workforce and career path options for pharmacy assistants...
TRANSCRIPT

Attachment A
TELEPHONE STAKEHOLDER CONSULTATIONS

Table A1: Telephone Stakeholder Consultations
Organisation Name Position
Pharmacy Guild of Australia – QLD Branch
Robyn Ede Branch Director
Louise Sullivan Branch Director Pharmacy Guild of Australia – Tasmanian Branch Jenny Fitzgibbon Jenard Personnel and Training (contractor
delivering Guild training) Patrick Reid Branch President
Ann Dalton Branch Director
Pharmacy Guild of Australia –ACT Branch
Fiona Syphers Training Manager
Pharmaceutical Society of Australia (QLD)
Peter Mayne Branch President
Pharmaceutical Society of Australia (SA)
Grant Kardachi Branch President
Pharmacy Board of South Australia
Peter Halstead Registrar
Pharmacy Council of Western Australia
Bob Brennan Registrar
Department of Human Services, Victoria
Anne-Louise Carlton Senior Policy Analyst
New South Wales Health Leanne O’Shaunessy Deputy Director, Legal and Legislative Services
Queensland Health Sue Cawcutt Project Manager, Legislative Projects Unit
ACT Health Rhys Ollerenshaw Manager, Health Policy
Department of Health and Community Services, NT
Christine Quirke Policy and Research Officer, Health Professions Licensing Authority
Western Australian Department of Health
Susan Hillier Acting Director, Legal Services
Department of Health and Human Services, Tasmania
Len Armsby Director, Legislation Development Review

Attachment B
STAKEHOLDER TELEPHONE CONSULTATION TEMPLATES
Pharmacy Boards (QLD, SA, TAS, ACT, NT) Terminology (1) “Dispensary assistants”: What is your preferred terminology and why? Guidelines (2) Are there any guidelines that describe what work can be performed by a pharmacy assistant /
dispensary assistant? Is there a ratio of pharmacists-to-pharmacy assistants in the dispensary? Do you see a need for guidelines? Why / why not?
Training (3) What courses of training do you recognise as being required to fulfil the duties of a pharmacy
assistant / dispensary assistant? Role / Use (4) What roles does the Board feel comfortable for a dispensary assistant to undertake? For example,
stacking shelves in the dispensary, selecting medication of the shelves, preparing labels? (5) The major activities of a pharmacist in the dispensing process is to:
check the medication history; review the dispensed medication; counsel the patient.
Are there any areas of these processes that could be undertaken by a dispensary assistant, with the appropriate training and supervision by a pharmacist? What are the impediments to this expansion?
(6) How would you respond to the suggestion by some stakeholders that a new role should be created
that extends beyond the current dispensary assistant role which would sit in between a dispensary assistant and a pharmacist (with appropriate supervision, training and IT risk management support)?
(7) What is your attitude to expanding the role of pharmacy assistants in the non-dispensing areas?
What are the impediments to this expansion? (8) Are you aware of any instances involving the inappropriate use of dispensary assistants, or
pharmacy assistants in the dispensing process? For example, have there been any individual case hearings?

Guild Branch offices and PSA Brach offices (QLD, SA, TAS, NT, ACT, WA) Terminology (1) “Dispensary assistants”: What is your preferred terminology and why? Guidelines (2) Do you see a need for guidelines on the use of dispensary assistants? Why / why not? Role / Use (3) What roles does the (Guild / PSA) feel comfortable for a dispensary assistant to undertake? For
example, stacking shelves in the dispensary, selecting medication of the shelves, preparing labels? (4) The major activities of a pharmacist in the dispensing process is to:
check the medication history; review the dispensed medication; counsel the patient.
Are there any areas of these processes that could be undertaken by a dispensary assistant, with the appropriate training and supervision by a pharmacist? What are the impediments to this expansion?
(5) How would you respond to the suggestion by some stakeholders that a new role should be created
that extends beyond the current dispensary assistant role which would sit in between a dispensary assistant and a pharmacist (with appropriate supervision, training and IT risk management support)?
(6) What is your attitude to expanding the role of pharmacy assistants in the non-dispensing areas?
What are the impediments to this expansion? Training (7) What training programs are you aware of, for both dispensing and non-dispensing? Who provides
them? What are the take-up rates? (Guild only): Is the Guild branch office training the same as the National Guild training?
(8) Any ideas on the reasons behind the poor uptake of training? (9) Is the current Level 4 Certificate training sufficient for effective retail management tasks in
community pharmacy (including marketing, HR and retail operations)? General (10) How would you more effectively use dispensary assistants?
State Governments (QLD, SA, TAS, NT, ACT, WA) (1) What are the relevant Acts that regulate the operation of pharmacies in your state? (2) What are the relevant sections (if any) of your State’s Pharmacy Act are applicable to the practice
of pharmacy assistants or dispensary assistants? (3) What are the relevant sections (if any) of your State’s Pharmacy Regulations that are applicable to
the practice of pharmacy assistants or dispensary assistants? (4) What timeline is the state working towards for the implementation of the recommendations of the
Wilkinson Report? Are these changes going influence the role of pharmacy assistants and dispensary assistants?
(5) Are there likely to be any other policy changes regarding the Pharmacy Act in the next 12 months
that we should be aware of? (6) What is the state’s view of expanding the role of pharmacy assistants and dispensary assistants?

Attachment C
REGULATORY FRAMEWORK BY STATE

- AUSTRALIAN CAPITAL TERRITORY POLICY FRAMEWORK -
Regulatory Framework for ACT Pharmacy and Dispensary Assistants Tasks Supervision Training Comments Pharmacy Act 1931, No 10
Section 48 None None
Poisons and Drugs Act 1978
None None None
ACT Poisons and drug Regulations
None None None
Guidelines / Other Mechanisms
The ACT Board of Pharmacy does produce guidelines. There is no information on or any specific mention of pharmacy or dispensary assistants.
Extracts from the relevant acts are summarised below. Pharmacy Act 1931, No. 10, Section 48: “A pharmacist shall not-
(a) keep or maintain any shop for selling or supplying medicines or drugs, or for compounding or dispensing prescriptions unless such shop is, while open for business, constantly under his or her own control or that of some other registered pharmacist, as an assistant or agent of a registered pharmacist; (b) permit any person, other than a bona fide assistant or apprentice in the course of his or her employment and under his or her actual personal supervision, or a registered pharmacist, to sell or supply medicines or drugs or compound or dispense prescriptions; (c) carry on business except under the actual personal supervision of himself or herself or some other registered pharmacist;”

- NEW SOUTH WALES POLICY FRAMEWORK -
Regulatory Framework for New South Wales Pharmacy and Dispensary Assistants Tasks Supervision Training Comments Pharmacy Act 1964 ,No 48
Section 28 None None
Poisons and Therapeutic Goods Act 1966 No 31
None None None
NSW Pharmacy Regulations
None None None
Guidelines / Other Mechanisms
The NSW Board releases Bulletins periodically on the state of the pharmacy industry. We understand there are specific notes about the roles of Pharmacy and Dispensary Assistants appearing in some of these Bulletins.
Extracts from the relevant acts are summarised below. Pharmacy Act 1964, No 48, Section 28 “Medicines to be dispensed by pharmacists
(1) A person, other than a pharmacist or a person acting under the personal supervision of a pharmacist, must not dispense or compound any medicine on the order or prescription of a medical practitioner or nurse practitioner. (2) This section does not prevent an authorised person from dispensing medicine in the ordinary course of his or her profession:
(a) if the practitioner does not charge for the medicine more than its cost to the practitioner, or (b) if, because of the circumstances of the case (such as where the medicine is dispensed in a location in which there is no pharmacist), it would be unreasonable to require the medicine to be obtained from a pharmacist, or (c) in such circumstances as may be prescribed by the regulations.
(3) In this section:
authorised person means a medical practitioner, or a nurse practitioner who is authorised to dispense the medicine concerned under section 17A of the Poisons and Therapeutic Goods Act 1966.”

- NORTHERN TERRITORY POLICY FRAMEWORK -
Regulatory Framework for Northern Territory Pharmacy and Dispensary Assistants Tasks Supervision Training Comments Pharmacy Act Section 39 (b) None None -
Poisons and Dangerous Drugs Act
None None None -
Therapeutic Goods and Cosmetics Act
None None None -
Health Regulation
None None None -
Guidelines / Other Mechanisms
Copies of Board Guidelines do exist and may refer to how pharmacists use assistants.
Extracts from the relevant acts are summarised below. 39. Conduct of business by pharmacist
(1) A pharmacist shall not – (a) keep or maintain any dispensary for selling or supplying medicines or drugs, or for
compounding or dispensing prescriptions unless such dispensary is, while open for business, constantly under his own control or that of some other registered pharmacist, as an assistant or agent of a registered pharmacist;
(b) permit any person, other than a bona fide assistant or apprentice in the course of his employment and under his actual personal supervision, or a registered pharmacist, to sell or supply medicines or drugs or compound or dispense prescriptions;
(c) carry on business as a pharmacist except under the actual personal supervision of himself or some other registered pharmacist;
(d) practise pharmacy except in his own name;

- QUEENSLAND POLICY FRAMEWORK -
Regulatory Framework for Queensland Pharmacy and Dispensary Assistants Tasks Supervision Training Comments Pharmacy Act, 1976
Repealed by the State Government.
Health (Drugs and Poisons) Regulation 1996
None None None
Pharmacists Registration Act 2001
None None None
Queensland Pharmacy Regulations
None None None
Health Regulations 1996
None None None
Bulletins Yes Yes Yes

- SOUTH AUSTRALIA FRAMEWORK -
Regulatory Framework for South Australian Pharmacy and Dispensary Assistants Tasks Supervision Training Comments Pharmacists Act 1991
None None None -
Controlled Substances Act 1984
None None None -
SA Pharmacy Regulations
None None None -
Guidelines / Other mechanisms
No guidelines or bulletins exist for the regulation of pharmacy or dispensary assistants in South Australia

- TASMANIAN POLICY FRAMEWORK -
Regulatory Framework Tasmanian Pharmacy and Dispensary Assistants Tasks Supervision Training Comments
Pharmacy Act 1908, (No 33 of 1908)
None None None
Pharmacists Registration Act 2001 (No 90 of 2001)
None None None
Poisons Act 1971
None None None
Poisons Regulations 2002
None Section 44.6 and 44. 7
None
Guidelines / Other Mechanisms
None Section 24.1 None
Extracts from the relevant acts are summarised below. Poisons Regulations 2002 Section 44:
“(6) A person, other than a pharmaceutical chemist or an assistant under the direct personal supervision of a pharmaceutical chemist, must not dispense a prescription for a restricted substance.
Penalty: Fine not exceeding 10 penalty units.
(7) A pharmaceutical chemist or an assistant under the direct personal supervision of a pharmaceutical chemist, subject to this regulation, is authorised to dispense a prescription for a restricted substance.”

- VICTORIAN POLICY FRAMEWORK -
Regulatory Framework for Victorian Pharmacy and dispensary Assistants Tasks Supervision Training Comments Pharmacists Act, 1974
None Section 28 None
Drugs, Poisons and Controlled Substances Act 1981
None None None
Regulation None None None Guidelines / Other Mechanisms
Division 5 – Section 485
Division 5 Section 482
Division 5 Section 483, 484A
Extracts from the relevant acts are summarised below.
28. Personal supervision of pharmacy or pharmacy department (1) When a pharmacy or a pharmacy department is open for business it shall at all times be
personally supervised by a pharmacist.
(2) Where a pharmacy or pharmacy department which is open for business is not personally supervised by a pharmacist—
(a) the pharmacist who ordinarily conducts the pharmacy practice; and (b) the pharmacist (if he is not the pharmacist referred to in paragraph (a)) who had in
respect of that period of time been placed in charge of and had undertaken personally to supervise the conducting of the pharmacy practice—
shall severally be guilty of an offence against this Act. Penalty: 25 penalty units.
(4) In this section "personally supervised by a pharmacist" means personally supervised by a pharmacist who is present at the pharmacy or the pharmacy department.

- WESTERN AUSTRALIA POLICY FRAMEWORK -
Regulatory Framework for Western Australian Pharmacy and Dispensary Assistants Tasks Supervision Training Comments
Pharmacy Act 1964
None Section 39 None -
Poisons Act 1964
None None None -
Pharmacy Regulation
None None None -
Guidelines / Other mechanisms
No guidelines or bulletins exist for the regulation of pharmacy or dispensary assistants in Western Australia
Extracts from the relevant acts are summarized below. 39. Dispensing
(1) A person shall not carry out the dispensing of any medicine or drug unless he is --
(a) a pharmaceutical chemist; (b) a person who carries out such dispensing under the immediate personal supervision of a pharmaceutical chemist; (c) a medical practitioner; or (d) a dentist or veterinary surgeon acting in the course of his profession.
(2) For the purposes of this section, a person shall be deemed not to be under the immediate personal supervision of a pharmaceutical chemist in a pharmacy if the number of persons engaged in dispensing medicine or drugs in that pharmacy who are not pharmaceutical chemists exceeds the number of pharmaceutical chemists exercising such supervision in that pharmacy.

Attachment D
SURVEY FORMS AND EXPLANATORY MATERIAL

PO Box 10086 Gouger Street Adelaide SA 5000 Level 1, 65 Henley Beach Road, Mile End SA 5031 Telephone: (08) 8150 5555 Facsimile: (08) 8150 5599
8th October 2003 Dear Pharmacy Manager/Owner,
Workforce and Career Options for Pharmacy Assistants The Pharmacy Guild of Australia has appointed Healthcare Management Advisors (HMA) to identify areas of current community pharmacy practice that may, with the provision of appropriate training, be assumed by dispensary and/or pharmacy assistants. As part of the consultancy, HMA are undertaking a limited, randomly selected survey of community pharmacies around Australia. The results of the survey will be analysed to develop a clear understanding of current roles performed by pharmacy and dispensary assistants, the training available - including its use - and views on the potential future roles of pharmacy and dispensary assistants. This survey has been approved by the Pharmacy Guild (Survey Approval No 543, AAA Rating) and the Commonwealth Government (Statistical Clearing House Approval Number 01435-01). Your input into this study would be greatly appreciated. We will pay the pharmacy $25 for completing the survey forms, a small recognition of the time invested (around 10 to 15 minutes for an average sized pharmacy). The survey should be completed on any weekday up until Friday 24th October 2003. Brief guidelines on completing the survey are attached to this letter. Pharmacy responses are confidential and no identifying information will be kept with the questionnaire. You will, however, need to include your name and address at the end of the questionnaire so we can send you a cheque. The unique pharmacy identifier will be deleted once processing of the survey is complete and will not be advised to third parties, including the Guild or the Department. Please arrange for the completion of the enclosed forms and their return in the enclosed reply paid envelope by Friday 24th October 2003. Thankyou for your help in this important study. Yours sincerely, Wayne Kinrade Project Director

Page 1.
Guidelines for Completing the Survey 1 SURVEY TIMING The survey can be completed on any given weekday at your convenience, up until Friday 24th October 2003. 2 SURVEY PROCESS Figure 1 below illustrates the simple process to complete the survey.
Figure 1: Survey Completion Process
This survey package contains three types of survey forms:
Survey Form 1, which should be completed by the pharmacist manager/owner. This is the white form in the package.
Survey Form 2, which should be completed by pharmacists working in your pharmacy on the day of the survey (other than the pharmacist manager/owner who completes Survey Form 1). This is the blue form in the package.
Survey Form 3, which should be completed by each pharmacy and dispensary assistant working in your pharmacy on the day the survey is undertaken (we have enclosed a number copies). These are the yellow forms in the package.
If you have not received a copy of each of these survey forms please contact HMA on the phone numbers below. Distribute survey forms to staff On the day you chose to complete the survey, you should distribute the relevant survey forms to your staff. If you need additional forms you can make photocopies, or you can contact HMA on the phone numbers below. Complete Survey Forms The pharmacist Manager/Owner should complete Survey Form 1, including the payment section at the end so that we can reimburse the pharmacy for participation. Any pharmacist, other than the pharmacist manager/owner, should complete Survey Form 2. If there is more than one pharmacist working on the day of the survey, they need to also complete a copy of Survey Form 2. All pharmacy and dispensary assistants working on the day of the survey need to each complete a Survey Form 3. Collect survey forms from staff Each copy of Survey Form 2 and Survey Form 3 has an envelope attached so staff can return their confidential responses to you.
Receive Survey
Package
Distribute Survey Forms
to Staff
Complete Survey Forms
Collect Survey Forms
from Staff
Return Survey Forms
to HMA

Page 2.
Please collect these envelopes from your staff and put them in the reply paid A4 envelope included in this package. Return survey forms Please return the completed survey forms to HMA’s Adelaide office using the pre-addressed, reply paid A4 envelope no later than Friday 24th October 2003. Please ensure you have included all the completed Survey Form 2s and Survey Form 3s collected from the pharmacists and pharmacy/dispensary assistants that were working on the day of the survey. 3 SURVEY PAYMENT We will pay the pharmacy $25 as a small recognition of the time invested to complete the survey forms. Upon receipt of the returned completed survey package, HMA will post a cheque to the pharmacy. 4 CONTACT DETAILS If you require further information or assistance, or need additional survey forms, we encourage you to contact an HMA staff member:
Wayne Kinrade, Project Manager: (03) 8415 0935
Malcolm Skene: (03) 8415 0936
Dave Menting: (03) 8415 0937 We would like to thank you for your cooperation and support in conducting this survey.

