2008 post conference update: chest. epidemiology
TRANSCRIPT
2008 Post Conference Update:CHEST
Epidemiology

PAH Registries: Functional Class at Diagnosis Indicates Delayed Diagnosis
Frost AE. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AP2217.
% Patients NYHA Functional Class III-IV at Diagnosis
72 73 7380
7175
0
20
40
60
80
100
REVEAL REVEAL-TR REVEAL NIH PHC NIH French
N=2967 N=2364 N=1009 N=578 N=187 N=674
Per
cen
t (%
)
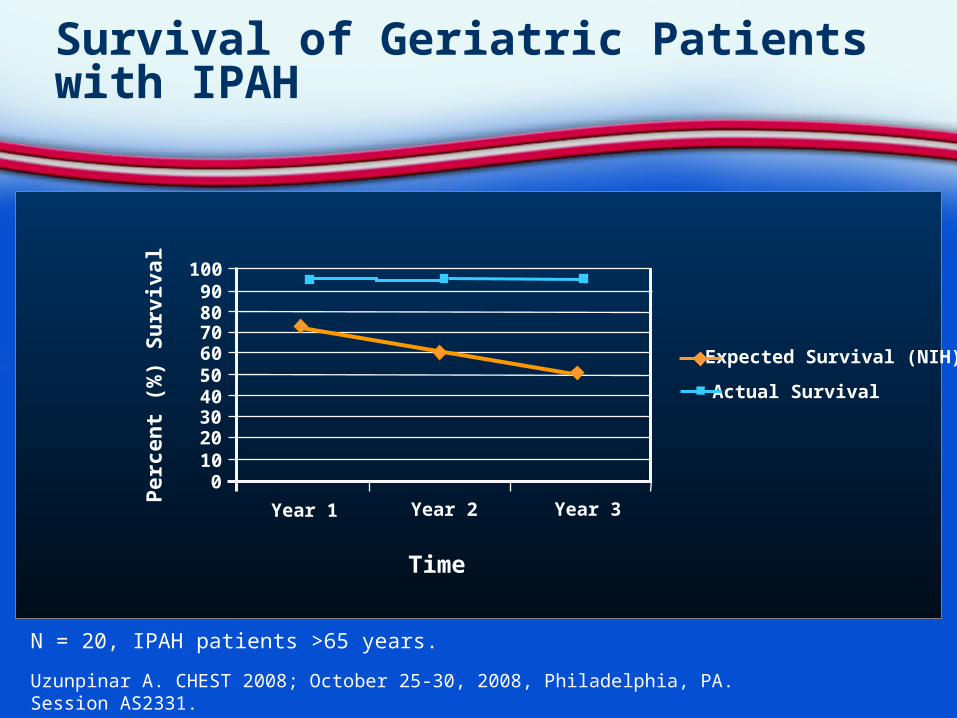
Survival of Geriatric Patients with IPAH
Uzunpinar A. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2331.
N = 20, IPAH patients >65 years.
Per
cen
t (%
) S
urv
ival
100908070605040302010
0
Year 1 Year 2 Year 3
Time
Expected Survival (NIH)
Actual Survival
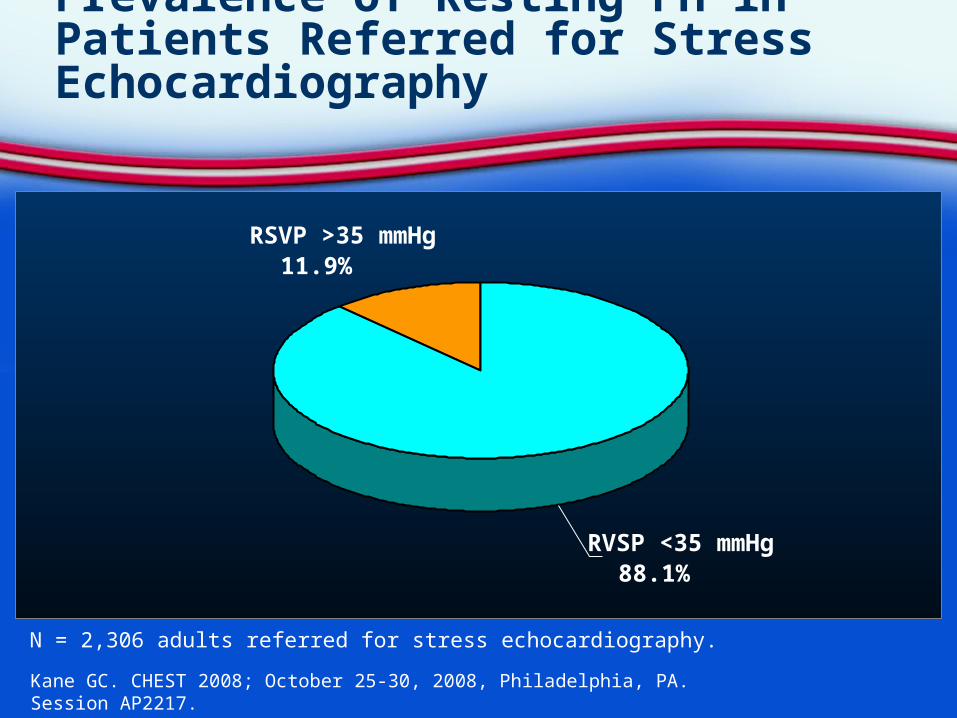
Prevalence of Resting PH in Patients Referred for Stress Echocardiography
Kane GC. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AP2217.
N = 2,306 adults referred for stress echocardiography.
RSVP >35 mmHg 11.9%
RVSP <35 mmHg 88.1%
Diagnostic and Outcomes Markers
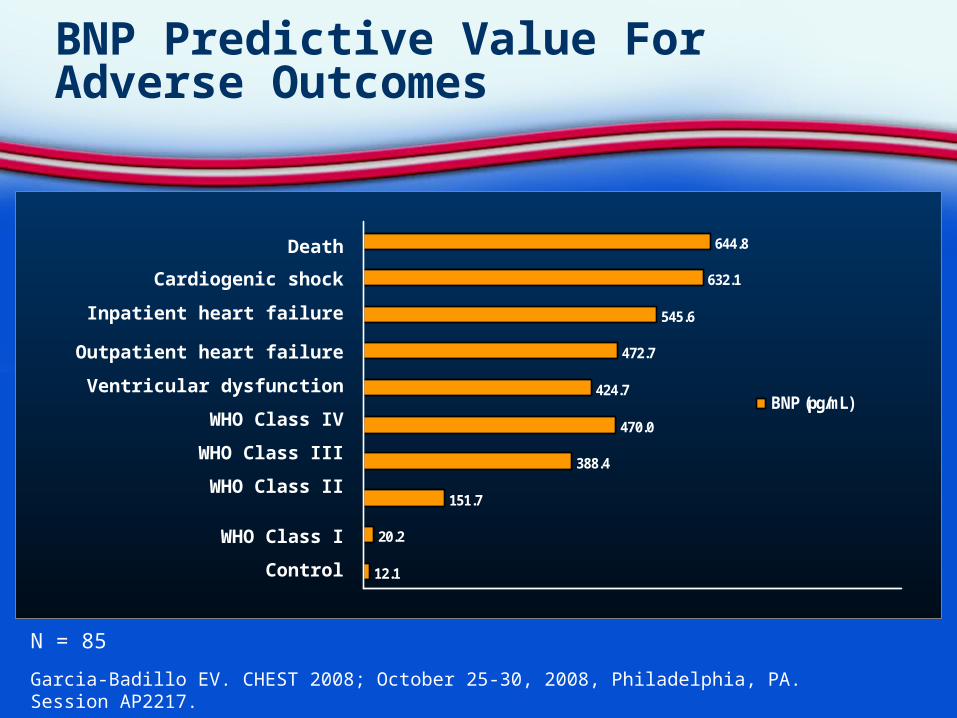
BNP Predictive Value For Adverse Outcomes
Garcia-Badillo EV. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AP2217.
