1 hypothalamic-pituitary-adrenal axis suppression following topical corticosteroid administration...
Post on 20-Dec-2015
230 views
TRANSCRIPT

1
Hypothalamic-Pituitary-Adrenal Axis Hypothalamic-Pituitary-Adrenal Axis Suppression Following Topical Suppression Following Topical
Corticosteroid AdministrationCorticosteroid Administration
Jean Temeck, M.D.Jean Temeck, M.D.
Medical OfficerMedical Officer Division of Pediatric Drug DevelopmentDivision of Pediatric Drug Development
FDAFDA
2
TopicsTopics
• Regulation of glucocorticoid secretionRegulation of glucocorticoid secretion• Spectrum of hormonal effects on the HPA axisSpectrum of hormonal effects on the HPA axis• Spectrum of clinical manifestations of AISpectrum of clinical manifestations of AI• Importance of diagnosisImportance of diagnosis• Diagnostic hormonal testsDiagnostic hormonal tests• Risk factors for HPA axis suppressionRisk factors for HPA axis suppression
3
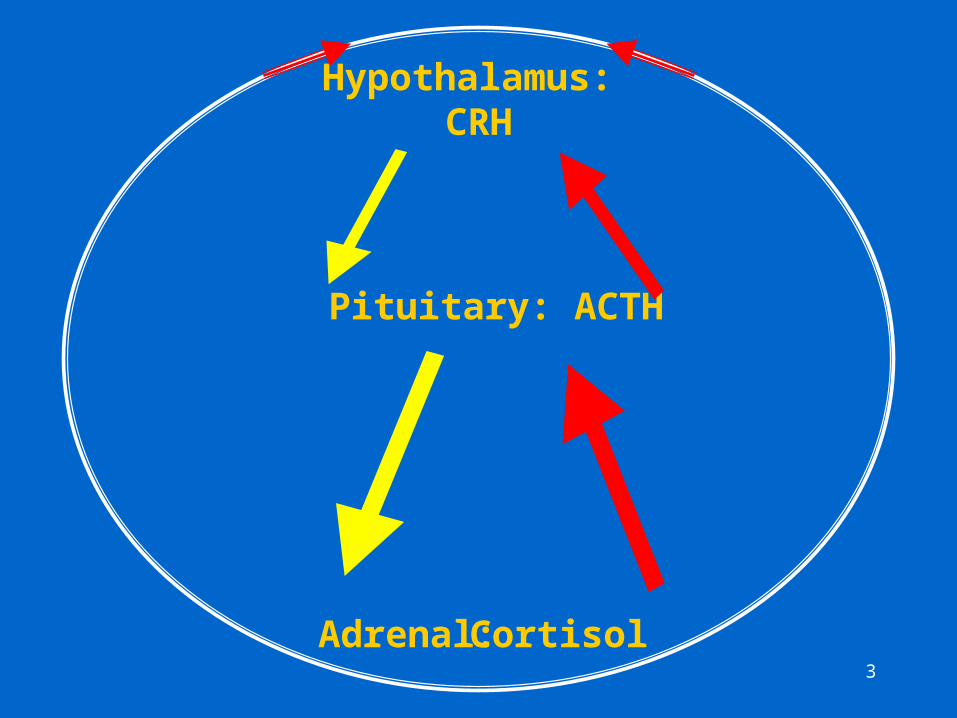
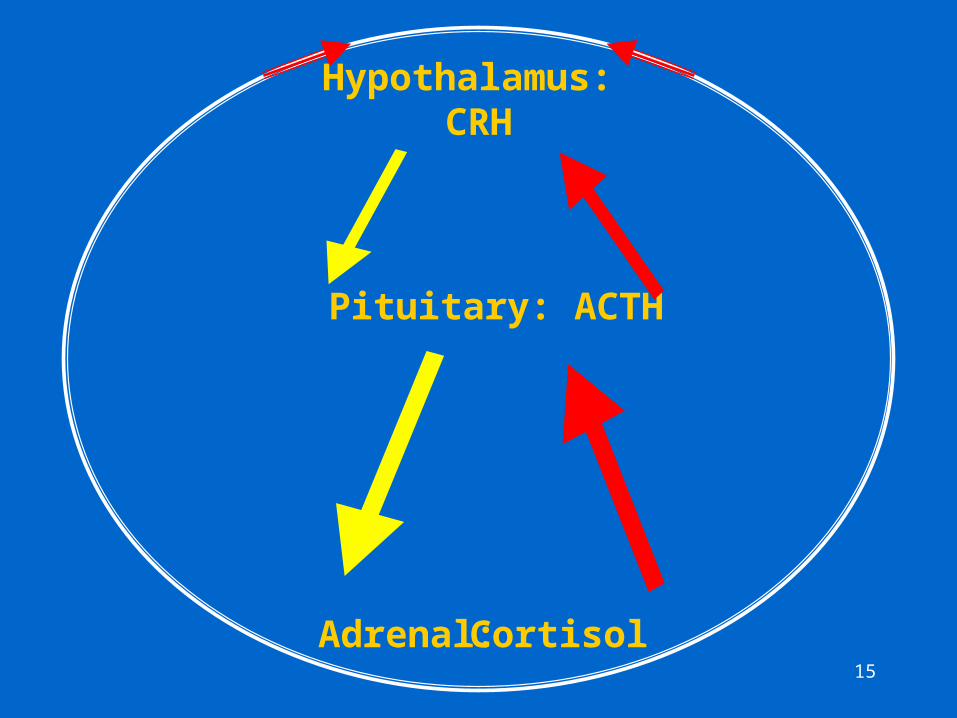
Hypothalamus: CRH
Adrenal: Cortisol
Pituitary: ACTH

