www.asthma-workplace.com. tools in the investigation of asthma in the workplace jean-luc malo md...
TRANSCRIPT

www.asthma-workplace.com

Tools in the investigation of
asthma in the workplace
Jean-Luc Malo MD
Hôpital du Sacré-Cœurde Montréal
Université de Montréal
Axe de rechercheen santé respiratoire
Centre asthme et travailCenter for Asthma in the Workplace

1. Review on available tools
2. How to use these tools
Tools
1. Questionnaires
2. Immunologial tests
3. Lung function tests

Standardized epidemiological questionnaire for asthma:
Developed by the EuropeanRespiratory Society*
Addition of questions relevant to theintensity and timing of symptomsin relation to the workplace(not standardized)
* Burney PGJ et al. Eur Respir J 1988
Content of the ERS Asthma Questionnaire
Nature of symptoms: shortness of breath, wheezing,
cough, sputum, tightness in the chest
Timing of symptoms: in the past year;
seasonal vs perennial
Provoking factors
Relevant personal and familial atopic history
Symptoms at the workplace (nose, eyes, chest)
Other chest conditions, smoking
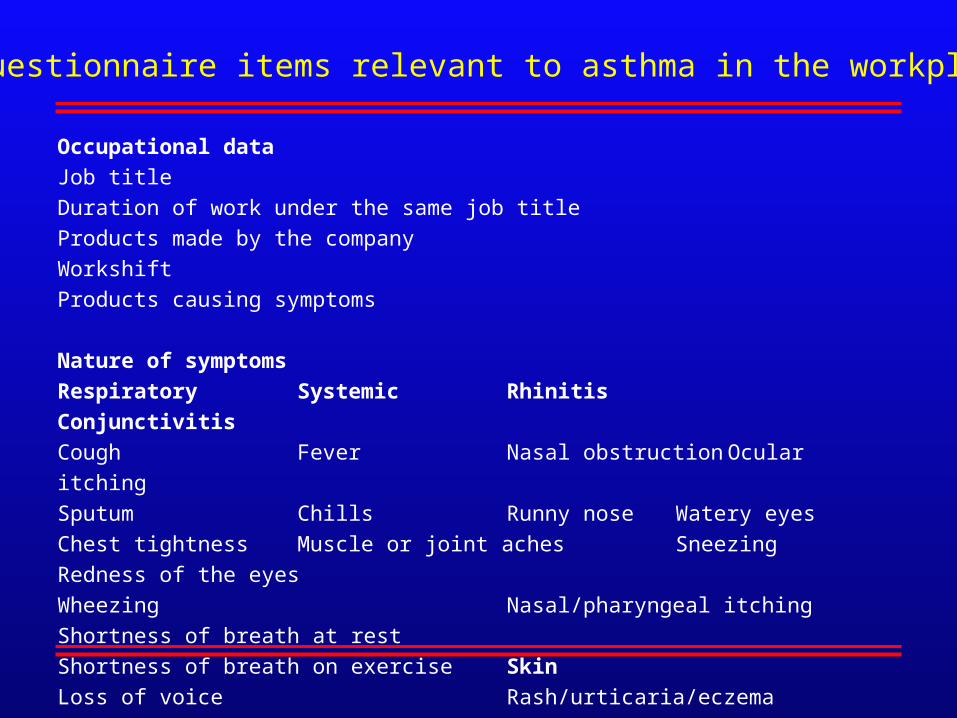
Questionnaire items relevant to asthma in the workplace
Occupational data
Job title
Duration of work under the same job title
Products made by the company
Workshift
Products causing symptoms
Nature of symptoms
Respiratory Systemic Rhinitis Conjunctivitis
Cough Fever Nasal obstruction Ocular itching
Sputum Chills Runny nose Watery eyes
Chest tightness Muscle or joint aches Sneezing Redness of the eyes
Wheezing Nasal/pharyngeal itching
Shortness of breath at rest
Shortness of breath on exercise Skin
Loss of voice Rash/urticaria/eczema
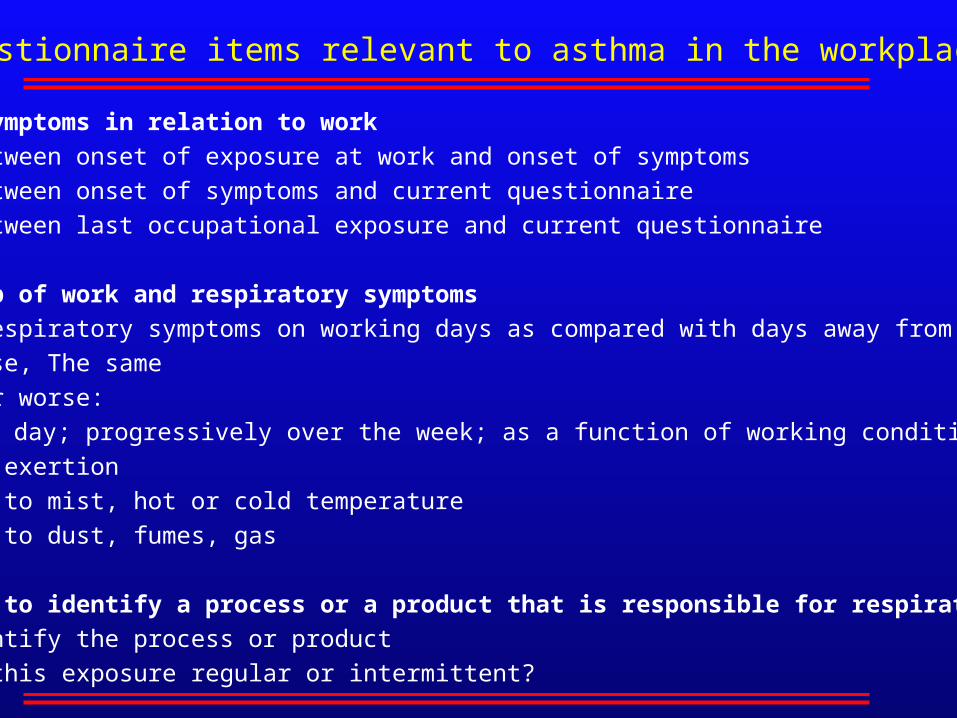
Timing of symptoms in relation to work
Interval between onset of exposure at work and onset of symptoms
Interval between onset of symptoms and current questionnaire
Interval between last occupational exposure and current questionnaire
Relationship of work and respiratory symptoms
Status of respiratory symptoms on working days as compared with days away from work:
Better, Worse, The same
If better or worse:
Every day; progressively over the week; as a function of working conditions.
On physical exertion
On exposure to mist, hot or cold temperature
On exposure to dust, fumes, gas
Possibility to identify a process or a product that is responsible for respiratory symptoms
If yes, identify the process or product
If yes, is this exposure regular or intermittent?
Questionnaire items relevant to asthma in the workplace