Survey Form 1
Approval Number 01435 - 01
Page 1.
This form is to be completed by the PHARMACIST MANAGER / OWNER. 1. Which of the following best describes the location of the pharmacy? (tick one only) Large shopping centre / mall. Strip shopping in large urban / suburban or regional setting. Neighbourhood / strip centre in a small town. Pharmacy located in a private hospital. Pharmacy located in a medical centre.
2. What model of dispensing is used at the pharmacy? (tick one only) Traditional. Semi-Forward. Forward.
3. What is the average number of scripts processed in a week at the pharmacy? (tick one only) 0 – 400. 401 – 800. 801 – 1200. 1201 – 1600. 1601 – 2000. More than 2000 scripts per week.
4. Which of the following best describes group membership of the pharmacy? (tick one only) Not in a group. Friendly Societies. Amcal. Guardian. Chemmart. Terry White.
Other group (please specify) ___________________
5. What is the estimated turnover of the pharmacy? (tick one only) Less than $1m. 2.5 – $3.0m. 1.0 – $1.5m. 3.0 – $3.5m. 1.5 – $2.0m. 3.5 – $4.0m. 2.0 – $2.5m. Greater than $4m.
6. What is an approximate estimate of the pharmacy’s turnover for each of the following product
categories? (a)
Prescription sales _____ % of total turnover. S2 and S3 medicines _____ % of total turnover. Complementary medicines _____ % of total turnover. Other _____ % of total turnover. Total 100 %
(a) To the nearest 10 per cent is adequate.

Page 2.
7. Is this pharmacy accredited under QCPP? (tick one only) No. Yes. Month/Year accredited __ __ / 200__
8. How long have you worked as a pharmacist in community pharmacy? (tick one only) Less than 1 year. 11 – 20 years. 1 – 5 years. 21 – 30 years. 6 – 10 years. More than 30 years.
9. There has been extensive discussion about the correct term used to describe staff trained to work in the
dispensary. Do you think that they should be referred to as: (tick one only) Pharmacy assistant? Dispensary assistant? Dispensary technician? Other (please specify) ______________________ For the remainder of this survey we will use the term ‘dispensary assistants’.
10. Is a dispensary assistant employed in this pharmacy? (tick one only) No (go to question 12). Yes.
11. If yes, what is the nature of their training in the dispensary? (tick one only) None. On the job. Certificate Level 3 (or equivalent) training delivered by the Pharmacy Guild. Certificate Level 3 (or equivalent) training delivered by another provider.
12. What is this pharmacy’s attitude to training of pharmacy assistants and dispensary assistants? (tick one only) Not my responsibility. Encouraged, but training should be paid for by staff. Encouraged, and the pharmacy is prepared to share the training cost with an employee. Encouraged, and the pharmacy is prepared to cover the training cost.

Page 3.
13. Please complete the following table on the staffing profile and work distribution within the pharmacy, on the day of the survey.
Functions performed (% of working time)
Front of Shop (e) Back of Shop (e)
Staff Type Remuneration per day ($) (a)
Hours worked on the day of the survey
(b) Dispensary S2/S3 and
other medicines
Other Retail Admin. Stock
Mgt. Total
Pharmacist Manager / Owner
(c) 100%
Pharmacist 1 100%
Pharmacist 2 100%
Pharmacist 3 100%
Trainee pharmacist 100%
Retail Manager 100%
Dispensary assistant 1 100%
Dispensary assistant 2 100%
Dispensary assistant 3 100%
Pharmacy assistant 1 100%
Pharmacy assistant 2 100%
Pharmacy assistant 3 100% Clerical or Administration 100%
(d)
(d)
Other
(a) Excluding salary on-costs (eg long service leave, workcover, payroll tax). (b) In estimating ‘hours per day’ include all activities involved in day-to-day management of the business. Exclude
other professional activities not directly involved in the day-to-day management eg professional development, involvement in Guild activities.
(c) Do not insert. Nominal salary based on the Guild Digest will be applied by HMA to ensure consistency across survey sites.
(d) Use this row where details need to be inserted on additional staff members. (e) Definitions: the proportion of time allocated to Front of Shop (dispensary, S2/S3 medicines and other retail) and
Back of Shop administration (including payroll administration, banking, sales, marketing planning and QCPP) and stock management (stock ordering and inventory management). For each individual should add to 100.
14. The following two tables are seeking your views on activities in the dispensary of this pharmacy. The
first table relates to the activities undertaken by dispensary assistants (Table 14a, please do not complete if there are no dispensary assistants working in the pharmacy). The second table relates to the activities undertaken by pharmacy assistants (Table 14b, please do not complete if there are no pharmacy assistants working in the pharmacy).
Page 4.
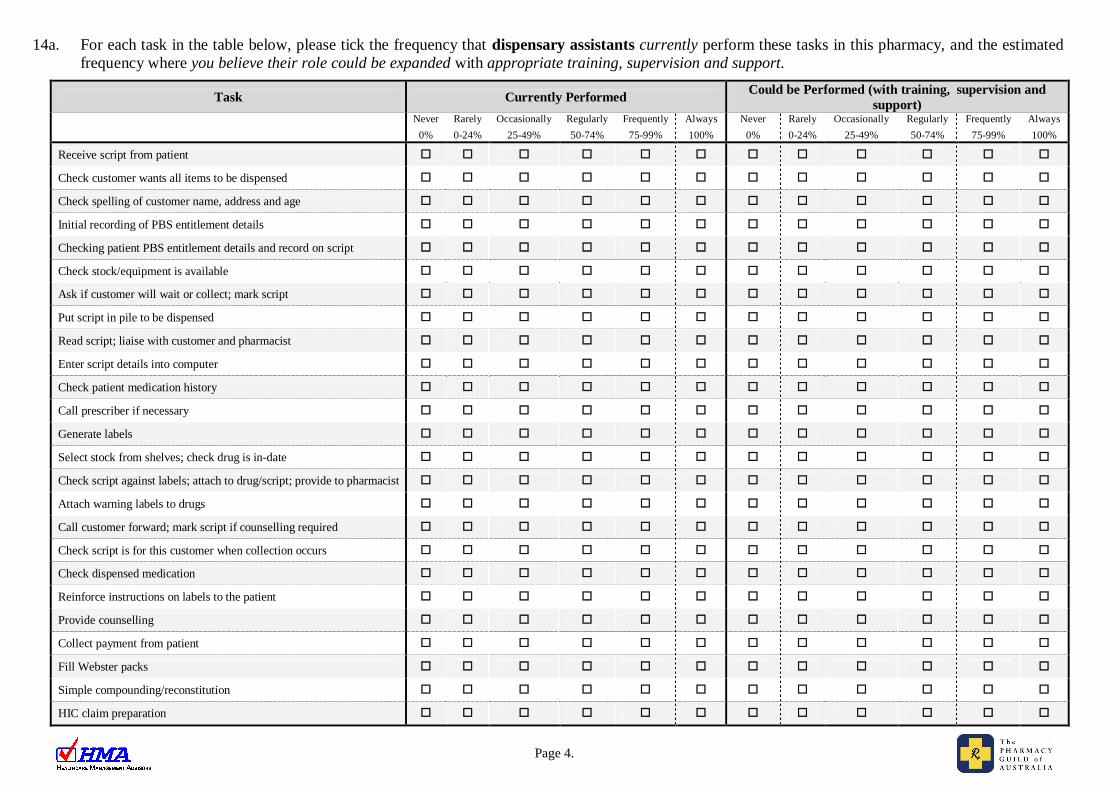
14a. For each task in the table below, please tick the frequency that dispensary assistants currently perform these tasks in this pharmacy, and the estimated frequency where you believe their role could be expanded with appropriate training, supervision and support.
Task Currently Performed Could be Performed (with training, supervision and support)
Never
0% Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Never 0%
Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Receive script from patient
Check customer wants all items to be dispensed
Check spelling of customer name, address and age
Initial recording of PBS entitlement details
Checking patient PBS entitlement details and record on script
Check stock/equipment is available
Ask if customer will wait or collect; mark script
Put script in pile to be dispensed
Read script; liaise with customer and pharmacist
Enter script details into computer
Check patient medication history
Call prescriber if necessary
Generate labels
Select stock from shelves; check drug is in-date
Check script against labels; attach to drug/script; provide to pharmacist
Attach warning labels to drugs
Call customer forward; mark script if counselling required
Check script is for this customer when collection occurs
Check dispensed medication
Reinforce instructions on labels to the patient
Provide counselling
Collect payment from patient
Fill Webster packs
Simple compounding/reconstitution
HIC claim preparation

Page 5.
14b. For each task in the table below, please tick the frequency that pharmacy assistants currently perform these tasks in this pharmacy, and the estimated frequency where you believe their role could be expanded with appropriate training, supervision and support.
Task Currently Performed Could be Performed (with training, supervision and support)
Never
0% Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Never 0%
Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Receive script from patient
Check customer wants all items to be dispensed
Check spelling of customer name, address and age
Initial recording of PBS entitlement details
Checking patient PBS entitlement details and record on script
Check stock/equipment is available
Ask if customer will wait or collect; mark script
Put script in pile to be dispensed
Read script; liaise with customer and pharmacist
Enter script details into computer
Check patient medication history
Call prescriber if necessary
Generate labels
Select stock from shelves; check drug is in-date
Check script against labels; attach to drug/script; provide to pharmacist
Attach warning labels to drugs
Call customer forward; mark script if counselling required
Check script is for this customer when collection occurs
Check dispensed medication
Reinforce instructions on labels to the patient
Provide counselling
Collect payment from patient
Fill Webster packs
Simple compounding/reconstitution
HIC claim preparation

Page 6.
15. This question seeks your views on staff activities outside the dispensary. For each task in the table below, please tick the frequency that pharmacy assistants and/or dispensary assistants currently perform these tasks in this pharmacy, and the estimated frequency where you believe their role could be expanded with appropriate training, supervision and support.
Task Currently Performed Could be Performed (with training, supervision and support)
Never
0% Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Never 0%
Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Selling/Product Knowledge Provide advice on S2 medicines (pharmacy only)
Provide advice on S3 medicines (pharmacist only)
Provide advice on complementary medicines (eg vitamins)
Provide advice on companion medicine sales
Provide other health care advice, product information, sell products Front of Shop Operations Pharmacy housekeeping (eg cleaning, rubbish removal)
Inventory management and ordering stock
Help maintain store safety and security Customer Service Greet pharmacy customers
Conduct point of sale administration and balance register at day end Administration Practices Operate and manage retail equipment (point of sale and till)
Prepare the pharmacy payroll Marketing Arrange product displays and merchandising
Prepare financial reports Quality and People Management Coordinate and supervise other pharmacy staff members
Recruit pharmacy staff
Perform formal assessments on staff members
Help to develop quality improvement procedures within the pharmacy
Train other pharmacy staff

Page 7.
Payment Details This section of the questionnaire will be used to reimburse you for your time. This payment is GST inclusive and should be treated in accordance with your normal business rules. Please note that all reports prepared by HMA will de-identify the pharmacy.
Please ensure your name and address is included. Pharmacy Name: ………………………………………………. Pharmacy Address: ………………………………………………. ………………………………………………. ………………………………………………. Date: / /2003 Day of week survey completed: ………………………………………………. Estimated TOTAL time taken to complete the survey forms ……………………………….. (ie total time of pharmacist manager/owner, pharmacists and pharmacy/dispensary assistants) – required for Commonwealth Government Statistical Clearing House reporting purposes.
Please collect the sealed envelopes from ALL staff completing the survey and place in the Reply Paid envelope attached.
THE END – THANK YOU FOR YOUR TIME

Survey Form 2
Approval Number 01435 - 01
Page 1.
A copy of this form is to be completed by ALL PHARMACISTS working in the pharmacy on the day of the survey (other than the Pharmacist Manager / Owner, who should complete Survey Form 1). The Pharmacy Guild of Australia has appointed Healthcare Management Advisors (HMA) to identify areas of current community pharmacy practice that may, with the provision of appropriate training, be assumed by dispensary and/or pharmacy assistants. As part of the consultancy, HMA are undertaking a limited randomly selected survey of community pharmacies around Australia. The survey has been approved by the Pharmacy Guild (Survey Approval No 543, AAA Rating) and the Commonwealth Government (Statistical Clearing House Approval Number 01435-01). Your input in this study would be greatly appreciated. Individual responses are confidential and no identifying information will be kept with the questionnaire. 1. How long have you worked as a pharmacist in community pharmacy? (tick one only) Less than 1 year. 11 – 20 years. 1 – 5 years. 21 – 30 years. 6 – 10 years. More than 30 years.
2. There has been extensive discussion about the correct term used to describe staff trained to work in the
dispensary. Do you think that they should be referred to as: (tick one only) Pharmacy assistant. Dispensary assistant. Dispensary technician. Other. Please specify ……………………………. For the remainder of this survey we will use the term ‘dispensary assistants’ for staff trained to work in the dispensary
3. The following two tables are seeking your views on activities in the dispensary of this pharmacy. The
first table relates to the activities undertaken by dispensary assistants in this pharmacy (if there are no dispensary assistants working in this pharmacy please do not complete Table 3a). The second table relates to the activities undertaken by pharmacy assistants (if there are no pharmacy assistants working in this pharmacy please do not complete Table 3b).

