2019 health plan guide - premera blue crosswellness tools and resources: employees who feel better...
TRANSCRIPT

2019 Health plan guide
FOR BUSINESSES WITH 1–50 EMPLOYEES

ABOUT PREMERA . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Why businesses choose Premera . . . . . . . . . . . . . . . . . 5
WE’RE IN YOUR CORNER . . . . . . . . . . . . . . . . . . . . . 6
Medical plan support programs . . . . . . . . . . . . . . . . . . . 6
Premera Wellness Program . . . . . . . . . . . . . . . . . . . . . . 7
MEDICAL PLANS . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Plus Bronze plans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
Plus Silver plans. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15
Plus Gold plans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
Plus HSA Qualified Bronze plans . . . . . . . . . . . . . . . . . 20
Plus HSA Qualified Silver plans . . . . . . . . . . . . . . . . . . 22
Plus HSA Qualified Gold plans . . . . . . . . . . . . . . . . . . . 24
Select HSA Qualified Bronze 5250 . . . . . . . . . . . . . . . . 25
Select Silver 3000 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26
Select Gold 1500 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27
DENTAL PLANS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Adult Core Dental . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31
Adult Dental Optima™ . . . . . . . . . . . . . . . . . . . . . . . . . . .32
Adult Dental Optima™ Voluntary . . . . . . . . . . . . . . . . . 33
Optional orthodontic coverage . . . . . . . . . . . . . . . . . . . 34
VISION PLANS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Premera’s adult vision plans . . . . . . . . . . . . . . . . . . . . . 36
Table of contents

Included in this guide are your 2019 plan options for:
MEDICAL | PHARMACY | DENTAL | VISION
We care for our customersThe customer is at the center of all we do—that’s why we offer plans that help you keep control of your expenses while giving your employees access to quality and affordable care.
4
Network strength provides choice and savings
• We offer an extensive provider network built for quality and value.
• Our provider network offers broad access to doctors and hospitals not only in Alaska, but also across the country.
Well-rounded benefits package
• We make it easy for you to attract and retain the best talent with appealing benefits packages that support the whole health of your employees.
• Choose from a range of plans to find the right balance that best fits the needs and budget for both your business and your employees.
Tools and programs for employees
• Our built-in support programs encourage your employees to engage in their healthcare, leading to healthier, happier employees.
• Online tools and apps help your employees find doctors, compare costs of services and medications, access pharmacy information, and review claims.
Administrative ease and support
• Integrate dental and pharmacy with your medical plans and simplify your work by dealing with only one health plan for all your healthcare administration.
• Effortlessly manage your health plans and pay bills online with our secure employer dashboard.
• Get ready-to-share resources that makes understanding benefits simple for you and your employees with the Employee Communications resource center. Log in to your secure employer website to get access.
Why businesses choose Premera
5
As a not-for-profit serving Alaska for over 65 years, we’re committed to having a positive impact in our communities. Through corporate giving, volunteering, and community engagement, we promote new partnerships and solutions to help make healthcare work better for the communities where we live and work.

Virtual care: Video or phone consultations with a Teladoc®* physician are available to your employees any time for a low copay.
24-Hour NurseLine: Free, confidential health advice from a registered nurse, available to your employees 24/7.
Alaska Medical Transportation Benefits: Premera plans include two types of medical transportation benefits to support your employees traveling to get the care they need. Travel is available for serious medical conditions that cannot be treated locally and for certain approved services for elective, non-emergent surgeries.
Wellness tools and resources: Employees who feel better do better. That’s why we offer tools and resources for employers and their employees through the Alaska Wellness Academy.
Low-cost fitness center memberships: Your employees get access to 9,000 fitness centers nationwide for only $25 a month (plus a $25 enrollment fee and applicable taxes).
CareCompass360®: This whole-person approach to health offers support services tailored to the unique needs of your employees who qualify.
Pregnancy and newborn support: Premera’s BestBeginnings Maternity program supports healthy babies and parents with personalized tools and encourages early discovery of high-risk pregnancies. Our program also helps reduce costs associated with high-risk pregnancies or newborns who end up in neonatal intensive care.
Preventive health: Preventive health services are part of every Premera plan. Our secure member website provides your employees with details about what is covered and suggested preventive routine exams, vaccinations, and screenings.
Mobile apps and online tools: Apps and digital tools give your employees more control when it comes to managing their healthcare. They can easily search for doctors, compare costs of services, track medications, review claims, and more.
Premera Pulse: Your employees can stay connected to their health plan benefits by simply activating their Premera Pulse account. With Premera Pulse they’ll receive proactive care notifications that help them take advantage of their health plan benefits and stay on top of recommended care. They can search for high-value doctors nearby, instantly book appointments with select primary care doctors, get timely alerts about their medication lists, and more.
We’re in your corner
All medical plans include these great support programs
*Teladoc is an independent company that provides virtual medical care services on behalf of Premera Blue Cross Blue Shield of Alaska.
6

Every Premera medical plan includes a Wellness Program to support you and your employees. We offer tools and resources that equip you with information to create a culture of well-being within your workplace.
Premera Wellness Program benefits for employers:
• Alaska Wellness Academy gives you tools and resources that equip you with information to create a culture of well-being within your workplace.
• Ready-to-share employee communications that help you deliver wellness tips and information to your employees.
Premera Wellness Program benefits for employees:
Employees get access to an employee assistance program that offers help with mental health, stress, grief and loss, illness or trauma, relationship conflicts, financial guidance, life adjustments, and more through:
• 3 confidential, face-to-face, counseling sessions per issue, free of charge.
• Unlimited access to lifestyle guidance resources with online support and direct access to a guidance consult by phone, online, or through a mobile app.
• Online health tools to set goals, track health information, access health reports, and create personalized wellness plans.
Premera Wellness Program
7

Providernetwork
We believe in working closely with doctors and hospitals to deliver great care for the customer together. That’s why our provider network is more than just a collection of contracts–it gives members access to quality care, good experiences, and services at a fair price.
8

National and worldwide network coverage with BlueCard®
Our large nationwide provider network includes over 1,000,000 providers and 6,900 hospitals. When you choose a Premera Blue Cross Blue Shield of Alaska health plan, it offers specific levels of healthcare benefits wherever your employees live or travel, across the country and worldwide.
Contact your producer or Premera representative for more details and to find out what level of BlueCard healthcare benefits are included in your Premera health plan.
Our broadest provider network offers access to over 4,000 preferred providers and 21 preferred hospitals across Alaska.
Heritage network
9

Medical plans
Premera offers a wide range of bronze, silver, and gold plans. All of these plans offer broad access to doctors and hospitals through the Heritage network as well as pediatric vision and pediatric dental at no additional cost. You can also pair any Premera medical plan with one of our adult dental and/or adult vision plans—allowing you to offer your employees a well-rounded benefits package all in one place.
10

With Premera medical plans, you can help your employees find the right balance between their budget and their healthcare needs.Plus vs. Select plans: Plus plans offer the flexibility of medical plans at all levels. Select plans offer a choice between gold and silver—or just bronze.
PPO plans: All of the medical plans outlined in this guide are preferred provider organization (PPO) plans. PPO plans work with a network of participating providers to deliver quality care at lower costs.
HSA-qualified plans: Health savings account (HSA)–qualified plans offer valuable benefits for covered services and are qualified to work in combination with an employee-owned, tax-advantaged HSA. The plans offer the option for ConnectYourCare (an independent company that administers HSA accounts for Premera customers at a federally insured bank).
Here’s one way your employees can save:When you choose a Plus or Select PPO medical plan your employees may get some office visits covered in full as well as lower copays if they designate an in-network primary care provider (PCP). These office visits are in addition to a no-cost visit for preventive services. Speak with your producer for complete details.
PLUS PPO SELECT PPO PLUS HSA SELECT HSA
PLAN TYPE
PPO plan X X X X
HSA-qualified with the option of ConnectYourCare X X
NETWORK
Heritage X X X X
LEVELS
Gold X X X
Silver X X X
Bronze X X X
DENTAL
Pediatric X X X X
Adult OPTIONAL BENEFIT ENHANCEMENT
VISION
Pediatric X X X X
Adult OPTIONAL BENEFIT ENHANCEMENT
Check out Premera’s adult dental plans on the following pages.
Together, Premera’s medical and dental plans encourage healthy habits and better outcomes, provide a robust network of providers, and make it easy and simple so you can take great care of your employees.
11

