working to prevent fetal alcohol spectrum disorders through high school and middle school curricula...
Post on 18-Dec-2015
215 views
TRANSCRIPT
Working to Prevent Working to Prevent Fetal Alcohol Spectrum DisordersFetal Alcohol Spectrum Disorders
Through High School and Through High School and Middle School CurriculaMiddle School Curricula
This presentation was designed for use in This presentation was designed for use in Educating Teachers, Administrators and Others Who Educating Teachers, Administrators and Others Who
Work with Children in the School System.Work with Children in the School System.
FASD
Indiana FASDPreventionTaskforce

Fetal Alcohol Spectrum Fetal Alcohol Spectrum Disorders:Disorders:
What They Are and How They What They Are and How They Impact Your StudentsImpact Your Students
FASD
Indiana FASDPreventionTaskforce
History of Fetal Alcohol History of Fetal Alcohol Spectrum DisordersSpectrum Disorders
• The effects of parental alcohol use have been known since the time of Aristotle
• First described in the literature by Jacqueline Rouquette in 1957, although the French physician Paul Lemoine (1968) is credited with the first publication
FASD
www.nlm.nih.gov/hmd/greek/greek_aristotle.html
History of Fetal Alcohol History of Fetal Alcohol Spectrum DisordersSpectrum Disorders
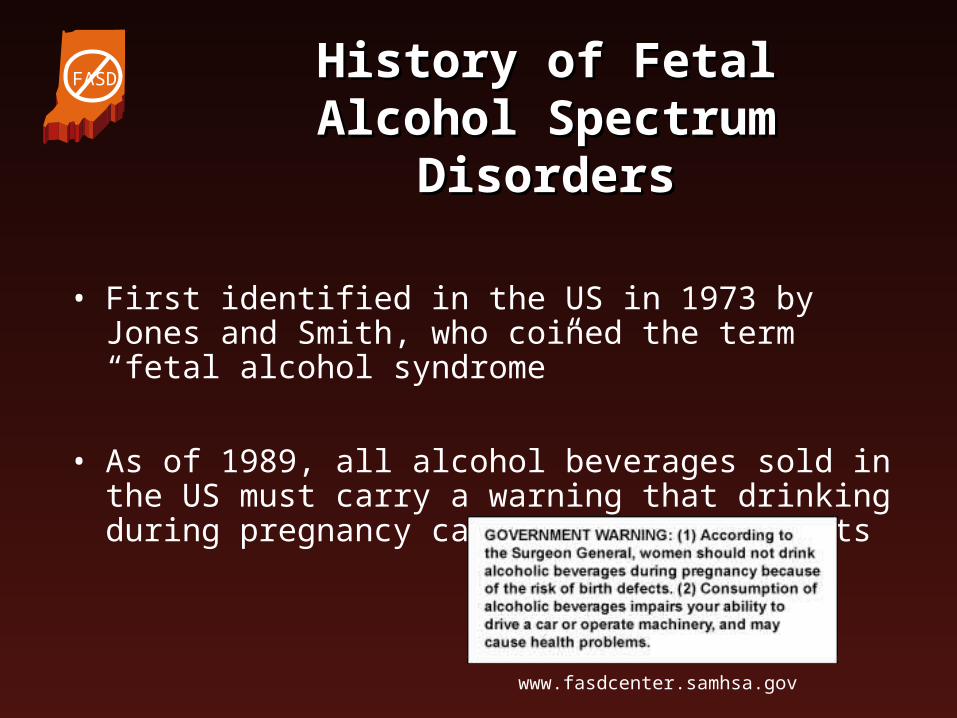
• First identified in the US in 1973 by Jones and Smith, who coined the term “fetal alcohol syndrome”
• As of 1989, all alcohol beverages sold in the US must carry a warning that drinking during pregnancy can cause birth defects
FASD
www.fasdcenter.samhsa.gov