Status of respiratory symptoms on weekends
They disappear
They improve
No change
Status of respiratory symptoms on vacations (more than one week)
They disappear
They improve
No change
If they disappear or improve, after how many days?
Timing of respiratory symptoms in relation to work
Interval between onset of work and onset of symptoms
Persistence or reappearance of symptoms on return to homeOnset of symptoms only on returning homeChange of timing of symptoms over time
Questionnaire items relevant to asthma in the workplace

Is the clinical history a satisfactory means
to diagnose occupational asthma ? *
Sensitivity: 87 %Specificity: 55 %Positive predictive value: 63 %Negative predictive value: 83 %
* Prospective clinical assessment of 162 patients
referred for possible occupational asthma.
Malo JL et al. Am Rev Respir Dis 1991
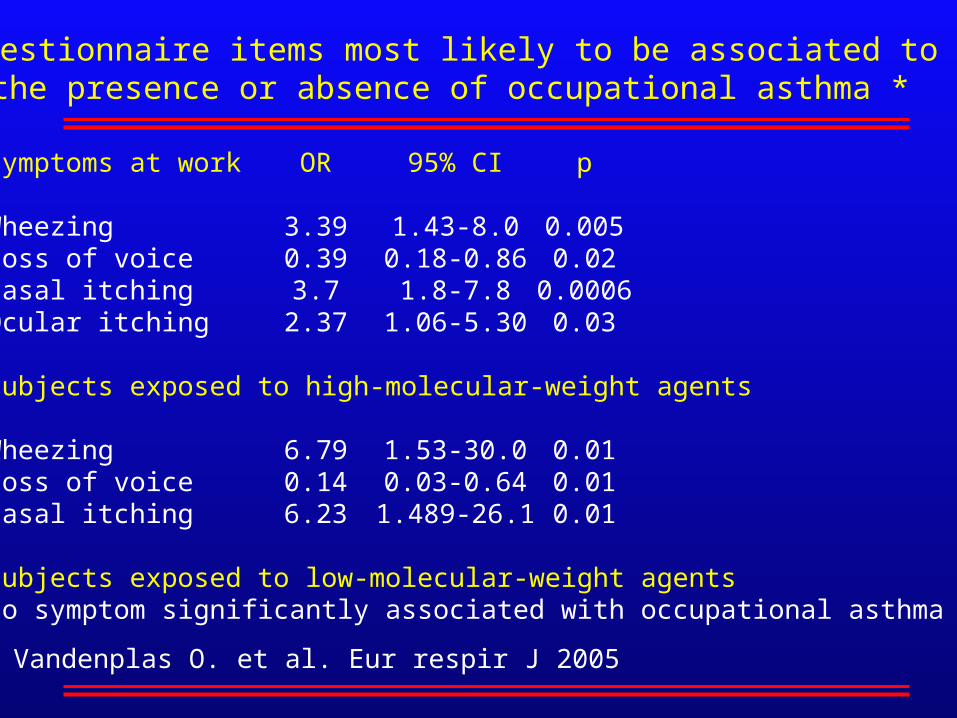
Symptoms at work OR 95% CI p
Wheezing 3.39 1.43-8.0 0.005Loss of voice 0.39 0.18-0.86 0.02Nasal itching 3.7 1.8-7.8 0.0006Ocular itching 2.37 1.06-5.30 0.03
Subjects exposed to high-molecular-weight agents
Wheezing 6.79 1.53-30.0 0.01Loss of voice 0.14 0.03-0.64 0.01Nasal itching 6.23 1.489-26.1 0.01
Subjects exposed to low-molecular-weight agentsNo symptom significantly associated with occupational asthma
Questionnaire items most likely to be associated tothe presence or absence of occupational asthma *
* Vandenplas O. et al. Eur respir J 2005

Tools
1. Questionnaires