Plus Bronze 5500Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS BRONZE 5500
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) $5,500 2x individual deductible
Coinsurance Amount you pay after your deductible is met 30% 40% 60%
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copays Family = 2x individual out-of-pocket maximum $7,900 $45,000
Office visits Designated primary care provider (PCP) office visit $55 Deductible, then 40% Deductible, then 60%
Non-designated PCP or specialist office visit $110Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES1 Ambulatory
patient services Outpatient services Deductible, then 30%Deductible, then 40% Deductible, then 60%
Office visits Spinal manipulation (12 visits PCY); Acupuncture (12 visits PCY) $55
2 Emergency services Emergency care Copay waived if directly admitted to inpatient facility $250 copay, then in-network deductible and coinsurance
Ambulance transportation (air and ground)$25 copay,
then deductible andin-network coinsurance
Emergent: Same as in-networkNon-emergent: Air – Ded, then 40% / Ded, then 60%;
Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 30%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 30% Deductible, then 40% Deductible, then 60%
5 Mental health and substance use disorder services, including behavioral health treatment
Office visit $110
Deductible, then 40% Deductible, then 60%Inpatient hospital: mental and behavioral health
Deductible, then 30%Outpatient services
6 Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY Deductible, then 30%
Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY Deductible, then $110
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY Deductible, then 30%
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 30% Deductible, then 40% Deductible, then 60%
8 Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9 Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions)
Deductible waived, then 30% Deductible waived, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Retail up to 90-day supply (3x 30-day supply cost) $25 / Ded $85 / Ded $175
Retail and specialty: Same as in-network
Mail Order: Not covered
Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
Mail order 90-day supply; 3x retail supply cost $75/ Ded $255/ Ded $525
Specialty Rx 30-day supplyDed 40%
Drug formulary M4ADDITIONAL BENEFIT EMBEDDED WITHIN THE MEDICAL PLAN
Hearing Hearing exam: 1 per 2 calendar yearsDeductible waived, then 20%
Hearing aids and hardware: $3,000 every 3 calendar years
Teladoc A full list of services is available on premera.com/ak/member $20 Not covered
12

Plus Bronze 6350Medical plan for 1–50 employees starting January 1, 2019 The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS BRONZE 6350
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) $6,350 2x individual deductible
Coinsurance Amount you pay after your deductible is met 30% 40% 60%
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copays Family = 2x Individual out-of-pocket maximum $7,900 $45,000
Office visits Designated primary care provider (PCP) office visit $55Deductible, then 40% Deductible, then 60%
Non-designated PCP or specialist office visit $110
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS COVERED SERVICES1 Ambulatory
patient servicesOutpatient services Deductible, then 30%
Deductible, then 40% Deductible, then 60%Office visits Spinal manipulation (12 visits PCY);
Acupuncture (12 visits PCY) $55
2 Emergency services Emergency care Copay waived if directly admitted to inpatient facility $250 copay, then in-network deductible and coinsurance
Ambulance transportation (air and ground)$25 copay,
then deductible andin-network coinsurance
Emergent: Same as in-networkNon-emergent: Air – Ded, then 40% / Ded, then 60%;
Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 30%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 30% Deductible, then 40% Deductible, then 60%
5 Mental health and substance use disorder services, including behavioral health treatment
Office visit $110
Deductible, then 40% Deductible, then 60%Inpatient hospital: mental and behavioral healthDeductible, then 30%
Outpatient services
6 Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY Deductible, then 30%
Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY Deductible, then $110
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY Deductible, then 30%
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 30% Deductible, then 40% Deductible, then 60%
8 Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9 Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25Eyewear: One pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: Pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full
Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions)
Deductible waived, then 30% Deductible waived, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Retail up to 90-day supply (3x 30-day supply cost)Mail Order 90-day supply; 3x retail supply costSpecialty Rx 30-day supplyDrug Formulary M4
$25/Ded, $85/Ded, $175
Retail and specialty: Same as in-network Mail order: not covered
$75/Ded, $255/Ded, $525Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
Deductible, then 40%
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible waived, then 20%
Teladoc A full list of services is available on premera.com/ak/member $20 Not covered
13

Plus Bronze 7900Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS BRONZE 7900
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) $7,900 2x individual deductible
Coinsurance Amount you pay after your deductible is met 0% 40% 60%
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copays Family = 2x individual out-of-pocket maximum $7,900 $45,000
Office visits Cost share Deductible, then 0% Deductible, then 40% Deductible, then 60%
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES 1 Ambulartory patient
services office visits
Outpatient servicesDeductible, then 0% Deductible, then 40% Deductible, then 60%Spinal manipulation (12 visits PCY);
Acupuncture (12 visits PCY)
2 Emergency services Emergency care Copay waived if directly admitted to inpatient facility $250 copay, then in-network deductible and coinsurance
Ambulance transporation (air and ground)$25 copay, then
deductible and in-network coinsurance
Emergent: Same as in-network Non-emergent: Air - Ded, then 40%/ Ded, then 60%
Ground - Same as in-network
3 Hospitalization Inpatient
Deductible, then 0%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 0% Deductible, then 40% Deductible, then 60%
5 Mental health and substance use disorder services, including behavioral health treatment
Office visit
Deductible, then 0% Deductible, then 40% Deductible, then 60%Inpatient hospital: mental and behavioral health
Outpatient services
6 Rehabilitation and habilitative services and devices Therapy Rehabilitation and habilitative therapy benefits have the same numberof visits, but are counted seperately
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY
Deductible, then 0% Deductible, then 40% Deductible, then 60%
Physical, speech, occupational, massage therapy: 45 visits PCY
Durable medical equipment Skilled nursing facility: 60 days PCY
7 Laboratory services Includes x-ray, pathology, imaging/diagnostics, MRI, CT, PET (pre-approval required for certain services) Deductible, then 0% Deductible, then 40% Deductible, then 60%
8 Preventive/wellness services and chronic disease management
Screenings, exams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9 Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25
Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contracts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays)
Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions)
Deductible waived, then 30% Deductible waived, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
Retail: up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M1
Deductible, then 0% Retail and specialty: Same as in-network Mail order: not covered
ADDITIONAL BENEFIT EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years
Deductible waived, then 20%
Teladoc $20 Not covered
14

Plus Silver 2000Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS SILVER 2000
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) $2,000 2x individual deductible
Coinsurance Amount you pay after your deductible is met 30% 40% 60%
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum $7,900 $45,000
Office visits Designated primary care provider (PCP) office visit$35 copay
First 2 PCP visits covered in full Deductible, then 40% Deductible, then 60%
Non-designated PCP or specialist office visit $75
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES1 Ambulatory
patient servicesOutpatient services Deductible, then 30%
Deductible, then 40% Deductible, then 60%Office visits Spinal manipulation (12 visits PCY);
Acupuncture (12 visits PCY) $35
2 Emergency services Emergency care $250 copay, then in-network deductible and coinsurance
Ambulance transportation (air and ground)$25 copay,
then deductible andin-network coinsurance
Emergent: Same as in-networkNon-emergent: Air – Ded, then 40% / Ded, then 60%;
Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 30%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 30% Deductible, then 40% Deductible, then 60%
5 Mental health and substance use disorder services, including behavioral health treatment
Office visit $75
Deductible, then 40% Deductible, then 60%Inpatient hospital: mental and behavioral healthDeductible, then 30%
Outpatient services
6 Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY Deductible, then 30%
Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY Deductible, then $75
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY Deductible, then 30%
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 30% Deductible, then 40% Deductible, then 60%
8 Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9 Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions)
Deductible waived, then 30% Deductible waived, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Retail up to 90-day supply (3x 30 day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M4
$25/$65/$150
Retail and specialty: Same as in-network Mail order: not covered
Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
$75/$195/$450
Deductible, then 40%
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible waived, then 20%
Teladoc A full list of services is available on premera.com/ak/member $20 Not covered
15

