youth high-risk behaviors: survey and results
TRANSCRIPT

Youth High-Risk Behaviors: Survey and Results
Patricia Stevens Juree Grifin
Youth seem to be engaging in increasingly severe risk behaviors. Understanding the connections between these behaviors and other factors may assist in de- veloping appropriate intervention/prevention programs. This article presents results from the Centers for Disease Conhpl and Prevention’s Youth Risk Behavior Survey. Results indicate a critical age for involvement in risk behaviors, gradual increase in risk behaviors over time, and gender differences in risk behaviors.
Both research and media reports over the past two decades indicate a significant change in the behavior of America’s young people. Studies have researched how this behavior has changed, what has influenced this behavior change, and how to prevent or remedy the negative results of these changes. Statistics show that young people more frequently engage in behaviors that are dangerous to their health and safety (Centers for Disease Control and Prevention [CDC], 1996a; Dinwiddie, 1994; Kann et al., 1993; Marcus, Giovino, Pierce, & Harel, 1993; Morris, Warren, & Aral, 1993; O’Carroll, Harel, & Waxweiler, 1993) Specifically, there has been a dramatic increase in the number of youth who are using mind-altering substances, who are involved in violence, and who are sexually active (Beauvais, Chavez, Oetting, Deffenbacher, & Cornell, 1996; Brownfield & Sorenson, 1991; CDC, 1996b).
The Youth Risk Behavior Survey (YRBS), an instrument developed by the CDC (1996b) to track risk behaviors in youth in Grades 7 through 12, indicates that nationwide one fifth of all students surveyed in these grades had taken a weapon to school, that 38.7% of students had been in a physical fight in the 12 months preceding the survey, and that more than half (53.1%) of all students had engaged in sex at the time they were surveyed. Thirty-two percent of all students reported heavy drinking (at least five drinks on one occasion during the month preceding the survey). In addition, 80.4% of all students surveyed reported having had at least one drink in their lifetime. Seventy-one percent of the young people who were surveyed reported that they had tried cigarettes. Marijuana use was reported by 42.4% nationally, and 7.0% of the youth surveyed reported that they had used some form of cocaine during their lifetime. Finally, 24.1% of the students re- ported that they considered attempting suicide in the year preceding the survey.
Patricia Stevens is director of the Marriage and Family Training Program, and Juree Griffin i s a doctoral student in the School of Education, both at the University of Colorado at Denver. Corre- spondence regarding this article should be sent to Patricia Stevens, Counseling Psychology and Counselor Education, University of Colorado at Denver, PO Box 173364, Campus Box 106, Den- ver, CO 8021 7-23364 (e-mail: [email protected]).
Journal of Addictions 6 Oflender Counseling October 2001 Volume 22 31

Equally alarming is the age at which youth begin to engage in these risk behav- iors, Increasing numbers of children ages 9 through 12 experiment with chemical substances. The 1996 YRBS indicated that 32.4% of youth who reported having had at least one drink in their lifetime were under the age of 13. This survey also indicated that 7.6% of youth under age 13 had tried marijuana. Nine percent of youth under the age of 13 had become sexually active. These early behavior choices put young people at risk for poor outcomes in later life in many areas, including social development, habitual substance use, and underemployment.
Two substantial bodies of literature offer insight into what processes or factors exist that may affect individuals and their involvement in risk behaviors. One body of research focuses on risk factors, or deficit models, that have an impact on the likelihood of engag- ing in a particular behavior, whereas the second body of research focuses on the concept of resiliency.
A risk profile includes any factors in the individual or the environment that are predictive of a certain behavior or set of behaviors (Eitelbach-Stitcher, 1996). A risk factor can be defined as a condition that, if present, increases the likelihood of a person developing an emotional or behavioral problem. Risk factors include a variety of circumstances or situ- ations. Risk factors associated with youth violence, for example, include severe parental discord, maternal mental Illness, overcrowded housing, and limited parenting skills (Garmezy, 1985). Risk may also be defined by where a person lives. If the environment supports social and economic conditions that perpetuate high crime and poverty, then it may con- tribute to individuals’ being at risk (Huizinga, Loeber, & Thornberry, 1993).
Longitudinal research suggests that a young person can usually cope with two risk fac- tors simultaneously, but when three or more are present, the outcome almost always re- sults in some emotional or behavioral problems. The combination of familial and i@- vidual risk factors significantly increases the likelihood that a young person will engage in some risk behavior. The absence of a “buffer” between the individual and any number of stressors or temptations weakens a youth’s chance to withstand pressure and life stress (Benson, Galbraith, & Espeland, 1995; Masten & Coatsworth, 1998). A buffer can be described as some positive “hook” or “link” that separates or shields a child from certain people, experiences, and circumstances.
The philosophy of resilience, unlike risk, is to determine what contributes to a “success- ful’’ and “well-adjusted” child. Many researchers have conducted studies on resilience in the individual (Dugan & Coles, 1989; Garbarino, 1992; Luthar & Zigler, 1991; Masten, Best, & Garmezy, 1990; Rutter, 1985; Simeonsson, 1995; Werner, 1993; Wolin & Wolin, 1993). The focus of most literature about resiliency is on understanding what factors help individuals succeed and persevere despite great stress in their lives. Benson (1997) de- scribed these factors as developmental assets. These are the attributes of an individual and the environment that serve as protection between that person and stressful life situations.
Several key features can be seen in children who are resilient. Children who survive and prosper despite incredible stress are often described as confident, hopeful, or optimistic and as having a sense of personal control (Luthar, 1991; Seligman, 1995; Werner, 1993). Children and adolescents who are resilient also draw support from others. Positive, supportive, and sustained relationships are crucial for normal social and emotional development. These youth tend to form
32 Journal of Addictions 6 Offender Counseling October 2001 Volume 22

relationships with important adults in their social environments. It is this involve- ment in and maintenance of a supportive relationship with an adult that seems to significantly buffer children from stress (Garmezy, 199 1; Pianta & Walsh, 1996; Walsh, 1996; Werner, 1993). As early as 1979, Bronfenbrenner stated, “In order to develop normally, a child needs the enduring, irrational involvement of one or more adults in care of and joint activity with the child. In short, somebody has to be crazy about the kid” (p. 38). These individual qualities and the relationships that children have with adults are a psychosocial inoculation that boosts the har- diness and resistance with which children face life stresses (Walsh, 1996).
There is an important interaction between risk factors and protective factors. The mere presence or absence of either type of factor does not determine a child’s outcome. It is the interaction of factors, risk or protective, with stressful life events that strongly affects a young person (Rutter, 1993). Awareness of multiple risk factors, risk behaviors or protective factors, and positive personal and environmental supports can be used by practitioners to predict developmental and behavioral outcomes (Benson, 1997; Werner & Smith, 1992).