Death
Cardiogenic shock
Inpatient heart failure
Outpatient heart failure
Ventricular dysfunction
WHO Class IV
WHO Class III
WHO Class II
WHO Class I
Control 12.1
20.2
151.7
388.4
470.0
424.7
472.7
545.6
632.1
644.8
BNP (pg/mL)
N = 85
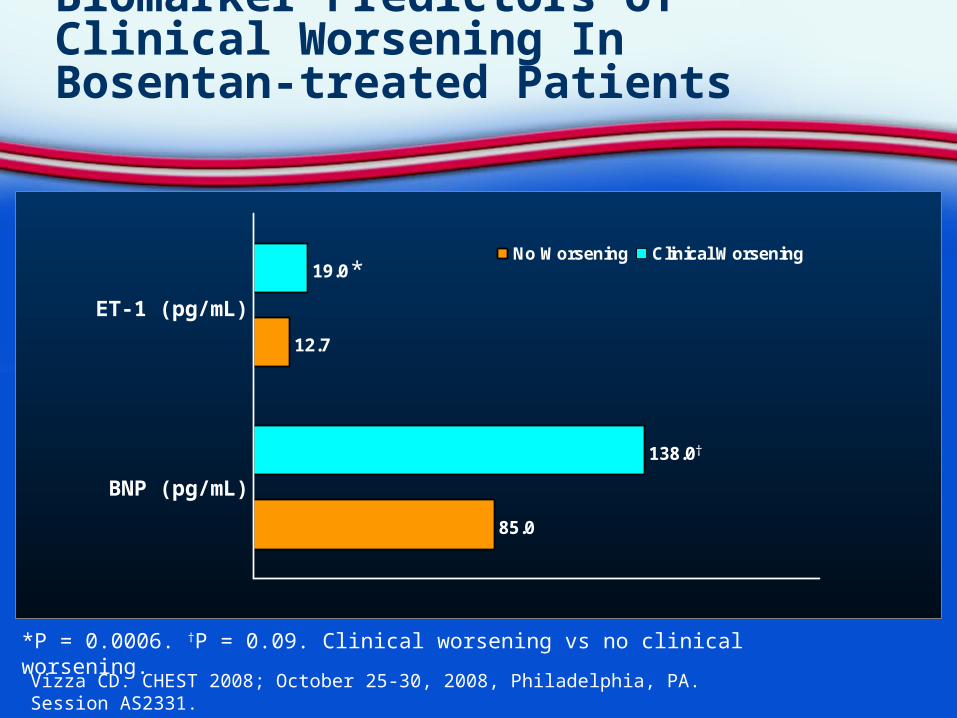
Biomarker Predictors of Clinical Worsening In Bosentan-treated Patients
Vizza CD. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2331.
*P = 0.0006. †P = 0.09. Clinical worsening vs no clinical worsening.
ET-1 (pg/mL)
85.0
138.0
19.0
12.7
No Worsening Clinical Worsening
BNP (pg/mL)
†
*
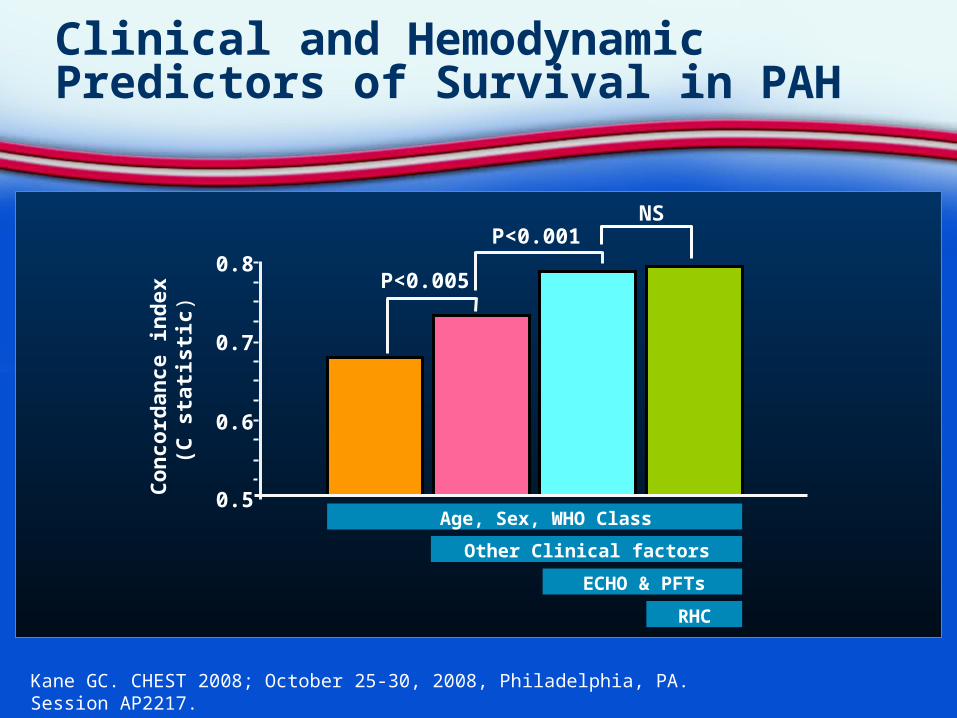
Clinical and Hemodynamic Predictors of Survival in PAH
Kane GC. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AP2217.
