your first patient of the day - brad sobolewski · your first patient of the day ... • lp –can...
TRANSCRIPT

Your first patient of the day
• 1 month old male with 2 days of fussiness
• Decreased stool output for 3 days
• Poor latch during breastfeeding noted at 3AM on day of arrival to the ED
• Started ‘spitting up’ later in the morning
• Was noted to be less alert as well
• Soft spot was ‘hollow’
• He was also ‘breathing real fast’
• He was making a grunting noise which the parents thought was due to him trying to poop

The details
• Birth and past medical history
– G1P1
– Birth weight 8 pounds 5 ounces
– C-section for failure to progress at 41 weeks
– No complications during pregnancy
• GBS and other labs negative
• Maternal health Hx negative
– Unconjugated hyperbilirubinemia required
phototherapy on DOL3
– Regained birth weight by DOL 7

You enter the room
• The infant’s skin is this color
• You suddenly turn this color

First impressions
• ABCDE’s
– He has an airway
– He is breathing fast and making a grunting noise
– He’s skin is a lovely shade of grayish purple
– He appears uncomfortable

Your physical exam
• VS HR205 BP90/65 RR50 T38.8
• GEN grunting, gray skin
• HEENT AF sunken, mmm, + tears
• CV rate >200, no murmurs, 1+ femoral and brachial pulses, cap refill 5 seconds
• PULM tachypneic, CTAB
• ABD firm and distended, tender, no masses, normally positioned anus
• GU nl male
• NEURO irritable, nl tone

One sick baby
• What are his
problems?
• What do you think is
going on?
• What do we need to
do about it?
Goals
• Discuss fever of uncertain source in infants 0 to 60 days
• Focus on the Emergency Department setting
– Clinical assessment
– Diagnostic evaluation
– Treatment strategy
• Discuss use of CCHMC Evidence Based Guidelines

Fever of uncertain source
• FUS is an acute febrile illness with
uncertain etiology after thorough H&P
– No focal infection (eg. otitis media)
• The prevalence of a serious bacterial
infection (SBI) in infants with fever is high
• Clinical exam alone is unable to reliably
predict presence of SBI
Etiology
• SBI include;
– Meningitis, bone and joint infections, soft tissue infections, pneumonia, UTI, sepsis/bacteremia, enteritis
• Most common causes of FUS
#1 systemic viral infections
#2 urinary tract infections
#3 upper and lower respiratory tracts
#4 middle ear

Etiology
• Prevalence is uncertain in the post Hib,
post prevnar era
• <1 month – 8.8-13.7% according to
Bachur, 2001, Kadish, 2001, Baker, 1999
• 1-2 months 5 to 8.7%
• CCHMC data
– <1 month 9%
– 1-2 months 8%

The villains
• Bacteria (Baker, 1999) – E. coli 39%
– Klebsiella 11%
– Group B strep 8%
– Enterococcus 6%
– E. cloacae 6%
– L. monocytogenes 6%
• Viruses – Up to 50% of infants between
Aug-Oct w/ FUS have enterovirus
– HHV-6 in 10% <90 days old
– HSV incidence is 30/100,000, of these only 7-14% present with FUS

Clinical assessment - Fever
• Rectal temperature!
– >38oC or 100.4oF
• Magnitude may not
predict severity
• How accurate is parental
report of fever felt by
touch alone?
– Answer: pretty darn good!
• Sens 82-89%
• Spec 76-86%

Clinical assessment - History
• Low risk for SBI – Rochester criteria – Term birth >37 weeks
– No previous hospitalizations
– No chronic illnesses
– Not hospitalized longer than mother
– Not treated for unexplained hyperbili
– Has not recived antibiotics
– No intrapartum maternal fever, GBS, antibiotics
– No focal bacterial infection on exam • Purulent otitis, skin/soft tissue infection, bone/joint infection
– Negative lab screen

Clinical assessment - Exam
• High risk findings include – Lethargy
– Poor or absent eye contact
– Failure of child to recognize parents, or failure to interact with persons/objects in the environment
– Poor perfusion of the extremities
– Acrocyanosis
– Mottling
– Cap refill >2 seconds in warm ambient environment
– Hyper/hypoventilation
– cyanosis
Per Yale Observation scale <24 months of age
My advice
Be thorough!