Plus Silver 2500Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS SILVER 2500
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) $2,500 2x individual deductible
Coinsurance Amount you pay after your deductible is met 30% 40% 60%
Out-of-pocket maximum
Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum $7,900 $45,000
Office visits Designated primary care provider (PCP) office visit$35 copay
First 2 PCP visits covered in full Deductible, then 40% Deductible, then 60%
Non-designated PCP or specialist office visit $75
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES1 Ambulatory
patient servicesOutpatient services Deductible, then 30%
Deductible, then 40% Deductible, then 60%Office visits Spinal manipulation (12 visits PCY);
Acupuncture (12 visits PCY) $35
2 Emergency services Emergency careCopay waived if directly admitted to inpatient facility $250 copay, then in-network deductible and coinsurance
Ambulance transportation (air and ground)$25 copay,
then deductible andin-network coinsurance
Emergent: Same as in-networkNon-emergent: Air – Ded, then 40% / Ded, then 60%;
Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 30%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 30% Deductible, then 40% Deductible, then 60%
5 Mental health and substance use disorder services, including behavioral health treatment
Office visit $75
Deductible, then 40% Deductible, then 60%Inpatient hospital: mental and behavioral healthDeductible, then 30%
Outpatient services
6 Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY Deductible, then 30%
Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY Deductible, then $75
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY Deductible, then 30%
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 30% Deductible, then 40% Deductible, then 60%
8 Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9 Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions)
Deductible waived, then 30% Deductible waived, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M4
$25/$65/$150
Retail and specialty: Same as in-network Mail order: not covered
Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
$75/$195/$450
Deductible, then 40%
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible waived, then 20%
Teladoc A full list of services is available on premera.com/ak/member $20 Not covered
16
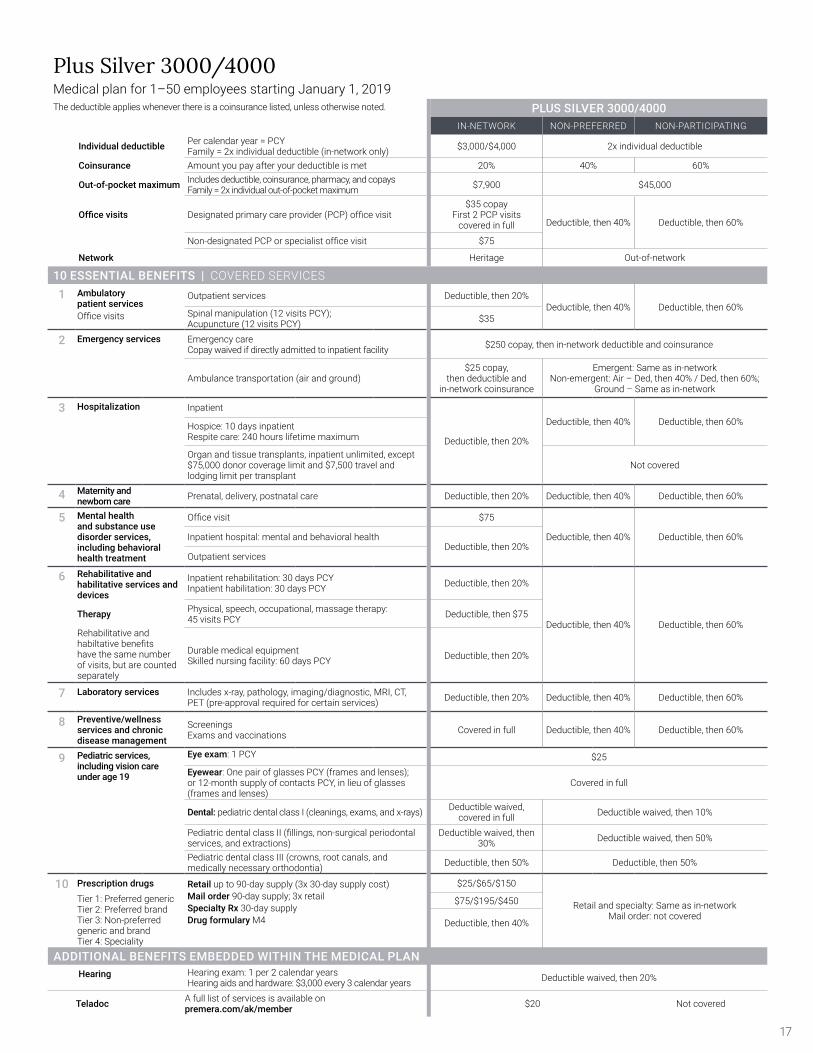
Plus Silver 3000/4000Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS SILVER 3000/4000
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) $3,000/$4,000 2x individual deductible
Coinsurance Amount you pay after your deductible is met 20% 40% 60%
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum $7,900 $45,000
Office visits Designated primary care provider (PCP) office visit$35 copay
First 2 PCP visits covered in full Deductible, then 40% Deductible, then 60%
Non-designated PCP or specialist office visit $75
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES1 Ambulatory
patient servicesOutpatient services Deductible, then 20%
Deductible, then 40% Deductible, then 60%Office visits Spinal manipulation (12 visits PCY);
Acupuncture (12 visits PCY) $35
2 Emergency services Emergency careCopay waived if directly admitted to inpatient facility $250 copay, then in-network deductible and coinsurance
Ambulance transportation (air and ground)$25 copay,
then deductible andin-network coinsurance
Emergent: Same as in-networkNon-emergent: Air – Ded, then 40% / Ded, then 60%;
Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 20%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 20% Deductible, then 40% Deductible, then 60%
5 Mental health and substance use disorder services, including behavioral health treatment
Office visit $75
Deductible, then 40% Deductible, then 60%Inpatient hospital: mental and behavioral healthDeductible, then 20%
Outpatient services
6 Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY Deductible, then 20%
Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY Deductible, then $75
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY Deductible, then 20%
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 20% Deductible, then 40% Deductible, then 60%
8 Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9 Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25Eyewear: One pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions)
Deductible waived, then 30% Deductible waived, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M4
$25/$65/$150
Retail and specialty: Same as in-network Mail order: not covered
Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
$75/$195/$450
Deductible, then 40%
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible waived, then 20%
Teladoc A full list of services is available on premera.com/ak/member $20 Not covered
17

