www.iccg.org a unified clinical genomics database nhgri - u41 genomic resource grant
TRANSCRIPT

www.iccg.org
A Unified Clinical Genomics Database
NHGRI - U41 Genomic Resource Grant

Variant Analysis for General Genome Report
3-5 million variants
~20,000 Coding/Splice Variants
20-40 “Pathogenic”
Variants
Published as Disease-Causing
Genes
5-10 Variants
Pharmacogenetics<1%
Rare CDS/Splice Variants
LOF in Disease Associated Genes
30-50 Variants
Review evidence for gene-disease association and LOF role
Review evidence for variant pathogenicity

Classification of Reported Pathogenic Variantsfound in Human Genomes
Benign18%
Likely Benign26%
Uncertain significance – 52%
Pathogenic – 2%
Likely Path – 1%

U41 Genomic Resource Grant: A Unified Clinical Genomics
Database
To raise the quality of patient care by:
• Standardizing the annotation and interpretation of genomic variants
• Sharing variant and case level data through a centralized database for clinical and research use
• Implementing an evidence-based expert consensus process for curating genes and variant interpretations

Supporting data collection, submission and curation
• Work with NCBI to design ClinVar to meet the needs of the community
• Develop data dictionary, ontologies, and work with standards bodies
• Define data submission and access policies for variant and case-level data including genotypes and phenotypes
• Work with labs to solicit and support data submission
• Evidence-based curation of structural variants - (Riggs et al. 2012 )
• Evidence-based curation of sequence variants (ACMG Committee work in progress)
• Develop a gene-centric resource to define the medical exome and provide tools to support use in genomic medicine
• Work with vendors to improve reagents for genomic analysis (CMA, WES, WGS)

www.ncbi.nlm.nih.gov/clinvar
NIH NCBI ClinVar

ClinVar Submitters Variants Genes
OMIM 23524 3077Harvard Medical School and Partners Healthcare 6996 155InVitae Inc. 5526 4International Standards For Cytogenomic Arrays 4194 46GeneReviews 2913 287ARUP Laboratories 1415 6LabCorp 1391 140Sharing Clinical Reports Project 902 2Finland Institute for Molecular Medicine 840 39Tuberous Sclerosis Database 431 1ClinSeq Project 425 35Leiden Muscular Dystrophy Database 220 10GeneDx 205 3Emory Genetics Laboratory 48 13American College of Medical Genetics and Genomics 23 1Osteogenesis Imperfecta Database; University of Leicester 15 3Ambry Genetics 10 1Other laboratories (19) 52 25Total 49130 3848

Sequencing Laboratories Which Have Agreed to Share Data
Alfred I Dupont Hospital for ChildrenAll Children's Hospital St. PetersburgAmbry LaboratoriesARUPAthena DiagnosticsBaylor Medical Genetic LaboratoriesBoston Children's Hospital Boston UniversityChildren's Hospital of PhiladelphiaChildren's Mercy Hospital, Kansas CityCincinnati Children's HospitalCity of Hope Molecular Diagnostic LabCureCMDDenver Genetic LaboratoriesDetroit Medical CenterEmory UniversityFullerton Genetics LaboratoryGeneDxCleveland ClinicGreenwood GeneticsHarvard-Partners Lab for Molec. MedicineHenry Ford HospitalHuntington Medical Research Institutes
Illumina Clinical Services Lab
Indiana University/Perdue UniversityInSiGHTLabCorp / Integrated Genetics / CorrelagenMasonic Medical Research Laboratory Mayo ClinicMt. Sinai School of MedicineNationwide Children's Hospital Nemours Biomolecular Core, Jefferson MedicalOregon Health Sciences UniversityProvidence Sacred Heart Medical CenterQuest DiagnosticsSickKids Molecular Genetic LaboratoryTransgenomicsUniversity of ChicagoUniversity of MichiganUniversity of Nebraska Medical CenterUniversity of OklahomaUniversity of PennUniversity of SydneyUniversity of WashingtonWomen and Children's HospitalWayne State University School of MedicineYale University