Clinical assessment - Exam
• The ‘toxic’ infant
– Lethargy
– Poor perfusion
– Hypo/Hyperventilation
– Cyanosis

Clinical assessment - Labs
• CBC
– Abnormal wbc >15,000 or <5,000
– Bands >1,500
– Note: wbc values do not predict risk of meningitis (Bonsu, 2003)
• Blood Culture
One Unit, Two
Units…
Ah, Ah, Ahhh
Clinical assessment - Labs
• Urinalysis
– Abnormal >10wbc/hpf
– Gram stain for bacteria • Sens 94%
• Spec 92%
• Urine culture
– Catheter! (bagged specimens are useless)
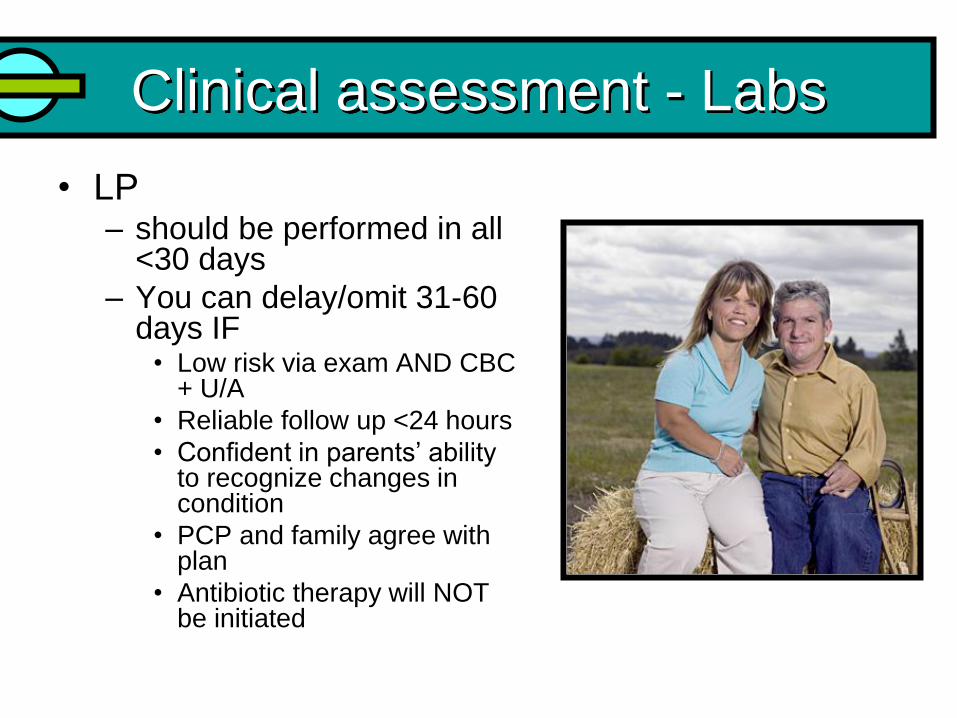
Clinical assessment - Labs
• LP – should be performed in all
<30 days
– You can delay/omit 31-60 days IF
• Low risk via exam AND CBC + U/A
• Reliable follow up <24 hours
• Confident in parents’ ability to recognize changes in condition
• PCP and family agree with plan
• Antibiotic therapy will NOT be initiated

Clinical assessment - Labs
• LP
– Can be performed lying on side or upright
– Most CCHMC MDs and holders prefer upright
– Better success after local infiltration of
anesthetic, and with early stylet removal
– Even if you get a bloody tap still initiate
antibiotic therapy

