yi shiau ng, convegno mitocon 2015
TRANSCRIPT

5th National Meeting for Mitochondrial Medicine, Bologna
Epidemiology of Mitochondrial Disease in The UK and The Development of A UK Cohort of Patients
with Mitochondrial Disease
Dr Yi Shiau NgClinical Research Associate
Newcastle University


Content
• Epidemiology of adult mitochondrial disease in the North East England
• Development of the UK Mitochondrial Disease Patient Cohort
• Utilization of cohort data
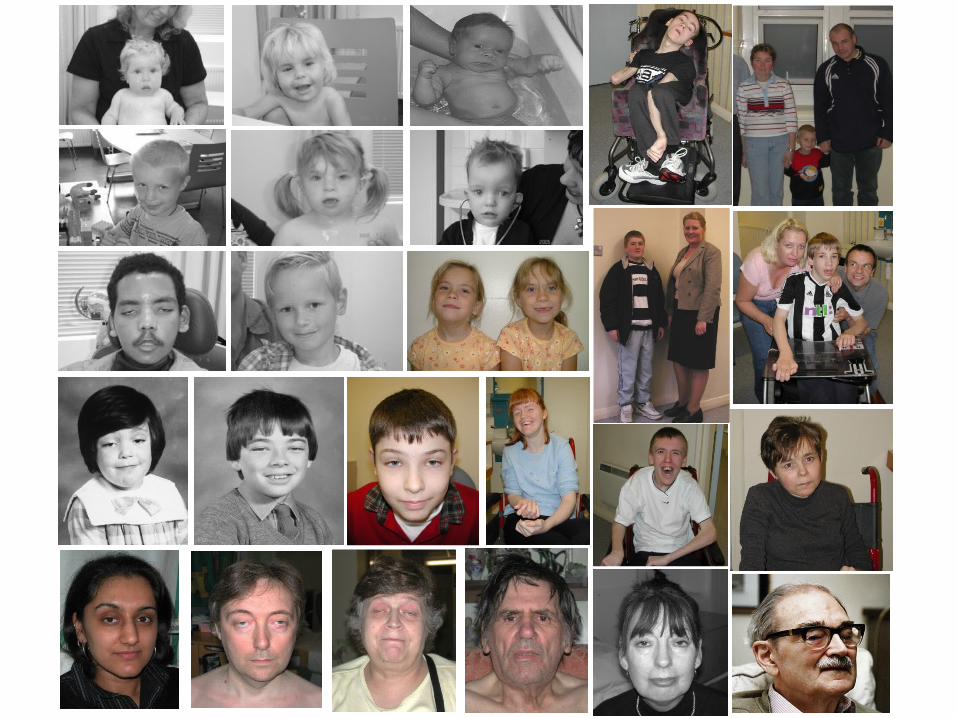
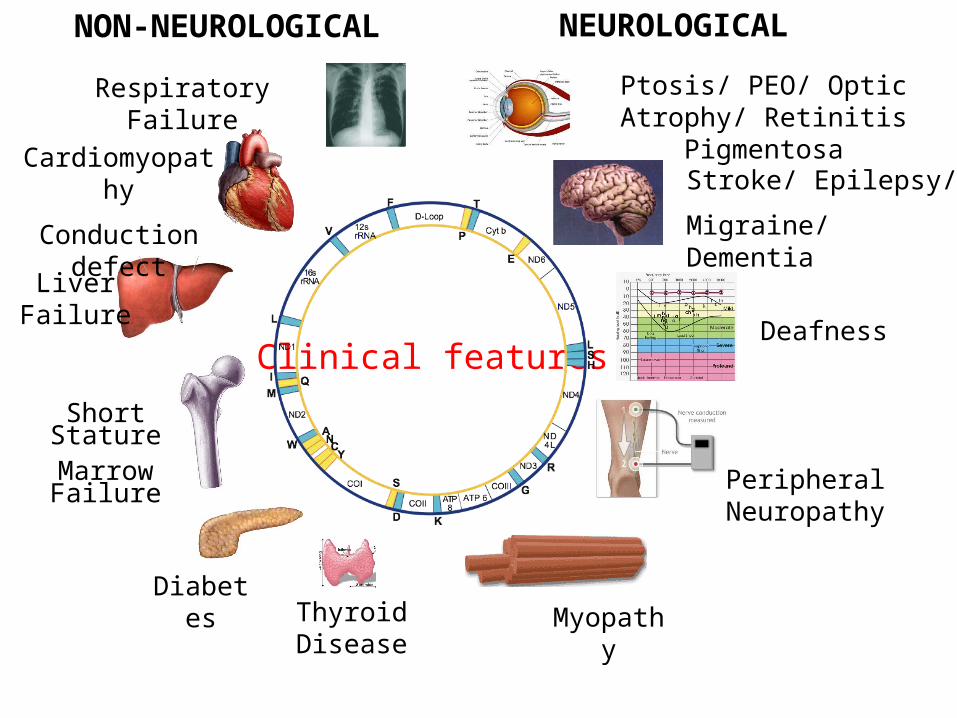
DiabetesThyroid Disease
Myopathy
Peripheral Neuropathy
Deafness
Stroke/ Epilepsy/
Migraine/ Dementia
Respiratory Failure Ptosis/ PEO/ Optic Atrophy/ Retinitis Pigmentosa
Cardiomyopathy
Conduction defect
Short StatureMarrow Failure
Liver Failure
NEUROLOGICALNON-NEUROLOGICAL
Clinical features

