ι · 2017-04-06 · fig. 4. irregular fold thickening in a patient with iymphoma. the thickness of...
TRANSCRIPT

대 한 방사 선 의 학회 지 1994 ; 31(5) : 925 - 932
소장검사의 판독지침:점막변화를중심으로1
임 재 훈
서 론
소장은 신체의 가장 가운데 있고, 길이가 약 4m 가량되
며, 구불거리고, 움직이며, 바륨의 장내 통과도 사람마다
또는 검사마다 달라 예측하기도 어렵고, 따라서 만족할만
한 조영이 어렵다. 점막주름이 정상적으로도 제멋대로이
고, 조영된 소장도 서로 겹쳐, 작은 이상은 찾기도 어렵고
따라서 가음성이 많다.초음파검사, CT 와 MR 도그 이용
이 사실상어렵거나불가능하여 방사선과의사들의 관심이
적은 일종의 사각지대이다.
필자는 소장검사에서 점막변화를 계통적으로 분류하고
진단에 이르는 분석방법을 제시한다. 형태변화를 근거로
감별진단 대상 질병의 가지수를 줄이고 좁은 범주내에서
임상소견을 종합하면 훨씬 쉽고 정확하게 진단에 이를수
있으리라 본다. 여기서 다루는 소장검사는 바륨을 먹은후
a b
1삼성서울병원 진 단방사선과 이 논문은 1994년 8월 11 일 접수하여 1994년 9월 1 3일에 채택되었음
회맹부위에 이르는 동안 시간별로 촬영하고 소장의 여러
부위 를 압박하여 푸시 하는 “small bowel follow - through
examination " 을 중심으로 기술하며 small bowel entero
clysis 는 포함하지 않는다. 전형적인 점막변화를 표본을
비교하며 설명한 후 몇 예의 증예를 들어 판독연습을 하도
록구성하였다.
정상소장검사
소장에는 점막주름이 있고이것이 소장의 연동운동에 따
라제멋대로 배열되므로 정상 소장검사에서 점막주름은꼬
불꼬불한 모양(criss-<:ross pattern)을 취한다 (Fig. 1). 소
장의 내경은 대략 2.5 cm 이고점막주름은그두께가 2mm
미만이다.
점막변화
소장병변에서는 필연적으로 점막이 두꺼워지고, 점막
‘ Fig . 1. a. Internal surface of the normal
proximal jejunum . Note the mucosal folds
with smooth , gentle curve , forming
criss-cross pattern. The thi ckness of the
fo1ds is less than 2 mm
b. Normal jejunum on follow-through
sma11 bowel examination showing criss
cross pattern of mucosal folds. There is
lack of parallelism of mucosal folds
… ι