Surveying risk behavior in youth not only serves research interests for prediction, but it may also give clearer indications of the absence of individual and environmental protec- tive factors that are of interest to professionals who work directly with youth at risk. Gathering this type of information is essential for planning intervention and establishing systems of support for youth who engage in risk behaviors. As schools and communities become more cooperatively involved in shaping the social development of children, this information is essential in guiding interactions with youth in a purposeful manner.
This study explored several factors related to risk behaviors. We wanted to investigate the link between family factors (such as family composition, number of moves in past year, membership by a family member in a gang) and reports of participation in health risk behaviors. Furthermore, the goal of the study was to develop profiles for both a “high risk” and a “resilient” adolescent in this population to inform intervention efforts with detailed information about the onset and types of risk behaviors in which youth are en- gaged (Andrews, Hops, Ary, Tildesley, & Harris, 1993; Hawley & DeHaan, 1996).
We considered several questions as a means to this end. These questions included (a) What is the frequency of risk behavior in this middle school population? (b) Which of these behaviors (if any) are related to one another? (c) Are positive behaviors (such as involvement in sports or having a job) related to lower levels of risk behavior? and (d) Are family factors (such as frequency of worship, parental marital status, having an adult home after school, and household composition) related to lower levels of risk behaviors?
Method
This study used theYRBS, developed by the CDC (1996b). TheYRBS is administered nationally every 2 years to a random sampling of high school students to document risk behaviors reported by youth and teens. The YRBS also has a middle school survey that was used in its original form in this study. We added additional questions to the survey to determine the presence of a connection between family structure, environmental condition, and risk behavior. These domains have been shown to
Journal of Addictions b Offender Counseling 8 October 2001 Volume 22 33

be possible buffers to protect against risk behavior involvement (Garmezy, 1991; Pianta & Walsh, 1996; Walsh, 1996; Werner, 1993).
The YRBS has been found to be a reliable measure, with 71.7% of the items rated as having substantial or higher reliability (kappa = 61%-100%). Data from a test-retest reliability study indicated that students report risk behaviors reliably over time on this measure (Brener, Collins, Kann, Warren, & Williams, 1995).
Participants
The sample pool for this study included a stratified random selection of sixth-, seventh-, and eighth-grade classrooms from all middle schools in a large, urban school district in the western United States ( N = 674 students). Four science classes per school were selected. One classroom each of sixth and seventh graders was sampled per school. In addition, two eighth-grade science classes per school were targeted. Further sampling measures were taken before the survey was adminis- tered. Using the Lotus random number generating function, random numbers were assigned to all the classrooms in all the schools that were included in the study (sixth through eighth grades). For the sixth- and seventh-grade sample, this study targeted classrooms with the lowest random number. Because, for this study, two classes per school were needed for the eighth-grade sample, the eighth-grade classrooms in each school with the two lowest random numbers were included.
The total classroom sample size included 23 sixth-grade science classes, 23 seventh-grade science classes, and 46 eighth-grade science classes. A total of 236 sixth-grade, 205 seventh-grade, and 233 eighth-grade eligible surveys were col- lected for analysis. The number of students surveyed per school varied according to absenteeism on the day that the survey was administered and whether the du- dents had parental permission to participate. Because all middle schools across the district were included, the degree to which the sample is representative of the district population is congruent with the district’s population demographics.
Procedure
Prior to their participation in the survey, students were required to return a per- mission form signed by their parents. An alternative activity was developed for the students who did not participate in the survey on the appointed day. Each classroom participating in the survey was read a standard set of instructions. We paid the classroom teachers who administered the survey for their services. After completion, the surveys were collected and sealed in an envelope to ensure par- ticipants’ anonymity and confidentiality. The survey administrator signed a sepa- rate form that ensured the confidentiality of the data and students’ anonymity.
Analvsis
After collection of the data, a variety of statistical analyses were executed to determine statistical significance. These included regression and multivariate analyses. Data for more detailed responses about the frequency of use or engage- ment in various risk behaviors were not included in this analysis because of in-
34 Journal of Addictions & Offender Counseling * October 2001 * Volume 22
consistent answers and, in some cases, the small number of responses to particu- lar questions. This limitation precluded our analyzing this information using the originally intended statistical tools. However, reporting the frequencies and pat- terns observed in the data informs the reader. Multiple patterns of behavior and interactions between factors warrant further investigation.
Results
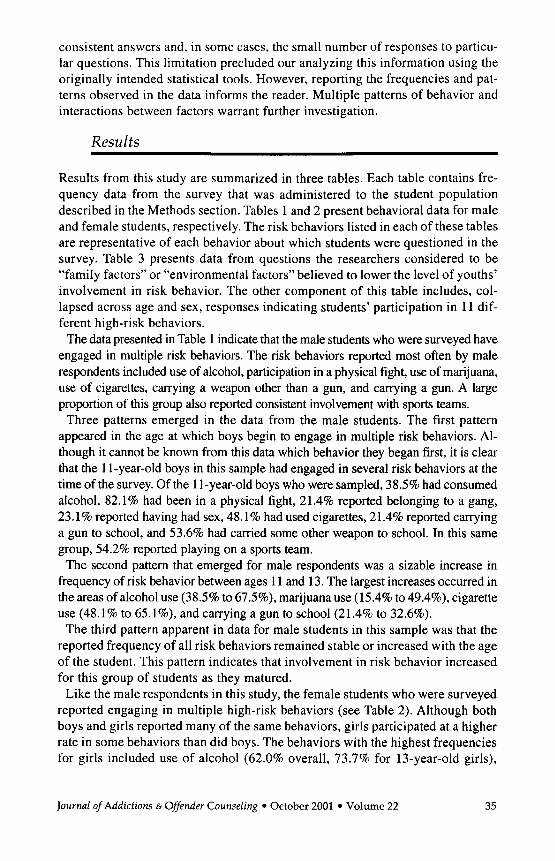
Results from this study are summarized in three tables. Each table contains fre- quency data from the survey that was administered to the student population described in the Methods section. Tables 1 and 2 present behavioral data for male and female students, respectively. The risk behaviors listed in each of these tables are representative of each behavior about which students were questioned in the survey. Table 3 presents data from questions the researchers considered to be “family factors” or “environmental factors” believed to lower the level of youths’ involvement in risk behavior. The other component of this table includes, col- lapsed across age and sex, responses indicating students’ participation in 11 dif- ferent high-risk behaviors.
The data presented in Table 1 indicate that the male students who were surveyed have engaged in multiple risk behaviors. The risk behaviors reported most often by male respondents included use of alcohol, participation in a physical fight, use of marijuana, use of cigarettes, carrying a weapon other than a gun, and carrying a gun. A large proportion of this group also reported consistent involvement with sports teams.