Documenting arguments will improve the evidence-based assessment of variants

53 discrepancies:60% differ based upon likelihood (Benign vs LB, P vs LP)34% differed VUS vs Likely Pathogenic/Likely Benign6% differed VUS vs Pathogenic
20% discrepant
U41/ClinVar pilot project
Scope Number of alleles
Total submitted to ClinVar 997
Multiple assertions 269
Comparison of three laboratories classifications for variants in 12 RASopathy genes: BRAF, CBL, HRAS, KRAS, MAP2K1, MAP2K2, NRAS, PTPN11, RAF1, SHOC2, SOS1, SPRED1

84% differences were Lab A reporting a more aggressive assertion (Pathogenic/Benign) than Lab B/C (LP, LB, VUS)
16% of differences were Labs B/C reporting a more aggressive assertion than Lab A
Lab Classification Differences

ACMG Lab QA Committeeon the
Interpretation of Sequence Variants
ACMGSue Richards (chair), Heidi Rehm (co-chair)
Sherri Bale, David Bick, Soma Das, Wayne Grody, Madhuri Hegde, Elaine Spector
AMPJulie Gastier-Foster, Elaine Lyon
CAPNazneen Aziz, Karl Voelkerding
12

Evidence supporting pathogenicity (check all that apply): I. Stand-alone □ Truncating variant (e.g. nonsense, frameshift, canonical +/-1,2 splice sites, initiation
codon) in a gene where loss of function is a known mechanism of disease1
□ Same amino acid change as a previously established pathogenic variant regardless of nucleotide change2
II. Strong □ De novo (paternity confirmed)3
□ Well-established in vitro or in vivo functional studies supportive of a deleterious effect on the gene or gene product4
□ Case-control studies show a p value <0.01 for enrichment in cases6
III. Supporting □ Located in a mutational hot spot and/or experimentally well-characterized functional
domain7 □ Variant occurs in a gene with high clinical specificity and sensitivity for a particular
phenotype and the proband has multiple, specific features of the disease8 □ Multiple lines of computational evidence support a deleterious effect on the gene or
gene product (conservation, evolutionary, splicing impact, etc)9
□ Type of variant fits known pathogenic variant spectrum for the disease10 □ Variant frequency in control data
Absent from controls in Exome Sequencing Project & 1000 Genomes, OR Case-control studies show p value between 0.01-0.05 for enrichment in cases
(only applies if well-phenotyped populations are available) and frequency is below highest general population minor allele frequency (MAF) expected for disease:6
General guidance: Autosomal dominant MAF <0.4% General guidance: X-linked MAF <0.4% males General guidance: Autosomal recessive MAF <1%
□ For recessive disorders, detected in trans with a pathogenic variant11
□ Assumed de novo, but without confirmation of paternity3
□ In-frame deletions/insertions in a non-repeat region or stop-loss variants12 □ Co-segregation with disease5 □ Novel missense change at an amino acid residue where a different missense change
determined to be pathogenic has been seen before2
5 Categories:PathogenicLikely PathogenicUncertain significanceLikely benignBenign
Pathogenic = 1 stand-alone OR 2 strong OR 1 strong + ≥3 supporting
Likely Pathogenic = 1 strong + 2 supporting OR ≥4 supporting Benign = 1 stand-alone OR 2 strong OR 1 strong + ≥3 supporting
Likely benign = 1 strong + 2 supporting OR ≥4 supporting

Evidence supporting benign classification (check all that apply): I. Stand-alone □ For autosomal recessive: ≥1% MAF frequency6
□ For autosomal dominant: ≥0.4% or lower depending on disease frequency and penetrance6
□ For X-linked: ≥0.4% or lower in males depending on disease frequency and penetrance6 □ Observed in a healthy adult individual for a recessive (homozygous), dominant
(heterozygous), or X-linked (hemizygous) disorder with full penetrance at an early age6
II. Strong □ Well-established in-vitro or in vivo functional studies shows no deleterious effect on
protein function or splicing4
□ Observed in trans with a pathogenic variant for a fully penetrant dominant gene/disorder11
□ Variant present in multiple mammalian species despite adjacent conservation9
III. Supporting □ Located in a highly variable region without a known function7 □ Multiple lines of computational evidence suggest no impact on gene or gene product
(conservation, evolutionary, splicing impact, etc)9 □ Type of variant does not fit known pathogenic variant spectrum10 □ Case-control studies show comparable frequencies (e.g. p > 0.05)6
□ Variant in a dominant gene that does not segregate in a family5 or is found in a case with an alternate cause of disease13
□ Observed in cis with a pathogenic variant11
*Variants should be classified as Uncertain Significance if other criteria are unmet

