2018 practice improvement program (pip) orientation
TRANSCRIPT

2018 Practice Improvement Program (PIP) Orientation
January 4th, 2018
San Francisco Health Plan
Practice Improvement Program (PIP)

Practice Improvement Program (PIP)
Leadership Team
Vanessa Pratt Manager, Population Health
Adam Sharma Director, Health Outcomes Improvement
Kanelle Barreiro Program Manager, Pay for Performance
Katherine Quen Specialist, Population Health
James Glauber, Chief Medical Officer

Agenda TIME ITEM
8:30 Welcome Review Agenda and Meeting Objectives
8:40 Program Overview
8:50 Review Changes in 2018 PIP Clinical Quality Domain Data Quality Domain Patient Experience Domain Systems Improvement Domain
9:40 Break
9:50 Review all other measures with no changes in 2018 Small group activity
10:25 Review 2018 Enrollment
10:45 Closing & Evaluation Distribution
Housekeeping
• Webinar will be recorded
• Slides will be sent out after
• Please mute phone lines, *6
• Don’t put phone lines on hold
• Ask questions throughout and at Q&A
• No question is silly

Objectives
• General overview of program
• Review changes and new measures
• Answer questions that will help you be successful

What is PIP?
Incentive program for SFHP Medi-Cal clinics
and medical groups to achieve improvements
in system and health outcomes.
•Comprehensive
•Collaborative
• Standardized
• Incentivizing
• Technical Assistance
PIP Guiding Principles

The History of PIP
2011 Program launch
Reporting only to incentivize
building capacity for reporting data
2013 Stronger commitment to quality-established
clinical thresholds, incentivized outreach
to higher risk populations
2014
2015
2016 Fewer
measures, simpler
deliverables, specialty care
access measures.
2017 Newer measures
were added to the Clinical Quality
domain to increase alignment with
external entities.
2018 New measures were added to the Systems
Improvement domain to support appropriate
utilization of primary care visits and expansion
of the palliative care Medi-Cal benefit.
Strength in Numbers P4P
measures rolled into CQ domain, all participants
held accountable for data quality
measures.
Improving access, narrowing the
number of measures to focus improvement on lowest performing.

PIP Participant Types
Academic Medical
Center (1)
Community Clinic (7)
Clinic-Based RBO (1)
IPA (3)
Individually Contracted
Specialty (1)
Standardized

PIP Incentives
Maximum quarterly payments are allocated based on
capitation and actual member months accrued
during each month of the quarter.
• 18.5% of Medi-Cal capitation
• 5% of Healthy Kids HMO capitation
incentivizing

Quadruple Aim
comprehensive
• Clinical Quality Domain
• Data Quality Domain
• All Domains
• Patient Experience Domain
• Patient Experience Domain
Improving Patient
Experience
Improving
Staff
Satisfaction
Improving Population
Health
Reducing the Per Capita
Cost of Health Care

PIP Measure Development
PIP Participants, SFHP stakeholders, NCQA, HEDIS, QMED, Meaningful
Use, DMHC, DHCS
SFHP Subject Matter Experts
Advisory Committee
collaborative

PIP Reporting Timeline
*Late baseline data submissions jeopardize the PIP database setup. We thank you in advance for your timeliness with your baseline data!
Quarter Quarter End Date Materials Due to SFHP Reporting Period
Enrollment Friday, January 19, 2018* For all measures, the
quarter’s end date serves as
the last day of the reporting
period. Please see each
measure’s specifications for
the first day of the
reporting period.
1 March 31, 2018 Monday, April 30, 2018
2 June 30, 2018 Tuesday, July 31, 2018
3 September 30, 2018 Wednesday, October 31, 2018
4 December 30, 2018 Thursday, January 31, 2019

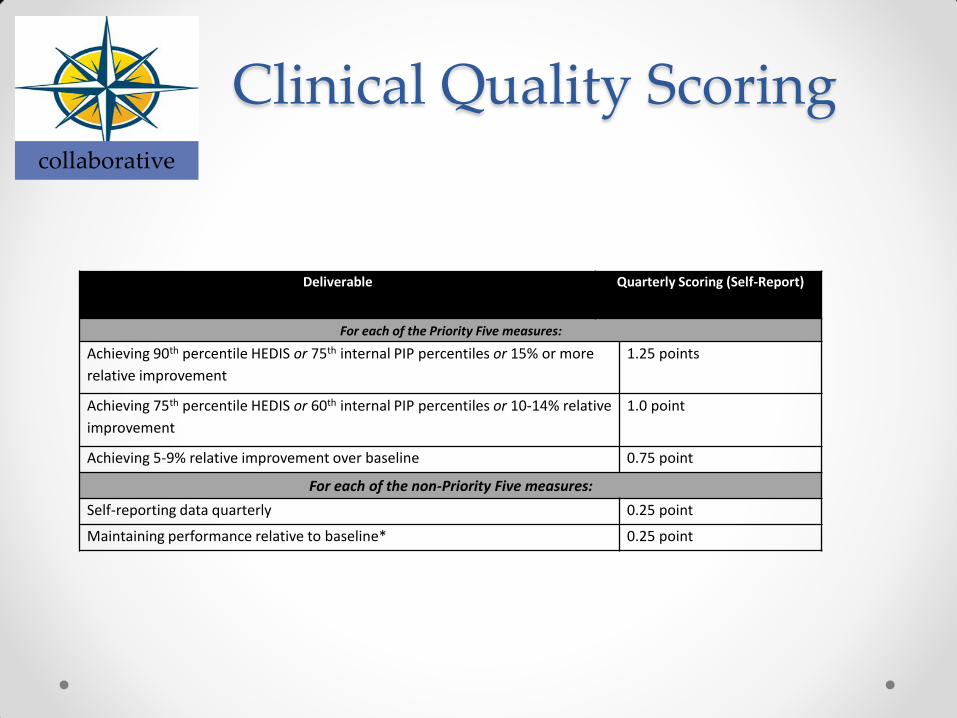
Clinical Quality Scoring collaborative
Deliverable Quarterly Scoring
(Self-Reported Data)
For each of the Priority Five measures:
Achieving 90th percentile HEDIS or 75th internal PIP percentiles or 15% or more
relative improvement
1.25 points
Achieving 75th percentile HEDIS or 60th internal PIP percentiles or 10-14%
relative improvement
1.0 point
Achieving 5-9% relative improvement over baseline 0.75 point
For each of the non-Priority Five measures:
Self-reporting data quarterly 0.25 point
Maintaining performance relative to baseline* 0.25 point

