workbook - careerforce · welcome to this workbook for: demonstrate knowledge of support needs of a...
TRANSCRIPT

US 20966 Level 3 Credits 6
Name
Workbook Demonstrate knowledge of support needs of a person with a brain injury in an
aged care, health, or disability setting

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 2

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 3
Contents
Before you start ................................................................................................................ 4
The human brain .............................................................................................................. 7
Brain injury ..................................................................................................................... 11
Levels of injury ............................................................................................................... 14
The effects of brain injury ............................................................................................... 17
Support needs of a person with a brain injury ................................................................ 22
Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 4
Before you start
Welcome to this workbook for:
Demonstrate knowledge of support needs of a person with a brain injury in an
aged care, health, or disability setting
Unit Standard 20966.
For this unit standard you will have:
this workbook.
a trainee assessment.
In this workbook you will learn more about:
the anatomy of the brain.
types of brain injuries.
the way brain injuries are classified.
effects of brain injury on behaviours.
the support needs of a person with brain injury.
When you see a
sticky note like
this, it gives a tip
or hint.
How to use this workbook
this is your workbook to keep – make it
your own by writing in it.
use highlighters to identify important ideas.
do the learning activities included
throughout this workbook. Write your
answers in the spaces provided.
you might find it helpful to discuss your
answers with colleagues or your
supervisor.
finish this workbook before you start on
the assessment.
When you see a
sticky note like this, it
gives a tip or a hint.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 5
Workbook activities
Stop – check what you know about this topic
You will see this stop symbol in places where you
are asked to stop and think about what you know
and:
record your current knowledge
or impressions.
check your knowledge.
This stop provides a reference point to return
to later. Stop activities have blue shading like this.
Rewind
When you see this rewind symbol, go back to:
think about what you know.
check your knowledge.
This rewind gives you an opportunity to add to,
change or confirm some of your initial thoughts
and ideas. Rewind activities have green shading
like this.
Learning activities
You will come across learning activities as you
work through this workbook.
These activities help you understand and apply
the information that you are learning about.
Learning activities have yellow shading like this.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 6
Before you go any further in this workbook, think about...
Brain injury
Name three ways a brain injury can occur.
1
2
3
What are three effects a brain injury could have on a person?
1
2
3

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 7
The human brain
The brain has many different parts that all perform different functions and interconnect
with each other in a variety of ways. All activities that we perform every day, whether
