201314 hand ortho hand fellow handbook1
DESCRIPTION
pdfTRANSCRIPT
Department of Orthopaedic Surgery
Orthopaedic Hand and Upper Extremity Fellowship Handbook February 2014

i
Table of Contents INTRODUCTION AND WELCOME ...................................................................... 1
MESSAGE FROM THE CHAIR .................................................................................. 1 MESSAGE FROM THE VICE CHAIR & FELLOWSHIP DIRECTOR ................................... 1 INTRODUCTION TO UVA ORTHOPAEDIC SURGERY .................................................. 1 A BRIEF HISTORY OF UVA ORTHOPAEDICS ........................................................... 2 THE SERVICES OFFERED BY UVA ORTHOPAEDICS ................................................. 3 OUR PROGRAM STRENGTHS ................................................................................. 4
Orthopaedic Faculty ....................................................................................... 4 Research ........................................................................................................ 4 Medical Library Facilities ................................................................................ 4 Outpatient Facilities ....................................................................................... 5 Inpatient and Surgical Facilities ..................................................................... 5 Medical School Affiliation ............................................................................... 6 Patient Population .......................................................................................... 6
SPECIAL NOTICE TO ALL EMPLOYEES .................................................................... 6 CONTACT INFORMATION ....................................................................................... 6
Direct Dial Paging .......................................................................................... 6 Direct Retrieval of Messages and Status/Location Changes ......................... 7 Staff ................................................................................................................ 7 Faculty ........................................................................................................... 8 Graduate Medical Education Office (GMEO) Housestaff ............................... 9
DUTY HOUR REQUIREMENTS ......................................................................... 10 UVA POLICY ..................................................................................................... 10
Duty Hour Logging and Monitoring .............................................................. 10 ORTHOPAEDICS POLICY ...................................................................................... 11 RECORDING DUTY HOURS AND CASE LOGS ......................................................... 13
FELLOW RESPONSIBILITIES ........................................................................... 14 HAND FELLOW EXPECTATIONS ............................................................................ 14 ATTENDING EDUCATIONAL RESPONSIBILITIES ....................................................... 14 CLINICAL RESPONSIBILITIES ................................................................................ 15
HAND SURGERY FELLOW BLOCK SCHEDULE ............................................ 16 OTHER GENERAL FELLOW RESPONSIBILITIES ....................................................... 17 MOONLIGHTING .................................................................................................. 17
SUPERVISION .................................................................................................... 18 ORTHOPAEDIC SURGERY ESCALATION OF CARE POLICY ....................................... 19 OPERATING ROOM SCHEDULES .......................................................................... 19
Posting Cases .............................................................................................. 20 DOCUMENTING AN ORTHOPAEDIC CONSULTATION IN DICTATION: A GUIDELINE ....... 20
Dictation Tips ............................................................................................... 21
ii
MAIN OR AND OPSC SCHEDULING ..................................................................... 21 MEDICAL DOCUMENTATION ................................................................................. 22
Documentation/Completion Standards ........................................................ 23 PATIENT INFORMATION SIGN-OUT POLICY ........................................................... 25 EXTERNAL TRANSFER REQUESTS ....................................................................... 26
PROGRAM OVERVIEW AND COMMON GOALS & OBJECTIVES ................. 27 OVERVIEW ......................................................................................................... 27 DESCRIPTION OF EDUCATIONAL EXPERIENCE ....................................................... 27 COMMON CORE COMPETENCY GOALS AND OBJECTIVES ....................................... 28
DETAILED EDUCATIONAL GOALS AND OBJECTIVES ................................. 31 PATIENT CARE ................................................................................................... 31 MEDICAL KNOWLEDGE ........................................................................................ 32 PRACTICE-BASED LEARNING AND IMPROVEMENT .................................................. 34 SYSTEMS-BASED PRACTICE ............................................................................... 35 PROFESSIONALISM ............................................................................................. 36 INTERPERSONAL AND COMMUNICATION SKILLS ..................................................... 37
CORE CURRICULUM TOPICS .......................................................................... 38 CURRICULUM GOALS .......................................................................................... 39
Basic Sciences ............................................................................................. 39 Traumatic Conditions ................................................................................... 39 Degenerative and Inflammatory Arthropathies, Osteonecroses .................. 40 Tendinitis and Other Soft Tissue Inflammatory Conditions .......................... 40 Congenital Differences ................................................................................. 40 Arthroscopy and Endoscopy ........................................................................ 41 Metabolic and Infectious Processes ............................................................ 41 Neurovascular Pathologies and Microsurgical Applications ........................ 41 Neoplastic Processes .................................................................................. 42 Pressure-related Phenomena and Thermal Injury ....................................... 42 Miscellaneous Disorders .............................................................................. 42 Hand and Upper Extremity Rehabilitation .................................................... 42
CONFERENCE REQUIREMENTS ..................................................................... 43 CONTINUING MEDICAL EDUCATION / LECTURE SERIES .......................................... 43
Conference Schedule .................................................................................. 44 Fracture Conference .................................................................................... 44 Core Curriculum Conference ....................................................................... 45 Grand Rounds .............................................................................................. 45 Quality Assurance (Morbidity and Mortality) Conference ............................. 45 Ethics & Professionalism Conference .......................................................... 46 Journal Club ................................................................................................. 46 Basic Science & Anatomy Conference ........................................................ 47 Visiting Professorship .................................................................................. 47 Multi-disciplinary Core Competency Lecture Series .................................... 47
PORTFOLIO ....................................................................................................... 47
iii
ASSESSMENT OF PERFORMANCE ................................................................ 48 UVA Policy ................................................................................................... 48 ACGME Policy ............................................................................................. 48 Department Policy ........................................................................................ 48
LEAVES OF ABSENCE / TIME AWAY FROM THE PROGRAM ...................... 49 VACATION POLICY .............................................................................................. 49
Allotted Vacation and Terms ........................................................................ 49 TRAVEL POLICY ................................................................................................. 50 UVA POLICY ..................................................................................................... 51
Maternity Leave ........................................................................................... 51 Paternity Leave ............................................................................................ 52
GENERAL INFORMATION ................................................................................ 52 MEDICAL LICENSE AND MALPRACTICE INSURANCE ................................................ 52 LAB SUPPORT .................................................................................................... 52
Microvascular Laboratory ............................................................................. 52 Research Expenses ..................................................................................... 52
COMPUTER SUPPORT ......................................................................................... 53 PRINTING AND COPYING SERVICES ...................................................................... 53 LAB COATS ........................................................................................................ 53 PERSONNEL RECORDS ....................................................................................... 53
POLICIES AND PRACTICES ............................................................................. 53 EMPLOYEE WARNINGS ....................................................................................... 53 UVA GRIEVANCE PROCEDURE ............................................................................ 54 REIMBURSEMENT OF EXPENSES .......................................................................... 54 FELLOW FUNDS ................................................................................................. 54
GME OFFICE FAQ AND INFORMATION .......................................................... 54 ADVOCACY ........................................................................................................ 55 BENEFITS .......................................................................................................... 55 CALL SUITE ....................................................................................................... 55 CASH BENEFIT ................................................................................................... 55 EMAIL ................................................................................................................ 55 EPIC ................................................................................................................ 55 FAC (LONG DISTANCE CODE) .............................................................................. 55 ID BADGES ........................................................................................................ 56 LOAN FORBEARANCE .......................................................................................... 56 MEAL MONEY .................................................................................................... 56 NEW INNOVATIONS ............................................................................................. 56 PARKING POLICY ................................................................................................ 56 PAYDAY ............................................................................................................. 56 PERSONAL INFORMATION CHANGES .................................................................... 56 TB TESTS AND MASK FITTING ............................................................................. 57 WEBSITE ........................................................................................................... 57 COMPUTER, AV EQUIPMENT AND THE RESIDENT LIBRARY ..................................... 57
iv
COUNSELING SERVICES ...................................................................................... 57 RESIDENT CALL AND COVERAGE ................................................................. 57
CALL SCHEDULE AND RESPONSIBILITIES .............................................................. 57 Night Float .................................................................................................... 58
DETAILED CALL SCHEDULE ................................................................................. 58 Pager #1206 (Ortho In-House Resident on call) .......................................... 58 Pager #1251 (Ortho ER Resident on call) ................................................... 58 Pager #1218 (Ortho Chief Resident on call) ................................................ 59
CALL COVERAGE DURING SPECIAL EVENTS ......................................................... 59 HIGH SCHOOL FOOTBALL COVERAGE .................................................................. 60 EMERGENCY DEPARTMENT HOLIDAY & WEEKEND NIGHT CALL ............................. 61

v
Appendices A. External Transfer Request Procedure B. Joint Commission Surgery Safety Admission Ticket Sample C UVA Graduate Medical Education Committee Policy No. 10: Duty Hours D. New Innovations, How to Log Duty Hours E. UVA Graduate Medical Education Committee Policy No. 23: New
Innovations F. UVA Graduate Medical Education Committee Policy No. 12: Levels of
Supervision for Graduate Medical Trainees G. Quality Assurance Conference Form H. Case Logs for Hand Procedures
1
Introduction and Welcome
Message from the Chair You have chosen the University of Virginia for your Orthopaedic Surgery Fellowship and we are delighted to have you. Our faculty is committed to ensuring that your training will be challenging yet rewarding, and that you will have the experiences needed to be an outstanding orthopaedic surgeon. Furthermore, the opportunities which will be available to you should prepare you well for any setting, private or academic, and any specialty. My expectation is that all interactions, whether between resident colleagues, faculty, or patients, be based on mutual respect and cooperation. Ideally, your education will be an active and interactive process of professional exchanges including information gathering and implementation of care pathways with increasing levels of responsibility. With that in mind, please recognize that we will be working together to achieve excellence in patient care, orthopaedic education and research. This handbook is designed to furnish you with information about the Department of Orthopaedic Surgery and to answer questions you may have concerning our everyday operations. If you have any questions that this handbook doesn’t answer, do not hesitate to ask any member of the faculty.
Message from the Fellowship Director With great pleasure I welcome you to the University of Virginia, Department of Orthopaedic Surgery Hand and Upper Extremity Fellowship Training Program. Our mission is to be a national and international leader in patient care, medical student, resident and fellow education, and musculoskeletal regenerative research. The strength of our program includes our dedicated faculty and our outstanding trainees. In 2013, the Orthopaedic Residency Review Committee granted the Orthopaedic Hand Fellowship a 5-year accreditation status. This is the maximum period of accreditation that can be obtained. Our commitment to Orthopaedic education and patient care, cutting edge research, and diversity were noted in the reaccreditation report. Our mission requires commitment to teamwork. This is essential for optimizing patient care and your education. I look forward to getting to know you and working closely with you to help you achieve your personal and academic goals.
Introduction to UVA Orthopaedic Surgery The Department of Orthopaedic Surgery is a national leader in musculoskeletal academics in the areas of patient care, orthopaedic education, and musculoskeletal research. We provide state-of-the-art comprehensive care for all musculoskeletal disorders, treatment by responsive physicians in the highest
2
quality facilities, and broad based primary and tertiary care. The department treats patients without regard to their ability to pay. We also provide quality graduate orthopaedic education through an intensive teaching and evaluation process and participate in national, international, professional and educational activities. The University of Virginia Medical Center serves as the home institution for residents during the five years of the Orthopaedic Surgery Residency Program. All but 40 weeks of training are spent in Charlottesville at the University of Virginia Medical Center, the Kluge Children’s Rehabilitation Center, the University of Virginia Outpatient Surgery Center (VASC), the Fontaine Orthopaedic Center, the UVA Hand Center, and the UVA Spine Center. The hospital, a Level-One Trauma Center, and the associated facilities provide the core clinical experience for the orthopaedic resident. Full-time University of Virginia Professors in the Department of Orthopaedic Surgery represent all Orthopaedic subspecialties. The formal educational program includes structured Orthopaedic teaching conferences in fracture management, subspecialty core conferences, Grand Rounds, Quality Assurance conferences, small group service-specific conferences, and Basic Science and Anatomy conferences to provide a comprehensive curriculum of fundamental Orthopaedic knowledge. Involvement with research is required and encouraged for all orthopaedic residents. With opportunities for research activity, residents gain invaluable experience in all facets of research: from proposal preparation and experimental design to podium presentations and manuscript submission.
A Brief History of UVA Orthopaedics The Department of Orthopaedic Surgery at the University of Virginia is one of the oldest in the country and dates back to 1932. From that year until 1949, Dr. Robert Funsten chaired the department. He was followed by Dr. J. Hamilton Allen, who in turn was succeeded by Dr. Warren G. Stamp in 1968. Dr. Funsten and Dr. Allen were excellent orthopaedic surgeons who by all accounts had an outstanding department. Dr. Stamp brought the department into the modern era – a department that not only excelled in clinical orthopaedics, but also in research and medical education, especially residency and fellowship training. At the time Dr. Stamp took the helm, the department consisted of two orthopaedic surgeons. Dr. Stamp successfully recruited a wide variety of excellent orthopaedic surgeons and research personnel and established an active and productive research lab. Several orthopaedic surgeons, who served either as faculty or as residents in the Stamp era, have served as chairmen of orthopaedic surgery departments across the country. Two have been presidents of the American Academy of Orthopaedic Surgery, the organization that represents orthopaedic surgeons in this country, and many others have held similar positions in other regional, national and international organizations. Dr. Gwo-Jaw Wang took over as chair in 1992. Dr. Wang expanded to thirteen full-time orthopaedic surgeons and upgraded the Division of Prosthetics and
3
Orthotics. The Department expanded its divisions by adding Foot and Ankle and Orthopaedic Oncology. Dr. Wang also added two additional fellowships – Adult Reconstruction and Spine to the Department. Dr. Cato T. Laurencin became the fifth Chair of the department in 2003. Clinically trained at Harvard, and Sports Medicine and Shoulder Fellowship trained, Dr. Laurencin brought a large research group with him from Drexel University in Philadelphia. The Department expanded a number of clinical divisions, including Adult Reconstruction and Sports Medicine. In addition, Dr. Laurencin created a University Research Center for Musculoskeletal Repair. Dr. Mark Abel served as the sixth permanent Chair of the department, named in 2008. Dr. Abel’s training included a surgical internship at Barnes Hospital, Washington University in St. Louis, MO, followed by residency training at the University of California San Diego (UCSD), which included a year of orthopaedic research. A fellowship year in Pediatric Orthopaedics and Scoliosis Surgery followed at the Children’s Hospital of San Diego. Here he developed his expertise in Motion Analysis for use as a clinical and research tool. Dr. Abel entered the United States Navy following fellowship and worked at the Portsmouth Naval Hospital. He joined the faculty of the University of Virginia in 1993. He has served on numerous medical school and hospital committees during his tenure, including the promotions and tenure committee, faculty search committees, Health Services Foundation Physician Advisory Committee, and the Children’s Medical Center Leadership Committee. He is an international expert in clinical management of pediatric neuromuscular and spinal disorders. Dr. A. Bobby Chhabra became Chair of Orthopaedics in August 2013 after serving as Vice-Chair for Dr. Abel since 2008. He has been a faculty member since 2002, and was instrumental in the creation of the University of Virginia Hand Center. Dr. Chhabra’s strength has been in Orthopaedic education for which he is nationally recognized. He has also served in a variety of committees and positions within the University of Virginia Health System and School of Medicine including a two-year term as the Associate Chief Medical Officer for Surgical Services. His advocacy skills created significant changes in the OR with regard to patient centric care, resource utilization, efficiency, quality, work place environment improvement, as well as employee satisfaction and accountability. Dr. Chhabra takes over a department that has grown to 23 faculty members and 13 physician assistants. His priority is to respond to the changing health care landscape which is moving toward a value-based care system. In addition, his objectives include improving the educational curriculum for our residents and fellows while incorporating the ACGME milestones and surgical simulation and enhancing musculoskeletal research and clinical trial productivity.