Large variant datasets
Intra-laboratory
Evidence-based review
Practice guidelines
Expert Curation
Single-Source Curation
Uncurated
Multi-Source Curation
Guideline
Inter-laboratory
dbSNP/dbVar
ClinVar
QC and Expert Concensus

Curation - ClinVar

Analysis of LOF Variants - single genome
False positive
Weak gene-disease association
Non-Mendelian
LOF not disease mechanism
Weak gene to disease association
10
Pathogenic - 2
VUS – 1 (novel)
Excluded46
Novel/Rare - 41
Common33 8
ReportedRare LOFs
(Both AR1 novel
1 known)
False Positives
13
NotMendelian
14
LOF not a disease Mechanism - 2
82 LOF variantsbelow 5% MAFfrom one case
Update database

1. Define genes with medical relevance2. Technical challenges
• High GC• Pseudogenes/homologies• Repeat expansions• Common sites of structural variation
3. Variant types (denote common vs rare types)• Sequence variants (substitutions, small indels)
• Loss-of-function vs. Gain-of-function• CNV – haploinsufficient vs. triplosensitive• Other structural changes (translocations, inversions, etc)• Imprinted loci• Repeat expansions
4. Medically relevant transcripts5. Gene regions of pathogenic relevance6. Patterns of inheritance (dominant, recessive, X-linked, mitochondrial, de novo, etc)7. Phenotypes and evidence base for phenotype associations8. Available approaches to define variant pathogenicity (assays, tools, etc)9. Clinical utility measures10. Clinical decision support opportunities
Gene-centric resource
Initiated through collaboration amongst CHOP, Emory, and Harvard/Partners and Structural Variant workgroup
U41 - Working with Existing Efforts
• NCBI (ClinVar, dbSNP, dbVar, dbGaP, GTR) and EBI
• NHGRI (CRVR, eMERGE, CSER, ROR), IRDiRC
• Regulatory and Standards: ACMG, CAP, CDC, FDA, ASHG, AMP, CMGS, Global Alliance
• Locus Specific Databases (LSDBs – LOVD and non-LOVD)
• InSiGHT, PharmGKB, MSeqDB, CFTR2, ENIGMA, etc
• Human Variome Project and HGVS
• PhenoDB (Ada Hamosh) and Human Phenotype Ontology (Peter Robinson)
• OMIM (Ada Hamosh) and GeneReviews (Bonnie Pagon)
• Patient Advocacy Groups (Genetic Alliance, Patient CrossRoads, UNIQUE, Disease Specific Groups)
• Industry partners (reagents, instruments, software, etc)

