با سلام بسم الله الرحمن الرحیم. by asadollah asadian md tuberculous pleural...
TRANSCRIPT
سالم با
بسم الله الرحمن الرحیم
BY ASADOLLAH ASADIAN MD
Tuberculous Pleural Effusion



EpidemiologyPleural TB is second most common extrapulmonary TB site behind lymph node involvement

PathogenesisTB Pleural effusion can be seen in either
primary disease or reactivation diseaseEffusion a result of the rupture of a subpleural
foci of TB into the pleural space that leads to a delayed hypersensitivity reaction to the TB antigens
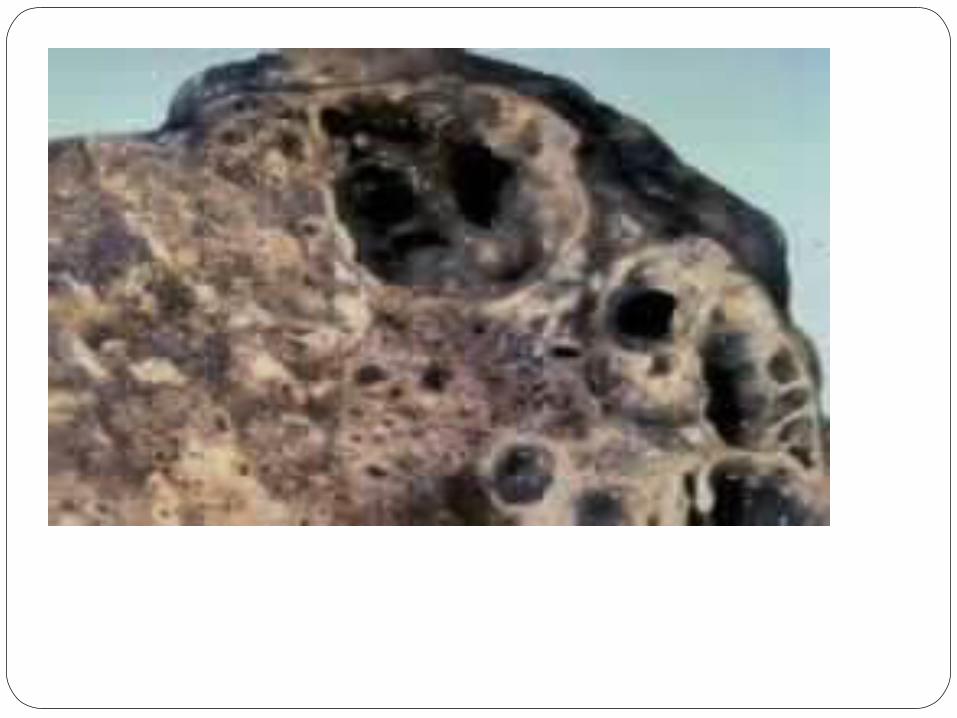
Tuberculous empyema – same mechanism as above with spillage of large amount of mycobacterium into pleural space purulent effusion that requires surgical intervention and can result in pleural fibrosis and restrictive lung disease

Clinical Presentationusually presents as an acute illness (1 wk –
1 mo symptoms)presenting symptoms: pleuritic chest pain
and nonproductive coughcommon to have other symptoms of TB –
night sweats, weight loss, dyspneaphysical exam consistent with pleural
effusion – decreased breath sounds, dullness to percussion at site of disease

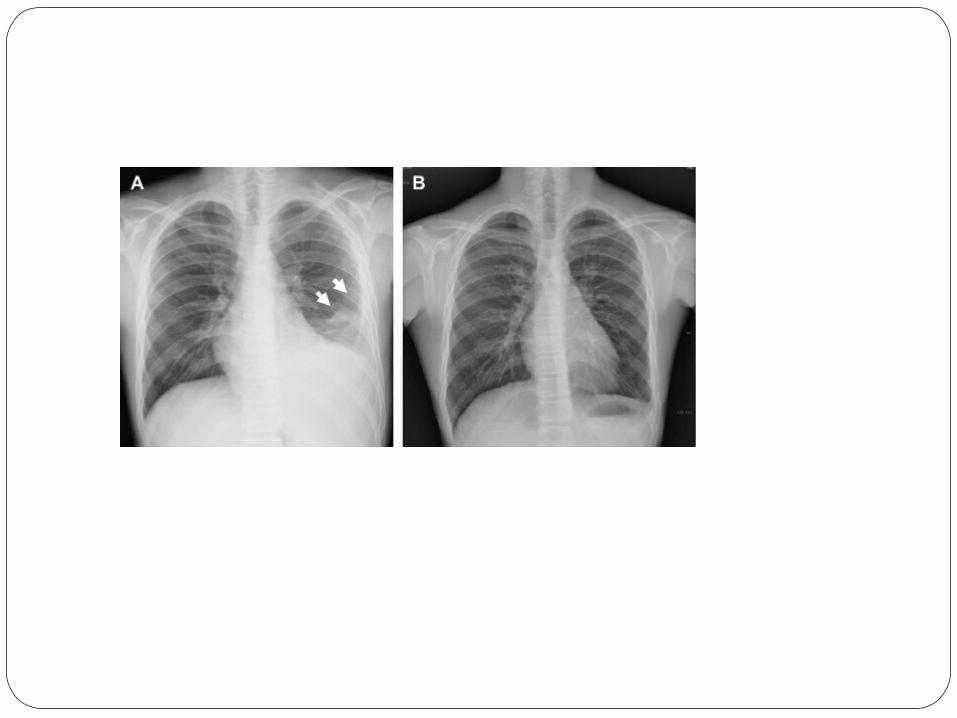
paraclinical PresentationCXR – small to moderate sized unilateral
pleural effusionPleural Fluid
-Straw colored appearance-exudative-pH 7.3 – 7.4-glucose usually > 60-Cell count usually 1000 – 6000 with
lymphocytic predominance