Co
nco
rdan
ce in
dex
(C
sta
tist
ic)
0.8
0.7
0.6
0.5
P<0.005
P<0.001NS
Other Clinical factors
RHC
Age, Sex, WHO Class
ECHO & PFTs
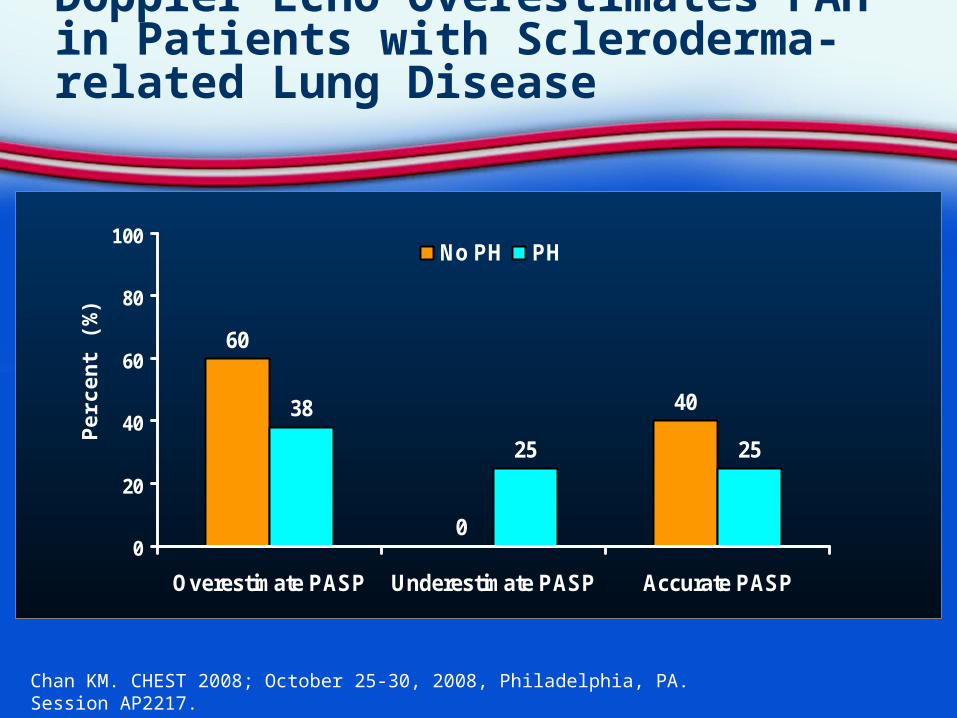
Doppler Echo Overestimates PAH in Patients with Scleroderma-related Lung Disease
Chan KM. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AP2217.
60
0
4038
25 25
0
20
40
60
80
100
Overestimate PASP Underestimate PASP Accurate PASP
No PH PH
Per
cen
t (%
)

PAH in Obese Patients: BMI Correlates With Worsening Hemodynamics
Kaw R. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AP2217.
N = 1600, patients undergoing right heart catheterization for suspected PH.*p < 0.05 versus comparator.
70
60
50
40
30
20
10
0RA Mean PA Systolic PA Diastolic PA Mean PCWP Mean
mm
Hg
BMI < 25 25≤BMI>30 30≤BMI>35 BMI≥35
**
*
*
*
*
*
* **
*
*
*

Clinical Pharmacology
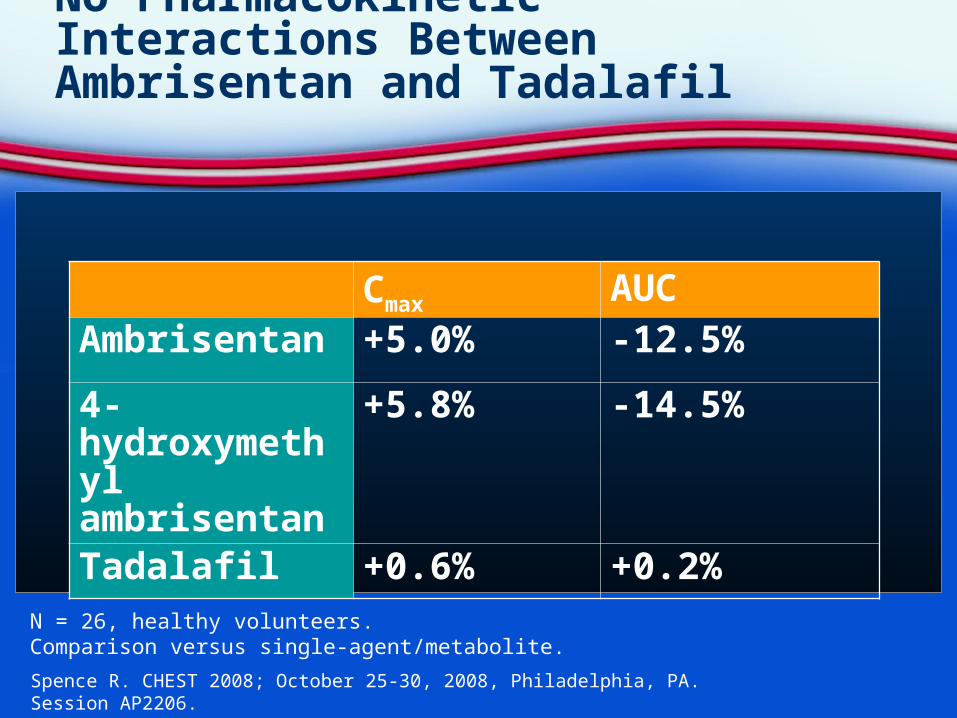
No Pharmacokinetic Interactions Between Ambrisentan and Tadalafil
Spence R. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AP2206.
Cmax AUCAmbrisentan +5.0% -12.5%4-hydroxymethyl ambrisentan
+5.8% -14.5%
Tadalafil +0.6% +0.2%
N = 26, healthy volunteers.Comparison versus single-agent/metabolite.
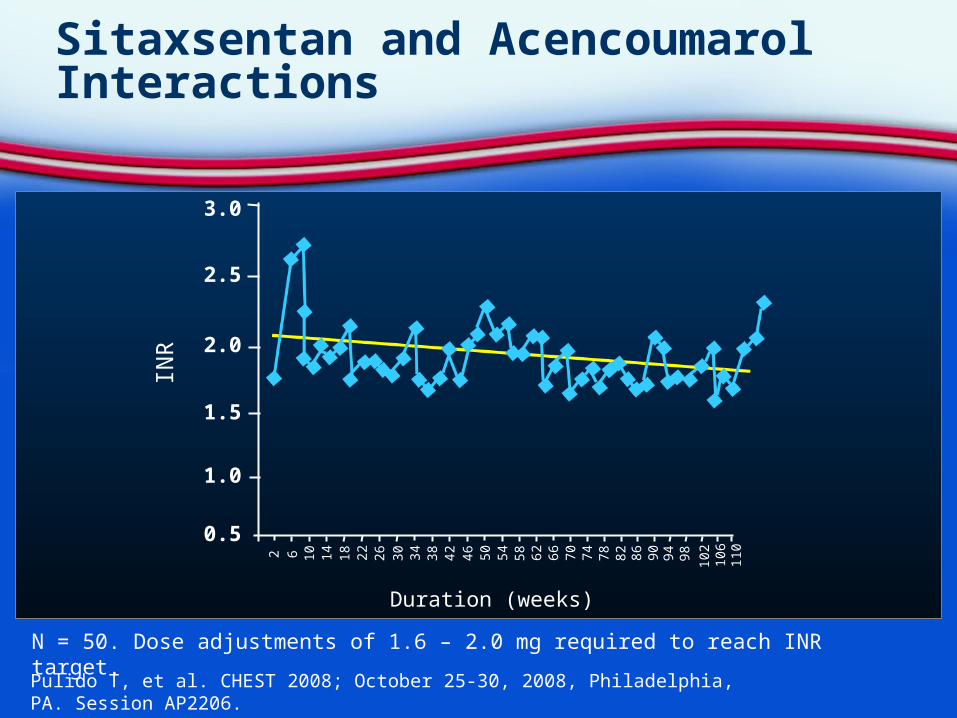
Sitaxsentan and Acencoumarol Interactions
Pulido T, et al. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AP2206.
N = 50. Dose adjustments of 1.6 – 2.0 mg required to reach INR target.