ClinGen: The Clinical Genome Resource Program
Collaboration between:• NHGRI U41 Grant
– PIs: Ledbetter (Geisinger), Martin (Geisinger), Nussbaum (UCSF), Mitchell (Utah), Rehm (Partners/Harvard)
• NHGRI U01 “Clinically Relevant Variant Resource” Grants– Grant 1 PIs: Bustamante (Stanford), Plon (Baylor)– Grant 2 PIs: Berg (UNC), Ledbetter (Geisinger), Watson
(ACMG)• NCBI
– ClinVar
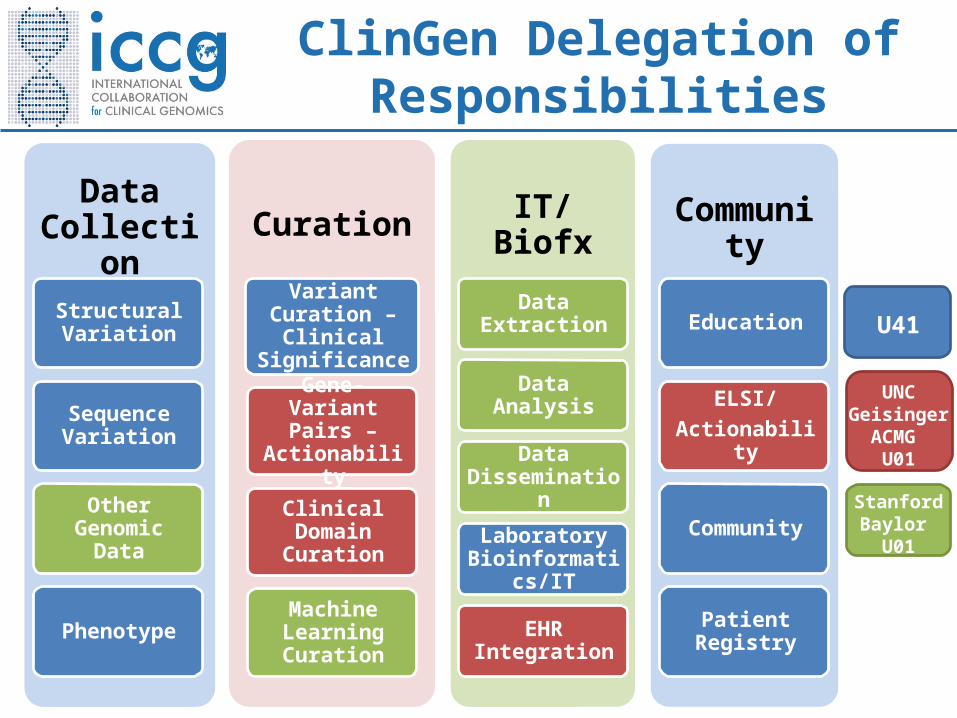
Data Collection
Structural Variation
Sequence Variation
Other Genomic Data
Phenotype
Curation
Variant Curation – Clinical
Significance
Gene-Variant Pairs –
Actionability
Clinical Domain Curation
Machine Learning Curation
IT/Biofx
Data Extraction
Data Analysis
Data Dissemination
Laboratory Bioinformatics/IT
EHR Integration
Community
Education
ELSI/Actionability
Community
Patient Registry
U41
UNCGeisinger
ACMG U01
StanfordBaylor
U01
ClinGen Delegation of Responsibilities

CoreDBDisease Area Curation Tool
ClinGen System Interactions
OMIM
Patient Registries
EHR Interface
Expert Curation of Genes and Variants by Clinical Domain and Disease Area Workgroups
dbGaP
LSDBs
LabsLabs
Labs(Genotypes & Phenotypes)
Gene Resource
(Medical Exome, Actionability)
CNV Curation Tool
(JIRA)
Application Interface
External Informatics Activities Enabled
ExpertCuratedVariants
Case-level Data
Variant-level Data
ClinVar
Disease WGs
Clinical Domain WGs
Data
Crowd-sourced Curation
Controlled Access
Public Access
Private
PharmGKB
Machine Learning Algorithms
PopulationDatasets
MedicalLit
Portal for the Public