they are physical or mental, and whether or not we are aware of it, are directed by
different parts of the brain.
The brain is protected by the skull but the inside of the skull is not completely smooth.
There are grooves for major blood vessels and ridges of bone. This means that even in a
head injury with no outward sign of damage, the brain can be bruised or cut, and blood
vessels may be damaged and leaking.
The effects of an injury to the brain will depend on what area of the brain is affected and
what functions that part of the brain controls.
Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 8
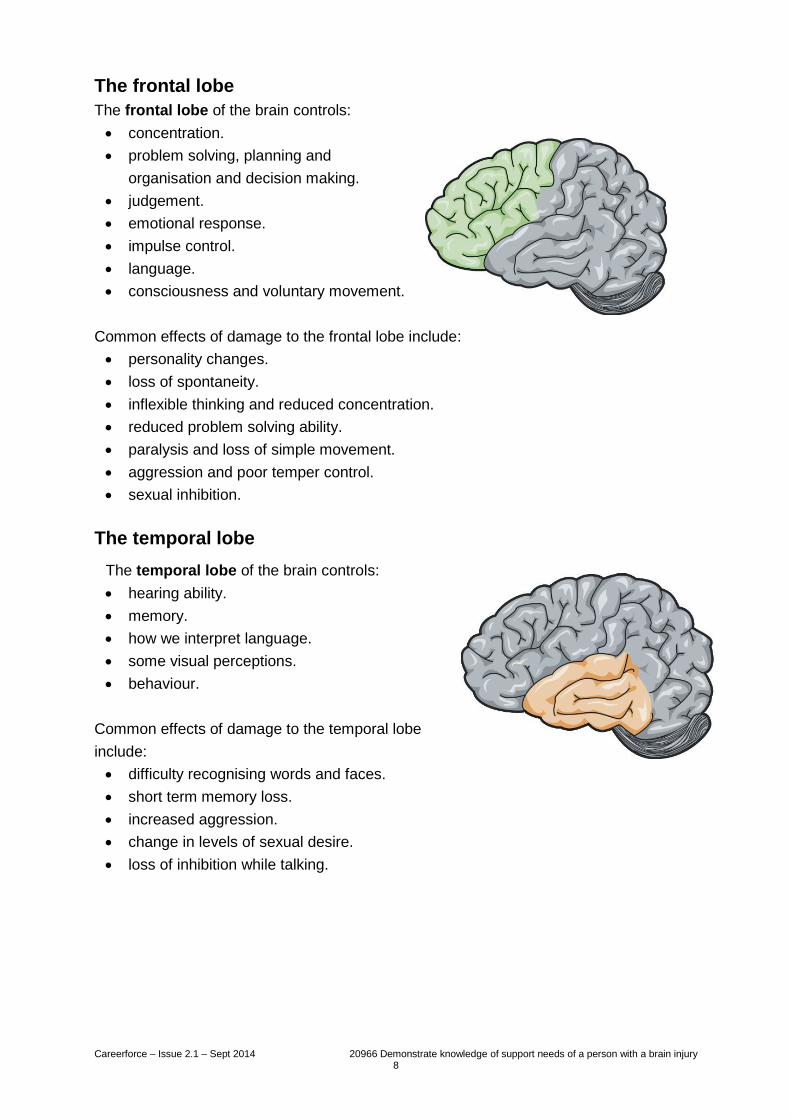
The frontal lobe
The frontal lobe of the brain controls:
concentration.
problem solving, planning and
organisation and decision making.
judgement.
emotional response.
impulse control.
language.
consciousness and voluntary movement.
Common effects of damage to the frontal lobe include:
personality changes.
loss of spontaneity.
inflexible thinking and reduced concentration.
reduced problem solving ability.
paralysis and loss of simple movement.
aggression and poor temper control.
sexual inhibition.
The temporal lobe
The temporal lobe of the brain controls:
hearing ability.
memory.
how we interpret language.
some visual perceptions.
behaviour.
Common effects of damage to the temporal lobe
include:
difficulty recognising words and faces.
short term memory loss.
increased aggression.
change in levels of sexual desire.
loss of inhibition while talking.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 9
The parietal lobe
The parietal lobe controls:
touch.
sensation – temperature and pain
perception.
spatial awareness – where the body is in
space.
Common effects of damage to the parietal lobe
include:
limb and facial movements affected.
changes in touch – how things feel.
difficulty distinguishing left and right.
problems with hand-eye coordination.
lack of awareness of body parts.
difficulty focusing visual attention.
problems with reading and drawing.
The occipital lobe
The occipital lobe controls vision, reading and
writing skills.
Common effects of damage to the occipital lobe
include:
difficulty identifying colours and recognising
drawn objects.
blind spots.
hallucinations.
difficulty with reading and writing.
The cerebellum is connected to the brain stem and coordinates movement and muscles,
balance and posture. Effects of damage to the cerebellum include tremors and dizziness,
slurred speech, the inability to grasp objects and problems with fine motor skills and
coordination.
The brain stem connects the brain to the spinal cord. The automatic functions of the
brain stem include those necessary for survival, such as breathing, heart rate, blood
pressure and the ability to cough and swallow.
Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 10
Hemispheres
The brain is divided into two halves, or hemispheres. Each hemisphere controls the
opposite side of the body. This means that a person who has a brain injury in the left
hemisphere may show the effects of this injury on the right side of their body.
The left hemisphere is responsible for the interpretation of information such as
mathematics, language, reasoning and some memory functions. The right hemisphere is
where the visual and spatial information is processed. The hemispheres are connected
by the corpus callosum which allows the two hemispheres to communicate.
LEARNING ACTIVITY
For the effects described in the following short scenarios, name at least one part of the
brain that could have been injured.
