withdrawal of antihypertensive therapy in the elderly
TRANSCRIPT
DRUG THERAPY Drugs & Aging 6 (6): 436<144.1995 117D-229XJ95/0006-ll436/S04.50/0
© Adis International Um~ed. All nghts reserved.
Withdrawal of Antihypertensive Therapy in the Elderly The Issues
Martin D. Fotherby Division of Medicine for the Elderly, Department of Medicine, University of Leicester, The Glenfield Hospital, Leicester, England
Contents Summary .................... . · 436 1. Studies of Antihypertensive Drug Withdrawal · 437
1. 1 Studies in Elderly Patients ........ . · 437 .439 .439
2. Factors Influencing Return to Hypertension . . 3. Antihypertensive Treatment Withdrawal in the Elderly 4. Mechanisms Involved in Maintenance of Normotension
4.1 Regression of Vascular Changes . . . . . . . . . . . 4.2 Baroreceptor Reset. . . . . . . . . . . . . . . . . . .
439 440 440 440 441 442 442 442 442
5. Which Older Patients Should be Considered for Treatment Withdrawal? 6. How Should Treatment be Withdrawn? . . . . . . . . . . . . 7. Advantages and Disadvantages of Treatment Withdrawal
7.1 Advantages .. 7.2 Disadvantages
8. Conclusions . . . . .
Summary Studies of antihypertensive drug withdrawal suggest that at least 20% of selected older patients with hypertension can remain normotensive without drug treatment for periods of up to 5 years. Success of drug withdrawal is greater in those patients controlled on low dose monotherapy who have low on-treatment blood pressure (BP), are not overweight and who have no ECG evidence of left ventricular hypertrophy. Compliance with lifestyle advice may increase the chance of successful drug withdrawal. Unfortunately, many older hypertensive patients have poorly controlled BPdespite treatment with antihypertensive drugs, and are overweight. These factors limit opportunities for drug withdrawal although they may not be so much of a problem in the very elderly. Patients who could be considered for a trial of antihypertensive drug withdrawal are those unhappy with such therapy who also: (a) have well controlled BPon monotherapy with no significant target organ damage, (b) have 'white-coat' hypertension, or (c) are very elderly (>80 years). The withdrawal of antihypertensive drugs can improve drug-induced metabolic abnormalities and symptoms, and appears safe providing there is a gradual reduction in drug dosages and close follow-up to detect a return to hypertension.
Withdrawal of Antihypertensive Therapy in the Elderly
Elevated blood pressure (BP) continues to be associated with a greater risk of cardiovascular disease in older people,Dl although the strength of this association in the very elderly is less clear.!2,3l Accordingly, studies have shown that pharmacological treatment of hypertension is of benefit in reducing these risks in people up to the age of 80 years and perhaps beyond.[4.6l Achieving and maintaining 'normotension' in individuals diagnosed as hypertensive is therefore desirable but, as the prevalence of hypertension has been estimated at >40% in people aged 60 to 79 years, the potential number of older individuals eligible for treatment is enormous.!?l Essential hypertension is considered incurable but treatable. Therefore, the concept of lifelong antihypertensive drug therapy has been established and widely accepted.
So why consider antihypertensive treatment withdrawal? Clearly, it is important to maintain normotension and hence reduce the risk of cardiovascular events. If normotension is maintained after drug withdrawal, the cost, adverse effects and any detrimental effects on quality of life incurred by drug treatment will be removed. This may be of particular relevance in patients who have continued on treatment well into their 80s, an age at which the benefits of treatment are less clearly established.l8l Also, drug withdrawal may shift the focus of concern in patients with hypertension from purely drug-based therapy to a broader consideration of reduction in overall cardiovascular risk. National and international guidelines on the management of hypertension now recognise that, in patients with well-controlled BP, a reduction in the dose and number of antihypertensive drugs, or cessation of drug therapy, is indicated.[9.11l
1. Studies of Antihypertensive Drug Withdrawal
Reduction or complete withdrawal of antihypertensive drug therapy has been considered since soon after the widespread introduction of such therapy. The first report of a drug withdrawal study was in 1956 by Perry and Schroeder.[l2l In a later study,D3l these same authors observed prolonged
© Adls International Limited. All rights reserved.