4
Spectrum of Effects of Exogenous Spectrum of Effects of Exogenous Glucocorticoids on the HPA AxisGlucocorticoids on the HPA Axis
• Effects on the HPA axis are variable as is Effects on the HPA axis are variable as is individual susceptibility to suppression:individual susceptibility to suppression:– No HPA axis suppression
– HPA axis suppression: secondary or central AI:
• suppression of the pituitary and hypothalamic secretions of ACTH and CRH, respectively
• degree of suppression is variable

5
Spectrum of Effects of Exogenous Spectrum of Effects of Exogenous Glucocorticoids on the HPA AxisGlucocorticoids on the HPA Axis
• Partial (mild) ACTH suppressionPartial (mild) ACTH suppression– basal ACTH & cortisol levels may be normal
– pituitary response to stress is impaired, but adrenal response may be normal
• Complete ACTH suppressionComplete ACTH suppression– Adrenal gland atrophy with severe or prolonged
ACTH suppression; basal cortisol decreased; entire HPA axis suppressed
6
Clinical SpectrumClinical Spectrum
• Abnormal hormonal response clinically relevantAbnormal hormonal response clinically relevant
• May be subclinicalMay be subclinical
• Symptoms may be nonspecific and insidiousSymptoms may be nonspecific and insidious
• Adrenal crisis (triggered by stress)Adrenal crisis (triggered by stress)– fever
– severe hypotension
– shock
– coma
– death
7
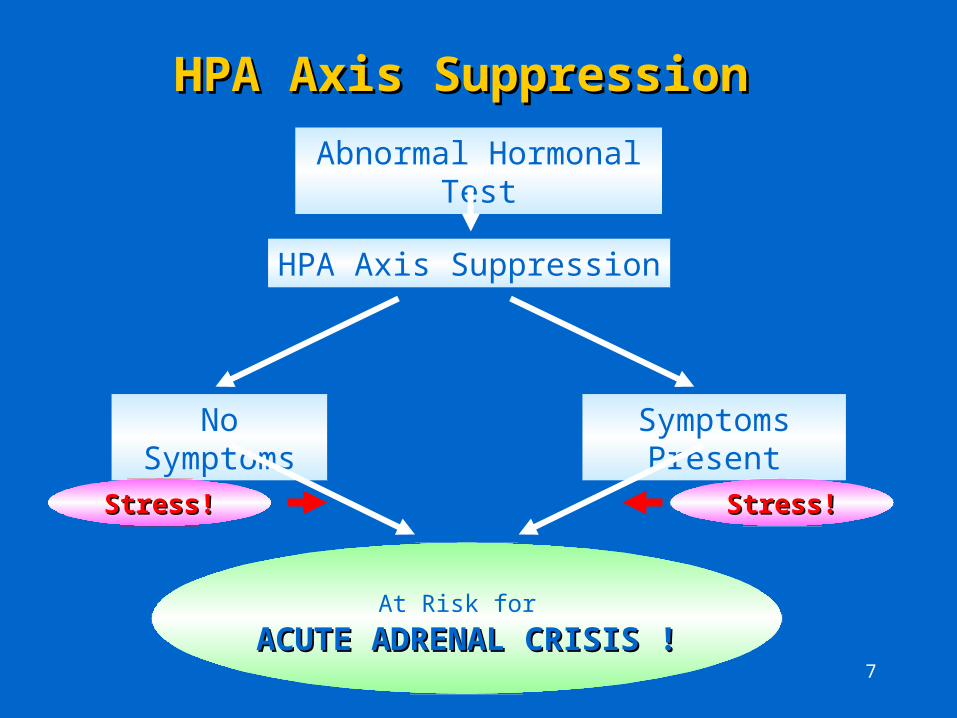
HPA Axis SuppressionHPA Axis Suppression Abnormal Hormonal Test
HPA Axis Suppression
No Symptoms Symptoms Present
At Risk for ACUTE ADRENAL CRISIS !ACUTE ADRENAL CRISIS !
Stress!Stress!Stress!Stress!