paraclinical PresentationCXR – small to moderate sized unilateral
pleural effusionPleural Fluid
-Straw colored appearance-exudative-pH 7.3 – 7.4-glucose usually > 60-Cell count usually 1000 – 6000 with
lymphocytic predominance



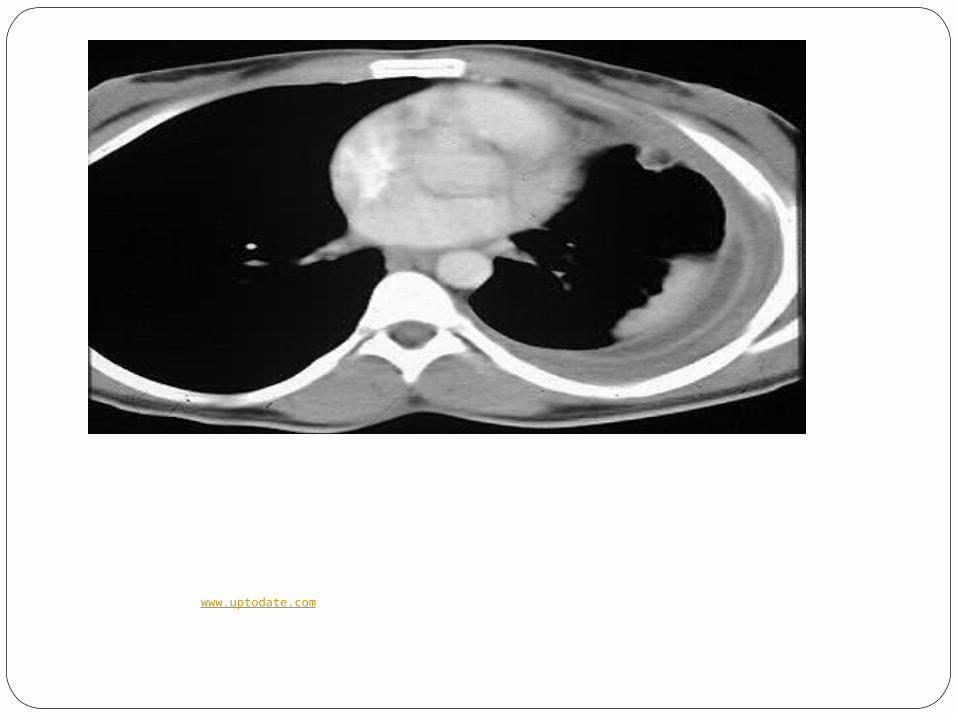
CT scan showing a parenchymal focus of tuberculosis close to the pleura and an ipsilateral pleural
effusion. Courtesy of Paul Stark, MD.www.uptodate.com 2008

Figure 1a. Patient 6.
Choi Y W et al. Radiology 2002;224:493-502
©2002 by Radiological Society of North America

Figure 1a. Patient 6.
Choi Y W et al. Radiology 2002;224:493-502
©2002 by Radiological Society of North America



DiagnosisTB skin test
-helpful if +, especially in areas of low prevalence of disease
-oftentimes negative but if repeated 6-8 weeks later usually +
Radiology-CXR with small – moderate sized unilateral effusion and
associated parenchymal lung lesions in 20-50% -CT scan better at documenting parenchymal lung
disease (80% of cases). Also better at delineating TB pleural effusion complications such as pleural thickening, calcification, loculated effusions, empyema, empyema necessitatis, and bronchopleural fistula