PIP Payment Methodology
• 90‐100% of points = 100% of payment
• 80‐89% of points = 90% of payment
• 70‐79% of points = 80% of payment
• 60‐69% of points = 70% of payment
• 50‐59% of points = 60% of payment
• 40‐49% of points= 50% of payment
• 30‐39% of points= 40% of payment
• 20‐29% of points = 30% of payment
• Less than 20% of points = no payment

Scorecard Review

PIP Website
Technical Assistance http://www.sfhp.org/providers/practice-improvement-
program-pip/
All 2018 measure resources will be listed here

Program Guide
2018 Changes
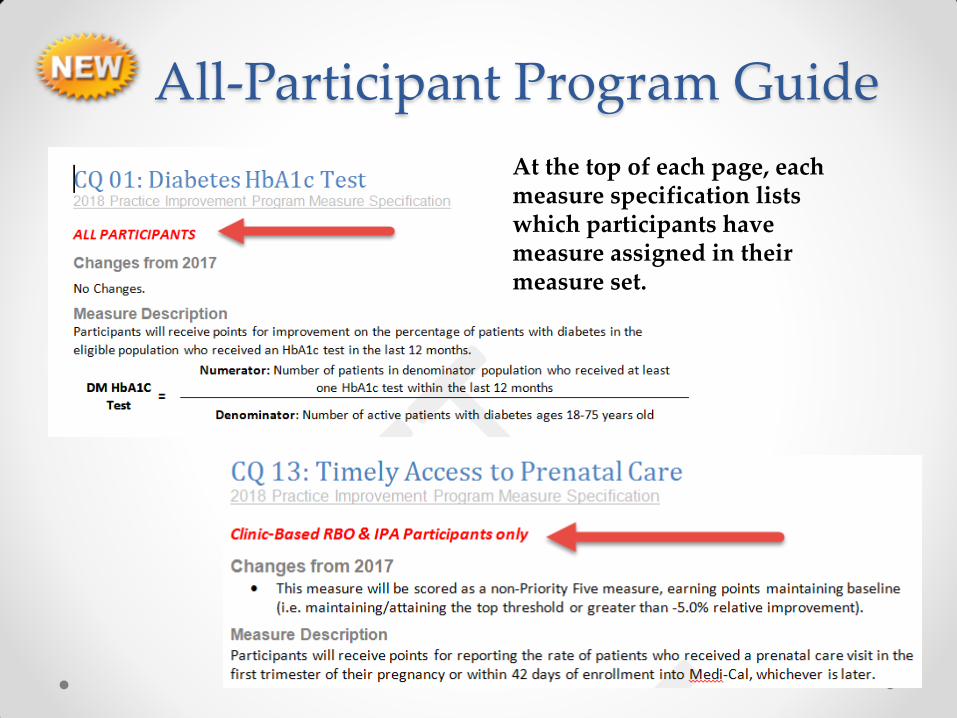
All-Participant Program Guide
At the top of each page, each measure specification lists which participants have measure assigned in their measure set.
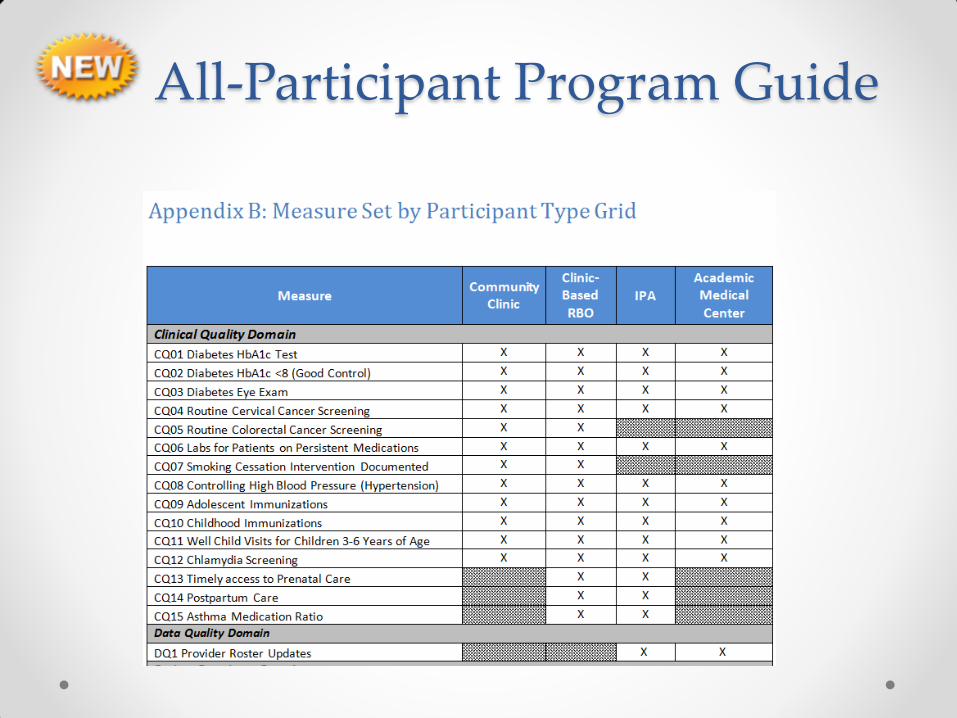
All-Participant Program Guide