8
Features of Glucocorticoid-Induced Features of Glucocorticoid-Induced Adrenal InsufficiencyAdrenal Insufficiency
• Prevalence unknown:Prevalence unknown:– lack of clinical suspicion:lack of clinical suspicion:
• absorption of topical corticosteroids may be unrecognized
• diagnostic hormonal testing not performed
• signs and symptoms may be subtle and non-specific
• attribution made to other causes

9
Features of Glucocorticoid-Induced Features of Glucocorticoid-Induced Adrenal InsufficiencyAdrenal Insufficiency
• Prevalence unknown:Prevalence unknown:– failure to detect if recovery of suppression is failure to detect if recovery of suppression is
rapidrapid
– failure to detect if a diagnostic test of low failure to detect if a diagnostic test of low sensitivity (i.e. high false negative rate) is sensitivity (i.e. high false negative rate) is performedperformed

10
Importance of Diagnosing Adrenal Importance of Diagnosing Adrenal InsufficiencyInsufficiency
Identifying patients with adrenal insufficiency, Identifying patients with adrenal insufficiency, even if mild, is important because:even if mild, is important because:
• life-threatening hypotension may occur during periods of stress (e.g. illness, trauma, surgery)
• the condition is totally preventable if supplemental glucocorticoids are administered

11
Diagnosis of Glucocorticoid-Induced: Diagnosis of Glucocorticoid-Induced: Secondary Adrenal InsufficiencySecondary Adrenal Insufficiency
• Basal hormonal testsBasal hormonal tests
• Dynamic testing:Dynamic testing: – tests of adrenocortical integrity (adrenal
gland integrity only)– tests of HPA axis integrity (hypothalamic,
pituitary and adrenal integrity)

12
Basal Hormonal TestsBasal Hormonal Tests
• Plasma cortisol (single or multiple):Plasma cortisol (single or multiple):– low sensitivity, thus, often non-diagnostic:
endogenous levels variable due to pulsatile secretion
• 24 hour urinary free cortisol:24 hour urinary free cortisol:– often non-diagnostic: lack of sensitivity at low levels,
i.e. low cortisol excretion may be normal
– errors in 24 hour urine collections

13
Basal vs. Dynamic TestsBasal vs. Dynamic Tests
• Since basal plasma and 24h cortisol levels are often non-diagnostic, it is necessary to perform dynamic testing to diagnose adrenal insufficiency.
• Advantage of dynamic testing: provide information regarding the function, reserve capacity and, hence, the ability of the adrenal gland or of the entire HPA axis to respond to stress.