Clinical assessment - Labs
• CSF studies – Tube 1 – protein and glucose
– Tube 2 – culture and gram stain
– Tube 3 – cell count and differential
– Tube 4 (Wasserman) – extra culture, hold
• Normal values for blood and urine do not rule out meningitis
• Enteroviral meningitis can have a CSF wbc of >1000! – Look for predominance of segs in a high wbc/hpf in bacterial
meningitis
• ‘Normal’ CSF values vary – Boston protocol <10 wbc/hpf
– Philadelphia protocol <8 wbc/hpf
– Rochester criteria <5 wbc/hpf

Cultures
• Try to obtain before giving antibiotics
– Don’t withhold if infant is septic/in shock
• Cultures should be watched for 36 hours at minimum
– Mean time to true positivity for B/C = 17.5 hours
– For blood contaminants = 27.9 hours
– Urine Cx = 16 hours
– CSF Cx = 18 hours

Other adjunctive studies
• Chest XRay
• Stool culture if diarrhea
• Viral studies (+ PCR does NOT rule out SBI)
– Enterovirus PCR of CSF (summer and fall) • Results available in 24 hours
– PCR is more sensitive than viral culture
– HHV-6 PCR
– HSV PCR of CSF (more on HSV later)

Treatment
• Supportive care
– ABCs
– O2 if sats <90%
– Fluid resuscitation w/ NS • Generally 20ml/kg, by if
you suspect heart failure, 10ml/kg may be appropriate
• And, oh yeah… ANTIBIOTICS!

Treatment
• Antibiotics in ALL infants less than 30 days w/ FUS
• NNT with ampicillin to prevent one case of Listeria or enterococcus is 138
AMPICILLIN 50mg/kg IV q6h
q12h <7days old
3rd generation cephalosporin
CEFOTAXIME 50mg/kg IV q8h
q8h bacteremia, q6h meningitis
GENTAMICIN 3mg/kg IV q24h 31-60d - 2.5mg/kg q12h
OR +
If you highly suspect Staph you can
use NAFCILLIN 20-50mg/kg IV q6h
instead of AMPICILLIN

Treatment
• 31-60 days - 3rd generation cephalosporin alone
• If infant is severely ill or UTI suspected add AMPICILLIN
– Listeria, gram + cocci, enterococcus (NNT= 527)
• Don’t give Ceftriaxone if…
– hyperbilirubinemic - since can displace bilirubin from its binding sites
– concurrent administration with intravenous calcium-containing solutions or products (including TPN) – causes potentially fatal precipitation reactions
3rd generation cephalosporin
CEFOTAXIME 50mg/kg IV q8h
q8h bacteremia, q6h meningitis
3rd generation cephalosporin
CEFTRIAXONE 50mg/kg IV q24h for bacteremia
100mg/kg IV q24h for meningitis
OR

Herpes
• What about Herpes?
– Laboratory evaluation
and/or treatment
should be considered
if risk factors are
present

Herpes
• Presentation of infants with neonatal HSV
– 7-14% have FUS
– 61% have no fever
– 95-98% present prior to 22 days of age
– 68% present with a vesicular rash on either the skin or mucous membranes
– 27% have seizures
• Overall incidence of HSV infection is 30/100,000 live births

Which one is due to HSV?
Answer: This is a trick question – neither are.
They are both examples of candidal diaper
dermatitis, which can look like HSV



Herpes
• Highest Risk – Primary maternal HSV infection at delivery
• 2/3 mothers who acquire HSV during pregnancy are symptom free
• Lower Risk Factors – Known exposure to HSV infected persons
• Caregiver with oral/genital herpes
– <37 weeks gestational age
– Fetal scalp electrodes
– Maternal STD Hx or unexplained fever at delivery
– CSF pleocytosis with negative gram stain and negative bact Cx
– Failure of fever to abate within 24-48 hours after starting ABx
– Unexplained CNS signs

Treatment - HSV
• Treatment
• Additional labs/studies recommended – Renal + glucose
– Liver panel
– Head CT
– CSF HSV PCR
– enterococcus PCR (if in season)
– Viral cultures • CSF
• Skin lesions
• Conjunctivae
• NP swab
• Rectal swab
ACYCLOVIR 20mg/kg IV q8h