대한방사선의 학회 지 1994 : 31 ( 5) : 925 - 932
Table 1. Classification of Mucosal change
Reg띠와 P와IJJ과k 빽
Lilidre~
Mucosal change
Heart failure
Re꽤sp빼cke띠명
Hm4h행 &없뼈、we떠Je리Jl]싫1 Coagulopathy
gastoenteritís Crohn’s disease
Tumor Lymphoma
Renal failure H쩌Iy’poalbumínemia
Vasculítis Thrombocytopeníc purpura
Proteín losíng enteropathy Henoch-Schonleín purpura Mesenteric chokíng Trauma
Radíation enteritis
Fig. 2 . Regular smooth thick ening due to mesenteric “ chok
Ing caused by retroperitoneal and mesenteric Iymph node
metastasis Irom pancreatic cancer. The thickness 01 the lolds
is approximately the same in width (2-3mm) , aligned parallel
to one another (instead 01 criss-c ross pattern ), and perpen
dicular to the bowel lumen. Note the normal serrated margin
wi th r ound “ incisor teeth"
꽤i 뼈e 싫。ma Eosínophilic Crohn’s dísease Lymphoma
Behcet dísease Leiomyosarcoma (Nodular lymphoid hyperplasia)
Fig . 3 . Reg비 ar spiky thickenin g due to submucosal hemo
rrhage in a patient wi th bl eed in g diathesis. The thickness 01
th e lolds is sli ghtly wider (3-4mm) than regu lar smooth
thickening. Thi ckness 01 the lolds are lairly th e same, aligned
parallel , an d perpendicular to the bowel lum en, producing
‘picket lence appearance" Note the se rrated margin wi th
sharp spiky “canine teeth"
α μ
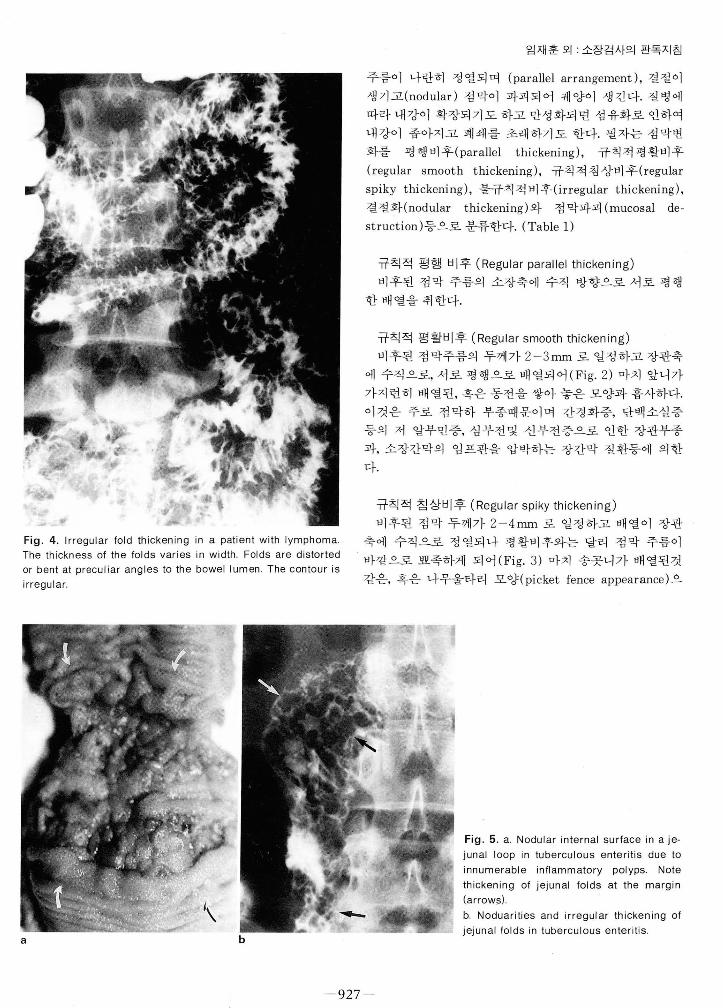
Fig. 4. Irregular fold thicken ing in a patient with Iymphoma. The thickness of the folds varies in width. Folds are distorted 。 r bent at preculiar angles to the bowel lumen. The contour is
irregular
임재훈 외 소장검사의 판독지침
주름이 나란히 정열되며 (parallel arrangement) , 결절이
생기고(nodular) 점막이 파괴되어 궤양이 생긴다. 질병에
따라내강이 확장되기도하고만성화되면 섬유화로인하여
내강이 좁아지고 폐쇄를 초래하기도 한다. 필자는 점막변
화를 평행비후(parallel thickening) , 규칙적평활비후
(regular smooth thickening) , 규칙적침상비후(regular
spiky thickening) , 불규칙적비후(irregular thickening) ,
결절화(nodular thickening)와 점막파괴 (mucosal de
struction)등으로 분류한다. (Table 1)
규칙적 평행 비후 (Regular parallel thickening)
비후된 점막 주름의 소장축에 수직 방향으로 서로 평행
한배열을취한다.
규칙적 평활비후 (Regular smooth thickening)
비후된 점막주름의 두께가 2-3mm 로 일정하고 장관축
에 수직으로, 서로 평행으로 배열되어 (Fig.2) 마치 앞니가
가지런히 배열된, 혹은 동전을 쌓아 놓은 모양과 흡사하다.
이것은 주로 점막하 부종때문이며 간경화증, 단백소설증
등의 저 알부민증, 심부전및 신부전증으로 인한 장관부종
과, 소장간막의 임프관을 압박하는 창간막 질환등에 의한
다.
규칙적 침상비후 (Regular spiky thickening)
비후된 점막 두께가 2-4mm 로 일정하고 배열이 장관
축에 수직으로 정열되나 평활비후와는 달리 점막 주름이
바깜으로 뾰족하게 되어 (Fig. 3) 마치 송곳니가 배열된것
같은, 흑은 나무울타리 모양(picket fence appearance)으
a
Fig. 5. a. Nodular internal surface in a je
junal loop in tuberculous enteritis due t。
innumerable inflammatory p이 yps. Note
thickening of jejunal folds at the margin (arrows)
b. Noduarities and irregular thickening of
jejunal folds in tuberculous enteritis
g