437
remission of hypertension in 5% of 316 patients after discontinuation of drug treatment. In 1962, Page and Dustan[l4l withdrew all treatment from 27 patients with previously severe hypertension; in 18 the BP increased, requiring reinstitution of treatment, but in the other 9 (33%) BP levels remained satisfactory without treatment for between 6 months and 5 years. Since this time, there have been many such studies, most uncontrolled and carried out in middle-aged patients. Comparison between studies and interpreting their relevance to clinical practice can be difficult as the degree of patient selection and BP criteria for withdrawal and reinstitution of therapy vary.
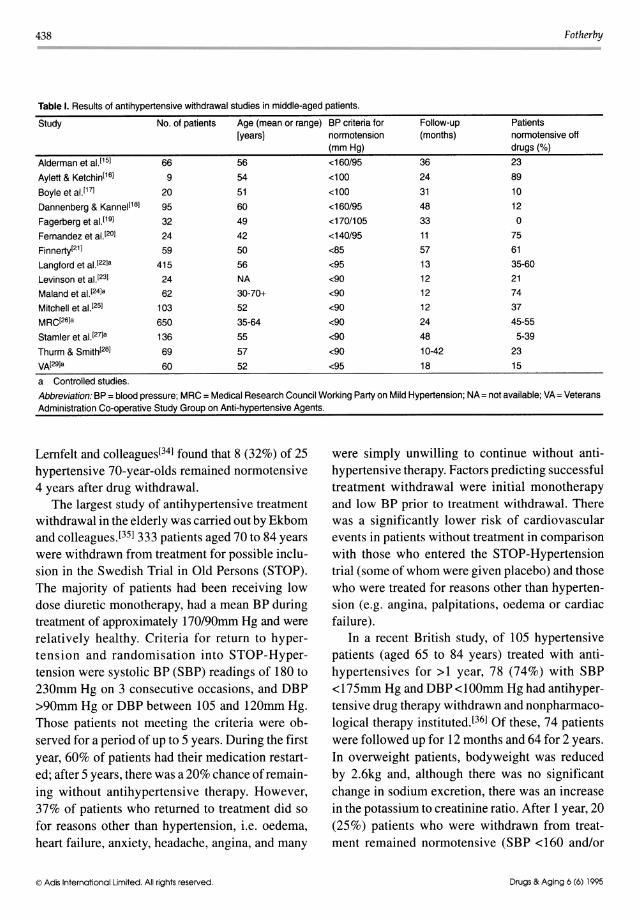
Table I summarises some of the studies carried out in middle-aged people which, on average, suggest that one-third of selected patients can be successfully withdrawn from treatment for periods of 1 to 4 years. Substitution of nonpharmacological therapy, such as body weight loss and sodium restriction, may more than double the probability of successful drug withdrawaU22,2?l
1,1 Studies in Elderly Patients
There have been relatively few studies of antihypertensive treatment withdrawal in the elderly, and only one where nonpharmacological methods have been substituted for drug therapy over a prolonged period, despite increasing evidence of the efficacy of such methods in this age group.[30.32l Early studies used criteria for defining hypertension at BP levels greater than those accepted today, making interpretation of results for today's practice unclear. Hansen and colleagues[33l withdrew antihypertensive therapy in 169 patients aged over 50 years; 51 (30%) rapidly became hypertensive. Of the remaining 118, 105 were over 60 years of age (mean age 75 years) and had diastolic BP (DBP) <110mm Hg three weeks after withdrawal. After 1 year, 43 (41 %) of these patients had DBP <llOmm Hg and remained untreated, while 15% developed hypertension (DBP > IIOmm Hg) and were treated. In 32% of patients, although DBP did not exceed 100mm Hg, treatment was restarted because of angina or congestive cardiac failure.
Drugs & Aging 6 (6) 1995
438 Fotherby
Table I. Results of antihypertensive withdrawal studies in middle-aged patients.