2. Lung function tests
3. Immunological tests

Assessment of bronchial caliber and responsiveness
Bronchial obstruction present in a minority of asthmatic
subjects but bronchial hyperresponsiveness present in
all at the time they have symptoms.
Various means to assess bronchial hyperresponsiveness but
inhaled methacholine the standard one: dose that causes a
20% change in FEV1 and that is equal or less than 8-16 mg/ml..

Assessment of bronchial responsiveness (methacholine)
Suggests that someone may have asthmaIf negative test, this virtually excludes current asthmaFalse positive test in rhinitis and COPD.
If negative test while a worker is at work andreports symptoms, this virtually excludes asthma and occupational asthma (butnot eosinophilic bronchitis).
If positive test while a worker is at work, thissuggests either asthma or occupational asthma.
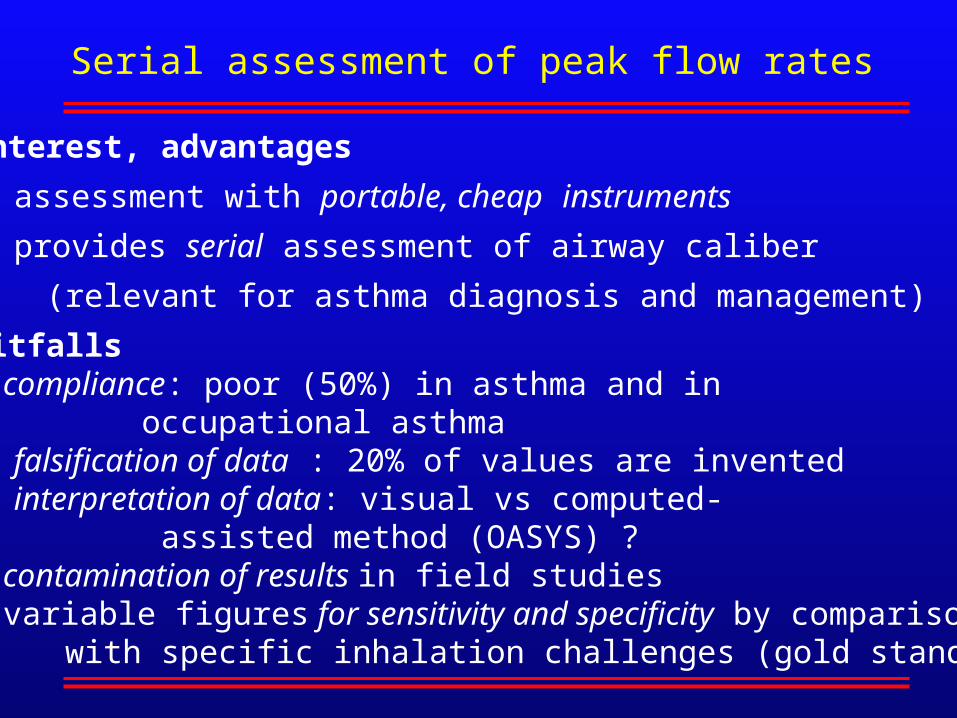
Serial assessment of peak flow rates
Interest, advantages
assessment with portable, cheap instruments
provides serial assessment of airway caliber
(relevant for asthma diagnosis and management)
Pitfalls compliance: poor (50%) in asthma and in occupational asthma falsification of data : 20% of values are invented interpretation of data: visual vs computed- assisted method (OASYS) ? contamination of results in field studies variable figures for sensitivity and specificity by comparison
with specific inhalation challenges (gold standard)


