your name and credentials central thalamic deep brain stimulation for treatment of chronic...
TRANSCRIPT

Your name and credentials
Central Thalamic Deep Brain Stimulation for Treatment of Chronic Post-Traumatic Minimally Conscious State: Challenges and Opportunities
Joseph T. Giacino, Ph.D.Director of Rehabilitation Neuropsychology, Spaulding Rehabilitation HospitalAssociate Professor, Harvard Medical School

Disclosure
Dr. Giacino has no significant financial relationship with any commercial or proprietary entity that produces healthcare-related products and/or services relevant to the content of this presentation.

Minimally Conscious State
The minimally conscious state is a condition of severely altered consciousness in which minimal but definite behavioral evidence of self or environmental awareness is demonstrated.
(Giacino, et al., Neurol, 2002)
Clinical Rationale for DBS in MCS
• Permanent minimally conscious state represents a devastating functional, social and economic outcome.
• Despite preservation of volitional behavior, response consistency frequently insufficient to support rehabilitation interventions and assistive devices designed to facilitate reliable communication and environmental control
• No existing treatment proven to alter the course of recovery from MCS.

Clinical Rationale for DBS in MCS
• fMRI findings demonstrate widely preserved cortical networks responsible for mediating language and visuoperceptual functions in MCS pts unable to follow commands or communicate reliably.
• Recent primate and rodent studies show dramatic modulation of behavioral performance in intact animals exposed to DBS

Neurophysiologic Rationale for DBS in MCS
• Thalamic intralaminar nuclei (ILN) influence parallel cortico-striato-pallidal-thalamocortical loop circuits of anterior forebrain.
• ILN provide wide, but selective, projections to downstream cortical fields.
• ILN comprised of neuronal populations that selectively activate and modulate cortical signals related to vigilance, sustained attention, motor intention, working memory.

Projections from ILN
Scannell et al. 1999
Multidimensional scaling of thalamocortical
connectivitiesAdapted from:Posner and Raichle 1994, Munkle et al. 2000.
Striatum

DMN Connectivity in DoC
(Vanhaudenhuyse, et al. Brain 2010)

Thalamic cell loss and outcomes ofmulti-focal severe brain injury
•Moderately disabled: neuronal loss in Anterior intralaminar nuclei •Severely disabled/MCS: inclusion of medial aspect of posterior intralaminar nuclei •Vegetative state: progressive loss of neurons across central thalamus extending into the more lateral posterior intralaminar nuclei
Maxwell, et al. Thalamic Nuclei after Human Blunt Head Injury J. Neuropathol Exp Neurol 2006. 65:478-488

Purpose of Current Research
To determine if deep brain stimulation applied to the thalamic ILN of patients in the chronic form of the minimally conscious state can facilitate further functional improvement.

Primary Aims
• To determine the acute, sub-acute and chronic effects of CT-DBS in promoting behavioral responsiveness and functional outcome in patients diagnosed with chronic MCS.
• To identify clinical and neurophysiologic predictors of response to CT-DBS
• To determine the relationship between behavioral, electrophysiologic and functional neuroimaging changes associated with CT-DBS.
Inclusion Criteria
• TBI• Medically stable• Meet diagnostic criteria for MCS• Inconsistent command-following,
verbalization or communication• > 12 months post-injury• Recovery plateaued• Age 18-55• Legal surrogate available for consent

Exclusion Criteria
• No large infarcts (> 50 cc’s) involving Broca’s or Wernicke’s areas
• No paramedian mesodiencephalic infarct• No co-morbid condition w/ life expectancy <
5 years• No contraindication for general anesthesia,
craniotomy or travel by air or train• No quadriparesis

Primary Outcome Measure:Coma Recovery Scale- Revised
Frequency of best score on selected subscales of the Coma Recovery Scale- Revised
(Giacino, et al, 1991, 2004)

• Arousal• Expressive speech• Purposeful limb movement• Dysphagia
Secondary Outcome Measures