North East England
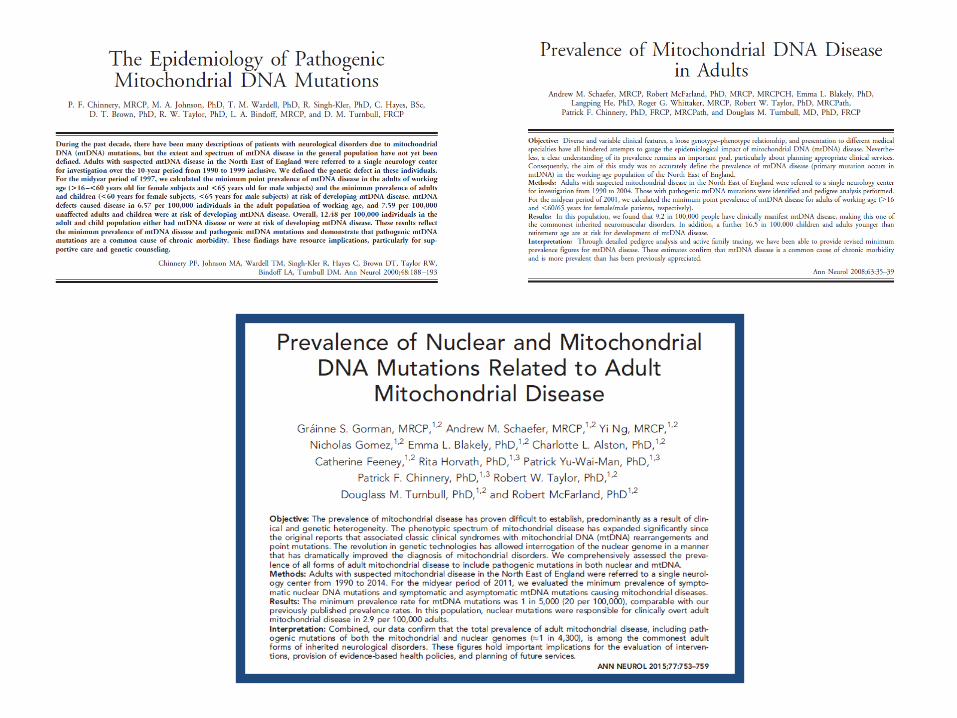
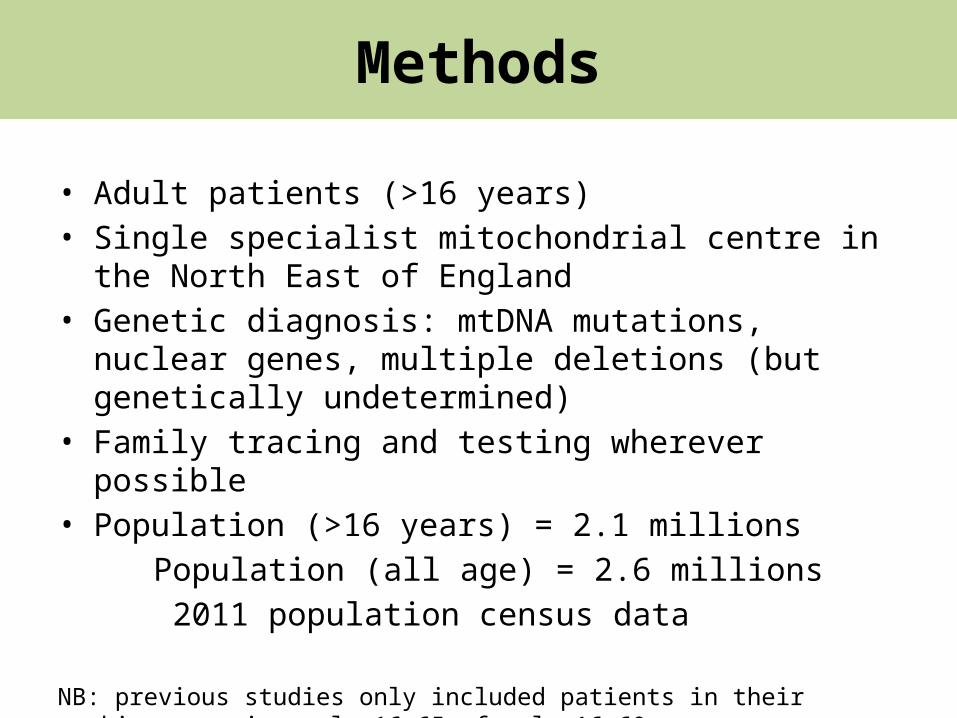
• Adult patients (>16 years)• Single specialist mitochondrial centre in the North East of
England• Genetic diagnosis: mtDNA mutations, nuclear genes, multiple
deletions (but genetically undetermined)• Family tracing and testing wherever possible• Population (>16 years) = 2.1 millions Population (all age) = 2.6 millions 2011 population census data
NB: previous studies only included patients in their working age, ie. male 16-65; female 16-60
Methods
Inclusion• CPEO• Ataxia• Seizure/ myoclonus• Stroke-like episode• Proximal myopathy• Exercise intolerance• Cardiomyopathy• Optic atrophy• Pigmentary retinopathy• Bilateral Deafness• Diabetes
Exclusion • Myalgia• Fatigue• Migraine• Dysphagia• Gastrointestinal upset• Cataracts
The Definition of Clinically Manifesting Mitochondrial Disease