Page 2.
3a. For each task in the table below, please tick the frequency that dispensary assistants currently perform these tasks in this pharmacy, and the estimated frequency where you believe their role could be expanded with appropriate training, supervision and support.
Task Currently Performed Could be Performed (with training, supervision and support)
Never
0% Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Never 0%
Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Receive script from patient
Check customer wants all items to be dispensed
Check spelling of customer name, address and age
Initial recording of PBS entitlement details
Checking patient PBS entitlement details and record on script
Check stock/equipment is available
Ask if customer will wait or collect; mark script
Put script in pile to be dispensed
Read script; liaise with customer and pharmacist
Enter script details into computer
Check patient medication history
Call prescriber if necessary
Generate labels
Select stock from shelves; check drug is in-date
Check script against labels; attach to drug/script; provide to pharmacist
Attach warning labels to drugs
Call customer forward; mark script if counselling required
Check script is for this customer when collection occurs
Check dispensed medication
Reinforce instructions on labels to the patient
Provide counselling
Collect payment from patient
Fill Webster packs
Simple compounding/reconstitution
HIC claim preparation

Page 3.
3b. For each task in the table below, please tick the frequency that pharmacy assistants currently perform these tasks in this pharmacy, and the estimated frequency where you believe their role could be expanded with appropriate training, supervision and support.
Task Currently Performed Could be Performed (with training, supervision and support)
Never
0% Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Never 0%
Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Receive script from patient
Check customer wants all items to be dispensed
Check spelling of customer name, address and age
Initial recording of PBS entitlement details
Checking patient PBS entitlement details and record on script
Check stock/equipment is available
Ask if customer will wait or collect; mark script
Put script in pile to be dispensed
Read script; liaise with customer and pharmacist
Enter script details into computer
Check patient medication history
Call prescriber if necessary
Generate labels
Select stock from shelves, check drug is in-date
Check script against labels; attach to drug/script; provide to pharmacist
Attach warning labels to drugs
Call customer forward; mark script if counselling required
Check script is for this customer when collection occurs
Check dispensed medication
Reinforce instructions on labels to the patient
Provide counselling
Collect payment from patient
Fill Webster packs
Simple compounding/reconstitution
HIC claim preparation

Page 4.
4. This question seeks your views on staff activities outside the dispensary. For each task in the table below, please tick the frequency that pharmacy assistants and/or dispensary assistants currently perform each task in this pharmacy, and the estimated frequency where you believe their role could be expanded with appropriate training, supervision and support.
Task Currently Performed Could be Performed (with training, supervision and support)
Never
0% Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Never 0%
Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Selling/Product Knowledge Provide advice on S2 medicines (pharmacy only)
Provide advice on S3 medicines (pharmacist only)
Provide advice on complementary medicines (eg vitamins)
Provide advice on companion medicine sales
Provide other health care advice, product information, sell products Front of Shop Operations Pharmacy housekeeping (eg cleaning, rubbish removal)
Inventory management and ordering stock
Help maintain store safety and security Customer Service Greet pharmacy customers
Conduct point of sale administration and balance register at day end Administration Practices Operate and manage retail equipment (point of sale and till)
Prepare the pharmacy payroll Marketing Arrange product displays and merchandising
Prepare financial reports Quality and People Management Coordinate and supervise other pharmacy staff members
Recruit pharmacy staff
Perform formal assessments on staff members
Help to develop quality improvement procedures within the pharmacy
Train other pharmacy staff

Page 5.
Please place your completed form in the attached envelope, seal it and return it to the owner / senior pharmacist on duty.
THE END – THANK YOU FOR YOUR TIME

Page 1.
Survey Form 3 Approval Number 01435 - 01
A copy of this form is to be completed by ALL PHARMACY ASSISTANTS and DISPENSARY ASSISTANTS working in the pharmacy on the day of the survey. The Pharmacy Guild of Australia has appointed Healthcare Management Advisors (HMA) to identify areas of current community pharmacy practice that may, with the provision of appropriate training, be assumed by dispensary and/or pharmacy assistants. As part of the consultancy, HMA are undertaking a limited randomly selected survey of community pharmacies around Australia. The survey has been approved by the Pharmacy Guild (Survey Approval No 543, AAA Rating) and the Commonwealth Government (Statistical Clearing House Approval Number 01435-01). Your input in this study would be greatly appreciated. Individual responses are confidential and no identifying information will be kept with the questionnaire. 1. What is your main job in this pharmacy? (tick one only) Pharmacy assistant. Dispensary assistant/technician. Front of shop manager. Front of shop sales (including beauty services, photo processing, etc). Back of shop administrative support (including bookkeeping, orders).
2. Working in the dispensary. For each task in the table below, please tick how often you perform
these tasks in this pharmacy.
Task How often do you do this task?
Never
0% Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Receive script from patient
Check customer wants all items to be dispensed
Check spelling of customer name, address and age
Initial recording of PBS entitlement details
Checking patient PBS entitlement details and record on script
Check stock/equipment is available
Ask if customer will wait or collect; mark script
Put script in pile to be dispensed
Read script; liaise with customer and pharmacist
Enter script details into computer
Check patient medication history
Call prescriber if necessary
Generate labels
Select stock from shelves; check drug is in-date
Check script against labels; attach to drug/script; provide to pharmacist
Attach warning labels to drugs

Page 2.
Task How often do you do this task?
Never
0% Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Call customer forward; mark script if counselling required
Check script is for this customer when collection occurs
Check dispensed medication
Reinforce instructions on labels to the patient
Provide counselling
Collect payment from patient
Fill Webster packs
Simple compounding/reconstitution
HIC claim preparation
3. Are there any tasks in the dispensary where you believe you could be more heavily involved (after
appropriate training and with supervision and support)?
___________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________
4. Working outside the dispensary. For each task in the table below, please tick how often you perform each task in this pharmacy.
Task How often do you do this task?
Never
0% Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Selling/Product Knowledge Provide advice on S2 medicines (pharmacy only)
Provide advice on S3 medicines (pharmacist only)
Provide advice on complementary medicines (eg vitamins)
Provide advice on companion medicine sales
Provide other health care advice, product information, sell products Front of Shop Operations Pharmacy housekeeping (eg cleaning, rubbish removal)
Inventory management and ordering stock
Help maintain store safety and security Customer Service Greet pharmacy customers Conduct point of sale administration and balance register at day end
Administration Practices Operate and manage retail equipment (point of sale and till)
Prepare the pharmacy payroll

Page 3.
Task How often do you do this task?
Never
0% Rarely 0-24%
Occasionally 25-49%
Regularly 50-74%
Frequently 75-99%
Always 100%
Marketing Arrange product displays and merchandising
Prepare financial reports Quality and People Management Coordinate and supervise other pharmacy staff members
Recruit pharmacy staff
Perform formal assessments on staff members Help to develop quality improvement procedures within the pharmacy
Train other pharmacy staff
5. Are there any tasks outside the dispensary where you believe you could be more heavily involved
(after appropriate training and with supervision and support)?
___________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________
6. What is your current level of training? (can tick more than one) Nil. Secondary schooling less than Year 12. Secondary schooling to Year 12. On the job training. Formal pharmacy training:
Guild Certificate I. Guild Certificate II. Guild Certificate III. Guild Industry Grade 3. Guild dispensary training. PSA dispensary training.
Other qualification (please specify course and provider) …………………………………………...
…………………………………………………………………………………………………………………………………………………………………..

Page 4.
7. What best describes your personal preferences to pursuing further education and training in relation to pharmacy? (tick one) Interested in undertaking further study about community pharmacy and plan to enrol in a
Certificate / further Certificate. Currently enrolled in a community pharmacy certificate course. Interested in undertaking further study in an area other than community pharmacy. Not interested in further study – satisfied with my current level of knowledge. Not interested in further study – not supported by my employer. Not interested in further study – not planning to stay in this type of position in the longer term.
8. What best describes the level of support you would expect to receive from your employer to
undertake further pharmacy-related study? (tick one) Actively encouraged by my employer to undertake further study with financial support / time off. Interested in undertaking further study but must be undertaken in my own time and at my own
expense. My employer has shown little or no interest in me undertaking further pharmacy-related study.
Please place your completed form in the attached envelope, seal it and return it to the owner / pharmacist on duty.
THE END – THANK YOU FOR YOUR TIME

Attachment E
ADDITIONAL SURVEY DATA FIGURES

Figure E1: Pharmacists’ views on the average frequency of tasks that could be performed by pharmacy and dispensary assistants within the dispensary
0 10 20 30 40 50 60 70 80 90 100
HIC claim preparation
Simple compounding/reconst itution
Fill Webster packs
Collect payment from pat ient
Provide counselling
Reinforce instruct ions on labels to the patient
Check dispensed medication
Check script is for this customer when collection occurs
Call customer forward; mark script if counselling required
At tach warning labels to drugs
Check script against labels; attach to drug/script; provide to pharmacist
Select stock from shelves; check drug is in-date
Generate lables
Call prescriber if necessary
Check patient medication history
Enter script details into computer
Read script; liaise with customer ad pharmacist
Put script in pile to be dispensed
Ask if customer will wait or collect; mark script
Check stock/equipment is available
Checking patient PBS ent itlement details and record on script
Initial recording of PBS entitlement details
Check spelling of customer name, address and age
Check customer wants all items to be dispensed
Receive script from pat ient
Average Frequency (% )Dispensary AssistantPharmacy Assistant

Attachment F
CASE STUDY SUMMARIES
Pharmacy 1 (NSW 1)
PHARMACY CHARACTERISTICS Location
NSW Metropolitan Neighbourhood/strip centre Dispensing Model
Semi-forward Size
Average weekly scripts: 1201 – 1600 Estimated turnover: $2.0 – $2.5m. DISPENSING PROCESS AT THE CASE STUDY SITE HMA sought the owner/manager’s views on the dispensing workflow diagram during the case study visit to verify its accuracy. The main points of difference were.
the pharmacy did not capture the time a script was lodged in the pharmacy; the dispensary assistant undertook many of the tasks that a pharmacist would do, apart from making
the final check of the medication, which was always done by one of the two qualified pharmacists.; and
one of the two pharmacists completed the entire dispensing process A summary of the dispensing process in this pharmacy is as follows:
(1) A member of staff welcomes the customer and takes the prescription from them. This could be the pharmacy assistant, the dispensary assistant, or one of the two pharmacists on duty.
(2) If a pharmacy assistant receives the script they will hand this to a pharmacist or to the dispensary assistant.
(3) The dispensary assistant would then enter the customer’s details from the script into the dispensing software (FRED).
(4) The dispensary assistant or pharmacist will then print the label and retrieve the medication from the shelves behind the terminals.
(5) The dispensary assistant or pharmacist will then stick the labels on the medication, including any warning stickers which would be highlighted by the dispensing software
(6) If the script was filled by the dispensary assistant it would then be shown to a pharmacist for checking before it was handed over to the customer.
(7) Neither pharmacist would get the medication checked by another staff member before handing it to the customer.
(8) In busier times the pharmacy assistant would hand the prescription to the customer and read all the warning labels to the customer before payment.
The pharmacist owner/manger spoke of three differences between their role and a dispensary assistant in the dispensing process:
(1) The dispensary assistant would always need to get the medication checked by a pharmacist before being given to the patient.

(2) The dispensary assistant would not provide intervention advice direct to the customer. Issues would always be highlighted to the Pharmacist who would then take appropriate action by speaking with the customer.
(3) A dispensary assistant would not be allowed to call the prescriber of the medication – this was always done by the pharmacist on duty.
DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process
According to the owner/pharmacist, the role of the pharmacy assistant was to greet customers as they came into the pharmacy, and then take the prescription from them. This is the handed to a pharmacist or a dispensary assistant to the filled. Although the pharmacy assistant had worked as a dispensary assistant before, she did not feel comfortable using the dispensing software. He did not envisage the role of the pharmacy assistant being expanded outside these parameters, unless they were willing to undertake further training, which could be in-the-job. The pharmacy did not employ anyone who had done the Guild or PSA training, but saw this as important for younger assistants coming though community pharmacies. The role of the dispensary assistant in the dispensing process The pharmacy employed only one dispensary assistant, who was working with two pharmacists on the day of HMA’s visit. The dispensary assistant appeared to be competent in her job - she had been dong the role for twenty-two years. She commented that she felt comfortable doing everything that was asked of her. She would feel extremely uncomfortable filling a prescription without it being checked by a pharmacist, and therefore is happy to get it checked before giving the medication to the patient. The pharmacist felt comfortable with the current role and responsibilities of the dispensary assistant. There were a number of things, however, that were mentioned as not being suitable for being undertaken by the dispensary assistant:
mixing creams for patients; patient counselling; filling methadone prescription; contacting the GP/prescriber; The pharmacy assistant felt quite comfortable with selling S3 drugs, although she did not perform this role in practice. She had had experience in the past as she had been working in community pharmacies for over 30 years in Australia and New Zealand. Although the pharmacy dispensed methadone, this was not undertaken by the dispensary assistant. However this was a role the pharmacist felt a confident dispensary assistant was able to complete. The dispensary assistant also did not fill Webster packs. The pharmacist made these up. The role of pharmacy and dispensary assistants in the non-dispensing workflow
The dispensary and pharmacy assistants did the same tasks out of the dispensary. Both ordered stock, cleaned the pharmacy, and gave advice to customers about non-medication. They were not involved in the hiring of additional staff, or the management of the accounts. This was not something that either assistant wanted to be involved in. Being involved in the business administration of the pharmacy was something that both pharmacists saw as being a task that could be undertaken by suitably qualified pharmacy assistants.
Although the pharmacy sold a wide range of products, it was skewed heavily toward prescription medication and S3 drugs. There was a supermarket opposite the pharmacy that sold most of the retail products stocked in the pharmacy. The dispensary assistant had done specialist courses in complementary medicines offered by the pharmacy offered. Pharmacy and dispensary assistant training
The pharmacist explained that none of the assistants at the store had completed either the Guild training or the PSA training. The owner/pharmacist did not have any objection to staff undertaking the training, and would allow them some work time to do the modules, but currently used experienced staff. The dispensary assistant said that she did not want to undertake any Guild training, however she would do a pharmacy technician course if it lead to an increased salary. The dispensary assistant has done a three-day course on complementary medicines. She did not see any value in doing any further modules on non-dispensary tasks such as marketing, HR or retail. The pharmacy assistant did not plan do any further training as she was only two years from retirement. Other Issues
The pharmacists did not see much room for expanding the role assistants currently provide. Although they are filling Webster packs, they are not servicing any nursing homes. The dispensary assistant saw the possibility of expanding their retail offering. One of the pharmacists was conducting medication reviews, however this was not the core business of the pharmacy. One of the pharmacists mentioned the possibility of taking customers’ blood pressure, however with a doctor’s surgery next door he was unsure how popular this kind of service would be.
Pharmacy 2 (NSW 2) PHARMACY CHARACTERISTICS Location
Sydney Metropolitan Shopping strip Dispensing Model
Forward Size
Average weekly scripts: 401 – 800 Estimated turnover: $1.0 – $1.5m. DISPENSING PROCESS AT THE CASE STUDY SITE HMA sought the owner/manager’s views on the dispensing workflow diagram during the case study visit to verify its accuracy. The main points of difference were:
the pharmacist would generally take the script from the customer and process all details on the computer;

the pharmacist would also generally counsel the patients when she was handing them the medication. A summary of the dispensing process in the pharmacy was as follows.
(1) The pharmacist received the script from the customer. In busier times, a pharmacy assistant was also able to collect the script from the customer.
(2) The pharmacist entered the patient details into a terminal at the desk in front of the dispensary. Once the details were entered, the pharmacist would place the script in a basket and hand it to the dispensary assistant who would be at the rear of the store. While the script was being transferred, the pharmacist would print the label on a printer located at the rear of the shop.
(3) The dispensary assistant would pick the medication from the shelf and attach the label which had been printed out. If the dispensary assistant was doing another task (such as filling Webster Packs), the pharmacist would complete the rest of the process without assistance.
(4) The dispensary assistant would place the medication next to the pharmacist for checking, or place it on a shelf behind the pharmacist’s counter.
(5) At this point the pharmacist would check the medication and would counsel the patient, if required, and then obtain payment. If no counselling was required, the assistant would obtain payment. The cash register was located toward the front of the store, away from the counselling counter.
(6) If the customer was not in the store at the completion of the dispensing process, the medication would be placed in a small plastic basket to the right of the pharmacist, ready for collection. Only medication checked by the pharmacist would be placed on these shelves.
DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process
The role of the dispensary and pharmacy assistant was used interchangeably. On the day HMA visited the pharmacy, the pharmacy assistant, who had not done the Pharmacy Guild training, was filling Webster packs. She was also observed running errands for the pharmacist and delivering prescriptions to customers. In discussions with the pharmacist/owner, it was stated that a key role of the pharmacist was to check that the correct medication was being dispensed. All other tasks were capable of being done by assistants. There were only three types of medication that the pharmacist would always counsel a patient on. These were:
a new type of medication for a customer; medication for children; and problem medication involving levels of toxicity. In all other cases, either the dispensary assistant, or pharmacy assistant could give the medication to a customer, providing it was first checked by the pharmacist on duty. The pharmacist had no issue with a competent assistant providing basic advice to a customer The pharmacist felt comfortable with the assistant advising on S2 drugs as long as they demonstrated knowledge of the correct questions to ask customers. The role of the dispensary assistant in the dispensing process In this pharmacy the role of the dispensary assistant was to fill scripts after a pharmacist had entered the data into the system (the pharmacy was using WiniFRED). The dispensary assistant would not enter the
patient data and would have little customer contact except in busy periods when they would hand the medication back to the customer and take the payment from them. The pharmacist did not think it was necessary to have them trained by either the Guild or the PSA, although she would not discourage an assistant from taking the course. The role of pharmacy and dispensary assistants in the non-dispensing workflow
The distinction between the dispensary and the pharmacy assistant was blurred; both categories of staff spent time in the dispensary and in the shop. A pharmacy assistant would rarely take the script from the customer, as this was generally done by the pharmacist at all but the most busy times. The assistants would also deliver prescriptions and other retail items to customers, as well as undertaking basic cleaning of the store and stacking shelves. Pharmacy and dispensary assistant training
None of the assistants in the pharmacy had completed Guild training. The oldest staff member was aged 64 and close to retirement. The pharmacist had been training her in the dispensary, but saw little need for certification. The assistant working on the day HMA conducted the case study visit had started a science degree, but was planning to take a leave shortly to try work in outside a community pharmacy. The assistant did not want to complete the training as she saw herself not being in the role long enough to get any benefit from the training. The pharmacist believed that specialist courses in retail, HR or marketing would be most useful in larger pharmacies where the pharmacist was checking many scripts in one day. This would ease the burden on the pharmacist if they could give responsibility for one of the administrative tasks to a capable assistant. Given the correct training, the pharmacists believed that the assistants could perform additional tasks that the pharmacist was currently performing, such as taking customers’ blood pressure, and diabetes screening. The pharmacist was in favour of the creation of a level above dispensary technician as it would provide a greater level of transferability between pharmacies, something she also believed the Guild training provided. She also saw the need for change in the regulations if such a new level were to be created. Other Issues
The pharmacist considered that on the job training was extremely important for assistants working in the dispensary, although it was recognised that this experience was not one hundred percent transferable across sites. It provided valuable “street knowledge” which could only be gained whilst working in a pharmacy.
Pharmacy 3 (NSW3) PHARMACY CHARACTERISTICS Location
New South Wales Rural Strip shopping centre in regional setting Dispensing Model