Plus Gold 500Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS GOLD 500
IN-NETWORK NON-PREFERRED NONPARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) $500 2x individual deductible
Coinsurance Amount you pay after your deductible is met 20% 40% 60%Out-of-pocket maximum
Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum $6,000 $45,000
Office visits Designated primary care provider (PCP) office visit$25 copay
First 2 PCP visits covered in full Deductible, then 40% Deductible, then 60%
Non-designated PCP or specialist office visit $50
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES1 Ambulatory
patient servicesOutpatient services Deductible, then 20%
Deductible, then 40% Deductible, then 60%Office visits
Spinal manipulation (12 visits PCY); Acupuncture (12 visits PCY) $25
2 Emergency services Emergency careCopay waived if directly admitted to inpatient facility $250 copay, then in-network deductible and coinsurance
Ambulance transportation (air and ground)$25 copay,
then deductible andin-network coinsurance
Emergent: Same as in-networkNon-emergent: Air – Ded, then 40% / Ded, then 60%;
Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 20%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 20% Deductible, then 40% Deductible, then 60%
5 Mental health and substance use disorder services, including behavioral health treatment
Office visit $50
Deductible, then 40% Deductible, then 60%Inpatient hospital: mental and behavioral healthDeductible, then 20%
Outpatient services
6 Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY Deductible, then 20%
Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY Deductible, then $50
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY Deductible, then 20%
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 20% Deductible, then 40% Deductible, then 60%
8 Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9 Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions)
Deductible waived, then 30% Deductible waived, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Tier 1: Preferred generic Tier 2: Preferred brand Tier 3: Non-preferred generic and brand Tier 4: Speciality
Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M4
$20/$40/$100
Retail and specialty: Same as in-networkMail order: not covered
$60/$120/$300
Deductible, then 20%
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible waived, then 20%
Teladoc A full list of services is available on premera.com/ak/member $20 Not covered
18

Plus Gold 1000/1500Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS GOLD 1000/1500
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) $1,000/$1,500 2x individual deductible
Coinsurance Amount you pay after your deductible is met 20% 40% 60%
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum $6,000 $45,000
Office visits Designated primary care provider (PCP) office visit$25 copay
First 2 PCP visits covered in full Deductible, then 40% Deductible, then 60%
Non-designated PCP or specialist office visit $50
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES1 Ambulatory
patient servicesOutpatient services Deductible, then 20%
Deductible, then 40% Deductible, then 60%Office Visits Spinal manipulation (12 visits PCY);
Acupuncture (12 visits PCY) $25
2 Emergency services Emergency careCopay waived if directly admitted to inpatient facility $250 Copay, then in-network deductible and coinsurance
Ambulance transportation (air and ground)$25 copay,
then deductible andin-network coinsurance
Emergent: Same as in-networkNon-emergent: Air – Ded, then 40% / Ded, then 60%;
Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 20%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 20% Deductible, then 40% Deductible, then 60%
5 Mental health and substance use disorder services, including behavioral health treatment
Office visit $50
Deductible, then 40% Deductible, then 60%Inpatient hospital: mental and behavioral healthDeductible, then 20%
Outpatient services
6Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY Deductible, then 20%
Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY Deductible, then $50
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY Deductible, then 20%
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 20% Deductible, then 40% Deductible, then 60%
8Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9 Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25
Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions)
Deductible waived, then 30% Deductible waived, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M4
$10/$40/$100
Retail and specialty: Same as in-network Mail order: not covered
Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
$30/$120/$300
Deductible, then 20%
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible waived, then 20%
Teladoc A full list of services is available on premera.com/ak/member $20 Not covered
19
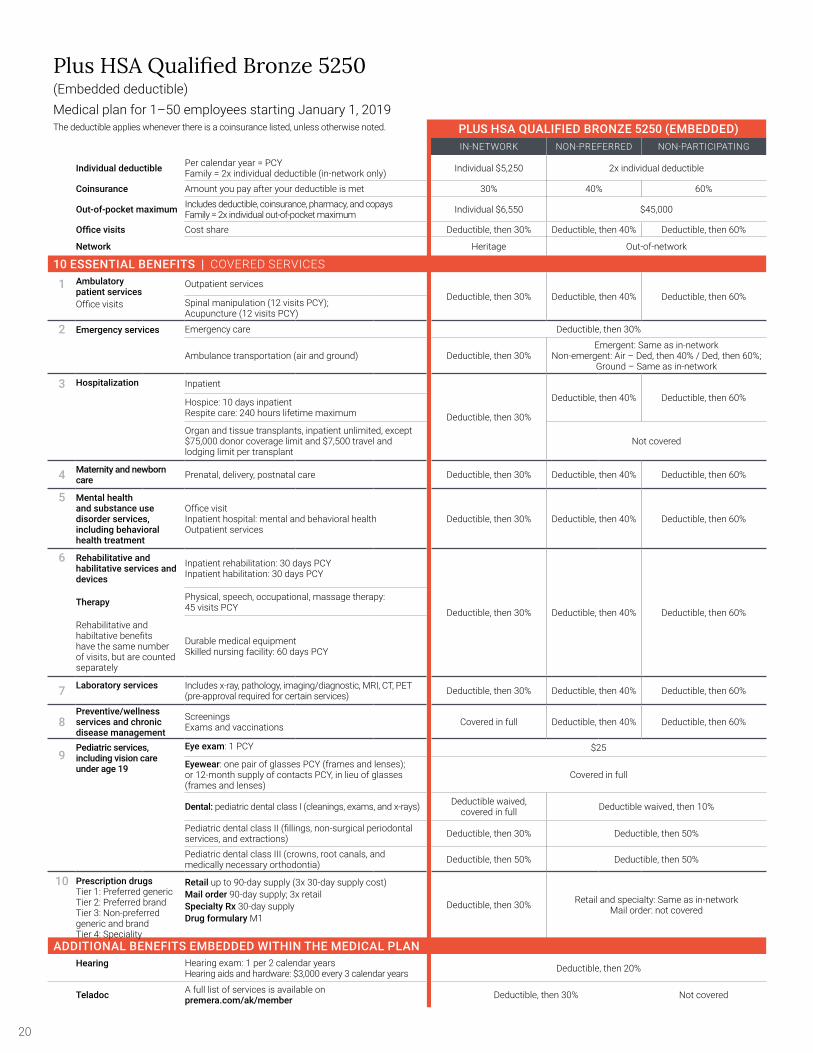
Plus HSA Qualified Bronze 5250(Embedded deductible)Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS HSA QUALIFIED BRONZE 5250 (EMBEDDED)
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) Individual $5,250 2x individual deductible
Coinsurance Amount you pay after your deductible is met 30% 40% 60%
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum Individual $6,550 $45,000
Office visits Cost share Deductible, then 30% Deductible, then 40% Deductible, then 60%
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES1 Ambulatory
patient servicesOutpatient services
Deductible, then 30% Deductible, then 40% Deductible, then 60%Office visits Spinal manipulation (12 visits PCY);
Acupuncture (12 visits PCY)
2 Emergency services Emergency care Deductible, then 30%
Ambulance transportation (air and ground) Deductible, then 30%Emergent: Same as in-network
Non-emergent: Air – Ded, then 40% / Ded, then 60%;Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 30%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 30% Deductible, then 40% Deductible, then 60%
5 Mental health and substance use disorder services, including behavioral health treatment
Office visitInpatient hospital: mental and behavioral healthOutpatient services
Deductible, then 30% Deductible, then 40% Deductible, then 60%
6 Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY
Deductible, then 30% Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 30% Deductible, then 40% Deductible, then 60%
8Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25
Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions) Deductible, then 30% Deductible, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugsTier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M1
Deductible, then 30% Retail and specialty: Same as in-network Mail order: not covered
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible, then 20%
Teladoc A full list of services is available on premera.com/ak/member Deductible, then 30% Not covered
20