Study No. of patients Age (mean or range) BP criteria for Follow-up Patients [years] normotension (months) normotensive off
(mmHg) drugs (%) Alderman et al.[15] 66 56 <160/95 36 23 Aylett & Ketchin[16] 9 54 <100 24 89 Boyle et al. [17] 20 51 <100 31 10 Dannenberg & Kannel[18] 95 60 <160/95 48 12 Fagerberg et al. [19] 32 49 <170/105 33 0 Fernandez et al. [20] 24 42 <140/95 11 75 Finnerty[21] 59 50 <85 57 61 Langford et al. [22]a 415 56 <95 13 35-60 Levinson et al. [23] 24 NA <90 12 21 Maland et al. [24]a 62 30-70+ <90 12 74 Mitchell et al. [25] 103 52 <90 12 37 MRc[26]a 650 35-64 <90 24 45-55 Stamler et al. [27]a 136 55 <90 48 5-39 Thurm & Smith[28] 69 57 <90 10-42 23 VA[29]a 60 52 <95 18 15 a Controlled studies.
Abbreviation: BP = blood pressure; MRC = Medical Research Council Working Party on Mild Hypertension; NA= not avai[able; VA= Veterans Administration Co-operative Study Group on Anti-hypertensive Agents.
Lernfelt and colleagues[341 found that 8 (32%) of 25 hypertensive 70-year-olds remained normotensive 4 years after drug withdrawal.
The largest study of antihypertensive treatment withdrawal in the elderly was carried out by Ekbom and colleagues.l351 333 patients aged 70 to 84 years were withdrawn from treatment for possible inclusion in the Swedish Trial in Old Persons (STOP). The majority of patients had been receiving low dose diuretic monotherapy, had a mean BP during treatment of approximately l70/90mm Hg and were relatively healthy. Criteria for return to hypertension and randomisation into STOP-Hypertension were systolic BP (SBP) readings of 180 to 230mm Hg on 3 consecutive occasions, and DBP >90mm Hg or DBP between 105 and l20mm Hg. Those patients not meeting the criteria were observed for a period of up to 5 years. During the first year, 60% of patients had their medication restarted; after 5 years, there was a 20% chance of remaining without antihypertensive therapy. However, 37% of patients who returned to treatment did so for reasons other than hypertension, i.e. oedema, heart failure, anxiety, headache, angina, and many
© Adis International Limited. All rights reserved.
were simply unwilling to continue without antihypertensive therapy. Factors predicting successful treatment withdrawal were initial monotherapy and low BP prior to treatment withdrawal. There was a significantly lower risk of cardiovascular events in patients without treatment in comparison with those who entered the STOP-Hypertension trial (some of whom were given placebo) and those who were treated for reasons other than hypertension (e.g. angina, palpitations, oedema or cardiac failure).
In a recent British study, of 105 hypertensive patients (aged 65 to 84 years) treated with antihypertensives for >1 year, 78 (74%) with SBP <175mm Hg and DBP <100mm Hg had antihypertensive drug therapy withdrawn and nonpharmacological therapy instituted.[361 Of these, 74 patients were followed up for 12 months and 64 for 2 years. In overweight patients, body weight was reduced by 2.6kg and, although there was no significant change in sodium excretion, there was an increase in the potassium to creatinine ratio. After 1 year, 20 (25%) patients who were withdrawn from treatment remained normotensive (SBP <160 and/or
Drugs & Aging 6 (6) 1995

Withdrawal of Antihypertensive Therapy in the Elderly
DBP <90mm Hg) whilst continuing with nonpharmacological therapy. Of the 64 patients followed up for 2 years, 13 (20%) who were normotensive at 18 months remained so at 2 years. The majority (75%) of patients restarting therapy did so within the first 3 months. There was no significant difference in baseline characteristics between those restarting therapy and those remaining off therapy at 1 year with respect to age; sex, number of antihypertensive agents taken, history of vascular disease, treatment duration, left ventricular mass index or mean DBP. However, a higher ontreatment SBP, a higher body mass index (BMI) and a higher ECG (sVl + rV6) voltage was associated with return to hypertension. Three patients restarted diuretic treatment for reasons other than hypertension: 2 had diuretic-dependent ankle oedema, and 1 had mild left ventricular failure.
2. Factors Influencing Return to Hypertension
When considering results from studies conducted in middle-aged and older patients, certain conclusions emerge.
Neither age nor gender has a consistent effect on the success of treatment withdrawal. This suggests that older individuals with a less compliant vascular system are as likely to remain normotensive off treatment as younger patients.