Semi-forward Size
Average weekly scripts: 801 – 1200 Estimated annual turnover: 2.0 – 2.5m. DISPENSING PROCESS AT THE CASE STUDY SITE A summary of the dispensing process in the pharmacy is as follows.
(1) The pharmacist received the script from the customer. In busier times, a pharmacy assistant or dispensary assistant would instead collect the script from the customer. They would also ask the customer if a generic brand drug was preferable if it were a cheaper option.
(2) The pharmacist (or assistant) would enter the patient details into a terminal at the desk in front of the dispensary. Once the details were entered, the pharmacist would place the script in a basket and hand it to the dispensary assistant who would be in the rear of the store.
(3) The dispensary assistant would enter script data into the computer, and print off the label. The dispensary assistant would pick the medication from the shelf, and attach the label, which had been printed out. She would also attach any form of warning label to the container.
(4) The dispensary assistant would place the medication in a container in readiness for the pharmacist to check the medication label.
(5) When not busy, the pharmacist would check the medication and if the patient required counselling he would attend to the patient, and then sell them the medication. The pharmacists preferred to always counsel patients if the medication was for a child, or if it were the first time a patient was taking the medication. If no counselling was required the pharmacy or dispensary assistant could give the medication to the patient. The patient would then pay for their filled prescription at the front or rear of the store.
DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process
The tasks that the pharmacy assistants were able to undertake were written down and had been attached to the walls of the dispensary. These tasks were never questioned by the pharmacy assistants and were closely followed. The pharmacy assistant would take the prescription during the busier periods of the day, however the pharmacist preferred to take the prescription if he could. The pharmacy assistant would enter the patient details in the computer. The prescription would then place the prescription on the back shelf ready for collection by the dispensary assistant or pharmacist on duty. The pharmacy assistant would hand back a prescription and take the payment for the medication when a pharmacist was busy. The exception to this would be when the medication was for a child, or it was new medication for the patient. The role of the dispensary assistant in the dispensing process The dispensary assistants completed nearly all of the dispensing process themselves, with only limited supervision of the pharmacist. Both dispensary assistants were both observed filling prescriptions whilst the pharmacist was on the floor counselling a patient. In all cases though, the dispensary assistant would show the pharmacist the medication and associated labels before it was handed to the customer.

The dispensary assistants had the responsibility of filling the Webster packs. These were always checked by the pharmacist before being given back to the patient. The dispensary assistants were also used to order medication for the dispensary. The pharmacist felt confident that a well-trained assistant could complete the entire dispensing process themselves, without their work needing to be checked by a pharmacist. The role of pharmacy and dispensary assistants in the non-dispensing workflow
The assistants were rotated through different roles on the shop floor. Each assistant would be responsible for a number of different retail areas in the shop, and there was an expectationa that they would develop enough knowledge to provide an expert opinion on the product. For example, the pharmacy assistant HMA spoke to was in charge of ordering and replacing the stock in the following areas:
skin care; first-aid; Revlon make-up; home aids; and chemist club. Other tasks that were preformed by the assistants include:
sales; home medication deliveries; cleaning; and unpacking stock deliveries; The pharmacist also hired an administrative assistant to help him run the back-office. They were responsible for paying the pharmacy account’s, providing a small marketing function and some scheduling. Pharmacy and dispensary assistant training
Assistants were given time at work to study for the Pharmacy Guild certificates. The pharmacist preferred to have his assistants study in the quieter periods of the year (January in the case of this pharmacy). The pharmacist believed the training provided a complete guide as to what the assistants were allowed to undertake in the dispensary Other Issues The dispensary assistant that HMA talked to was happy in her current role, and although she enjoyed working in the dispensary, she also got satisfaction from dealing directly with customers. She did not seem enthusiastic about the role of a dispensary technician because of the extra study that this involved. Pharmacy 4 (Vic 1) PHARMACY CHARACTERISTICS Location
Victoria Metropolitan Shopping strip
Dispensing Model
Forward Size
Average weekly scripts: under 400 Estimated annual turnover: not specified. THE DISPENSING PROCESS AT THE CASE STUDY SITE HMA sought the pharmacist owner/manager’s views on the dispensing workflow diagram during the case study visit to verify its accuracy. The pharmacist confirmed its accuracy but stressed that given the small size of the pharmacy and the low script volume, the pharmacist usually undertook the entire dispensing process. At the time of the case study visit, there was only the pharmacist working in the pharmacy. The pharmacist would therefore undertake the entire dispensing process, from greeting the customer to filling the script to collecting payment. The pharmacist commented that the pharmacy assistant would may greet the customer if the pharmacist was busy. The pharmacist would usually send the customer to the assistant for payment for their script. Note that there were no dispensary assistants employed in this pharmacy. DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process The role of the pharmacy assistant was very limited in this pharmacy. In busy times, the assistant would receive the script from the customer, and collect Medicare numbers. They also collected the customer’s payment at the end of the process. The pharmacy assistant did not tend to go into the dispensary at all, and did not undertake any data entry into the pharmacy computer system. The role of the dispensary assistant in the dispensing process There were no dispensary assistants employed in this pharmacy. There was also no need to employ a dispensary assistant given the low script volume. The pharmacist interviewed did not have a firm view on the role of dispensary assistants, as they had not tended to work in pharmacies that use dispensary assistants. They thought that in an “ideal world” an assistant could do all the processing of a script, dispensary inventory and stock control, etc, which would allow the pharmacist to focus purely on the customer. They thought that there was “definitely” scope to increase the role of dispensary assistants in the dispensing process The role of pharmacy and dispensary assistants in the non-dispensing workflow This was a small pharmacy, which employed only one pharmacy assistant. The assistant worked across most aspects of front-of-shop including cleaning, customer liaison, and stock rotation. In larger pharmacies, the pharmacist also thought that assistants could undertake processing wages and bookkeeping. Pharmacy and dispensary assistant training In the pharmacist’s experience, assistants working in larger pharmacies tended to be “well-trained”, both within and outside the dispensary. The pharmacist commented that it was difficult to maintain good training for assistants in small pharmacies, as small pharmacies do not have the flexibility of larger pharmacies.

The pharmacist stressed the importance of getting a good, fast learner, who can do things on their own. Other issues The pharmacist was unsure about the creation of an intermediate level between the pharmacist and a current dispensary assistant.
Pharmacy 5 (Vic 2) PHARMACY CHARACTERISTICS Location
Victoria Metropolitan Shopping strip Dispensing model
Forward Size
Average weekly scripts: 2000+ Estimated turnover: not specified THE DISPENSING PROCESS AT THE CASE STUDY SITE HMA sought the pharmacist owner/manager’s views on the dispensing workflow diagram during the case study visit to verify its accuracy. The pharmacist confirmed the accuracy of the overall process diagram for this pharmacy, however, pointed out that the person undertaking each task varied. This pharmacy used a ‘true’ forward pharmacy model and employed five pharmacists and five dispensary assistants. The pharmacist would usually greet the customer, take them aside to a counselling area (three enclosed desks). They would take the script whilst talking to the customer and enter the details into the pharmacy system. Once completed, the label would print in the dispensing area, and a dispensary assistant would fill the script. They would then place the dispensed medication in a basket (with the repeat forms if required) and return it to the pharmacist and customer. The pharmacist would then check the dispensed medication. counsel the patient as required, and either the pharmacist or a dispensary assistant would collect the customer’s payment. This process appears to reflect a ‘retail version’ of hospital pharmacy practice. This pharmacy had successfully implemented a forward pharmacy model. The pharmacist interviewed argued that this “pharmaceutical care” model was the way forward for pharmacy. It facilitated pharmacist contact with customers, which focussed the dispensary assistant on the processing the script for the pharmacist. There appeared to be adequate support and checking mechanisms in place, including the use of a scanner and a second check of the dispensed medication. DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process

There were no pharmacy assistants employed in this pharmacy, as the pharmacy specialises on prescriptions with very little retail. The role of the dispensary assistant in the dispensing process The dispensary assistants tended to work almost exclusively in the dispensary (to free up the pharmacists’ time to focus on customers). Their role would involve receiving the label on the printer in the dispensary, getting the medication from the shelves, scanning the medication to make sure that it was the medication matched the script, and placing the medication, labels and forms in a basket for the pharmacist. They were not meant to stick the label on the medication, as this was one of the final checks for the pharmacist to do. They would then present the basket to the pharmacist. The dispensary assistants did not interact with customers very often. If a dispensary assistant did greet a customer (if all pharmacists were too busy) they would accept the script, check the patient’s details and give the script to a pharmacist. The dispensary assistants oversaw the dispensary stock, including rotation, ordering, contacting manufacturers to discover where orders were, unpacking received stock and stacking dispensary shelves. The dispensary assistant commented that working in this pharmacy was “more rewarding” than previous pharmacies that they had worked in. The role of pharmacy and dispensary assistants in the non-dispensing workflow As this pharmacy specialised on prescriptions, there was no need for many of the typical ‘front-of-shop’ operations required in many pharmacies. The dispensary assistant commented that they get involved in “everything outside the dispensary”. The pharmacist thought that dispensary assistants could have greater involvement in S2 and S3 medications (eg Ventolin) under the supervision of a pharmacist. Pharmacy and dispensary assistant training The pharmacist thought that the Guild’s current training is a “good start”. They thought that the training was flexible and that the pharmacy could manage training around its ongoing operations effectively. Both the pharmacist and dispensary assistant thought that some questions in the non-dispensary training were repetitive and redundant. The pharmacist suggested that there should be more focus on skills such as interviewing, communication, handling people and looking after “tough customers”. They argued that these skills were more important than product knowledge. The pharmacist also commented that every pharmacist needs to train their dispensary assistants on-the-job. The pharmacist thought that the suggestion of a part-time degree was a good idea, however, tremendously difficult to implement (eg do dispensary assistants get credits for work history?). Other issues The pharmacist saw the value in the creation of an intermediate level between the pharmacist and a current dispensary assistant, however, they thought that this pharmacy’s current forward dispensing model worked very well and saw no reason to change.

Pharmacy 6 (Vic 3) PHARMACY CHARACTERISTICS Location
Victorian Metropolitan Shopping strip Dispensing model
Semi-forward Size
Average weekly scripts: 2000+ Estimated turnover: not specified DISPENSING PROCESS AT THE CASE STUDY SITE HMA discussed the forward dispensing model with the pharmacist owner/manager, and sought their views on the dispensing workflow diagram presented by HMA. The pharmacist confirmed its accuracy for this pharmacy. A pharmacy assistant would greet the customer, take the prescription, check its details and put in a pile in the dispensary. A dispensary assistant would take the script and enter the information into the pharmacy system. The pharmacist thought that the IT systems were adequate to support dispensary assistants checking a patient’s medication history (interactions adequately flagged). If any interaction was observed, the dispensary assistant would make note of it for the pharmacist. The dispensary assistant would then assemble the script and put it aside in a basket for the pharmacist. The pharmacist would then check the medication and give it to the customer, and counsel as required. DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process The pharmacist confirmed that the role of the pharmacy assistant was to accept the script from the customer and check its completeness. The pharmacy assistants may give the checked dispensed medication to a customer. They would usually collect a customer’s payment. The role of the dispensary assistant in the dispensing process The dispensary assistant would effectively undertake the entire dispensing process on receiving the script, through to the final check of the medication (this check would always be completed by a pharmacist). The dispensary assistant would give the dispensed medication to customers and reinforce instructions – usually only for repeat customers. The dispensary assistant commented that they “can’t do much with the medical history of new customers, so the get the pharmacist”. Both the pharmacist interviewed and the dispensary assistant stressed that a pharmacist would always check the medication history and provide the counselling. Dispensary assistants also generally did all stock control and ordering in the dispensary. They looked after any dispensary promotions (eg blood pressure). Webster packing was also usually completed by the dispensary assistant. Occasionally the dispensary assistant would call the prescribing doctor.

The pharmacist commented that this dispensary assistant was experienced, and a “good employee”. They emphasised that the use of a dispensary assistant was dependant on the “quality” of the employee, not their official role. The role of pharmacy and dispensary assistants in the non-dispensing workflow Pharmacy assistants worked only in the front-of-shop operations of the pharmacy, while the dispensary assistant worked in the dispensary. The pharmacist commented that they tried to “keep the roles separate”. The pharmacist thought that the role of assistant could be expanded outside the dispensary. They argued that any pharmacy assistant should be able to provide “advice on vitamins, anti-fungals, etc”. They also thought that dispensary assistants could increase their involvement in S2 and S3 medicines. The dispensary assistant said that they already provide “quite a bit” of advice on S2 and S3 medicines, with the “pharmacist always supervising”. This was particularly the case when busy. The dispensary assistant also was involved in compounding (eg mixing creams), once again under the supervision of the pharmacist. Both the pharmacists interviews agreed that they prefer to play a supervisory role here, which allows the dispensary assistant to undertake the task. They thought that the Guild should provide more training to help facilitate this. The pharmacy employed a full-time front-of-shop manager’ to oversee and run the front-of-shop operations. This employee does all the ordering, liaising with reps, merchandising and staff rostering. There was a separate bookkeeper – the pharmacist thought that any employee involved would really need accounting expertise. The dispensary assistant said that they would tend to focus on purely the dispensary, but they had “some involvement” in the front-of-shop operations. Pharmacy and dispensary assistant training The pharmacist thought that the Guild training was excellent. They found it difficult to get part-time staff to the training. The dispensary assistant had completed the Guild training programs. The pharmacy staff were supportive of the training. The dispensary assistant thought that there could be more content on specifically what they are allowed to do and what they are not allowed to do. They said that there was constant confusion on this topic. They also thought that there should be more ongoing training (eg an “advanced dispensary assistant course” and a more simple course). They argued that this would recognise the large variation in experience/competence of dispensary assistants. Both the pharmacists and dispensary assistant thought that there should be more training in relation to extemporaneous products (“measuring, mixing, etc”). They also argued that the Guild training should be more hands-on. They recognised that this would make the course longer. The dispensary assistant often trained other pharmacy assistants in S2 and S3 medication. Other issues The pharmacist appreciated the difficulty in specifying exactly what a new role for dispensary assistants could and could not do. They argued that this role could potentially be more involved in S3 medication counselling (with appropriate training), webster packing, checking dosages and the preparation of extemporaneous products. Obviously, suitable training would need to support these additional tasks. The pharmacist commented that this pharmacy used to be a forward pharmacy, however, the build up of customers caused a large backlog in busy times. Under their current semi-forward model, the pharmacist can select which customers require counselling.