Bill has had a severe head injury. He is unable to breathe for himself and cannot swallow
food or water. He is in hospital on life support.
An area of the brain likely to have been damaged is:
Mary has become almost blind as a result of her brain injury. She has difficulty
recognising colours and recognising drawn objects. She has lost most of her reading and
writing skills.
An area of the brain likely to have been damaged is:
John’s personality has changed quite dramatically since his brain injury. He gets very
agitated and irritable. He is often aggressive. He cannot remember names or faces and
he cannot hear very well any more.
An area of the brain likely to have been damaged is:

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 11
Brain injury
There are two broad types of brain injury: congenital and acquired.
Congenital means that the injury is present at birth, having occurred either during the
development of the baby or during the birth process. Cerebral palsy is a common
example of this type of brain injury.
Acquired means that the brain injury has been ‘acquired’ during the person’s lifetime. An
acquired brain injury (ABI) includes any injuries occurring after birth, whether these result
from an injury involving trauma (such as a blow to the head) or an injury that does not
involve a trauma (non-traumatic), for example, a stroke.
Although ABI is the overall term, it is also sometimes used to differentiate an injury that is
non-traumatic from one that is a traumatic brain injury (TBI).
Traumatic brain injury
A TBI occurs when an outside force impacts the head hard enough to cause the brain to
move within the skull and be damaged or if the force causes the skull to break and
directly hurt the brain.
If the impact moves the brain within the skull but does not damage the skull, it is called a
closed head injury.
If the impact causes the skull and protective layers around the brain to be fractured,
come out of place, or be penetrated, it is called an open head injury.
Causes of TBI include:
car, motorbike
and bicycle
accidents.
falls.
sports injuries.
assaults.
firearm injuries.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 12
The brain is made of extremely delicate, soft tissue that can be compressed, pulled and
stretched and is essentially floating in fluid within the skull. An impact to the head or a
violent movement such as shaking can cause a diffuse (generalised) injury to the brain –
for example, concussion – and/or a focal injury, where a specific area of the brain is
damaged.
A focal (localised) injury occurs in one specific part of the brain due to brain tissue being
cut or torn, blood vessels being cut blocked or rupturing, or blood mixing with the tissues
to form bruises or collections of blood (haematomas).
A diffuse (global) injury is widespread damage to the brain caused by swelling and/or
damage to the axons which are the transmitters of the neurons.
It is common for both focal and global injuries to be present at the same time, so a
person may have generalised symptoms as well as problems specific to the area of brain
that has been damaged.
Concussion is the most common brain injury (around 90% of cases) and is an example
of a diffuse or global injury. Concussion is also known as mild traumatic brain injury or
MTBI. The effects of concussion usually wear off within days or weeks, but for a small
percentage of cases, the symptoms may last for months or even years. This condition is
known as post-concussion syndrome.
A more severe form of diffuse injury is diffuse axonal injury (DAI) which may be caused
by an acceleration/deceleration injury or by ischaemia (lack of blood supply). Most
people who have DAI will have experienced a prolonged period of unconsciousness or
may be in a coma from which they will never regain consciousness. Those people who
do wake up often remain significantly impaired.
A traumatic brain injury can also be:
primary – occurs at the time of the trauma.
secondary – may develop over a period of hours or days following the initial injury
as a result of swelling, pressure or chemical changes, or lack of oxygen.
The skull is a rigid box, and the amount of space taken up by the brain, blood and
cerebrospinal fluid (CSF) is a delicate balance. The pressure inside the skull is called
intracranial pressure (ICP). When this balance is disrupted, for example, by swelling or
an accumulation of blood between the brain and the skull, the ICP will start rising and
further brain damage may occur.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 13
Acquired brain injury (non-traumatic)
The brain can be injured by not receiving enough oxygen, bleeding within the brain or
swelling of the brain.
Causes of non-traumatic acquired brain injury include:
stroke.
aneurysm.
heart attack.
meningitis.
brain tumours.
alcohol and drug abuse.
toxic chemicals (poisoning).
hypoxia (not enough oxygen), or anoxia (no oxygen) for example, from near
drowning, choking, strangulation, chest injuries, allergic reactions.