The Services Offered by UVA Orthopaedics Adult Reconstruction Orthopaedic Trauma
4
Hand, Upper Extremity and Microvascular Surgery Sports Medicine Spine Surgery Pediatric Orthopaedics Orthopaedic Oncology Ambulatory Orthopaedics Foot and Ankle Surgery Prosthetics and Orthotics
Our Program Strengths
Orthopaedic Faculty The department prides itself on having a very approachable and proactive faculty. Any trainee is free to address individual issues with the program director or Chair at any time. Each subspecialty that has a fellowship program (Sports Medicine, Hand/Upper Extremity, Adult Reconstruction, Foot & Ankle Surgery, and Spine Surgery) has multiple attending physicians participating in the subspecialty, in order to avoid diluting resident experience. Since this is a group practice, other staff members provide coverage for staff members that are called away from their practices. This facilitates continuity of patient care and fellow training.
Research The department’s research has gained national and international recognition. Both the research faculty and facilities have markedly expanded. The department has several Ph.D. primary and joint faculty members. The influx of research funding and a recently awarded N.I.H. Training grant provide multiple opportunities for trainees to actively contribute and participate in cutting-edge research. During their training here all residents and fellows are exposed to experimental design and are taught the process of producing scientifically sound research, from drafting proposals to presenting their data at national meetings. All trainees are provided opportunities for research, and are required to produce one peer-reviewed publication prior to graduation. Basic science research emphasizes musculoskeletal tissue repair and research translation with biomaterial and tissue engineering approaches.
Medical Library Facilities The main medical library is staffed with experienced employees and is well stocked with current orthopaedic textbooks and journals. A vast array of journals, textbooks, computers, and databases are available from 7:00am to 12:00am in the library. Additional computers are available in the residents call room, ED, inpatient floor, and departmental offices. The Orthopaedic Department has its own orthopaedic library, with current journals and textbooks, which can be used for quick reference work. Additionally, there are work cubicles available for fellow in the departmental office space. A collection of Academy OKU and self-

5
assessment CD’s are available for checkout. The department has also invested in online book collections for resident use.
Outpatient Facilities The UVA Hand Center and The UVA Spine Center opened their doors in 2010 at the 415 Building at Fontaine Research Park. These state-of-the-art clinics provide convenient specialty specific care with all ancillary services located in clinic. The main clinic is on the first floor of the Fontaine Orthopaedic Center, adjacent to the 50-bed inpatient HealthSouth Rehabilitation hospital. The clinic features free patient parking; physician workstations with computers and online clinical archive and radiograph access in each pod; four orthopaedic clinic pods with four exam rooms each and a cast room; a minor surgical treatment room; in-house dedicated orthopaedic radiology technicians with four x-ray pods, onsite MRI, ultrasound, and fluoroscopy; in-house radiologists; and handicapped patient parking and access. Prosthetics and Orthotics (P&O) is located at the Townside Shopping Center on 250 West near Kluge Children’s Rehabilitation Center (KCRC). This facility fabricates artificial limbs and braces on site for both UVA patients and other patients of Central Virginia physicians. Because P&O is a division of Orthopaedics, it is important to properly order and medically document P&O services. All P&O prescriptions and Letters of Medical Necessity must be signed and dated by the ordering physician. Please make certain that the Letter of Medical Necessity has been correctly and fully completed with an appropriate diagnosis for the ordered service. Also, UVA Compliance requires that all P&O prescriptions for Medicare/Medicaid patients that are signed by residents be documented by the attending physician within his/her clinic note. KCRC is where the Pediatric Orthopaedic Division is located. Drs. Abel, Romness, and Lather see all of their UVA outpatients at this site. In addition to these clinic services, Dr. Abel has a Motion Analysis and Motor Performance Laboratory for both clinical and research purposes. This laboratory is just one of four on the East Coast.
Inpatient and Surgical Facilities The UVA Medical Center, opened in 1990, remains a state-of-the-art facility, providing the residents with the latest in technology and resources. There is a dedicated Orthopaedic inpatient unit, with a full-time nursing staff, Physical & Occupational Therapy staff, and a social worker. This was the first hospital in the country with the capability to perform 3-D computer-guided and Virtual Fluoroscopic pelvic and extremity surgery. The adjacent Outpatient Surgery Center (OPSC) provides six operating rooms for outpatient surgery, and houses our Bioskills lab with state-of-the-art endoscopic and internal fixation practical stations. The University Hospital has 27 state-of-the-art operating rooms.
6
Medical School Affiliation Being a part of the University and the Health Sciences Foundation provides numerous financial and academic benefits. Ready access to the Medical School faculty and facilities provides the residents with excellent research and academic opportunities. The University, through its Research and Development Fund, provides startup funding up to $20,000 for junior faculty to initiate research projects with the residents. Most of the faculty have funded clinical and basic science research programs.
Patient Population UVA is the major referral center for a large area in Central Virginia and the Appalachians to the West. The next closest level-one trauma center is 75 miles to the East, with a much larger radius extending to the North, West, and South. A high percentage of difficult and challenging cases are referred in from outside sources as far away as West Virginia, Tennessee, and North Carolina. This referral base complements the more routine cases available from the local community. The department’s share of local orthopaedic care has increased commensurate with the improved facilities in the last decade, and we now control well over 70% of the local orthopaedic care.
Special Notice to All Employees The personal pronoun “he” as used in this handbook is used for convenience and refers to people of both sexes. It is not to be considered a reflection of superiority or inferiority of either sex.
Contact Information Fellows are responsible for updating their Status/Location codes in the Registry System on a regular basis. Access to the Registry System is made by dialing 511 from within the hospital or by dialing 982-3501 from outside the hospital. The system Status/Location codes are: 10 – Available for Radio Paging 16 – Calls are being taken by (PIC/Name) 17 – Can be reached at (telephone number) 18 – Unavailable until (date or time) 19 – Not on Call 20 – Not available, Messages being stored 21 – Available on outside pager
Direct Dial Paging (500 plus PIC) To place a direct page to medical staff and employees without operator assistance, dial 500 plus the user’s PIC from any University telephone. The system will prompt you through each transaction. Once familiar with the system, you can overdial any prompt to speed your transaction.
7
Use a # at the end of your call back number (message) or just hang up. From outside the University dial 982-3500 plus the user’s PIC.
Direct Retrieval of Messages and Status/Location Changes (Dial 511 plus PIC) The UVA Registry System allows users to directly retrieve their messages and change their status/location codes. From any University telephone dial 511 plus your PIC. If you have an optional Security Code, you will be prompted to enter it before proceeding further. From outside the University dial 982-3501 plus your PIC.
Staff Orthopaedics Business Office, Fax 3-0230 Mike Boblitz, Administrative Director, Phone 3-0225 Mary-Leigh Thacker, Accounting and Billing Manager, Phone 3-0226 Rose Herndon, Accounts Payable, Phone 3-0220 Orthopaedics Office
Laura Simmons, Dr. Abel’s and Chhabra’s Office, Phone 3-5647 Mindy Franke, Educational Programs Coordinator, (Fellowship,
Residency, Student, and Observer Liaison), Phone 3-0265, PIC 4667 Diane Sullivan, Orthopaedic Reception, Phone 3-0270 Laura Simmons, Orthopaedics Grants Administrator, Phone 3-5647 Amy Radigan, PA (Hand), Phone 2-6195, PIC 6355 Kelsey Parente, PA (Hand), Phone 2-6195, PIC 6480 Joe Hart, PhD, Research Faculty (Sports), Phone 3-0256 Wendy Novicoff, PhD, Research Faculty (Adult Recon), Phone 3-0296 Vasantha Reddi, PhD, Research Staff (Spine), Phone 3-5382
8
Faculty Physician Ofc
Phone PIC Secretary Secy
Phone Fax
Abel, Mark (clinical) 4-2364 3076 Brenda Lawson 2-4215 2-1727 Abel, Mark (admin) 3-0250 3076 Marla Langdon 3-0218 3-0290 Brockmeier, Steve 3-0273 3574 Vickie Blackwell 3-0067 3-0242 Brown, Thomas 3-0293 3795 Vallerie Staton-Bickley 3-0278 3-0290 Browne, James 3-0279 3512 Vallerie Staton-Bickley 3-0278 3-0290 Carson, Eric 2-6539 6467 Kathy Johnson 2-4832 3-0290 Chhabra, A. Bobby 3-0268 3637 Marla Langdon 3-0218 3-0290 Cui, Quanjun 3-0236 3725 Susan Fitzgerald 3-0266 3-0242 Dacus, A. Rashard 2-6704 3317 Diane Sullivan 3-0270 3-0242 Deal, D. Nicole 3-0282 6134 Vickie Blackwell 3-0067 3-0242 Diduch, David 3-0275 4137 Lora Everly 3-0291 3-0242 Domson, Gregory 3-0266 Susan Fitzgerald 3-0266 3-0242 Freilich, Aaron 4-1796 3324 Vickie Blackwell 3-0067 3-0242 Gwathmey, Winston 4-2375 3062 Debbie Handy 3-0245 3-0242 Kahler, David 3-0237 2434 Diane Sullivan 3-0270 3-0242 Lather, Leigh Ann 2-4832 6004 Sarah Dellinger 2-4832 3-0290 Miller, Mark 2-4801 4073 Vallerie Staton-Bickley 3-0278 3-0290 Park, Joseph 3-5381 3947 Debbie Handy 3-0245 3-0242 Perumal, Venkat 3-0825 3984 Debbie Handy 3-0245 3-0242 Romness, Mark 4-2301 3392 Tammy Brown 2-4214 2-1727 Shen, Frank 3-0276 3007 Lora Everly 3-0291 3-0242 Shimer, Adam 3-0258 6278 Susan Fitzgerald 3-0289 3-0242 Weiss, David 3-0292 3148 Kathy Johnson 3-0274 3-0290 Yarboro, Seth 3-0267 6843 Kathy Johnson 3-0274 3-0290
Musculoskeletal Radiology Faculty Mark Anderson, Chief of Service, Phone 2-0275, PIC 4132 Bennett Alford, Phone 4-9377, PIC 4138 Michelle Barr, Phone 3-9974, PIC 2210 Michael Fox, Phone 4-9377, PIC 6729 Christopher Gaskin, Phone 3-6410, PIC 3088 MSK Reading Room – 545 Building, Fontaine, Phone 2-6382 UVA HAND CENTER Appointments 982- HAND (4263) Fax 924-1124 Surgery Scheduling (Vickie Musselman), Phone 2-6233 Fontaine Clinic, Fax 3-5460 Main Line Appointments, Phone 3-5432, Fax 3-0382 Authorization/Referrals, Phone 3-9167
9
Return Appointments, Phone 3-5433 Staff Notes/Supply Orders, Phone 3-5436 Registration, Phone 3-5428 or 3-5427 HSF Patient Accounts, Phone 3-0388, Fax 3-5612 Cast Technician, Phone 3-5444, Fax 3-5486 Surgery Scheduling, Phone 3-5435, Fax 3-0295 Triage Nurses, Phone 3-5440, Fax 3-5486 UVA SPINE CENTER
Front Desk 243-1531 Internal Scheduling Phone 3-3633
Surgery Scheduling (Kim Vest), Phone 243-1537 UVA SPORTS CENTER
Front Desk 243-7778 Internal Scheduling Phone 3-7778
Surgery Scheduling (Amanda Davis), Phone 243-5066 Primary Care Center, Fax 3-0235 Medical Record Requests/Forms, Phone 3-0233 Patient Lists, Phone 3-0234 X-Rays 3-6700 OPSC 2-6100 6East 4-2485
Graduate Medical Education Office (GMEO) Housestaff GMEO Office – 243-6297 GMEO Fax Number – 244-9438 Risk Management (Malpractice/Claims History) – 924-5595
10
Duty Hour Requirements
UVA Policy The Office of Graduate Medical Education shall require all ACGME and non-ACGME residency and fellowship programs to participate in the documentation of duty hours in New Innovations, to ensure graduate medical trainees are not being placed at risk for fatigue, and to document compliance with each program’s individual Residency Review Committee (RRC) and the Accreditation Council for Graduate Medical Education (ACGME) regulations. Duty hours are defined as all clinical and academic activities required for the educational program; i.e., patient care (direct patient care: both inpatient and outpatient), administrative duties relative to patient care, the provision for transfer of patient care; time spent in-house during call activities, and scheduled activities such as required conferences. Duty hours do not include reading and preparation time spent away from the duty site. Duty hours restrictions are based upon the ACGME Duty Hour rules as found in the Common Program Requirements on the ACGME website: http://www.acgme.org/acWebsite/home/home.asp.
1. Faculty and fellows must be educated to recognize the signs of fatigue and sleep deprivation and must adopt and apply policies to prevent and counteract its potential negative effects on patient care and learning. This information is contained on a LIFE curriculum course on DVD which is shown to residents/fellows/faculty once annually. The DVD is kept in Mindy Franke’s office as a resident/fellow/faculty resource.
2. The Institution mandates that all graduate medical programs comply with their individual RRC regulations regarding duty hours restrictions.
3. The Institution mandates that all non-ACGME accredited programs comply with the ACGME Duty Hour rules as found in the Common Program Requirements on the ACGME website: http://www.acgme.org/acWebsite/home/home.asp and the Specialty-specific Duty Hours Definitions (4/29/2011) located at: http://www.acgme.org/acWebsite/dutyHours/DH_Definitions.pdf.
4. The Institution does not allow exceptions to the 80 hour weekly limit on duty hours.
Duty Hour Logging and Monitoring Program Directors will complete and submit a duty hours tracking report to the GMEC Subcommittee on Duty Hours Compliance on the following schedule:
• Programs at low risk for violations will complete one survey for the one month period of their choosing and will submit to the GMEO the second Friday after the end of that rotation. Low risk is having no risk of true duty
11
hour violations and absence of any of the additional measures noted to designate it high risk.
All fellows are responsible for recording their own hours in New Innovations. Any trainee wishing to discuss a duty hour concern may do so confidentially with their program director, GMEO staff, or the DIO. Trainees are encouraged to utilize the anonymous incident reporting line at 434-806-9521. To see complete text of this policy, please see Appendix C, Graduate Medical Education Committee Policy No. 10, Duty Hours, effective date November 16, 2011.
Orthopaedics Policy The Orthopaedic Hand & Upper Extremity Fellowship program schedules fellow assignments to be in compliance with all applicable ACGME requirements. Faculty members know, honor, and assist in implementing the applicable duty hour limitations. Fellows comply with those limitations, accurately report duty hours, and cooperate with duty hour monitoring procedures. All involved identify and report sources of potential duty hour violations, and collaborate to devise appropriate corrective action. Duty hours are defined as all clinical and academic activities related to the program. This includes patient care, administrative duties relative to patient care (including those, if any, conducted from home), provision of transfer of patient care, on-call time spent in-house, and scheduled activities such as conferences. Duty hours do not include reading and preparation time spent away from the duty site. Scheduled duty periods are defined as assigned duty at this hospital or other training site encompassing hours which may be within the normal work day, beyond the normal work day, or a combination of both. Fellow Duty Hours are to be recorded for a one-month period during the year, in the New Innovations Software system. See Appendix D for directions on how to log Duty Hours. The following delineates our policies on duty hours for Orthopaedic Surgery Trainees.
1. Weekly limit: Duty hours are limited to 80 hours per week, averaged over a four-week period, inclusive of all in-house call activities.
2. Days off: Fellows have one day (24 hour period) every week free of all duty (including at-home call), when averaged over a four-week period.
3. Maximum duty period length a. Duty periods are limited to 24 hours of continuous duty in the
hospital. The fellow may remain on-site for transition of care and/or to attend an educational conference when that transition is completed, but may not perform additional clinical duties (including continuity clinic) during those additional 4 hours.
12
b. After 16 hours of continuous duty, fellows are encouraged to engage in strategic napping, especially when the 16 hour mark occurs between 10pm and 8am.