History of Fetal Alcohol History of Fetal Alcohol Spectrum DisordersSpectrum Disorders
• In 1978, the term “fetal alcohol effects” (FAE) was coined to describe conditions that are presumed to be caused by prenatal alcohol exposure but don’t meet the diagnostic criteria of FAS
• In 1996, the Institute of Medicine of the National Institutes of Health proposed the terms partial FAS, alcohol-related neurodevelopmental disorder (ARND), and alcohol-related birth defects (ARBD)
• Now considered “fetal alcohol spectrum disorders”
FASD
History of Fetal Alcohol History of Fetal Alcohol Spectrum DisordersSpectrum Disorders
• “Fetal alcohol spectrum disorders (FASD) is an umbrella term describing the range of effects that can occur in an individual whose mother drank alcohol during pregnancy. These effects may include physical, mental, behavioral, and/or learning disabilities with possible lifelong implications. The term FASD is not intended for use as a clinical diagnosis.”
National Taskforce on Fetal Alcohol Syndrome and Fetal Alcohol Effects, 2004
FASD

Fetal Alcohol Spectrum Fetal Alcohol Spectrum Disorders (FASD)Disorders (FASD)
Possible Diagnoses– Fetal alcohol syndrome (FAS)
– Partial FAS (pFAS)
– Alcohol-related neurodevelopmental disorder (ARND)
– Alcohol-related birth defects (ARBD)
+ =
FAE (fetal alcohol effects) is an older term used to describe the last three listed above.
FASD
On any given day in the On any given day in the United States…United States…
• 10,657 babies are born
• 4 of these babies are born with spina bifida
• 1 of these babies is HIV positive
• 100 of these babies are born with a FASD
• 3 of these babies are born with muscular dystrophy
• 10 of these babies are born with Down syndrome
• 20 of these babies are born with FAS
From the Executive Summary of the IOM Report. FAS Community Resource Center. http://www.come-over.to/FASCRC
FASD
How Common is FAS and FASD?How Common is FAS and FASD?
• The prevalence of FAS is estimated to be about 1 in 500 to 1 in 1000 births
• The prevalence of FASD is estimated to be nearly 1 in 100 births
Eustance LW et al., 2003
FASD

How much is too much?How much is too much?
• The more alcohol consumed during pregnancy, the higher the risk for adverse effects– Binge drinking is particularly harmful!
• No amount of alcohol has been proven ‘safe’ to consume during pregnancy
• Every FASD is 100% preventable!
FASD

What is a Drink?What is a Drink?
A Binge is four or more drinks on one occasion for a woman; five or more for a man
A Drink is 12 ounces of beer, five ounces of wine, or 1.5 ounces of hard liquor
= =
FASD
The Effect of Alcohol onThe Effect of Alcohol on a Baby’s Development a Baby’s Development
• Alcohol freely crosses the placenta from the mother to the baby
• Blood alcohol levels of the baby are approximately equal to that of the mother, within minutes of consumption
• The critical period is the entire pregnancy
FASD
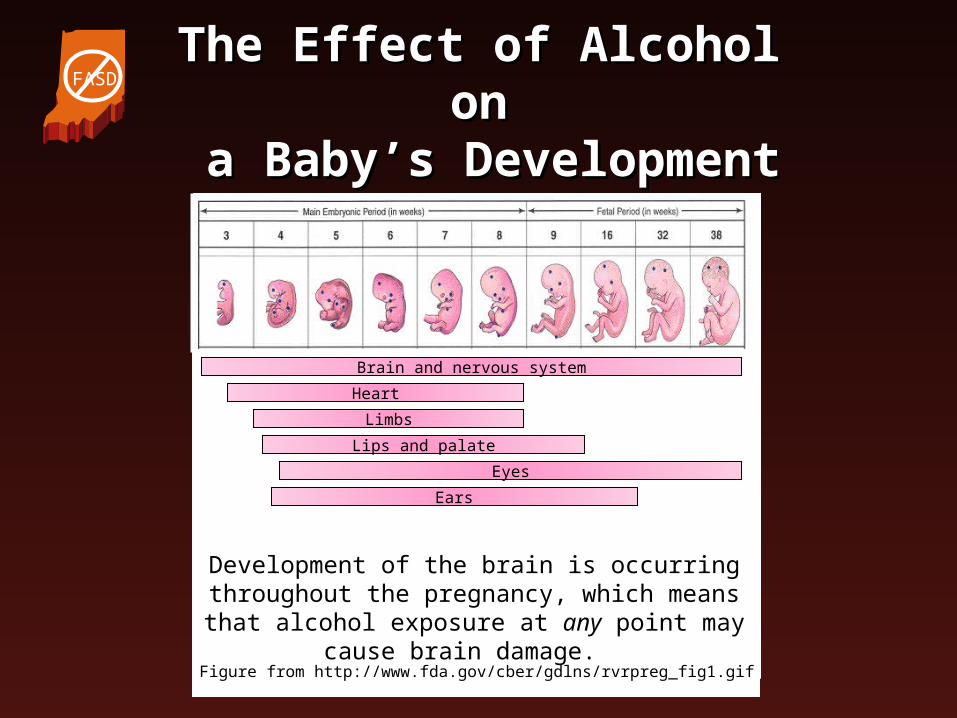
The Effect of Alcohol onThe Effect of Alcohol on a Baby’s Development a Baby’s Development
Brain and nervous system
Heart
Limbs
Lips and palate
Ears
Eyes
Figure from http://www.fda.gov/cber/gdlns/rvrpreg_fig1.gif
Development of the brain is occurring throughout the pregnancy, which means that alcohol exposure
at any point may cause brain damage.
FASD
The Diagnosis of FASThe Diagnosis of FAS
Defined by four criteria:1. Exposure to alcohol while in the womb
2. Characteristic facial features
3. Growth problems
4. Involvement of the central nervous system (the brain)
FASD