Many studies have reported that lower pretreatment BP is associated with a longer period of normotension,£22,24,27,291 However, in Ekbom's study of older people, pretreatment BP was not associated with maintenance of normotension,l351
In younger and older people, studies have found that lower on-treatment BP levels were associated with the maintenance of normotension.[23,35,361
Most studies require antihypertensive therapy to have been regularly taken for> 1 year prior to withdrawal. No consistent effect of the duration of drug treatment prior to withdrawal on the maintenance of normotension has been reported in young or older patients. However, monotherapy and low doses may be associated with a greater chance of successful treatment withdrawal.[351
© Adls International Umited. All rights reserved.
439
Fotherby and colleagues[361 found that being overweight at the time of drug withdrawal was an independent predictor of return to hypertension in older patients. This association had been previously reported in younger patients,£271
Fagerberg and colleagues[191 found larger prewithdrawal left ventricular mass (LVM) in patients who rapidly returned to hypertension compared with those whose BP increased more slowly. However, in older patients, although echocardiographically determined LVM was not predictive of return to hypertension, a lower ECG (sVl + rV6) voltage was associated with maintenance of normotension.[361 A similar finding was reported in younger patients by Imataka and colleagues, [371 but not by Levinson and colleagues,l231
In summary, it appears that older patients are as likely as younger patients to be successfully withdrawn from treatment. Those patients receiving low dose monotherapy with low on-treatment BP, ideal bodyweight and no evidence ofleft ventricular hypertrophy on ECG will have the greatest chance of remaining normotensive off treatment.
3. Antihypertensive Treatment Withdrawal in the Elderly
In an unselected group of 130 patients aged 65 to 92 years receiving antihypertensive treatment for more than 1 year, 46% of those aged 65 to 79 years had poorly controlled hypertension (SBP >160mm Hg) and almost one-half were overweight. [381 The older patients (>80 years) tended to have better controlled blood pressure, lower BMI and lower ECG (sVI + rV6) voltage, suggesting a greater potential for successful treatment withdrawal in this group.
4. Mechanisms Involved in Maintenance of Normotension
It is likely that some persons diagnosed as hypertensive on the basis of only 2 or 3 BP readings (the practice of up to 70% of doctors[391) do not have sustained hypertension. High BP levels tend to fall on successive occasions,[401 particularly elevated SBP levels in older people,l411 Conse-
Drugs & Aging 6 (6) 1995

440
quently, with time, BP readings may fall into the normotensive range whether or not antihypertensive therapy is administered. This observation has been made in the placebo arm of various intervention studies.l42)
4,1 Regression of Vascular Changes
Hypertension is implicated in vascular wall thickening and left ventricular hypertrophy, and these in tum may contribute to the maintenance of hypertension.l43) A period of normotension induced by drugs can lead to a regression of these changes, at least partially. [44) Following drug withdrawal, it is hypothesised that normotension will persist because of normalisation of the structural changes. However, the initial stimulus to hypertension may persist, leading to elevated BP and the recurrence of vascular and ventricular hypertrophy. Indeed, it has been reported that lower LVM is correlated with a longer period of normotension following treatment withdrawal; however, all patients eventually returned to hypertension.l 19)
4,2 Baroreceptor Reset
It has been suggested that after a period of normotension the carotid baroreceptor could be reset at a lower leveI.l28) However, there is little experimental evidence of this.l45)
5. Which Older Patients Should be Considered for Treatment Withdrawal?
There are no detailed published guidelines discussing which patient groups should be considered for a trial of antihypertensive drug withdrawal. However, some reports suggest that it may be possible to attempt a careful progressive reduction in dose and number of drugs used in patients with BP which is well controlled on prolonged treatment, with cautions against complete cessation in patients correctly diagnosed as hypertensive.[IO,II) In a discussion involving representatives of national hypertension guidelines from the USA, Canada, United Kingdom, New Zealand and the World Health OrganisationlInternational Society of Hyper-
© Adis Intematlonal Limited. All rights reserved.