Three patterns emerged in the data from the male students. The first pattern appeared in the age at which boys begin to engage in multiple risk behaviors. Al- though it cannot be known from this data which behavior they began first, it is clear that the 1 1-year-old boys in this sample had engaged in several risk behaviors at the time of the survey. Of the 1 1-year-old boys who were sampled, 38.5% had consumed alcohol, 82.1% had been in a physical fight, 21.4% reported belonging to a gang, 23.1% reported having had sex, 48.1% had used cigarettes, 21.4% reported carrying a gun to school, and 53.6% had carried some other weapon to school. In this same group, 54.2% reported playing on a sports team.
The second pattern that emerged for male respondents was a sizable increase in frequency of risk behavior between ages 1 1 and 13. The largest increases occurred in the areas of alcohol use (38.5% to 67.5%), marijuana use (15.4% to 49.4%), cigarette use (48.1% to 65.1%), and carrying a gun to school (21.4% to 32.6%).
The third pattern apparent in data for male students in this sample was that the reported frequency of all risk behaviors remained stable or increased with the age of the student. This pattern indicates that involvement in risk behavior increased for this group of students as they matured.
Like the male respondents in this study, the female students who were surveyed reported engaging in multiple high-risk behaviors (see Table 2). Although both boys and girls reported many of the same behaviors, girls participated at a higher rate in some behaviors than did boys. The behaviors with the highest frequencies for girls included use of alcohol (62.0% overall, 73.7% for 13-year-old girls),
Journal of Addictions 6 Offender Counseling October 2001 Volume 22 35
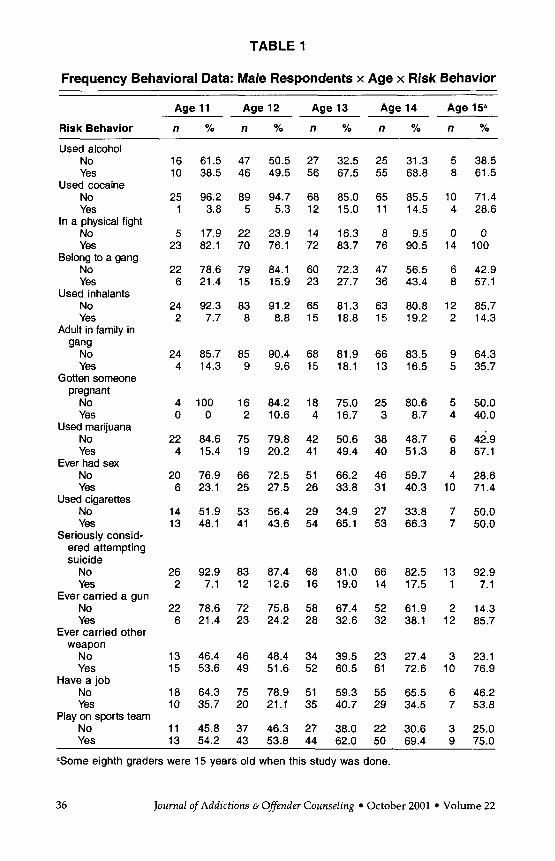
TABLE 1
Frequency Behavioral Data: Male Respondents x Age x Risk Behavior
Age 11 Age 12 Age 13 Age 14 Age 15"
Risk Behavior n % n % n Yo n Yo n 70
Used alcohol No Yes
Used cocaine No Yes
No Yes
No Yes
No Yes
gang No Yes
pregnant No Yes
Used marijuana No Yes
Ever had sex No Yes
No Yes
In a physical fight
Belong to a gang
Used inhalants
Adult in family in
Gotten someone
Used cigarettes
Seriously consid- ered attempting suicide
No Yes
No Yes
weapon No Yes
Have a job No Yes
Play on sports team No
Ever carried a gun
Ever carried other
16 61.5 47 50.5 27 32.5 25 31.3 5 38.5 10 38.5 46 49.5 56 67.5 55 68.8 8 61.5
25 96.2 89 94.7 68 85.0 65 85.5 10 71.4 1 3.8 5 5.3 12 15.0 11 14.5 4 28.6
5 17.9 22 23.9 14 16.3 8 9.5 0 0 23 82.1 70 76.1 72 83.7 76 90.5 14 100
22 78.6 79 84.1 60 72.3 47 56.5 6 42.9 6 21.4 15 15.9 23 27.7 36 43.4 8 57.1
24 92.3 83 91.2 65 81.3 63 80.8 12 85.7 2 7.7 8 8.8 15 18.8 15 19.2 2 14.3
24 85.7 85 90.4 68 81.9 66 83.5 9 64.3 4 14.3 9 9.6 15 18.1 13 16.5 5 35.7
4 100 16 84.2 18 75.0 25 80.6 5 50.0 0 0 2 10.6 4 16.7 3 8.7 4 40.0
22 84.6 75 79.8 42 50.6 38 48.7 6 42.9 4 15.4 19 20.2 41 49.4 40 51.3 8 57.1
20 76.9 66 72.5 51 66.2 46 59.7 4 28.6 6 23.1 25 27.5 26 33.8 31 40.3 10 71.4
14 51.9 53 56.4 29 34.9 27 33.8 7 50.0 13 48.1 41 43.6 54 65.1 53 66.3 7 50.0
26 92.9 83 87.4 68 81.0 66 82.5 13 92.9 2 7.1 12 12.6 16 19.0 14 17.5 1 7.1
22 78.6 72 75.8 58 67.4 52 61.9 2 14.3 6 21.4 23 24.2 28 32.6 32 38.1 12 85.7
13 46.4 46 48.4 34 39.5 23 27.4 3 23.1 15 53.6 49 51.6 52 60.5 61 72.6 10 76.9
18 64.3 75 78.9 51 59.3 55 65.5 6 46.2 10 35.7 20 21.1 35 40.7 29 34.5 7 53.8
11 45.8 37 46.3 27 38.0 22 30.6 3 25.0 Yes 13 54.2 43 53.8 44 62.0 50 69.4 9 75.0
a.Some eighth graders were 15 years old when this study was done.