FAS Facial FeaturesFAS Facial Features
FASD
pubs.niaaa.nih.gov
NOTE: Although these features are associated with fetal alcohol syndrome, they may also be seen in people who do not have a FASD.
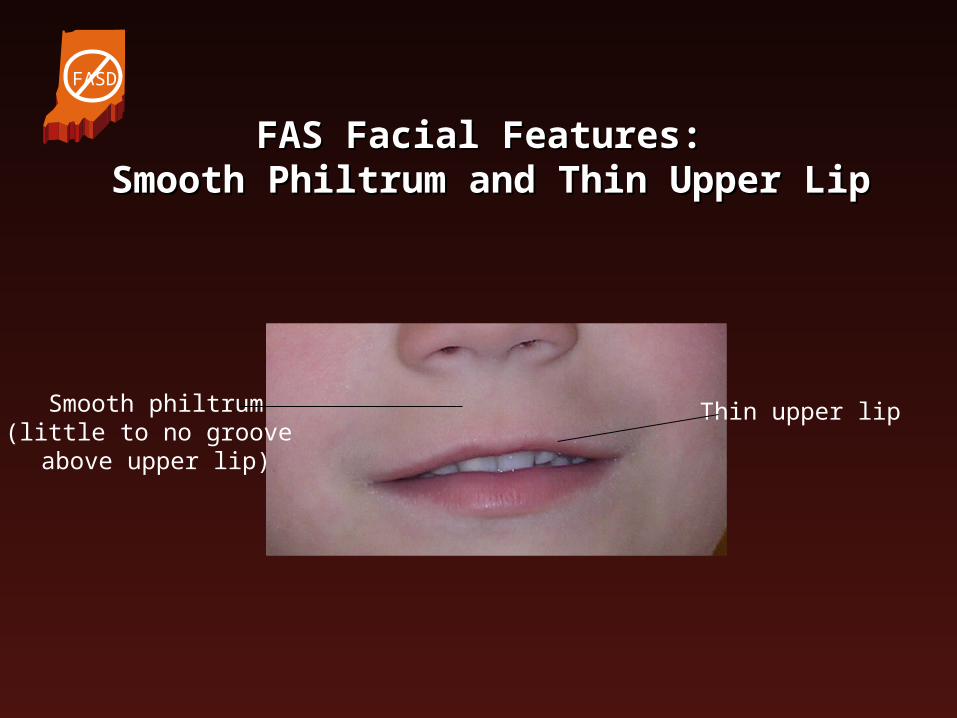
FAS Facial Features: FAS Facial Features: Smooth Philtrum and Thin Upper LipSmooth Philtrum and Thin Upper Lip
Thin upper lipSmooth philtrum(little to no groove above upper lip)
FASD
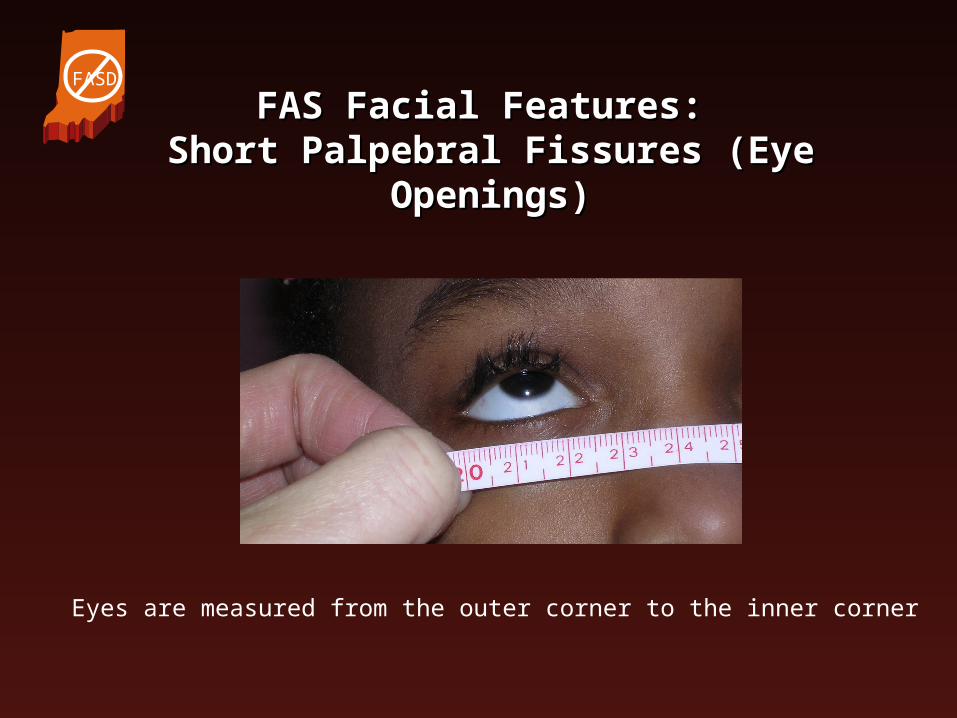
FAS Facial Features: FAS Facial Features: Short Palpebral Fissures (Eye Openings)Short Palpebral Fissures (Eye Openings)
Eyes are measured from the outer corner to the inner corner
FASD