Differential DiagnosisLymphocytic Effusion
TBMalignancyLymphomaCollagen vascular diseasePost coronary artery bypass grafting






DiagnosisTB skin test
-helpful if +, especially in areas of low prevalence of disease
-oftentimes negative but if repeated 6-8 weeks later usually +
Radiology-CXR with small – moderate sized unilateral effusion and
associated parenchymal lung lesions in 20-50% -CT scan better at documenting parenchymal lung
disease (80% of cases). Also better at delineating TB pleural effusion complications such as pleural thickening, calcification, loculated effusions, empyema, empyema necessitatis, and bronchopleural fistula
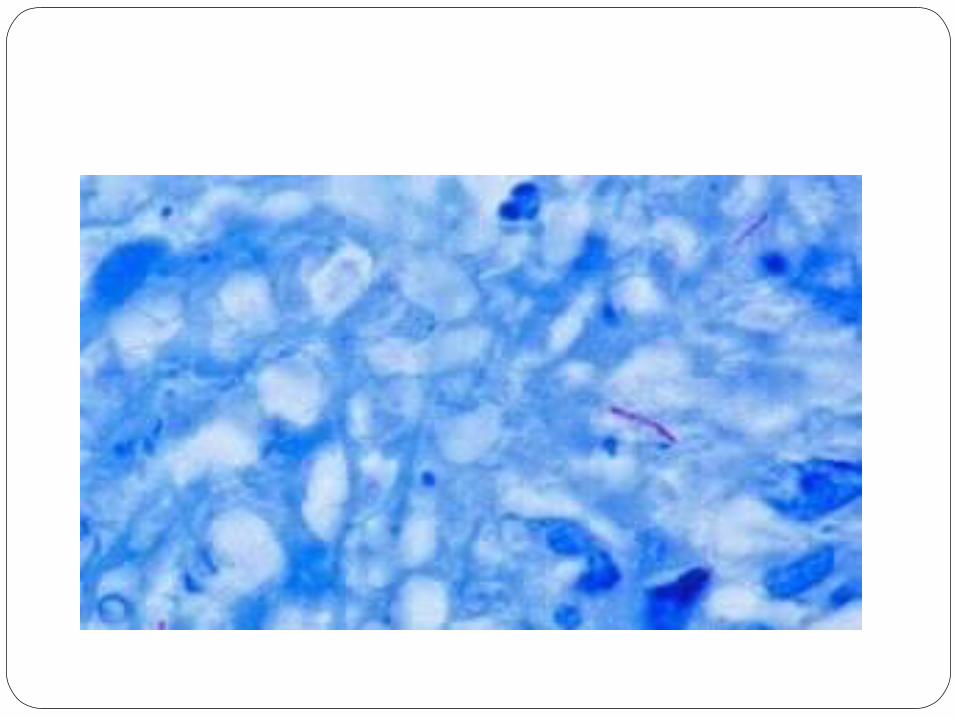
DiagnosisSputum
-can have + M Tuberculosis cultures 20-50% time
-increased yield on sputum cultures with parenchymal lung lesions on radiographs
-should still be pursued in areas where other means of diagnosis not available
Diagnosis – Pleural FluidMicrobiology
Adenosine Deaminase (ADA)
enzyme in purine salvage pathway that is important in differentiation of lymphoid cells and has increased activity with increased lymphocyte activity
high sensitivity (90-100%)cutoff is 40: >40 supportive of TB, <40 virtually
excludes TBInterferon gamma
produced by t-lymphocytes to activate macrophagesincreased in TB pleural effusion due to increased