Tools
1. Questionnaires
2. Lung function tests
3. Immunological tests

Immunological assessment of specific antibodies
Highly sensitive for high-molecular-weight agents
to develop the disease, one has to be “sensitized”
Interesting for some low-molecular-weight agents
(metal salts, isocyanates)

Sensitivity, specificity, and predictive values of diagnostic tests
compared with specific inhalation challenges *
Diagnostic tests Sensitivity Specificity PPV NPV
(%) (%) (%) (%)
Clinical history 87 14 75 50
Methacholine test 90 7 68 25
Skin prick tests 100 21 74 100
History + skin prick tests 94 36 76 71
PPV, positive predictive value; NPV, negative predictive value.
* Nurses exposed to latex. From Vandenplas O et al. J Allergy Clin Immunol 2001
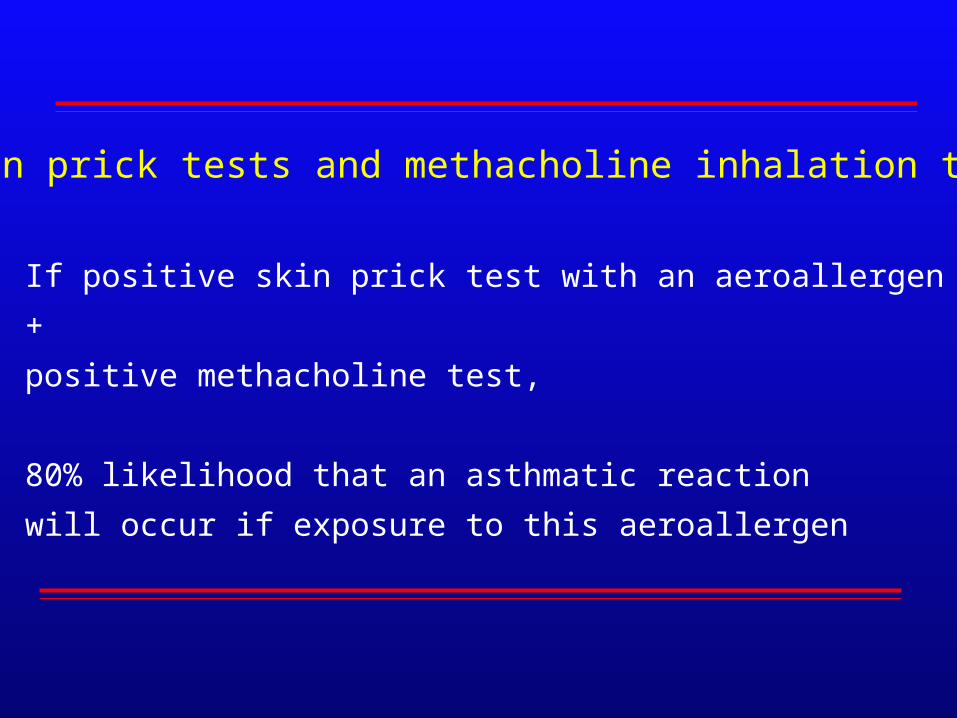
Skin prick tests and methacholine inhalation test
If positive skin prick test with an aeroallergen