Fotherby
tension (WHO/lSH), all agreed that antihypertensive therapy could be decreased or withdrawn in selected patients because (a) there may be uncertainty about the initial diagnosis, (b) the disease process may have changed, e.g. because of life sty Ie changes, and (c) unnecessary therapy should be eliminated.l46) The British Hypertension Society guidelines suggest that treatment may be withdrawn in some patients with well-controlled BP and no evidence of target organ damage.£9) The US Joint National Committee V recommendations state that in general complete cessation of antihypertensive drug therapy is not indicated, but if BP has been controlled for one year on at least 4 visits then it may be possible to reduce drug therapy, particularly if lifestyle treatment is continued'£") WHO/ISH guidelines suggest that after prolonged BP control it may be possible to attempt a reduction in dosage or number of drugs used, especially in patients complying with non-drug therapy.£IO)
More specifically, in the elderly, groups which could be considered for antihypertensive drug therapy reduction and withdrawal, followed by substitution of nonpharmacological methods, are as follows. • Well-controlled hypertensive patients: individ
uals who have been receiving monotherapy for more than 1 year with well controlled BP levels (e.g. <150/90mm Hg), who have no evidence of significant target organ damage, and who are unhappy taking tablets and request a trial of treatment withdrawal.
• ?Never truly hypertensive: patients with wellcontrolled BP levels (e.g. <150/90mm Hg) in whom treatment was started after only 2 or 3 BP readings and who may have been wrongly diagnosed as hypertensive. Such patients are less likely to have evidence of hypertensive target organ damage compared with truly hypertensive patients.
• Patients with 'white coat' hypertension: although high clinic BP levels tend to fallon repeated measurements, levels taken repeatedly in the clinic, especially by a doctor, may be signif-
Drugs & Aging 6 (6) 1995

Withdrawal of Antihypertensive Therapy in the Elderly
icantly higher than levels taken at home by the patient or an automatic BP monitor.l41,47] This 'white coat' hypertension may affect 20% of younger patients and an even greater percentage of the elderly.l48-50] The condition may not be benign but probably has a lower cardiovascular risk than sustained hypertension.[5I,52] The condition can be suspected in people with elevated clinic BPs, but no risk factors for hypertension nor any evidence of target organ damage or left ventricular hypertrophy. In such patients, particularly those who complain of hypotensive symptoms on treatment or who are even mildly intolerant of drug therapy, a trial of treatment withdrawal is appropriate.
• Patients with orthostatic hypertension: in patients with an SBP fall ~20mm Hg on standing
.. from a lying position, the prevalence of orthostatic hypotension has been reduced by withdrawal of antihypertensive drugs and institution of nonpharmacological methods.[53] For patients who have symptomatic orthostatic hypotension, a trial of antihypertensive drug reduction or withdrawal would be appropriate.
• Removal of stimulus for hypertension: despite being correctly diagnosed as having sustained hypertension, if lifestyle changes (e.g. reduction in weight or alcohol intake) have been initiated, antihypertensive treatment may no longer be required provided the lifestyle changes are continued.
• The very elderly: in people over 80 years of age, the benefits of antihypertensive treatment are unclear. [8] Higher BP levels and evidence of cardiovascular disease may be factors favouring treatment. For patients entering this age range and receiving antihypertensive drugs who have conditions that can be symptomatically helped by such treatment (e.g. angina and congestive cardiac failure), treatment should be continued. In general, if patients are happy to remain on treatment and experience no adverse effects, it is reasonable to continue. For those without overt cardiovascular disease who do not want to take medications daily, there may be less need for
© Adls International limited. All rights reserved.
441
continuing treatment even with BP levels up to 160/90mm Hg. A trial of treatment withdrawal can be offered; if quality of life deteriorates or, for example, dyspnoea or oedema occur or BP rises to very high levels (>1801l05mm Hg), treatment can be reinstituted.
6. How Should Treatment be Withdrawn?
The first consideration is to establish that BP is well controlled with treatment by taking multiple measurements over a prolonged period; standing measurements should be taken into consideration if they are significantly lower than sitting or supine measurements.
Ideally, patients should have been advised regarding nonpharmacological methods of BP lowering on first diagnosis, although this is often not the caseP9] Prior to treatment withdrawal, where appropriate, patients should be given individualised advice on reducing sodium intake, reducing alcohol intake, participating in more aerobic exercise, increasing dietary potassium intake and losing weight.
The patient should be involved in the decision to withdraw treatment and should be aware that it is a trial, i.e. treatment may need to be restarted and hence the need for continued follow-up. There are 2 main concerns: the possible rebound effect on stopping treatment (an infrequent problem) and, more commonly, return of elevated BP.