3.0
2.5
2.0
1.5
1.0
0.5
2
Duration (weeks)
INR
6 10 14 18 22 26 30 34 38 42 46 50 54 58 62 66 70 74 78 82 86 90 94 98 102
106
110

Short-term Clinical Trials
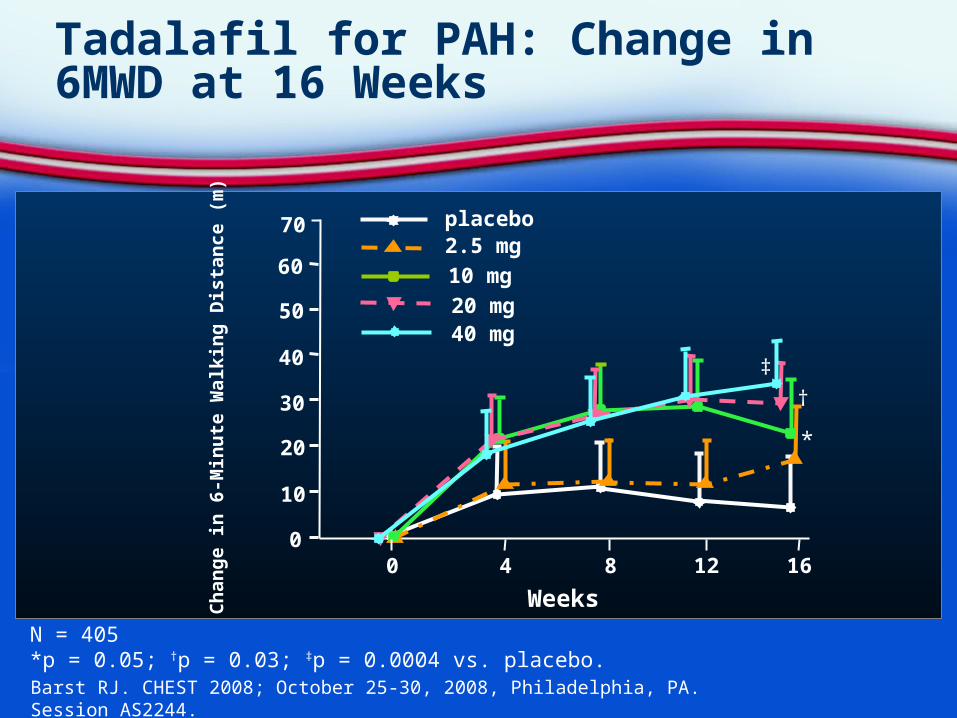
Tadalafil for PAH: Change in 6MWD at 16 Weeks
Barst RJ. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
N = 405*p = 0.05; †p = 0.03; ‡p = 0.0004 vs. placebo.
†
*
‡
70
60
50
40
30
20
10
00 4 8 12 16
placebo2.5 mg
10 mg
20 mg40 mg
Weeks
Ch
ang
e i
n 6
-Min
ute
Wal
kin
g D
ista
nce
(m
)
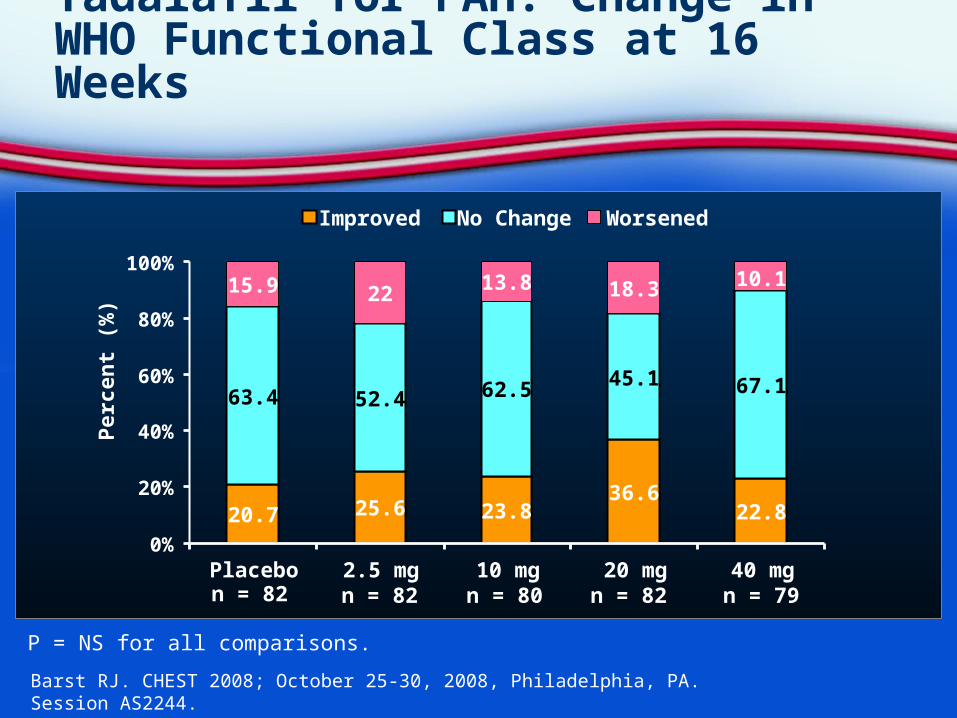
Tadalafil for PAH: Change in WHO Functional Class at 16 Weeks
Barst RJ. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
P = NS for all comparisons.