4. Individual exceptions to maximum duty hour period: In unusual circumstances, a fellow may remain beyond their scheduled period of duty to continue to provide care to a single patient. These policies apply:
a. The extension of the duty hour period must be initiated voluntarily by the fellow – never assigned, or suggested, by a faculty member.
b. Possible justifications for this extension of the duty hour period include: required continuity of care for a severely ill or unstable patient, or a complex patient with whom the fellow has been involved; events of exceptional educational value; or humanistic attention to the needs of a patient or family.
c. The fellow must transfer the care of all other patients to the resident team responsible for their continuing care.
d. The fellow will text or page the Program Director within 12 hours to notify him that continuous care over 24 hours was provided, including the name of the patient, the date, and the specific reason for remaining on duty.
e. The Program Director will review each submission of additional service.
5. Time off between scheduled duty periods: Fellows are in their final year of education and therefore have flexibility in their duty hour assignments, which might be irregular or extended. It is desirable that these fellows have eight hours free of duty between scheduled duty hour periods, but there will be circumstances when they must stay on duty to care for their patients or return to the hospital with fewer than eight hours free of duty. Those circumstances may include required continuity of care for a severely ill or unstable patient, or a complex patient with whom the fellow has been involved; events of exceptional educational value; or, humanistic attention to the needs of a patient or family. Such instances of fewer than eight hours away from the hospital must be reported to, and will be monitored by, the Program Director.
6. At-Home call: At-home call must satisfy the requirement for one-day-in-seven free of duty. Time spent in the hospital by a fellow on at-home call must be reported in, and count toward, the 80-hour maximum weekly hour limit. Return to the hospital for episodic care whole on at-home call does not initiate a new “off-duty period.”
13
Saturday Elective Time Saturday elective cases will be preferentially covered by the on-call team. For complex cases to be done on the weekend the staffing attending will determine if fellow coverage will be needed. The fellows must remain compliant with all duty hour regulations.
Recording Duty Hours and Case Logs All trainees are required to log their time into the New Innovations system. See the Graduate Medical Education Manual for GME Policy No. 23, “New Innovations” Appendix E, and Appendix D for instruction on how to enter your time.
Case Logs must be entered each week. This is an ACGME requirement. See Appendix H for instruction on how to enter your cases in the ACGME Case Log System. Failure to comply with this requirement may result in a probationary status for lack of professionalism and this will become a permanent part of the trainee’s file. Random checks of compliance will be performed by the coordinator and director.
14
Fellow Responsibilities
Hand Fellow Expectations The fellow should:
1. Make every attempt to see as many initial visits in clinic as possible 2. See as many patients they have operated on post-operatively for follow-up
care as possible 3. Be responsible for the coordination of all Wednesday conferences and
Journal Clubs – which means coordinating and attending lectures 4. Be familiar with all patients on the Orthopaedics Hand Service, rounding
on patients they operate on and coordinating with the residents on service, during the months they are on Ortho. They should do the same for Plastic Surgery Hand Service during their Plastics months.
5. Be available for all evening cases during the week regardless on which service they are on call with
6. Complete the microsurgery course within the first three months of arrival (Basic Microsurgery Certificate from Randy Amiss)
7. Complete the Stern’s Bibliography, reading all articles by the end of the year. This is a self-study and should be done on their own. Dr. Deal has a recent version of this resource.
8. Read JHS every month from cover to cover 9. Immerse themselves in Hand Surgery during the course of the year
including ER involvement, aggressive clinic involvement, and being available for OR cases
10. When the assigned attending is out of town, the fellow is required to notify the other attending to make sure they are kept busy working with the other attending
11. Complete at least one manuscript by the end of the year that should be submitted for publication
12. Become comfortable with the use of hand therapy in both non-operative and post-operative management of common hand problems and should spend one-half day per quarter with the hand therapy clinic
13. Photo document index cases, and should prepare pre-, intra- and post-operative pictures of the event
14. Sit for the Certificate of Added Qualifications in Hand Surgery upon completion of the fellowship
Attending Educational Responsibilities While all six Hand faculty are involved with educating the Hand fellow on a daily basis, participate in all conferences, actively participate in emergency Hand and Upper Extremity call, and jointly are involved in the education of all Hand Fellows, Plastics, and Orthopaedic Surgery residents on the Hand service, each faculty member has an area of expertise for which they are responsible in educating the fellows.

15
1. Dr. Bobby Chhabra, Chair of Orthopaedic Surgery, has a diverse practice but his special areas of interest are athletic injuries of the upper extremity, arthroscopy, elbow trauma, and reconstruction, congenital hand surgery, and brachial plexus injuries. He also has a vast experience in wrist reconstruction and microvascular free fibular transfer for large segmental bony defects. His basic science area of research is zone II flexor tendon repairs. His experience and knowledge in this area gives him the responsibility of being the primary educator for the fellows in these areas.
2. Dr. Rashard Dacus has a diverse hand practice but his main areas of interest are upper extremity sports injuries as well as shoulder fractures and arthritis reconstruction. He also has experience in upper extremity trauma including the hand and wrist. He is the primary educator for shoulder pathology in the fellowship.
3. Dr. Nicole Deal, Fellowship Program Director, has a diverse practice that includes upper extremity trauma. She has extensive experience with microvascular reconstruction including nerve injury and repair. Her basic science area of interest is tissue engineering techniques for nerve repair. She is the primary educator for nerve injury and repair for our fellows.
4. Dr. Aaron Freilich has experience in upper extremity trauma and reconstruction. His main area of focus is in microvascular reconstruction and this is his primary area of education for our fellows.
5. Dr. Raymond Morgan, Chair, Plastic Surgery, is our senior faculty member with a very diverse practice in Plastics Hand Surgery. He has extensive experience in congenital hand surgery as well as soft tissue reconstruction and rheumatoid arthritis. These are his main areas of focus for fellow education.
6. Dr. David Drake, the Plastics Hand Fellowship Director, has vast experience in free tissue transfer for limb reconstruction. This is his area of expertise and focus for fellow education.
The six faculty members above provide an extremely comprehensive scope of hand and upper extremity surgery for all ages. The combination of their unique interests and skills allow for a comprehensive fellow education program.
Clinical Responsibilities The fellow will participate in the pre- and post-operative care of patients in both inpatient and outpatient settings. The fellow will be expected to develop a detailed understanding of the diagnostic work-up of common and complex hand problems, including the use and interpretation of appropriate musculoskeletal imaging studies, electrodiagnostic studies, vascular studies, and selective injections. The fellow will become comfortable with the application of hand therapy in both non-operative and post-operative management of common hand
16
problems, and will have the opportunity to work directly with the therapist to ensure in-depth understanding of the techniques of splinting and the use of various modalities. The fellow will also participate in the daily rounds on inpatients on service. In addition to outpatient and inpatient clinical responsibilities, the fellow will spend a minimum of two full days each week in the operating room developing surgical skills. Over the course of the year, the fellow should become comfortable with the technical aspects of all areas of hand surgery, including adult and pediatric reconstruction, adult and pediatric trauma, peripheral nerve surgery, hand burns, and wrist arthroscopy. The fellow will be expected to become facile in the performance of these procedures and will also be involved in overseeing both Plastic Surgery and Orthopaedic Surgery residents in the operating room.
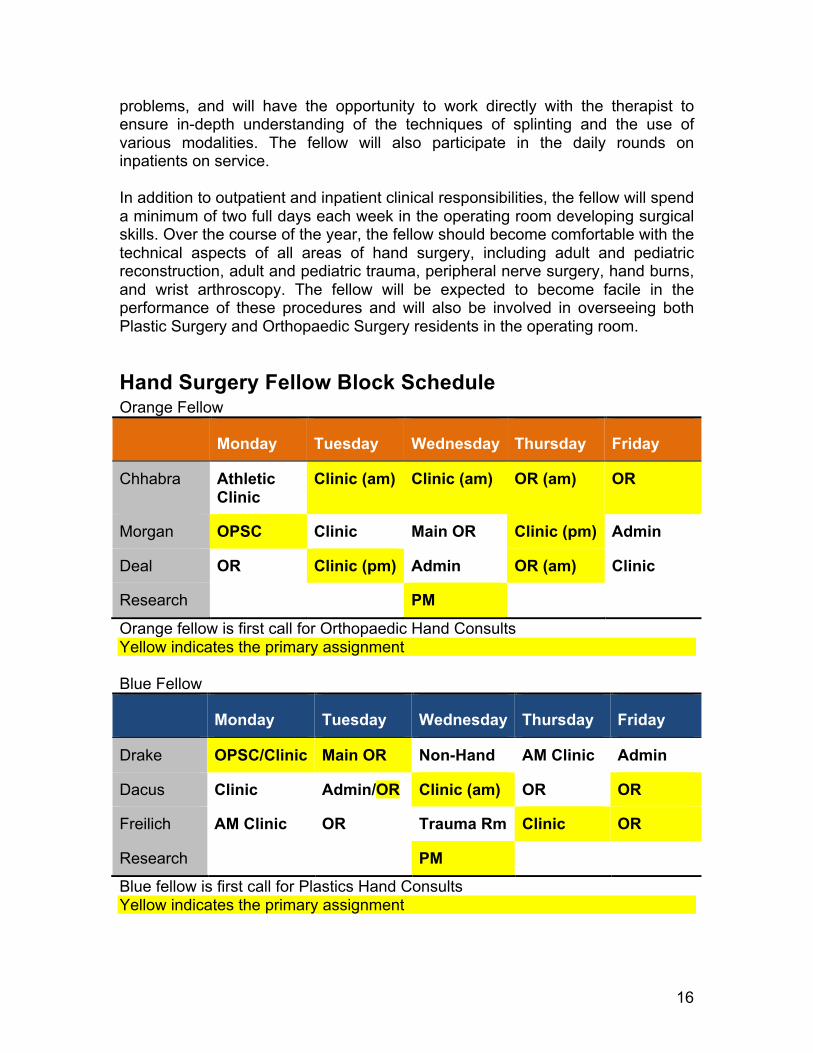
Hand Surgery Fellow Block Schedule Orange Fellow
Monday Tuesday Wednesday Thursday Friday
Chhabra Athletic Clinic
Clinic (am) Clinic (am) OR (am) OR
Morgan OPSC Clinic Main OR Clinic (pm) Admin
Deal OR Clinic (pm) Admin OR (am) Clinic
Research PM
Orange fellow is first call for Orthopaedic Hand Consults Yellow indicates the primary assignment Blue Fellow
Monday Tuesday Wednesday Thursday Friday
Drake OPSC/Clinic Main OR Non-Hand AM Clinic Admin
Dacus Clinic Admin/OR Clinic (am) OR OR
Freilich AM Clinic OR Trauma Rm Clinic OR
Research PM
Blue fellow is first call for Plastics Hand Consults Yellow indicates the primary assignment
17
We realize that the clinical experience will vary with the fellows’ background and may be tailored to the individual’s needs. For example, first call responsibilities to the ER may be arranged if the fellow has not had this experience. We will also arrange protected time for research if the fellow has an approved project.
Other General Fellow Responsibilities 1. New Innovations time entry is not optional. Trainees are reminded of the
University’s Honor Code when entering time into the New Innovations System.
Fellowship work hours are monitored by the Program Directors, the Program Coordinator, and the GME Office. The New Innovations system records and monitors work hours and reports any violations to the Residency Coordinator and Program Directors. Duty hours are entered weekly for a one-month period during the academic year.
2. Case Logs – The fellow case logs are currently maintained within the New Innovations Procedure Logger. Additional references including procedure (CPT) codes are available at the ACGME website http://www.acgme.org
Moonlighting No moonlighting is allowed in the Department of Orthopaedic Surgery. Educational and service activity that UVA Orthopaedic Surgery Trainees provide for local varsity sports activity (physical exams, presence at games, etc) will count toward duty hours and any stipends will be placed in the Resident & Fellow Education fund within the UVA Alumni Association account. All money received will be shared by trainees in the form of books, subscriptions, or the year-end visiting professor activity.
18
Supervision The Orthopaedic Hand and Upper Extremity Fellowship Program recognizes and supports the importance of graded and progressive responsibility in graduate medical education. The goal is to promote assurance of safe patient care, and the fellow’s maximum development of the skills, knowledge, and attitudes needed to enter the unsupervised practice of medicine. Supervising Physician is defined as a faculty physician, or a licensed independent practitioner, including non-physician faculty working in conjunction with the orthopaedic surgery department. Four levels of supervision are recognized. They are:
1. Direct: The supervising physician is physically present with the fellow and the patient and prepared to take over the provision of patient care if/as needed.
2. Indirect: there are two types of indirect supervision: a. Indirect supervision with direct supervision immediately available:
the supervising physician is present in the hospital (or other site of patient care) and is immediately available to provide Direct supervision. The supervisor may not be engaged in any activities (such as a patient care procedure) which would delay his/her response to a fellow requiring direct supervision.
b. Indirect supervision with direct supervision available: the supervising physician is not required to be present in the hospital or site of patient care, or may be in-house but engaged in other patient care activities, but is immediately available through telephone or other electronic modalities, and can be summoned to provide Direct Supervision.
3. Oversight: The supervising physician is available to provide review of procedures/encounters with feedback provided after care is delivered
The Orthopaedic Hand and Upper Extremity Fellowship program establishes schedules which assign qualified faculty physicians, or appropriate other licensed independent practitioners, to supervise at all times and in all settings in which fellows of the Orthopaedic Hand and Upper Extremity Fellowship program provide any type of patient care. The minimum amount/type of supervision required in each situation is determined by the definition of the type of supervision specified, but is tailored specifically to the demonstrated skills, knowledge, and ability of the individual fellow. In all cases, the faculty member functioning as a supervising physician should delegate portions of the patient’s care to the fellow, based on the needs of the patient and the skills of the fellow.
19
In every level of supervision, the supervising faculty member must review progress notes, sign procedural and operative notes, and discharge summaries. Faculty members must be continuously present to provide supervision in ambulatory settings, and be actively involved in the provision of care, as assigned.
Orthopaedic Surgery Escalation of Care Policy All fellows must communicate with the appropriate supervising faculty member, according to these guidelines: the fellow shall notify the responsible Attending Physician within 90 minutes of any of the following events:
1. Patient admission to hospital 2. Transfer of patient to or from the intensive care unit or to a higher level of
care 3. Need for intubation or ventilator support 4. Cardiac arrest or significant changes in hemodynamic status (i.e., Code
12 or MET team activation) 5. Development of significant neurological changes 6. Development of major wound complications 7. Medication errors requiring clinical intervention 8. Any significant clinical problem that will require an invasive procedure or
operation 9. Patient death 10. Notification of patient representative that family wishes to lodge a formal
complaint 11. Activation of IRPA for anything other than routine procedures 12. Patient and/or family request to speak to the attending
Please see Appendix F for Graduate Medical Education Committee Policy No. 12, “Graduate Medical Trainee Supervision Policy”, effective date March 21, 2012, “Protocol for Implementation of Policy No. 12: Graduate Medical Education Supervision”, and Orthopaedic Hand and Upper Extremity Fellowship Program Policy, “Fellowship Supervision Policy”.
Operating Room Schedules Surgery is to be scheduled through each service’s surgery schedulers. The Chief Resident on each service is responsible for the sequence of cases, for any additions or subtractions, and for the appropriate equipment and positioning. The information required includes a realistic appraisal of the amount of time necessary to complete the procedure, use of the intensive care unit postoperatively, and estimated blood loss. The ‘physician section’ of the Surgical Safety Admission Ticket should be filled out completely and checked with the attending, see sample in Appendix B .
20
The Orthopaedic residents responsible for first cases at OPSC or the main OR will be in the operating room and changed into OR attire by 7:10am (9:10am on Wednesdays). Emergent cases should be booked with the OR Staff and the Anesthesia Department only after all pertinent workups have been completed. The information provided should be detailed.