If possible, drug therapy should be withdrawn in a stepwise manner. Although the drug is rarely used nowadays, sudden withdrawal of clonidine can lead to rebound hypertension and a hypertensive crisis.l54] It is also suggested that ~-blockers should be reduced in a gradual manner over 1 to 3 weeks as sudden cessation may exacerbate preexisting angina or provoke myocardial infarction in patients with ischaemic heart disease.[55,56] However, this is rarely a problem in hypertensive patients,[57] and if patients are intolerant of ~-blockers, e.g. they develop dyspnoea, these drugs should be stopped immediately. The withdrawal of diuretics may lead to rebound oedema or may unmask
Drugs & Aging 6 (6) 1995
442
mild congestive cardiac failure.l581 In older patients, reducing the dose or taking diuretics on alternate days, then every third or fourth day over several weeks may reduce the chance of oedema developing.
Studies in older patients have shown that between two-thirds and three-quarters of those who return to hypertension do so within the first 3 to 6 months. Therefore, during the first 3 months after withdrawal of antihypertensive drugs, BP should be measured every 2 to 3 weeks and then every 4 to 8 weeks, depending on the BP level, for the first year. If BP remains in the normotensive range after this, measurements can be taken every 3 to 6 months. However, if BP elevations do occur, more frequent measurements will need to be taken to confirm sustained hypertension.
7. Advantages and Disadvantages of Treatment Withdrawal
7.1 Advantages
Although the clinical significance of metabolic abnormalities secondary to antihypertensive agents is unclear, most return towards pretreatment levels on drug withdrawal. Rises in mean serum potassium levels of 0.6 mmollL,[27] decreases in the prevalence of hypokalaemia of approximately 25%, and falls in serum urate level of 11 to 40% have been found on withdrawal of mainly diuretic-based treatment. [56.2 1] Other adverse effects attributed to treatment should improve. Cooper and colleagues[591 found that most symptoms, except headache, significantly improved within 2 weeks following drug withdrawal.
There may be some financial savings from reduced drug use, but these will be limited because only a minority of treated hypertensive patients will be suitable for drug withdrawal, and savings may be offset by the need for continued and initially closer follow-up.
7.2 Disadvantages
As noted above, withdrawal of certain drugs may unmask or exacerbate underlying conditions
© Adis International limited. All rights reserved.
Fotherby
such as angina, oedema or cardiac failureP9,581 However, in terms of total mortality, drug withdrawal in selected elderly patients has been found to be 'safe' p 51 Loss to follow-up is a potential problem requiring effective call-back procedures. A cardiovascular event may occur following treatment withdrawal despite maintenance of normotension, and it should be explained to patients at the outset that such events can occur on or off treatment. Documentation of BP readings is essential.
8. Conclusions
Some older treated hypertensive patients with well controlled hypertension and no significant cardiovascular disease can be considered for a trial of drug withdrawal in a gradual, stepwise manner. This may be of particular relevance to individuals over 80 years of age where the risks and benefits of treatment are less clear. Relevant lifestyle advice should be given prior to drug withdrawal. Continued and close follow-up is necessary to monitor BP levels and adherence to the lifestyle advice.
References I. Potter JF, Fotherby MD. Hypertension in tbe elderly. In: Martin
A, Camm AJ, editors. Geriatric cardiology, principles and practice. Chichester: John Wiley & Sons, 1994: 301-31
2. Langer RD, Ganiats TG, Barrett-Connor E. Paradoxical survival with higher blood pressures in older men. BMJ 1989; 298: 1356-7
3. Mattila K, Haavisto M, Rajala S, et al. Blood pressure and five year survival in tbe very old. BMJ 1988; 296: 887-9
4. SHEP Co-operative Research Group. Prevention of stroke by anti-hypertensive drug treatment in older persons witb isolated systolic hypertension. JAMA 1981; 265: 255-264
