wrist & hand injury in sports -...
TRANSCRIPT

Wrist & Hand Injury in Sports
Return to Play Criteria, Clinical Pearls, & Rehab Considerations
PBATS Baseball Medicine Conference 2018
Jennifer Allen,PT,DPT,OCS,SCS,CHT

Disclosures

Wrist & Hand Injury in Sports
Agenda:
• Common Injuries in Baseball & Softball
• Rehabilitation Considerations
• Clinical Pearls for Wrist & Hand
• Return to Play Criteria
3

“Rehabilitation of the Hand 6th Edition”
Berger, R. Rehabilitation of the Hand (2010)
Upwards of 25% of all Sports Injuries are injuries to the wrist and hand

“Epidemiology & Effect of Sliding Injuries in Major and Minor League Baseball”
Camp, C., et al. Am Journal Sports Medicine (2017)
1/336 slides results in injury of some type25.3% of all injuries – Hand/Fingers
31.3% of Hand/Finger Injuries Require Surgery

“Baseball & Softball injuries: Elbow, Wrist & Hand”
Trehan, S., et al. J Hand Surg Am (April 2015)
*Hook of Hamate Fracture *TFCC Tears*Thumb UCL Injury Scapholunate Ligament TearHand/Finger Fracture Extensor Carpi Ulnaris Instability*Mallet Finger Ulnar Head SubluxationFlexor Tendon Injuries Ulnar Impaction SyndromeFlexor Pulley Injuries Digital Ischemia/Microvascular TraumaAdductor Pollicis Longus Injury Bouttonniere Deformity

“Hook of Hamate Fracture in Competitive Baseball Players”
Baseball
Cause:- Repetitive Swinging/Batting- Rogue Pitches
Main Points:- High rate of non-union with conservative care- Surgical repair with Ulnar Nerve Decompression (Guyon
Canal)- Return to play Avg 5.7 wks (Baseball)
7
Bachoura, B., et al. Hand (2013)
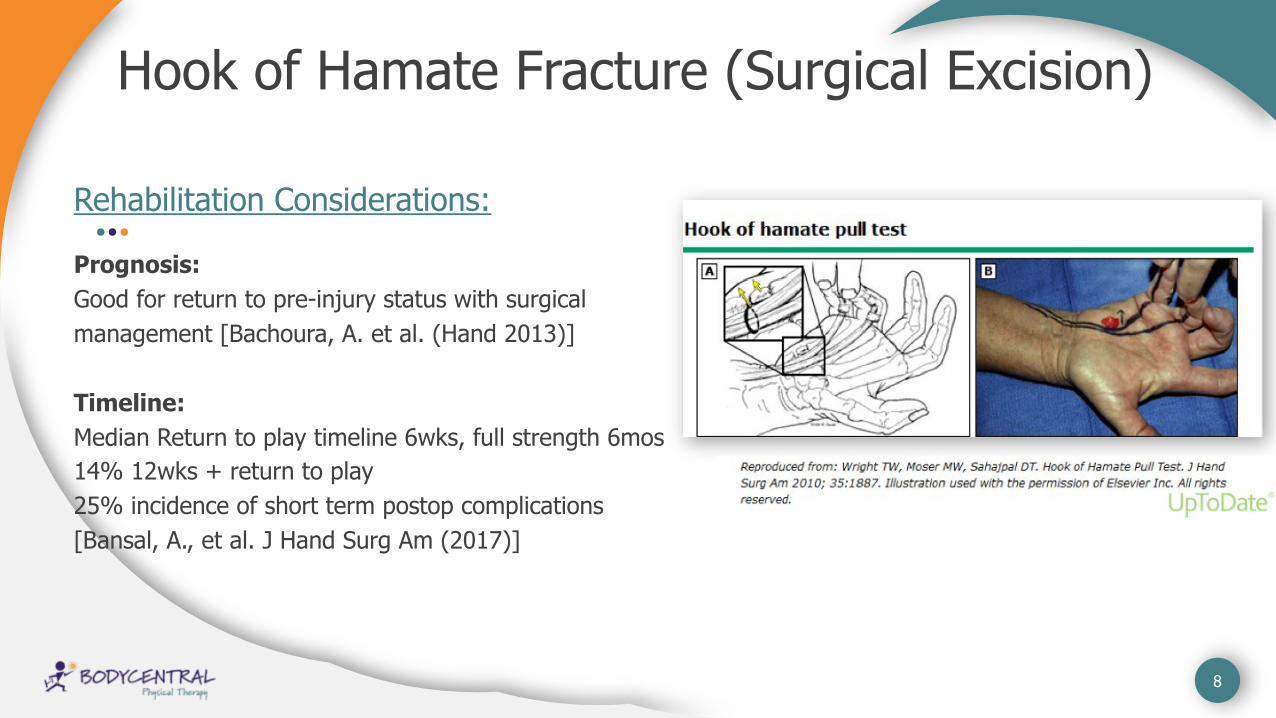
Hook of Hamate Fracture (Surgical Excision)
Rehabilitation Considerations:
Prognosis: Good for return to pre-injury status with surgical
management [Bachoura, A. et al. (Hand 2013)]
Timeline:Median Return to play timeline 6wks, full strength 6mos
14% 12wks + return to play
25% incidence of short term postop complications
[Bansal, A., et al. J Hand Surg Am (2017)]
8

