmol (+25 food, 12 in, + 6 secr.) skin 0,3 mmolskin 0,3 mmol
Small changes in fluxes can have profound effect of Small changes in fluxes can have profound effect of plasma Caplasma Ca

2.10.2009 ellyte.ppt 34
FUNCTIONS OF CALCIUM
StructuralStructural NeuromuscularNeuromuscular
BloodBlood Signal systemsSignal systems
Bone, teethBone, teeth Control of excitability;Control of excitability;
Neurotransmitter Neurotransmitter releaserelease
Muscle contractionMuscle contraction Coagulation (Coagulation (§§ 22) 22) MessengerMessenger

2.10.2009 ellyte.ppt 35
PLASMA CALCIUM
TOTAL
2,25 – 2,60 mmol/l
diffusible 54 % protein-bound 46 %
free - ionized 47 %
7% complexed
CLINICAL CHEMISTRY: TOTAL OR IONIZED ?
pH!

2.10.2009 ellyte.ppt 36
EC CALCIUM REGULATING HORMONES
PTH & calcitriol!PTH & calcitriol! Calcitonin is of minor importance. Calcitonin is of minor importance. Also regulation of phosphorus and perhaps magnesium Also regulation of phosphorus and perhaps magnesium o PTH – a 84 AA peptide from 115 AA precursor. AAs 1-PTH – a 84 AA peptide from 115 AA precursor. AAs 1-
34 are active34 are activeo Short half lifeShort half life Calcitriol is a steroid hormone derived from vit. DCalcitriol is a steroid hormone derived from vit. D The 2The 2ndnd hydroxylation in liver is strictly controlled hydroxylation in liver is strictly controlled Calbindin D in gutCalbindin D in gut Receptors in other tissues – role in cellular Receptors in other tissues – role in cellular
proliferation and differentiation and in immune proliferation and differentiation and in immune response ?response ?

2.10.2009 ellyte.ppt 37
FUNCTIONS OF PTH
BONEBONE Release of calcium Release of calcium [Ca [Ca2+2+]] Osteoclastic resorptionOsteoclastic resorption
KIDNEYKIDNEY Calcium reabsorbtion Calcium reabsorbtion [Ca [Ca2+2+]] 22ndnd hydroxylation of vit.D hydroxylation of vit.D Ca, P absorbtion Ca, P absorbtion PhosphaturiaPhosphaturia [PO[PO44] ]
Decrease of HCODecrease of HCO33-- reabsorbtion reabsorbtion pHpH

2.10.2009 ellyte.ppt 38
HYPOCALCAEMIA - CAUSES HypoparathyroidismHypoparathyroidism
Congenital (with Di George sy.)Congenital (with Di George sy.) Acquired – autoimmune, surgery, hemochromatosis, Acquired – autoimmune, surgery, hemochromatosis,
tumorstumors PseudohypoparathyroidismPseudohypoparathyroidism
2 hereditary disorders of PTH signaling pathway (cAMP 2 hereditary disorders of PTH signaling pathway (cAMP dependent)dependent)
Magnesium deficiency (pseudo ?)Magnesium deficiency (pseudo ?) DeficiencyDeficiency of of vit vitaminamin D (!) D (!) DDisorders of vitisorders of vitaminamin D metabolism D metabolism – end stage renal disease – end stage renal disease Acute pancreatitis, transfusions with citrate, neonatalAcute pancreatitis, transfusions with citrate, neonatal

2.10.2009 ellyte.ppt 39
HYPOCALCAEMIA - SYMPTOMS
Stupor, numbness, paraesthesiaStupor, numbness, paraesthesia Muscle cramps and spasms „tetany“Muscle cramps and spasms „tetany“ Laryngeal stridorLaryngeal stridor ConvulsionsConvulsions ChvostekChvostek+ Trousseau+, long QT on ECG+ Trousseau+, long QT on ECG Cataract in chronic hypocalcaemiaCataract in chronic hypocalcaemia Rickets (rRickets (rachitisachitis)) in vitamin D deficiency in vitamin D deficiency
OSTEOPOROSIS ???

2.10.2009 ellyte.ppt 40
HYPERCALCAEMIA - CAUSES
COMMON (COMMON (90%90% of all of all)) Primary hyperparathyroidismPrimary hyperparathyroidism Malignancies – bone metastasis (?), PTHrP and other Malignancies – bone metastasis (?), PTHrP and other
humoral factorshumoral factors LESS COMMONLESS COMMON
ThyrThyreeotoxicosis, sarcoidosisotoxicosis, sarcoidosis UNCOMMONUNCOMMON
Lithium treatment, tbc, immobilisation, adrenal failure, renal Lithium treatment, tbc, immobilisation, adrenal failure, renal failure, hereditaryfailure, hereditary
BUT ALSO HYPERPARATHYROIDISM WITHOT BUT ALSO HYPERPARATHYROIDISM WITHOT HYPERCALCAEMIAHYPERCALCAEMIA Compensatory in vitamin D deficiency, renal diseaseCompensatory in vitamin D deficiency, renal disease

2.10.2009 ellyte.ppt 41
HYPERCALCAEMIA - SYMPTOMS
Weakness, tiredness, weight lossWeakness, tiredness, weight loss Imparied concentration, drowsiness (coma)Imparied concentration, drowsiness (coma) Anorexia, nausea, vomiting, constipationAnorexia, nausea, vomiting, constipation Polyuria, dehydrationPolyuria, dehydration Renal calculi, nephrocalcinosisRenal calculi, nephrocalcinosis short QT, arrhytmiasshort QT, arrhytmias

2.10.2009 ellyte.ppt 42
MAGNESIUM 60 % 60 % in bones, higher in in bones, higher in ICFICF than in ECF than in ECF OnlyOnly 0,3 % 0,3 % in blood,in blood, 30% prote 30% proteiinn bound bound SerumSerum 0,7 – 1,0 mmol/l 0,7 – 1,0 mmol/l Regulator is not knownRegulator is not known! ! adadrerenal medullanal medulla, in, inssululiin, n,
parathormparathormoon ???n ??? RegulaRegulatedted resorb resorbtion fromtion from GIT ? GIT ? 8 mmol/d is enough ? Is deficiency common ?8 mmol/d is enough ? Is deficiency common ? Excretion through urine and stoolExcretion through urine and stool

2.10.2009 ellyte.ppt 43
MAGNESIUM
Neuromuscular excitability (inhibition – Neuromuscular excitability (inhibition – mediated through decreased secretion of mediated through decreased secretion of acetylcholine?) acetylcholine?)
Bone structureBone structure Enzyme activity, energy production, Enzyme activity, energy production,
transport mechanisms, ribosomestransport mechanisms, ribosomes Regulation of haemocoagulation and Regulation of haemocoagulation and
membrane functionmembrane function

2.10.2009 ellyte.ppt 44
MAGNESIUM
Cardioprotective antiischemic, antihypoxic Cardioprotective antiischemic, antihypoxic effectseffects
Sedative effect on NSSedative effect on NS AntihypertensiveAntihypertensive AntithromboticAntithrombotic

2.10.2009 ellyte.ppt 45
MAGNESIUM
Deficiency associated with soil and plant deficit Deficiency associated with soil and plant deficit Þ grass tetany of cattle
Some drugs and stress can increase excretion Unhealthy diet (alcohol) High doses of calcium (!)
CONSEQUENCES Spasmophilia is more often a consequence of Mg deficiency
as of Ca Tiredness, irritability, tremor Dysmenorea, preeklampsia arrythmias