Per
cen
t (%
)
n = 82 n = 82 n = 82 n = 80 n = 79
20.7 25.6 23.836.6
22.8
63.4 52.4 62.5 45.1 67.1
15.9 22 13.8 18.3 10.1
0%
20%
40%
60%
80%
100%
Placebo 2.5 mg 10 mg 20 mg 40 mg
Improved No Change Worsened

Long-term Clinical Trials
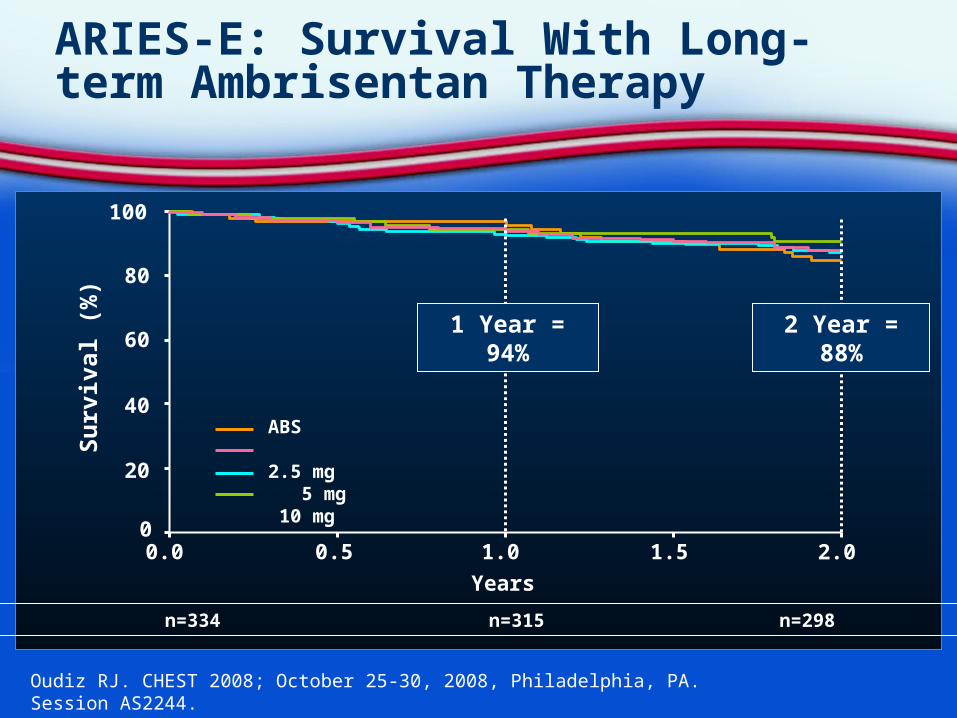
ARIES-E: Survival With Long-term Ambrisentan Therapy
Oudiz RJ. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
0
20
40
60
80
100
0.0 0.5 1.0 1.5 2.0
Years
Su
rviv
al (
%)
ABS 2.5 mg 5 mg 10 mg
At Risk: n=383 n=334 n=315 n=298 n=255
2 Year = 88%1 Year = 94%
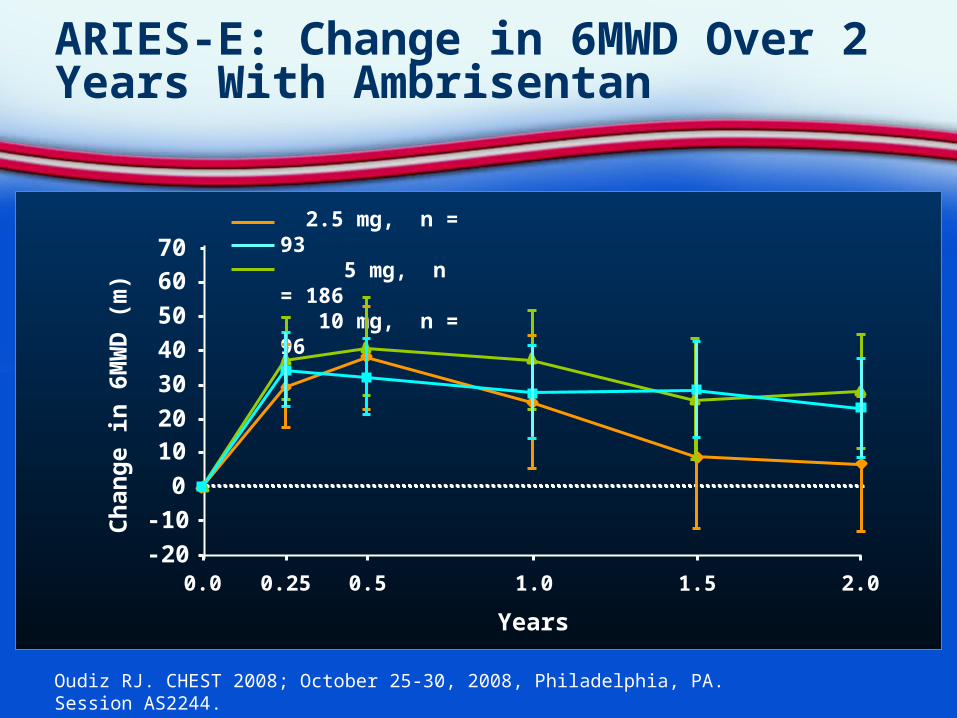
ARIES-E: Change in 6MWD Over 2 Years With Ambrisentan
Oudiz RJ. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
Ch
ang
e in
6M
WD
(m
)
Years
-20
-10
0
1020
30
40
50
60
0.0 0.25 0.5 1.0 1.5 2.0
70 2.5 mg, n = 93 5 mg, n = 186 10 mg, n = 96
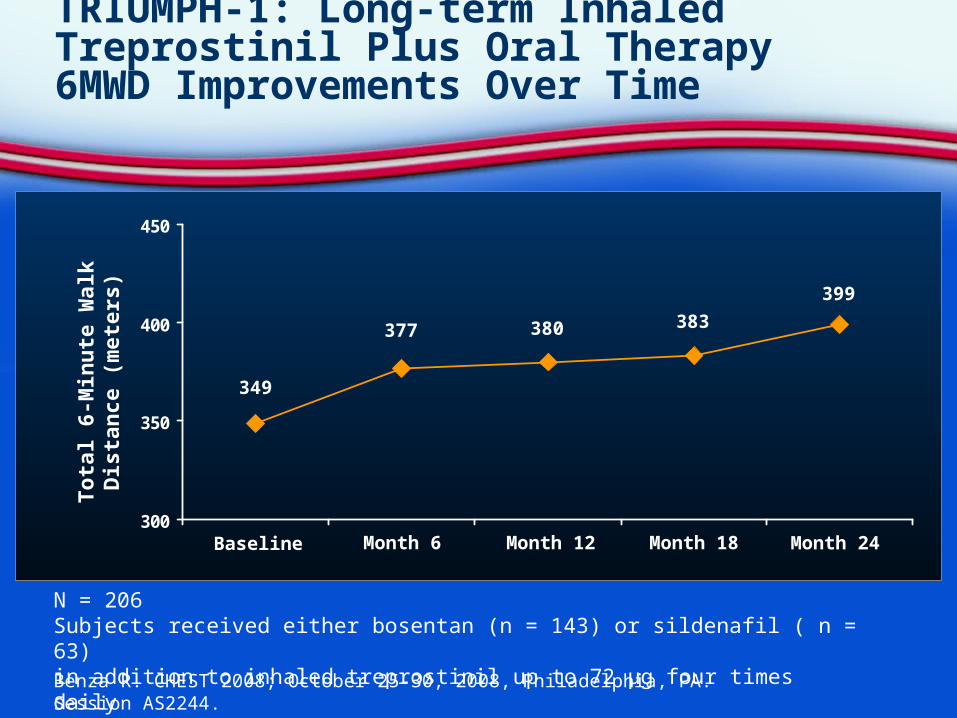
TRIUMPH-1: Long-term Inhaled Treprostinil Plus Oral Therapy 6MWD Improvements Over Time
Benza R. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
300
350
400
450
Baseline Month 6 Month 12 Month 18 Month 24
349
377 380 383
399