LEARNING ACTIVITY
Read each short scenario. Tick to show whether you think the resulting brain injury
would be considered traumatic or non-traumatic.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 14
Levels of injury
The terms used to describe the level of brain injury is an indication of the possible long-
term effects on the person. There are three broad classifications:
mild brain injury.
moderate brain injury.
severe brain injury.
The tools used for assessing the classification of a brain injury include a combination of
the:
Glasgow Coma Scale (GCS) score.
length of time a person is in a coma.
length of time a person has post-traumatic amnesia (PTA).
The Glasgow Coma Scale
This scoring system rates a person’s level of consciousness at a particular time.
The scores are used to record a person’s response in three areas:
eye opening.
verbal response.
motor response.
The scores for each area are added together to give the GCS score.
Eye opening Verbal Motor
Spontaneous 4 Oriented 5 Follows commands 6
To speech 3 Confused 4 Localises pain 5
To pain 2 Inappropriate words 3 Withdraws to pain 4
None 1 Non-specific sounds 2 Decorticate posture (bending) 3
None 1 Decerebrate posture
(straightening)
2
None 1
The initial GCS score after a head injury can indicate how severe the injury may be. A fall
in the score over a period of time is even more significant. The lowest score possible
is 3.
A GCS score of 8 or less is the definition of a coma.
Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 15
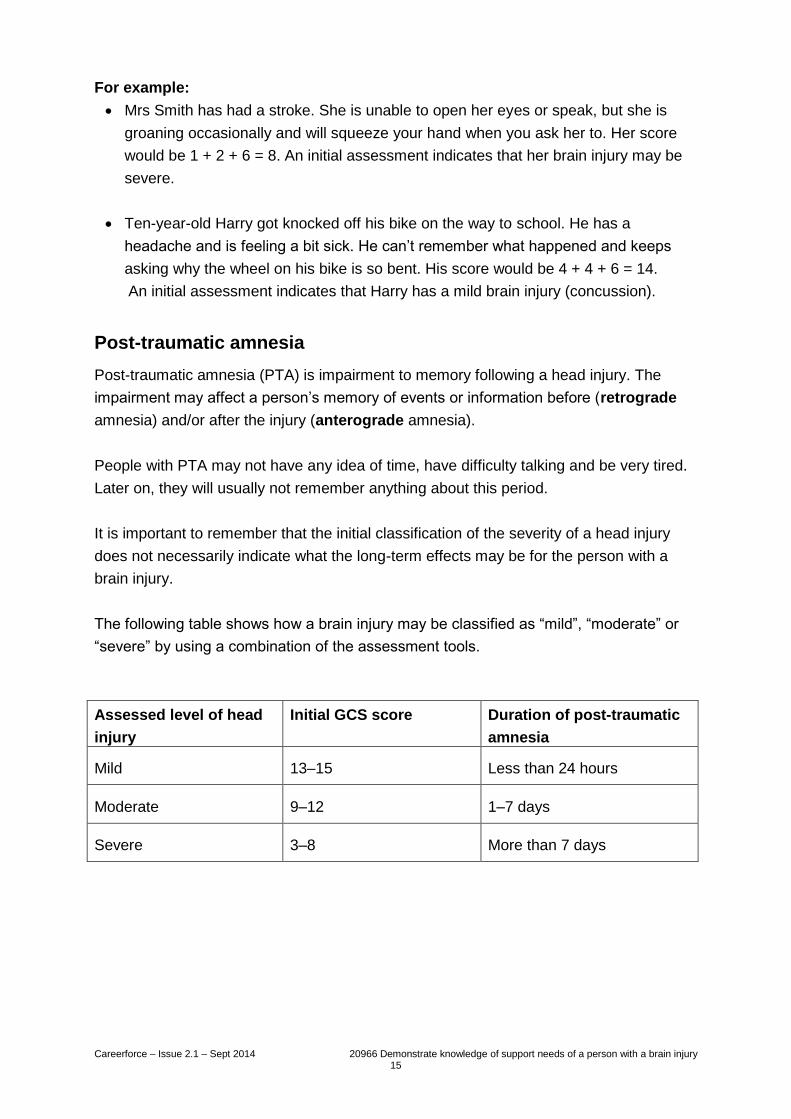
For example:
Mrs Smith has had a stroke. She is unable to open her eyes or speak, but she is
groaning occasionally and will squeeze your hand when you ask her to. Her score
would be 1 + 2 + 6 = 8. An initial assessment indicates that her brain injury may be
severe.
