working with you for better health the diabetic foot angela walker diabetes specialist podiatrist
TRANSCRIPT

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
The Diabetic Foot
Angela WalkerDiabetes Specialist Podiatrist

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
“Why Worry …?” Approximately 15% of all people with diabetes will be
affected by foot ulcer during their lifetime;
85% of diabetes-related amputations are preceded by foot ulcers (International Diabetes Federation) ;
Up to 70% of amputations are performed on people with Diabetes;
“Someone, somewhere, loses a leg because of diabetes every 30 seconds of everyday…”
Lancet. 2005;366:1674

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Multifactorial Aetiology
Vascular: macro and microangiopathy results in poor skin quality, poor healing and potential for ulceration and amputation.
Neuropathy causes loss of sensation, potential for injury, infection, leading to ulceration and possible amputation.
Delayed immune response: any injury to the foot is a potential cause for concern.
Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Diabetic Ischaemia
Micro-vascular and Macro-vascular
Pathology identical to non-diabetics
Earlier onset
Complications of high blood pressure, high cholesterol and smoking are all amplified by diabetes
1 Cigarette reduces peripheral blood flow by 30% for 1 hour.

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Reduced or Absent Hair
Changes in Nail & Rate
of Growth
History ofIntermittent Claudication
Faint or Absent Pulses
Anhydrosis& Fissures
Loss of Wrinkling ofSkin Around Joints
Skin Colour & Temperature

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Peripheral Neuropathy
Dysfunction of sensory, motor and autonomic nerves:
Loss of protective pain sensation – increased susceptibility to foot ulceration
Motor – high medial longitudinal arch, clawed toes, prominent metatarsals
Autonomic – dry, fissured skin, sweat loss, distended dorsal veins

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Well nourished tissue
Diminished / absent sensation
“Cramping, Tingling, Aching, Burning,
Numbness”

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Callus at pressure points
Good DP and PT pulses
Painless ulcerations
Charcot Deformities

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Bilateral Charcot

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Differential Diagnosis
Neuropathic
Warm Normal colourPalpable pulsesSkin well nourished Callus at pressure pointsUlceration plantar
Neuroischaemic
CoolPalePulses diminished/ absentSkin thin shiny no hairNo callus fissuring at bony prominencesUlcers peripheral
Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
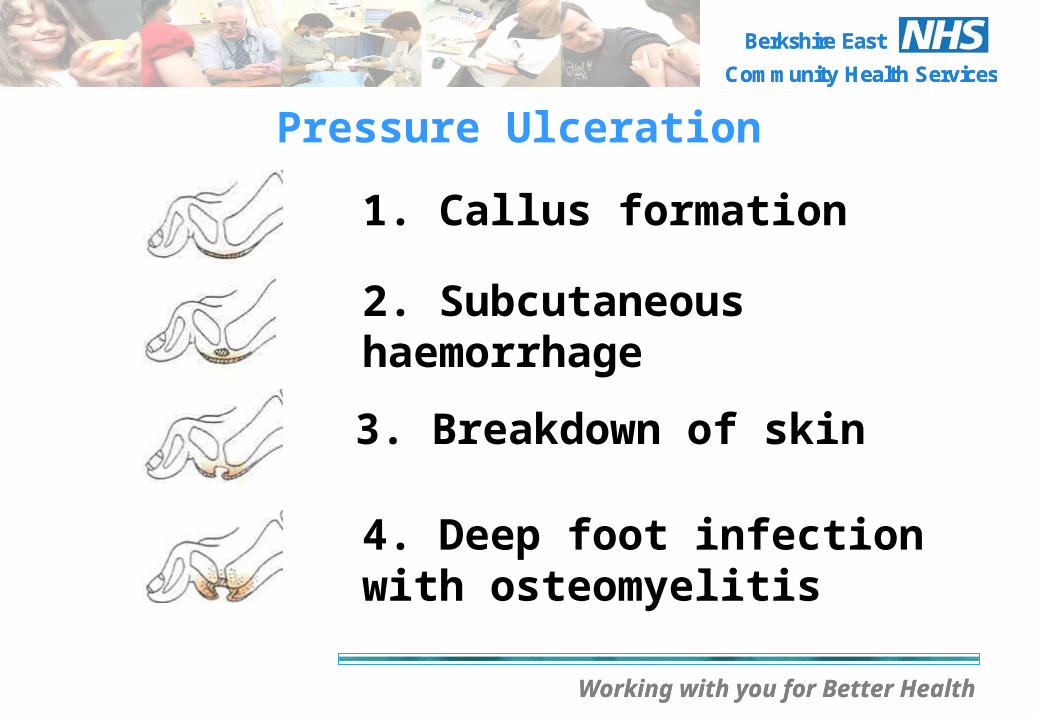
Pressure Ulceration
1. Callus formation
2. Subcutaneous haemorrhage
3. Breakdown of skin
4. Deep foot infection with osteomyelitis