Treatment - HSV
• The bottom line – treat if… – Mom had HSV at delivery, or infant has been
exposed
– The baby seizes or has worrisome neurologic signs
– There is clinical evidence to suggest that HSV is present
Routine treatment
with Acyclovir is
NOT recommended

Disposition
• <30 days definitely buys you an admission
– Approximately 3% of infants that are ‘low risk’ STILL have SBI
• 31-60 days can be managed at home or inpatient
• Low-risk infants 31-60 days can be D/C home IF
– Baby meets all history and exam findings for ‘LOW RISK’
– Negative labs (LP not necessarily needed)
– They have excellent follow up <24 hours – CALL THE PMD!
– Parents are comfortable
– You can admit without antibiotics if labs are negative but parents are uncomfortable or follow up is lacking
– Some MDs may wish to give IM/IV CEFTRIAXONE and D/C home • If you give antibiotics you SHOULD do an LP too
• Consider PICU or RCNIC if…
– Shock
– Bacterial meningitis suspected

When you are at CCHMC
• In EmSTAT click on the orders tab

Choose the Fever/Sepsis set from the list of ‘Standard Order Panels’
It will take you to a screen
where you can order all of
the requisite labs

Then click
to order the appropriate
antibiotics
Choosing these orders is most appropriate for a 0-30 day old with FUS

Evidence based guidelines
• You can always access the guidelines
You’ll find the guidelines on the Pediatric
Residents tab on CenterLink while
working at CCHMC
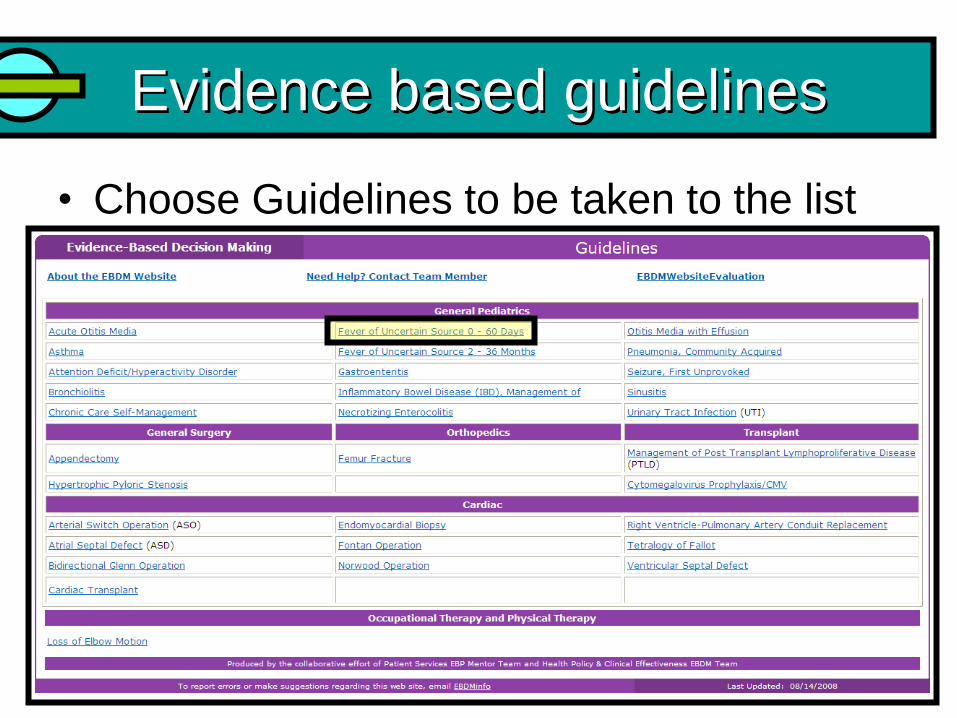
Evidence based guidelines
• Choose Guidelines to be taken to the list

Evidence based guidelines
• You can download the pdfs
• When away from CCHMC you can still
access the guidelines
– http://www.cincinnatichildrens.org/svc/alpha/h/
health-policy/ev-based/default.htm
• You can also search for Evidence Based
Care Guidelines after directing your
browser of choice to cincinnatichildrens.org
Case #1
• 3 week old former 39
week infant with temp of
38.4, feeding well, no
respiratory distress,
excellent perfusion
– Labs?
– Antibiotics?
– Disposition?