14
Dynamic TestsDynamic Tests
• Dynamic tests of adrenocortical integrity (assesses Dynamic tests of adrenocortical integrity (assesses only adrenal gland responsiveness):only adrenal gland responsiveness):– Cosyntropin (ACTH) stimulation test:
• high-dose ACTH
• low-dose ACTH
• Dynamic tests of HPA axis integrity (assesses the Dynamic tests of HPA axis integrity (assesses the responsiveness of the hypothalamus, pituitary and responsiveness of the hypothalamus, pituitary and adrenal glands):adrenal glands):– ITT
– Corticotropin-releasing hormone test (CRH)
15
Hypothalamus: CRH
Adrenal: Cortisol
Pituitary: ACTH
16
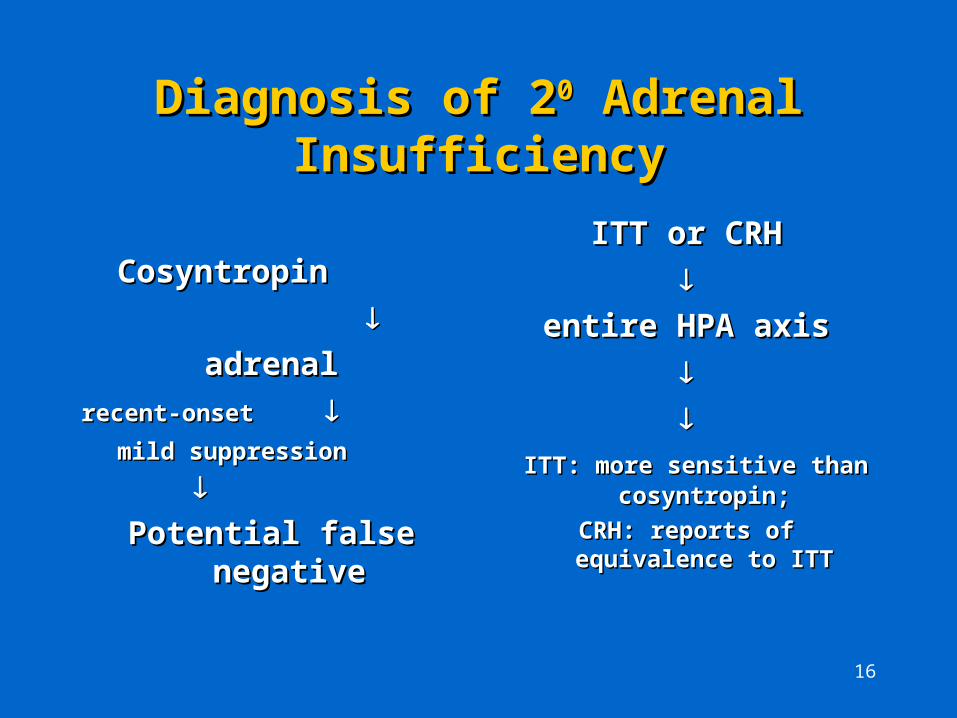
Diagnosis of 2Diagnosis of 200 Adrenal Insufficiency Adrenal Insufficiency
CosyntropinCosyntropin
adrenaladrenal
recent-onset recent-onset mild suppressionmild suppression
Potential false negativePotential false negative
ITT or CRHITT or CRH
entire HPA axisentire HPA axis
ITT: more sensitive than ITT: more sensitive than cosyntropin;cosyntropin;
CRH: reports of equivalence to ITTCRH: reports of equivalence to ITT
17
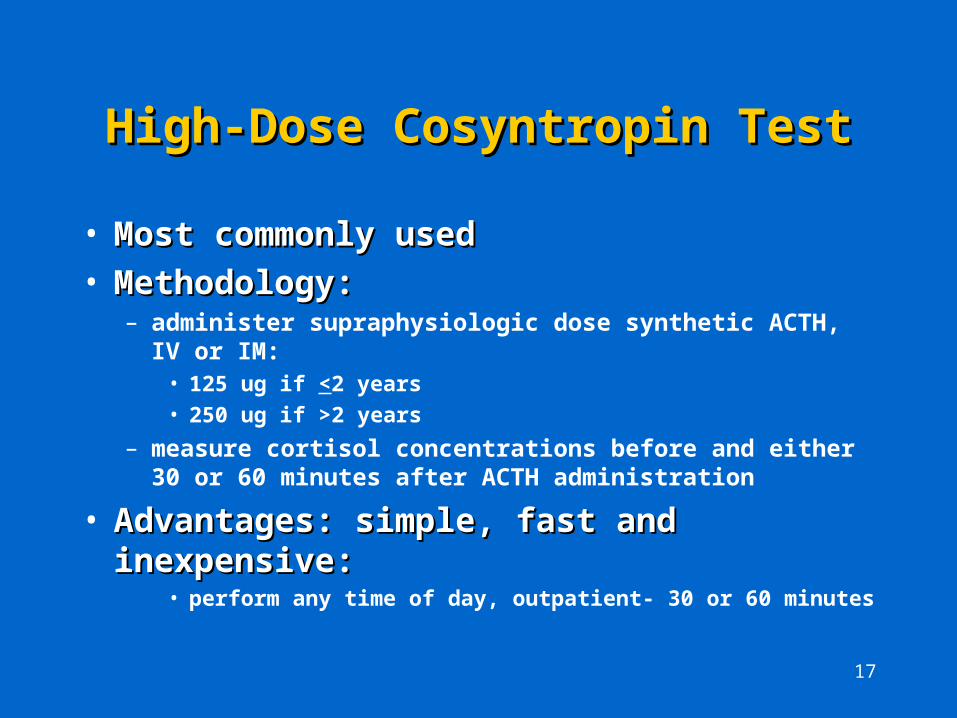
High-Dose Cosyntropin TestHigh-Dose Cosyntropin Test
• Most commonly usedMost commonly used• Methodology:Methodology:
– administer supraphysiologic dose synthetic ACTH, IV or IM:• 125 ug if <2 years
• 250 ug if >2 years
– measure cortisol concentrations before and either 30 or 60 minutes after ACTH administration
• Advantages: simple, fast and inexpensive:Advantages: simple, fast and inexpensive:• perform any time of day, outpatient- 30 or 60 minutes