Hook of Hamate Post-op Rehab
- Cast Immobilization - 10-14 days- Physician Dependent
Surgical Excision of Hook
- General Conditioning - Cardio- Intensity based on
edema/pain
Immobilization Period
- Wrist ROM- Digital ROM- Desensitization- Edema Reduction
Immediate Mobilization 2wks
- Strengthening Progression
- Desensitization- Padding for RTP- Sport Specific – 6wks
Strengthening-RTP 3-6wks
9

Clinical Pearls:Hook of Hamate Post Surgery
*Early desensitization over scar to decrease hypersensitivity 3min, 3x/day*Scar mobilization and Ulnar Nerve Glides to improve soft tissue mobility
*Silicone gel pads, relief foam pads, padded batting gloves for return to activity.

Hand Rehabilitation/Hamate
Silicone Cupping
Hamate PadHamate Dry Needling

Mallet Finger
Rehabilitation Considerations:Non-Op Splinting:Prognosis good with complianceContinuous splinting of DIP in full extension/hyperextensionMinimum 6wks, up to 10+wks
12

Mallet Finger Post-Op
Rehabilitation Considerations:
Post-Op Stabilization: Surgery Indicated with 1/3 of articular surface fxPrognosis good for full return
***No difference in long term outcomes noted surgery vs non surg, night splinting vs none
Bloom, J., et al. Plastic and Reconstructive Surgery (2013)
13

Mallet Finger Progression
- Splinting 6-10wks- No Passive DIP flexion
after splinting for additional 4wks
- Start AROM with MD approval when splinting ceases
Non-Op Management
- K Wire Fixation/or other- Immobilized up to 6wks- Then follow protocol
same as non-operative
Operative Management
- Generally started 4 wksafter splinting is discontinued
- Watch for Extensor Lag
PROM (Both)
- Strength Progression- Goal is Functional ROM
and minimal Extensor Lag
- Progress timeline with PROM
Strength/Function
14

Clinical Pearls:Mallet Finger
*Skin breakdown is one cause of poor outcomes in treating Mallet Finger. Less skin breakdown with custom splints. (Mallet Mender, Thermoplastic custom)
Valdes, K., et al. Journal of Hand Therapy (2015)
*Athletes must keep DIP in extension when washing hands, etc. Loss of extension results in restart of the timeline.