Clinical Quality Domain:
2018 Changes

SFHP option discontinued
• Overall, this decision will benefit our provider network in
various ways:
o Fewer charts will be requested from providers during the SFHP
HEDIS pursuit
o Fewer SFHP dollars will be spent on the administration of the HEDIS
pursuit
o Further development of PIP self-reporting capacities
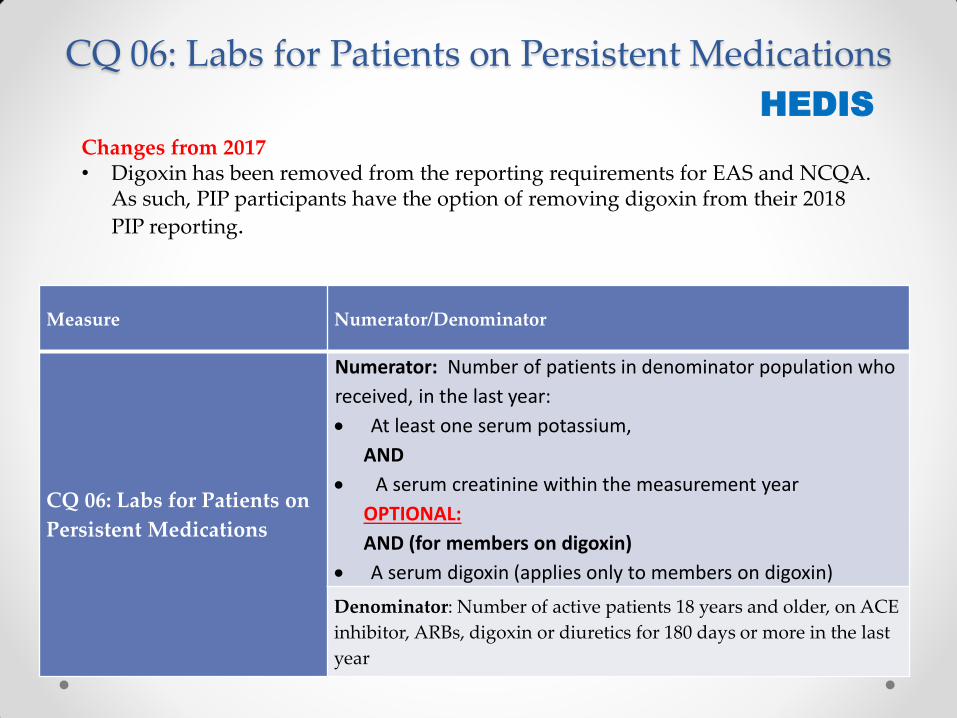
CQ 06: Labs for Patients on Persistent Medications
Measure Numerator/Denominator
CQ 06: Labs for Patients on
Persistent Medications
Numerator: Number of patients in denominator population who
received, in the last year:
At least one serum potassium,
AND
A serum creatinine within the measurement year
OPTIONAL:
AND (for members on digoxin)
A serum digoxin (applies only to members on digoxin)
Denominator: Number of active patients 18 years and older, on ACE
inhibitor, ARBs, digoxin or diuretics for 180 days or more in the last
year
HEDIS
Changes from 2017 • Digoxin has been removed from the reporting requirements for EAS and NCQA.
As such, PIP participants have the option of removing digoxin from their 2018
PIP reporting.

CQ09: Adolescent Immunizations
Measure Numerator/Denominator
CQ09: Adolescent
Immunizations
Numerator: Number of patients in the denominator population who
received one meningococcal vaccine on or between the member’s
11th and 13th birthday and one (Tdap) or (Td) vaccine on or
between the member’s 10th and 13th birthdays, and two HPV
vaccines between the member’s 9th and 13th birthday.
Denominator: Number of active patients who turned 13 years old
during the last year
Changes from 2017 In alignment with clinical guidelines that recommend the inclusion of HPV in the vaccination schedule for adolescents, CQ9 Adolescent Immunizations was replaced by CQ12 Adolescent Immunizations (with HPV).

CQ09: Adolescent Immunizations
Measure 75th percentile 60th percentile
CQ09 Adolescent Immunizations 73.00% 50.40%
Measures without comparable NCQA HEDIS thresholds, a PIP network threshold will be used based on prior year’s PIP participant data:
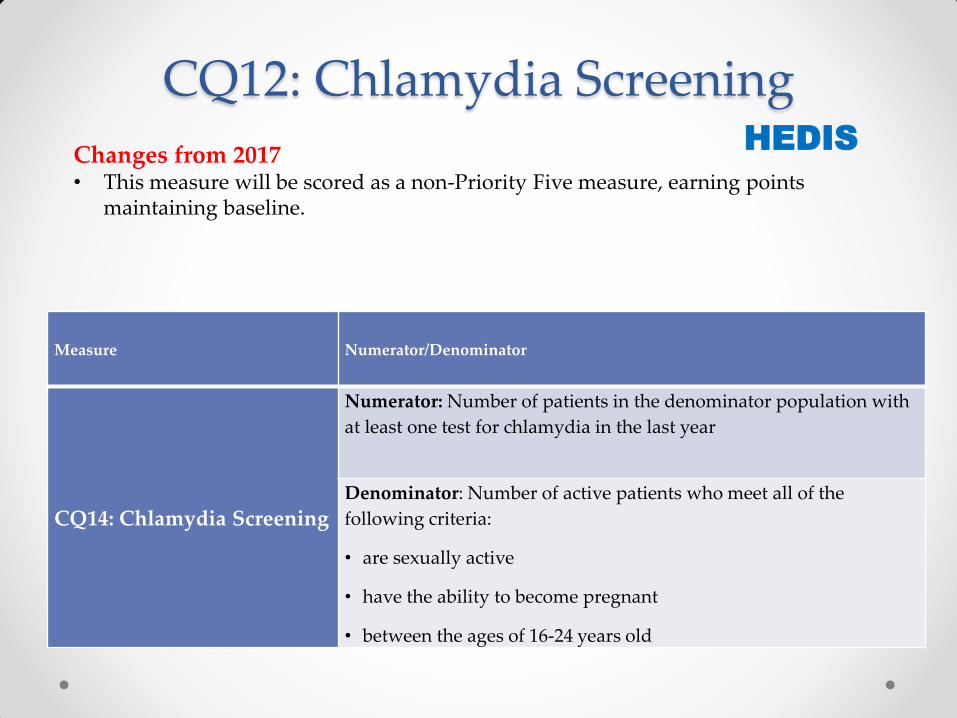
CQ12: Chlamydia Screening
Measure Numerator/Denominator
CQ14: Chlamydia Screening
Numerator: Number of patients in the denominator population with
at least one test for chlamydia in the last year
Denominator: Number of active patients who meet all of the
following criteria:
• are sexually active
• have the ability to become pregnant
• between the ages of 16-24 years old
Changes from 2017 • This measure will be scored as a non-Priority Five measure, earning points
maintaining baseline.
HEDIS

CQ13-CQ14: Perinatal Care
Measure Numerator
CQ15: Timely Access to
Prenatal Care
Numerator: Number of patients in the denominator population
who received a prenatal in the first trimester of their pregnancy or
within 42 days of enrollment into Medi-Cal, whichever is later.
CQ16: Postpartum Care
Numerator: Number of patients in the denominator population
who had a postpartum visit between 21 - 56 days after delivery.
HEDIS Changes from 2017 • This measure will be scored as a non-Priority Five measure, earning points
maintaining baseline.
Denominator: Number of active patients who had a live birth in the
last year.