International Collaboration for Clinical Genomics
– Over 190 institutional members
– Over 2800 individual members
Annual Conference June 10-12, 2014, Bethesda, MD– Attendees include laboratory directors, physicians, genetic counselors,
researchers, parents, government employees, regulatory agency representatives, and vendor partners
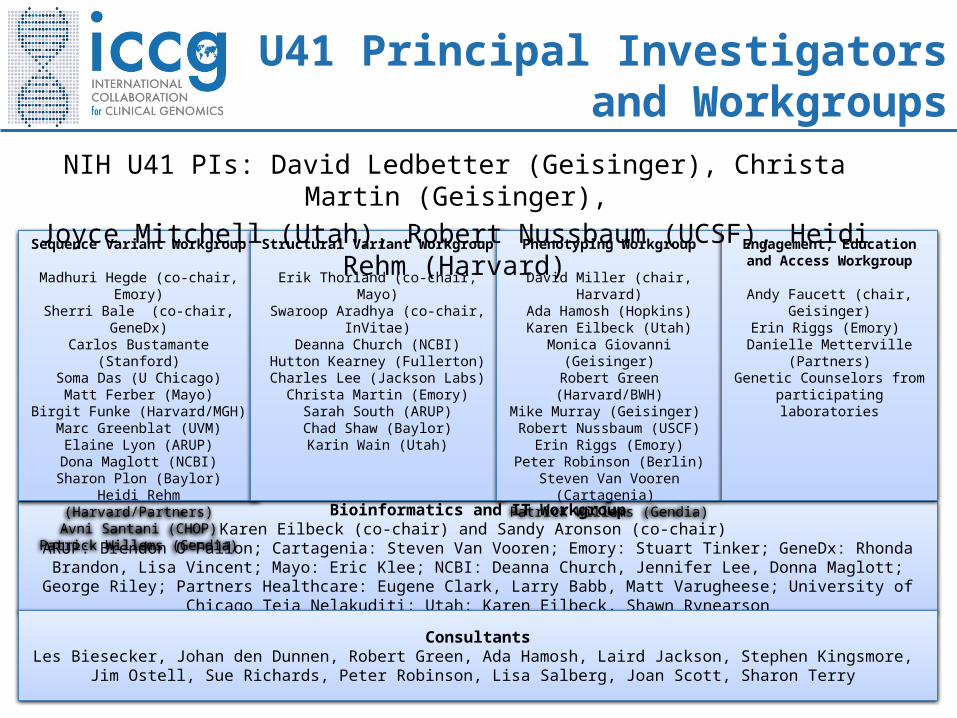
Bioinformatics and IT WorkgroupKaren Eilbeck (co-chair) and Sandy Aronson (co-chair)
ARUP: Brendon O’Fallon; Cartagenia: Steven Van Vooren; Emory: Stuart Tinker; GeneDx: Rhonda Brandon, Lisa Vincent; Mayo: Eric Klee; NCBI: Deanna Church, Jennifer Lee, Donna Maglott; George Riley; Partners Healthcare: Eugene Clark, Larry
Babb, Matt Varugheese; University of Chicago Teja Nelakuditi; Utah: Karen Eilbeck, Shawn Rynearson
Sequence Variant Workgroup
Madhuri Hegde (co-chair, Emory)Sherri Bale (co-chair, GeneDx)Carlos Bustamante (Stanford)
Soma Das (U Chicago)Matt Ferber (Mayo)
Birgit Funke (Harvard/MGH)Marc Greenblat (UVM)
Elaine Lyon (ARUP)Dona Maglott (NCBI)Sharon Plon (Baylor)
Heidi Rehm (Harvard/Partners)Avni Santani (CHOP)
Patrick Willems (Gendia)
Structural Variant Workgroup
Erik Thorland (co-chair, Mayo)Swaroop Aradhya (co-chair, InVitae)
Deanna Church (NCBI)Hutton Kearney (Fullerton)
Charles Lee (Jackson Labs)Christa Martin (Emory)Sarah South (ARUP)Chad Shaw (Baylor)Karin Wain (Utah)
Phenotyping Workgroup
David Miller (chair, Harvard)Ada Hamosh (Hopkins)
Karen Eilbeck (Utah)Monica Giovanni (Geisinger)Robert Green (Harvard/BWH)
Mike Murray (Geisinger) Robert Nussbaum (USCF)
Erin Riggs (Emory)Peter Robinson (Berlin)
Steven Van Vooren (Cartagenia) Patrick Willems (Gendia)
Engagement, Education and Access Workgroup
Andy Faucett (chair, Geisinger)Erin Riggs (Emory)
Danielle Metterville (Partners)Genetic Counselors from participating laboratories
ConsultantsLes Biesecker, Johan den Dunnen, Robert Green, Ada Hamosh, Laird Jackson, Stephen Kingsmore,
Jim Ostell, Sue Richards, Peter Robinson, Lisa Salberg, Joan Scott, Sharon Terry
U41 Principal Investigators and Workgroups
NIH U41 PIs: David Ledbetter (Geisinger), Christa Martin (Geisinger), Joyce Mitchell (Utah), Robert Nussbaum (UCSF), Heidi Rehm (Harvard)