FAS Facial FeaturesFAS Facial Features
FASD
www.come-over.to/FAS/JohnGrowsUp.htm

The Effect of Alcohol The Effect of Alcohol on Growthon Growth
• Alcohol consumption increases the risk for having a baby with growth problems
• After birth, exposed children may continue to have a decreased growth rate and subsequent short stature
Day and Richardson, 2004, AJMG 127C:28-34. www.cdc.gov/growthcharts
FASD

Alcohol Affects Alcohol Affects Overall Brain SizeOverall Brain Size
Photo by Sterling Clarren, MDhttp://www.come-over.to/FAS/FASbrain.htm
Brain of a healthy baby
Brain of a baby exposed to alcohol
FASD

Alcohol Affects Brain FunctionAlcohol Affects Brain Function
• Developmental delays
• Learning difficulties
• Mental retardation
• Speech/language disorders
• Problems with memory, perception, sensory integration, or tactile defensiveness
FASD
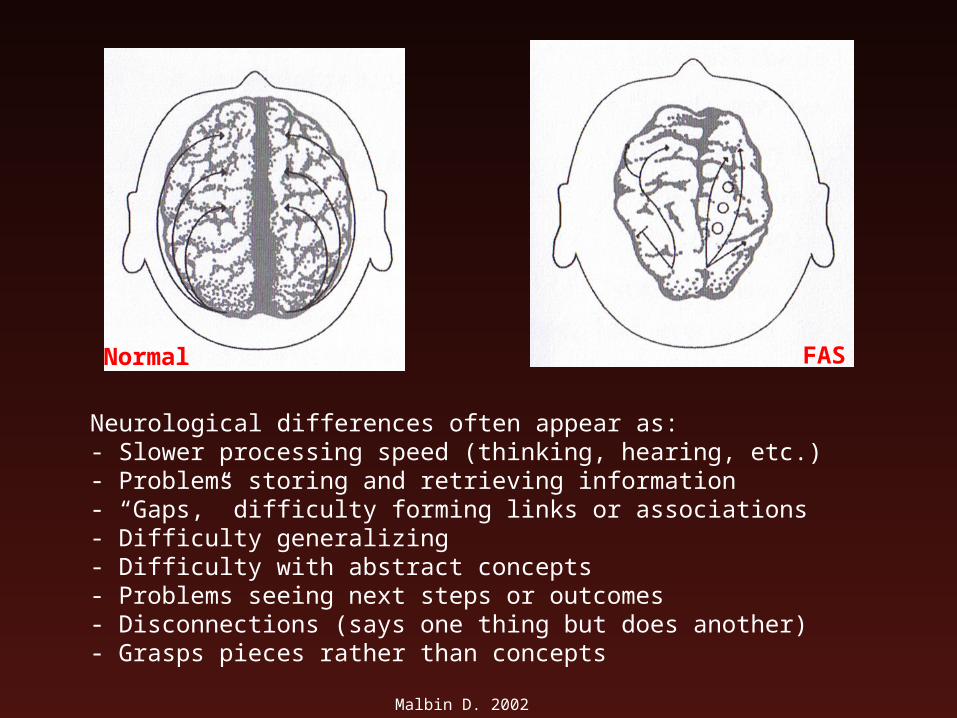
FASNormal
Malbin D. 2002