N = 206Subjects received either bosentan (n = 143) or sildenafil ( n = 63) in addition to inhaled treprostinil up to 72 µg four times daily
To
tal 6
-Min
ute
Wal
kD
ista
nce
(m
eter
s)
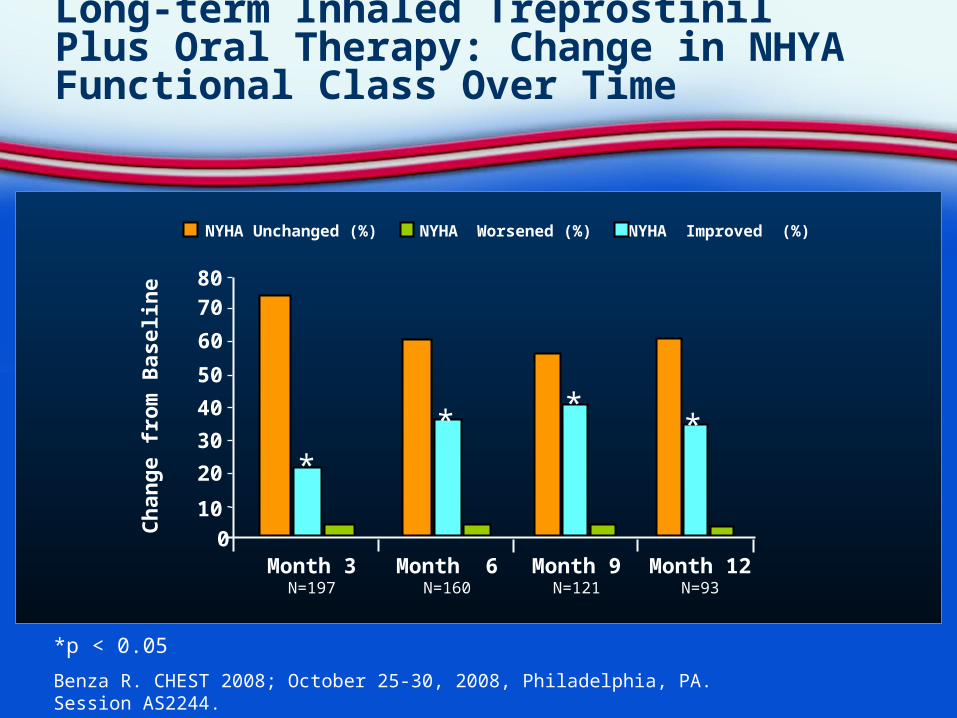
Long-term Inhaled Treprostinil Plus Oral Therapy: Change in NHYA Functional Class Over Time
Benza R. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
*p < 0.05
NYHA Unchanged (%) NYHA Worsened (%) NYHA Improved (%)
Month 12N=93
Month 9N=121
Month 6N=160
Month 3N=197
Ch
ang
e fr
om
Bas
elin
e
8070
60
50
40
30
20
10
0
***
*
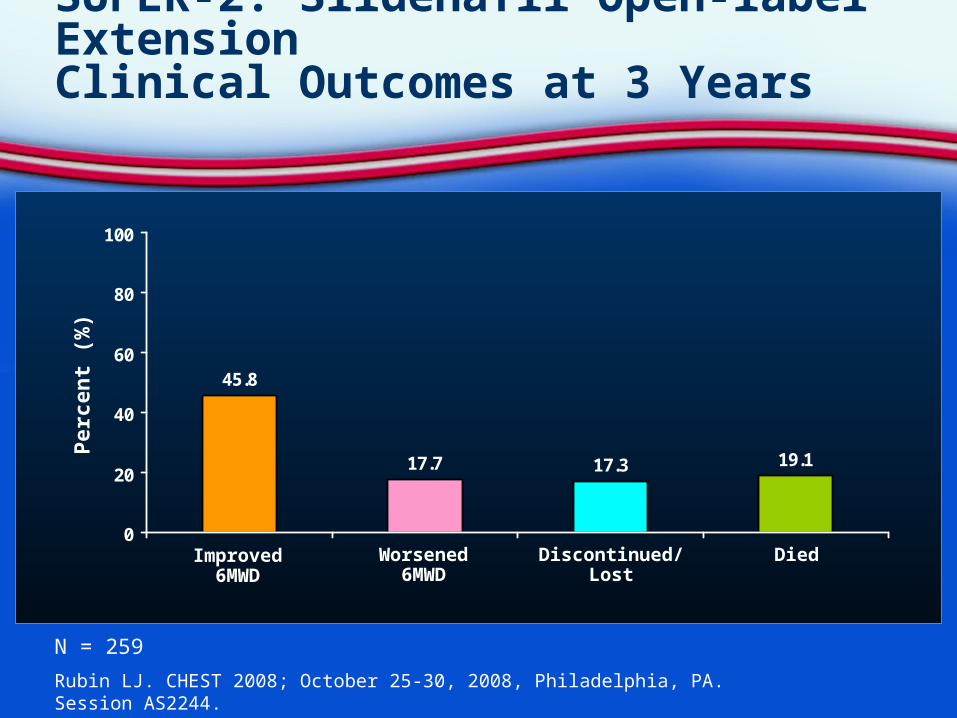
SUPER-2: Sildenafil Open-label ExtensionClinical Outcomes at 3 Years
Rubin LJ. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
45.8
17.7 17.3 19.1
0
20
40
60
80
100
Improved6MWD
Worsened6MWD
Discontinued/Lost
Died
Per
cen
t (%
)
N = 259
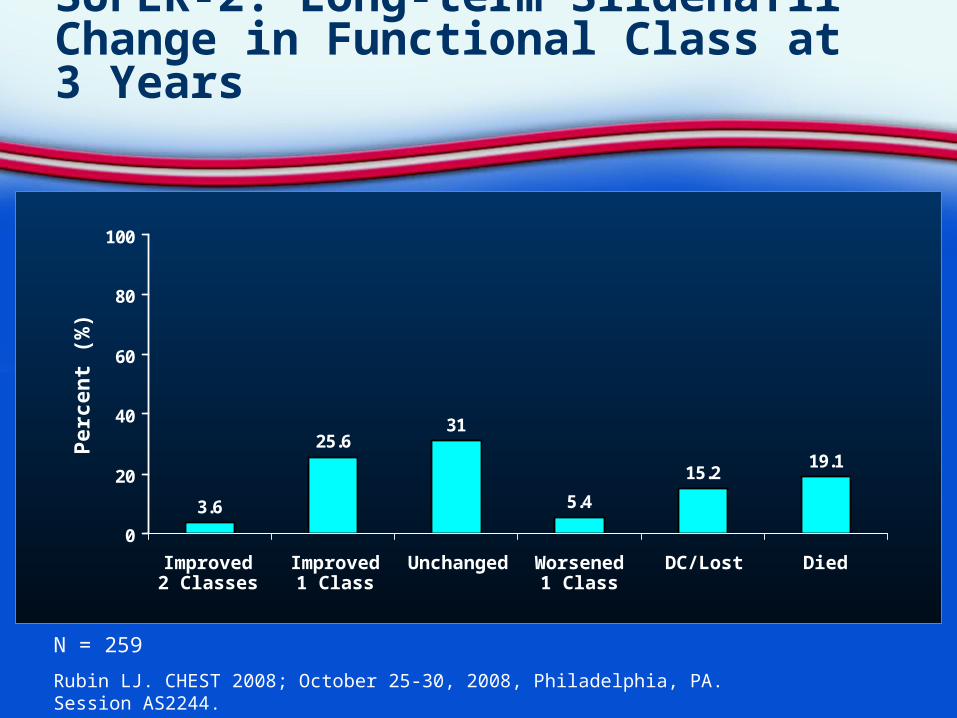
SUPER-2: Long-term Sildenafil Change in Functional Class at 3 Years
Rubin LJ. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
3.6
25.631
5.4
15.219.1
0
20
40
60
80
100
N = 259
Improved2 Classes
Improved1 Class
Worsened1 Class
Unchanged DC/Lost Died
Per
cen
t (%
)

Long-term Outcomes in Patients Transitioned From Epoprostenol to SC Treprostinil