mtDNA mutations
Disease= 9.6/100,000- m.3243A>G- Three LHON mutations (m.11778G>A, m.3460G>A & m.14484T>C)- Single, large scale deletion- m.8344A>G- 8 other point mutations
At risk= 10.7/100,000* All single deletion cases were sporadic in the cohort
Nuclear genes
Disease= 2.9/100,000- SPG7 (ar)- PEO1 (ad)- OPA1 (ad)- POLG (ar)- RRM2B (ad)- 4 other nuclear genes- Multiple deletions
At risk= 5.9/100,000* Heterogenous nature of inheritance patterns
Total prevalence = (9.6+ 10.7+ 2.9)/100,000 1 in 4300
Content
• Epidemiology of adult mitochondrial disease in the North East England
• Development of the UK Mitochondrial Disease Patient Cohort
• Utilization of cohort data
Unmet Clinical Research Need
1.Lack of natural history data2.No meaningful clinical trials3.No evidence-based guidelines
Why develop a Mitochondrial Disease Patient Cohort?

Three Nationally Commissioned Mitochondrial Service
Dr V Nesbitt
Dr R Pitceathly
Julie Phipps
Mitochondrial Disease Patient Cohort
• Initiated in 2009
• New ethics approval in England (01/2014) and Scotland (03/2014)
• Diagnosis of Mitochondrial Disease– Genetic or Biochemical
• Children and Adults – no age limits– Including those with limited capacity for consent
• Living patients
Inclusion Criteria
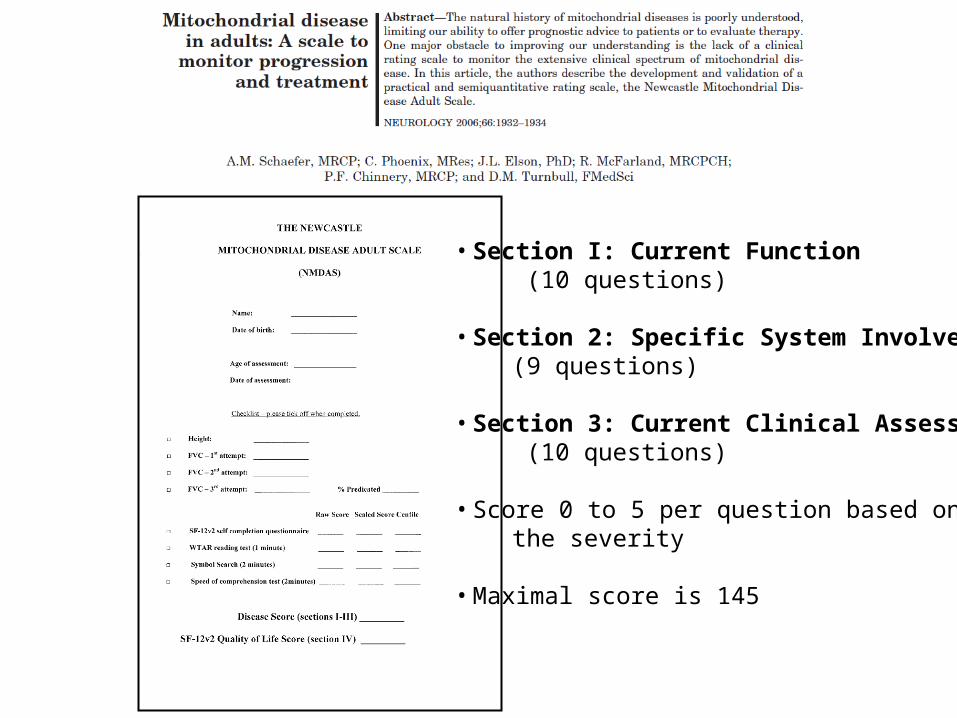
• Section I: Current Function (10 questions)