Neurological differences often appear as:- Slower processing speed (thinking, hearing, etc.)- Problems storing and retrieving information- “Gaps,” difficulty forming links or associations- Difficulty generalizing- Difficulty with abstract concepts- Problems seeing next steps or outcomes- Disconnections (says one thing but does another)- Grasps pieces rather than concepts
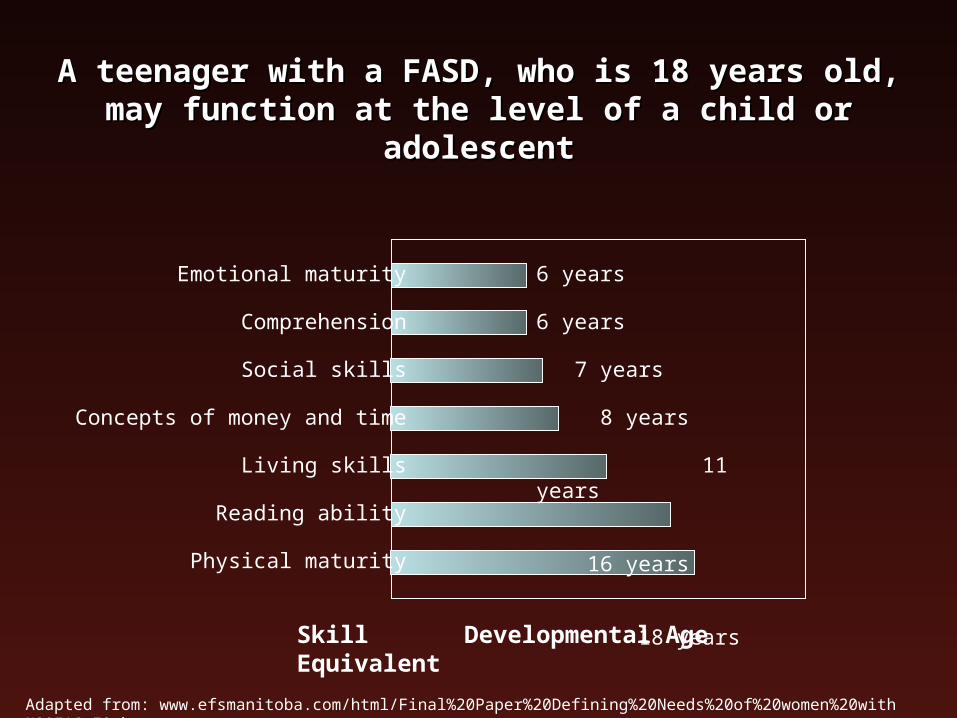
A teenager with a FASD, who is 18 years old, may A teenager with a FASD, who is 18 years old, may function at the level of a child or adolescentfunction at the level of a child or adolescent
Emotional maturity
Comprehension
Social skills
Concepts of money and time
Living skills
Reading ability
Physical maturity
6 years
6 years
7 years
8 years
11 years
16 years
18 years
Skill Developmental Age Equivalent
Adapted from: www.efsmanitoba.com/html/Final%20Paper%20Defining%20Needs%20of%20women%20with%20FAS_E2.htm
Primary vs. Secondary Primary vs. Secondary DisabilitiesDisabilities
• Primary disabilities result from brain damage due to the alcohol exposure
• Secondary disabilities develop over time due to lack of intervention and unmet needs – they are believed to be preventable
FASD