Plus HSA Qualified Bronze 6000(Embedded deductible)Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS HSA QUALIFED BRONZE 6000 (EMBEDDED)
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) Individual: $6,000 2x individual deductible
Coinsurance Amount you pay after your deductible is met 30% 40% 60%Out-of-pocket maximum
Includes deductible, coinsurance, pharmacy, and copays Family = 2x individual out-of-pocket maximum Individual: $6,650 $45,000
Office visits Cost share Deductible, then 30% Deductible, then 40% Deductible, then 60%
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES
1 Ambulartory patient services Office visits
Outpatient servicesSpinal manipulation (12 visits PCY); Acupuncture (12 visits PCY)
Deductible, then 30% Deductible, then 40% Deductible, then 60%
2 Emergency services Emergency care. Copay waived if directly admitted to inpatient facility Deductible, then 30%
Ambulance transporation (air and ground) Deductible, then 30%Emergent: Same as in-network
Non-emergent: Air - Ded, then 40%/ Ded, then 60% Ground - Same as in-network
3 Hospitalization Inpatient
Deductible, then 30%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 30% Deductible, then 40% Deductible, then 60%
5 Mental health and substance use disorder services, including behavioral health treatment
Office visitInpatient hospital: mental and behavioral healthOutpatient services
Deductible, then 30% Deductible, then 40% Deductible, then 60%
6 Rehabilitation and habilitative services and devices
Therapy Rehabilitation and habilitative benefits have the same number of visits, but are counted seperately
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY
Deductible, then 30% Deductible, then 40% Deductible, then 60%Physical, speech, occupational, massage therapy: 45 visits PCY
Durable medical equipment Skilled nursing facility: 60 days PCY
7 Laboratory services Includes x-ray, pathology, imaging/diagnostics, MRI, CT, PET (pre-approval required for certain services) Deductible, then 30% Deductible, then 40% Deductible, then 60%
8 Preventive/wellness services and chronic-disease management
Screenings Exams and vaccinations Deductible, then 30% Deductible, then 40% Deductible, then 60%
9 Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25
Eyewear: One pair of glasses PCY (frames and lenses); or 12-month supply of contracts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions) Deductible, then 30% Deductible, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
Retail: up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M1
Deductible, then 30% Retail and specialty: Same as in-network Mail order: not covered
ADDITIONAL BENEFIT EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible, then 20%
Teladoc Deductible, then 30% Not covered
21

Plus HSA Qualified Silver 2700(Embedded deductible)Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS HSA QUALIFIED SILVER 2700 (EMBEDDED)
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) Individual $2,700 2x individual deductible
Coinsurance Amount you pay after your deductible is met 25% 40% 60%
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum Individual $5,400 $45,000
Office visits Cost share Deductible, then 25% Deductible, then 40% Deductible, then 60%
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES
1 Ambulatory patient services Outpatient services
Deductible, then 25% Deductible, then 40% Deductible, then 60%Office visits Spinal manipulation (12 visits PCY);
Acupuncture (12 visits PCY)
2 Emergency services Emergency care Deductible, then 25%
Ambulance transportation (air and ground) Deductible, then 25%Emergent: Same as in-network
Non-emergent: Air – Ded, then 40% / Ded, then 60%;Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 25%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 25% Deductible, then 40% Deductible, then 60%
5
Mental health and substance use disorder services, including behavioral health treatment
Office visitInpatient hospital: mental and behavioral healthOutpatient services
Deductible, then 25% Deductible, then 40% Deductible, then 60%
6Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY
Deductible, then 25% Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 25% Deductible, then 40% Deductible, then 60%
8Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays)
Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions) Deductible, then 30% Deductible, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugsTier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M1
Deductible, then 25% Retail and specialty: Same as in-network Mail order: not covered
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible, then 20%
Teladoc A full list of services is available on premera.com/ak/member Deductible, then 25% Not covered
22

Plus HSA Qualified Silver 3500(Embedded deductible)Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS HSA QUALIFIED SILVER 3500 (EMBEDDED)
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) Individual $3,500 2x individual deductible
Coinsurance Amount you pay after your deductible is met 20% 40% 60%
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum Individual $5,000 $45,000
Office visits Cost share Deductible, then 20% Deductible, then 40% Deductible, then 60%
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES1 Ambulatory
patient servicesOutpatient services
Deductible, then 20% Deductible, then 40% Deductible, then 60%Office Visits Spinal manipulation (12 visits PCY);
Acupuncture (12 visits PCY)
2 Emergency services Emergency care Deductible, then 20%
Ambulance transportation (air and ground) Deductible, then 20%Emergent: Same as in-network
Non-emergent: Air – Ded, then 40% / Ded, then 60%;Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 20%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 20% Deductible, then 40% Deductible, then 60%
5
Mental health and substance use disorder services, including behavioral health treatment
Office visitInpatient hospital: mental and behavioral healthOutpatient services
Deductible, then 20% Deductible, then 40% Deductible, then 60%
6Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY
Deductible, then 20% Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 20% Deductible, then 40% Deductible, then 60%
8Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25
Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays)
Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions) Deductible, then 30% Deductible, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M1
Deductible, then 20% Retail and specialty: Same as in-network Mail order: not covered
Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible, then 20%
Teladoc A full list of services is available on premera.com/ak/member Deductible, then 20% Not covered
23

Plus HSA Qualified Gold 1500(Aggregate deductible)Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. PLUS HSA QUALIFIED GOLD 1500 (AGGREGATE)
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (aggregate ) Individual: $1,500 2x individual deductible
Coinsurance Amount you pay after your deductible is met 20% 40% 60%
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum (aggregate) Individual: $3,000 $45,000
Office visits Cost share Deductible, then 20% Deductible, then 40% Deductible, then 60%
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES1 Ambulatory
patient services Outpatient servicesDeductible, then 20% Deductible, then 40% Deductible, then 60%
Office visits Spinal manipulation (12 visits PCY); Acupuncture (12 visits PCY)
2 Emergency services Emergency care Deductible, then 20%
Ambulance transportation (air and ground) Deductible, then 20%Emergent: Same as in-network
Non-emergent: Air – Ded, then 40% / Ded, then 60%;Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 20%
Deductible, then 40% Deductible, then 60%Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 20% Deductible, then 40% Deductible, then 60%
5
Mental health and substance use disorder services, including behavioral health treatment
Office visitInpatient hospital: mental and behavioral healthOutpatient services
Deductible, then 20% Deductible, then 40% Deductible, then 60%
6Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY
Deductible, then 20% Deductible, then 40% Deductible, then 60%Therapy Physical, speech, occupational, massage therapy:
45 visits PCY
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 20% Deductible, then 40% Deductible, then 60%
8Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full Deductible, then 40% Deductible, then 60%
9
Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25
Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions) Deductible, then 30% Deductible, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugsTier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M1
Deductible, then 20% Retail and specialty: Same as in-network Mail order: not covered
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible, then 20%
Teladoc A full list of services is available on premera.com/ak/member Deductible, then 20% Not covered
24

Select HSA Qualified Bronze 5250(Embedded deductible)Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. SELECT HSA QUALIFIED BRONZE (EMBEDDED)
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) Individual $5,250 2x individual deductible
Coinsurance Amount you pay after your deductible is met 30% Hospital: 40% Hospital: 60%
All other facilities and professional: Same as in-network
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum Individual $6,550 $45,000
Office visits Cost share Deductible, then 30% Same as in-network
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES
1 Ambulatory patient services
Outpatient servicesDeductible, then 30%
Hospital: Deductible, then 40%
Hospital: Deductible, then 60%
Office visits Spinal manipulation (12 visits PCY); Acupuncture (12 visits PCY) All other facilities and professional: Same as in-network
2 Emergency services Emergency care Deductible, then 30%
Ambulance transportation (air and ground) Deductible, then 30%Emergent: Same as in-network
Non-emergent: Air – Ded, then 40% / Ded, then 60%;Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 30%
Hospital:Deductible, then 40%
Hospital:Deductible, then 60%
Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum All other facilities and professional: Same as in-network
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 30%
Hospital: Deductible, then 40%
Hospital:Deductible, then 60%
All other facilities and professional: Same as in-network
5
Mental health and substance use disorder services, including behavioral health treatment
Office visitInpatient hospital: mental and behavioral healthOutpatient services
Deductible, then 30%Deductible, then 40% Deductible, then 60%
All other facilities and professional: Same as in-network
6Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY
Deductible, then 30%
Hospital: Deductible, then 40%
Hospital: Deductible, then 60%
Therapy Physical, speech, occupational, massage therapy: 45 visits PCY
All other facilities and professional: Same as in-network
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 30%
Hospital:Deductible, then 40%
Hospital: Deductible, then 60%
All other facilities and professional: Same as in-network
8Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full
Deductible, then 40% Deductible, then 60%
All other facilities and professional: Same as in-network
9Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25
Eyewear: One pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: Pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions) Deductible, then 30% Deductible, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M1
Deductible, then 30% Retail and specialty: Same as in-network Mail order: not covered
Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible, then 20%
Teladoc A full list of services is available on premera.com/ak/member Deductible, then 30% Not covered
25