Posting Cases All trainees should be familiar with the logistics of posting cases for the main operating room for both elective and emergent cases. It is the Chief Resident’s responsibility to notify the Attending on call when a patient is “sent for” as well as when the patient enters the operating room.
Documenting an Orthopaedic Consultation in Dictation: A Guideline This is a guideline and not a template. You need to ask the specific attending or the Chief Resident on call what the individual attending would like to see included in a consult.
1. Getting started: all consults should be dictated on the Medquest system or typed into EPIC as a Consult Note / H&P with the name of the orthopaedic attending of record and, if known, the name of the faculty orthopaedist who will take care of the patient on a follow-up appointment. Specifically state the attending on call and the follow-up attending in the dictation.
2. All consults begin after establishing who the consulting team is and what they wish to know or what need as a procedure for the patient. All dictations should begin with “I was consulted by Dr. {insert name} of the {name of service} to evaluate OR and treat ….”
3. Don’t document unnecessary, irrelevant and speculative information, i.e., “The patient was injured in an MVA” not “This drunken, unrestrained driver of a stolen Hummer missed a curve on an unfinished stretch of State Road 39 and crashed into a bridge piling.” Unless you were riding in the vehicle and witnessed it, it is just hearsay and best left off the record.
4. Pertinent positives and negatives in both history and physical findings. Not a complete head-to-toe review of systems and exam. But focus your questions and exam to the injured or pathologic systems and body parts.
5. Before formulating an opinion and plan, discuss with a senior level resident and document that resident’s level of participation – if they examined the patient with you or helped with a reduction or helped determine if surgery or MSK procedure was indicated.
6. If the patient needs surgery or an invasive procedure, be certain to mention that the senior level resident and attending orthopaedist were informed and agreed with this plan.
7. Formulating a plan: these are suggestions and you are to be as specific as you can about who will be following up on these suggestions. If there is urgency to anything be sure to document that you made that fact clear to a
21
named person on the consulting team. Do not provide treatment suggestions if you were asked to make a diagnosis only.
8. For outpatient follow-up for ED and in-patient consults always give a narrow range of possible return dates and communicate this to the receiving service in as many ways as possible, particularly if the problem has urgency (i.e. needs to be seen in 1-2 days). If you’ve discussed the situation with the ultimate receiving service, it is acceptable to say that the patient may be contacted with a follow-up appointment by the resident or the attending (or someone designated by that attending to make appointments) of that service.
9. If you are being asked to accept the patient and have Orthopaedics be the responsible service, be certain to speak with the accepting attending or his resident and document that. Always mention that the attending is aware of what is happening. In the event that the faculty orthopaedist does his or her own evaluation, try to make the evaluation and treatment plan you dictate coincide with that of the attending.
10. The dictated consultation should include: Why you were consulted, who the patient was, what the problem was you were asked to solve, who helped you solve the problem, what you believed the situation was (diagnosis), what needed to be done, how your suggestions were to be implemented, and when the service was or can be provided.
Dictation Tips 1. Push button BEFORE beginning to speak 2. Do not speak like an auctioneer; normal speaking tempo 3. Enunciate and speak clearly 4. Do not put your mouth too close to the recording device 5. Please organize your thoughts BEFORE beginning to dictate. Order is the
Presentation of the patient, the Medical History, the Physical Exam, and the Assessment & Plan
6. Keep notes brief and succinct while conveying all necessary pertinent information
7. Remember to dictate an attending of record for each ED encounter at the START of your dictation (NOT the subspecialty attending the patient was referred to for follow-up unless previously arranged with said subspecialty attending)
Please see Attachment E for a copy of Dictating Instructions and Guidelines for the automated system.
Main OR and OPSC Scheduling Add-ons:
• For OPSC: If a case is an add on (a case posted within 3 business days of the DOS) you must call and ask permission and the posting slip must be faxed (817-8470) with the pre-auth written on it.
22
• For Main: If a case is a late post (added on or after noon the day before the DOS) it must be faxed (2-3972) or be turned into the Control Desk. The resident must also page 1311 and speak to the Anesthesia resident. All add-ons for the day of must go through the Control Desk.
Change in DOS: • For OPSC: If a case that has already been posted is rescheduled, the
resident/attending must notify the scheduling office by email of the new DOS. Please don’t send another posting slip.
• For Main: If a case that has already been posted is rescheduled, the resident/attending must notify the scheduling office either by email or in person. If the resident chooses to notify the scheduling office by phone or in person, a follow-up email will be required to confirm. The resident will be notified if a new posting slip is needed.
Change in Procedure / Other Information: • For OPSC: If a case that is already posted is changed, i.e., different or
additional procedure/CPT code, the resident must notify the scheduling office by email. Please don’t send another posting slip.
• For Main: If a case that is already posted is changed, i.e., different or additional procedure/CPT code, the resident must notify the scheduling office either by phone or in person, a follow-up email will be required to confirm. The resident will be notified if a new posting slip is needed.
Holding Time / 3rd Discretionary Time: • For OPSC: Please remember if you hold time at OPSC, that the hold only
lasts five business days starting the day after the OPSC is notified. After that point in time, if posting slips have not been submitted, the time will be released to the general public.
• For Main: Holds may be put on the 3rd discretionary room or open time by emailing CL Scheduling–Main OR and they don’t expire, but should be patient-specific and followed up by posting slips as soon as possible.
Medical Documentation Adapted from the March 5, 2008 Medical Documentation Message, from Dr. Susan Kirk, DIO. A complete legible medical record is the permanent way to document a patient’s condition, plan of care and response to treatment. Patient safety depends on clear communication both verbal and written. Please remember the following:
• Include time and date on all medical record documentation • Sign every note in legible format with your credentials (MD, DO, etc) • Always include your PIC number to further clarify the author of the note • At each contact point make sure the medications “match up.” This is
medication reconciliation. Medication list must be complete and do not use the phrase “resume home meds.” The complete list of medications
23
should be in the discharge summary with name, dose, route and duration if it is limited. Medication reconciliation is done more efficiently now through the EPIC electronic medical record.
Never use these abbreviations:
• U, write out units • IU, write out international units • QD, write out daily • QOD, write out every other day • MS or MSO4, write out morphine sulphate • Don’t use a trailing zero, 1.0 can be mistaken for 10
Always
• Use a leading zero if the amount is less than one, e.g., 0.25 mg of Digoxin. Even better would be 250 micrograms
• Indicate your plan of care in the admission or clinic note
Documentation/Completion Standards General Documentation Guidelines: • Include the patient name, medical record #, service, and date of service • Hand-written documentation, such as consent forms, must be legible • All medical records are legal documents • Sign, date, and write PIC # on all documents • If not documented, it is as though it did not happen Record Completion: Timely Completion of Medical Records is needed for continuity of patient care; JCAHO, HCFA, and PRO compliance; third party payment; and, legal protection for the patient, physician, and hospital. Discharge Summary: • Dictation delinquency: 5 days post discharge • Signature deficiency: 14 days post discharge • Responsibility: Attending physician
Note: "Transfers" of patients between inpatient units and Psychiatric Medicine, Physical Medicine/Rehabilitation, or KCRC are treated as discharges and re-admissions. A final Discharge Summary must be dictated when a patient is discharged from the current unit. Contact the Admissions Office (4-2264) for assistance with questions.
Operative Reports: • Dictation delinquency: 24 hours after surgery • A brief operative note is required to be present in the medical records
immediately post-op.
24
• Signature deficiency: 14 days post surgery • Responsibility: Attending physician History and Physical: • Completion time frame: Performed no more than 7 days prior to admission or
within 24 hours of admission. Verbal Orders: • Completion time frame: Within 24 hours of order. Designated Resident: • The responsible Resident shall ensure that information regarding the correct
responsible Attending and designated Resident is kept current in EPIC.
Medical Record Requests: Patient Care Requests: • Emergency Room: Call 4-5283 to have medical records delivered
immediately. • Inpatient: HIS is notified of all admissions. Record deliveries are made to the
nursing units every two hours. • Outpatient: The Resource Scheduling System provides the opportunity to
request medical records upon scheduling. Other requests must be submitted to HIS at least 3 days prior to the patient's visit. The medical records are made available to the clinic one-day prior to the patient's appointment date. Most medical records will be available on EPIC.
Clinical Studies/Non-Patient Care: • Contact 4-2196
Record Management/Chart Control: Responsibilities for Ensuring Timely & Confidential Provision of Information: • Medical records are NOT TO BE REMOVED from the patient care units,
except by HIS staff after patient discharge. • Medical records must be "CHARGED OUT" to the location in which they are
being used. Notify HIS (4-5283) immediately of any changes in the medical record's location, destination or requestor.
Returning the record: • Inpatient Admission: 24 hours post discharge • Emergency Room: 24 hour following patient's visit • Outpatient Clinics: 48 hours following patient's visit • Studies and Research: Within 7 working days after they are made available
25
Release of Medical Information: • Original records are never to be given to external requestors or removed from
the hospital complex. • Medical information cannot be released to individuals without the written
consent of the patient, subpoena, a court order or statute. • Access to patient care and financial data shall be strictly controlled and given
to an individual only on a job function NEED-TO-KNOW basis.
Patient Information Sign-Out Policy SERVICES Joints/Adult Reconstruction/Oncology Trauma Spine Pediatrics Foot and Ankle Hand Sports MORNING SIGN-OUT (Sunday – Saturday) –MOST IMPORTANT The primary resident from each service and/or team must place a copy of their service EPIC patient list on the 6-East workroom board after morning rounds (these lists will be for the floor NP’s information). Communication should also be reinforced through the EPIC system and verbally at minimum. When necessary, additional sign-out details over email should be provided. The list should include (in brief) the following for each primary orthopaedic patient:
1. Surgery and POD 2. Activity: WB status/Restrictions 3. Anticoagulation plan/restrictions (if applicable) 4. Discharge status (if applicable)
a. NP will assist with Final D/C “medically cleared” orders, and D/C orders ONLY when asked and/or notified to do so by primary team). This request may be placed on EPIC list.
b. Each team remains responsible for completing its own patients’ discharge instructions, summaries, and follow-up appointments.
5. Pertinent and/or active critical issues over past 24hrs (low BP, SOB, AMS, etc.) that could possibly alter hospital course and need follow-up by the primary team at the close of each day.
6. The NP will call to clarify any major floor issues/questions that she is unsure about.
EVENING SIGN-OUT(Monday – Friday) The primary resident on each service should update their service’s patient information as follows at the close of each day.
1. Newly Admitted Patients - Should be added to that team’s EPIC patient list (with the same information required in the morning) and a copy of that list placed in 6-East workroom or on the electronic board. This is for main OR and new ER/clinic/direct admits. (Note: Residents should NOT have to come back from VASI or Fontaine for sign-out purposes after morning sign-out unless they have admitted a patient and/or deem it necessary.)
26
2. Old Patients - Pertinent issues/changes that occurred throughout the day should be communicated to the night float/overnight resident as necessary.
NIGHT FLOAT/OVERNIGHT RESIDENT
1. The NF/ON resident coming on each evening will be provided with copies of the EPIC patient lists used during the day or will have direct communication from the daytime call residents. This will be left in the 6-East workroom by the NP upon her leaving each evening. This information will be supplemented by emails, pages, and/or phone calls regarding any issues handled by the resident(s) on call during the day. Communication is important both by phone and by email, and the night float resident should be paged if important tasks are pending.
2. Each morning following the NF/ON resident(s) shift, they will be responsible for relaying patient care information to the resident(s) coming on call for that day. This will include, but not be limited to:
a. Cases on call to the OR b. Active/outstanding/pending inpatient/ER consultations c. Orthopaedic inpatient issues overnight
External Transfer Requests When an outside referring physician calls in through the page operator or call center they are asked if the call is about a potential patient transfer or for a consult. If for a potential transfer, then the call is immediately linked into the Bed Center; if for a consult then the resident and/or attending would be paged. Please see Appendix A for the hospital’s External Transfer Request Procedures document.
27
Program Overview and Common Goals & Objectives
Overview The University of Virginia Orthopaedic Hand Fellowship is designed to provide comprehensive training in all aspects of surgery of the hand. The Department of Orthopaedic Surgery and the Department of Plastic Surgery jointly provide clinical and didactic training, as well as exposure to the opportunities for research. The fellowship year is divided between six full-time faculty physicians. Dr. Chhabra is the Director and Drs. Drake, Morgan, Dacus, Deal and Freilich are the Hand Faculty. Please contact Dr. Chhabra if there are any issues that we can address to make this fellowship a truly exceptional experience for you. The Fellowship Program at the University of Virginia requires that all trainees obtain competence in the six areas listed below. The six competencies will be taught and evaluated through a variety of techniques: didactic presentations, clinical experience, teaching rounds, attending observation, Journal Club discussion, individual study and review, 360 degree evaluations, In-Training examinations, and successful completion of web-based training modules (NetLearning).
1. Patient Care: Effective, appropriate and compassionate evaluation and treatment of patients. This includes information gathering, decision-making, safe and effective performance of procedures, and communication with other members of the health care team.
2. Medical Knowledge: The acquisition and integration of medical knowledge pertinent to Orthopaedic Surgery. The ability to utilize and analyze basic and clinical scientific literature in support of appropriate treatment decisions.
3. Practice-Based Learning and Improvement: The ability to objectively appraise one’s own ability (as well as the specialty’s) to evaluate patient care with regards to scientific literature and information technology as well as the teaching of other health care professionals and trainees.
4. Interpersonal and Communication Skills: The ability to effectively listen and communicate with patients, families and health care professionals via written communication, verbal and non-verbal methods.
5. Professionalism: Develop respect, compassion and integrity for gender, age, and cultural differences in the patient population as well as in the health care workforce. A commitment to ethical principles and practice, continued professional education and development of selflessness in the providing of medical care.
6. Systems-Based Practice: Develop an awareness and understanding of health care delivery systems and the interaction of health care with society with respect to health care cost, access to care, and optimal patient care.
Description of Educational Experience The Hand Fellow has rotating schedules each three months of the year. The educational experience is consistent, and the fellow will work with both

28
Orthopaedic Surgery and Plastic Surgery faculty physicians each week. Time in each department is shared with surgery days and clinics divided evenly and research time respected. Individual and shared group learning experiences are available on a daily basis. Education in surgery is designed to simultaneously develop cognitive knowledge, judgment, technical ability, and teaching skills. The practice of surgery requires the application of clinical data and technical skills to sure disease. Surgical judgment is that combination of knowledge, confidence, ability, and compassion that leads to the successful practice of our specialty. It is attained through consistent mentoring and professional development. It is essential to participate in the entire patient interaction from initial evaluation through the surgical process to final discharge. Our program is designed to facilitate that experience for the entire fellowship program, with intense one-on-one interaction on a daily basis between the attending and the fellow.
Common Core Competency Goals and Objectives Patient Care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
• Communicate effectively and demonstrate caring and respectful behaviors when interacting with patients and their families;
• Gather essential and accurate information about their patients; • Make informed decisions about diagnostic and therapeutic interventions
based on patient information and preferences, up-to-date scientific evidence, and clinical judgment;
• Develop and carry out patient management plans; • Counsel and educate patients and their families; • Demonstrate the ability to practice culturally competent medicine; • Use information technology to support patient care decisions and patient
education; • Perform competently all medical and invasive procedures considered
essential for the area of practice; • Provide health care services aimed at preventing health problems or
maintaining health; • Work with health care professionals, including those from other
disciplines, to provide patient-focused care. Medical Knowledge about established and evolving biomedical, clinical, and cognate sciences, as well as the application of this knowledge to patient care.
• Demonstrate an investigatory and analytic thinking approach to clinical situations;
• Know and apply the basic and clinically supportive sciences which are appropriate to orthopaedic surgery.
Practice-based Learning & Improvement that involves the investigation and evaluation of care for their patients, the appraisal and assimilation of scientific evidence, and improvements in patient care based on constant self-evaluation and life-long learning.