Case #2
• 5 week old former 35 week old infant
• Fever to 100.7oF rectally at home
• Looks well in the ED
• Can we apply the CCHMC guidelines to this infant?

Case #3
• You are seeing a 7 week old girl at Clinton Memorial
• Former 39 week infant
• Fever to 102 at home for 2 days
• Feeding well
• Crying but consolable
• Defervesces with Tylenol
• Visiting family in Ohio – they live in Chicago
• What are you going to do?

Back to our first patient
• He was clearly quite sick
• We obtained
– CBC, B/C
– U/A, U/C
– CSF labs
– Serum glucose
• We also elected to get
– XRays
– I-STAT
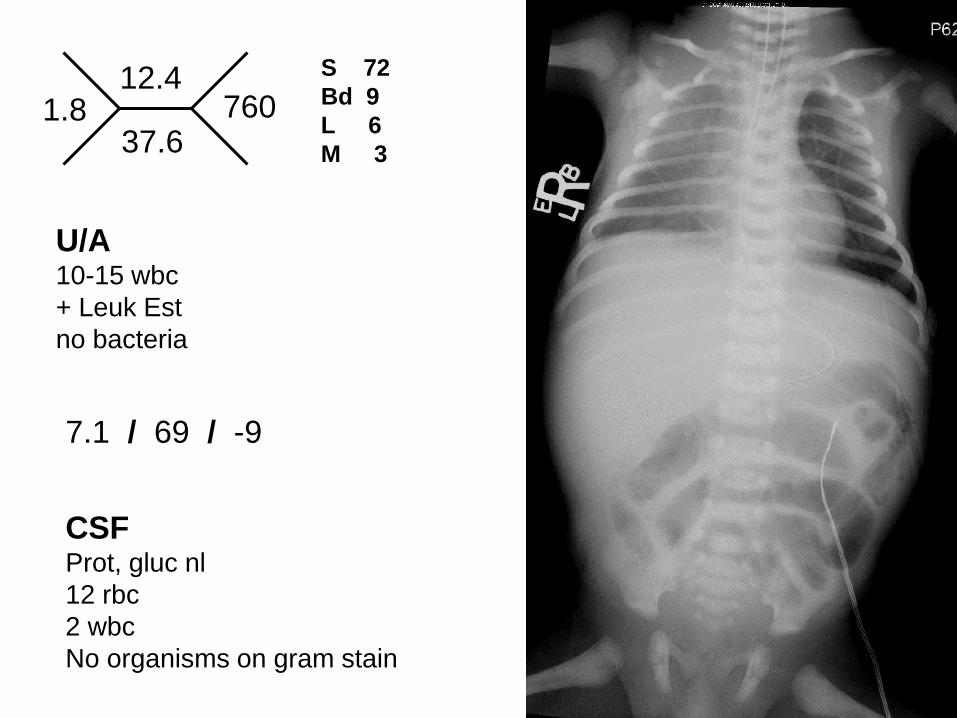
S 72
Bd 9
L 6
M 3
12.4
37.6 760 1.8
7.1 / 69 / -9
U/A 10-15 wbc
+ Leuk Est
no bacteria
CSF Prot, gluc nl
12 rbc
2 wbc
No organisms on gram stain

Back to our first patient
• He was started on Ampicillin and Cefotaxime
• He was intubated for worsening respiratory distress
• Resuscitated w/ 60ml/kg NS – though MAPs still in 50’s started on Dopamine for perfusion
• Admitted to the RCNIC
• Cultures grew E. coli in blood and urine – Dx E. coli urosepsis
• Developed a protracted septic ileus
• D/C after 27 days in the ICU – returned to breast feeding and doing well