5. DahlofB, Lindholm MH. Hansson L, et al. Morbidity and mortality in tbe Swedish trial in old patients with hypertension (STOP-Hypertension). Lancet 1991; 338: 1281-5
6. Medical Research Council Working Party. MRC trial of treatment of hypertension in older adults: principal results. BMJ 1992; 304: 405-12
7. Miall WE, Chinn S. Screening for hypertension; some epidemiological observations. BMJ 1974; 2: 595-7
8. Bulpitt C, Fletcher A, Amery A, et al. The hypertension in the very elderly trial (HYVET). J Hum Hypertens 1994; 8: 631-2
9. Sever P, Beevers G, Bulpitt C, et al. Management guidelines in essential hypertension: report of tbe second working party of tbe British Hypertension Society. BMJ 1993; 306: 983-7
10. The Guideline Sub-Committee of tbe WHO-ISH Mild Hypertension Liaison Committee. 1993 Guidelines for tbe Management of Mild Hypertension. Memorandum from a World Health OrganisationlIntemational Society of Hypertension Meeting. J Hypertens 1993; 22: 392-403
Drugs & Aging 6 (6) 1995

Withdrawal of Antihypertensive Therapy in the Elderly
II. Joint National Committee on detection, evaluation and treatment of high blood pressure. The fifth report of Joint National Committee on detection, evaluation and treatment of high blood pressure (JNC V). Arch Intern Med 1993; 153: 154-83
12. Perry HM, Schroeder AJ. Studies on the control of hypertension. VI. Some evidence for reversal of the process during hexamethonium and hydralazine therapy. Circulation 1956; 13: 528-31
13. Perry HM, Schroeder AJ, Catanzaro FJ, et al. Studies on the control of hypertension. B. Mortality, morbidity and remissions during twelve years of intensive therapy. Circulation 1966; 33: 958-72
14. Page IH, Dustan HP. The systems of normal blood pressure after discontinuing treatment in hypertensive patients. Circulation 1962;25:433-6
15. Alderman MH, Davis TK, Gerber LM, et al. Anti-hypertensive drug withdrawal in a general population. Arch Intern Med 1986; 146: 1309-11
16. Aylett M, Ketchin S. Stopping treatment in patients with hypertension. BMJ 1991; 303: 345-6
17. Boyle RM, Price ML, Camilton r.1. Thiazide withdrawal in hypertension. J R Coli Physicians Lond 1979; 13: 172-3
18. Dannenberg AL, Kannel WB. Remission of hypertension: the natural history of blood pressure treatment in the Framingham study. JAMA 1987; 257: 1477-3
19. Fagerberg B, Wikstrand J, Berglund G, et al. Withdrawal of anti-hypertensive drug treatment: time course for redevelopment of hypertension and effects upon left ventricular mass. J Hypertens 1992; 10: 587-93
20. Fernandez PG, Galway AB, Kim BK. Prolonged normotension following cessation of therapy in uncomplicated essential hypertension. Clin Invest Med 1982; 5: 31-7
21. Finnerty FA. Stepdown treatment of mild systemic hypertension. Am J Cardiol 1984; 53: 1304-7
22. Langford HG, Blaufox D, Oberman A, et al. Dietary therapy slows the return of hypertension after stopping prolonged medication. JAMA 1985; 235: 657- 64
23. Levinson PD, Khatri 1M, Freis ED. The systems of normal BP after withdrawal of drug treatment in mild hypertension. Arch Intern Med 1982; 142: 2265-8
24. Maland LJ, Lutz LJ, Castle CH. The effects of withdrawing diuretic therapy on blood pressure in mild hypertension. J Hypertens 1983; 5: 539-44
25. Mitchell A, Haines B, Adsett A, et al. The likelihood of remaining normotensive following anti-hypertensive drug withdrawal. J Gen Intern Med 1989; 4: 221-5
26. Medical Research Council Working Party on Mild Hypertension. Course of blood pressure in mild hypertensives after withdrawal of long term anti-hypertensive treatment. BMJ 1986; 293: 988-92
27. Stamler R, Stamler J, Grimm R, et al. Nutritional therapy for high blood pressure: final report of a four year randomised control trial - the hypertension control programme. JAMA 1987; 257: 1484-91
28. Thurm RH, Smith WM. On resetting of barostats in hypertensive patients. JAMA 1967; 201: 301-4
29. Veterans Administration Co-operative Study Group on Antihypertensive Agents. Return of elevated blood pressure after withdrawal of anti-hypertensive drugs. Circulation 1975; 51: 1107-13
30. Hagberg JM, Motan AS], Martin WH, et al. Effects of exercise training in 60 to 69-year-old persons with essential hypertension. Am] Cardiol 1989; 64: 348-53
© Adis Intemational Umited. All rights reserved.