29
• Identify strengths, deficiencies, and limits in one’s knowledge and expertise;
• Set learning and improvement goals; • Identify and perform appropriate learning activities; • Systematically analyze practice using quality improvement methods, and
implement changes with the goal of practice improvement; • Incorporate formative evaluation feedback into daily practice; • Locate, appraise, and assimilate evidence from scientific studies related to
their patients’ health problems; • Use information technology to optimize learning; • Participate in the education of patients, families, students, residents and
other health professionals; • Analyze practice experience and perform practice-based improvement
activities using a systematic methodology; • Locate, appraise, and assimilate evidence from scientific studies related to
their patients’ health problems; • Obtain and use information about their own population of patients and the
larger population from which their patients are drawn; • Apply knowledge of study designs and statistical methods to the appraisal
of clinical studies and other information on diagnostic and therapeutic effectiveness;
• Use information technology to manage information, access online medical information, and support their own education;
• Facilitate the learning of students and other health care professionals. Interpersonal & Communication Skills that result in the effective exchange of information and collaboration with patients, their families, and other health professionals.
• Communicate effectively with patients, families, and the public, as appropriate, across a broad range of socioeconomic and cultural backgrounds;
• Communicate effectively with physicians, other health professionals, and health related agencies;
• Act in a consultative role to other physicians and health professionals; • Maintain comprehensive, timely, and legible medical records; • Create and sustain a therapeutic and ethically sound relationship with
patients; • Use effective listening skills and elicit and provide information using
effective nonverbal, explanatory, questioning, and writing skills; • Work effectively with others as a member or leader of a healthcare team
or other professional group. Professionalism, as manifested through a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to patients of diverse backgrounds.
• Respect for patient privacy and autonomy;
30
• Demonstrate respect, compassion, and integrity; a responsiveness to the needs of patients and society that supersedes self-interest; accountability to patients, society and the profession; and a commitment to excellence and ongoing professional development;
• Demonstrate a commitment to ethical principles pertaining to provision or withholding of clinical care, confidentiality of patient information, informed consent, and business practices;
• Demonstrate sensitivity and responsiveness to patients’ culture, age, gender, and disabilities;
• Demonstrate sensitivity and responsiveness to fellow health care professionals’ culture, age, gender, and disabilities.
Systems-based Practice, as manifested by actions that demonstrate an awareness of and responsiveness to the larger context and system of health care, as well as the ability to call effectively on other resources in the system to provide optimal health care.
• Work effectively in various health care delivery settings and systems relevant to orthopaedic surgery;
• Coordinate patient care within the health care system relevant to orthopaedic surgery;
• Incorporate considerations of cost awareness and risk-benefit analysis in patient and/or population-based care as appropriate;
• Advocate for quality patient care and optimal patient care systems; • Work in inter-professional teams to enhance patient safety and improve
patient care quality; • Participate in identifying system errors and implementing potential
systems solutions; • Understand how their patient care and other professional practices affect
other healthcare professionals, the healthcare organization, and the larger society and how these elements of the system affect their own practice;
• Know how types of medical practice and delivery systems differ from one another, including methods of controlling healthcare costs and allocating resources;
• Practice cost-effective health care and resources allocation that does not compromise quality of care;
• Advocate for quality patient care and assist patients in dealing with system complexities;
• Know how to partner with health care managers and healthcare procedures to assess, coordinate, and improve health care and know how these activities can affect system performance.
31
Detailed Educational Goals and Objectives
Patient Care
Goals The Hand Fellow must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
Competencies 1. Communicate effectively and demonstrate caring and respectful behaviors
when interacting with patients and their families 2. Develop and carry out patient management plans 3. Gather essential and accurate information about patients 4. Counsel and educate patients and their families 5. Demonstrate the ability to practice culturally competent medicine 6. Make informed decisions about diagnostic and therapeutic interventions
based on patient information and preferences 7. Use information technology to support patient management plans 8. Perform competently all medical surgical invasive procedures considered
essential to hand surgery 9. Provide healthcare services aimed at preventing health problems or
maintaining health 10. Work with other health care professionals to provide patient focused care
Objectives Upon completion of this training program, the Hand Fellow will demonstrate proficiency in the following areas:
1. Evaluate and surgically treat patients with tendon injuries requiring the use of primary and secondary tennorrhaphy techniques (including tendon grafting, implantation of a tendon spacer, tenolysis, and tenodesis). Included in this experience would be experience with tendon transfer and tendon balancing
2. Evaluate and surgically treat patients with nerve injuries of the upper extremity requiring repair and reconstruction, including upper-extremity peripheral nerves, nerve graft, neurolysis, neuroma management, nerve decompression and transposition
3. Evaluate and surgically treat patients requiring restoration of functional cutaneous coverage of the hands and fingers (including flaps, grafts, and microvascular free tissue transfer)
4. Evaluate and surgically treat patients requiring musculotendon transfer or substitution techniques
5. Evaluate and surgically treat patients requiring restoration of digital function from the manifestations of arthritis, including synovectomy, arthroplasty, arthrodesis, joint repair and reconstruction, including contracture release and management of stiff joints
32
6. Evaluate and surgically treat patients with fractures and dislocations including phalangeal and metacarpal with and without internal fixation, carpus, radius, and ulna with and without internal fixation and injuries to joints and ligaments
7. Evaluate and treat patients with established brachial plexus injuries including tendon and nerve transfers
8. Evaluate and manage patients with benign and malignant tumors of the upper extremity
9. Evaluate and treat patients with acute and chronic ischemia of the upper extremity
10. Understand the application of hand therapy and rehabilitation to the practice of hand surgery including upper extremity pain management
11. Effectively demonstrate competency in the management techniques of tendon repair; fracture fixation of the hand, wrist, and forearm; nerve repair; nerve decompression; and arthroscopy of the wrist
12. Effectively demonstrate competency in the performance of arthroscopy of the wrist
13. Evaluate patients with disorders of the wrist, small joints of the hand, and treat with arthroscopic management
14. Demonstrate familiarity with the diagnosis and management of congenital anomalies including syndactyly, polydactyly, and radial aplasia
15. Evaluate and manage patients with Dupuytren’s Disease 16. Demonstrate efficiency with foreign body and implant removal 17. Evaluate and manage patients with osteonecrosis, including Kienbock’s
Disease 18. Evaluate and manage patients needing thumb reconstruction including
pollicization, toe to hand transfer, and thumb metacarpal lengthening 19. Demonstrate competency in bone graft techniques with autogenous and
synthetic material, including corrective osteotomies of long bones 20. Evaluate and treat patients needing replantation or revascularization 21. Manage and provide coverage for burns of the upper extremity
Medical Knowledge
Goals The Hand Fellow must demonstrate knowledge of established and evolving biomedical, clinical, epidemiological, and social-behavioral sciences, as well as the application of this knowledge to patient care.
Competencies 1. Demonstrate an investigatory and analytic approach to clinical situations 2. Know and apply the basic clinically supportive sciences that are
appropriate to hand surgery
33
Objectives 1. Know the principles, indications and techniques of tendon reconstruction
in the hand including: a. Tendon grafting – sources, methods, indications b. Tendon transfers c. Use of prosthetics – indications, timing, techniques
2. Develop a thorough understanding of functional deficits resulting from loss of segments of the anatomic system
3. Develop an understanding of the diagnostic techniques for evaluation of functional loss, including EMG and conduction studies, arteriography, conventional radiographs, CT scan, and MRI evaluation
4. Develop an understanding of the management of nerve injuries of the upper extremity including primary, delayed primary and secondary repair
5. Demonstrate knowledge of the techniques of grouped interfascicular nerve grafting and of nerve-graft harvesting (including use of vascularized nerve grafts)
6. Demonstrate knowledge of the indications and techniques for reconstruction of the amputated thumb, including lengthening, pollicization, free whole toe transfer, and free wrap-around techniques
7. Develop knowledge of the indications for and specific technical methods of skin and soft tissue coverage including skin grafts, local flaps, distant flaps, and free tissue transfers
8. Demonstrate knowledge of the specific requirements and resurfacing techniques for areas of critical innervations in the hand
9. Demonstrate understanding of the use of tendon transfer and pedicle muscle/tendon substitution (including use of free muscle transfer) to redistribute functional activities in the upper extremity
10. Demonstrate knowledge of the indications and techniques (including joint replacement) for treatment of hand and wrist dysfunction and joint deformities secondary to trauma or non-traumatic disorders
11. Demonstrate an understanding of the consequences of derangement of the bony architecture of the hand and wrist and the methods and techniques for bone stabilization and reconstruction
12. Develop understanding of the indications and techniques for correction of bony deficits of the hand including lengthening, free non-vascularized bone grafting, and free microvascular bone transfer techniques
13. Demonstrate understanding of the principles of management of patients with brachial plexus injuries including radiologic and electrical evaluation and surgical treatment (early and late)
14. Demonstrate knowledge of the vascular, boney, and ligamentous structures of the wrist and understand the principles and techniques of intracarpal fusion, arthrodesis, tendon interposition, fracture management, joint replacement, and proximal row carpectomy
15. Demonstrate proficiency in discussions of the pathophysiology of sympathetic mediated pain syndromes (RSD) and knowledge of the peri-operative diagnosis and management of a patient with this disorder
34
16. Develop efficiency in the evaluation and management of benign and malignant tumors of the upper extremity
17. Demonstrate experience in dealing with the acute and chronic management, both operatively and non-operatively, of the burned upper extremity
18. Learn to synthesize a management plan for patients with hand problems by conducting a thorough and efficient clinical history and physical examination and have an understanding of:
a. Implications of systemic, emotional, and situational factors for the treatment of hand disorders
b. Relevant basic science and anatomy (gross and arthroscopic) related to the hand and wrist
c. Presenting basic treatment options, including home exercises, medications and surgery, along with the alternatives and risks of each
19. Develop an understanding of the diagnosis and treatment of: a. A core group of traumatic lesions (including fractures, tendon
injuries, dislocations and instability problems, nerve injuries, soft tissue loss, reflex sympathetic dystrophy and amputations)
b. Non-traumatic disorders (including arthrosis, compression neuropathies, tendonitis, contractures, ganglions, tumors, and palsies
20. Learn the elements of efficient and safe hand surgery, including: a. Preoperative planning b. Positioning and preparation c. Surgical approaches
Practice-Based Learning and Improvement
Goals The Hand Fellow, using an individual critique of patient care practice outcomes, will be able to demonstrate methods of improvement in patient care through the recognition and practice of lifelong learning skills in the surgical field as judged against applicable standards of patient care. The Hand Fellow must also demonstrate the ability to investigate and evaluate their care of patients, to appraise and assimilate scientific evidence, and to continuously improve patient care based on constant self-evaluation and lifelong learning.
Competencies 1. Identify strengths, deficiencies and limits in one’s knowledge and expertise 2. Set learning and improvement goals 3. Identify and perform appropriate learning activities 4. Systematically analyze practice, using quality improvement methods, and
implement changes with the goal of practice improvement 5. Incorporate formative evaluation feedback into daily practice
35
6. Locate, appraise and assimilate evidence from scientific studies related to the patients’ health problems
7. Use information technology to optimize learning 8. Participate in the education of patients, families, students, residents, and
other health professionals as documented by evaluations of the Hand Fellow’s teaching abilities by faculty and/or other learners
9. Analyze practice experience and perform practice-based improvement activities using a systematic methodology
10. Obtain and use information about their own population of patients and the larger population from which their patients are drawn
11. Apply knowledge of study designs and statistical methods to the appraisal of clinical studies and other information on diagnostic and therapeutic effectiveness
Objectives 1. Evaluate patient care through a personal QA program 2. Review personal portfolio for patient safety issues 3. Appraise scientific evidence as to correctness of data 4. Appraise scientific evidence as to applicability in patient are 5. Assimilate new scientific knowledge to improve patient care
The measurable objective for this area will be the graded review of the evaluations by faculty of this specific goal. This will be performed on a quarterly basis and be based on direct daily evaluation, evaluation of an ongoing portfolio, and of performance at journal club activities.
Systems-Based Practice
Goals Upon completion the Hand Fellow will understand the role of Systems-Based Practice in the management of their patients and recognize the importance of this as a lifelong process for optimal health care. Specifically, the Hand Fellow will gain understanding of how the specialty is utilized in the context of maximizing results and minimizing expenditures. The Fellow will also be able to recognize inefficient resource allocation and how this impacts the total health care system.
Competencies 1. Work effectively in various health care delivery settings and systems
relevant to the clinical specialty 2. Coordinate patient care within the health care system relevant to hand
surgery 3. Incorporate considerations of cost awareness and risk-benefit analysis in
patient care 4. Participate in identifying systems errors and in implementing potential
systems solutions 5. Advocate for quality patient care and optimal patient care systems
36
6. Work in inter-professional teams to enhance patient safety and improve patient care quality
7. Understand how their patient care and other professional practices affect other healthcare professionals, the healthcare organization, and the larger society and how these elements of the system affect their own practice
8. Know how types of medical practice and delivery systems differ from one another, including methods of controlling healthcare costs and allocating resources
9. Practice cost-effective health care and resource allocation that does not compromise quality of care
10. Advocate for quality patient care and assist patients in dealing with system complexity
11. Know how to partner with healthcare manager and healthcare procedures to assess, coordinate, and improve healthcare and know how these activities can affect system performance.
Objectives The Hand Fellow will be able to demonstrate an awareness of the health care system, respond to the larger context of the health care system and manage health care system resources to provide optimal care as judged against applicable standards of patient care.
1. Define cost-effective patient care 2. Describe how to meld together both high-quality and cost-effective care
methods in providing health care 3. Demonstrate risk-benefit analysis in day-to-day patient care 4. Describe the appropriate use of specialists in health care 5. Describe the use of non-physician health care team members in daily care
of the patient 6. Demonstrate the role of the individual physician in the development of the
overall health care system at the local, state, national and international level
7. Describe the importance of using the political process to enhance the medical health care system
This will be assessed through the competency-based clinical reports as well as through learning modules provided through the Institutional GME Office.
Professionalism
Goals The Hand Fellow will demonstrate understanding, manifest a commitment to carrying out professional responsibilities, adherence to ethical practices and sensitivity to diverse patient populations. He will present himself in a respectful, professional, honest and congenial manner in all interactions with patients, colleagues, and other health care professionals and ancillary staff.
37
Competencies 1. Compassion, integrity, and respect for others 2. Responsiveness to patient needs that supersedes self-interest 3. Respect for patient privacy and autonomy 4. Accountability to patients, society, and the profession 5. Commitment to excellence and ongoing professional development 6. Sensitivity and responsiveness to a diverse patient population, including
but not limited to diversity in gender, age, culture, race, religion, disabilities, and sexual orientation
7. Commitment to ethical principles pertaining to provision of withholding of clinical care, confidentiality of patient information, informed consent, and business practices
8. Sensitivity and responsiveness to fellow health care professionals’ culture, age, gender, and disabilities
Objectives 1. Demonstrate a commitment to professional responsibilities 2. Perform patient care in an ethical manner 3. Display sensitivity to the needs of a diverse patient population 4. Demonstrate the principles of the highest standard of patient care 5. Demonstrate commitment to continuity fo patient care 6. Demonstrate sensitivity to patient age, gender, and culture
Frequent feedback of professionalism will be given through the clinical evaluation.
Interpersonal and Communication Skills
Goals The Hand Fellow must demonstrate interpersonal and communication skills that result in the effective exchange of information and teaming with patients, their families, and professional associates. Upon completion, the Hand Fellow will be able to communicate in a collaborative and collegial model with patients, patients’ families, and members of the health care team relevant and important information.