36 Journal of Addictions & Offender Counseling October 2001 Volume 22
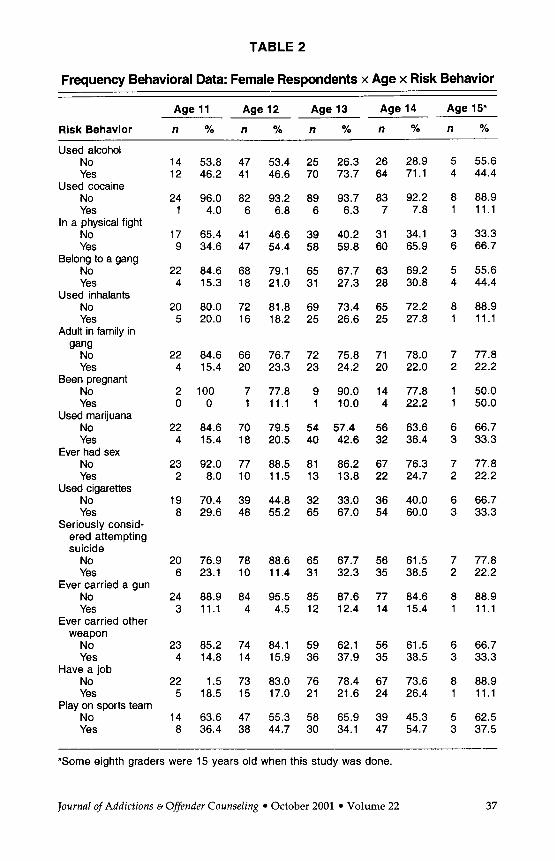
TABLE 2
Frequency Behavioral Data: Female Respondents x Age x Risk Behavior
Age 11 Age 12 Age 13 Age 14 Age 15"
Risk Behavior n % n % n % n % n %
Used alcohol No Yes
Used cocaine No Yes
No Yes
In a physical fight
Belong to a gang No Yes
No Yes
Clang No Yes
Been pregnant No Yes
Used marijuana No Yes
Ever had sex No Yes
No Yes
Used inhalants
Adult in family in
Used cigarettes
Seriously consid- ered attempting suicide
No Yes
No Yes
weapon No Yes
Have a job No Yes
Play on sports team No Yes
Ever carried a gun
Ever carried other
14 53.8 47 53.4 25 26.3 26 28.9 12 46.2 41 46.6 70 73.7 64 71.1
24 96.0 82 93.2 89 93.7 83 92.2 1 4.0 6 6.8 6 6.3 7 7.8
17 65.4 41 46.6 39 40.2 31 34.1 9 34.6 47 54.4 58 59.8 60 65.9
22 84.6 68 79.1 65 67.7 63 69.2 4 15.3 18 21.0 31 27.3 28 30.8
20 80.0 72 81.8 69 73.4 65 72.2 5 20.0 16 18.2 25 26.6 25 27.8
22 84.6 66 76.7 72 75.8 71 78.0 4 15.4 20 23.3 23 24.2 20 22.0
2 100 7 77.8 9 90.0 14 77.8 0 0 1 11.1 1 10.0 4 22.2
22 84.6 70 79.5 54 57.4 56 63.6 4 15.4 18 20.5 40 42.6 32 36.4
23 92.0 77 88.5 81 86.2 67 76.3 2 8.0 10 11.5 13 13.8 22 24.7
19 70.4 39 44.8 32 33.0 36 40.0 8 29.6 48 55.2 65 67.0 54 60.0
20 76.9 78 88.6 65 67.7 56 61.5 6 23.1 10 11.4 31 32.3 35 38.5
24 88.9 84 95.5 85 87.6 77 84.6 3 11.1 4 4.5 12 12.4 14 15.4
23 85.2 74 84.1 59 62.1 56 61.5 4 14.8 14 15.9 36 37.9 35 38.5
22 1.5 73 83.0 76 78.4 67 73.6 5 18.5 15 17.0 21 21.6 24 26.4
14 63.6 47 55.3 58 65.9 39 45.3 8 36.4 38 44.7 30 34.1 47 54.7
5 55.6 4 44.4
8 88.9 1 11.1
3 33.3 6 66.7
5 55.6 4 44.4
8 88.9 1 11.1
7 77.8 2 22.2
1 50.0 1 50.0
6 66.7 3 33.3
7 77.8 2 22.2
6 66.7 3 33.3
7 77.8 2 22.2
8 88.9 1 11.1
6 66.7 3 33.3
8 88.9 1 11.1
5 62.5 3 37.5
"Some eighth graders were 15 years old when this study was done.
Journal of Addictions B Offender Counseling October 2001 Volume 22 37
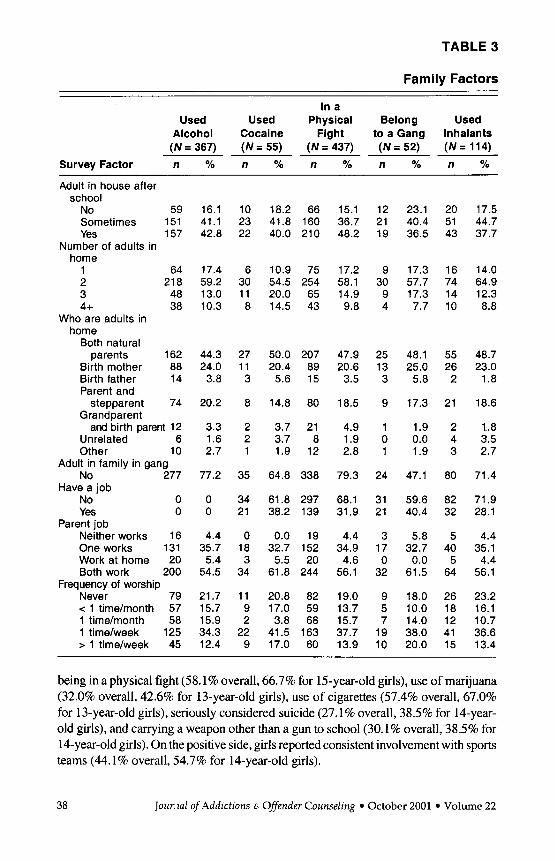
TABLE 3
Family Factors
In a Used Used Physical Belong Used
Alcohol Cocaine Fight to a Gang Inhalants ( N = 367) ( N = 55) ( N = 437) (N= 52) ( N = 114)
Survey Factor n % n % n % n % n %
Adult in house after school
No 59 Sometimes 151 Yes 157
Number of adults in home
1 64 2 21 8 3 48 4+ 38
Who are adults in home
Both natural parents 162
Birth mother 88 Birth father 14 Parent and
stepparent 74 Grandparent
and birth parent 12 Unrelated 6 Other 10
No 277
No 0 Yes 0
Neither works 16 One works 131 Work at home 20 Both work 200
Never 79 < 1 time/month 57 1 time/month 58 1 time/week 125 > 1 time/week 45
Adult in family in gang
Have a job
Parent job
Frequency of worship
16.1 10 18.2 41.1 23 41.8 42.8 22 40.0
17.4 6 10.9 59.2 30 54.5 13.0 1 1 20.0 10.3 8 14.5
44.3 27 50.0 24.0 1 1 20.4 3.8 3 5.6
20.2 8 14.8
3.3 2 3.7 1.6 2 3.7 2.7 1 1.9
77.2 35 64.8
0 34 61.8 0 21 38.2
4.4 0 0.0 35.7 18 32.7 5.4 3 5.5 54.5 34 61.8
21.7 1 1 20.8 15.7 9 17.0 15.9 2 3.8 34.3 22 41.5 12.4 9 17.0
66 160 21 0
75 254 65 43
207 89 15
80
21 8 12
338
297 139
19 152 20 244
82 59 68 163 60
15.1 12 23.1 20 36.7 21 40.4 51 48.2 19 36.5 43
17.2 9 17.3 16 58.1 30 57.7 74 14.9 9 17.3 14 9.8 4 7.7 10
47.9 25 48.1 55 20.6 13 25.0 26 3.5 3 5.8 2
18.5 9 17.3 21
4.9 1 1.9 2 1.9 0 0.0 4 2.8 1 1.9 3