Take home point #1
• FUS is an acute febrile illness with uncertain etiology after thorough H&P – Rectal temperature!
– >38oC or 100.4oF
• Clinical exam alone cannot reliably predict presence or absence of SBI – The ‘toxic’ infant
• Lethargy
• Poor perfusion
• Hypo/Hyperventilation
• Cyanosis

Take home point #2
• 30 days or less and FUS
– Blood, Urine, and CSF studies
– Ampiciliin + Cefotaxime OR Gentamicin
– Admission
Remember, bagged
specimens are
USELESS!
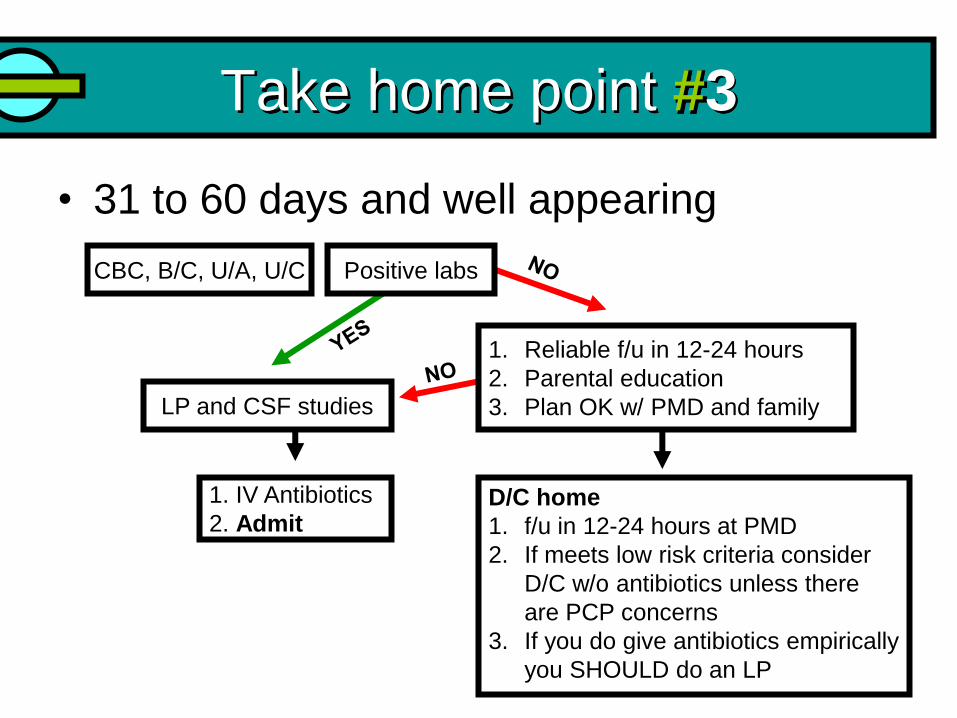
Take home point #3
• 31 to 60 days and well appearing
CBC, B/C, U/A, U/C Positive labs
1. Reliable f/u in 12-24 hours
2. Parental education
3. Plan OK w/ PMD and family
1. IV Antibiotics
2. Admit
LP and CSF studies
D/C home
1. f/u in 12-24 hours at PMD
2. If meets low risk criteria consider
D/C w/o antibiotics unless there
are PCP concerns
3. If you do give antibiotics empirically
you SHOULD do an LP

Take home point #4
• HSV – Mom had HSV at delivery, or infant has been
exposed
– The baby seizes or has worrisome neurologic signs
– There is clinical evidence to suggest that HSV is
present
• Treat with Acyclovir – Don’t forget adjunctive labs
Take home point #5
• The CCHMC Evidence based Guidelines
are a Great Resource
• Familiarize yourself with them before your
rotation
• pdfs are always available on the web
– http://www.cincinnatichildrens.org/svc/alpha/h/
health-policy/ev-based/default.htm