+
positive methacholine test,
80% likelihood that an asthmatic reaction
will occur if exposure to this aeroallergen
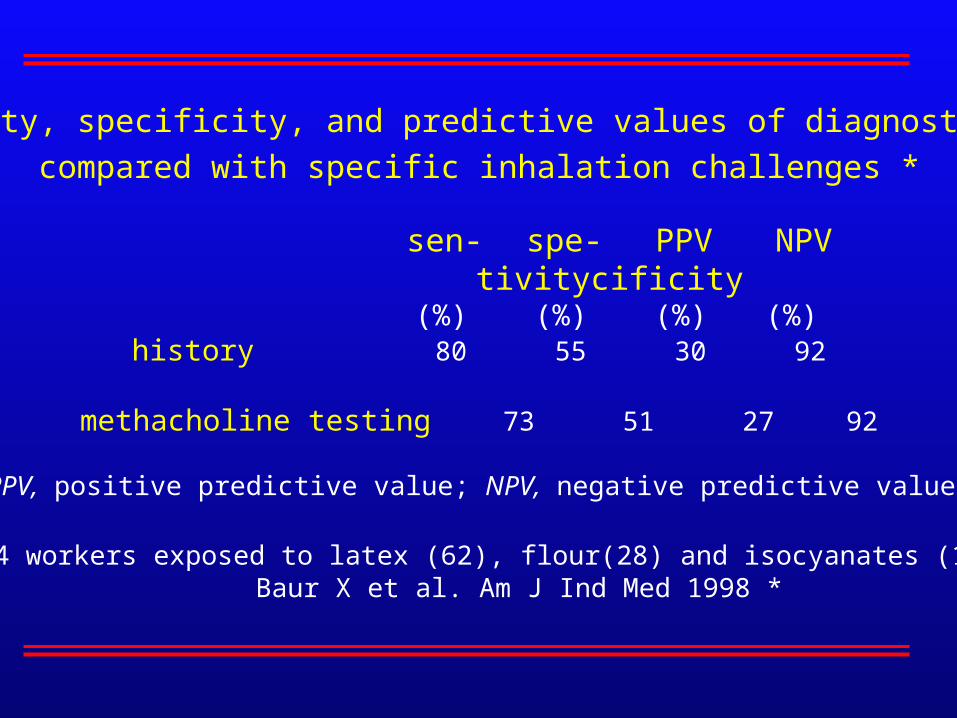
Sensitivity, specificity, and predictive values of diagnostic tests
compared with specific inhalation challenges *
sen- spe- PPV NPVtivity cificity
(%) (%) (%) (%) history 80 55 30 92
methacholine testing 73 51 27 92
PPV, positive predictive value; NPV, negative predictive value.
* 204 workers exposed to latex (62), flour(28) and isocyanates (114);Baur X et al. Am J Ind Med 1998 *
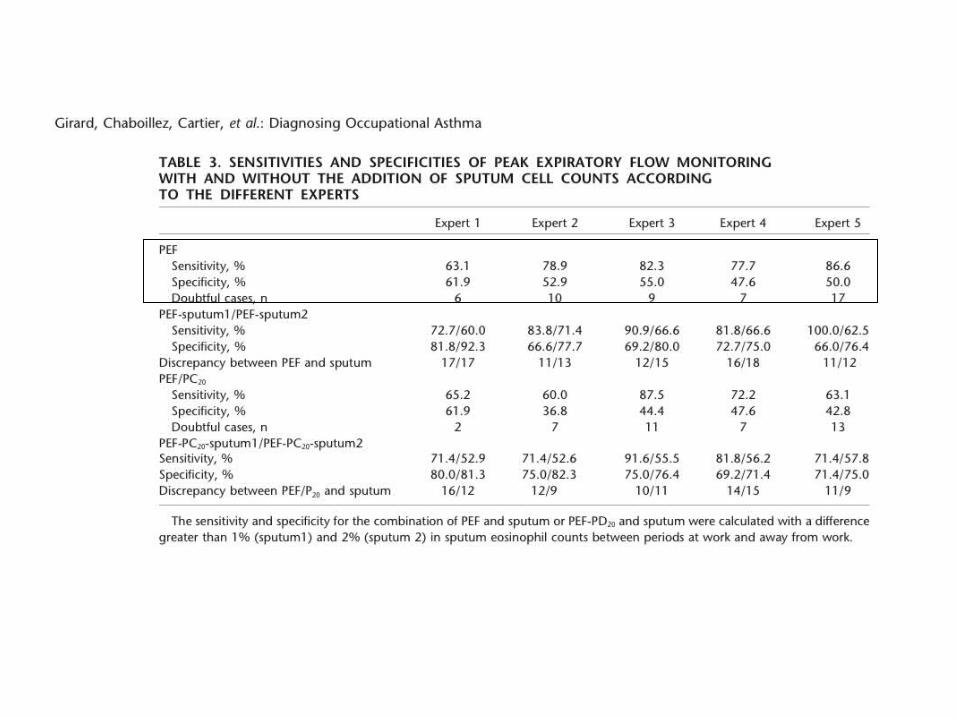
Girard F et al. Am J Respir Crit Care Med 2004
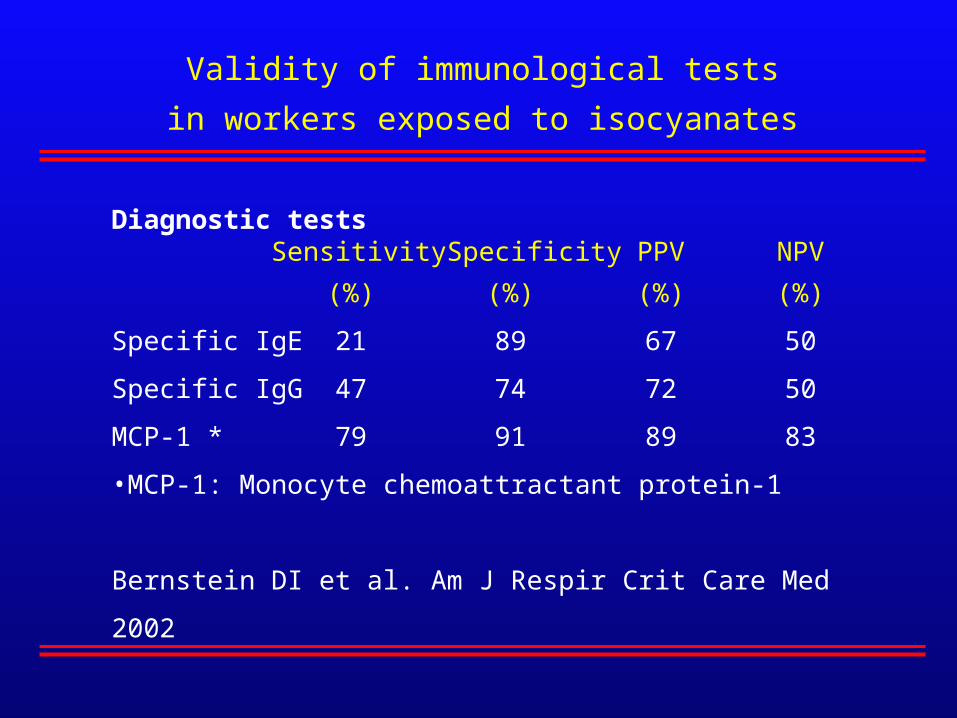
Diagnostic tests Sensitivity Specificity PPV NPV
(%) (%) (%) (%)
Specific IgE 21 89 67 50
Specific IgG 47 74 72 50
MCP-1 * 79 91 89 83
•MCP-1: Monocyte chemoattractant protein-1
Bernstein DI et al. Am J Respir Crit Care Med 2002
Validity of immunological tests
in workers exposed to isocyanates

1. Review on available tools
2. How to use these tools

Compatible historyand/or exposure to a relevant agent
Immunological tests possible:skin prick tests,
specific antibodies
Methacholine inhalation test(working period)
abnormalnormal
No asthma,no occupational asthma
PEF monitoringand/or referral
Positive:sensitization
Negative:no sensitization
No occupationalasthma
Skin pricktests not feasible(low molecularweight agents)
Surveillance of asthma in the workplace
Conclusion
Several tools to be used in combination in surveillance programs
or investigation of individual cases of possible workplace asthma.
For high-molecular-weight agents and some low-molecular-weight
agents: skin prick tests and methacholine test while at work
For most low-molecular-weight agents: ?