79.3
68.1 31.9
4.4 34.9 4.6 56.1
19.0 13.7 15.7 37.7 13.9
24
31 21
3 17 0 32
9 5 7 19 10
47.1
59.6 40.4
5.8 32.7 0.0 61.5
18.0 10.0 14.0 38.0 20.0
80
82 32
5 40 5 64
26 18 12 41 15
17.5 44.7 37.7
14.0 64.9 12.3 8.8
48.7 23.0 1 .8
18.6
1.. 8 3.5 2.7
71.4
71.9 28.1
4.4 35.1 4.4 56.1
23.2 16.1 10.7 36.6 13.4
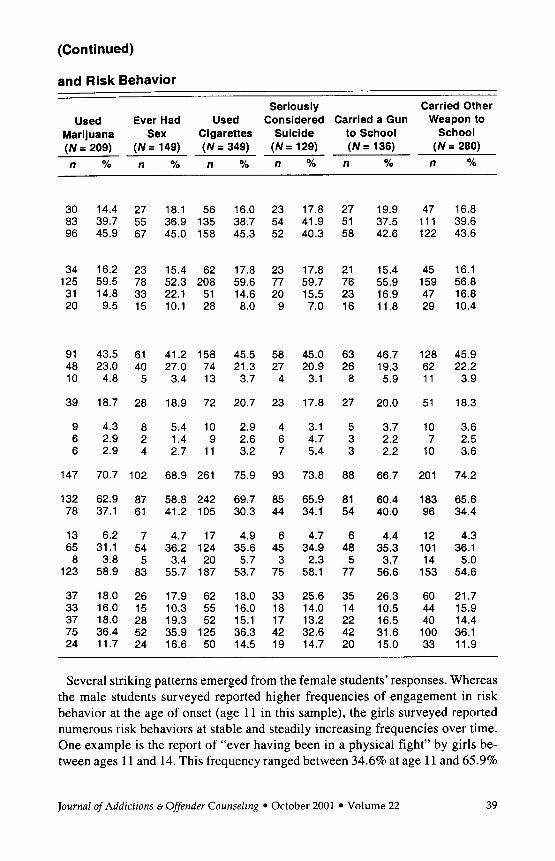
being in a physical fight (58.1% overall, 66.7% for 15-year-old girls), use of marijuana (32.0% overall, 42.6% for 13-year-old girls), use of cigarettes (57.4% overall, 67.0% for 13-year-old girls), seriously considered suicide (27.1 % overall, 38.5% for 14-year- old girls), and carrying a weapon other than a gun to school (30.1% overall, 38.5% for 14-year-old girls). On the positive side, girls reported consistent involvement with sports teams (44.1% overall, 54.7% for 14-year-old girls).
38 Jour.1~2 of Addictions E. Offender Counseling October 2001 Volume 22
(Continued)
and Risk Behavior
Seriously Carried Other Used Ever Had Used Considered Carried a Gun Weapon to
Marijuana Sex Cigarettes Suicide to School School
% n YO ( N = 209) ( N = 149) ( N = 349) ( N = 129) ( N = 136) ( N = 280) n YO n % n % n % n
30 14.4 27 18.1 56 16.0 23 17.8 27 83 39.7 55 36.9 135 38.7 54 41.9 51 96 45.9 67 45.0 158 45.3 52 40.3 58
34 16.2 23 15.4 62 17.8 23 17.8 21 125 59.5 78 52.3 208 59.6 77 59.7 76 31 14.8 33 22.1 51 14.6 20 15.5 23 20 9.5 15 10.1 28 8.0 9 7.0 16
91 48 10
39
9 6 6
147
132 78
13 65 8
123
37 33 37 75 24
43.5 23.0 4.8
18.7
4.3 2.9 2.9
70.7
62.9 37.1
6.2 31.1 3.8 58.9
18.0 16.0 18.0 36.4 11.7
61 40 5
28
8 2 4
102
87 61
7 54 5 83
26 15 28 52 24
41.2 158 27.0 74 3.4 13
18.9 72
5.4 10 1.4 9 2.7 1 1
68.9 261
58.8 242 41.2 105
4.7 17 36.2 124 3.4 20 55.7 187
17.9 62 10.3 55 19.3 52 35.9 125 16.6 50
45.5 58 45.0 63 21.3 27 20.9 26 3.7 4 3.1 8
20.7 23 17.8 27
2.9 4 3.1 5 2.6 6 4.7 3 3.2 7 5.4 3
75.9 93 73.8 88
69.7 85 65.9 81 30.3 44 34.1 54
4.9 6 4.7 6 35.6 45 34.9 48 5.7 3 2.3 5 53.7 75 58.1 77
18.0 33 25.6 35 16.0 18 14.0 14 15.1 17 13.2 22 36.3 42 32.6 42 14.5 19 14.7 20
19.9 37.5 42.6
15.4 55.9 16.9 11.8
46.7 19.3 5.9
20.0
3.7 2.2 2.2
66.7
60.4 40.0
4.4 35.3 3.7 56.6
26.3 10.5 16.5 31.6 15.0
47 16.8 1 1 1 39.6 122 43.6
45 16.1 159 56.8 47 16.8 29 10.4
128 45.9 62 22.2 1 1 3.9
51 18.3
10 3.6 7 2.5 10 3.6
201 74.2
183 65.6 96 34.4
12 4.3 101 36.1 14 5.0 153 54.6
60 21.7 44 15.9 40 14.4 100 36.1 33 11.9
Several striking patterns emerged from the female students’ responses. Whereas the male students surveyed reported higher frequencies of engagement in risk behavior at the age of onset (age 11 in this sample), the girls surveyed reported numerous risk behaviors at stable and steadily increasing frequencies over time. One example is the report of “ever having been in a physical fight” by girls be- tween ages l l and 14. This frequency ranged between 34.6% at age l l and 65.9%
Journal of Addictions &Offender Counseling October 2001 Volume 22 39
for 14-year-old girls. Other examples of the increase between ages 11 and 14 in- clude gang involvement (15.3% to 30.8%), marijuana use (15.4% to 36.4%), sexual activity (8.0% to 24.7%), cigarette use (29.6% to 60.0%), and carrying a weapon other than a gun to school (14.8% to 38.5%).