대 한 방사선 의 학회 지 1994; 31 ( 5) : 925- 932
로 보인다. 대개 점막하 출혈에 의한다고 생각되며 이런 모
양을 초래하는 질환으로는 창간막혈관허혈증, 혈관염, 특
발성 혈소판감소성 자반증, H enoch-Schonlein purpura,
혈액응고장애, 장관외상과 방사선 장염등 장관출혈을 초래
하는질환이 있다.
불규칙 비후 (Irregu lar thickening)
비후된 점막의 두께가 일정치 않고 방향이 서로 평 행이
아니고장관축 방향에 수직으로배열되지 않고제멋대로이
며 급격히 구부러 지거나(bent) 없어진다 (Fig. 4). 이러한
6 7
a b
d e
점막비후는점막하 조직에 염증세포나암세포의 침윤에 의
하며 호산구성장염 (eosinophili c gast r oenteri t i s ) , Crohn
병이나 럼프종에서 나타난다.
결절성 비후 (Nod비 ar thickening)
점막비후의 모양이 불규칙하고 점막주름이 평행으로 정
열되지 않고 제멋대로이며 특히 결절의 형 태를 취하는 경
우로(Fig. 5 ) 주로 장결핵, Crohn 병, Behect 병 , Yersinia
장염등의 염증성 질환과럼프종등의 종양에서 이러한모양
이 나타난다.
c
Fig. 6 . Gross appearance of mucosal de
struction in jejunal Iymphoma. Note total
lack of jejunal folds (arrowheads) within
the internal surface of the tumor. The
margin of the tumor is sharp (curved ar
rows)
Fig.7 ‘ Total destruction of mucosal lolds
in jejunal leiomyosarcoma. Note irregular
margin without criss-cross normal jejunal
lolds. Also noted are irregular thic- kened
101 ds (arrows)
Fig. 8 . Diagramatic representation 01
various types of mucosal change
a. Regular smooth thickening
b. Regular spiky thickening
c. Irregular thickening
d. Nodular thickening. 81ack area rep
resents 1 inear ulcer
e. Mucosal destruction (black area) ass
oci ated with irregular and nodular thick
enlng
- 928 -