numbers of T-lymphocytes presentmore sensitive and specific vs. ADA, but more
expensive and less available so not used as much
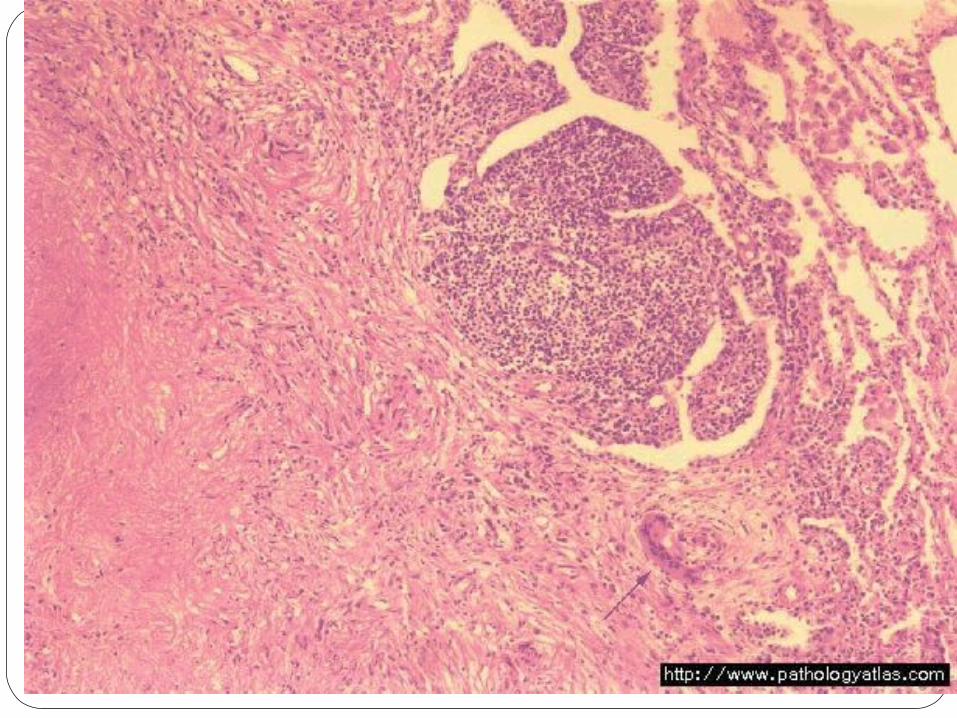
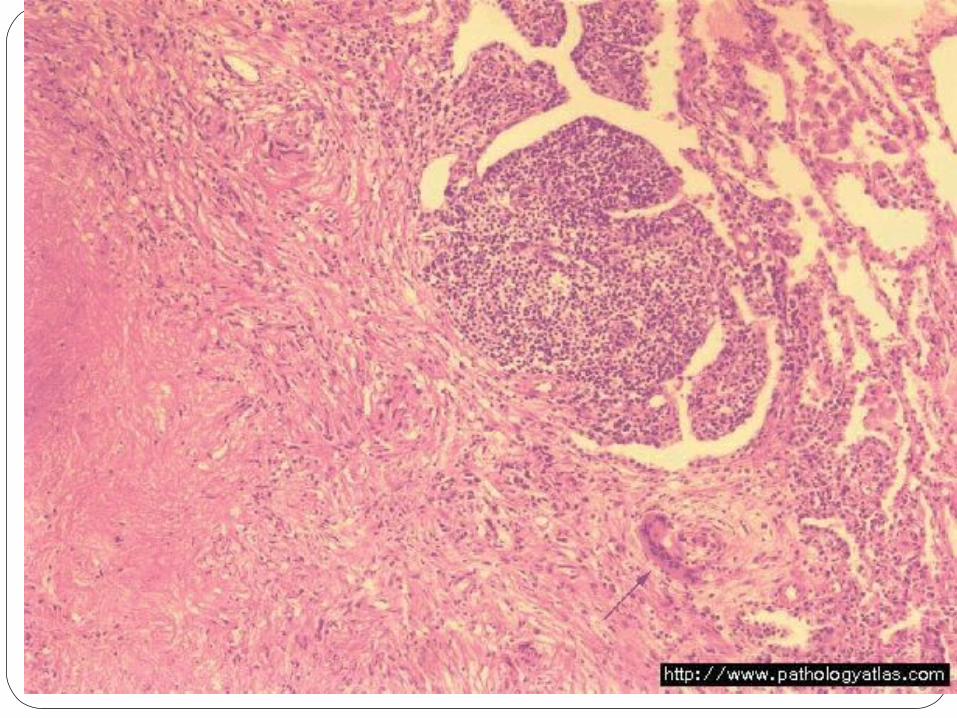
DiagnosisPleural Biopsy
most sensitive testtissue via closed needle biopsy or
thoracoscopyHistology: caseating granulomas (50-97%)Culture for M Tuberculosis + in 40-80%Combo of above two leads to diagnosis in 60
– 95% cases
Goal of treament
(I ) e thsubseqto prevent uent development of active TB (2 ) to relieve the symptoms of the patient, (3) to prevent the development of a fibrothorax.

Treatment If left untreated, effusions usually resolve in 4-16
weeks and are followed by development of active pulmonary TB or extrapulmonary TB in 43-65% cases
Antimicrobial therapy is the same as for pulmonary TB 4 drug therapy for 2 months with isoniazid, rifampin,
pyrazinamide, and ethambutol followed by 4 mo of isoniazid and rifampin
Steroids have been studied in TB pleural effusion with no definite benefit. Studies did note earlier resolution of symptoms (fever,
chest pain, dyspnea) in patients treated with steroids, but no difference in the development of pleural thickening, adhesions, or residual lung function.
rereeeqrrrrrrrrr