• Section 2: Specific System Involvement (9 questions)
• Section 3: Current Clinical Assessment (10 questions)
• Score 0 to 5 per question based on the severity
• Maximal score is 145
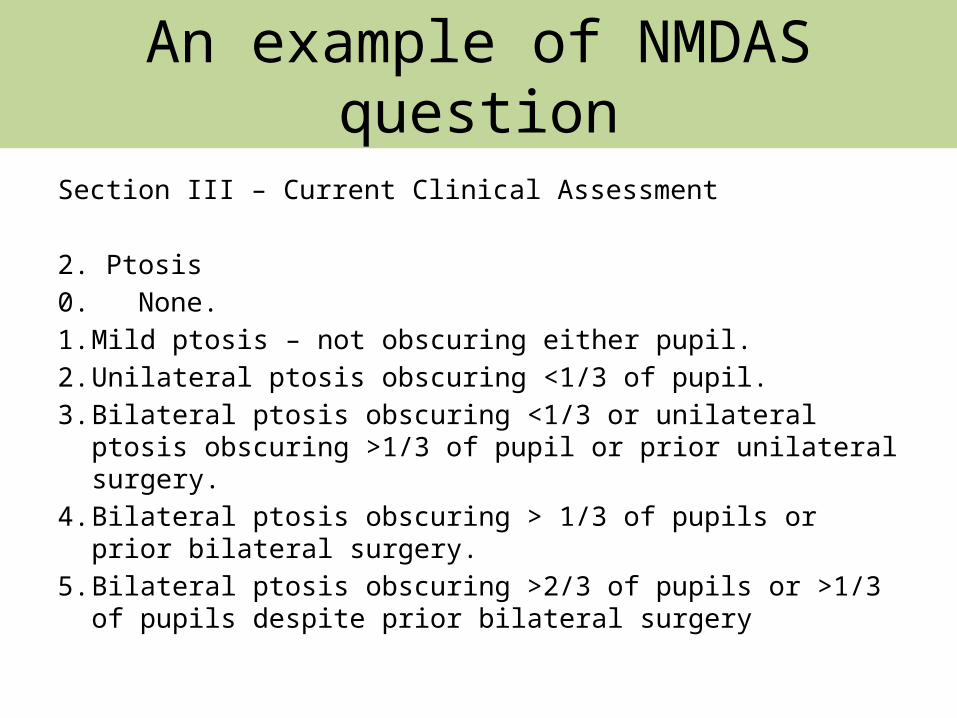
An example of NMDAS question
Section III – Current Clinical Assessment
2. Ptosis0. None.1. Mild ptosis – not obscuring either pupil.2. Unilateral ptosis obscuring <1/3 of pupil.3. Bilateral ptosis obscuring <1/3 or unilateral ptosis obscuring
>1/3 of pupil or prior unilateral surgery.4. Bilateral ptosis obscuring > 1/3 of pupils or prior bilateral
surgery.5. Bilateral ptosis obscuring >2/3 of pupils or >1/3 of pupils despite
prior bilateral surgery

Ptosis
Single, large scale deletion of mtDNA
POLG gene mutation PEO1 (Twinkle) gene mutation
Single, large scale deletion of mtDNA
m.3243A>G mutation(deceased)
m.8344A>G mutation



Geographical Distribution of All Cohort Patients(n=1218)
Newcastle56%
London32%
Oxford 6%
Others5%
Figure. Patient recruitment
Last updated on 6/5/2015

Newcastle Patient Cohort
• 689 patients recruited
• 6.6% = deceased during follow up (n=45)
• 87% of patients >16 years
• 63% = Female (n=404)
9075604530150
90
80
70
60
50
40
30
20
10
0
Age
Fre
quency
Mean 45.30StDev 18.63N 638
Figure. Age of patients from Newcastle cohort
Last updated on 6/5/2015