18
High-Dose Cosyntropin TestHigh-Dose Cosyntropin Test
• Controversy regarding normal cortisol response:Controversy regarding normal cortisol response:
• criteria in cosyntropin label (30 minute test):– basal cortisol >5 ug/dl, increment > 7ug/dl, peak >18 ug/dl
– low basal cortisol level does not suffice to make the diagnosis
– since the test can be performed at any time during the day and only the peak plasma cortisol remains unchanged during the day, this single criterion should be used for the 30’ test.
• since basal cortisol levels vary throughout the day and the higher the basal level, the lower the incremental cortisol rise, consensus regarding a normal response appears to be a peak cortisol level >18ug/dl at 30 minutes.
19
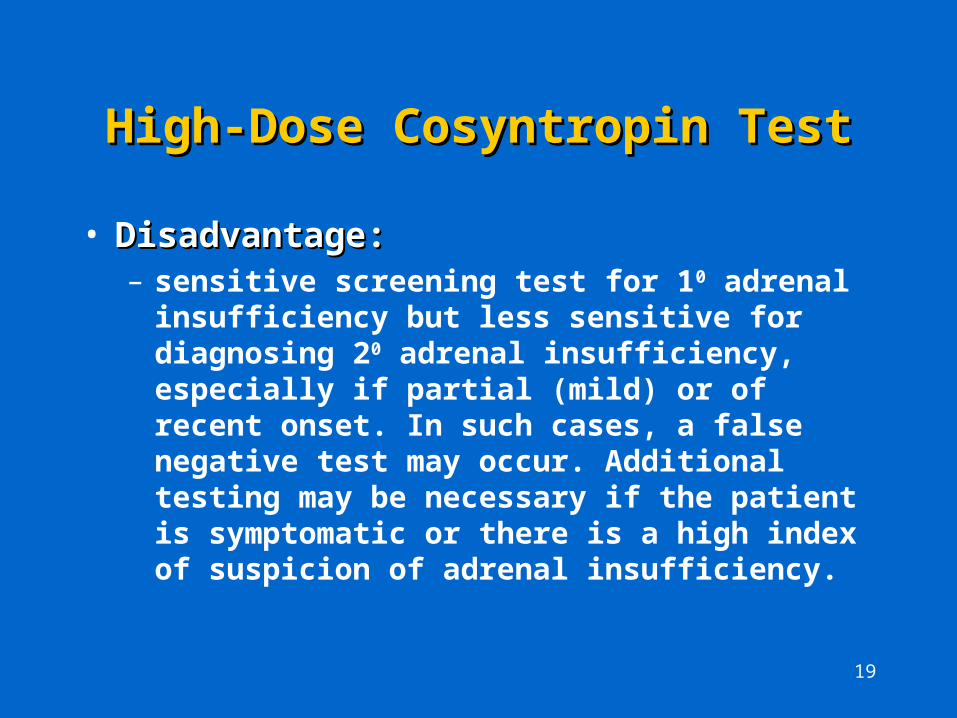
High-Dose Cosyntropin TestHigh-Dose Cosyntropin Test
• Disadvantage:Disadvantage:– sensitive screening test for 10 adrenal insufficiency
but less sensitive for diagnosing 20 adrenal insufficiency, especially if partial (mild) or of recent onset. In such cases, a false negative test may occur. Additional testing may be necessary if the patient is symptomatic or there is a high index of suspicion of adrenal insufficiency.