The other significant pattern that was apparent in the data for female youth in this sample was the increase in reported frequency of risk behavior between ages 11 and 12 and between ages 12 and 13. Data for girls transitioning from age 11 to age 12 indicated a sharp increase in reports of physical fighting (34.6% to 54.4%), gang membership (15.3% to 21.0%), marijuana use (15.4% to 20.5%), and cigarette use (29.6% to 55.2%). Another dramatic increase occurred between the ages of 12 and 13. In this case, the increase in risk behavior was also seen in some behaviors other than the behaviors that had shown increases for the 11- to 12-year-old girls. Data for 12- to 13-year-olds showed an increase in alcohol use (46.6% to 73.7%), inhalant use (18.2% to 26.6%), marijuana use (20.5% to 42.6%), cigarette use (55.2% to 67.0%), consideration of suicide attempt (1 1.4% to 32.3%), and carrying a weapon other than a gun to school (15.9% to 37.9%).
An unanticipated result indicated by the data was in the area of suicidality. “Serious consideration” of attempting suicide varied distinctly for boys and girls. Overall, 27.1% of girls who were surveyed reported a serious consideration of attempting suicide whereas 15.1% of all boys who were surveyed considered suicide. Consider- ation of a suicide attempt peaked for girls at age 14 (38.5%) and at age 13 for boys (19.0%). Reports of serious consideration of suicide also varied by ethnicity. A total of 129 students reported that they had seriously considered attempting suicide. Of this number, 27.1% (n = 35) were Anglo, 10.1% (n = 13) were African American, 40.3% (n = 52) were Hispanic, and 22.5% (n = 29) were of mixed ethnic origin:
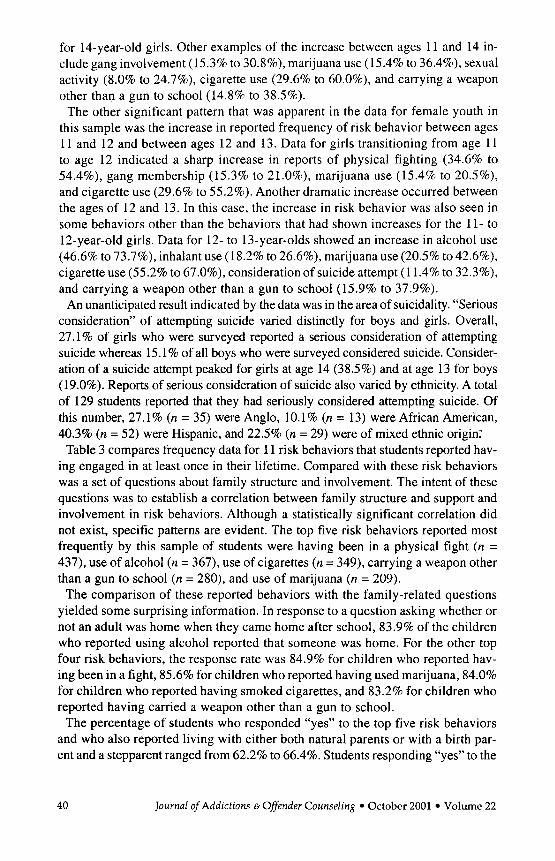
Table 3 compares frequency data for 11 risk behaviors that students reported hav- ing engaged in at least once in their lifetime. Compared with these risk behaviors was a set of questions about family structure and involvement. The intent of these questions was to establish a correlation between family structure and support and involvement in risk behaviors. Although a statistically significant correlation did not exist, specific patterns are evident. The top five risk behaviors reported most frequently by this sample of students were having been in a physical fight (n = 437), use of alcohol (n = 367), use of cigarettes (n = 349), carrying a weapon other than a gun to school (n = 280), and use of marijuana (n = 209).
The comparison of these reported behaviors with the family-related questions yielded some surprising information. In response to a question asking whether or not an adult was home when they came home after school, 83.9% of the children who reported using alcohol reported that someone was home. For the other top four risk behaviors, the response rate was 84.9% for children who reported hav- ing been in a fight, 85.6% for children who reported having used marijuana, 84.0% for children who reported having smoked cigarettes, and 83.2% for children who reported having carried a weapon other than a gun to school.
The percentage of students who responded “yes” to the top five risk behaviors and who also reported living with either both natural parents or with a birth par- ent and a stepparent ranged from 62.2% to 66.4%. Students responding “yes” to the
40 Journal of Addictions 6 Oflender Counseling October 2001 Volume 22
top five risk behaviors also reported attending some form of religious worship one time or more per week. These frequencies were use of alcohol (46.7%), in a physical fight (51.6%), use of marijuana (48.1%). use of cigarettes (50.8%), and carrying a weapon other than a gun to school (48.0%).
Uncommonly high frequencies appeared between responses of “yes” across several risk behaviors included in Table 3 and having an adult gang member in the family. Fifty-three percent of students who reported that they were active gang members also reported that an adult in their household was in a gang. Of students who reported using cocaine or marijuana, having sex, and carrying a gun to school, a median of 33.3% also reported having an adult gang member in their household.
Family factors did not seem to have a great impact on suicidality. Of the students who reported seriously considering a suicide attempt, 82.2% of them reported that an adult was in the house after school most of the time. Forty-five percent of students responding “yes” to serious consideration of suicide reported that they lived with both of their natural parents. Another 17.8% reported living with one natural parent and a stepparent. Perhaps most surprising was the relationship between “seriously considered suicide” and frequency of worship. Of students responding “yes” to hav- ing seriously considered a suicide attempt, 47.3% reported that they attended some form of worship one or more times per week.
Discussion
Results of the study indicate that the students in this sample engage in multiple high-risk behaviors. Many of the behaviors seem to overlap-when students re- ported doing one type of behavior, they also reported engaging in other high-risk behaviors at a very high rate. High-risk behaviors, such as carrying a weapon, drinking alcohol, smoking marijuana, being sexually active, and being involved with gangs, typically occurred together. No statistically significant relationship was determined between or among behaviors. Anecdotally, the highest noted re- lationship was between inhalants and other risk behaviors.
Some risk behaviors were reported at a higher frequency when analyzed by sex. The behaviors that varied most were reported gang membership and sexual activity by male students. The reported frequency of gang membership was comparable in both sexes until age 14, at which time this figure for boys jumped from 27.7% at age 13 to 43.4%. The frequency and increase were not as high for girls, increasing from 27.3% to 30.8% in reported gang membership. Re- ports of serious considerations of suicide attempts differed for boys and girls. As was presented earlier in this article, serious consideration of attempting suicide peaked for 13-year-old boys at 19.0%. These figures were quite dif- ferent for girls. Responses to the same question peaked for 14-year-old girls at 38.5%. Serious consideration of a suicide attempt also varied by ethnic subgroup. Of this number, 27.1% ( n = 35) were Anglo, 10.1% ( n = 13) were African American, 40.3% ( n = 52) were Hispanic, and 22.5% (n = 29) were of mixed ethnic origin.