m.3243A>G32%
m.8344A>G6%
m.8993T>C/G2%
Other mtDNA point mutations11%
Single dele-tion15%
PEO16%
POLG6%
RRM2B3%
OPA13%
Other nuclear genes
5%
Multiple dele-tions6%
Other genetically undetermined6%
Genotypes in Newcastle patient cohort (n=689)
Last updated on 6/5/2015
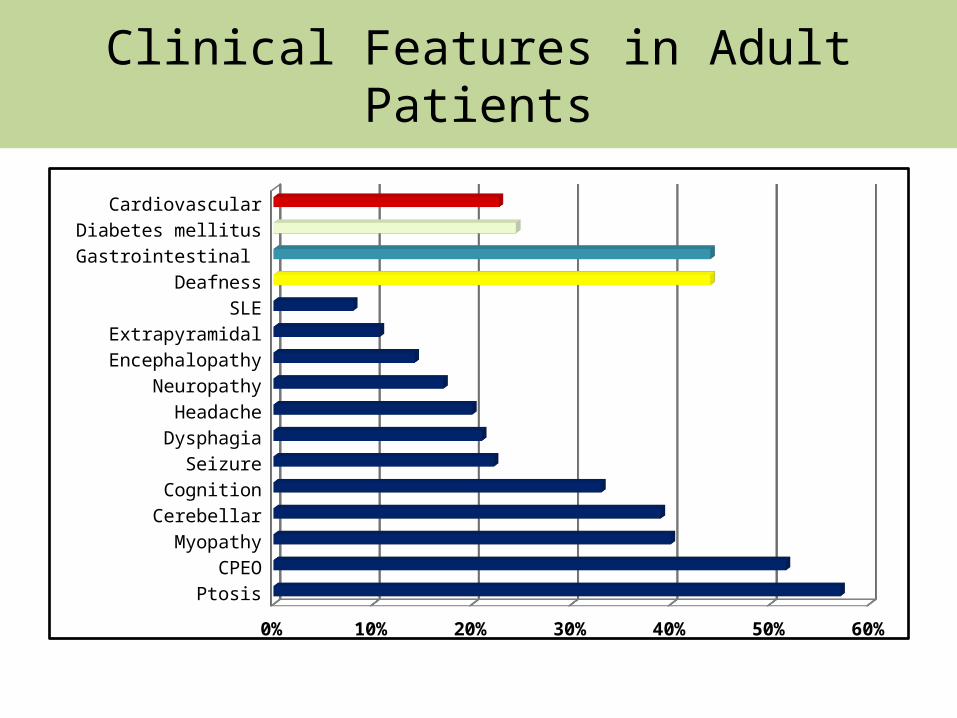
Clinical Features in Adult Patients
PtosisCPEO
MyopathyCerebellarCognition
SeizureDysphagiaHeadache
NeuropathyEncephalopathyExtrapyramidal
SLEDeafness
Gastrointestinal Diabetes mellitus
Cardiovascular
0% 10% 20% 30% 40% 50% 60%

Disease Burden defined by NMDAS
TWINKLE (PEO1)Single deletionRRM2BPOLG1m.8344A>Gm.3243A>G
100
80
60
40
20
0
Genotype
NM
DA
S s
core
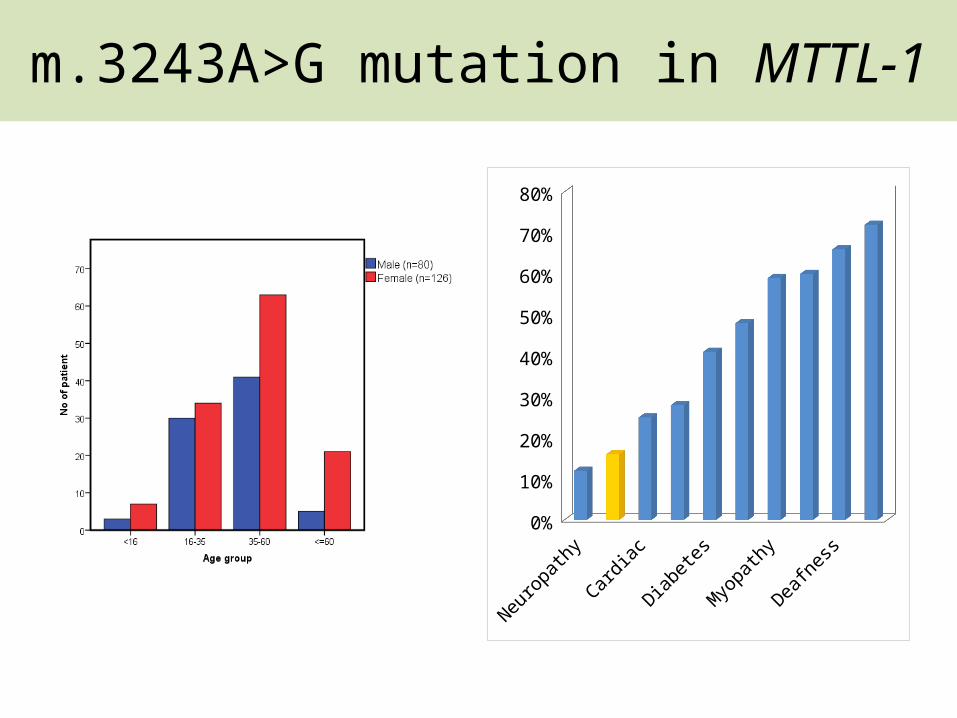
m.3243A>G mutation in MTTL-1
Neuropathy
Stroke-lik
e episode
Cardiac
CPEO
Diabetes
Exerci
se intolerance
Myopathy
Migraine
Deafness GI0%
10%
20%
30%
40%
50%
60%
70%
80%