Ten-year-old Harry got knocked off his bike on the way to school. He has a
headache and is feeling a bit sick. He can’t remember what happened and keeps
asking why the wheel on his bike is so bent. His score would be 4 + 4 + 6 = 14.
An initial assessment indicates that Harry has a mild brain injury (concussion).
Post-traumatic amnesia
Post-traumatic amnesia (PTA) is impairment to memory following a head injury. The
impairment may affect a person’s memory of events or information before (retrograde
amnesia) and/or after the injury (anterograde amnesia).
People with PTA may not have any idea of time, have difficulty talking and be very tired.
Later on, they will usually not remember anything about this period.
It is important to remember that the initial classification of the severity of a head injury
does not necessarily indicate what the long-term effects may be for the person with a
brain injury.
The following table shows how a brain injury may be classified as “mild”, “moderate” or
“severe” by using a combination of the assessment tools.
Assessed level of head
injury
Initial GCS score Duration of post-traumatic
amnesia
Mild 13–15 Less than 24 hours
Moderate 9–12 1–7 days
Severe 3–8 More than 7 days
Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 16
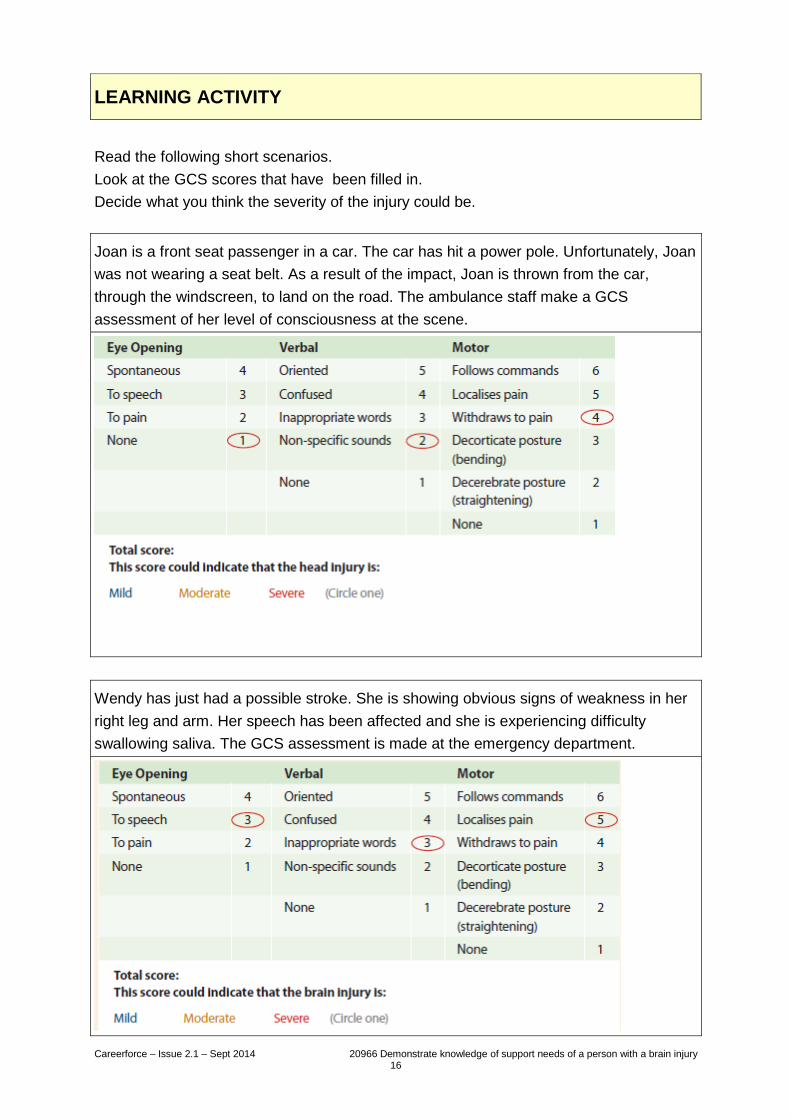
LEARNING ACTIVITY
Read the following short scenarios.