20
Low-Dose Cosyntropin TestLow-Dose Cosyntropin Test
• Newer testNewer test • Method not standardized regarding dose or timing of Method not standardized regarding dose or timing of
samplessamples:
– administer a physiologic ACTH dose intravenously
– measure cortisol before and serially post-ACTH
• Other issues:Other issues:– physiologic ACTH dosing may be more sensitive than
supraphysiologic dosing for mild or recent-onset secondary AI
– dose not commercially available (dilutional errors, variability in dose administered among tests, binding to plastic tubing)

21
Low-Dose vs. High-Dose TestLow-Dose vs. High-Dose Test
Low-DoseLow-Dose• dose not available
• physiologic ACTH dose
• frequent, carefully timed venous sampling
• no consensus on method of performance
• no consensus regarding normal response criteria: lower limit cortisol cut-off
High-Dose High-Dose (Standard Dose)(Standard Dose)
• dose commercially available
• supraphysiologic ACTH dose
• single cortisol level post-ACTH, no precise timing
• method of performance has been standardized
• peak cortisol >18ug/dl at 30 minutes is generally accepted as a normal response.
22
Insulin Tolerance Test (ITT)Insulin Tolerance Test (ITT)
• Hypoglycemia: potent stress stimulus for ACTH Hypoglycemia: potent stress stimulus for ACTH releaserelease
• Methodology:Methodology:– intravenous insulin 0.05 U/kg after an overnight fast
– plasma cortisol and glucose levels before and at 30, 45, 60 and 90 minutes
• Criteria for normal response:Criteria for normal response:– with serum glucose <40 mg/dl, plasma cortisol should
rise to >18-20 ug/dl at 60 to 90 minutes post-insulin.
23
Insulin Tolerance Test (ITT)Insulin Tolerance Test (ITT)
• Advantages:Advantages:– direct and definitive assessment of HPA axis
• Disadvantages:Disadvantages:– requires intensive in-patient physician monitoring
– risk of morbidity (seizures, neurological impairment) and mortality from hypoglycemia. Therefore, rarely, if ever, used. Safer alternatives are available.

24
Corticotropin-Releasing Hormone Corticotropin-Releasing Hormone (CRH) Test(CRH) Test
• Newer testNewer test
• CRH stimulates release of ACTH and, hence, cortisolCRH stimulates release of ACTH and, hence, cortisol
• 1100 (adrenal) vs. 2 (adrenal) vs. 200 (pituitary) vs. 3 (pituitary) vs. 300 (hypothalamic): (hypothalamic):– 10: basal ACTH is high and with ACTH but not cortisol;
– 20: basal ACTH is low and does not respond to ACTH;
– 30: basal ACTH is low and shows an exaggerated response to ACTH
• Methodology:Methodology:– administer CRH 1 ug/kg intravenously
– measure plasma ACTH and cortisol levels periodically for 90 to 180 minutes post-CRH.
25
Advantages of the CRH TestAdvantages of the CRH Test
• Direct and definitive assessment of HPA axis Direct and definitive assessment of HPA axis integrity.integrity.
• The CRH test may have equivalent diagnostic The CRH test may have equivalent diagnostic value to the ITT.value to the ITT.
• Safe for outpatient useSafe for outpatient use
26
Disadvantages of CRH TestDisadvantages of CRH Test
• ExpensiveExpensive
• Requires multiple blood samplesRequires multiple blood samples
• Errors in blood collection and storage may occur.Errors in blood collection and storage may occur.
• Normal responses of ACTH and cortisol are Normal responses of ACTH and cortisol are laboratory-dependent.laboratory-dependent.
• No consensus regarding criteria for a normal response.No consensus regarding criteria for a normal response.
• Not an FDA approved indication as a diagnostic for AI.Not an FDA approved indication as a diagnostic for AI.
• Additional studies are needed to confirm its usefulness Additional studies are needed to confirm its usefulness as a diagnostic test for adrenal insufficiency.as a diagnostic test for adrenal insufficiency.