Secondary Disabilities in FASDSecondary Disabilities in FASD
• Mental health issues• Disrupted school
experiences• Inappropriate sexual
behavior• Trouble with the law• Confinement in jail or
treatment facilities
• Alcohol and drug problems• Dependent living• Employment problems
http://come-over.to/FAS/
FASD
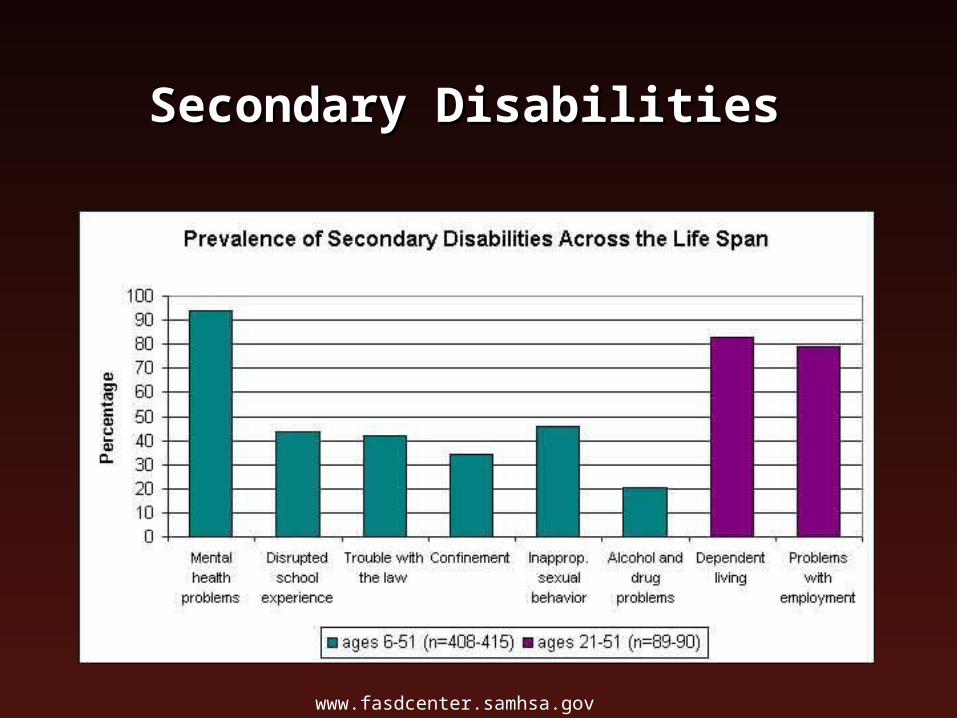
Secondary DisabilitiesSecondary Disabilities
www.fasdcenter.samhsa.gov

Long Term Consequences Long Term Consequences of FASof FAS
• Only 3% of children lived with biological mother
• Independent living was uncommon
• Poor behavior was common
• Average academic function was between 2nd and 4th grade
FASD
(Streissguth et al. 1991)
The Cost of FASThe Cost of FAS
• The comprehensive lifetime cost of one baby with FAS is at least $2 million
• The cost to American taxpayers for FAS is estimated to be $5 million a day, or up to $6 billion each year
Lupton, et al. 2004; Substance Abuse and Mental Health Services Administration
FASD
Strengths of Strengths of Individuals with a FASDIndividuals with a FASD
• Friendly • Likeable• Helpful• Determined• Loving, caring, kind,
sensitive, loyal and compassionate
• Energetic and hardworking
• Have points of insight• Not malicious• Cuddly and cheerful• Happy in an accepting and
supportive environment• Fair and cooperative• Spontaneous, curious, and
involved
FASD

Strengths of Strengths of Individuals with a FASDIndividuals with a FASD
• Highly verbal• Highly moral with a deep sense of fairness• Kind with younger children and animals• Creative• Eager to please
FASD

Strengths of Strengths of Individuals with a FASDIndividuals with a FASD
• Learn by doing, by being shown, and/or by relationship
• Learn through consistency, continuity, and relevance
• Able to participate in problem solving with appropriate support
• Often have a strong long-term visual memory
FASD

Working with individuals Working with individuals with a FASDwith a FASD

Working with Working with Individuals with a FASDIndividuals with a FASD
• Build on strengths
• Use teaching strategies that focus on these strengths
FASD

A Paradigm ShiftA Paradigm Shift
“We must move from viewing the individual as failing if s/he does not do well in a program to viewing the program as not providing what the individual needs in order to succeed.”
- Dubovsky, 2000
FASD
Systems of Care for Those Systems of Care for Those with a FASDwith a FASD
• Healthcare services
• Educational services
• Social and community services
• Legal and financial services
FASD