Journal of Addictions 6 Offender Counseling October 2001 Volume 22 41
These differences suggest that girls and boys of different ethnicities struggle with unique issues during adolescence and may be susceptible to social and peer pressures unique to their sex and culture.
Although this study did not survey youth below age 11, it was remarkable how many students were already engaged in multiple risk behaviors at this age. This finding suggests that experimentation with or use of substances, or both, and in- volvement in other risk behaviors may have occurred before age 11. The stability and chronicity of these risk behaviors over time are cause for great concern. For both boys and girls, engagement in a particular risk behavior that had begun at age 11 either remained constant or increased steadily with the age of the student.
One would expect behavior to be maintained or intensified over time in the absence of some interruption or alternative to that behavior. These data suggest that there is no buffer process acting in the lives of these youth that might change the course of their behavioral choices. Huizinga et al. (1993) showed very similar results with longitudinal data from their work in Denver, Pittsburgh, and Roches- ter documenting risk behavior. The chronicity of risk behavior was documented through increased rates of risk behavior as the youth whom they tracked matured.
Another noteworthy result was the appearance of certain “vulnerable” periods, or age transitions, after which reports of particular risk behaviors increased markedly. Some of these increases occurred between ages 11 and 12 and others between ages 12 and 13. For some youth, these are the ages at which they move into middle school or junior high school. This pattern was common for both boys and girls. The appearance of critical transition periods after which risk behaviors in- crease markedly should signal practitioners to intervene not only after the behav- ior worsens but also long before it begins.
Patterns in responses regarding family factors and engagement in risk behavior did not support the original hypothesis of the impact of family structure and en- vironment. The expectation was that factors, such as the marital status of parents and the composition of the household, would be related to decreased numbers of youth involved in risk behaviors. Across the 11 risk behaviors compared with family-related questions, a mode of 82% responded “sometimes” or “yes” that there was an adult home after school. Over 60.0% of respondents in any one risk behavior category also reported that they lived with either both natural parents or with one parent and a stepparent. Clearly, the marital status of parents did not have a great impact on behavioral choices for this sample of students.
It became clear in analyzing the results of this study that in order to establish a link between family structure and environment and lower levels of risk be- havior, a different type of question needed to be asked. The informational questions that we designed did not provide the knowledge about relationships between and among family members that we had anticipated. It is this informa- tion about relationships that may speak to the behavior choices being made by these children. Researchers need to examine the quality of the relationships within the family and how the quality of the relationship influences behavior to gain a better understanding of the correlation between family and risk-behavior participation.
42 Journal of Addictions &Offender Counseling October 2001 Volume 22
Perhaps most interesting among the comparisons between family and risk be- havior was the reported frequency of worship. A range of 46.6% to 58.0% of the students reported attending some form of religious worship one time or more weekly across all 11 risk behaviors (see Table 3). For example, of the students who reported being in a gang, 58.0% of them also reported attending a worship service at least one time per week.
The high frequency of reported worship attendance despite risk behavior may be accounted for by cultural norms and expectations involving participation in organized religion. The city in which this study was conducted has a large His- panic population and that population’s norms regarding church attendance may have influenced these results.
Summary
The results of this study have several implications that are descriptive of youth risk behavior. First, youth are engaging in multiple high-risk behaviors rather than a single risk behavior. Typical combinations for this sample included use of drugs and alcohol, sexual activity, and some form of physical aggression usually associated with a gang or a weapon. Second, students begin these risk behaviors at an early age (age 11 for this study). Third, students are not participating in risk behaviors on an experimental level. Instead, young people are engaging in com- binations of risk behaviors throughout their teenage development. Furthermore, reports of engaging in risk behaviors increase at each age level through the teen years. Rather than “growing out of it,” youth are becoming firmly entrenched in patterns of high-risk behaviors. Fourth, girls and boys engage in particular com- binations of risk behaviors based on their sex. In this sample, girls seemed to be more susceptible to pressures culminating in serious consideration of a suicide attempt whereas boys tended to report higher rates of gang membership and sexual activity. Finally, both boys and girls seem to experience “critical” ages at which times they are more vulnerable than at other times. These ages fall around the years typically associated with a major life change, such as the move from el- ementary school to middle school and the move from middle school to high school. In the absence of intervention, involvement in risk behavior will likely increase following these critical periods. Young people may resort to increased risk be- havior as a method of coping.
Implications for Counseling
Schools, counselors, families, and communities have a high level of concern for the youth in their neighborhoods. This survey is compelling evidence that many youth may be headed toward highly negative outcomes as adults. The long-term impact of early and sustained multiple risk behaviors is easy to predict. What these young people face could include a lifetime of chronic substance use, poor achievement, limited employment, health problems, incarceration, and possibly premature death.
Journal of Addictions 6 Offender Counseling October 2001 Volume 22 43
What can be done to intervene, to change the course of their choices? What can be done to help establish that buffer in their lives that will protect them as they grow? Many practitioners have asked similar questions. Their great concern for the future of young people has produced a variety of activities and large-scale intervention programs designed to prevent the onset of risk behavior, to curb the cycle of risk behavior, and to help develop the buffer that young people need.
Durlak (1995) presented a thorough review of the components of effective prevention programs as well as programs that have been demonstrated to be effective in producing long-term behavior change. There are several “best practices” to follow in implement- ing school-based prevention programs. First, intervention should begin early. School personnel need to catch children before those critical periods, when risky behavior seems to increase, to help them explore and shape their beliefs about risky behavior. Second, youth need factual information about what drugs, weapons, gangs, and so forth can do to them-now and in the future. Third, they need to have the opportunity to evaluate their own feelings about these behaviors, and, finally, they must learn and practice the skills to help them make good choices.
The timing and the target of the intervention are important. Most systemic programs begin somewhere during Grades 5 through 8. For prevention focused on substance use, it is common to attend to the drugs used with high frequency, such as alcohol and cigarettes. Successful prevention of use of these drugs significantly decreases the chances of youth using riskier substances (Johnson et al., 1990).
The duration of the program and the ecological impact of the program also make a difference. Prevention programs should be implemented over a continuous length of time. Short, reactive intervention programs do not have the impact intended (the durability of program impact). Often such programs lack the scope and intensity required to support lasting behavioral change in students (Simeonsson, 1995). In order to internalize the values and behaviors that protect children from choosing risky behavior, they need to see, hear, and think about these values as they mature (Durlak, 1995). Furthermore, programs should try to address as broad an ecologi- cal scope as possible to have an impact on the several systems by which students are influenced (Durlak, 1995).
Although the data from this study showed that boys and girls participated in several common risk behaviors, it also showed that girls tended to report more serious consideration of suicide whereas boys reported being sexually active and belonging to gangs at a higher rate. This suggests that girls and boys may need different types of intervention involving these behaviors or supporting psychoso- cia1 traits that are unique to each sex. Unfortunately, there seems to be little in the current literature on prevention or intervention programs tailored specifically for either sex.