27
Risk Factors For HPA Axis Risk Factors For HPA Axis Suppression with Topically Suppression with Topically
Administered CorticosteriodsAdministered CorticosteriodsVariable individual susceptibility and time to recovery.Variable individual susceptibility and time to recovery.
Risk Factors:Risk Factors:
• steroid properties:steroid properties:– potency
– half-life
• vehiclevehicle (e.g. cream, lotion, ointment)
28
Risk Factors For HPA Axis Risk Factors For HPA Axis Suppression with Topically Suppression with Topically
Administered CorticosteriodsAdministered Corticosteriods
• extent of absorption:extent of absorption:– increased:
• thin stratum corneum
• heat and moisture (enhanced by occlusion)
• abraded or inflamed skin
• dose:dose:– concentration
– body surface area exposed
– contact time
29
Risk Factors For HPA Axis Risk Factors For HPA Axis Suppression with Topically Suppression with Topically
Administered CorticosteriodsAdministered Corticosteriods
• cumulative dose:cumulative dose:– dosing interval
– duration of treatment
30
Summary 1Summary 1
• Topical corticosteroids are systemically absorbed, Topical corticosteroids are systemically absorbed, thereby secondary adrenal insufficiency may occur. thereby secondary adrenal insufficiency may occur.
• Symptoms of AI may be subtle and non-specific.Symptoms of AI may be subtle and non-specific.• Diagnosis may not be suspected clinically or Diagnosis may not be suspected clinically or
attribution is made to other causes.attribution is made to other causes.• Patients with secondary AI are at risk for an acute Patients with secondary AI are at risk for an acute
adrenal crisis, regardless of the degree of suppression adrenal crisis, regardless of the degree of suppression or the presence of symptoms.or the presence of symptoms.
• Acute adrenal crisis is preventable if supplemental Acute adrenal crisis is preventable if supplemental glucocorticoids are administered before or early in glucocorticoids are administered before or early in the course of stress.the course of stress.

31
Summary 2Summary 2
• Although risk factors for HPA axis suppression may Although risk factors for HPA axis suppression may be present, individual susceptibility is variable.be present, individual susceptibility is variable.
• Hormonal testing is required for diagnosis.Hormonal testing is required for diagnosis.
• Basal hormonal tests are often non-diagnostic.Basal hormonal tests are often non-diagnostic.
• Dynamic hormonal testing is generally required.Dynamic hormonal testing is generally required.
• Dynamic tests of HPA axis integrity are more Dynamic tests of HPA axis integrity are more sensitive for the diagnosis of mild or recent-onset sensitive for the diagnosis of mild or recent-onset secondary AI than tests which measure only secondary AI than tests which measure only adrenocortical reserve.adrenocortical reserve.
32
Summary 3Summary 3
• A negative high-dose cosyntropin test may warrant A negative high-dose cosyntropin test may warrant additional testing particularly if the patient is additional testing particularly if the patient is symptomatic or if there is a high index of clinical symptomatic or if there is a high index of clinical suspicion of secondary adrenal insufficiency.suspicion of secondary adrenal insufficiency.
• When HPA axis suppression is diagnosed, treatment When HPA axis suppression is diagnosed, treatment should follow standard medical practice.should follow standard medical practice.
• Patients should be followed to document full recovery Patients should be followed to document full recovery of the HPA axis.of the HPA axis.