Management of Management of Children with a FASDChildren with a FASD
• Physical, occupational, and speech therapies• Psychiatrist or psychologist
– Medications for ADHD, anxiety, depression, seizures, explosive behavior, etc.
– Counseling
• Pediatrician or developmental pediatrician familiar with FASD
• Other specialists as needed
FASD

Strategies for Working with Strategies for Working with Individuals Who Have a FASDIndividuals Who Have a FASD
• For executive function deficits:– Use short-term consequences specifically
related to the behavior– Establish achievable goals– Provide skills training and use a lot of role
playing
FASD
Strategies for Working with Strategies for Working with Individuals Who Have a FASDIndividuals Who Have a FASD
• For information processing problems:– Check for understanding– Use literal language– Teach the use of calculators and computers– Look for misinterpretations of words or actions
and discuss them when they occur
FASD
Strategies for Working with Strategies for Working with Individuals Who Have a FASDIndividuals Who Have a FASD
• For memory problems:– Provide one direction or rule at a time and
review rules regularly– Provide repetition of instructional strategies– Use frequent reminders
FASD
Strategies for Working with Strategies for Working with Individuals Who Have a FASDIndividuals Who Have a FASD
• For sensory integration issues:– Simplify the individual’s environment– Take steps to avoid sensory triggers, which
may include:• Wearing clothes with tags or clothes made of certain fabrics• Being in overly stimulating environments (i.e. crowded and
loud places)• Being in the presence of bright lights
FASD
Strategies for Working with Strategies for Working with Individuals Who Have a FASDIndividuals Who Have a FASD
• For self-esteem and personal issues:– Use person-first language– Do not isolate the person– Address issues of grief and loss– Do not blame people for what they cannot do– Set the person up to succeed
FASD
Strategies for Working with Strategies for Working with Individuals Who Have a FASDIndividuals Who Have a FASD
• To facilitate communication:– Use a slow pace and soft tone– Use simple, concrete directions and cues– Use more than one form of communication– Avoid the use of idioms– Avoid sarcasm– Use simple, clear language
FASD
Strategies for Working with Strategies for Working with Individuals Who Have a FASDIndividuals Who Have a FASD
• To facilitate learning:– Allow longer periods to learn and/or complete
tasks– Break skills into smaller steps– Use concrete examples– Teach skills in the environment in which they
are to be used
FASD
Strategies for Working with Strategies for Working with Individuals Who Have a FASDIndividuals Who Have a FASD
• Provide a stable, predictable nurturing environment
• Concentrate on strengths and talents• Accept the child’s limitations• Be consistent with discipline, school, and
behaviors…• Use positive reinforcement• Closely supervise and be a good role
model!• Honor the person’s feelings• REPEAT, REPEAT, REPEAT!
FASD
Strategies for Working with Strategies for Working with Individuals Who Have a FASDIndividuals Who Have a FASD
• For teenagers:– Focus education on job training and daily
living skills– Closely monitor and supervise– Moderately increase responsibilities– Provide clear guidance/rules about
behavior– Provide sex education– Provide appropriate/safe recreational
activities
FASD
Strategies for Working with Strategies for Working with Individuals Who Have a FASDIndividuals Who Have a FASD
• Discipline:– Traditional behavioral interventions
typically don’t work– Consider whether the behaviors reflect
neurological differences– Consider the environment– Invite the person into to the discussion
and try to identify “stuck points”
FASD
Key Words to RememberKey Words to Remember
• Concrete• Consistent• Repetition• Routine• Simplicity• Specific• Structure• Supervision
FASD