Competencies 1. Communicate effectively with patients and families across a broad range
of socio-economic and cultural backgrounds 2. Communicate effectively with physicians, other health professionals, and
health-related agencies 3. Work effectively as a member or leader of a health care team or other
professional group 4. Act in a consultative role to other physicians and health care professionals 5. Maintain comprehensive, timely, and legible medical records
38
6. Create and sustain a therapeutic and ethically sound relationship with patients
7. Use effective listening skills and elicit and provide information using effective nonverbal, explanatory, questioning, and writing skills
Objectives 1. Discuss the patient/s medical condition, progress and outcome with the
patient and patient’s family (if requested) to assure complete understanding
2. Team with the patient, their family, and other health care providers to optimize the patient’s recovery
3. Demonstrate effective communication with other health care professionals 4. Demonstrate education of the patient’s family 5. Demonstrate counsel of the patient’s family 6. Document patient education and counseling 7. Document development of patient care plan 8. Demonstrate ability to obtain informed consent, including the components
of condition, proposed treatment, alternative treatment, complications, risk, benefits, outcomes of treatment and alternatives
9. Demonstrate maintenance of patient confidentiality in communication with family, friends, and other health care workers
10. Demonstrate integration and understanding in how professionalism and communication are critical and essential in overall optimal patient care and equally crucial in risk management and therefore effective Systems-Based Practice
Core Curriculum Topics The following topics should be covered in conferences over the course of the fellow’s year:
1. Skin Repair/Flaps/Grafts 2. Fingertip/Nailbed Injuries/Amputations 3. Tendon Repair 4. Nerve Repair/Compression neuropathy 5. Fractures/Bone Grafts/Wrist Arthroscopy 6. Inflammatory Joint Disease/Rheumatoid Arthritis 7. Hand Tumors/Dupuytren’s 8. Replantation/Microsurgery/Toe-Hand Transfers 9. Congenital Disorders 10. Vascular Disorders 11. Thermal Injuries 12. Upper Extremity Pain Management 13. Hand Therapy/Rehabilitation/Prosthetics
39
Curriculum Goals
Basic Sciences 1. Appreciation for basic and advanced surgical anatomy of the bones, soft
tissues, nerves and vessels associated with the hand, wrist, forearm, elbow and shoulder. Additionally, facility with the anatomy of other selected regions of the body utilized in microsurgical reconstruction is required.
2. Familiarity with the science of healing tissue, including bone, nerve, tendon, ligament and vessel.
3. Understanding of the pertinent biomechanics of normal and pathologic bone, and the relationship of force transmission to creation of osseous injury.
4. Knowledge of the length-tension relationships of musculotendinous units and their expression in normal and pathologic states.
5. Awareness of metabolic and autoimmune balance that affects the tissues of the upper extremity.
6. Knowledge of macroscopic and microscopic anatomy and physiology of nerves and vessels as they relate to the normal and pathologic status of the hand and upper extremity.
7. Appreciation of hydraulics and fluid flow sciences as they relate to the vascular system and its disturbances or pressure-related pathologies.
8. Familiarity with basic pharmacology as it relates to the drugs and agents utilized in the practice of Hand Surgery.
9. Knowledge of the embryology, especially as it relates to upper extremity development, teratogenesis and basic genetics.
Traumatic Conditions 1. Fractures and/or dislocations of the bones and joints of the hand and
upper extremity, including open and closed injuries of the tubular bones and dislocations of all elements of the osteoarticular column (simple and complex).
2. Specific fractures and nonunions of the carpus, in addition to treatment of acute and chronic wrist instability patterns.
3. Role of arthroplasty and/or arthrodesis in management of acute trauma to the bones and joints of the hand and upper extremity.
4. Eponymous fractures and dislocations of the forearm axis (Galeazzi, Monteggia, Essex-LoPresti).
5. Lacerations or injuries associated with tissue loss, including those requiring advanced coverage options.
40
6. Logical and systematic treatment of “combined” injuries that present with soft tissue, bony and neurovascular involvement.
7. Knowledge of ballistic injury and other foreign body management of the hand and upper extremity.
8. Management of tendon laceration of the hand and upper extremity (flexor and extensor tendons of the hand and wrist, biceps and triceps tendons).
Degenerative and Inflammatory Arthropathies, Osteonecroses 1. Degenerative or inflammatory arthritis of the small joints treated with
debridement (mucous cyst), arthrodesis or arthroplasty. 2. Degenerative or inflammatory arthritis of the wrist treated by proximal row
carpectomy, partial fusion, denervation, total wrist fusion or wrist arthroplasty.
3. Degenerative or inflammatory conditions of the elbow treated by arthroscopic debridement, interposition biologic arthroplasty or total elbow replacement arthroplasty.
4. Degenerative arthritis of the shoulder treated with shoulder arthroplasty. 5. Recognition and treatment of Kienbock’s and Pressier’s disease. 6. Post-traumatic or developmental pathologies that may accelerate the
development of degenerative arthrosis (ex., Radius malunion, Madelung’s).
Tendinitis and Other Soft Tissue Inflammatory Conditions 1. Trigger finger and trigger thumb. 2. DeQuervain’s stenosing tenosynovitis. 3. Intersection syndrome 4. Synovitis and tenosynovitis associated with inflammatory arthritis. 5. Medial and lateral epicondylitis. 6. Rotator cuff tendinitis. 7. Cumulative trauma disorders.
Congenital Differences 1. Hypoplastic or absent thumb and radial club hand (pollicization,
augmentation, microsurgical reconstruction, non-microsurgical reconstruction including metacarpal lengthening).
2. Central and ulnar deficiency. 3. Syndactyly and polydactyly. 4. Duplicate thumb. 5. Role of extraperiosteal toe phalanx transfers for terminal deficiency. 6. Madelung’s Deformity. 7. Poland’s Syndrome.
41
8. Other syndromes with manual manifestations (Cornelia DeLange, Nail-Patella, etc.).
9. Understanding of basic genetics, embryology and collaborative approaches with other professionals dealing with pediatric patients (Pediatrician, Therapists, Geneticists, Social Workers, Parental Support Groups, etc.).
Arthroscopy and Endoscopy 1. Understanding of the indications for and performance of upper extremity
arthroscopy for diagnosis and treatment (elbow, wrist, selected small joints of the hand).
2. Use of endoscopic visualization for upper extremity nerve decompression (ex., Carpal tunnel release).
Metabolic and Infectious Processes 1. Diagnosis and management of crystalline arthropathy (gout, pseudogout)
specifically as it is in contradistinction to suppurative processes. 2. Decompression of suppurative tenosynovitis, hand space abscesses or
suppurative arthritis of the hand, wrist, elbow and shoulder, paronychia and felons.
3. Management of postoperative infectious complications of the hand and upper extremity, including those with in-dwelling hardware or joint implants.
4. Basic knowledge of microbiology, including common pathogens. Additional knowledge of atypical infections seen and treated by hand surgeons (HIV, TB, mycobacterial infections, etc.).
5. Appreciation for the management of metabolic bone disease and osteoporosis as it relates to the practice of hand surgery.
Neurovascular Pathologies and Microsurgical Applications 1. Management of compressive or polyneuropathy (carpal tunnel, cubital
tunnel, radial tunnel, sensory nerve disturbances). 2. Treatment of brachial plexus lesions, including direct repair, necrotization
and transfers to restore function after brachial plexus injury. 3. Management of neuromata and adhesive neuritis. 4. Management of acute nerve and vessel lacerations (isolated or
combined). 5. Non-microsurgical tissue coverage options, including skin grafting,
complex flap closures and pedicled transfers. 6. Microsurgical capabilities for employment in acute and elective
circumstances for wound coverage (free tissue transfer).
42
7. Revascularization or replantation of upper (and selected lower) extremity amputations.
8. Tendon transfers for isolated or combined nerve palsies (radial, median, ulnar) or brachial plexus palsy.
9. Vasospastic, embolic and vascular insufficiency disorders (Raynaud’s, hypothenar hammer syndrome, etc.).
Neoplastic Processes 1. Ganglion cysts, and other benign tumors including inclusion cyst, giant cell
tumor, nerve-associated tumors, vessel-associated tumors. 2. Malignant melanoma, including integrated approaches in collaboration
with Oncologists. 3. Squamous cell carcinoma. 4. Metastatic Cancer with manual/upper extremity manifestation. 5. Dupuytren’s Contracture diagnosis and treatment. 6. Enchondroma, osteoid osteoma and other bone-associated tumors.
Pressure-related Phenomena and Thermal Injury 1. Diagnosis and treatment of evolving compartment syndrome. 2. Management of first, second, and third-degree burns. 3. Indications for and performance of hand and forearm fasciotomies and
digital escharatomies. 4. Management of frostbite. 5. High-pressure injection injuries.
Miscellaneous Disorders 1. Sympathetically-mediated pain-dysfunction syndromes. 2. Conversion reaction and Munchausen’s Syndrome. 3. Child Abuse.
Hand and Upper Extremity Rehabilitation 1. Knowledge of the indications for and collaborative employment of
contemporary protocols for upper extremity rehabilitation in nonsurgically-managed and postoperative patients.
2. Appreciation for advanced concepts of hand rehabilitation, including work hardening, vocational evaluation and workplace ergonomics.
3. Appropriate consultation with additional professionals (Social Work, Psychology, etc.) in the treatment of patients for hand and upper extremity pathologies.
43
Conference Requirements
Continuing Medical Education / Lecture Series A minimum of one hour each week is devoted to Orthopaedic didactic presentations in the basic sciences. A formal lecture is presented weekly, either by a resident, basic science faculty member, staff orthopedist, or visiting consultant. All resident lectures are supervised and backed-up by one or more designated attending physicians. Additional Orthopaedic Pathology lectures are given one to two times per month by our orthopaedic oncologist. While these lectures are often clinical topics, the basic science issues relevant to these topics are incorporated into each didactic lecture. Additional basic science presentations are integrated into the Grand Rounds and Chairman’s conference schedules. An annual conference evaluation form is filled out by the trainees at the end of each academic year to ensure improvement and enhancement of the Orthopaedic learning experience. Hand Fellows should plan to attend those conferences in Orthopaedics that are pertinent to their education. Each month there are six required upper-extremity conference for the Hand Fellow. A combined-service Hand Journal Club is held every two to three months to review the latest issue of the Journal of the American Society for Surgery of the Hand. Each quarter, a Monday evening conference will be devoted to Continuing Quality Improvement. A record of all conferences given and attended should be recorded by the fellow for documentation. Every Thursday at 7:00am, an Upper-Extremity Conference is held in the Conference Room at the outpatient surgery center. One Tuesday per month at 6:30am, Orthopaedic Surgery Competency Lectures is devoted to Hand and Upper Extremity Surgery. One Thursday every 2 months at 6:30 am, a combined MSK radiology/ortho hand conference is held to review interesting and educational radiology findings and correlate with surgical findings. This conference is held in the conference room on the 2nd floor of the 545 building at Fontaine. The Morgan-McCue Lectureship in Hand Surgery is presented in the spring of each year. A noteworthy Hand Surgeon is invited to visit in honor of the founders of the fellowship program at the University of Virginia. In addition, two or three visiting professor lectures will be arranged, and the fellow will help the fellowship program directors for Plastics (Drs. Drake and Dacus) to organize topics and case presentations. A written log of all conferences attended should be maintained for the year. Please keep this up to date, as accuracy improves greatly when this log is completed at the event.
44
Conference Schedule Skeleton weekly conference schedule for Orthopaedics: Monday 06:15-06:30 Fracture conference – didactic session 06:30-07:15 Fracture conference – cases Tuesday 06:15-07:15 Core Curriculum conference Wednesday 07:00-0800 Early conference on a rotating schedule OITE Review (Pathology Conference) 08:00-09:00 Grand Rounds (2x/month)
Quality Assurance (Morbidity and Mortality) 1x/month Friday 06:30-07:30 Basic Science/Anatomy (didactic/dissection) Lecture Journal Club One Thursday evening each month at the home of an
attending Visiting Professor Held at the end of year in conjunction with resident
graduation Multi-disciplinary Core Competency Lecture Series Held once a month on the
second Wednesday from 7-8am
Fracture Conference Monday mornings, 06:15-07:15, Moss Amphitheater (1st floor main hospital) Over the course of each academic year, we attempt to cover all major topics relating to adult and pediatric fractures. We use a discussion of the previous week’s fractures following a scheduled didactic presentation with representative cases. It is expected that the junior residents will have read the assigned topic in Rockwood and Green (reading assignments are on the conference schedule). Assigned residents will present a lecture on the scheduled topic. The lecture should last no more than 15 minutes, and should include detailed discussion of at least one recent or classic paper from the literature. The speakers should try to concentrate on the current concepts and controversial aspects of the specific fracture being discussed, so as to supplement, rather than reiterate, the assigned reading. A slide presentation with a handout is required. One of the Trauma attendings will then present either a short didactic lecture or a case-based interactive exercise for the junior residents. There will be significant interaction with the junior residents, and adequate preparation for the scheduled topic is expected. One to two Mondays each month will be devoted to pediatric fractures. The first 30 minutes of conference will be topic specific, followed by presentation of the week’s cases.
45
The junior residents will be responsible for presenting x-rays of all the previous week’s surgical and non-surgical cases to each conference. Junior residents who have initially seen the patients should be prepared to present and discuss the management of these cases at every fracture conference.
Core Curriculum Conference Tuesday mornings, 06:15-07:15, Operating Room Classroom (2nd floor main hospital) The subspecialty conference ensures that all residents are exposed to a core curriculum covering all orthopaedic subspecialties. All conferences are given by an appropriate attending and resident, with the format of the lecture left to the discretion of the attending (case review, slide presentation, article review, etc). Assigned readings are provided to the residents one week in advance to reinforce the presented materials. The subspecialty conference rotates services and topics on a 2-year schedule.
Grand Rounds Wednesday mornings, 07:00-09:00, Fontaine Conference Room, 3rd Floor Wednesday morning is an institution-wide dedicated conference time; surgical cases start at 9:30am. The Wednesday Orthopaedic conference schedule is divided into two lectures. Grand Rounds conferences are held two times per month. Each chief resident and fellow is required to present one grand rounds presentation during the academic year. Throughout the year, the department also hosts several visiting lecturers during the Grand Rounds schedule. These are invited speakers from within the University community, as well as eminent National and International speakers. Many of these presenters are funded by industry, and some are invited by the senior residents and paid for with departmental funds. Topics include clinical orthopaedics, osteoporosis, medical ethics, systems-based practice, and other related topics.
Quality Assurance (Morbidity and Mortality) Conference During this conference, held the first Wednesday of the month, residents present complications to all residents and faculty. Complications are documented for departmental Continuous Quality Improvement, including the nature of the complication, the root cause, contributing factors, and strategies for future prevention. Chief or Senior residents are required to submit a report for each service including the number of surgical procedures, number of admissions and the number of complications for the previous month. This information as well as a description of the complication and action taken must be submitted on the appropriate form (Appendix G) to Dr. Mark Romness. One case of good
46
educational value should be presented (with x-rays) to the department from each service.
Ethics & Professionalism Conference The University of Virginia School of Medicine is fortunate to have a very active in-house Department of Medical Ethics. This department provides a 24-hour ethics consultation service for inpatients. Residents are encouraged to consult the Ethics service for any questions regarding difficult decisions with informed consent and refusal of care. This service has responded with rapid input in issues regarding informed consent, competency, and withdrawal of support for orthopaedic patients in the past year. For obtunded patients without an identifiable surrogate, the Ethics service has helped to arrange court-appointed surrogates with medical power of attorney in short order. All of the faculty strive to provide ethical and cost-effective care to patients, without regard to ability to pay for care, and in doing so teach by example. According to institutional policy, clinics are not separated or stratified with regard to the patient’s socioeconomic status, and all care is provided without regard to the patients’ insurance status or ability to pay. Since the inception of the bi-monthly Ethics feature in the Journal of Bone and Joint Surgery in 2000, and the inception of the AMA’s Virtual Mentor, we have included these features in our monthly Journal Club discussions. Lectures in medical ethics are integrated into the Grand Rounds and Basic Science Conferences. Past topics have been thought provoking supplements to the journal club reviews and clinical teaching. In addition, residents in the research laboratory attend eight hours (four sessions, two hours each) of meetings during the research year or during the ten-week lab rotation. Each session consists of a lecture followed by a discussion group that includes postdoctoral fellows and graduate students in the Health Sciences and the Graduate School of Arts and Sciences Research Training Programs. The ethics mini-course is designed to emphasize the ethical standards practiced at the University of Virginia in Medicine and Research.