Study Phases
Pre-operative Baseline Evaluation
• ~ 1 month duration • Standard rehabilitation provided• CRS-R assessments and other
secondary assessments• Primary outcome variable(s)
selected Inpatient Stay/ DBS Implant
• ~7-10 days• DBS implantation surgery• Post operative physiological
studies/fMRI• Externalized stimulation
programmingPost-operative Baseline Assessment
• 1 month duration• DBS OFF• Standard rehabilitation continues• Serial CRS-R and other secondary
neuropsychological assessments continue
DBS Stimulation Titration & Recovery
• 2 week stimulation titration• Optimize stimulation parameters• 2 week wash-out• Continue standard rehabilitation
program• Serial CRS-R and other secondary
neuropsychological assessments continue Double-blind, Cross-over
Intervention• 6 month duration• Randomized to monthly ON/OFF
sequences• Continue standard rehabilitation
program• Serial CRS-R and secondary
neuropsychological assessments continue
Open-Label Follow-up• Through 24 months post-
implantation• DBS stimulation and
rehabilitation as indicated• Continued safety monitoring

Patient 1
• 33 y/o RH male• Injury: Blunt head trauma following assault resulting in b/l SDH
(R>L)– Initial GCS=3– VS to MCS in mth 2-3
• Course: 2 yrs inpatient rehab + 4 yrs nursing home– Total care required, Unable to communicate with family/staff
• Clinical status on re-admission (6.5 yrs post-injury): – Inconsistent command-following– Nonverbal except for rare single-word verbalization – Unable to communicate reliably (yes/no)– Unable to use common objects– Diagnosis: MCS– MRI: R frontal encephalomalacia + small R paramedian
thalamic infarct (2ndary to central herniation)

100
85
75
65
55
45
35
Co-registrationFDG-PET/MRI

T2*-Weighted MRI w/ Co-registered fMRI
FORWARD BACKWARD OVERLAP

20
Electrode placement

ILN DBS PatientPatient 1: Electrode placement

Results
0
100
200
300
400
500
600
700
800
900
-309
-296
-283
-270
-257
-244
-231
-218
-205
-192
-179
-166
-153
-140
-127
-114
-101 -88
-75
-62
-49
-36
-23
-10
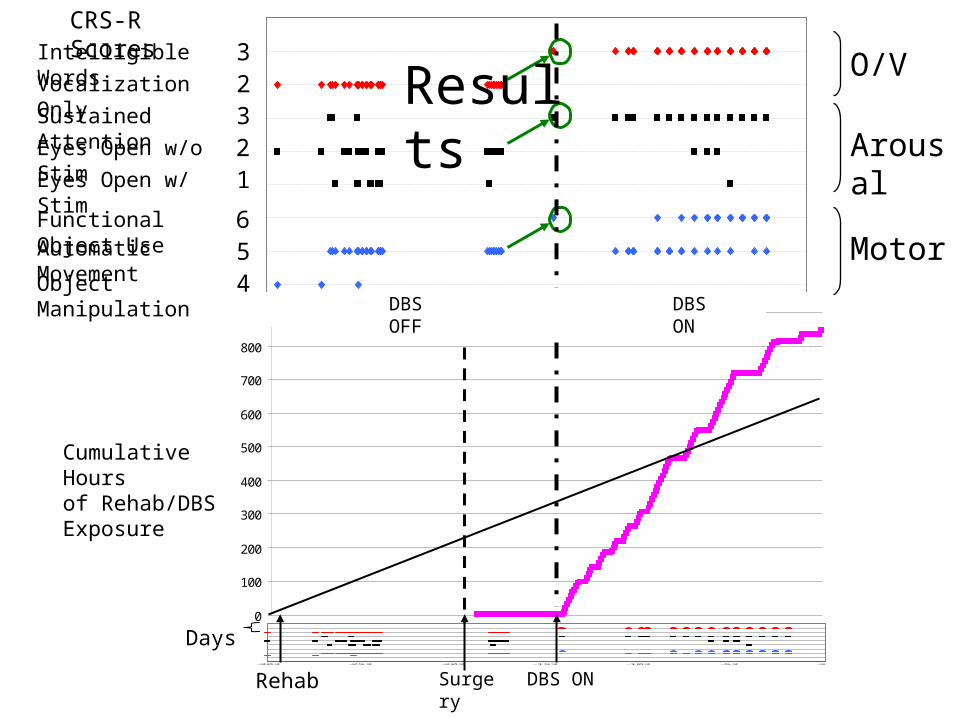
Cumulative Hours of Rehab/DBS Exposure
Days
Rehab
23
123
456
Surgery
Intelligible Words
-303 -253 -203 -153 -103 -53 -3
DBS ON
Vocalization OnlySustained AttentionEyes Open w/o StimEyes Open w/ Stim
Functional Object Use
Object Manipulation
Automatic Movement
CRS-R Scores
DBS ONDBS OFF
Results O/V
Arousal
Motor