For More InformationFor More Information
• Fetal Alcohol Spectrum Disorders: Trying Differently Rather Than Harder, by Diane Malbin, MSW. Available at www.FASCETS.org.
• Fetal Alcohol Syndrome: A Parents Guide to Caring for a Child Diagnosed with FAS, by Leslie Evans, MS, et al. Available for download at http://otispregnancy.org/pdf/FAS_booklet.pdf
• Fetal Alcohol Syndrome, Fetal Alcohol Effects: Strategies for Professionals, by Diane Malbin, MSW. Hazelden Foundation, Center City, MN.
• Fetal Alcohol Syndrome: Practical Suggestions and Support for Families and Caregivers, by Kathleen Tavenner Mitchell, MHS, LCADC, and the National Organization on Fetal Alcohol Syndrome. Available at http://www.nofas.org/estore
FASD
ReferencesReferences
• Alan Guttmacher Institute. Facts on American teens’ sexual and reproductive health. www.guttmacher.org/pubs/fb_ATSRH.htm
• The Centers for Disease Control and Prevention. Fetal alcohol spectrum disorders. www.cdc.gov/ncbddd/fas/fasprev.htm
• Day NL and Richardson GA. 2004. An analysis of the effects of prenatal alcohol exposure on growth: A teratologic model. American Journal of Medical Genetics Part C. 127C:28-34.
• Eustace LW, et al. 2003. Fetal alcohol syndrome: A growing concern for healthcare professionals. Journal of Obstetric, Gynecologic, and Neonatal Nursing. 32:215-221.
• The Institute of Medicine. 1996 Report on FAS. http://www.come-over-.to/FAS/ IOMsummary.htm• Lupton C, et al. 2004. Cost of fetal alcohol spectrum disorders. American Journal of Medical
Genetics Part C. 127C:242-50.• Mattson SN, et al. Teratogenic effects of alcohol on brain and behavior. National Institute on
Alcohol Abuse and Alcoholism. http://pubs.niaaa.nih.gov/publications/ arh25-3/185-191.htm• Spadoni AD, et al. 2007. Neuroimaging and fetal alcohol spectrum disorders. Neuroscience and
Biobehavioral Reviews 31:239-245.• Streissguth AP, et al. 1991. Fetal alcohol syndrome in adolescents and adults. Journal of the
American Medical Association. 265(15):1961-7. • Streissguth AP, et al. 2004. Risk factors for adverse life outcomes in fetal alcohol sydnrome and
fetal alcohol effects. Developmental and Behavioral Pediatrics 25(4):228-238.• Substance Abuse and Mental Health Services Administration Fact Sheets.
http://www.fasdcenter.samhsa.gov/grabGo/factSheets.cfm
FASD

Helpful WebsitesHelpful Websites
• National Organization on Fetal Alcohol Syndrome- www.nofas.org
• Fetal Alcohol Syndrome, Education and Training Services, Inc.- www.fascets.org
• The FASD Center for Excellence, Substance Abuse and Mental Health Services Administration- www.fascenter.samhsa.gov
• FASlink- http://www.acbr.com/fas/• The Arc- http://www.thearc.org/fetalalcohol.html• The Centers for Disease Control and Prevention-
http://www.cdc.gov/ncbddd/fas/default.htm
FASD

Indiana ResourcesIndiana Resources
• The Fetal Alcohol Syndrome Center of Indiana - Indiana University Medial Center
975 West Walnut Street, IB 130Indianapolis, IN 46202Phone: 317-274-2450 Fax: 317-274-2387 Provides diagnosis, education and patient advocacy for those
affected with prenatal alcohol exposure.
• CNS - Center for Neurobehavioral Sciences3010 E. StateFt. Wayne, IN 46805Phone: 260-471-2300 Toll Free: 1-800-901-8416Provides therapy, education and patient advocacy for those
affected with prenatal alcohol exposure. Organizes a support group for parents and caregivers (and other interested parties) of those with a FASD.
FASD
Indiana ResourcesIndiana Resources
• Indiana Department of Health - IN Perinatal Network (IPN), Prenatal Substance Use Prevention Program (PSUPP)
2 N Meridian Street; Indianapolis, IN 46204Phone: 317-233-1269 Fax: 317-233-1300
Referrals and early intervention for substance-using pregnant
women. Training for professionals.
• Indiana Protection and Advocacy Services4701 N Keystone Avenue, Suite 222, Indianapolis, IN 46205 Phone: 800-622-4845 or 317-722-5555
Fax: 317-722-5564Statewide agency for persons with developmental
disabilities.www.in.gov/ipas
FASD

www.health.state.mn.us/fas/catalog

Slides developed by: Lisa J. Spock, Ph.D., C.G.C.Gordon Mendenhall, Ed.D.
Assisted by: David D. Weaver, M.D.Becky Kennedy, M.Ed.James M. Ignaut, M.A., M.P.H., C.H.E.S.
Supported by: Indiana University School of MedicineIndiana State Department of HealthIndiana Department of EducationUniversity of Indianapolis