Pharmacy 7 (Qld 1)
PHARMACY CHARACTERISTICS Location
Queensland Rural Neighbourhood/strip centre in a small town Dispensing Model
Semi-forward Size
$1.0 – $1.5 Million DISPENSING PROCESS AT THE CASE STUDY SITE HMA sought the owner/manager’s views on the dispensing workflow diagram during the case study visit to verify its accuracy. The main points of difference were:
the dispensary assistant may check with the pharmacist for stock availability; and the pharmacist may take prescriptions when he is on the shop floor. The dispensary workflow at this site is defined in more detail below:
(1) A member of staff welcomed the customer and took the prescription from them. This could be the pharmacy assistant, the dispensary assistant, or the pharmacist on duty
(2) If a pharmacy assistant received the script they would hand this to a pharmacist or to the dispensary assistant who were generally behind the dispensary counter in the pharmacy.
(3) The dispensary assistant would then enter the customer’s details from the script into the dispensing software (FRED).
(4) The dispensary assistant or pharmacist will then print the label and retrieve the medication from the shelves behind the terminals.
(5) If the dispensary assistant is processing the prescription, they will pass the label and medication to the pharmacist to check. If correct, the pharmacist will stick the label on the medication.
(6) Either the pharmacy assistant, or the dispensary assistant would provide counselling to the customer for routine scripts. Complex or new script counselling would be undertaken by the pharmacist.
(7) The pharmacy assistant received payment at the front of the store. DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process
According to the pharmacist/owner “the pharmacy assistant role is well defined through the Guild Training.” Currently the pharmacy assistant took the prescription from the customer and then gave it to the pharmacist who spent most of their time behind the dispensary counter which was situated at the rear of the store. The pharmacist would check the patient details on the computer and also record the time the prescription has been brought into the store. If it was a routine prescription, the pharmacy assistant would

hand it back to the customer. In more complex cases the pharmacist would hand the prescription back to the customer, before payment occurred. The pharmacist believed that assistants should only be able to do more tasks if the laws governing what they can and cannot do are changed. The role of the dispensary assistant in the dispensing process Some aspects of the dispensary assistant’s work was similar work to the pharmacist, apart from providing the final check of the medication before it was given to the customer. She could receive the script from the customer if she was on the shop floor, after which she would commence processing the script by adding details to the system and finding the medication on the shelves. The dispensary assistant did not place labels on the medication. That was the role of the pharmacist. The dispensary assistant reported that they would not feel uncomfortable if the role expanded to include doing a final check of medication without showing the pharmacist (however currently she gives the medication to the pharmacist for the final check). The role of the dispensary assistant was not confined to the dispensary and she enjoyed doing work on the shop floor, such as providing product advice to customers as they moved through the store. She also stocked shelves, priced stock, cleaned and used the cash register. The pharmacist believes that qualified pharmacy and dispensary assistants could undertake some administration tasks such as contact with doctors. The role of pharmacy and dispensary assistants in the non-dispensing workflow
Both the pharmacy and the dispensary assistants spent time on the shop floor. Their main task was cleaning, stacking shelves, pricing products, using the cash register and providing non-medication related advice to customers. They did not play a role in the administration of the business such as HR, marketing or retail strategy. The pharmacist’s wife did the accounts for the business. Pharmacy and dispensary assistant training
The pharmacist considered that:
“Training helps in defining the boundaries for what assistants can and cannot do…..The depth of training is providing adequate learnings for assistants.”
The pharmacist believed that the Guild offered “dynamic” training that was easily transferable to other pharmacies. Furthermore they felt that it was extremely comprehensive in providing information on procedural issues involved with working in the pharmacy/dispensary. The dispensary assistant had completed the Guild training. The pharmacist required this training to be completed by all the dispensary assistants hired. The dispensary assistant did not do all the modules because she had Recognised Prior Learning (RPL) and was at Level 3. It was commented that a business management course for pharmacy assistants would be useful as this would provide valuable support to pharmacists. The dispensary assistant also expressed interest in completing a staff/people management course as she did not think she had the skills or the confidence to lead a team of assistants. The regulations would need to change in order for the pharmacist to feel comfortable with the increased roles and responsibilities of his assistants in the dispensary. It was also commented that the training completed by assistants was in module format and this could be completed on-site at the pharmacy. This was very important at a rural pharmacy where it took aver three hours to drive to the nearest capital city.

Other Issues
Some of the reasons that the pharmacist was doing more tasks at this site compared with a metropolitan pharmacy related to the size of the store. Tasks they undertook included stocking the shelves and reordering of stock. The pharmacist believed there was scope, with the proper training, for pharmacists to offer minor clinical work. He gave the example of removing minor bodies in the eye. He offered some other suggestions for an increased service range, such as:
immunisation; gene screening; testing for diabetes; and some simple screening, such as for people with suspected broken arms and sporting injuries. He suggested these examples of new activity because of the lack of nurses, GPs and allied health professionals in the area.
Pharmacy 8 (Qld 2) PHARMACY CHARACTERISTICS Location
Queensland Rural Neighbourhood strip shopping centre Dispensing Model
Traditional Size
$1.0 – $1.5 Million DISPENSING PROCESS AT THE CASE STUDY SITE Dispensary assistants used the dispensing system computer but only for claim generation. Pharmacists used the computer to update patient information. The pharmacist/owner did not allow dispensary or pharmacy assistant to update customer information. The pharmacist always handed the medication to the customer. The role of the dispensary assistant in the dispensing process
The role of the dispensary assistant was limited to picking the medication from the shelves, and acting in the role of pharmacy assistant. The pharmacist commented that this was more a result of the experience of the current dispensary assistant, rather than the belief that dispensary assistants should never input patient data into the computer. The pharmacist believed that dispensary assistants did not have the training to ask the correct questions of the customer. He believed that they are in a similar position to young pharmacists with recently completed degrees. The dispensary assistant mentioned that she would feel uncomfortable in providing any advice other than non-clinical retail advice.

The pharmacy was in the process of employing a further qualified dispensary assistant. They were running a fairly expensive model with three pharmacists and only one dispensary assistant. The pharmacist interviewed noted the difficulties in recruiting suitably qualified dispensary assistants. The dispensary assistant was required to discus script issues with the the pharmacist aware if there was any change in the medication being prescribed for a patient. The role of the pharmacy assistant in the dispensing process
The pharmacy assistants undertook a “reception and retailing role.” They were not able to give any clinical advice to patients. This was regulated and controlled; previous assistants had been dismissed for giving clinical advice to customers. The role of the pharmacy assistant in the dispensing process was limited to taking the prescription from the patient, and then returning it to the patient once it had been dispensed. The assistant felt she could do more, but acknowledged that she would require training in order to do so. The role of pharmacy and dispensary assistants in the non-dispensing workflow
The assistants played a far greater role in the non-dispensing process than the pharmacists. The role was to provide retail assistance to customers in the store, stacking the shelves, some pricing, and selling non pharmaceutical products. They were not involved in running of the business. This was the responsibility of the pharmacist and his wife, also a pharmacist. An additional responsibility of the dispensary assistant was to order retail stock. Shop floor duties took up about sixty percent of her time. Pharmacy and dispensary assistant training
There was support expressed for the creation of a new pharmacy technician role by the three pharmacists working at the case study site, as well as by the dispensary assistant. The reasons that this was considered to be useful were:
there was a belief amongst the pharmacists that it would entice more males into the profession; currently they were finding it difficult to attract adequately qualified dispensary assistants; and the dispensary assistant felt she had no further options if she wanted to progress at the pharmacy. The pharmacist/owner suggested that science students could take such a new course as a series of electives at University. Both the assistants had enjoyed the training they had undertaken. The dispensary assistant had completed the PSA course. She believed this was “more thorough” than the Guild training. The pharmacy assistant had completed Level One Guild training. She had been given time off at work to complete this. She found this an enjoyable and rewarding experience and would like to undertake more training if the opportunity arose. Although she said the course was challenging “it doesn’t compare to working and the challenges that it provides on a daily basis”. The training had made her feel comfortable in the role she performed and she believed it was important to have a job in the pharmacy whilst doing the course as it cemented her learnings. Neither assistant had thought about doing the retail, HR or marketing courses. Other Issues
The pharmacy had found it difficult to attract qualified dispensary assistants. The pharmacist believed not enough pharmacy staff were doing the training and there should be more promotion of the courses

throughout community pharmacies. They had placed three advertisements over a three-week period seeking a dispensary assistant but only received one suitable applicant that they would hire. Pharmacists were leaving the profession earlier, as graduates were not seeing pharmacy as a long-term career. The two graduate pharmacists the pharmacy employed were leaving to study law and business. The increasing age of the population was placing pressure on pharmacists. The pharmacy serviced hostels in the area, and were often called out up to five times a day to service these. This placed pressure on the pharmacy through decreased margins.
Pharmacy 9 (Qld 3) PHARMACY CHARACTERISTICS Location
Queensland Metropolitan Neighbourhood/strip centre in a small town Dispensing Model
Traditional Size
$1.0 – $1.5 Million 400-800 scripts per week. DISPENSING PROCESS AT THE CASE STUDY SITE The pharmacist completed the majority of the dispensing process by themselves. The reasons given for this approach to workload management were:
(1) Personal preference. One of the major reasons the pharmacist moved to the country was to do more of the dispensary process.
(2) Adequate time. The pharmacist was not busy, having large periods of inactivity during the middle of the day. The busiest times were from 8am-10am and from 3pm-6pm.
(3) Confidence in assistants. The pharmacist did not have full confidence in the assistants to put medication on the shelves.
The dispensary workflow used is defined in more detail below: (1) A member of staff welcomed the customer and took the prescription and Medicare card from them.
When HMA visited, it tended to be either the pharmacy assistant, or the store manager that completed these tasks.
(2) The pharmacy assistant takes the prescription to the pharmacist or to the dispensary assistant who was generally behind the dispensary counter in the pharmacy.
(3) The pharmacist entered the customer details from the script into the dispensing software (FRED).
(4) The pharmacist then printed the labels and retrieved the medication from the shelves behind their desk.
(5) If the dispensary assistant was processing the prescription, they would stick the label on the medication and show it to the pharmacist to check.

(6) The pharmacist provided patient counselling. If the prescription was a repeat, the pharmacy assistant would hand the medication to the customer and reiterate any warnings that had been stuck on the package.
(7) The pharmacy assistant received payment at the counter below the dispensary
The role of the dispensary assistant in the dispensing process
The dispensary assistant did not do much work in the dispensary, as the pharmacist kept a tight reign over the process. When the pharmacist was busy however, the dispensary assistant would assist in taking the medication from the shelf and re-stocking shelves with medication. She seemed eager to do more in the dispensary including updating patient data on the computer system. She would also provide assistance to the pharmacy assistant by helping to greet customers and give the scripts to the pharmacist. The pharmacist felt there was scope for a suitably trained assistant to sell S3 drugs. The store manager (who acted as a pharmacy assistant) said she would feel comfortable in selling S3 drugs to customers. She had worked in pharmacy for 20 years, and felt confident about all the tasks that needed to be performed. The role of the pharmacy assistant in the dispensing process
The role of the pharmacy assistant in the dispensary process was to collect scripts and Medicare cards from the customer. At the end of the dispensing process, if no counselling was required by the pharmacist, the assistant would hand the medication to the customer and receive payment. The pharmacy assistant felt confident that with some further training she would be able to work in the dispensary. The role of pharmacy and dispensary assistants in the non-dispensing workflow
The assistant was involved with selling retail products and was also assigned responsibility for general cleanliness within the retail area and stock levels of the shelves. The assistants would also provide non-clinical advice to patients. The assistants also served customers who would use the building society service that was offered at the Pharmacy. Generally assistants would be trained in the building society tasks after six months on the job. This component of the pharmacy’s activity could get quite busy in the afternoon as other traders closed for the day. Pharmacy and dispensary assistant training
The pharmacy assistant mentioned she had received a letter from the Guild advising her on the training courses offered. She had not started a course, but planned to begin her level 1 module over the next few months. She mentioned she would like to complete additional training up to level three. The dispensary assistant did not see it as a priority to undertake specialist retail or marketing training, although she had enjoyed the training she had done over the last three years and thought it was a valuable experience. She felt that after three years in the job she had adequate knowledge of retail issues to provide a high quality service to customers without a requirement for additional training. Other Issues
The store manager had been in the position for 20 years and felt very comfortable undertaking that role. She was effectively a pharmacy assistant but did retail stock ordering as well. The pharmacy and dispensary assistant were both trained nurses. They had decided to quit nursing as it was not what they expected. The pharmacist believed their nursing training could be used more

effectively by holding a series of customer information sessions on topics such as diabetes and baby care. Until recently the pharmacy had a nurse come into the store for a morning once a week providing a baby health service, including weighing and offering minor clinical advice to parents. Both assistants felt comfortable in providing this type of service to the community.
Pharmacy 10 (SA1) PHARMACY CHARACTERISTICS Location
South Australia Rural Shopping strip Dispensing model
Semi-forward Size
Average weekly scripts: 401 – 800 Estimated turnover: $1.0 – $1.5m DISPENSING PROCESS AT THE CASE STUDY SITE HMA sought the pharmacist owner/manager’s views on the dispensing workflow diagram during the case study visit to verify its accuracy. The pharmacist confirmed its accuracy for this pharmacy. The pharmacy assistant would receive the script, review it for completeness, and place it into a plastic basket. If the patient was waiting for the script, the pharmacy assistant would clip a blue peg on the basket. If the patient wanted a generic brand the pharmacy assistant would clip a yellow peg on the basket. The pharmacy assistant would then place the basket on the bench in the dispensary. There were no dispensary assistants employed in this pharmacy. There was a locum pharmacist working at the time of the case study visit, who would complete the end-to-end dispensing process. They would pick the medication off the shelf, then enter the customer’s details into the dispensing system. A significant proportion of scripts were repeats (estimated by the pharmacist at around 85-90% of all scripts), so there was less data entry than other pharmacies that this pharmacist had worked in. The pharmacist would then put the medication back in the plastic basket and place it on a separate shelf (in alphabetical order), awaiting collection by the customer. DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process The role of the pharmacy assistant was limited to receiving the script from the customer and ensuring its completeness (ie checking customer’s name, address, etc). They then collected the customer’s payment at the end of the process. One pharmacy assistant commented that they usually knew each customer; they would always check that the medication in the basket was for that customer, and as they gave them the medication they would generally point out the medication directions (eg take with food). If the patient began to ask questions, they would defer to the pharmacist. This was the extent of their involvement in the dispensing process. Pharmacy assistants did not undertake any data entry into the pharmacy computer system at all.
Two pharmacy assistants usually filled Webster packs for the local nursing home, community-based patients and the Aboriginal Elder Care program. The pharmacist then checked each pack. A pharmacy assistant would then deliver the pack to the nursing home/community. The HIC claims were put together by the pharmacy assistant, and then checked by the pharmacist. The pharmacy assistant would assist with dispensary stock control, and would monitor and order drugs as required. They said they also had some liaison with drug representatives. The role of the dispensary assistant in the dispensing process There were no dispensary assistants employed in this pharmacy. The pharmacist interviewed had worked solely in small rural pharmacies. They could not express a definitive view on the role of dispensary assistants, as dispensary assistants tended not to work in these pharmacies. The pharmacist thought that if the dispensary became “very busy”, a dispensary assistant could key data into the computer system while the pharmacist assembled the scripts. The role of pharmacy and dispensary assistants in the non-dispensing workflow As expected in a pharmacy of this small to medium size, pharmacy assistants tended not to specialise in any particular aspect of non-dispensing operations, rather they worked across the entire front-of-shop (ie they worked in home health, the baby section, vitamins, first aid, etc). They were also involved in stock control, rotation and buying. The pharmacist commented that it was the tasks outside the dispensary that gives pharmacy assistants far more importance than being “simply a shop assistant”. Pharmacy assistants were involved in back-office functions such as staff rostering, banking and administration. Pharmacy and dispensary assistant training The pharmacy assistant had completed training through the pharmacy banner group’s head office. They had also completed a Guild training course on vitamins, as well as store-based training sessions on various new products. When questioned on pharmacy assistant training, the pharmacist commented that “all-in-all, their training seems pretty good”. Other issues The pharmacist thought that the creation of an intermediate level between the pharmacist and a current dispensary assistant was a good idea. They thought that a pharmacist would still have to undertake the final check of the dispensed medication.
Pharmacy 11 (SA2) PHARMACY CHARACTERISTICS Location
South Australia Metropolitan Shopping centre

Dispensing model
Forward Size
Average weekly scripts: 1200 – 1600 Estimated turnover: $1.0 – $1.5m DISPENSING PROCESS AT THE CASE STUDY SITE HMA discussed the forward dispensing model with the pharmacist owner/manager, and sought their views on the dispensing workflow diagram presented by HMA. The general processing of a script under the forward dispensing model was as follows: (1) Customers tend to go to a central counter, in the middle of the shop, for script processing. A
pharmacy assistant usually receives the script from the customer. They then fill out a ‘customer prescription information’ form, which is a paper-based form that captures the customer’s name, brand preference, Medicare number, etc. The form is a standard form used across all the banner group’s pharmacies.
(2) This form, together with the script, is put in a plastic tray and placed on the desk at the front of the
dispensary (note that this was a forward pharmacy). (3) The dispensary assistant or pre-registrant pharmacist then usually enters the script into the system.
The pre-registrant pharmacist, dispensary assistant or pharmacist would then process the script. If the medication was a new drug for the customer, this was stamped on the script, as a signal to provide CMI/counselling to the patient when they collect the medication. The pharmacist owner/manager estimated that around one-third of all scripts required counselling.
(4) The form, script and medication were then placed on a certain section of the bench for a pharmacist
to check. (5) The pharmacist would counsel the patient as required (if the form indicated that this was new
medication or any other issue flagged). If no counselling was required, either the pharmacist, dispensary assistant or intern pharmacist may give the patient their medicine.
(6) Any staff member (depending on how busy the store is) will then collect the customer’s payment at
the store’s exit. HMA note the following points on this pharmacy’s dispensing process: (1) The use of standard information stamps. The dispensary assistant would enter the script details
into the pharmacy system. If there was a drug change or interaction it would be flagged by the system (Amfac). The dispensary assistant would then stamp on script (using a rubber stamp) to indicate to the pharmacist that they will need to consider this issue when checking the dispensed script and providing patient counselling. The pharmacy manager/owner commented that the dispensary assistant “knows their limits” and would refer to the pharmacist. Example stamps were ‘had before’, ‘interaction’, ‘check’ and ‘see pharmacist’.
(2) The final check of medication. A pharmacist would always perform a final check of all
medication that was dispensed.

DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process
The pharmacist manager/owner confirmed that the role of the pharmacy assistant was to accept the script from the customer. The pharmacy assistant would usually greet the customer, depending on how busy the pharmacy was. They would then fill out the ‘customer prescription information’ form. All shop staff were specifically trained to complete this form. Pharmacy assistants may give the checked dispensed medication to a customer. They would usually collect a customer’s payment. The role of the dispensary assistant in the dispensing process
This site made very effective use of dispensary assistants in the dispensing process using a forward pharmacy dispensing model. Dispensary assistants would effectively undertake the entire dispensing process on receiving the script, through to the final check of the medication (this check would always be completed by a pharmacist). The same process in the dispensary would apply for dispensary assistants and for intern pharmacists. If no counselling was required, the dispensary assistant may give the patient their medicine and collect their payment. Both the pharmacy owner/manager and a pharmacist commented that the dispensary assistants (in this pharmacy) “know their limits – they have been trained to get the pharmacist when required”. Dispensary assistants also generally did all the stock control in the dispensary, and the completion of the HIC claims. They may also be involved in nursing home deliveries; the dispensary assistant would go to the nursing home, collect the scripts and take patients’ details, and process these scripts upon return to the pharmacy. The pharmacist would then check the dispensed medication. Webster packing was often completed by a dispensary assistant (or an intern pharmacist), which is then checked by a pharmacist. The role of pharmacy and dispensary assistants in the non-dispensing workflow
Pharmacy assistants tended to specialise in a particular area of the front-of-shop operations of the pharmacy. Each assistant was responsible for their section – they provide product advice to customers, saw product representatives to order stock, received stock and put it on the shelves. The pharmacy employed a full-time ‘service manager’ to oversee and run the front-of-shop operations and the pharmacy staff roster. Dispensary assistants would also help out in front-of-shop activities depending on how busy the pharmacy was. This would usually involve assisting customers with product information. The pharmacist owner/manager thought that dispensary assistants could be more involved in S3 medication counselling with increased training. They commented that “it would be good if they could be involved from ‘go to woe’ with S3 medicines. Pharmacy and dispensary assistant training
The banner group to which this pharmacy belonged conducted its own in-house training programs for its pharmacy support staff. The pharmacist owner/manager commented that the group was currently ensuring that all staff were “certificate training accredited”. This included running their own dispensary assistant training course (equivalent to the Guild training). Their training programs were a combination of face-to-face and workbook training. The pharmacist owner/manager said that the group was “very supportive” of assistant training. Other issues

This banner group had a pool of pharmacy staff that could be rotated through their stores (over 30 stores in South Australia). This helped to formalise training for support staff. The pharmacist owner/manager thought that the ‘forward model’ did not significantly impact on the role of pharmacy/dispensary assistants. They felt that the layout of the shop and the delegation capabilities of the pharmacist were more important. They also commented that the model worked well, as the pharmacist was close enough to interact with the customers, while also being close enough to supervise other staff. The pharmacist owner/manager thought that it was a good idea to create an intermediate level between the pharmacist and a current dispensary assistant. They argued that this role could also be more involved in S3 medication counselling (with appropriate training), which would leave more time for the pharmacist to counsel patients on S4 medicines.
Pharmacy 12 (WA 1) PHARMACY CHARACTERISTICS Location
Western Australia Metropolitan Shopping centre Dispensing model
Traditional Size
Average weekly scripts: 0-400 Estimated turnover: $1.0-$1.5m Dispensary assistant used in the pharmacy: No DISPENSING PROCESS AT THE CASE STUDY SITE HMA discussed the dispensing model with the pharmacist owner and sought their views on the dispensing workflow diagram presented by HMA. The general processing of a script was described as similar to the template. The pharmacist liked to give out all dispensed prescriptions to patients, especially new scripts, but pharmacy assistants might “hand out repeat scripts.” DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process
The pharmacist stated that the pharmacy assistants had no formal role in the dispensary, other than to receive scripts from the patient. However, it was also commented that:
“….a pharmacy assistant may occasionally select a medicine off the shelf, and only when the pharmacist is busy.”

The pharmacist commented that “it is difficult to see how a dispensary/pharmacy assistant could be more heavily involved in the dispensing process, even with more sophisticated software support….and in any case it would be difficult to justify financially in a pharmacy with a relatively small proportion of turnover attributable to prescription sales [40%].” The senior pharmacy assistant commented that she would “put through the details [into the dispensing software] a couple of times per week when there is a run of scripts so that they are ready for [the pharmacist] to check ….but I have problems dealing with the abbreviations and I have to stop work whenever there are interactions [identified by the software].” The role of the dispensary assistant in the dispensing process
Not applicable. There was no dispensary assistant employed in the pharmacy. The role of pharmacy and dispensary assistants in the non-dispensing workflow
A lot of the pharmacy turnover was attributable to sales of retail products other than prescription medicines. The pharmacy was operating in an area frequented by a large number of tourists. Apart from retail sales, the pharmacy assistants were heavily involved in ordering stock, unpacking, pricing, and stocktaking. Pharmacy and dispensary assistant training
The senior pharmacy assistant commented that she “could not be bothered doing a course.” Other issues
The pharmacist commented that dispensary assistants were less common in Western Australia that other states/territories because pharmacies were generally smaller in size (and therefore found it difficult to warrant use of a dispensary assistant). The pharmacist noted that in his 30 years of professional experience he had never worked with a dispensary assistant.
Pharmacy 13 (WA 2) PHARMACY CHARACTERISTICS Location
Western Australia Metropolitan Shopping centre Dispensing model
Traditional Size
Average weekly scripts: 401– 800 Estimated turnover: Less than $1.0m Dispensary assistant used in the pharmacy: No

DISPENSING PROCESS AT THE CASE STUDY SITE HMA discussed the dispensing model with the pharmacist owner/manager, and sought their views on the dispensing workflow diagram presented by HMA. The general processing of a script was different from the template in the following areas:
the age of patient was not recorded on the script unless it related to a child; the pharmacy assistant recorded if the patient was ‘waiting’ by marking ‘W’ on the script; and the pharmacist always took responsibility for each script being ‘signed off.’ Key steps in the dispensing process were: (1) The pharmacy assistant received scripts from patients and completed a ‘prescription receipt’, which
included clarification of whether a patient was prepared to use a generic drug. Depending on workloads, this collection process for the script could also be done by the pharmacist (“If I don’t have a script I will tend to greet the patient,” said the pharmacist). The pharmacist said that they may take up to 50% of scripts at the time of initial patient contact.
(2) The script would then be placed in a dispensing box and placed on the ‘waiting for processing’ shelf.
(3) The pharmacist would collect the dispensing box from the shelf. (4) The pharmacist would check the medication history and print the label, prior to selecting the stock. (5) The labels and cautionary and advisory labels would then be placed on the picked stock. (6) Prepared medication would then be placed on the ‘waiting for checking’ shelf. All medications
were checked by another member of the dispensary. (7) Counselling was generally undertaken by the pharmacist unless the medication was not being
dispensed for the first time and there was only a simple point to be made to the patient. First time counselling (new patient and/or new medication) was always undertaken by the pharmacist.
DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process
The pharmacy assistant in this shop had a small and tightly defined role around their involvement in the dispensing process. This comprised involvement in the ‘drop off and collection’ of scripts. Depending on workloads, this collection process for the script could also be done by the dispensary assistant or pharmacist. When a new script came in the recipient in the pharmacy would complete a ‘prescription receipt’, which included clarification of whether a patient was prepared to use a generic drug. The pharmacist said that pharmacy assistant involvement was inappropriate in several areas: (1) Checking patient history: pharmacy assistants would not have a full appreciation of the impacts
that a drug may have, including the range of possible drug impacts, interactions, and drug allergic reactions.
(2) Call prescribers: the doctor needs to be confident that the person on the other end of the phone line “knows what they are talking about”.
(3) Webster packs: patients were very reliant on the pharmacy for the accuracy of pack loading and this could be hard to check in the packs.
(4) First time counselling: it was very important that the patient understood why they were taking a drug, how to take it, how long for, possible side effects, and to check what other medications they may have.
Pharmacy assistants could be more involved in reconstitution of drugs “but I have the time” and therefore this did not occur. The pharmacy assistant was undertaking Guild Level IV training at the time of the visit. She had worked in the pharmacy for some time and was involved in checking the patient’s medication history. The pharmacist described her as ‘exceptional’ and said that she would not allow all assistants to undertake

such roles. The pharmacy assistant was also involved in providing simple instructions to patients on the use of medications (eg antibiotics). However, the pharmacist commented that she “liked to do it [the dispensing process] from start to finish”. This was generally feasible in the pharmacy because of the relatively small prescription volume. The pharmacy assistant noted that on weekends when working with the proprietor the assistant would be allowed to enter the script details into the dispensing system. However, during the week the pharmacist would prefer to enter the script details “unless we are very busy.” The role of the dispensary assistant in the dispensing process Not applicable. There was no dispensary assistant employed in the pharmacy. The role of pharmacy and dispensary assistants in the non-dispensing workflow The pharmacy assistant undertook ordering, prepared daily printouts of script activity, stocktakes, saw sales representatives, and prepared rosters. The proprietor managed the pharmacy accounts (using MYOB). Pharmacy and dispensary assistant training
The pharmacy was supportive of assistant undertaking certificate training. The pharmacy was currently supporting one assistant to undertake Level IV training. It had also paid for another member of staff to obtain recognition of prior learning. This had occurred prior to the introduction of accreditation. The pharmacy assistant undertaking Level IV was allowed up to 20% time off to undertake their training. The course was “adding value but it does get tedious and repetitive.” Other issues
The pharmacy used a scanner to reduce the risk of picking errors.
Pharmacy 14 (Tas 1) PHARMACY CHARACTERISTICS Location
Tasmania Metropolitan Shopping centre Dispensing model
Semi-forward Size
Average weekly scripts: 1600 – 2000 Estimated turnover: $3.5 – $4.0m

DISPENSING PROCESS AT THE CASE STUDY SITE HMA sought the pharmacist owner/manager’s views on the dispensing workflow diagram during the case study visit to verify its accuracy. The main points of difference were:
the pharmacy does not capture the age of patient unless it is a child; the pharmacy captures the time a script is brought in sometimes; the dispensary assistant or a pharmacist checks that the stock for a script is in the dispensary (usually
the pharmacist); entering patient information into the dispensing system is very different for new patients than for
existing patients; and the patient’s Medicare number is used as the unique identifier (rather than patient demographics)
wherever possible, and is always checked. A summary of the dispensing process used in this pharmacy is as follows: (1) A pharmacy assistant receives the script from the customer. They then complete a ‘prescription
receipt’ form, which is a paper-based form that captures the customer’s name, whether they will wait, etc.
(2) This form is then put in its own plastic tray with the script and placed on the lower shelf in the
dispensary, waiting to be dispensed. The trays are placed in priority order for dispensing. (3) The dispensary assistant or pharmacist would then enter the customer’s details from the script into
the dispensing software. (4) The dispensary assistant or pharmacist would then print the label and select the item(s) from the
shelves while the label is printing. (5) Each item was scanned to check that items were as per the medication information entered into the
dispensing software. (6) The labels were then placed on the medication(s). (7) The medication was put back into the plastic tray, which was placed on the upper shelf in the
dispensary, ready to be checked. (8) A different pharmacist (or dispensary assistant) would check the items when there was a lull in the
dispensing process. (9) The checked medication was then placed on a separate shelving system, awaiting customer
collection. HMA found this dispensing process to be systematic and thorough, complemented by a logical layout in the dispensary. Some key points to note about the process are: (1) The use of a scanner. The pharmacist owner/manager thought the use of a scanner in the
dispensary was a major asset. The scanner was used to check that the drug selected from the shelf matched the item(s) entered into the dispensing software (ie it helped to detect picking errors). The scan was undertaken once the pharmacist or dispensary assistant had picked the medication from the self, just before the label has been put on the medication container.
(2) Multiple shelves. There was an effective use of two separate shelves for the pre-dispensed and
post-dispensed (unchecked) medication. Once checked, completed scripts were then put in a third shelving system to the side of the dispensary.

(3) Rigorous checking process. Every dispensed medication was checked by another pharmacist or the dispensary assistant.
The pharmacist owner/manager confirmed that, in most cases, the only difference between the dispensing process for the dispensary assistant and a pharmacist was the checking stage and the patient counselling stage. The number of new patients per week impacted on the amount of data entry that had to be completed. This pharmacy had a large number of new patients each week (around 125), which required “continually entering new data”. This was probably a function of its size and location (ie in a relatively large shopping plaza). DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process
The pharmacist owner/manager said that the role of the pharmacy assistant was to accept the script from the customer; the pharmacy assistant usually greeted the customer and entered the customer’s name, address details, date, etc on the ‘prescription receipt’ form. Pharmacy assistants did not undertake data entry into the dispensing system. The pharmacist owner/manager saw it as impossible to expand pharmacy assistants’ role outside accepting the script from the customer, and could not envisage expanding their role in the dispensing process. The role of the dispensary assistant in the dispensing process
The pharmacist owner/manager described the dispensary assistant as “exceptional” and “extremely competent”. The dispensary assistant has been with the pharmacy for eight years. The dispensary assistant would often complete the entire dispensing process, except for checking, which was always done by another pharmacist. They would check the customer’s medication history; in the dispensing system (Fred), a screen would indicate whether a drug was a new drug for this patient. If there is any anomaly, the dispensary assistant would put a red sticker on the prescription receipt form, which flagged that the pharmacist needed to talk to that patient. The dispensary assistant would then fill the script. The dispensary assistant said that they felt entirely comfortable doing the entire process. They felt that if there was any question at all that they were not confident with then they would go straight to the pharmacist. In cases where the dispensary assistant did the dispensing a sticker indicating the dispensary assistant’s name was placed on the prescription receipt form. This acted as a trigger for the pharmacist to thoroughly check the script at the end of the process. In those cases, the pharmacist would make sure that the prescription details were correct. They would check:
the drug and drug strength; the dosage; the drug quantity; to ensure the correct patient; to ensure the correct doctor; and that the drug’s expiry date, C&A labels and batch number were visible. The pharmacist would then initial the script to ‘sign it off’.