CQ15: Asthma Medication Ratio
Measure Numerator/Denominator
CQ17: Asthma Medication
Ratio
Numerator: Number of patients in the denominator population who
have a ratio of 0.5 or greater of controller asthma medications to
total asthma medications in the measurement year.
Denominator: Number of active patients between the ages 5-64 with persistent asthma as defined as one or more of the following in the past two years: • At least one ED visit with a primary diagnosis of asthma • At least one inpatient encounter with a primary diagnosis of
asthma • At least four outpatient visits with a diagnosis of asthma and at
least two asthma medication dispensing events • At least four asthma medication dispensing events
• If the patient was only dispensed short acting medications (leukotriene modifier or antibody inhibitor) they should also have a diagnosis of asthma in any setting
HEDIS Changes from 2017 • This measure will be scored as a non-Priority Five measure, earning points
maintaining baseline.

Data Quality Domain
2018 Changes
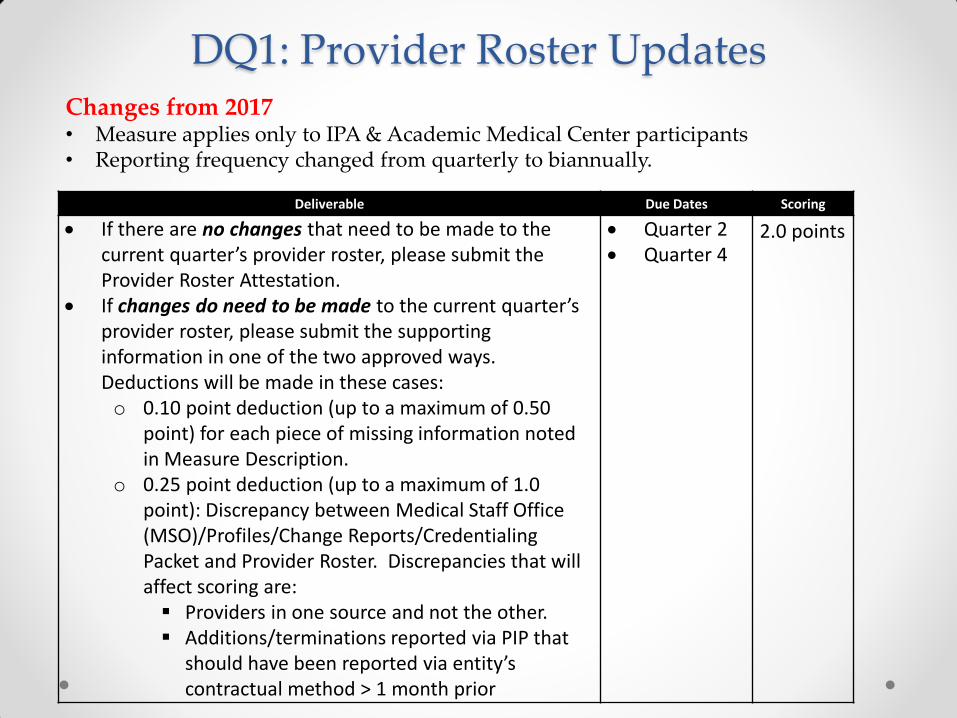
DQ1: Provider Roster Updates
Deliverable Due Dates Scoring
If there are no changes that need to be made to the current quarter’s provider roster, please submit the Provider Roster Attestation.
If changes do need to be made to the current quarter’s provider roster, please submit the supporting information in one of the two approved ways. Deductions will be made in these cases: o 0.10 point deduction (up to a maximum of 0.50
point) for each piece of missing information noted in Measure Description.
o 0.25 point deduction (up to a maximum of 1.0 point): Discrepancy between Medical Staff Office (MSO)/Profiles/Change Reports/Credentialing Packet and Provider Roster. Discrepancies that will affect scoring are: Providers in one source and not the other. Additions/terminations reported via PIP that
should have been reported via entity’s contractual method > 1 month prior
Quarter 2 Quarter 4
2.0 points
Changes from 2017 • Measure applies only to IPA & Academic Medical Center participants • Reporting frequency changed from quarterly to biannually.

Patient Experience Domain
2018 Changes

PE8: Expanding Access to Services
Changes from 2017 • There are two new options for 2018:
• Option Three: Patient-centered scheduling practices • Option Four: Improvements in transgender health are new in 2018
• The option to offer primary care services by staff other than PCPs was retired to create opportunity for new improvement projects.
• Option Five was modified to include a range of access improvement projects.
Option One: Best Practices in Hepatitis C Screening & Treatment
Option Two: Improvements in Opioid Safety
Option Three: Patient-Centered scheduling Practices
Option Four: Improvements in Transgender Health
Option Five: Access Improvement Project

PE8: Expanding Access to Services
Deliverables Due Dates Scoring
Deliverable A: Submit service
expansion plan using required
template
Quarter 1
2.0 points for completed template
Deliverable B: Submit example
materials from service expansion
Quarter 3 1.0 points for example materials
Deliverable C: Attestation service
expansion has occurred, signed by
Medical Director or equivalent
Quarter 4 1.0 points for signed attestation

Systems Improvement Domain
2018 Changes

SI1: Depression Screening and Follow-up
Depression
Screening
Rate
=
Numerator: Total number of patients in the denominator with a
depression screening in the measurement year.
Denominator: Total number of active patients at least 12 years
of age during the measurement year.
Numerator Measurement Option #2: Measure depression screening using other
registry methods. Participants choosing this option must report their methodology for
measuring depression screening.
Changes from 2017 • The Depression Screening Rate will become pay-for-performance in Q3 2018. • Follow-up to a positive screen was added as a qualitative component of this measure.
PART A: Rate of patients receiving depression screening

SI1: Depression Screening and Follow-up
Appropriate Follow-up on or within 30 days of positive screen
1. Additional evaluation for depression
Follow-up with a case manager, with documented assessment of depression symptoms.
Telephone visit with diagnosis of depression or other behavioral health condition.
Assessment on the same-day as the positive screen, including additional depression assessment indicating no
depression or no symptoms that require follow-up.
2. Referral to a practitioner who is qualified to diagnose and treat depression
Follow-up behavioral health encounter, including assessment, therapy, collaborative care, medication
management, acute care, and telehealth encounters.
Follow-up outpatient visit, with a diagnosis of depression or other behavioral health condition.
3. Pharmacological Intervention
Dispensed anti-depressant medication
PART B: Create a system/clinic-wide protocol with pathways for each of the four appropriate follow-ups to a positive screen.