Look at the GCS scores that have been filled in.
Decide what you think the severity of the injury could be.
Joan is a front seat passenger in a car. The car has hit a power pole. Unfortunately, Joan
was not wearing a seat belt. As a result of the impact, Joan is thrown from the car,
through the windscreen, to land on the road. The ambulance staff make a GCS
assessment of her level of consciousness at the scene.
Wendy has just had a possible stroke. She is showing obvious signs of weakness in her
right leg and arm. Her speech has been affected and she is experiencing difficulty
swallowing saliva. The GCS assessment is made at the emergency department.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 17
Headaches are the
most common
physical complaint
people experience
after an injury to the
head or neck.
The effects of brain injury
Even a mild brain injury can be clinically significant due to the impact it may have on a
person’s ability to function. The part of the brain that has been injured, the severity of the
injury and the presence of other injuries will also affect the degree of impairment.
The unit standard talks of the neuropathy of the brain injury and possible sequelae. This
means the change in physical and/or mental condition following the brain injury.
People may be impaired in their ability to live independently, return to work or school, or
participate in social and recreational activities and relationships. People may need help
with basic daily activities such as bathing, dressing, eating and walking. These
impairments will also affect the injured person’s family/whānau.
A person’s functioning includes:
cognition.
behaviour.
emotion.
communication.
physical function.
The physical effects of a brain injury such as loss of movement, difficulty with speech,
headaches and seizures are often easily recognised and able to be understood.
The cognitive and emotional effects of brain injury are often more difficult to recognise
and/or understand and these can affect a wide range of cognitive functions and a
person’s behaviour patterns, including:
memory.
thinking and concentration.
insight.
responses and reactions.
planning and problem solving.
social skills.
flexibility.
initiative/motivation.
irritability and temper control.
impulsive behaviour.
self-centredness.
verbal aggression.
low mood.
anxiety.
dizziness, visual difficulties and light sensitivity.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 18
Changes in behaviour patterns are often a direct result of a brain injury and they can
have a significant effect on the person’s life and on the lives of others, such as family and
friends.
The nature of these behavioural changes and their effects and their impact means that it
can even be difficult at times for the person with the brain injury to recognise and
understand that these things are directly related to the brain injury.
Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 19
Fatigue
Fatigue is one of the most frequently reported symptoms after a brain injury. It can have
a major effect on a person’s ability to return to work or cope with other daily activities.
Fatigue can worsen other symptoms, such as headaches, cognitive difficulties and
behavioural problems. It can also contribute to emotional problems such as anxiety and
depression. Two types of fatigue are recognised:
1 Cognitive fatigue – when mental effort without physical exertion causes severe
tiredness and an inability to carry on. This is the most common type of fatigue
suffered after a brain injury.
2 Physical fatigue – when less than expected levels of physical exertion cause
severe tiredness and an inability to continue. This kind of fatigue often gets a lot
better as people get stronger and more active.
Fatigue can affect every single thing that a person does. Because fatigue can be mental
as well as physical, activities that were easy before the brain injury such as reading a
book, eating, walking and talking, or watching television, can cause tiredness or fatigue.