The pharmacist owner/manager felt comfortable with the dispensary assistant providing “simple information about the medication” to the customer, but “never patient counselling”. For example, the information that would be provided by the dispensary assistant would include simple instructions (eg about antibiotics). The dispensary assistant said that they would provide “general information” (eg take medication with food). Once a patient began to ask questions, the dispensary assistant would refer them to the pharmacist. This point was stressed by the dispensary assistant; they said that if the customer has any questions, or if they were at all not sure abut an issue, they would refer straight to the pharmacist. The dispensary assistant said this was also a compliance issue (a belief that if the pharmacist comes down to talk to the patient, it must be important, etc). The pharmacist owner/manager indicated that the only real difference between the dispensing process for a pharmacist and the dispensary assistant was the checking process. The pharmacist would “more thoroughly check” those processed by the dispensary assistant. The dispensary assistant pointed out several activities in the dispensary that they did not undertake. These were:
mixing creams, etc (“extemporary activities”), as the pharmacist has to check the balances anyway, they might as well just do the lot to avoid double handling;
contacting the GP; recording the monthly balance on narcotics scripts; and patient ‘counselling’. The pharmacist owner/manager argued that the IT systems were very comprehensive, and flag any minor problems automatically on the screen. This provided adequate support and warnings on drugs that people often made mistakes on (PDL warnings). When processing a script the user needed to override these warnings to proceed through to the next stage of processing the script. The HIC claims process was usually completed by the dispensary assistant (or student pharmacist). Filling Webster packs was usually done by a part-time assistant, who did this activity for a number of pharmacies. In their absence, the dispensary assistant sometimes did this task. Once again, each pack was always checked by a pharmacist. The pharmacist owner/manager said that the more complicated scripts tended not to be processed by the dispensary assistant. These were usually scripts with many medications. The role of pharmacy and dispensary assistants in the non-dispensing workflow
The pharmacist owner/manager expressed the view that an assistant could undertake most activities in the pharmacy outside the dispensary, “depending on their ability”. In this pharmacy, an assistant managed the point of sale software, completed the staffing and rostering of assistants (not pharmacists, which was done by the senior pharmacist), promotions, buying and stock control. Pharmacy assistants were not involved in the administration of the payroll, which was done by a part-time administration officer/bookkeeper. The owner of the pharmacy always wrote business plans, determined financial strategy, etc. Pharmacy and dispensary assistant training
The pharmacist owner/manager said that the pharmacy encouraged pharmacy and dispensary assistants’ training and covered all training-related expenses.
The dispensary assistant completed dispensary training in 1996 (equivalent to the current Guild Level 3 certificate), which they found to be “very good”. The assistant was currently completing Certificate IV training, which they felt was “a lot of work”, however the material was “very usable” and “just makes sense”. They also commented that this training had helped them in their day-to-day work; they would complete a section of the training package and then apply it in their everyday activities. They were also looking at completing a vitamin course at Swinburne University by distance learning. The dispensary assistant commented that the pharmacy was very flexible around training programs, and allowed time off to go to training. For example, they had taken 3 consecutive days off five times in a six month period to complete the Certificate IV (including RPL). They have also found Jenard (the private provider of ‘Guild training’ in Tasmania) to be flexible, and coursework could be completed by distance learning if required. The dispensary assistant said that training programs were found largely through word-of-mouth or by searching the internet. Pharmacy assistants often get to know staff at other pharmacies via product information sessions, etc. Other issues
The dispensary assistant thought that there should be guidelines which make clearer what dispensary assistants can and cannot do. They also commented that the Guild was a good contact point to answer questions. For example, issues regarding training, and queries on pay. The dispensary assistant was indifferent about the creation of an intermediate level between the pharmacist and a current dispensary assistant. They were already completing many of the tasks in the dispensary, and felt that a person needed to have hands-on experience to perform checking of medication.
Pharmacy 15 (Tas 2) PHARMACY CHARACTERISTICS Location
Tasmania Rural Shopping strip Dispensing model
Traditional Size
Average weekly scripts: under 400 Estimated turnover: less than $1m DISPENSING PROCESS AT THE CASE STUDY SITE HMA sought the pharmacist owner/manager’s views on the dispensing workflow diagram during the case study visit to verify its accuracy. The pharmacist confirmed that it was accurate for this pharmacy.
The owner of the pharmacy was the only pharmacist employed at the pharmacy. They would complete the vast majority of the end-to-end dispensing process. The pharmacy assistant would receive the script from the patient and place it on the bench in the dispensary. The pharmacist would then undertake the entire dispensing process. If required, he would counsel the patient when they collected their script (often from over the high bench in the dispensary). The pharmacy assistant would then complete the sales transaction by collecting the customer’s payment. DISCUSSIONS AT THE CASE STUDY SITE The role of the pharmacy assistant in the dispensing process
The role of the pharmacy assistant was to receive the script from the customer and give it to the pharmacist. After the pharmacist has processed the script, the pharmacy assistant would give the medication to the customer, ask them to sign the script and collect the payment. The role of the dispensary assistant in the dispensing process
There were no dispensary assistants employed in this pharmacy. However the pharmacist had views on their role based on other pharmacies that he had worked in. The pharmacist owner/manager felt that a dispensary assistant could undertake dispensary activities up to putting the label on the medication (ie entering the data into the dispensing software, generating the label, selecting the stock from the shelves). He said that he would never allow a dispensary assistant to put a label onto the medication. He maintained that the pharmacist should always do this; this was the pharmacist’s time to check the label against the product. This was driven by his view that the pharmacist is ultimately responsible for that script. The pharmacist argued that best practice is to never have two labels or two products in one’s hand at any given point in time. The pharmacist believed that there is limited scope to increase the role of dispensary assistants in the dispensing process in a pharmacy of the kind he operated, given its dispensing volume. He thought that this would be the case for most one-owner, rural or city pharmacies. One area that the pharmacist felt could be delegated to assistants was “orders” (eg national diabetes services scheme). This appeared to be largely an administrative function. The role of pharmacy and dispensary assistants in the non-dispensing workflow
The pharmacy assistants undertook the usual “shop work”. This included re-stocking shelves, serving customers, and cleaning. There were only two assistants in the pharmacy so formal rostering was not required (“just a phone call”). Similarly, both assistants coordinated the ordering and buying of stock. This was described as “common sense” as there was not a large stock turnover in the pharmacy due to its size. The more senior pharmacy assistant did the books for the pharmacy. The pharmacy assistant thought that their role could be expanded on the “health side”, providing more information and guiding customers to what they want and need. They envisaged that the pharmacist would oversee and check this. Pharmacy and dispensary assistant training
The more junior of the pharmacy assistants had recently completed Certificate I through Jenard (see below). They described the training as “a lot of common sense”, however “very worthwhile”. They

thought that it provided good hints, especially on medication. It also provided a good grounding on how to deal with certain customer management situations, and provided a good context for pharmacy (they had worked in other retail industries). The pharmacy assistant was planning to undertake further training (ie Certificate II and potentially Certificate III). They said that this pharmacy’s attitude to training was “pretty good”. Most of the training that she had completed was outside work hours by distance learning. She commented that the senior pharmacy assistant occasionally went to Hobart for training courses. Other issues
The pharmacy assistant stressed the importance of customer service in rural pharmacy, and highlighted the need to be extremely aware of all customers. They pointed out that it was imperative to not put anyone offside, as the result could be a significant loss of customers and a large impact on the business.

Attachment G
TIME-AND-MOTION DATA
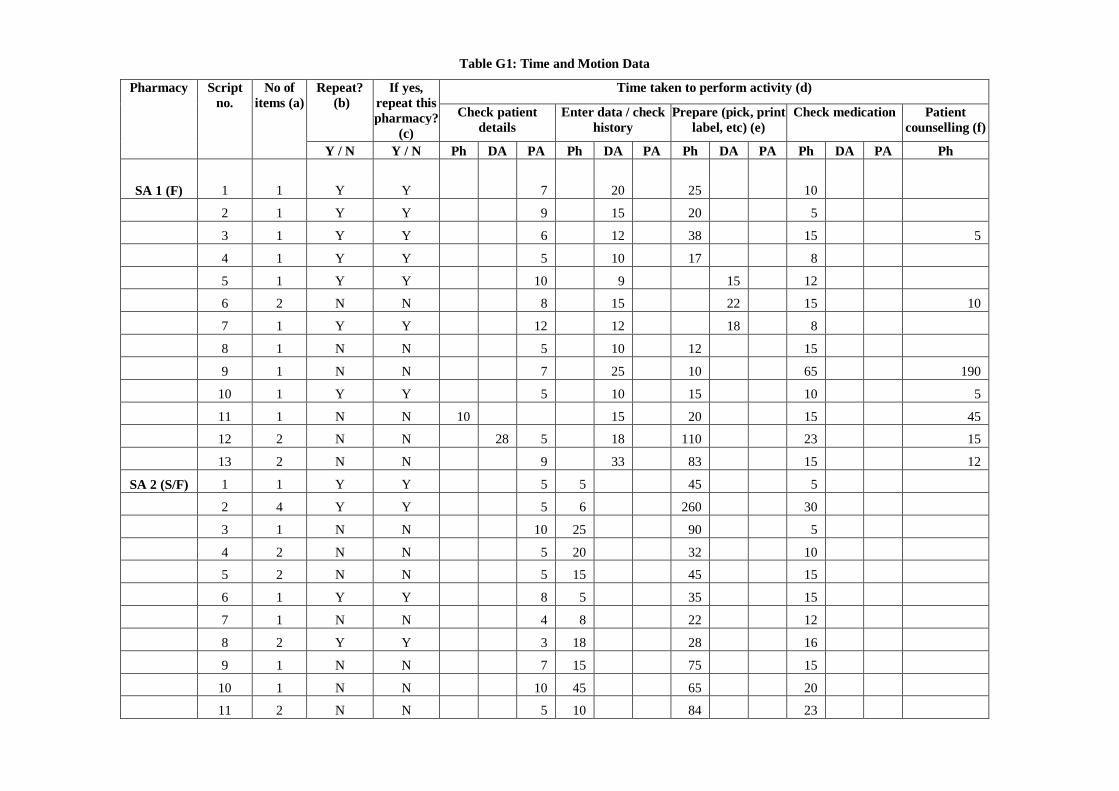
Table G1: Time and Motion Data
Time taken to perform activity (d) Repeat? (b)
If yes, repeat this pharmacy?
(c) Check patient
details Enter data / check
history Prepare (pick, print
label, etc) (e) Check medication Patient
counselling (f)
Pharmacy Script no.
No of items (a)
Y / N Y / N Ph DA PA Ph DA PA Ph DA PA Ph DA PA Ph
SA 1 (F) 1 1 Y Y 7 20 25 10
2 1 Y Y 9 15 20 5
3 1 Y Y 6 12 38 15 5
4 1 Y Y 5 10 17 8
5 1 Y Y 10 9 15 12
6 2 N N 8 15 22 15 10
7 1 Y Y 12 12 18 8
8 1 N N 5 10 12 15
9 1 N N 7 25 10 65 190
10 1 Y Y 5 10 15 10 5
11 1 N N 10 15 20 15 45
12 2 N N 28 5 18 110 23 15
13 2 N N 9 33 83 15 12
SA 2 (S/F) 1 1 Y Y 5 5 45 5
2 4 Y Y 5 6 260 30
3 1 N N 10 25 90 5
4 2 N N 5 20 32 10
5 2 N N 5 15 45 15
6 1 Y Y 8 5 35 15
7 1 N N 4 8 22 12
8 2 Y Y 3 18 28 16
9 1 N N 7 15 75 15
10 1 N N 10 45 65 20
11 2 N N 5 10 84 23
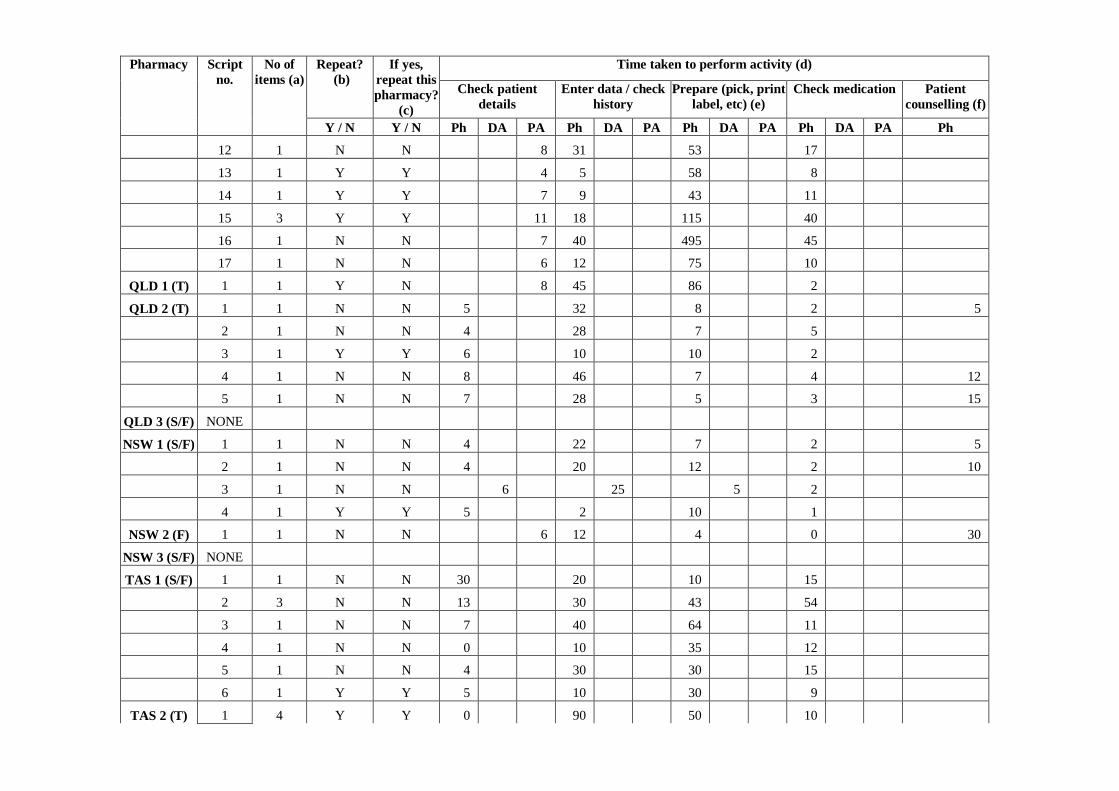
Time taken to perform activity (d) Repeat? (b)
If yes, repeat this pharmacy?
(c) Check patient
details Enter data / check
history Prepare (pick, print
label, etc) (e) Check medication Patient
counselling (f)
Pharmacy Script no.
No of items (a)
Y / N Y / N Ph DA PA Ph DA PA Ph DA PA Ph DA PA Ph
12 1 N N 8 31 53 17
13 1 Y Y 4 5 58 8
14 1 Y Y 7 9 43 11
15 3 Y Y 11 18 115 40
16 1 N N 7 40 495 45
17 1 N N 6 12 75 10
QLD 1 (T) 1 1 Y N 8 45 86 2
QLD 2 (T) 1 1 N N 5 32 8 2 5
2 1 N N 4 28 7 5
3 1 Y Y 6 10 10 2
4 1 N N 8 46 7 4 12
5 1 N N 7 28 5 3 15
QLD 3 (S/F) NONE
NSW 1 (S/F) 1 1 N N 4 22 7 2 5
2 1 N N 4 20 12 2 10
3 1 N N 6 25 5 2
4 1 Y Y 5 2 10 1
NSW 2 (F) 1 1 N N 6 12 4 0 30
NSW 3 (S/F) NONE
TAS 1 (S/F) 1 1 N N 30 20 10 15
2 3 N N 13 30 43 54
3 1 N N 7 40 64 11
4 1 N N 0 10 35 12
5 1 N N 4 30 30 15
6 1 Y Y 5 10 30 9
TAS 2 (T) 1 4 Y Y 0 90 50 10

Time taken to perform activity (d) Repeat? (b)
If yes, repeat this pharmacy?
(c) Check patient
details Enter data / check
history Prepare (pick, print
label, etc) (e) Check medication Patient
counselling (f)
Pharmacy Script no.
No of items (a)
Y / N Y / N Ph DA PA Ph DA PA Ph DA PA Ph DA PA Ph
2 1 Y Y 0 15 30 5
3 1 Y Y 0 22 60 20
4 1 Y Y 0 5 10 5
5 3 Y Y 0 18 60 10 5
6 1 N N 0 153 40 4 2
WA 1 (T) NONE
WA 2 (T) 1 4 Y Y 10 48 300 15 65
2 3 Y Y 32 65 70 10 20
3 1 N N 5 180 70 20
4 1 N N 10 45 45 10 25
5 1 N N 5 25 100 15 55
VIC 1 (F) 1 2 Y Y 0 20 60 10 15
2 1 Y Y 0 10 20 10 10
3 2 Y Y 0 35 30 10 5
4 1 N N 10 5 40 20 0
5 1 N N 15 20 60 10 15
6 2 N N 10 90 30 10 30
7 1 N N 15 70 35 20 40
8 4 Y Y 0 30 75 15 30
VIC 2 (F) NONE
VIC 3 (SF) 1 2 Y Y 15 25 10 10 15
2 2 Y Y 20 10 5 15 0
3 5 N N 30 25 10 5 0
4 1 Y Y 10 5 25 5 5
5 3 Y N 20 20 35 15 55
6 1 Y N 10 10 15 5 15