Select Silver 3000Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. SELECT SILVER 3000
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) $3,000 2x individual deductible
Coinsurance Amount you pay after your deductible is met 30% Hospital: 40% Hospital: 60%
All other facilities and professional: Same as in-network
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum $7,900 $45,000
Office visits Cost share $75 Same as in-network
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES
1 Ambulatory patient services Outpatient services Deductible, then 30% Hospital:
Deductible, then 40%Hospital:
Deductible, then 60%
Office visits Spinal manipulation (12 visits PCY); Acupuncture (12 visits PCY) Office visit cost share All other facilities and professional: Same as in-network
2 Emergency services Emergency careCopay waived if directly admitted to inpatient facility $250 copay, then in-network deductible and coinsurance
Ambulance transportation (air and ground)$25 copay, then
deductible and in-network coinsurance
Emergent: Same as in-networkNon-emergent: Air – Ded, then 40% / Ded, then 60%;
Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 30%
Hospital:Deductible, then 40%
Hospital:Deductible, then 60%
Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum All other facilities and professional: Same as in-network
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4 Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 30%
Hospital: Deductible, then 40%
Hospital:Deductible, then 60%
All other facilities and professional: Same as in-network
5
Mental health and substance use disorder services, including behavioral health treatment
Office visit Office visit cost share Hospital: Deductible, then 40%
Hospital:Deductible, then 60%
Inpatient hospital: mental and behavioral health Deductible, then 30% All other facilities and professional: Same as in-network
6
Rehabilitative and habilitative services and devices
Therapy
Rehabilitative and habilitative benefits have the same number of visits, but are counted separately
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY Deductible, then 30%
Hospital: Deductible, then 40%
Hospital: Deductible, then 60%Physical, speech, occupational, massage therapy:
45 visits PCY Deductible, then $75
Durable medical equipmentDeductible, then 30%
Skilled nursing facility: 60 days PCY All other facilities and professional: Same as in-network
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 30%
Hospital:Deductible, then 40%
Hospital: Deductible, then 60%
All other facilities and professional: Same as in-network
8Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full
Deductible, then 40% Deductible, then 60%
All other facilities and professional: Same as in-network
9Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25
Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions)
Deductible waived, then 30% Deductible waived, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M4
$25/$65/Ded, 50%
Retail and specialty: Same as in-network Mail order: not covered
Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
$75/$195/ Ded, 50%
Deductible, then 30%
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible waived, then 20%
Teladoc A full list of services is available on premera.com/ak/member $20 Not covered
26

Select Gold 1500Medical plan for 1–50 employees starting January 1, 2019The deductible applies whenever there is a coinsurance listed, unless otherwise noted. SELECT GOLD 1500
IN-NETWORK NON-PREFERRED NON-PARTICIPATING
Individual deductible Per calendar year = PCY Family = 2x individual deductible (in-network only) $1,500 2x individual deductible
Coinsurance Amount you pay after your deductible is met 20% Hospital: 40% Hospital: 60%All other facilities and professional: Same as in-network
Out-of-pocket maximum Includes deductible, coinsurance, pharmacy, and copaysFamily = 2x individual out-of-pocket maximum $6,000 $45,000
Office visits Cost share $50 Same as in-network
Network Heritage Out-of-network
10 ESSENTIAL BENEFITS | COVERED SERVICES1 Ambulatory
patient services Outpatient services Deductible, then 20% Hospital: Deductible, then 40%
Hospital: Deductible, then 60%
Office visits Spinal manipulation (12 visits PCY); Acupuncture (12 visits PCY) Office visit cost share All other facilities and professional: Same as in-network
2 Emergency services Emergency careCopay waived if directly admitted to inpatient facility $250 copay, then in-network deductible and coinsurance
Ambulance transportation (air and ground)$25 copay, then
deductible and in-network coinsurance
Emergent: Same as in-networkNon-emergent: Air – Ded, then 40% / Ded, then 60%;
Ground – Same as in-network
3 Hospitalization Inpatient
Deductible, then 20%
Hospital:Deductible, then 40%
Hospital:Deductible, then 60%
Hospice: 10 days inpatient Respite care: 240 hours lifetime maximum All other facilities and professional: Same as in-network
Organ and tissue transplants, inpatient unlimited, except $75,000 donor coverage limit and $7,500 travel and lodging limit per transplant
Not covered
4Maternity and newborn care Prenatal, delivery, postnatal care Deductible, then 20%
Hospital: Deductible, then 40%
Hospital:Deductible, then 60%
All other facilities and professional: Same as in-network
5
Mental health and substance use disorder services, including behavioral health treatment
Office visit Office visit cost shareDeductible, then 40% Deductible, then 60%
Inpatient hospital: mental and behavioral healthDeductible, then 20%
Outpatient services All other facilities and professional: Same as in-network
6Rehabilitative and habilitative services and devices
Inpatient rehabilitation: 30 days PCY Inpatient habilitation: 30 days PCY Deductible, then 20%
Hospital: Deductible, then 40%
Hospital: Deductible, then 60%
Therapy Physical, speech, occupational, massage therapy: 45 visits PCY Deductible, then $50
Rehabilitative and habiltative benefits have the same number of visits, but are counted separately
Durable medical equipmentSkilled nursing facility: 60 days PCY Deductible, then 20% All other facilities and professional: Same as in-network
7 Laboratory services Includes x-ray, pathology, imaging/diagnostic, MRI, CT, PET (pre-approval required for certain services) Deductible, then 20%
Hospital:Deductible, then 40%
Hospital: Deductible, then 60%
All other facilities and professional: Same as in-network
8Preventive/wellness services and chronic disease management
ScreeningsExams and vaccinations Covered in full
Deductible, then 40% Deductible, then 60%
All other facilities and professional: Same as in-network
9Pediatric services, including vision care under age 19
Eye exam: 1 PCY $25Eyewear: one pair of glasses PCY (frames and lenses); or 12-month supply of contacts PCY, in lieu of glasses (frames and lenses)
Covered in full
Dental: pediatric dental class I (cleanings, exams, and x-rays) Deductible waived, covered in full Deductible waived, then 10%
Pediatric dental class II (fillings, non-surgical periodontal services, and extractions)
Deductible waived, then 30% Deductible waived, then 50%
Pediatric dental class III (crowns, root canals, and medically necessary orthodontia) Deductible, then 50% Deductible, then 50%
10 Prescription drugs Retail up to 90-day supply (3x 30-day supply cost)Mail order 90-day supply; 3x retailSpecialty Rx 30-day supplyDrug formulary M4
$10/$40/Ded, 50%
Retail and specialty: Same as in-network Mail order: not covered
Tier 1: Preferred genericTier 2: Preferred brandTier 3: Non-preferred generic and brandTier 4: Speciality
$30/$120/Ded, 50%
Deductible, then 20%
ADDITIONAL BENEFITS EMBEDDED WITHIN THE MEDICAL PLANHearing Hearing exam: 1 per 2 calendar years
Hearing aids and hardware: $3,000 every 3 calendar years Deductible waived, then 20%
Teladoc A full list of services is available on premera.com/ak/member $20 Not covered
27