점 막파괴 (Destroyed mucosa)
정막이 염증세포나 암세포로 침윤되어 두꺼워지고 파괴
되어 궤양이 생기기도하여 정상점막주름이 소실되어 바륨
조영상 모양이 불규칙하고 제멋대로 취하게 된다(Fig.6).
점막비후, 결절, 종괴등과 함께 불규칙한 모양의 궤양을 형
성하며 궤양이 장벽 밖으로도 형성되어 대단히 큰 궈l 양/
공동을 형성한다(Fig. 7). 이러한 병변을 초래하는 경우는
영증성질환 중에서는 특히 Crohn 병이나 Behcet 병이 있
고, 대부분 종양질환, 즉 선암, 럼프종과 평활근종/평활근
육종등이 있다.
소장의 점막변화를 이와같이 5가지로 분류할 수 있고,
전형적인 경우의 모식도를 Fig. 8에 제시한다. 이러한 점막
비후의 양상은 확실히 구별되기도 하지만 때로는 어느 양
감사의 말:자료수집 에 협조하여 주신 경희대학병원 진단
방사선과의국원 일동에게 감사를드린다.
임재훈 외 · 소장검사의 판독지침
상인지 구별이 안되는 경우도 있으며 병이 심하거나 약함
에 따라서 같은 질환이 서로 다른 형태로 보이기도 한다.
따라서 소장의 질환을 점막 변화와 함께 임상소견이나 검
사소견, 또는 다른 방사선 검사 결과를 참고하여 진단하면
보다 정확한진단에 이를수있다.
*~ C그 고 C그
Lr 헌
1. Goldberg H 1. Sheft DJ. Abnormalities in small intesteine contour and caliber. A working classification. Radiol Clin North
Am 1976 ‘ 14 ; 46-475 2. Li shtenstein JE. Aspects of radiologic-pathologic correlation
In : Herlinger H, Maglinte DDT eds. Clinical radiology of the
small intestine ‘ Philadelphia : Saunders, 1989: 54-571 3. Herlinger H, Maglinte DDT, Rubensin SE. Small bowel imaging
- an overview of indications and a practical approach to the
interpretation of abnormalities. In : Herlinger H, Maglinte DDT eds. Clinical radiology of the small intestine .. Philadelphia Saunders , 1989: 573-592
Journal of the Korean Radiological Society, 1994; 31 (5) : 925- 932
Abnormalities of Mucosal Folds of the Small Intestine: a Guide in Interpretation of Small Bowel Series'
Jae Hoon Li m , M :D .
l Department o( Diagnostic Imaging Samsung Medical Center
Normal small intestinal folds are less than 2mm in thickness and criss-cross in appearance. Many diseases
of the small interstine produce an abnormality in mucosal folds, namely thickening and parallel (perpendiulcer
to the bowel lumen) arrangement of folds , nOdularity, destruction , and ulcer. Diseases causing submucosal
edema produce regular smooth thickening whereas diseases producing submucosal hemorrhage produce reg
비 ar spiky thickening. Inflammatory bowel diseases and Iymphoma produce irregular (in width , or distorted or
bent at peculiar angles to the bowel lumen) thickening nodularity of the mucosa. Severe inflammatory
processes as well as malignant tumors produce mucosal destruction and ulcer. Proposed here is an approach
to narrow the category of disease processes based on mucosal fold abnormality. This approach with sufficient
clinical history is invaluable in the interpretation of small bowel series
Address reprint requests to : Jae Hoon Lim, M.D. Department of Di agnostic l maging Samsung Medical Center Tel. 82-2-3410-2501 Fax. 82-2-3410-2529, 255
- 929 -

대한방사선의학회지 1994 ; 31 (5) ; 925 - 932
I 소장검 사의 판독연습 : 문제
Fig.9.
Fig.11 .
Fig . 10.
Case 1 . A 23-year-old woman presented with intermittant lower gastrointerstinal bleeding and fainting. These symptoms started 2 years before and waxed and waned thereafter. She looked pale. Serum hemoglobin level was 2.6g %. A small bowel sereis (Fig. 9, a spot film of the left lower abdomen) was done.
Case 2. A 33-year-old man admitted because of diffuse abdominal pain accompanied by diarrhea and melena for 15 days. Physical examination disclosed nosignificant abnormality. Laboratory findings were elevated leucocyte count in peripheral blood , 74, OOO/m미, with differential count being neutrophil , 64 % and Iymphocyte 36 %. Chest radiograph showed infiltration in the left upper lung field suggesting active p비 monary tuberculosis. A small bowel follow-through examination (Fig. 1 이 disclosed subtle mucosal abnormal ity
'Case 3. A 41-year-old woman presented with abdominal pain of sudden onset. She had a history of similar attack 6 months before. Physical examination disclosed diffuse abdominal tenderness. A small bowel series was performed (Fig. 11 )
- 930

Fig . 12.
Fig . 13.
임재훈 외 소장검사의 판독지침
Case 4. A 32-year-old woman admitted because of general weakness. Physical examination revealed diffuse mass feeling in the upper abdomen. A small bowel series (Fig. 12)was performed.
Case 5. A 24-year-old woman presented with diffuse abdominal pain. Physical examination disclosed no specific abnormality. A small bowel series (Fig. 13) was
performed
- 93 1 -

대 한 방사선 의 학회 지 1994 ; 31 (5) : 925- 932
Fig.14.
Fig.15.
Case 6. A 64-year-old man admitted with discomfort in the upper left part of the abdomen. Physical examination disclosed no gross abnormality. Ultrasound and CT examination disclosed a large mass in the upper left part of abdomen. A small bowel examination (Fig 14) was performed to evaluate the bowel loops.
Case 7. A 66-year-old woman complained of tarry stool and severe abdominal pain of sudden onset. A small bowel series (Fig. 15) was pertormed.
< 해 답은 965, 966 page를 보세 요 >
요
Q J