Behavioral Performance: Pre-DBS v. DBS On v. DBS Off

Conclusions
• Results support DBS modulation of specific cognitive and behavioral functions (arousal, functional limb movement, swallowing).– Target behaviors occur more frequently with DBS on.
• Some evidence of DBS carryover effects (speech)• Mechanism of effect:
– CL co-activates with anterior cingulate and SMA– Mesial frontal circuit (incl. cingulate/SMA) mediates
response preparedness, motor intention and drive functions.

Implications
• DBS may be able to be linked to cognitive rehabilitation and/or pharmacologic interventions– Augment existing treatment strategies by
supporting neuronal mechanisms.– Improve attentional and intentional functions• Working memory, selective attention, initiation,
planning, execution, self-monitoring, spatial awareness.
– Restore functional capacity/independence.

Non-functional communication
MCS EMCS pI-ADL I-ADL
Functional communication
Partial Independence
Independent
Cognitiveslowing
I-Work I-SchoolI-Social
Severe disability
Therapeutic aims for cognitively-based DBS
following TBI Moderate disability
Mild disability
Impaired NoParticipation Impairment

Study Aims
1.To establish the feasibility of targeting and activating central thalamic fiber projections (central lateral and parafascicular nuclei) carrying brainstem arousal afferents en route to downstream cortical fields.
2.To determine the effects of CT-DBS on executive functions in persons with persistent disability lasting ≥ 24 months after moderate-severe TBI.
3.To determine whether exposure to CT-DBS is associated with improvements in vocational productivity, social participation, self-reported psychological health and quality of life.
4.To establish the safety profile of CT-DBS when administered to survivors of moderate-severe TBI in the chronic phase of recovery.

Research Team/Supporting Agencies (DBS TBI I: MCS)
Weill - Cornell JFK Medical Center Cleveland Clinic
Nicholas Schiff, MD (PI) Joseph T. Giacino, PhD (PI) Ali Rezai, MD (PI)Joseph Fins, MD Kathleen Kalmar, PhD Andre Machado, MD, PhDJonathan Victor, MD, PhD Caroline McCagg, MD Ken Baker, PhD
Erik Kobylarz, MD, PhD Jeanne O’Connor, PA-C Cindy Kubu, PhDMary Conte, PhD Brian Fritz, PhD Sierra Farris, PA-CJennifer Hersh, MA Mindy Gerber, MA, CCC-SLP Chris Butson, PhDFred Plum, MD Kathleen Donahue, OTR Cameron McIntyre, PhD
Beth Isenberg, CTRSTraci Biondi, OTR
Supported in part by:
National Institute of Health- National Center for Medical Rehabilitation Research: R21HD40987:“Multidisciplinary assessment of severe brain injury.”Charles A. Dana FoundationFood and Drug Administration: IDE # G030240 (for Kinetra Neurostimulator)Cleveland Clinic Foundation Brain Neuromodulation CenterOhio Department of Development BRTT and Third Frontier programJane and Lee Seidman Neuromodulation Research FundCleveland Clinic Innovations, IntElect Medical, Inc.

• Weill-Cornell Medical College– Nicholas Schiff, MD (PI)– Joseph Fins, MD– Jonathan Baker, PhD– Sudhin Shah, MD
• Spaulding Rehabilitation Hospital– Joseph Giacino, PhD (PI)– Sabrina Taylor, PhD
Research Team (DBS TBI II Severe TBI)
• Stanford University– Jaimie Henderson, PhD (PI)– Stephanie Kolakowsky-
Hayner, PhD
• Cleveland Clinic– Andre Machado, MD, PhD
• University of Utah– Chris Butson, PhD– Guido Gerig, PhD