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Osteomyelitis
Approximately 25% of foot ulcers will be affected by osteomyelitis (Young, Diabetic Foot Journal, 2008);
Surgery is not always necessary especially in patients without life or limb-threatening infections;
82% of patients studied by Game and Jeffcoate (Diabetologia, 2008) were able to avoid surgery with one or more courses of antibiotics.

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Foot problems can be Deceptive
Is the diabetic ulcer infected?
Compare the temperature of both legs Check blood glucose levels Pain is serious in the neuropathic foot Localised superficial infection is probably the
tip of the iceberg Healed wounds need appropriate protection
to prevent recurrence

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Debridement
Neuropathic ulcers – need to be debrided as soon as possible to determine the depth of the ulcer and removal of necrotic tissue
Ischaemic ulcers – should not be debrided unless signs of infection present.

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Before Sharp Debridement

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
After Sharp Debridement
Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Wound Dressing
Aseptic technique;
Change dressings daily, more regularly when strike through noted on dressing;
Diabetic Foot wounds should be kept dry and clean at all times;
Do NOT soak the foot or bath/shower the patient;
Apply saline with gauze to clean wound surface.

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Wound Dressings cont’d
Do NOT use hydrocolloid dressing as occlude and macerate the wound;
Simple wound dressing over ulcer site and secured;
Offload with appropriate foot wear/bed rest/turn patient regularly;
Review wound regularly and refer early if wound deteriorates;
Antibiotics?

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Infection raises blood sugar
High blood sugar inhibits body fighting infection
Infection gets worse
The Cycle of Diabetic Infections

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Criteria for Wound Dressing Selection
Does the dressing:
Stay intact & in-situ?Prevent leakage?Cause maceration/allergy or sensitivity?Reduce pain?Reduce odour?
Is the dressing:
Comfortable, conformable, flexible?Suitable for leaving in place for the duration?Easy to remove?Easy to use?Cost effective?

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Who to refer to the Diabetes Specialists in WPH
New Ulceration;
New Swelling;
New Discoloration over all or part of the foot;
People with painful leg and foot symptoms whose diabetic control is poor;
Deterioration of a presenting wound: ↑Odour ↑Discharge ↑Redness ↑Pain ↑Swelling ↑Feeling unwell
Suspected Charcot – Plaster Nurse.

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Where to Refer
Diabetes Specialist Team: Dr Dove/Dr Akinsola Ward 5 Ext ???
Tissue Viability Nursing Team Ext ???
Vascular Team Ext ???
Plaster Room Ext ???
Podiatry Department Ext 4221 (Fax referral: stating Patient Diabetic with active ulcer)

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
On Discharge….. Acute problem contact Diabetes Centre Podiatry, King
Edward VII Hospital by:Fax on ext 6624.
Patient with diabetic complications. Referral to Community Podiatry Clinics based in Slough, Windsor, Ascot, Bracknell, Langley.
For type 1 or type 2 patient education or advice send for group education via the Diabetes Centre these Education Sessions are held in Community locations.

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Summary of Care Planning
Good glycaemic control Offloading pressure Safe removal of callus Safe removal of slough, necrotic tissue Treat infection Allow drainage of exudate Encourage patient compliance/patient education
Best form of treatment is prevention

Working with you for Better Health
Berkshire East
Community Health Services
Working with you for Better Health
Berkshire East
Community Health Services
Any Questions?