Evolution of stroke-like episode
16/12/2010 24/04/2012
DWI
01/03/2013
DWI
02/07/2014 02/01/2015
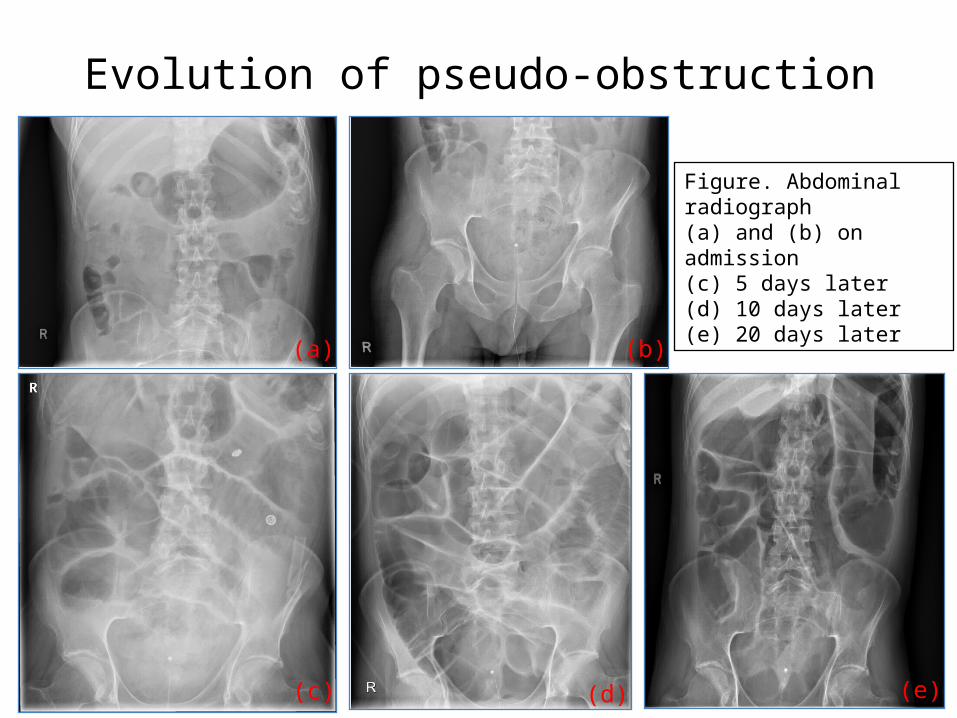
Evolution of pseudo-obstruction
(a)
(c) (d)
(b)
(e)
Figure. Abdominal radiograph(a) and (b) on admission(c) 5 days later(d) 10 days later (e) 20 days later
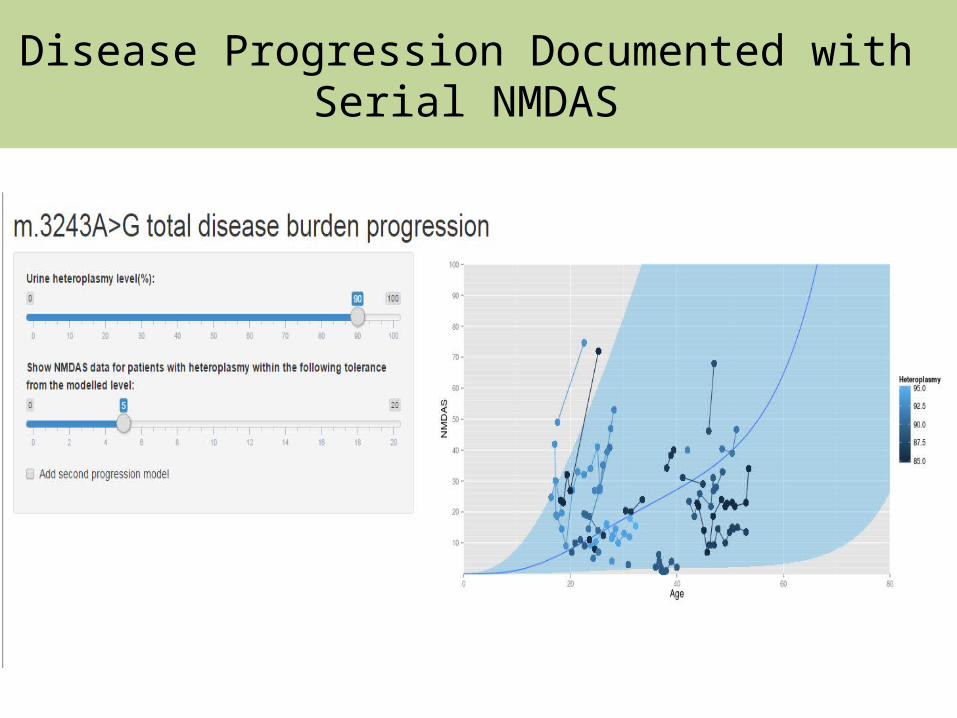
Disease Progression Documented with Serial NMDAS
Content
• Epidemiology of adult mitochondrial disease in the North East England
• Development of the UK Mitochondrial Disease Patient Cohort
• Utilization of cohort data