Dental plans
Good oral health is pivotal to your employee’s overall health. Here’s why : Regular preventive oral health visits assist with early detection and management of diseases. When you offer your employees both dental and medical benefits from Premera, you help encourage healthy habits.
28

Pediatric dental benefits are already included in Premera medical plansYour employees will receive pediatric dental coverage because it’s already embedded in their Premera medical plan. This allows you to provide your employees coverage for essential dental treatments for anyone age 18 or younger.
This embedded benefit includes a range of services from routine dental cleanings and x-rays to root canals and extractions. In addition, this coverage offers:
• The ability to visit any dentist*
• No waiting period
Because pediatric dental just isn’t enough, Premera offers options for adult dental benefitsTo complement the embedded pediatric dental coverage your employees get with their medical plans, we offer adult (anyone age 19 or older) dental options as a great way to provide ample value to your employees’ medical plan.
*Different in-network and out-of-network deductibles and coinsurance apply based on service. Speak to your producer for more details.
29
DENTAL BENEFITS ADULT CORE DENTAL ADULT DENTAL OPTIMA ADULT DENTAL OPTIMA VOLUNTARY
Cost to employer $ $$ $0
Member’s out-of-pocket cost
Member coinsurance is higher when seeing an out-of-network dentist
Member coinsurance is the same for in-network and out-of-network
dentists
Member coinsurance is the same for in-network and out-of-network
dentists
Expanded benefits for Major dental services (such as dentures, bridges, implants, oral and periodontal surgery)
Not covered Covered Covered (implants not included)
Orthodontia1 No option Optional No option
Employee-funded plan2 No No Yes
Note: For a summary of plan benefits and limitations, see plan details to follow. 1 For groups with 26 or more enrolled employees 2 Employer contributes 0%–49% of premium. Minimum enrollment is 2 or 30% of eligible employees (whichever is greater).
CHOOSE BETWEEN TWO ADULT DENTAL OPTIONS:
Adult Core Dental
Adult Core Dental can be paired with any medical plan to provide your employees core dental benefits at a lower cost.
Adult Dental Optima and Adult Dental Optima Voluntary
Adult Dental Optima and Adult Dental Optima Voluntary are separate dental plans. You can pair either of these with your medical plan to provide adult dental coverage and a broader range of services for your employees.
30

Benefits apply after dental calendar year deductible is met, unless otherwise noted. Dental deductible and coinsurance represent member’s cost share
PCY = Per Calendar Year
COVERED SERVICES IN-NETWORK OUT-OF-NETWORK
Individual dental deductible PCY $50
DIAGNOSTIC AND PREVENTIVE
Cleanings 2 PCY
Covered in full Dental deductible waived, then 10%
Routine oral exams 2 PCY
Routine x-rays full mouth: 1 every 60 months / bitewings: 2 PCY to maximum of 4
BASIC
Non-routine, problem-focused, or emergency exams 1 PCY shared limit
Dental deductible, then 30% Dental deductible, then 50%
Non-routine x-rays panoramic 1 every 60 months / periapical unlimited
Fillings once every 24 months
Periodontal maintenance 4 PCY
Periodontics, non-surgical services scaling / root planing 1 per quadrant every 24 months
Endodontics 1 per lifetime
Simple / surgical extractions
General anesthesia
MAJOR
Recementing / repair of crowns 1 every 24 months, 6 months after placement
Dental deductible, then 50% Dental deductible, then 50%Installation of crowns porcelain, ceramic, and metal only, once every 7 years
Build-ups crowns only, 1 every 7 years
ANNUAL DENTAL PLAN MAXIMUM $1,000 PCY
NOTE: Coinsurance amounts based on allowable charges. Balance billing may apply if a provider is not contracting with Premera Blue Cross.
Adult Core DentalWith Adult Core Dental, you can offer your adult employees and their adult dependents the core benefits they need to keep their smiles healthy.
Preventive services like cleanings, routine exams, and routine x-rays are covered in full to help them properly care for their overall health—with no waiting period.
In addition, they will have the freedom to choose any dental care provider, but will enjoy lower overall out-of-pocket costs when that provider is in network.
31
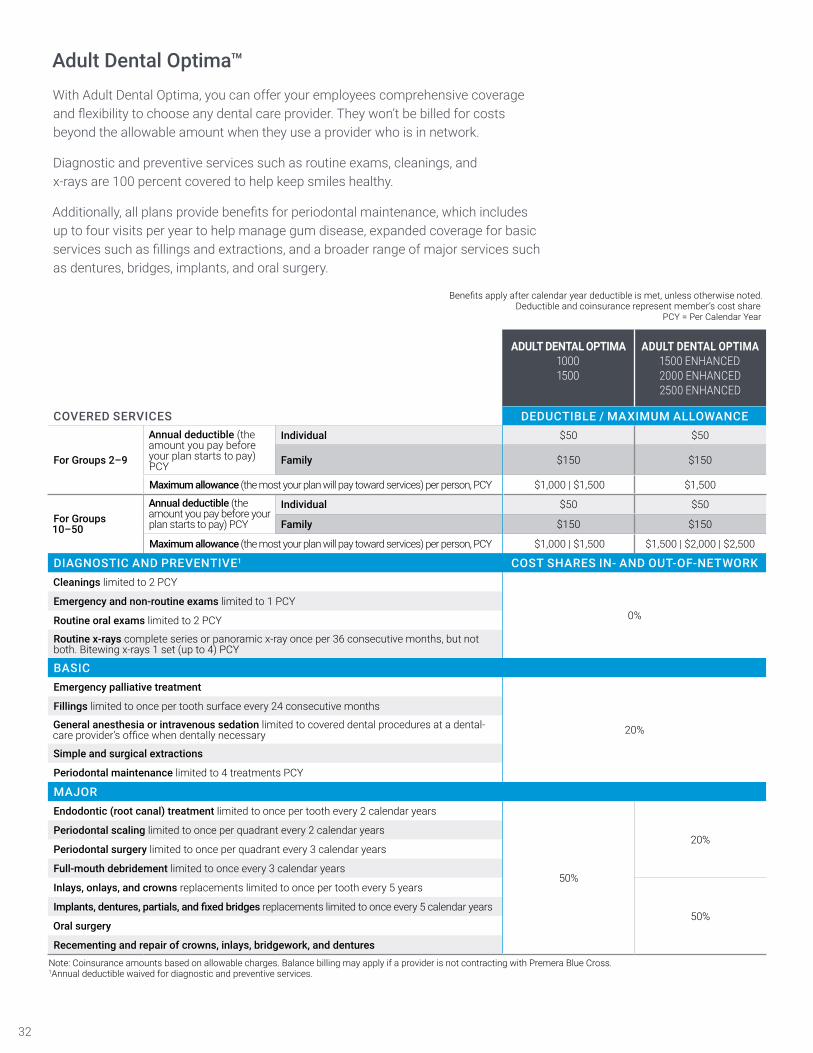
Adult Dental Optima™With Adult Dental Optima, you can offer your employees comprehensive coverage and flexibility to choose any dental care provider. They won’t be billed for costs beyond the allowable amount when they use a provider who is in network.
Diagnostic and preventive services such as routine exams, cleanings, and x-rays are 100 percent covered to help keep smiles healthy.
Additionally, all plans provide benefits for periodontal maintenance, which includes up to four visits per year to help manage gum disease, expanded coverage for basic services such as fillings and extractions, and a broader range of major services such as dentures, bridges, implants, and oral surgery.
Benefits apply after calendar year deductible is met, unless otherwise noted. Deductible and coinsurance represent member’s cost share
PCY = Per Calendar Year
ADULT DENTAL OPTIMA 1000 1500
ADULT DENTAL OPTIMA 1500 ENHANCED2000 ENHANCED 2500 ENHANCED
COVERED SERVICES DEDUCTIBLE / MAXIMUM ALLOWANCE
For Groups 2–9
Annual deductible (the amount you pay before your plan starts to pay) PCY
Individual $50 $50
Family $150 $150
Maximum allowance (the most your plan will pay toward services) per person, PCY $1,000 | $1,500 $1,500
For Groups 10–50
Annual deductible (the amount you pay before your plan starts to pay) PCY
Individual $50 $50
Family $150 $150
Maximum allowance (the most your plan will pay toward services) per person, PCY $1,000 | $1,500 $1,500 | $2,000 | $2,500
DIAGNOSTIC AND PREVENTIVE1 COST SHARES IN- AND OUT-OF-NETWORKCleanings limited to 2 PCY
0%Emergency and non-routine exams limited to 1 PCY
Routine oral exams limited to 2 PCY
Routine x-rays complete series or panoramic x-ray once per 36 consecutive months, but not both. Bitewing x-rays 1 set (up to 4) PCY
BASICEmergency palliative treatment
20%
Fillings limited to once per tooth surface every 24 consecutive months
General anesthesia or intravenous sedation limited to covered dental procedures at a dental-care provider’s office when dentally necessary
Simple and surgical extractions
Periodontal maintenance limited to 4 treatments PCY
MAJOREndodontic (root canal) treatment limited to once per tooth every 2 calendar years
50%
20%Periodontal scaling limited to once per quadrant every 2 calendar years
Periodontal surgery limited to once per quadrant every 3 calendar years
Full-mouth debridement limited to once every 3 calendar years
Inlays, onlays, and crowns replacements limited to once per tooth every 5 years
50%Implants, dentures, partials, and fixed bridges replacements limited to once every 5 calendar years
Oral surgery
Recementing and repair of crowns, inlays, bridgework, and denturesNote: Coinsurance amounts based on allowable charges. Balance billing may apply if a provider is not contracting with Premera Blue Cross.1Annual deductible waived for diagnostic and preventive services.
32