SI1: Depression Screening and Follow-up
Deliverable Due Dates PIP Network
Threshold
Quarterly
Scoring
Deliverable A: Self-report the numerator and denominator as noted in the Measure Description.
Quarter 1 & Quarter 2 (reporting only)
N/A 1.0 point
Quarter 3 & Quarter 4 (pay-for-performance)
Percentile
TBD
1.0 point
Percentile
TBD
0.5 point
Deliverable B: Documentation of system/clinic-wide protocol with pathways for each of the four appropriate follow-ups to a positive screen, submitted via Wufoo. IPA participants only: Provide an attestation signed by Medical Director, or equivalent, verifying at least three sites have developed a clinic-wide protocol with pathways for each of the four appropriate follow-ups to a positive screen described in the table below.
Quarter 3 N/A 4.0 points

SI2: Follow-Up After Hospital Discharge
Quarterly Office
Visit Follow-Up
After Hospital
Discharge Rate
=
Numerator: Total number of discharges in the
denominator with an eligible follow-up visit 1-7
calendar days post discharge
Denominator: Total number of inpatient discharges
during the quarter
Deliverable Due Date Threshold Scoring
Submit quarterly numerator
and denominator as noted
above via quantitative data
template.
Quarter 1 Quarter 2 Quarter 3 Quarter 4
50% 1.0 point
40% 0.5 point
Changes from 2017 • Numerator definition was updated to support clinical best practice that a follow-up visit
post discharge should not occur on the same-day as discharge.

SI5: Percent of Members with a Primary Care Visit
Quarterly Primary
Care Visit Rate =
Numerator: Number of SFHP members in the denominator
population with at least one PCP visit in the last year
Denominator: Total number of continuously enrolled SFHP Medi-
Cal members assigned to your organization during the quarter.
Deliverable Due Date Scoring
Deliverable A: Receive PCP
visit rate.
SFHP to provide
in Quarter 1,
Quarter 2,
Quarter 3, and
Quarter 4
To be scored Q4 2018
2.0 points for achieving 5% or more absolute
improvement over baseline* or achieving SFHP average
PCP visit rate.
1.5 points for achieving 3% absolute improvement over
baseline.*
1.0 points for achieving 1% absolute improvement over
baseline.*
Deliverable B: Submit
improvement plan
template (for participants
not meeting SFHP average
PC visit rate in Q1 2018)
Quarter 2 2.0 points
*Baseline will be determined by Q4 2017 PCP visit rate
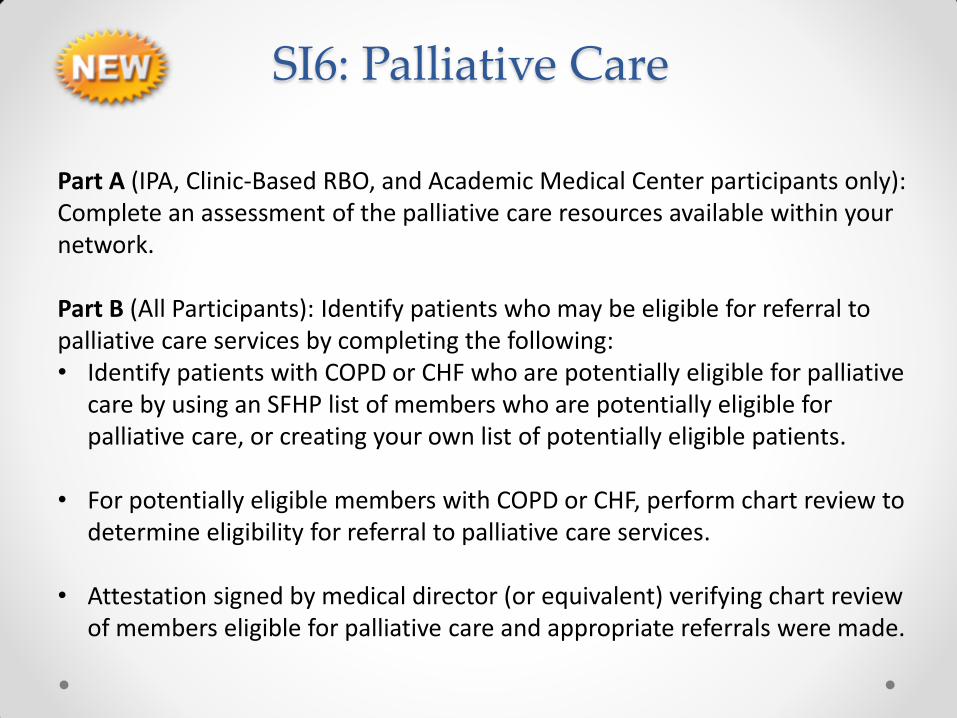
SI6: Palliative Care
Part A (IPA, Clinic-Based RBO, and Academic Medical Center participants only): Complete an assessment of the palliative care resources available within your network. Part B (All Participants): Identify patients who may be eligible for referral to palliative care services by completing the following: • Identify patients with COPD or CHF who are potentially eligible for palliative
care by using an SFHP list of members who are potentially eligible for palliative care, or creating your own list of potentially eligible patients.
• For potentially eligible members with COPD or CHF, perform chart review to
determine eligibility for referral to palliative care services.
• Attestation signed by medical director (or equivalent) verifying chart review of members eligible for palliative care and appropriate referrals were made.