Time taken to perform activity (d) Repeat? (b)
If yes, repeat this pharmacy?
(c) Check patient
details Enter data / check
history Prepare (pick, print
label, etc) (e) Check medication Patient
counselling (f)
Pharmacy Script no.
No of items (a)
Y / N Y / N Ph DA PA Ph DA PA Ph DA PA Ph DA PA Ph
7 2 Y N 10 15 15 10 72
8 2 Y N 20 15 25 15 10
(a) The number of items on the script - this can be found by identifying the number of labels printed, the number of medications dispensed (b) Is the script a repeat? A repeat has a large yellow band across the CENTRE of the script (note that some non-repeat scripts have yellow on the base of the script) (c) Is the repeat from this pharmacy or another pharmacy? If this pharmacy, they only enter a small digit code into the computer (4 numbers?); if it is an external repeat they
enter person's name and other details (d) Seconds spent on each activity by the pharmacist, dispensary assistant and/or the pharmacy assistant; record time in relevant column for each staff member completing the
tasks (e) The preparation of medication stage appears to commence when the labels are printed (tbc through the case studies) (f) This may not occur during the observation period because the patient may not return within the hour

Attachment H
INTERNATIONAL ORGANISATIONS CONTACTED

Table H1: Overseas Stakeholder Organisations Contacted by HMA
Country Organisation Name Outcome
European Foundation for the Advancement of Healthcare Practitioners No response
Austria Österreichische Apothekerkammer No response Österreichischer Apothekerverband No response Denmark Danmarks Apotekerforening No response Dansk Farmaceutforening No response Finland Association of Finnish Pharmacies No response Finnish Pharmacists Association No response Finnish Pharmacists Society No response
France Association de Pharmacie Galénique Industrielle (APGI) No response
Conseil National de l'Ordre des Pharmaciens Provided documentation and other contact details
Fédération des Syndicats Pharmaceutiques de France No response Société Française de Pharmacie Clinique No response
Syndicat National des Pharmaciens Praticiens Hospitaliers et Praticiens Hospitaliers Universitaires No response
Union des Syndicats de Pharmaciens d'Officine No response
Germany Bundesvereinigung Deutscher Apotekerverbande (ABDA) No response
Italy Federazione Ordini Farmacisti Italiani (FOFI) No response
Federfarma Provided background information
Netherlands Royal Dutch Society for the Advancement of Pharmacy No response Dutch Scientific Institute for Pharmacy Practice No response Norway Norges Farmaceutiske Forening No response Norsk Farmaceutisk Selskap No response
Spain Consejo General de Colegios Oficiales de Farmaceuticos No response
Sweden National Corporation of Swedish Pharmacies (Apoteket) No response
Apotekarsocieteten No response Sveriges Farmacevtförbund No response
United Kingdom Royal Pharmaceutical Society of Great Britain Provided extensive documentation
Academy of Pharmaceutical Scientists No response Ireland Pharmaceutical Society of Ireland No response
USA American Pharmacists Association Referred queries to PTCB (below)
National Association of Boards of Pharmacy Provided documentation Suggested contacting PTCB
American Society of Health System Pharmacists No response
American Association of Pharmaceutical Scientists (AAPS) No response
American Association of Pharmacy Technicians No response National Pharmacy Technician Association No response
American Association of Colleges of Pharmacy Provided advice Suggested contacting PTCB
Pharmacy Certification Board
Provided background information and extensive documentation
Canada Canadian Pharmacists Association (CPhA) No response
Canadian Association of Pharmacy Technicians Provided background information and website link

Attachment I
PHASE 2 DISCUSSION PAPER

Workforce and Career Options for Pharmacy Assistants
Discussion Paper on Draft Recommendations
Background
Overview of the Project In late 2002 the Pharmacy Guild of Australia (the Guild) appointed Healthcare Management Advisors (HMA) to identify those areas of current practice that may, with the provision of appropriate training, be assumed by dispensary and/or pharmacy assistants. The full terms of reference for the project are at Attachment A. HMA has prepared a detailed Phase 1 Report that provides an overview of the duties of pharmacy support staff, describes the regulatory framework applying to pharmacy support staff, and summarises key stakeholder issues raised in initial consultations. The report presents findings from a survey of 80 community pharmacies, undertaken to gain an understanding of current workflow processes, and case studies that looked at the allocation of tasks in more detail. HMA also carried out comprehensive research on the use and training of pharmacy/dispensary assistants (or their equivalents) in relevant overseas models.1 In late July 2004 the Phase 1 Report was circulated for comment to key stakeholders in the community pharmacy field, including representatives of State and Territory Guilds and Pharmaceutical Societies, pharmacy boards, departments of health/human services in each State/Territory, and heads of schools of pharmacy. Purpose of this Paper This paper outlines the draft recommendations that are being proposed by HMA based on the project work undertaken so far. HMA is seeking comments from stakeholders on the draft recommendations and the Phase 1 Report by the 8th September 2004. The paper also presents some suggested issues that the field may choose to comment on in preparing comments. Draft Recommendations
Draft Recommendation #1: The industry, in consultation with regulatory bodies and professional associations, should develop models to trial the training, facilitation and support for greater use of dispensary assistants with the input and checking of medication history. These trials should address issues of workflow and information technology support and should enable the key stakeholders to assess how these refined processes work in practice. Trials should only occur where the supervising pharmacist is comfortable that appropriate mechanisms are in place to ensure that patient safety and quality of care is not compromised. Draft Recommendation #2: In conjunction with the trials flagged in draft recommendation #1, the industry, in consultation with regulatory bodies and professional associations, should develop models to trial the training, facilitation and support for greater use of dispensary assistants in checking dispensed medication. These trials should address issues of workflow and information technology support and should enable the key stakeholders to assess how these refined processes work in practice. Trials should only occur where the supervising pharmacist is comfortable that 1 An electronic copy of the report can be obtained from HMA’s Adelaide Office, Ph 08 8150 5555

appropriate mechanisms are in place to ensure that patient safety and quality of care is not compromised. Background: A key part of the analysis undertaken by HMA was based on identifying common tasks in the dispensing process. The framework used is provided at Attachment B. The community pharmacy survey undertaken as part of the project, supported by observations at some case study sites, indicated that in many cases dispensary assistants are already checking patients’ medication history. The survey data suggested that pharmacy manager/owners and salaried pharmacists thought that dispensary assistants would check a patient’s medication history in approximately 50% of scripts processed, and this could be increased to around 60%. Dispensary assistants reported completing this task 80% of the time. Pharmacy manager/owners thought that dispensary assistants could enter patient information into the pharmacy system over 80% of the time. The survey data indicated that pharmacy manager/owners believe that dispensary assistants currently check the dispensed medication in about 50% of dispensed scripts and could not see more involvement in this task. The dispensary assistants reported this figure to be around 70%. Suggested Issues for Comment:
Are there other elements of the dispensing process, other than checking patients’ medication history and checking dispensed medication, that dispensary assistants could assume greater responsibility for?
What legal, financial, industrial and training issues need to be considered in undertaking the proposed trials?
How feasible is it to get greater uniformity across the field in the use of dispensary assistants across the key elements of the dispensing process?
Draft Recommendation #3: Mandating the broadening of roles by dispensary assistants should not extend to any involvement in patient counselling around dispensed medications. Background: The survey data did not support dispensary assistants being involved in regularly providing patient counselling to patients. The pharmacy manager/owners surveyed thought that dispensary assistants could undertake patient counselling on an occasional basis. This was consistent with the pharmacy manager/owners’ views expressed during the case study visits. On this basis, HMA sees a very limited role for dispensary assistants in providing patient counselling in Australia in the short to medium term. Suggested Issues for Comment:
Would it be possible to involve dispensary assistants in the patient counselling processes with greater training?
What should the nature of the training be? Draft Recommendation #4: There should be no extension of the role of pharmacy assistants in the dispensing process beyond their current tasks that concentrate on initial handling of the script, provision of the script to a patient where no pharmacist counselling is required, and collection of payments. Background: The findings from the survey, case studies and overseas research imply that pharmacy assistants should maintain a limited role in the dispensing process, restricted to: the initial handling of the script; and
the final collection of the script and payment.

Suggested Issues for Comment
Are there any other elements of the dispensing process where greater pharmacy assistant involvement could be considered?
Draft Recommendation #5: The Guild should consider change management initiatives aimed at facilitating greater use of assistants in operational roles where they have received Level III or IV certification to reduce the under-utilisation of existing training and trained staff. Background: The survey data and case studies suggested there is substantial scope for facilitating greater involvement of pharmacy/dispensary assistants in providing advice on S2 and S3 medication, complementary medicines, and ‘higher level’ operational activities such as financial reporting and people management. Suggested Issues for Comment:
How can the industry extend the take-up of Level III and IV certification courses by non-professional staff?
How can pharmacy managers/owners be encouraged to fully utilise the skills that their non-professional staff may wish to make greater use of following training?
Other Issues
If there is general support for the previous recommendations, further consideration on a number of other issues will be required. Terminology HMA consider there should be a nationally consistent term used to encompass the role of dispensary assistant / technicians. We suggest using the descriptor ‘community pharmacy technician’. Such terminology has several advantages, including:
a more professional connotation than ‘dispensary assistant’, which would be warranted if recommendations #’s 1 and 2 were implemented;
reduces the risk of confusing the role of community pharmacy technicians with hospital technicians by using the term ‘community pharmacy’; and
ensuring uniformity across the industry, in contrast to the current confusing use of terms. Careful consideration will need to be given to the industrial implications of such an approach before proceeding towards further implementation. Suggested Issues for Comment
Are there any impediments to a more common and standardised use of the term ‘community pharmacy technician’?
Training Subject to the general acceptance of draft recommendations 1-5, the greater involvement of dispensary assistants in medication history and checking dispensed medications would need to be reflected in the formalised National Competency Standards for assistants. This would become a specified minimum training standard. The extent of changes (if required) will be addressed in Phase 3 of the original project brief (outside of the scope of the current project). Suggested Issues for Comment
What changes to the National Competency Standards are required to facilitate more comprehensive training of dispensary assistants in checking medication history and checking dispensed medications?
Consistent Pharmacy Practice Guidelines Subject to the general acceptance of draft recommendations 1-5, the greater involvement of dispensary assistants in checking patient medication history and checking dispensed medications would need to be reflected in professional policy and practice guidelines. This would include specifying:
the minimum training standard of dispensary assistants; the activities that dispensary assistants can and cannot do; and the ratio of dispensary assistants-to-pharmacists in the dispensary (the 1:1 ratio could be relaxed if
there was additional support processes in operation). Suggested Issues for Comment
Are there other changes to professional policy and practice standards that need to be considered in response to draft recommendations 1-5?
Regulation and Certification The greater involvement of dispensary assistants in checking patient medication history and checking dispensed medications may need to be formalised through central registration processes, managed at a State and Territory Pharmacy Board level. A lack of regulation of dispensary assistants would make it difficult to discipline technicians in the event of misconduct. Suggested Issues for Comment
Could disciplinary processes be managed via a process other than legal regulation? Why would this form of regulation be more appropriate? Consideration of a role between a pharmacist and dispensary assistant During the situation analysis and case study process HMA sought stakeholder’s views on the creation of a new workforce role between a pharmacist and dispensary assistant. This would create a pharmacy service delivery model more closely approximating those operating in Sweden, Denmark and the Netherlands where there is extensive use of prescriptionists. Stakeholders had mixed views on the creation of such a role during initial consultations. HMA noted that some stakeholders were very supportive, without being specific about what such a position could and could not do. However, in general the views expressed by stakeholders did not support the creation of an intermediate role that would operate without the day-to-day supervision of a pharmacist and also be involved in patient counselling. Similar mixed views were expressed during the case study visits. Such an intermediate role would represent a significant change from current practice, and professional and community expectations. It may warrant future consideration in the medium-to-longer term, particularly in a rural context, where dispensing without the presence of a pharmacist in the pharmacy would assist in improving access to medicines. Such a workforce response is currently being investigated in the UK. Suggested Issues for Comment
Would creation of a prescriptionist role help the community pharmacy sector deal with the emerging workforce shortage of pharmacists?
A prescriptionist role has been introduced in several European countries with advanced health care systems. What makes such a role unsuitable in an Australian context?
How could the duties of a prescriptionist be different from a dispensary assistant?

Next Steps
The remaining stages of the project are:
seek stakeholder views on the draft recommendations for potential roles of dispensary and pharmacy assistants through circulation of the Phase 1 report for comments, by 8th September 2004;
estimate the impact of the changed roles through focus groups with pharmacists in Sydney, Melbourne, Brisbane and Adelaide; and
prepare the Phase 2 final report that synthesises the key findings from Phase 1, the results of our consultations and the cost/benefit modelling.
The final recommendations will be presented into the final project report to the EAG, after taking into consideration findings from the remaining processes described above. Healthcare Management Advisors 28 July 2004
Attachment A: Workforce and Career Options for Pharmacy Assistants: Project Scope
An extract from the project tender on the scope of the consultancy is provided below: “SCOPE OF THE PROJECT The main focus of this project is to identify those areas of current practice that may, with the provision of appropriate training, be assumed by dispensary and/or pharmacy assistants to free the pharmacist for professional and cognitive services. As noted above, there are currently a variety of guidelines for the use of dispensary assistants in state and territory jurisdictions. Training has been in place for several years, and has Pharmacy Board recognition where such a requirement exists. However, there is scope for this training to be used more widely to improve the skills of existing dispensary assistants, and it is expected that the project will examine this aspect in detail. Comprehensive training has also been available in areas related to front of shop operations since 1995. More recently, the demand for training at a higher level than previously available has become evident, indicating that more tasks are being delegated to non-pharmacist staff. The project is expected to encompass a number of phases. Firstly it will establish the current situation in Australia with regard to the use of dispensary assistants and compare that to several overseas models. Secondly, possible additional roles for dispensary assistants will be investigated and, if identified, endorsed by the industry. In addition, the project will investigate those roles that may be delegated to pharmacy assistants in the retail management area, to further assist pharmacists find time to devote to new initiatives. Finally, if identified as a need in Phase 2, competency standards and appropriate training will be developed to reflect the additional dispensary assistant and retail management roles. It is envisaged that the results of Phase 2 will be used to inform the detailed approach to Phase 3. It is expected that the successful tenderer will consult widely with stakeholders. Phase 1 Analysis of current workflow practices in community pharmacy dispensaries
Analysis of current role and usage of dispensary assistants in community pharmacy
Comparison of Australian dispensary assistant roles and usage with overseas models
Analysis of retail management functions currently undertaken by pharmacy assistants
Development of best practice models for pharmacies (relevant to different size or structure)
Phase 2 Identification of potential additional roles for dispensary assistants in community pharmacy (dispensing and other)
Identification of additional retail management roles and functions that may be delegated to pharmacy assistants
Industry and Pharmacy Board recognition of new roles
Cost benefit analysis of dispensary assistants in pharmacy (business case).”

Attachment B: Dispensary Workflow: Identification of Key Tasks
During our consultations the Pharmacy Board of New South Wales provided HMA with a high level process diagram of the standardised dispensing process in community pharmacy using the traditional model of dispensing. Figure B1 provides an adapted version of that framework.
Figure B1: Key tasks and responsibilities in a traditional dispensing model
Present Script Check if all items tobe dispensed
Check spelling ofcustomer name,address and age
Provide information(if required)
Record time scriptpresented [TBC]
Check entitlem’tdetails and record
on script
Provide information(if required)
Checkstock/equipment is
available
Ask if customerwill wait or collect;
mark script
Put script in pile tobe dispensed
Read script; liasewith customer and
pharmacist
Provide information(if required)
Enter script detailsinto computer
Check patientdemographics andmedication history
Provide information(if required)
Customer Pharm Assist Dispens Assist Pharmacist
Check script againstlabels; attach todrug and script
Call prescriber ifnecessary
Generate labels
Select stock
Attach warninglabels to drugs
Call customer
Check dispensedmedication, mark
script if counsellingrequired
Check script is forthis customer
Reinforceinstructions on
labels
Receive instructions(and conselling
where appropriate)Provide counselling
& CMI (whereappropriate)
Collect payment
Source: derived from Price Waterhouse Urwick (undated), provided to HMA by NSW Pharmacy Board