Hand Rehabilitation- Mallet Finger
16

Triangular Fibrocartilage Complex Tears(TFCC)
Rehabilitation Considerations:TFCC Components:
- TFC Disc (poor healing capability)- Meniscus Homologue- Radioulnar ligaments- Sheath of Extensor Carpi Ulnaris- Ulnar Collateral Ligament- Ulnolunate and Ulnotriquetral ligaments
Symptoms:- Ulnar sided Wrist Pain- Clicking/Popping, Instability- Pain with weight bearing
17

“Triangular Fibrocartilage Complex (TFCC) Tears”
Rehabilitation Considerations:
- Traumatic vs Degenerative
- Prognosis:- Trial of Conservative Care is Recommended- Chronic Injuries respond less favorably to conservative care- Surgical repair recommended for high level athletes- Instability DRUJ recommend surgical repair
Brownstein, B., et al Cinahl Clinical Review (2018)
18

19
TFCC Management
Conservative Care:
- For degenerative tears, sedentary patient- Type IA tears (Central Perforation), may heal
due to vascularity (Baseball)- Patients without DRUJ instability- Time? In season?- Return to play varied – (weeks-months)
Surgical Intervention:
- Recommended for high level athletes not responding to conservative care
- Tear of TFCC with Instability DRUJ- Return to play avg 3.3 months
No Baseball Specific outcome comparison studies conservative care vs surgical repair
Brownstein, B., et al. Cinahl Clinical Review (2018)

TFCC Tear Management
- Splint 4-6wks- Modalities- ROM, jt mobilization- Splinting PRN after
initial 6wks- Strengthening when
pain decreases
Conservative RX- Splint 1-2 wks post op- ROM, jt mobilization- Strengthening 4wks+- Athlete return to sport
specific activity 6wks
TFCC Arthroscopic Debrid- Splint 4-8 wks- ROM, edema control,
scar management when splint removed
- Strengthening - Athlete return to sport
12wks (avoid impact)
TFCC Repair- Ulnar Impaction- 1-6wks immobilization- ROM, edema reduction,
scar management- 10-12 week return to
activity
Ulnar Shortening
20

Clinical Pearls:TFCC Rehabilitation
Brownstein, B., et al. Cinahl Clinical Review (2018)
*Restore Supination ROM – loss in Supination is associated with poor functional outcomes
*Start Strengthening first in Supination, Then in wrist Neutral, followed by Pronation. The ulnar sided wrist forces are the least in Supination and the most in the Pronated position. Using this progression will decrease strain in that region as it heals.

TFCC Clinical Tools:
www.wristwidget.com

Thumb UCL Injury
Rehabilitation Considerations:
Grade I Injury- Painful but stableGrade II Injury- Painful with some laxity, possible fractureGrade III Injury- Painful, severe laxity, fracture (it’s over)
Partial tears- conservative trialComplete tear or Stener Lesion, surgical intervention recommendedStener Lesion: Torn UCL is pulled out from aponeurosis of adductor pollicis and gets trapped
23

UCL Thumb Injury Timelines
- Cast/Functional Splint 2-4wks
- Thumb must be stable in flexion for good outcome
- Rehab- key pinch first, delay tip pinch and full grip for up to 8wks
- Stability is most important
Non Surgical (acute/partial)
- Ligamentous repair of structure then
- Splinting x 4wks- Flex/Ext ROM first 4-
6wks- Slow strength return
with protection of repair- 12 wk return to activity- Recommend splinting
for return to activity
Surgical Repair
- Similar to Ligamentous repair
- Indicated for Chronic Tears
- Palmaris/Plantaris grafts- Slow strength/function
progression
Surgical Reconstruction
- Taping - Splinting- short thumb
spica- Soft splints available- Slow return- stability
most important, avoid early stressors
Return to Play
24

Clinical Pearls:Thumb UCL Injury
Tsiouri, C., et al. Hand(2009)
*In rehabilitation of the Thumb UCL injury, ligament protection and joint stability are #1 Priority.
* Start with Key Pinch Strengthening first, then slowly progress to Tip pinch and full grip strengthening around weeks 8-10. Splinting recommended for return to play.