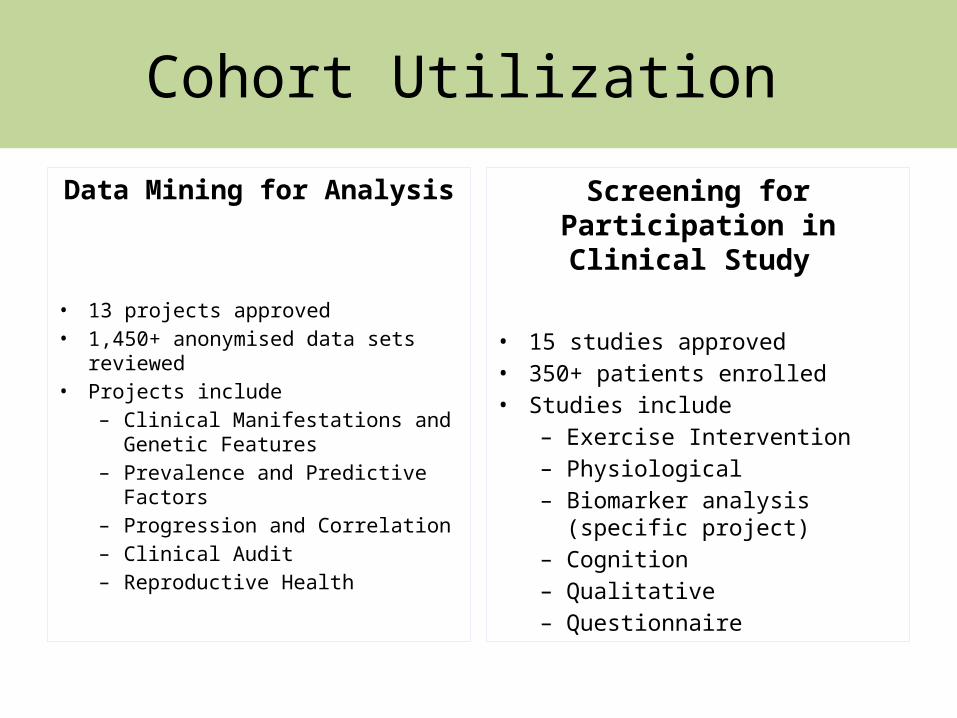
Cohort Utilization
Data Mining for Analysis
• 13 projects approved • 1,450+ anonymised data sets
reviewed • Projects include
– Clinical Manifestations and Genetic Features
– Prevalence and Predictive Factors – Progression and Correlation– Clinical Audit – Reproductive Health
Screening for Participation in Clinical Study
• 15 studies approved • 350+ patients enrolled • Studies include
– Exercise Intervention– Physiological– Biomarker analysis (specific
project) – Cognition– Qualitative – Questionnaire