Journal Club One of the senior residents selects articles from the current edition of the JBJS for discussion each month at the home of one of the orthopaedic attendings. The attendings are also asked to suggest seminal articles from the subspecialty journals and the British journal for inclusion in the journal club schedule. The Ethics features in JBJS and AMA’s Virtual Mentor are discussed bi-monthly as part of the ethics curriculum. Approximately two hours per month are devoted to journal club.

47
Basic Science & Anatomy Conference Friday mornings, 06:30-07:30, Jordan Hall 1-17 A weekly conference offers comprehensive coverage of Orthopaedic Basic Science and Applied Surgical Anatomy over the course of each academic year. Attending physicians with appropriate subspecialty interest are designated to participate in each weekly conference. Basic science topics are covered twice monthly, one session is devoted to didactic anatomy presentations or radiology correlates presented by the musculoskeletal radiologists. The final session monthly is devoted to a cadaveric prosection (prepared by the research resident) to review the important anatomical material for the particular body region. Attending physicians are assigned to the sessions with which they have the most expertise.
Visiting Professorship A formal visiting professorship is sponsored each year in conjunction with the graduation banquet for the senior residents. The Chief Residents choose an eminent speaker for a one-day lectureship. The visiting professor generally gives two to three hours of didactic lectures, followed by two to three hours of case presentations by the residents. Chief Residents join the visiting professor for breakfast, lunch, and dinner on the Friday of the Professorship. The end of year banquet and awards ceremony is traditionally held at the Rotunda, a central campus structure designed by Thomas Jefferson, where all doctorates have been granted since the University’s founding in 1825.
Multi-disciplinary Core Competency Lecture Series These monthly conferences are held in Jordan Hall Amphitheater on the second Wednesday of the month from 7-8am. Two residents (intern on service and 1 second year) are assigned to attend each meeting and are therefore excused from participation in that Wednesday’s Orthopaedics Grand Rounds lectures. These residents are responsible for signing-in for the lecture and taking enough notes to present the topic to their fellow residents in the form of a 1-page report, due to the Directors and Coordinator within a week of the conference.
Portfolio The Hand Fellow will be required to assimilate ongoing experience in an organized portfolio. The outline for the portfolio is given below, and will be discussed in detail during orientation. This document is extremely important, as it serves as confirmation of the fellow’s experience and maturation as a hand surgeon. Contents should be organized as follows:
• Curriculum Vitae & Personal Statement • Patient Care/Experience
o Case Log o Microsurgery Course Certification o Patient Letters
48
• Medical Knowledge o Hand Self-Assessment Scores
• Professionalism Documentation/Development o Lectures Attended o Lectures Presented o Visiting Professor Presentations
• Interpersonal and Communication Skills o Teaching Evaluations
• Evidence of Systems-Based Practice o Faculty Evaluations o Evaluation from Head of OR Service o NetLearning Modules Completed
• Practice-Based Learning and Improvement o Index Case Documentation o Quality Assurance Presentations
• Scholarly Activity o Research Project o Abstracts Submitted o Papers Submitted/Presented o Awards
Assessment of Performance UVA Policy
POLICY AND PROCEDURES FOR THE ASSESSMENT OF PERFORMANCE OF RESIDENTS This document is maintained on UVA’s Graduate Medical Education Office website at http://www.healthsystem.virginia.edu/internet/housestaff/housestaff.cfm
ACGME Policy
Documents for program requirements are housed on the ACGME website at http://www.acgme.org/acWebsite/downloads/RRC_progReq/260orthopaedicsurgery07012007.pdf
Department Policy
Quarterly Evaluations At the end of each quarter, standardized evaluations are completed by the supervising faculty member(s) of the fellow, by the fellow of the faculty member(s), peer review by the residents, PAs and fellows, and nurse’s evaluations on the fellow. Additionally, twice annually the fellow and faculty are asked to evaluate the program. These evaluations reflect the six competencies identified by the ACGME. These evaluations are completed within the New
49
Innovations Software system. The faculty evaluation of the fellow should be discussed directly with the fellow prior to submission to the Residency Coordinator for filing in the trainee’s records. Fellow evaluations of the faculty are kept confidential and are blinded and randomized with resident evaluations before comments are shared with the faculty during their annual review. Rotation evaluations are blinded and randomized and are reviewed annually by the Education & Curriculum Committee for resident and fellow education improvement. Any significant deficiencies are discussed at the next Orthopaedic Faculty meeting. Significant or recurring deficiencies in performance warrant a referral to the Resident Advocacy & Remediation Committee. This committee has the authority to act on these identified deficiencies. Sanctions may include assigning a faculty mentor for more frequent evaluations; remediation with committee recommendations for improvement in performance and review after each rotation; and in extreme cases, termination. All sanctions are subject to institutional (UVA Health System) Grievance policies.
Assessment of Training Program Program effectiveness is critically evaluated twice annually at the Education & Curriculum Committee Meetings. The quality and content of the conferences are reviewed and recommendations are made concerning positive changes. Clinical evaluations of fellow performance are not specifically reviewed during these meetings. Fellow input regarding conferences are sought by faculty and resident members of the committee. As the Program Director has an open door policy, trainees often voice concerns or complaints regarding conferences and faculty, and these are taken into consideration when scheduling the upcoming academic conference calendar.
Leaves of Absence / Time Away from the Program
Vacation Policy
Allotted Vacation and Terms Fellows will have the following vacation allowance during an academic year (August 1 – July 31):
1. Two weeks of personal time off (14 days – including 10 business days and two weekends)
2. One week of conference time (5 business days) with conference preapproved by the fellowship director
3. Five days off during the Holiday Season of Christmas-New Year’s If time off is used inappropriately or without prior approval, probation will automatically be instituted and the trainee involved will lose the remainder of their vacation time for the year.
50
Travel Policy Fellows traveling to conference on educational funds should consult with the Program Director and Program Coordinator for pre-approval submission guidelines. A pre-travel authorization workbook will need to be completed as early as possible that includes flight, mileage, hotel, registration fees, parking, and per diem for the destination location. No travel outside of the continental US are supported. Exceptions may be made in the case of research presentations at international conference, where the resident is the primary podium presenter, and should be discussed with the Program Director. Please fill out any associated attachments out completely and accurately, using UVA’s Travel website for guidance on Per Diem rates and current Travel Workbook forms. http://www.procurement.virginia.edu/main/travel/TravelBasics.html. Fellows are responsible for keeping all travel receipts and should submit a signed and completed travel workbook within seven (7) days of return. Receipts include credit card statements showing charges for registration, air fare, and hotel. An itemized, zero balance receipt must be obtained from the hotel, and all non-reimbursable items must be deducted. Items not reimbursed include entertainment, some room service, and bar/courtesy charges. Receipts for parking, taxis/shuttles, luggage fees, and boarding passes must be submitted. Failure to keep boarding passes or other required receipts may result in the resident’s travel reimbursement being reduced or rejected. Travel must be submitted, approved by the department, and keyed within 30 days of travel or the traveler risks non-reimbursement of their traveling expenses. In the unlikely event that a trainee is absent for more than twenty (20) working days without approval or extenuating circumstances, he risks being denied residency certification. Accurate expense accounts and receipts of activities must be returned by the fellow to the Program Coordinator within 7 days of travel to comply with IRS and University regulations. Please see the web for current directions and forms to complete www.healthsystem.virginia.edu/internet/orthopaedics/travel.cfm In addition to the above, fellows will be allowed to attend legitimate national meetings at which they are presenting papers for the first time (not posters), which have been accepted. Examples of this type of meeting are:
• AOA Residents’ Conference • AAOS Annual Meeting • ORS Annual Meeting
Funding for other meeting presentations are to be provided by the PI of the study. Supplemental funding by the Department will be considered on a case by case basis.

51
Funding for these meetings is in addition to each fellow’s individual allotment, and MUST be done in advance to ensure reimbursement. Receipts need to be turned in within 5 working days and need to be submitted to the Business Office within 10 working days. All questions regarding travel funding should be directed to the Department’s Business Office.
UVA Policy Please see the Housestaff webpage regarding leaves and request for absence included in the Graduate Medical Trainee Manual at http://www.healthsystem.virginia.edu/internet/housestaff/housestaff.cfm. Scroll down to the Policies and Manuals section and click on the link to Graduate Medical Trainee Manual for the most current policies for Housestaff. The department of Orthopaedic Surgery seeks to provide all trainees with appropriate time off to ensure well-being and to conform to both the ACGME and ABOS regulations. Any time away from the training program must adhere to university and department policy, and board requirements. All orthopaedic department fellows may take up to four weeks of paid “medical leave” per year without extending the length of their training if they have an unexpected medical problem (i.e., broken leg) separate from vacation leave.
Maternity Leave The trainee must inform the department chair, vice chair, and program director and coordinator of their pregnancy or adoption date as soon as this information is confirmed in order to facilitate appropriate planning, which may include a revised education plan for the remainder of the trainee’s training and must be sent to the board. Under normal circumstances, the trainee should expect to take six weeks of maternity leave without extending her training period. Four weeks would be paid as “medical leave” with the addition of up to two weeks being allowed to be taken as vacation leave if the trainee has this leave available to them. Additional time taken away from the program due to medical necessity will need to be made up at the end of the trainee’s program in order to fulfill all requirements for sitting for the specialty board. It will be the program’s responsibility to create an appropriate makeup program for the additional time. The trainee’s obstetrician will determine the date of return to duty. It is recommended that the trainee try to schedule less demanding rotations during her third trimester and for the first month post partum. Decisions about call during the third trimester and the first month post partum will be made in conjunction with the trainee’s obstetrician. Fellows will not be expected to “make up” call nights missed while away on maternity leave. Loss of time from training for maternity leave will not be reason for termination from the program. The fellow must comply with all OSHA and safety regulations as they apply. The trainee will make every attempt to schedule elective tests and appointments outside of working hours. In no case will a fellow be not allowed to attend or be forced to
52
reschedule her appointments or tests simply because they occur within the normal working day. The trainee may take full benefit of the Family Medical Leave Act of 1993, which states that an employee has up to 12 weeks of job-protected unpaid leave during any 12 month period, if the fellow is eligible to do so.
Paternity Leave One week paid vacation around the time of birth, in addition to other vacation time is allowed by the department.
General Information
Medical License and Malpractice Insurance The Code of Virginia requires each resident or fellow to obtain a Virginia Medical License to practice medicine for bonafide hospital patients who are being seen as an official part of this department’s approved training programs. The malpractice insurance, which the hospital has purchased for trainees, provides coverage only while the fellow is acting within the scope of his employment.
Lab Support
Microvascular Laboratory The department will pay the expenses for the trainee’s time spent in the Microvascular Laboratory. Randy Amiss, R.N., is the Plastics Microsurgery technician and runs the microsurgery lab (4-2016) in the Department of Plastic Surgery. Randy is accessible at all times to assist with developing the fellow’s microsurgical skills. We strongly urge fellows to complete the microsurgical training experience early in the year, then practice with him frequently; this will enhance overall microsurgery experience. A certificate of completion will be given at the completion of the course and should be included in the fellow’s Portfolio.
Research Expenses The fellow will have ready access to the research laboratories of both departments, including cellular biology labs, the microvascular lab of the Plastic Surgery department, the biomechanics lab of the Orthopaedics department, and the anatomy lab of the medical school Each of these labs has full-time basic science researchers available to the fellow. Additionally, the trainee will have ample opportunity to do clinical research, including clinical trials, chart reviews, or case studies.
53
All research projects will have a faculty member as the senior investigator, and presentation of publishable research will be supported by the department of the faculty investigator. The fellow will have up to a full day each week to conduct research activities. The fellow is required to participate in a clinical research project and to complete a paper for a peer-reviewed publication. Faculty members will present their current research at a conference in August or September, and the fellow should commit to a project at that time. A timeline for completion of the project will be formulated to assure completion.
Computer Support The Department maintains computers with a variety of peripherals for trainees use in the Departmental office, the Department Library, and the call room. These computers are loaded with a variety of software that includes MS Office, Internet Explorer, and various medical online search engines. In addition to the available software, trainees have access to a number of AAOS CD-ROM educational materials. The computers allow the fellow to perform patient order entry for their assigned inpatients. EPIC Super Users are also available by phone to help with the EPIC medical record system. According to Section 117 of the Copyright Act, copying of computer software is prohibited except for the purpose of making an archival copy. Blank CDs and jewel cases are available from the Fellowship Coordinator to store data.
Printing and Copying Services All photocopies should be made using the copiers at the Orthopaedic Offices or clinics. Trainees may obtain copy cards from the GME Office to make copies elsewhere on grounds.
Lab Coats Each trainee receives two (2) monogrammed laboratory coats upon arrival with the University to be worn during patient-care activities.
Personnel Records Personnel records are kept in a locked filing cabinet within the Residency Office, and are continually updated. Access to your file is granted with the coordination of the Fellowship Coordinator.
Policies and Practices
Employee Warnings Initial intervention for trainee difficulties with respect to performance, behavior and conduct are handled with face-to-face conference with the Program Director. If the conference does not resolve the problem, the Resident Advocacy & Remediation Committee is convened to discuss the issue and to formulate an action plan. If remediation is recommended, the trainee is notified in writing.
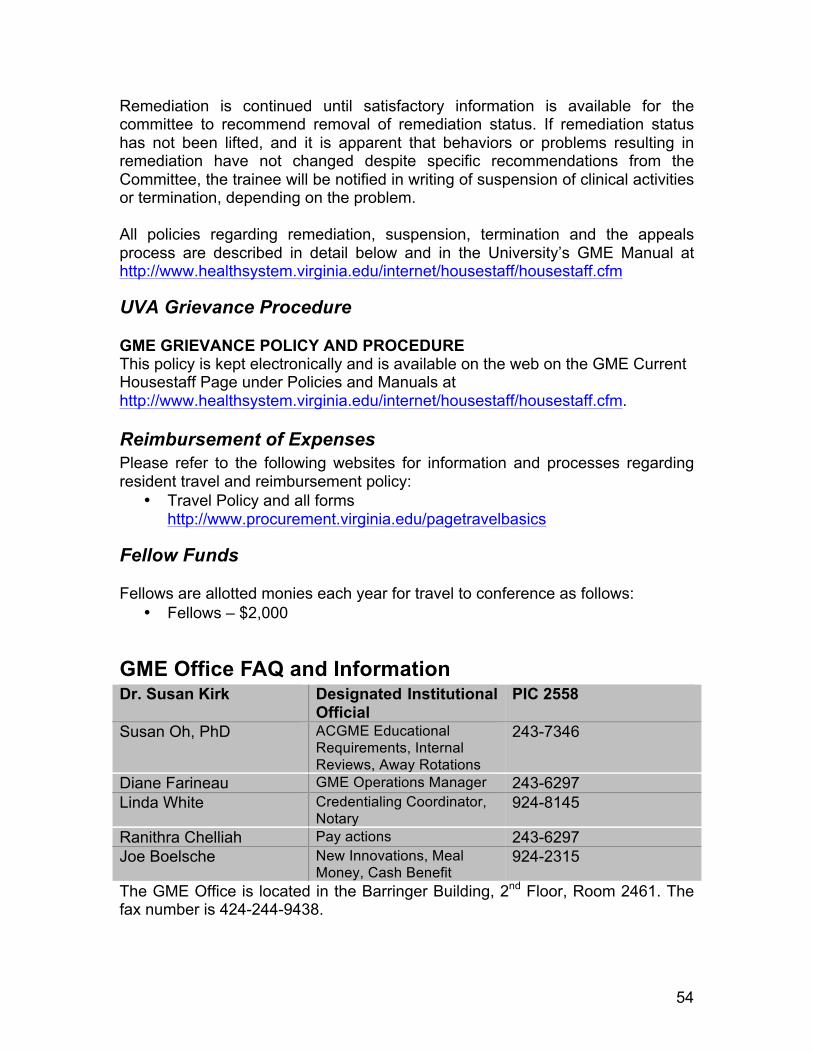
54
Remediation is continued until satisfactory information is available for the committee to recommend removal of remediation status. If remediation status has not been lifted, and it is apparent that behaviors or problems resulting in remediation have not changed despite specific recommendations from the Committee, the trainee will be notified in writing of suspension of clinical activities or termination, depending on the problem. All policies regarding remediation, suspension, termination and the appeals process are described in detail below and in the University’s GME Manual at http://www.healthsystem.virginia.edu/internet/housestaff/housestaff.cfm
UVA Grievance Procedure
GME GRIEVANCE POLICY AND PROCEDURE This policy is kept electronically and is available on the web on the GME Current Housestaff Page under Policies and Manuals at http://www.healthsystem.virginia.edu/internet/housestaff/housestaff.cfm.