Yan C. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
NNYA Functional Class Pre- and Post-Transition (6 months of therapy)
N = 30
60
50
40
30
10
20
0
Pe
rce
nta
ge
o
f P
ati
en
ts (
%)
NYHA CLASS
I II III IV
Pre-transition
Post-transition
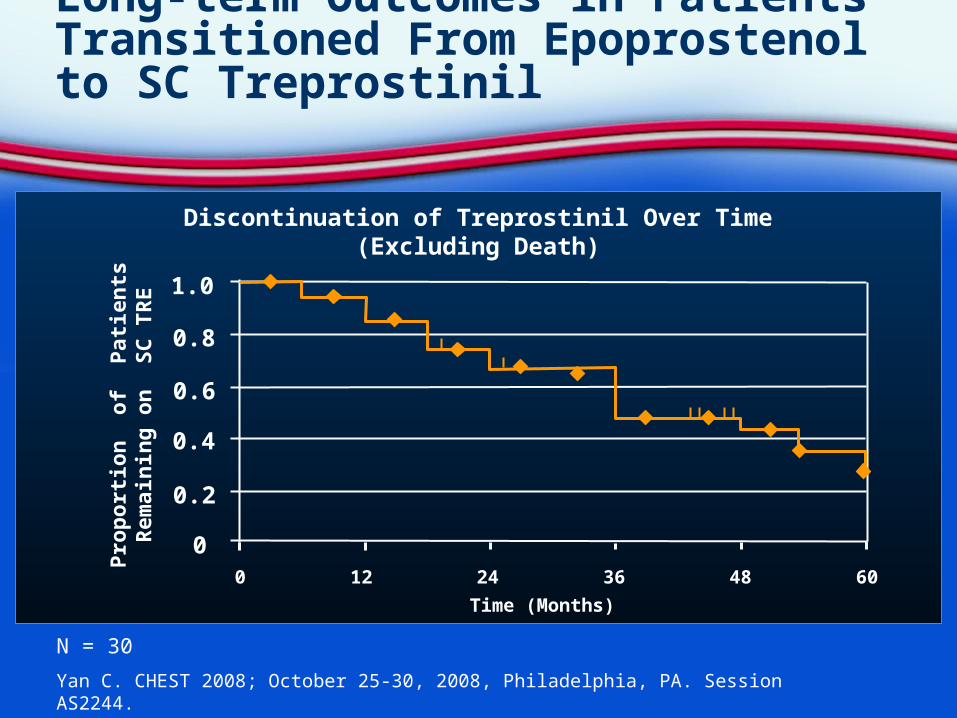
Long-term Outcomes in Patients Transitioned From Epoprostenol to SC Treprostinil
Yan C. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
Discontinuation of Treprostinil Over Time(Excluding Death)
N = 30
1.0
0.8
0.6
0.4
0.2
00 12 24 36 48 60
Time (Months)
Pro
po
rtio
n o
f P
atie
nts
Rem
ain
ing
on
SC
TR
E

Adverse Effects of PAH Therapies
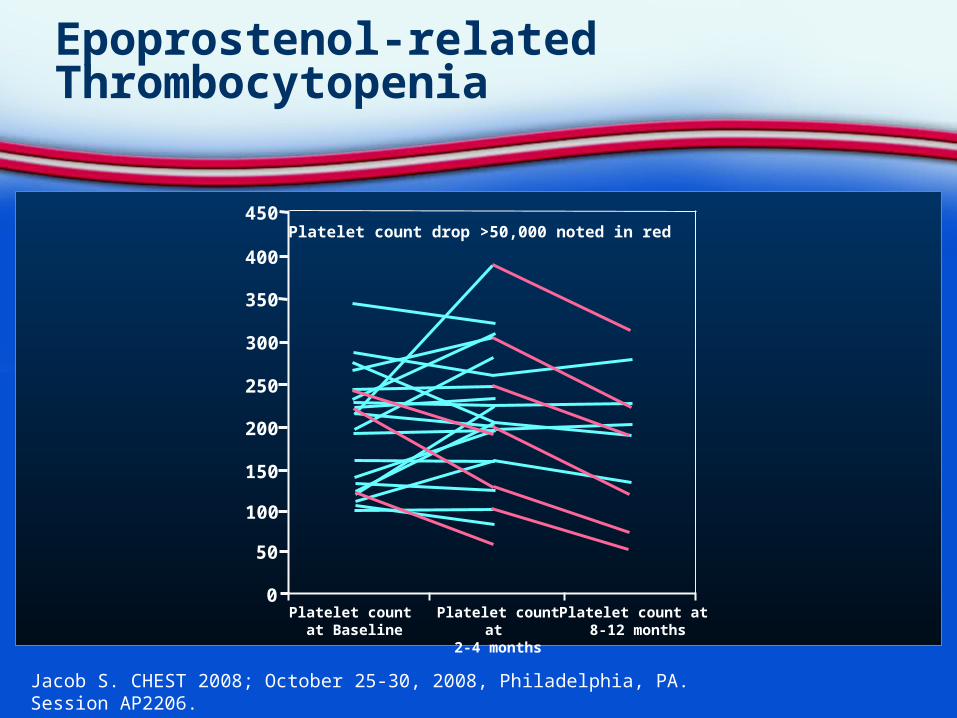
Epoprostenol-related Thrombocytopenia
Jacob S. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AP2206.
Platelet count drop >50,000 noted in red
Platelet count at Baseline
Platelet count at 2-4 months
Platelet count at 8-12 months
450
400
350
300
250
200
150
100
50
0
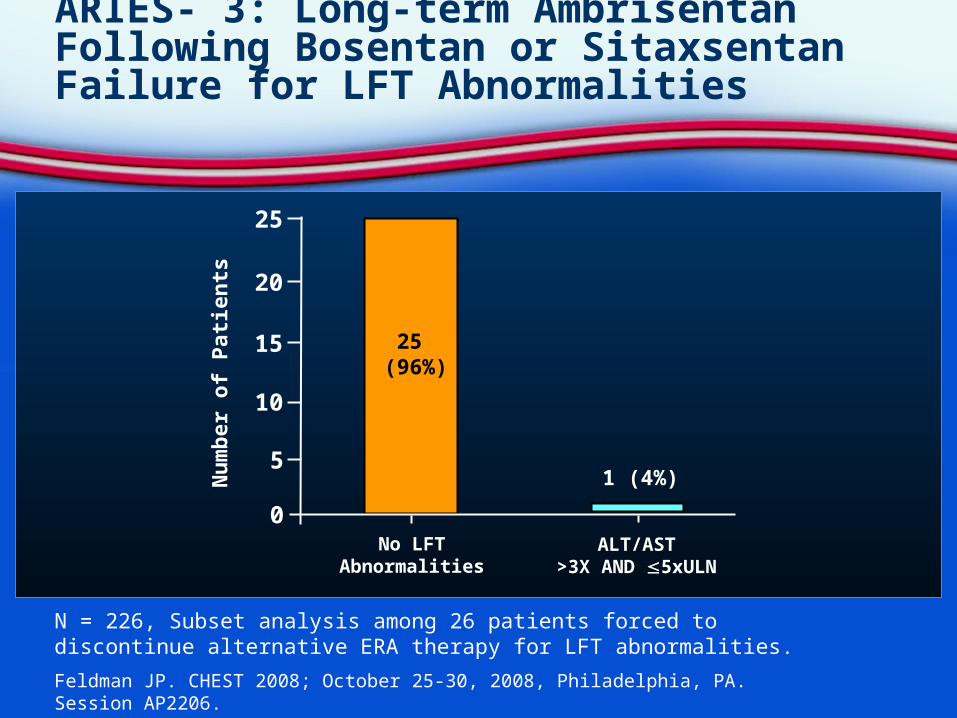
ARIES- 3: Long-term Ambrisentan Following Bosentan or Sitaxsentan Failure for LFT Abnormalities
Feldman JP. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AP2206.