Fatigue associated with brain injury can appear suddenly and require a longer recovery
time than usual fatigue. Indicators of fatigue include:
feeling tired, lethargic or exhausted.
becoming mentally tired easily.
becoming easily irritated or frustrated with things that were previously easy to do.
becoming bored with activities that used to be interesting.
having difficulty getting organised and completing tasks.
starting a task but not being able to complete it.
missing out an important step in a task.
forgetting the topic of a conversation, or details that a person has just been told.
having problems concentrating.
loss of appetite.
slower movements and slower speech.
irritability or anxiety.
increasing forgetfulness.
poor vision.
poor coordination and/or poor balance.
Fatigue seems to be brought on most quickly by activities that require prolonged
concentration such as desk work and reading.
As people get fatigued, their body’s energy will continue to fall, and activities that are
difficult when a person is rested and refreshed become even more difficult.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 20
A ‘head injury’ may
include injuries such
as a broken jaw or
fractured skull. It does
not necessarily
involve an injury to
the brain.
Cognitive and emotional effects of brain injury
Forgetting people’s names, appointments, details you read in the newspaper, the topic of
a conversation, where you live and where you have put things can all have significant
effects on a person.
Having difficulty concentrating may mean that hobbies and interests that a person once
enjoyed are no longer so easy to engage in and this can create problems due to
boredom and frustration.
An inability to respond quickly may mean that things like answering questions,
performing a task or keeping up with a conversation are difficult.
Difficulties with problem solving, planning and organising may mean that a person with a
brain injury may not know where to start with a specific task or know what comes next in
a process such as making a cup of tea, cooking a meal, or getting dressed.
Inflexibility resulting from a brain injury may cause a person to get stuck with a certain
train of thought or become very repetitive. Changes in routine may be difficult to cope
with. Self-centredness can be a consequence of a brain injury and cause a person to be
demanding and appear inconsiderate or disinterested in others or their points of view.
Injury to the parts of the brain that help us make decisions and control our behaviour can
cause people to do things that are seen as inappropriate or embarrassing socially. It may
also be unsafe for them to be in a workshop or kitchen or to cross the road by
themselves. It may cause a person to talk too much or about inappropriate subjects.
People with a brain injury may have difficulty controlling their emotions. They might cry
too much or too often, or laugh at inappropriate times. This can be embarrassing for
them and for others. A common emotional consequence of this behaviour can be
depression and associated lack of motivation.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 21
LEARNING ACTIVITY
Choose a person you currently support and answer the following questions.
How did this person suffer a brain injury?
Was this a traumatic or non-traumatic injury?
Was this injury classified as mild, moderate or severe?
What are some of the effects this injury has had on the person?
What impact do these effects have on the life of the person?

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 22
Support needs of a person with a brain
injury
The kind of support that a person with a brain injury needs will vary from person to
person. The support immediately following a brain injury will be more focussed on the
immediate medical support the person requires. Ongoing support will be required for
rehabilitation.
The type and level of support will depend on the severity of the brain injury and the
effects that the brain injury has had on the person. Support may be required for physical
needs such as coping with dysphagia (difficulty swallowing) or reduced mobility. Support
may also be required for social needs like communicating with people and joining in
activities.
As a support worker, you will be involved in the care of a person with a brain injury by
being part of either a multidisciplinary team or an interdisciplinary team.
Multidisciplinary team
A multidisciplinary team is a group of health care workers who are members of different
disciplines, each providing specific services to the person who is being supported. The
multidisciplinary team approach utilises the totality of skills that people can offer from
their varying perspectives. This approach can either:
involve separate consultations with the person.
have members attending regular meetings in the absence of the person being
supported.
be a one-stop-shop, where each member of the multidisciplinary team carries out a
consultation with the person, as part of one appointment or meeting.

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 23
Interdisciplinary team
An interdisciplinary team is a team of health care workers/providers who work together
to:
meet the needs of the person who is being supported.
determine how care will be delivered.
explore ways in which the health of the person can be best supported.
The interdisciplinary team approach tends more towards integrating the separate
disciplines around a common understanding and holistic view of all aspects of the health
and wellbeing of the person who is being supported.
These teams will work and operate in different ways, in accordance with:
the workplace’s policies and procedures.
the health status of the person who is being supported.
the level of care and support needed.
in some cases, the intervention of the person with the brain injury.