SI6: Palliative Care
Deliverable Due Date Scoring
Deliverable A
(for IPA, Clinic-Based RBO, and
Academic Medical Center participants
only):
Submit template outlining the palliative
care services and/or resources available
within your network.
Quarter 2 2.0 points
Deliverable B (All Participants) : Submit
attestation signed by a medical director
(or equivalent), verifying that chart
review was performed for members with
COPD potentially eligible for palliative
care and appropriate referrals were
made.
Quarter 4 4.0 points

Questions?

BREAK!

Review All Remaining Measures

Clinical Quality Domain
Clinical Quality Scoring collaborative
Deliverable Quarterly Scoring (Self-Report)
For each of the Priority Five measures:
Achieving 90th percentile HEDIS or 75th internal PIP percentiles or 15% or more
relative improvement
1.25 points
Achieving 75th percentile HEDIS or 60th internal PIP percentiles or 10-14% relative
improvement
1.0 point
Achieving 5-9% relative improvement over baseline 0.75 point
For each of the non-Priority Five measures:
Self-reporting data quarterly 0.25 point
Maintaining performance relative to baseline* 0.25 point

CQ01-CQ03: Diabetes (All Participants)
Measure Numerator
CQ 01: Diabetes HbA1c Test
Numerator: Number of patients in denominator population
who received at least one HbA1c test within the last 12
months
CQ 02: Diabetes HbA1c <8
(Good Control)
Numerator: Number of patients in denominator whose most
recent HbA1c level is < 8.0 in the last 12 months
CQ 03: Diabetes Eye Exam
Numerator: Number of patients in denominator population
with retinal exam or dilated eye exam performed by an eye
care professional in the past 12 months OR a negative retinal
or dilated eye exam performed by an eye care professional in
last 24 months
HEDIS
Denominator: Number of active patients with diabetes ages 18-75 years old

CQ04: Cervical Cancer Screening (All Participants)
Measure Numerator/Denominator
CQ04: Routine Cervical
Cancer Screening
Numerator: Number of patients with cervices ages 24-64 who
received one or more Pap tests during the past 3 years OR patients
with cervices ages 30-64 who received cervical cytology and HPV
co-testing during the past 5 years
Denominator: Number of active patients with cervices ages 24-64
years old
HEDIS
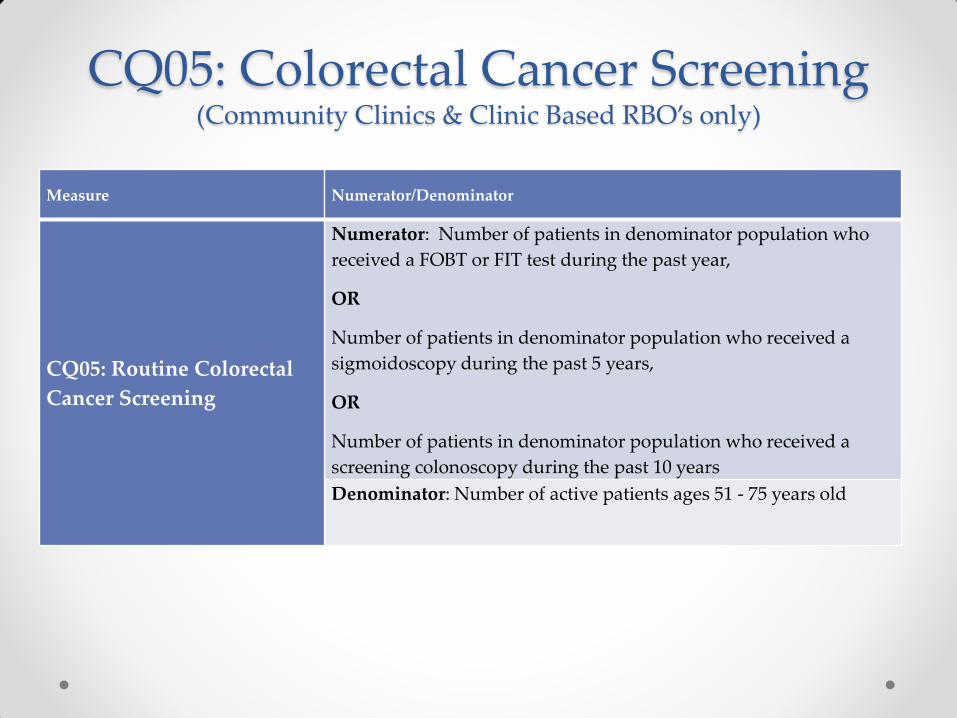
CQ05: Colorectal Cancer Screening (Community Clinics & Clinic Based RBO’s only)
Measure Numerator/Denominator
CQ05: Routine Colorectal
Cancer Screening
Numerator: Number of patients in denominator population who
received a FOBT or FIT test during the past year,
OR
Number of patients in denominator population who received a
sigmoidoscopy during the past 5 years,
OR
Number of patients in denominator population who received a
screening colonoscopy during the past 10 years
Denominator: Number of active patients ages 51 - 75 years old

CQ 07: Smoking Cessation Intervention (Community Clinics & Clinic Based RBO’s only)
Measure Numerator/Denominator
CQ 07: Smoking Cessation
Intervention
Numerator: Number of patients in denominator population with a
documented smoking cessation counseling intervention in the EHR or
registry in the last 2 years
Denominator: Number of active patients who are (must meet all of
the following):
a) 18 years or older
b) Have a documented history of tobacco use in the past 2 years
c) Seen for at least one outpatient visit within the past 2 years

CQ08: Controlling High Blood Pressure (All Participants)
Measure Numerator/Denominator
CQ08: Controlling High
Blood Pressure
Numerator: Number of patients in the denominator population in
which the most recent BP reading in an outpatient visit within the
reporting period was documented as follows:
• 18-59 years of age whose BP was <140/90 mm Hg;
• 60-85 years of age with a diagnosis of diabetes whose BP was
<140/90 mm Hg;
• 60-85 years of age without a diagnosis of diabetes whose BP was
<150/90 mm Hg.
Denominator: Number of active patients with hypertension ages 18-
85 years old
HEDIS