Key Pinch

Isolated Extension
27

Intrinsic Strengthening
28

Intrinsic Strengthening
29

Tendon Gliding Exercises (Edema & Mobility)
30

31
Hand Rehabilitation
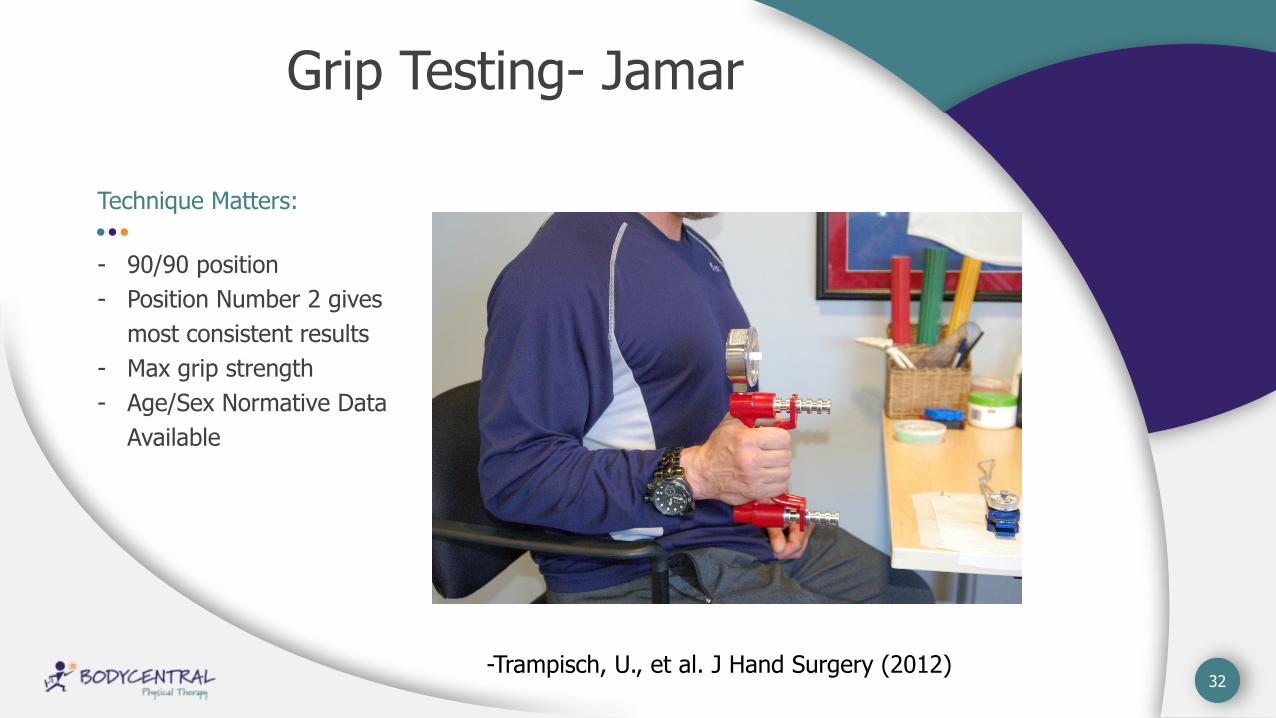
Grip Testing- Jamar
Technique Matters:
- 90/90 position- Position Number 2 gives
most consistent results- Max grip strength- Age/Sex Normative Data
Available
32-Trampisch, U., et al. J Hand Surgery (2012)

33
Hand & Wrist Return to Play Criteria
“Functional” ROM in affected Digit/Joints
Healing Timeline/Structure Dependent
Grip Strength – 20psi needed for ADLS
Pinch Strength- 5-7psi Needed for ADLS
Grip Strength: Goal <15% R vs L, Return to sport at 25%
Pain Tolerance (Splinting, taping, padding)
Psychological Factors, Fear
Sport Demands Specific to Athlete’s Injury

Contact InfoJen Allen,PT,DPT,OCS,SCS,CHT
520-982-9966
www.Bodycentralpt.net
Bodycentral PT Ultimate Sports Asylum1991 E Ajo Way, Ste 149Tucson, AZ 85713