More than ever, young people in this country are engaging in and becoming entrenched in patterns of behavior that are serious threats to their safety. Although the data col- lected in this study do not reveal startling new information, the study does reinforce the urgent necessity of developing preventiodintervention programs for children. It is im- perative that counselors become involved at all levels of prevention and intervention programs, educational programs, and in social advocacy for these programs.
44 Journal of Addictions & Offender Counseling October 2001 Volume 22
Endnote. This study was completed in Denver, Colorado, approximately 18 months before the Columbine incident in Littleton. We must, as a profession and a com- munity, find ways to reengage children and youth with our families and our com- munities. Our youth are the hope of tomorrow. They are our responsibility.
References
Andrews, J., Hops, H., Ary, D., Tildesley, E., & Hams, J. (1993). Parental influence on early adolescent substance use: Specific and nonspecific effects. Journal of Early Adolescence, 13. 285-310.
Beauvais, F,, Chavez, E., Oetting, E., Deffenbacher, J., & Comell, G. (1996). Drug use, violence, and victimization among White American, Mexican American, and American Indian dropouts, students with academic problems, and students in good academic standing. Journal ofCounseling Psychology, 43(3), 292-299.
Benson, P. (1997). All children are our children. San Francisco: Jossey-Bass. Benson, P., Galbraith, J., & Espeland, P. (1995). What kids need to succeed. Minneapolis, MN: Free
Spirit. Brener, N., Collins, J., Kann, L, Warren, C., &Williams, B. (1995). Reliability of the Youth Risk Behavior
Survey questionnaire. American Journal of Epidemiology, 141, 575-580. Bronfenbrenner, U. (1979). The ecology of human development. Cambridge, MA: Harvard University
Press. Brownfield, D., & Sorenson, A. (1991). Religion and drug use among adolescents: A social support
conceptualization and interpretation. Deviant Behavior: An Interdisciplinary Journal, 12, 259-216. Centers for Disease Control and Prevention. (1996a). 1996 YRBS information and results. Avail-
able at http:llwww.cdc.govlnccdphpldasNyrbsI Centers for Disease Control and Prevention. (1996b). Youth risk behavior survey. Atlanta, GA:
Author. Dinwiddie, S. (1994). Abuse of inhalants: A review. Addiction, 89, 925-939. Dugan, T., & Coles, R. (Eds.). (1989). The child in our times: Studies in the development of resil-
Durlak, J. A. (1995). School-based prevention programs for children and adolescents. Thousand
Eitelbach-Stitcher, C. (1996). Risk and resiliency. Alexandria, VA: Macro International. Garbarino, J. (1992). Children in danger: Coping with the consequences of community violence.
San Francisco: Jossey-Bass. Garmezy, N. (1985). Stress-resistant children: The search for protective factors. In J. E. Stevenson
(Ed.), Recent research in developmental psychopathology: Journal of child psychology and psy- chiatry (pp. 213-233). Oxford, England: Pergamon Press.
Garmezy, N. (1991). Resiliency and vulnerability to adverse developmental outcomes associated with poverty. American Behavioral Scientist, 34, 416430.
Hawley, D., & DeHaan, L. (1996). Toward a definition of family resilience: Integrating life-span and family perspectives. Family Processes, 35, 283-298.
Huizinga, D., Loeber, R., & Thornberry, T. (1993). Longitudinal study of delinquency, drug use, sexual activity, and pregnancy among children and youth in three cities. Public Health Reports, I08(Suppl. I) , 90-96.
Johnson, C. A., Pentz, M. A., Weber, M. D., Dwyer, J. H., Baer, N., MacKinnon, D. P., Hansen, W. B., & Flay, B. R. (1990). Relative effectiveness of comprehensive community programming for drug abuse prevention with high-risk and low-risk adolescents. Journal of Consulting and Clini- cal Psychology, 58, 447456.
Kann, L., Warren, W., Collins, J., Ross, J., Collins, B., & Kolbe, L. (1993). Results from the na- tional school-based 1991 Youth Risk Behavior Survey and progress toward achieving related health objectives for the nation. Public Health Reports, 108(Suppl. I ) , 47-55.
Luthar, S. (1991 ). Vulnerability and resilience: A study of high-risk adolescents. Child Develop- ment, 62, 600-616.
iency. New York: BrunnerlMazel.
Oaks, CA: Sage.
Journal of Addictions &Offender Counseling October 2001 Volume 22 45

Luthar, S., & Zigler, E. (1991). Vulnerability and competence: A review of research on resilience
Marcus, S., Giovino, G. A,, Pierce, J., & Harel, Y. (1993). Measuring tobacco use among adoles-
Masten, A,, Best, K., & Garmezy, N. (1990). Resilience and development: Contributions from the
Masten, A,, & Coatsworth, J. (1998). The development of competence in favorable and unfavor-
Morris, L., Warren, C., & Aral, S. (1993). Measuring adolescent sexual behaviors and related health
O’Carroll, P., Harel, Y., & Waxweiler, R. (1993). Measuring adolescent behaviors related to inten-
Pianta, R., & Walsh, D. (1996). High-risk children in schools. New York: Routledge. Rutter, M. (1985). Resilience in the face of adversity: Protective factors and resistance to psychi-
Rutter, M. (1993). Resilience: Some conceptual considerations. Journal of Adolescent Health, 14,
Seligman, M. (1995). The optimistic child. New York: Houghton Mifflin. Simeonsson, R. (1995). Risk, resilience, and prevention: Promoting the well-being of all children.
Walsh, F. (1996). The concept of family resilience: Crisis and challenge. Family Process, 35, 261-281. Werner, E. (1 993). Risk, resilience, and recovery: Perspectives from the Kauai Longitudinal Study.
Werner, E., & Smith, R. (1992). Overcoming the odds: High-risk children from birth ro adulthood.
Wolin, S., & Wolin, S. (1993). The resilient se& How survivors of troubled families rise above
in childhood. American Journal of OrthopJychiatry, 61, 6-22.
cents. Public Health Reports, lOd(Supp1. I ) , 20-24.
study of children who overcome adversity. Development and Psychopathology, 2, 425-444.
able environments. American Psychologist, 53(2), 205-220.
outcomes. Public Health Reports, IOd(Supp1. I), 31-37.
tional injuries. Public Health Reports, lOd(Supp1. I ) , 15-19.
atric disorder. British Journal of Psychiatry, 147, 598-61 1.
626-63 1.
Baltimore: Brookes.
Development and Psychopathology, 5, 503-5 15.
Ithaca, N Y Cornell University Press.
adversity. New York: Villard.
46 Journal of Addictions 6 Offender Counseling October 2001 Volume 22