CQ10: Childhood Immunizations (All Participants)
Measure Numerator/Denominator
CQ10: Childhood
Immunizations
Numerator: Number of patients in the denominator population who
received all of the following vaccines by their second birthday:
• four diphtheria, tetanus and acellular pertussis (DTaP);
• three polio (IPV); one measles, mumps and rubella (MMR);
• three haemophilus influenza type B (HiB);
• three hepatitis B (HepB),
• one chicken pox (VZV); and
• four pneumococcal conjugate (PCV)
Denominator: Number of active patients who turned 2 years old during
the last year
HEDIS

CQ11: Well Child Visits for Children 3-6 Years of Age
(All Participants)
Measure Numerator/Denominator
CQ10: Childhood
Immunizations
Numerator: Number of patients in the denominator population
who had at least one well-child visit with a PCP during the past
year.
Denominator: Number of active patients 3-6 years old
HEDIS

Patient Experience Domain

PE1: Third Next Available Appointment (Community Clinics & Clinic Based RBO’s only)
Deliverable Due Dates # of Days
Reduced
Threshold Scoring
Submit the median
established patient follow-
up visit TNAA for each of
the final 5 full weeks of
the reporting period.
Note: SFHP will determine
median of five pieces of
data and use it to score
performance.
Quarter 1
Quarter 2
Quarter 3
Quarter 4
n/a
14
calendar
days or
less
2.0
points
> 10 days
15-21
calendar
days or
less
1.5
points
5-9 days n/a 1.0 point

PE2: Show Rate (Community Clinics, Clinic-based RBOs, & Academic Medical Centers only)
Monthly Show Rate =
Numerator: Of the total appointments in the denominator,
the number of appointments which patients kept.
Denominator: Total number of pre-scheduled
appointments for a PCP/PCP team visit during any given
calendar month.
Deliverable Due Dates Relative
Improvement Threshold Quarterly
Scoring
Submit monthly data each quarter via the quantitative template. Note: SFHP will determine quarterly show rate by combining numerators and denominators for each month in the quarter, and using it to determine performance.
Quarter 1
(Timeframe: Jan, Feb, Mar)
Quarter 2
(Timeframe: Apr, May, Jun)
Quarter 3
(Timeframe: Jul, Aug, Sept)
Quarter 4
(Timeframe: Oct, Nov, Dec)
n/a 85% or
more
1.0 point
10%
80-84% 0.75
point
5-9% n/a 0.5 point

PE3: Office Visit Cycle Time (Community Clinics, Clinic-based RBOs, & Academic Medical Centers only)
Deliverable Due Dates # Minutes
Reduced
PIP
Network
Threshold
Quarterly
Scoring
Self-report the median cycle time for each month in the quarter.
Quarter 1
(Data Collection Period: Jan, Feb, Mar)
Quarter 2
(Data Collection Period: Apr, May, Jun)
Quarter 3
(Data Collection Period: Jul, Aug, Sept)
Quarter 4
(Data Collection Period: Oct, Nov, Dec)
10 or more
minutes
reduced
75th
percentile
64 minutes
or less
1.0 point
5-9 minutes
reduced
60th
percentile
65-69
minutes
0.5 point

PE4: Staff Satisfaction Improvement Strategies (All Participants)
Deliverables Due Dates Scoring
Deliverable A: Submit template with the following included:
Baseline score of a staff satisfaction survey o If survey has multiple questions, only one score may be chosen.
For participants using Net Promoter survey, chosen question must be “How likely are you to recommend organization as a place to work?”
Survey type (Gallup, Net Promoter, etc.) Survey date (completed October 1, 2015-January 15, 2016) Survey question Response rate (numerator/denominator) 1-2 priority areas identified for improvement
Quarter 1 0.5 point for completed template, if required response rate met.
0 point if required response rate not met.
Deliverable B: Submit template with a report of activities implemented
specifically to address priority areas identified for improvement
Quarter 3 0.5 point for completed template
Deliverable C: Submit template with the following included:
Survey type (must be same as baseline) Survey date (completed August 1, 2016-October 15, 2016) Survey question (must be same as baseline) Response rate (numerator/denominator)
Quarter 3 0.5 point for completed template, if required response rate met.
0 point if required response rate not met.
Deliverable D: Improvement on staff satisfaction survey score, submitted via
the Quantitative Data Template.
o Score must represent question chosen for baseline.
Quarter 3 If required response rate met: 1.0 point for > 4.0% relative
improvement 1.0 point for 2.0% - 3.9% relative
improvement
If required response rate not met: 0 point

PE5: Improvement in Patient Experience of Primary Care Access (All Participants)
Patient Experience Survey Tool Criteria
Criteria Rationale 1. Conducted and analyzed by or audited by
third party
Supports consistent and unbiased survey methodology
1. Surveyed population is a random sample
of all Medi-Cal patients
Results can be generalized across the population
1. Survey conducted at least twenty-four
hours after visit concludes
Surveys conducted during or immediately after a visit can
offer a limited view of the patient’s full experience, including
follow-up services needed post visit
1. Tool has been validated Validation ensures that the tool is reliable; meaning, that it
yields results that reflect patient perception of the health
care system
1. Includes access-related questions Access to care represents the biggest opportunity for
improvement for San Francisco’s Medi-Cal population, as it is
the lowest ranking area on member surveys
1. Sampling methodology ensures that each
question obtains at least thirty responses
Results can be considered statistically meaningful

PE5: Improvement in Patient Experience of Primary Care Access
Deliverables Due Dates Scoring
Deliverable A: Submit template with:
CG-CAHPS or equivalent baseline data
A description of the qualitative data collection
methodology (sampling methodology, questions
asked, and number of patients participating)
An analysis of themes found in qualitative data
Plan to improve results, based on qualitative
data
Quarter 2 2.0 points for completed template
Deliverable B: Submit template with report of
activities implemented
Quarter 3 1.0 point for completed template
Deliverable C: Submit re-measurement score for CG-
CAHPS or equivalent survey on Quantitative Data
Template
Quarter 4 2.0 points for >3% absolute
improvement
1.0 point for 2-2.99% absolute
improvement
0.0 points for <2% absolute
improvement
Deliverable D: Submit template with re-measurement
data collection methodology.
Quarter 4 0.5 points