N = 226, Subset analysis among 26 patients forced to discontinue alternative ERA therapy for LFT abnormalities.
25
20
15
10
0No LFT
AbnormalitiesALT/AST
>3X AND 5xULN
1 (4%)5N
um
ber
of
Pat
ien
ts
25 (96%)
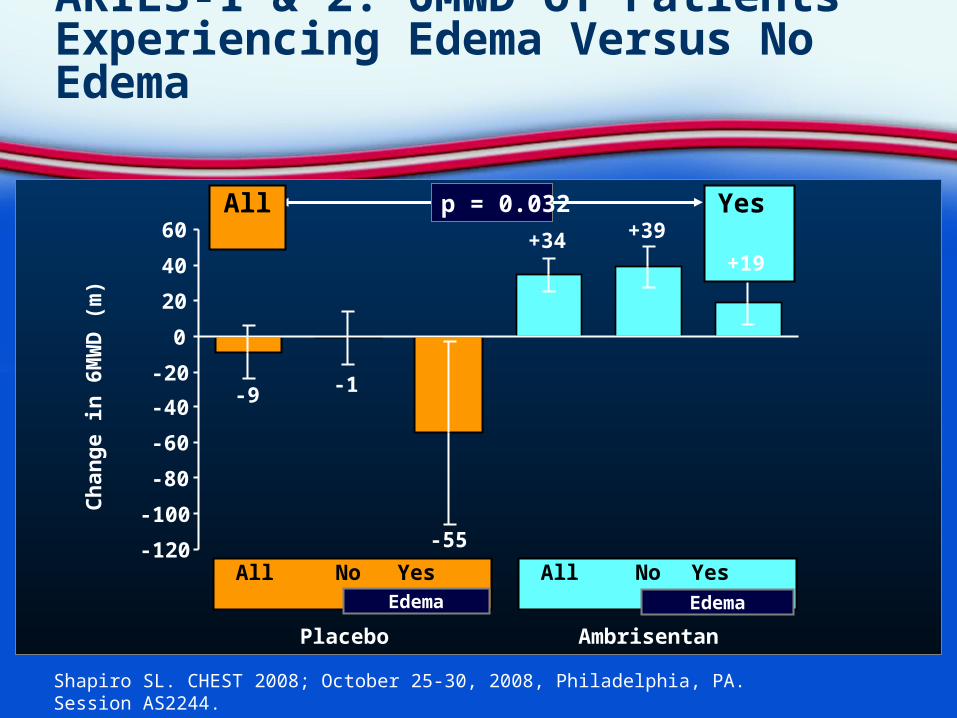
ARIES-1 & 2: 6MWD of Patients Experiencing Edema Versus No Edema
Shapiro SL. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2244.
Placebo Ambrisentan
All No Yes
All No Yes
-120
-100
-80
-60
-40
-20
0
20
40
60
Ch
ang
e in
6M
WD
(m
)
p = 0.032All Yes
-9 -1
-55
+34 +39
+19
EdemaEdema

Expanding Populations
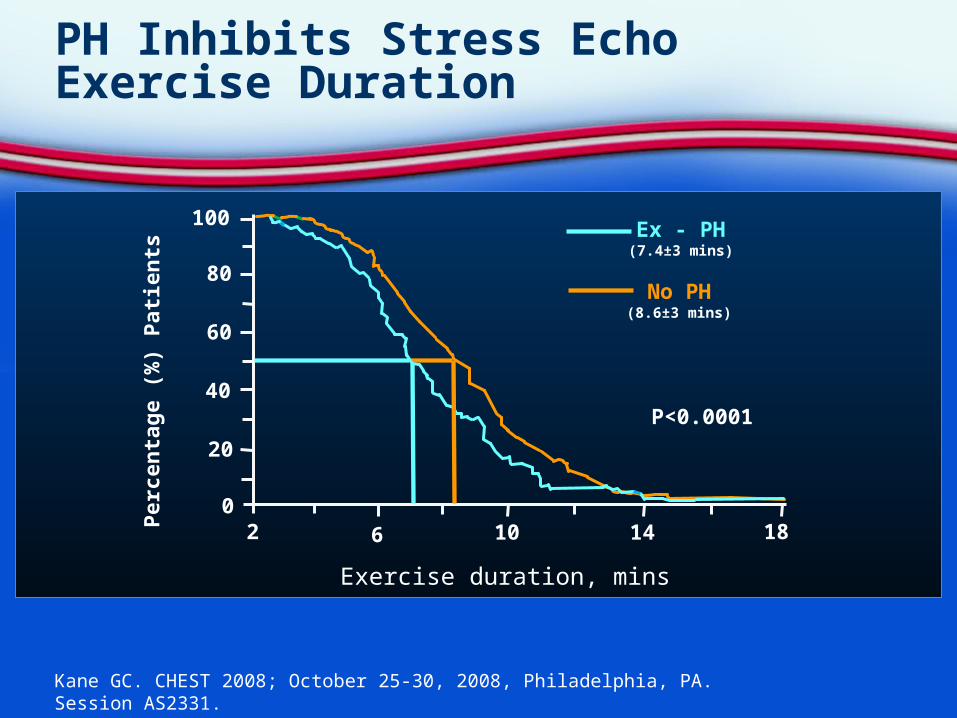
PH Inhibits Stress Echo Exercise Duration
Kane GC. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session AS2331.
Exercise duration, mins
6 10 14 182
100
80
60
40
20
0
No PH(8.6±3 mins)
Ex - PH(7.4±3 mins)
P<0.0001
Per
cen
tag
e (%
) P
atie
nts
PAH in Sickle Cell Disease
10% of sickle cell patients will have PAH/PH Pathophysiology not necessarily related to
occlusion— Soluble factors have been identified
Mixed PH (PAH combined with diastolic dysfunction) associated with 11-fold relative risk of mortality
Clinical trials of PAH medications in sickle cell have been slow to recruit
Barst RJ, Machado RF, Mubarak KK. CHEST 2008; October 25-30, 2008, Philadelphia, PA. Session 15983.

Summary: CHEST 2008
Evidence suggests PAH treatment can be effective in wide range of patient types and ages
Tadalafil may provide a new choice in PDE-5 inhibitor class
Inhaled treprostinil in combination with oral therapy may provide an additional choice in prostacyclin class
Long-term data for ambrisentan, sildenafil show 2+ years of benefit in survival and time to clinical worsening