Each team will be made up of different personnel who can include:
support workers.
family/whānau.
occupational therapists.
general practitioners.
social workers.
physiotherapists.
speech and language therapists.
a dietitian.
a registered nurse.
a clinical psychologist.
the person with the brain injury.
The composition of the team will vary in accordance with the needs of the person. Each
team member will have knowledge and skills in particular areas. By working as a team,
they bring their combined knowledge and skills to the responsibilities, accountability and
level of care that they are providing.
The role that support workers take in contributing to the rehabilitation process will be
determined by:
their job specifications.
the role and responsibilities they have within the team.
how they feed back to the team the current needs of the person and rate of
progress in achieving key goals.
Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 24
There is no set model used in the rehabilitation process, as each rehabilitation plan is
individualised to meet the needs of the person being supported. However, each
rehabilitation plan will indicate the membership of the team, and outline each person’s
contributions, roles and responsibilities.
For example:
Jane is a physiotherapist. Her role in the team is to assess and treat problems to do with
movement and balance. Her responsibilities include:
explaining to the person and their family/whānau what is involved in the
rehabilitation process.
finding out what the person and their
family want to achieve with the
programme so that their goals can
be included in the plan.
re-evaluating the person’s exercises
over time so that the plan remains
relevant and up to date.
showing others how they can
support and encourage the person.
Whatever model is used, the team’s objective is to work collectively to address the
person’s holistic needs, promote wellness and independence (when and where
possible), and meet the goals as set out in the rehabilitation plan.
For example, Wendy has had a stroke. She has obvious signs of weakness in her right
leg and arm. Her speech has been affected and she is experiencing difficulty swallowing
saliva. Wendy is very fatigued after just a few activities that require her to concentrate.
Wendy requires support for coping with her difficulty swallowing and reduced mobility.
She needs physical support in cleaning her house and doing her laundry and shopping.
Wendy needs support with her social needs, like communicating with people and joining
in activities.
A multidisciplinary team in the community has resources to help. A speech therapist and
a dietitian can help Wendy with her communication and her difficulties with swallowing.
A physiotherapist can help Wendy with exercises and support devices for the weakness
in her right leg and arm. An occupational therapist can help Wendy join in activities
organised by local NGOs or church groups. A social worker can organise support for
Wendy with cleaning her house and doing her laundry and shopping.
Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 25
LEARNING ACTIVITY
Think of a person you are currently supporting and answer the following questions about
their support.
In what physical areas does this person require support?
In what social areas does this person require support?
Who are the members of the support team and what are their roles?
What is your role in the support team?
What resources are available in the community to support this person?

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 26
Rewind to pages 11, 12, 14, 19 and 24.
What is the difference between a traumatic brain injury and a non-traumatic brain injury?
Define concussion. What kind of a brain injury is it? How common? How severe?
What are the two most common physical complaints people may have after a
head injury?
1
2
What are the three tools used to classify the severity of a brain injury?
1
2
3
What is the primary objective of the support given to a person with a brain injury?

Careerforce – Issue 2.1 – Sept 2014 20966 Demonstrate knowledge of support needs of a person with a brain injury 27
Completion and assessment
Congratulations!
You have come to the end of the workbook. Please check over all the activities in this
workbook to make sure you have completed them.
Your assessment is next
You need to complete the trainee assessment successfully to be credited with this unit
standard.
Your assessor will sign you off once you have completed the assessment tasks
satisfactorily.
Acknowledgements
Careerforce thanks the people who have contributed to this workbook by:
researching and validating content.
providing advice and expertise.
testing the activities.
sharing personal experiences.
appearing in photographs.
The images contained in these workbooks are visual illustrations only and are not representative of
actual events or personal circumstances.
Creative Commons
This work is licenced under a Creative Commons Attribution-NonCommercial Licence. You are free to
copy, distribute and transmit the work and to adapt the work. You must attribute Careerforce as the
author. You may not use this work for commercial purposes. For more information contact Careerforce
www.careerforce.org.nz

Careerforce – Issue 2.1 – Sep 2014