PE6: Primary Care Access as Measured by Appointment Availability Survey Compliance (Academic Medical Centers & IPAs)
Primary Care
Appointment
Availability
=
Numerator: Total number of primary care providers in compliance
with DMHC Appointment Availability standards listed in the measure
specification (must be compliant in both categories)
Denominator: Total number of primary care providers that respond
to the Appointment Availability Survey
Deliverable Due Date Scoring
Participate in provider
appointment availability
survey
(via phone, online, or
fax)
Quarter 4. No submission
due from participants.
8.0 points for achieving a
80% compliance rate

PE7: Improvement in Specialty Access as Measured by HP-CAHPS
(Clinic-Based RBOs & IPAs)
Deliverable Due Date Scoring
Deliverable A: Receive re-measurement score SFHP to provide in
August 2018
To be scored Q2 2018
4.0 points for achieving 4% or more
absolute improvement over baseline
score on the specialist access question
3.0 points for achieving 3.0-3.9%
absolute improvement
2.0 points for achieving 2.0-2.9%
absolute improvement
Deliverable B: Submit template with
Score for HP-CAHPS specialist access
question as reported by SFHP
An analysis of themes found in qualitative
data
Plan to improve results, based on
qualitative data
Quarter 4 2.0 points for completed template

Systems Improvement Domain

SI3: Opioid Safety (Community Clinics, Clinic-based RBOs & Academic Medical Centers)
Quarterly Opioid
Safety Rate =
Numerator: Total number of opioid registry patients who meet the opioid safety
requirements: all of the following must be documented in the last 12 months:
one drug urine screen (does not have to be random)
a signed opioid treatment agreement
CURES report reviewed
Denominator: Total number of patients in Opioid Registry on the last day of the
Quarter
Deliverable Due Date Quarterly Scoring
Deliverable A: Self-report the numerator and
denominator as noted in the Measure
Description
Quarter 1 Quarter 2 Quarter 3 Quarter 4
0.5 point for > 60%
0.25 point for 50-59%
0 points for 49% or less
Part B: Submit template with the names of 5
SFHP members with opioid safety risk
reviewed during the months of the quarter by
the Controlled Substance Review Committee.
Include brief documentation of committee
recommendations and attestation that CURES
report reviewed. CURES must be run no more
than one month prior to review.
Quarter 1 Quarter 2 Quarter 3 Quarter 4
0.1 point/member, up to 0.5 point,
will be awarded for submitting (via
secure email) the completed
template listing the 5 SFHP
members reviewed by the
Controlled Substance Review
Committee to

SI4: Providers Open to New Members (IPAs only)
Quarterly Rate of
Providers Open to
New Members
=
Numerator: PCPs in the denominator open to new members and
to auto-assigned members. Auto-assigned members are new
members who do not choose a Primary Care Provider on
enrollment with SFHP.
Denominator: Total number of PCPs affiliated with SFHP as of the
last week of the Quarter.
Deliverable Due Date Relative
Improvement
Threshold Quarterly
Scoring
No deliverables required for this measure.
Quarter 1 Quarter 2 Quarter 3 Quarter 4
> 15% > 80% 2.0 points
10-14% 70-79% 1.5 points
5-9% 60-69% 1.0 point

PIP Enrollment Process
Two steps:
1. Wufoo form
2. Enrollment Attestation: Data Sharing Consent form
2017 Q4 data will be used for 2018 baseline

Wufoo Form

Wufoo Form
Section 1: General Information & Participant Contact
Information

Wufoo Form Section 2: PIP Alignment Survey

Wufoo Form Section 3: Clinical Quality Domain Reporting

Wufoo Form Section 4: Patient Experience & Systems Improvement
Domain Measure Questions
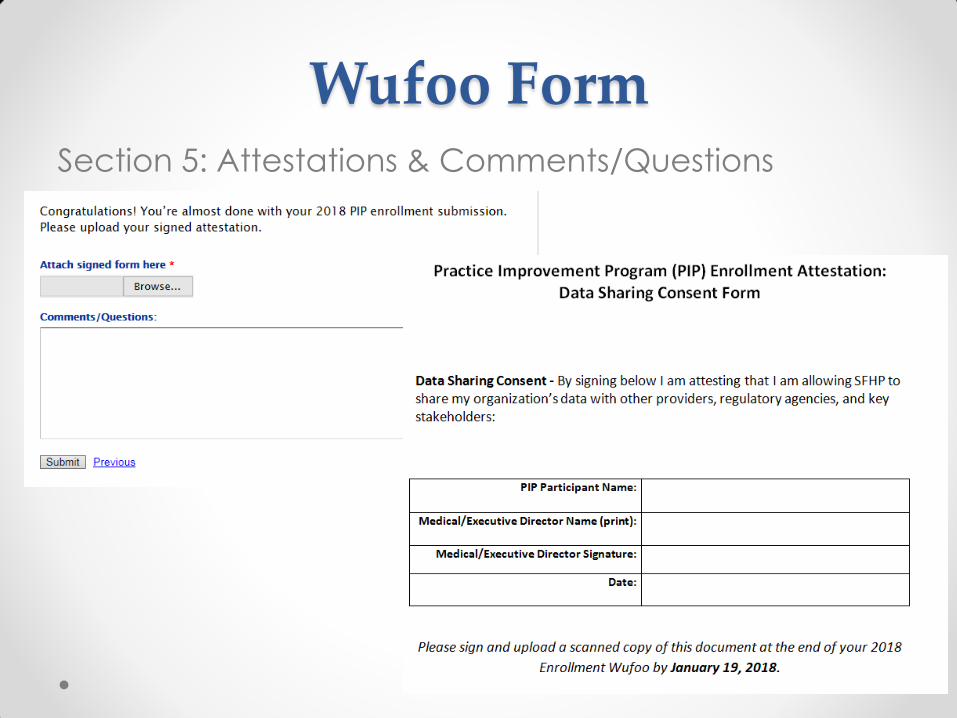
Wufoo Form Section 5: Attestations & Comments/Questions

Questions?

Evaluation
We appreciate your honest feedback on the
evaluation!

Questions? Contact information:
Kanelle Barreiro
Program Manager, Pay for Performance
(415) 615-5102
Katherine Quen
Specialist, Population Health
(415) 615-5660
Website: http://www.sfhp.org/providers/practice-improvement-program-pip/