Reimbursement of Expenses Please refer to the following websites for information and processes regarding resident travel and reimbursement policy:
• Travel Policy and all forms http://www.procurement.virginia.edu/pagetravelbasics
Fellow Funds
Fellows are allotted monies each year for travel to conference as follows: • Fellows – $2,000
GME Office FAQ and Information Dr. Susan Kirk Designated Institutional
Official PIC 2558
Susan Oh, PhD ACGME Educational Requirements, Internal Reviews, Away Rotations
243-7346
Diane Farineau GME Operations Manager 243-6297 Linda White Credentialing Coordinator,
Notary 924-8145
Ranithra Chelliah Pay actions 243-6297 Joe Boelsche New Innovations, Meal
Money, Cash Benefit 924-2315
The GME Office is located in the Barringer Building, 2nd Floor, Room 2461. The fax number is 424-244-9438.
55
Advocacy Everyone in the GME Office is available to the trainees to assist or direct you towards the resources you need. The office maintains an anonymous hotline that you may call at any time for any reason. (434) 806-9521.
Benefits Benefit enrollment forms must be turned in within 31 days of payroll start date. Trainees may speak to a benefits counselor any time between 8:00am and 5:00pm by calling (434) 243-3344. Health insurance and retirement benefits are detailed fully on the GME Current Housestaff Page under the Benefits and Work Life section.
Call Suite The GME maintains a call suite in the zero level (northeast corner) of the main hospital that has program-designated call rooms, float rooms (for use by any trainee called in overnight), a lactation room, a gym, a lounge, and shower facilities. This space is reserved exclusively for the GME trainees and can be accessed using your ID badge.
Cash Benefit In addition to the trainee’s base salary, each trainee receives a cash benefit of approximately $1040. This is designated to offset the cost of parking. If you elect NOT to have parking, you will still receive this money, distributed over each of the 24 pay periods, to use however you would like.
Email Your email ID can be found in New Innovations. Logging in the first time you will use that ID + the last 4 digits of your social security number as the password. Logging into email remotely can be done at www.healthsystem.virginia.edu. If you have issues, please call the helpdesk at (434) 924-5334.
EPIC Trainees are granted access to EPIC once they’ve completed the required CBLs and classes. The trainee should receive an email asking them to agree to the user permission statement. If you have trouble accessing EPIC or for any EPIC related questions please call (434) 982-EPIC.
FAC (long distance code) Each trainee is given a “forced access code” that will allow you to make patient-related long distance calls (not international). This can be found in New Innovations. To use, please dial an “8” first. You will hear two beeps, then enter the FAC number. Once you hear a dial tone, dial your long distance number as normal, including the “1” at the beginning.
56
ID Badges ID badges must be worn at all times above the waist. If you have a problem with your card not giving you proper access to a building or area, please call the GME Office at 243-6297.
Loan Forbearance Both the GME Office and your Coordinator can complete these forms.
Meal Money Some services with a heavy inpatient presence receive a monthly meal allowance. This process is driven by the Housestaff Council. If you are on a service that does get meal money, this is loaded onto your ID badge on the first of every month. The Orthopaedic Hand Fellow does not take overnight call, and therefore does not receive these funds.
New Innovations All of the trainee’s personal information, including relevant identification numbers (NPI, DEA, SMS, Virginia Medical License, etc) can be found in New Innovations. In the event that you forget your password or need to have it reset, your Coordinator can help you.
Parking Policy
If you elect not to get parking and change your mind during the year, please contact Diane Farineau in the GME Office. Please know that the University has a ZERO TOLERANCE POLICY concerning staff, faculty, or trainee parking in patient parking areas. Also, please be aware that your parking will need to be renewed in May, prior to your departure, that will cover your final months. You will be notified by email when it is due. Please see the Housestaff Policy webpage at http://www.healthsystem.virginia.edu/internet/housestaff/benefits.cfm#parking for current parking information.
Payday Payday for GME members is bi-weekly. The first two paychecks must be picked up in person, by you, at the Payroll Office, 1222 Jefferson Park Avenue, 2nd floor, between 8:00am and 5:00pm. After the first two pays, your check will be automatically deposited to the bank account designated by you on the Direct Deposit form submitted during orientation.
Personal Information Changes Please alert the GME Office and your coordinator if you move, get married, have children, etc, so that your records can be appropriately updated.
57
TB Tests and Mask Fitting These happen annually. They are conditions of continued employment. Failure to meet these requirements may result in your suspension without pay. Directions will be sent to you from Employee Health.
Website Please familiarize yourself with the GME website for information about educational programming and opportunities, such as the GME Certificate Program, and the GME Institutional Curriculum series, the Housestaff Council, and other resources for trainees. http://www.healthsystem.virginia.edu/internet/housestaff/housestaff.cfm.
Computer, AV Equipment and the Resident Library The main medical library is staffed with exceptional employees and is well stocked with current orthopaedic textbooks and journals. A vast array of journals, textbooks, computes, and databases are available from 7am to midnight daily in the library. Additional computers are available in the call room, ER, inpatient floor, and department offices. The Orthopaedic Department has its own orthopaedic library, with current journals and textbooks, which can be used for quick reference work. Additionally, there are work cubicles available for trainee use. A collection of Academy OKU and self-assessment CD’s are available for checkout. Computer terminals with internet access are available in all clinical settings.
Counseling Services The pressures and demands of medical training can be stressful both to the individual and to relationships. Confidential evaluation and treatment services are available through a number of resources. Should service be desired, contact the GME Office and/or the Faculty and Employee Assistance Program (FEAP).
Resident Call and Coverage The following policies are in effect regarding resident call and coverage.
Call Schedule and Responsibilities The objective of on-call activities is to provide residents with continuity of patient care experiences throughout a 24-hour period. In-house call is defined as those duty hours beyond the normal workday when residents are required to be immediately available in the assigned institution. PGY-2 and PGY-4 residents rotate on the Night Float service which covers 7pm to 7am Sunday through Thursday each week. Daytime Trauma residents take over during the weekdays. Friday 7am through Sunday 7pm the PGY-2 residents
58
take in-house call every third weekend on average. PGY-3 through PGY-5 residents take no in-house call. The PGY-3 and PGY-4 residents take pager call every third weekend on average. Chief (PGY-5) residents take second call from home every third weekend on average, and are responsible for all patients seen in the ER and all consults and must be available to immediately assist junior residents with difficult patients in the ED or on the floor.
Night Float • Night float residents (PGY-2 and PGY-4) rotate on in-house call from 7pm
– 7am Sunday through Thursday and are allowed to operate until noon on Fridays ONLY.
• The remaining residents take call from Friday night through Sunday at 7pm when the night float residents return.
• Conference attendance is required for all residents on the night float rotation.
Detailed Call Schedule
Pager #1206 (Ortho In-House Resident on call) • Monday – Thursday 7am to 7pm, Friday 7am to 4pm: Day call junior
resident • Sunday – Thursday nights 7pm to 7am: Night float junior resident • Friday 4pm to Saturday 6am: Weekend Friday/Sunday junior resident on
call • Saturday 6am to Sunday 6am: Weekend Saturday junior resident on call • Sunday 6am to 7pm: Weekend Friday/Sunday junior resident on call
The junior resident is required to talk to the Chief on call about all consults. The Chief Resident should be involved in all decisions regarding in-patient and out-patient consults and is to direct triage and patient management of all consults. The Chief Resident on call is to review all fracture and joint reductions, particularly before a patient is discharged from the ER.
Pager #1251 (Ortho ER Resident on call) • Monday – Thursday 7am to 7pm, Friday 7am to 4pm: Day call junior
resident • Sunday – Thursday nights 7pm to 7am: Night float junior resident • Friday 4pm to 11pm: Weekend Friday/Sunday mid-level resident on call • Friday 11pm to Saturday 6am: Weekend Friday/Sunday junior resident on
call • Saturday 6am to 11pm: Weekend Saturday mid-level resident on call • Saturday 11pm to Sunday 6am: Weekend Saturday junior resident on call • Sunday 6am to 7pm: Weekend Friday/Sunday mid-level resident on call
59
The PGY-3 and 4 resident covering E.R. calls on Friday and Saturday must be available even after 11 pm to assist in operative cases and to assist the in-house junior resident who takes over primary call at 11 pm. While the senior may not get direct E.R. consults after 11 pm they must be available to assist the junior resident and provide guidance and be involved in all operative cases that go to the O.R. on Friday and Saturday nights.
Pager #1218 (Ortho Chief Resident on call) • Monday – Thursday 6am to 6pm, Friday 6am to 4pm: Day call chief
resident • Sunday – Thursday nights 6pm to 6am: Night float chief resident • Friday 4pm to Saturday 6am: Weekend Friday/Sunday chief resident on
call • Saturday 6am to Sunday 6am: Weekend Saturday chief resident on call • Sunday 6am to 7pm: Weekend Friday/Sunday chief resident on call
The night float chief and the chief resident covering weekend call is required to be involved in every consult that is seen during call coverage and be the direct contact to the faculty on call for all operative cases and admissions. The chief residents are required to provide guidance for posting all surgical cases so that appropriate equipment and positioning is on the posting slip so that there are no delays during surgical intervention. The Chief Resident or Night Float Chief is required to see all admissions, operative cases, and patients with a change in status (transfer to unit).
Call Coverage During Special Events 1. OITE Examination (November) – Two fellows take call (Friday 8pm –
Saturday 6pm), covering floor and ER call. All residents are off call from Friday 8pm through Saturday 6pm when normal call resumes.
2. ORS/AAOS (Winter/Early Spring) – R-4 assumes role of Chief resident Friday through Sunday as follows:
Tuesday – Thursday – Night Float Residents (normal) Friday – Saturday – PGY-4 (Chief), PGY-3 (ER), PGY-2 (In-House) Sunday until 7pm – PGY-4 (Chief), PGY-3 (ER), PGY-2 (In-House) Sunday after 7pm – Night Float Residents (normal)
3. Visiting Professor Lectureship (Graduation Weekend, May/June) • Visiting Professor arrives in Charlottesville on Thursday afternoon
for dinner with the Chiefs residents • Friday is educational day culminating in the graduation banquet • Leisure activities end by 3pm on Saturday • All Chiefs will make 15-20 minute presentation to the Visiting
Professor, suitable for publication but not necessarily submitted. An outline or manuscript is required to be delivered 2 – 4 weeks prior to lectureship to the Program Director for review and approval

60
• Chiefs are excused from call from Thursday evening until Sunday 7am; all services to be managed by other residents during this time
Thursday – Night Float Residents (normal) Friday – PGY-4/3 (Chief), AOTP/PGY-2(ER-In House/24hr), PGY-1 (In-House-16hr) Saturday 7am-3pm – PGY-4/3 (Chief), AOTP/PGY-2 (ER-In House/24 hr), PGY-1 (In-House-16hr) Saturday 3pm – Sunday PGY-4/3 (Chief), AOTP/PGY-2 (ER-In House/24 hr), PGY-1 (In-House-16hr) Sunday – 7am – 7pm – Fellow (Chief), ER and In-house/1251 and 1206 – Regular Call Schedule
• Roanoke call – All residents will work through Thursday, with the on-call resident being released Thursday evening at 10pm so they can make it back to Charlottesville for Friday morning’s lectureship start. All residents are free of clinical duties on Friday and Saturday until 3pm when the on-call resident is to return for call by 5pm in Roanoke Saturday night.
High School Football Coverage Resident physicians in the department of Orthopaedic Surgery at the University of Virginia may elect to cover high school football games in the city of Charlottesville, Albemarle County, and other neighboring counties. This is an elective outreach program sponsored by the Department of Orthopaedics that will abide by the following guidelines:
1. Each resident will be linked to an attending physician. Prior to each session each resident physician will be assigned to an attending physician for supervision, call, etc.
2. Resident coverage of high school sports is not required as a part of the residency curriculum; this is an elective. Those who desire this educational experience provide coverage on a strictly volunteer basis. Goals and objectives of this elective will be reviewed with the resident prior to the elective.
3. Each resident who covers a high school sports team will be required to attend the annual athletic team coverage orientation which is held annually during the first week of August. UVA attending physicians provide current information regarding athletic injury recognition, management, and return-to-play guidelines. CPR training/certification is also offered during this orientation course.
4. Resident physicians will not directly receive payment or compensation in any form from the high schools they are covering. Travel cost reimbursement of no more than $10 per game covered may be paid directly to the resident by the school. All other monetary contributions from high schools will be paid directly to the University of Virginia, Department of Orthopaedic Surgery Alumni Fund. This money will be earmarked for use by residents providing coverage to purchase books, fund additional conference travel/registration fees, etc. Funds from this source may also be used to support the annual athletic team coverage orientation.
61
5. The residents will be covered by their University of Virginia liability insurance when providing coverage of these games.
6. As this is a recognized elective educational activity, time spent covering sporting events does count against duty hour work requirements. It is not considered moonlighting as resident physicians do not receive direct payment for their services.
7. Since this is an elective, all residents participating will be evaluated by the attending providing supervision.
Emergency Department Holiday & Weekend Night Call 1. The PGY3/4 resident on ER call (1251 pager) will handle all emergency
room consults between 4pm to 11pm (Fridays), 6am to 11pm (Saturdays), and 6am to 7pm (Sundays). The resident will evaluate and present each patient to the chief resident and attending physician on-call, and will accompany all surgical cases to the operating room regardless of the time of the case during that 24 hour period.
2. The In-House PGY2 resident (1206 pager) will handle emergency room calls while the ER resident is in the operating room, and will handle all calls from the floor, all inpatient consults, and all ER consults between the hours of 11pm and 6am with the PGY3/4 resident on call providing backup.
3. The resident is to inform the Chief Resident on call of all emergency admissions to the individual service before admission is arranged. It is the chief resident’s responsibility to ensure that the attending orthopaedic surgeon has seen the patient pre-operatively and is present for the operative procedure.
4. Before leaving each day, the resident should sign out to the resident on In-House call and provide complete information about existing or anticipated problems on the service. It is necessary to check the EPIC service specific list and electronic board the first thing each morning for admissions and messages for each particular service.
All patient encounters in the Emergency Department must be discussed with the attending on call. PGY-1 or PGY-2 residents must also communicate with the Chief Resident on call and the Chief Resident is required to be present for the performance of procedures with which the junior resident is not yet proficient or experienced. Documentation of Emergency Room encounters must reflect that the case was discussed with the Attending on call. In addition, if follow-up care is to be provided by another attending based on subspecialty, this must be so noted in the dictation, with the name of the particular attending with whom the patient will follow-up.