Cardiac Involvement in the Mito Cohort (Newcastle)
• 18% (n=78)
• It is more prevalent in mtDNA mutations than common nuclear genes.
Genotype Prevalence
m.3243A>G 25%
m.8344A>G 26%
Single deletion 15%
POLG 1/21
PEO1 0
RRM2B 1/15

Types of Cardiac Involvement
m.3243A>G
m.8344A>G
Other mtD
NA
Single
deletion
POLG
RRM2BOPA1
Other nucle
ar
MD & others
0
10
20
30
40
50
Cardiomyopathy (including LVH) Conduction defect LV impairment LVH + WPW WPW Other
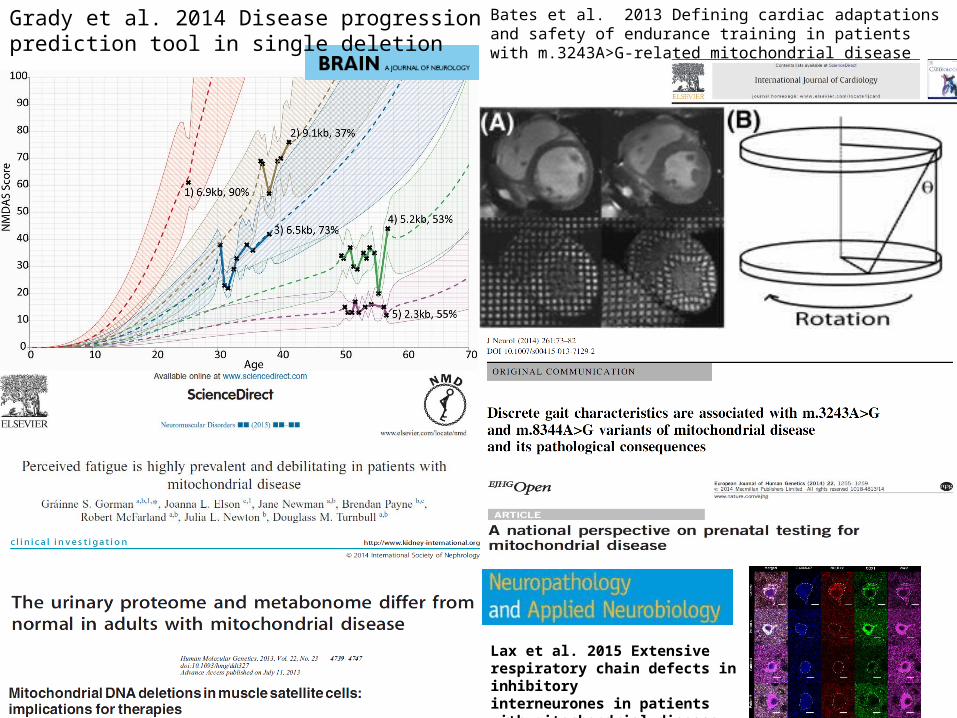
Grady et al. 2014 Disease progression prediction tool in single deletion
Bates et al. 2013 Defining cardiac adaptations and safety of endurance training in patients with m.3243A>G-related mitochondrial disease
Lax et al. 2015 Extensive respiratory chain defects in inhibitoryinterneurones in patients with mitochondrial disease
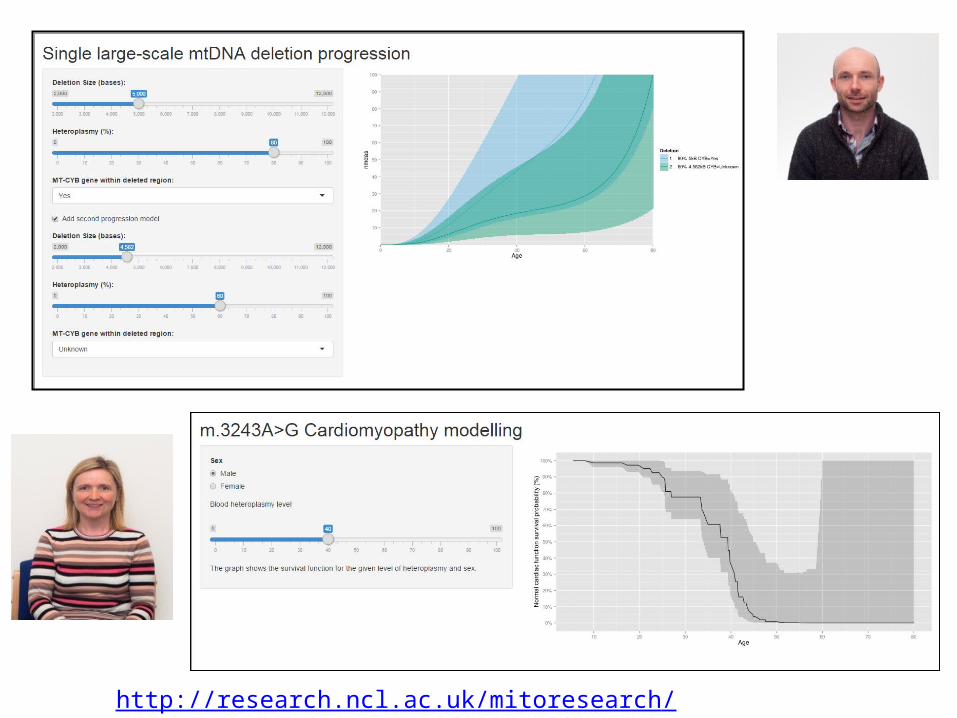
http://research.ncl.ac.uk/mitoresearch/

Best Practice Guidelines
http://www.newcastle-mitochondria.com/service/patient-care-guidelines/8 guidelines freely available; 2 in progress
Future Direction
• Clinical trial readiness
• International collaboration

Treatment – The Evidence (2012)
Cochrane Database Syst Rev. 2012 Apr 18;4:CD004426. doi: 10.1002/14651858.CD004426.pub3.


GRAZIE MILLE
Faculty of Medical Science, Newcastle University