Adult Dental Optima VoluntaryWith Adult Dental Optima Voluntary, you can offer valued dental coverage to your employees and help them save money by funding up to 50 percent of their premiums.
Employees can choose any licensed or certified dental care provider for their care. When they use an in-network provider, they’ll get the dental care they need and won’t be billed for costs beyond the allowable amount.
Diagnostic and preventive services such as routine exams, cleanings, and x-rays are 100 percent covered to help keep their smiles healthy.
Additionally, all plans provide benefits for periodontal maintenance, including up to four visits per year to help manage gum disease, as well as basic and major services such as fillings, extractions, crowns, inlays, and dentures.
Benefits apply after calendar year deductible is met, unless otherwise noted. Deductible and coinsurance represent member’s cost share
PCY = Per Calendar Year
COVERED SERVICES DEDUCTIBLE / MAXIMUM ALLOWANCE
For Groups 2–50Annual deductible PCY
Individual $50
Family $150
Maximum allowance per person, PCY $1,000
COST SHARES IN- AND OUT-OF-NETWORK
DIAGNOSTIC AND PREVENTIVE1
Cleanings limited to 2 PCY
0%Routine oral exams limited to 2 PCY
Routine x-rays complete series or panoramic x-ray once per 36 consecutive months, but not both. Bitewing x-rays 1 set (up to 4) PCY
BASIC
Emergency and non-routine exams limited to 1 PCY
20%
Emergency palliative treatment
Fillings limited to once per tooth surface every 24 consecutive months
Periodontal maintenance limited to 4 visits PCY
General anesthesia or intravenous sedation limited to covered dental procedures at a dental-care provider’s office when dentally necessary
Simple and surgical extractions
MAJOR2
Dentures, partials, and fixed bridges replacements limited to once every 5 calendar years
50%
Endodontic (root canal) treatment limited to once per tooth every 2 calendar years
Full-mouth debridement limited to once every 3 calendar years
Inlays, onlays, and crowns replacements limited to once per tooth every 5 years
Oral surgery
Periodontal scaling once per quadrant every 2 calendar years
Periodontal surgery once per quadrant every 3 calendar years
Recementing and repair of crowns, inlays, bridgework, and dentures
Note: Coinsurance amounts based on allowable charges. Balance billing may apply if a provider is not contracting with Premera Blue Cross Blue Shield of Alaska. 1 Annual deductible waived for diagnostic and preventive services. 2A 12-month waiting period applies to members who have not had continuous comparable dental coverage under the group’s prior dental plan.
33

Optional orthodontic coverage
You can choose to offer additional dental coverage to customize your benefits package.
ADULT DENTAL OPTIMA
ORTHODONTIA1
Diagnostic services and active / retention treatment including appliances 50%1 up to lifetime maximumMonthly orthodontic adjustments including retention treatment
Lifetime maximum per person $1,500
Age limit No age limit
1 Benefits provided at 50% of allowable charges; not subject to deductible or coinsurance. Available only with 26 or more enrolled employees.
Participation and contribution requirements for adult dental plans
Depending on the funding type and group size, there are different options for how much you can choose to contribute to premiums. You must also meet the participation requirements in order to offer the plan.
FUNDING TYPE / GROUP SIZE EMPLOYER CONTRIBUTION PARTICIPATION REQUIREMENTS
Non-voluntary plans 2–4 employees 50%–100% of premium 100% participation
Non-voluntary plans 5–50 employees 50%–100% of premium Minimum of 5 employees or 50% of eligible employees, whichever is greater
Voluntary plan 2–50 employees 0%–49% of premium Minimum of 2 employees or 30% of eligible employees, whichever is greater
34

Vision plans
Routine eye and hearing exams can lead to earlier diagnosis of chronic diseases. Choose the level of vision and hearing coverage that works best for your business and your employees.
35

DENTAL BENEFITS CORE VISION MANDATED OFFERING VISION
Exam Covered in full up to $125 per calendar year 1 visit per calendar year, $25 copay
Eyewear $150 every 2 consecutive calendar years
1 pair of lenses, per calendar year; 1 pair of frames every 2 consecutive calendar years ($90 retail max);
contacts $170 retail max; $350 annual maximum, shared with vision exam
Choose from two adult (anyone age 19 or older) vision plan options:
Offering vision benefits along with medical and dental is easier to manage for both your business and your employees.
In fact, routine eye exams can lead to earlier diagnosis of chronic diseases.
Plus, offering all of your employees’ benefits with Premera means you get the ease of dealing with just one health plan. Your employees and their covered dependents enjoy the simplicity of one card, one customer service phone number, and one website.
36

What our customers say
@premera THANK YOU SO MUCH for helping me get my question answered. Jennifer in Alaska just gave me the info I needed.The gentleman I spoke with was knowledgeable and helpful. Could not have been handled more professionally.Whato remove such a financial hardship. One of the best customer experiences I’ve had over the phone.It’s awesome that they’re actually paying attention, it’s good to know this is a way to reach them. Got the call this morning—issue resolved!We couldn’t have asked for a better person to help us through all we’ve been through with my wife’s strokes.Shout-out to @premera Customer Service rep Carrie in Spokane WA for helping me w/my insurance. #insurance #premera #bestcustomerserviceI felt so helpless, but now I feel like I have help.I have faith that Adrian will have the issue resolved today. He promised me a card and the numbers I need

This brochure is not a contract. It is only a summary of the major benefits provided by these plans. For full coverage provisions, including a description of waiting periods, limitations, and exclusions, please contact your Premera representative or producer.
Find out
Visit premera.com/ak/employer.
Talk with your Premera representative or producer.
027474 (10-04-2018)