443
31. Fotherby MD, Potter JE Effects of moderate sodium restriction on clinic and twenty-four hour ambulatory blood pressure in elderly hypertensive subjects. J Hypertens 1993; 11: 657-63
32. Fotherby MD, Potter JE Potassium supplementation reduces clinic and ambulatory blood pressure in elderly hypertensive patients. J Hypertens 1992; 10: 1403-8
33. Hansen AG, Jenson H, Laugesen LP, et al. Withdrawal of antihypertensive drugs in the elderly. Acta Med Scand 1983; 676 Suppl.l: 178-85
34. Lernfelt B, Landahl S, Svanvorg A, et al. Overtreatment of hypertension in the elderly? J Hypertens 1990; 8: 483-90
35. Ekbom T, Lindholm LH, Oden A, et al. A five year prospective, observational study of the withdrawal of anti-hypertensive treatment in elderly people. J Intern Med 1994; 345: 581-8
36. Fotherby MD, Potter JE Possibilities for anti-hypertensive drug therapy withdrawal in the elderly. J Hum Hypertens 1994; 8: 857-63
37. Imataka K, Nakaoka H, Amano M, et al. The effects of monotherapy and withdrawal of anti-hypertensive drugs in the treatment of hypertension. Jpn Heart J 1988; 29: 823-9
38. Fotherby MD, Potter JE Possibilities for drug withdrawal and non-pharmacological therapy in the elderly. Age Ageing 1994; 23 Suppl. I: 18
39. Fotherby MD, Harper GD, Potter JE General practitioners management of hypertension in elderly patients. BMJ 1992; 305: 750-2
40. Watson RDS, Lumb R, Young MA, et al. Variation in cuff blood pressure in untreated outpatients with mild hypertension: implications for initiating anti-hypertensive treatment. J Hypertens 1987; 5: 207-11
41. Fotherby MD, Potter JE Variation of within visit blood pressure readings at a single visit in the elderly and their relationship to ambulatory measurements. J Hum Hypertens 1994; 8: 107-11
42. A Report by the Management Committee of the Australian Therapeutic Trial in Mild Hypertension. Untreated mild hypertension. Lancet 1982; II: 185-91
43. Folkow B. The structural facts in primary hypertension: its relevance for the future principles of treatment. J Hypertens 1987; 5 Suppl. 5: 5611-3
44. DahlofB, Hanson L. The influence of anti-hypertensive therapy on the structural arterial changes in essential hypertension: different effects of hydrochlorothiazide. J Gen Intern Med 1993; 234: 271-9
45. Carretta R, Fabris B, Balini G, et al. Baroreflex function after therapy withdrawal in patients with essential hypertension. Clin Sci 1983; 64: 259-63
46. Alderman MH, Cushman WC, Hill MN, et al. International round table discussion of national guidelines for the detection, evaluation and treatment of hypertension. Am ] Hypertens 1993; 6: 974-81
47. Mancia G, Parati G, Pomidossi G, et al. Alerting reaction and rising blood pressure during measurement by physician and nurse. Hypertension 1987; 9: 209-15
48. Krakoff OR, Eison H, Phillips RH, et al. The effect of ambulatory blood pressure monitoring on the diagnosis and cost of treatment for mild hypertension. Am Heart J 1988; 116: 1152-4
49. Lerman CE, Brodie OS, Hui T, et al. The white coat hypertension response. Prevalence and predictors. J Gen Intern Med 1989; 4: 225-31
50. Ruddy MC, Bialy GB, Maika ES, et al. The relationship of plasmarine activity to clinic and ambulatory blood pressure
Drugs & Aging 6 (6) 1995

444
in elderly people with isolated systolic hypertension. J Hypertens 1988; 6 Suppl. 4: S412-5
51. Kuwajima I, Suzuki Y, Fujisawa A, et al. Is white coat hypertension innocent? Structure and function of the heart in the elderly. Hypertension 1993; 22: 826-31
52. Sokolow M, Perloff 0, Cowan R. Contribution of ambulatory blood pressure to the assessment of patients with mild to moderate elevations of office blood pressure. Cardiovasc Rev Rep 1980; 1: 295-303
53. Fotherby MD, Potter JE Orthostatic hypotension and antihypertensive therapy in the elderly. Postgrad Med J 1994; 70: 878-81
54. Garbus SB, Weber MA, Priest RT, et al. The abrupt discontinuation of anti-hypertensive treatment. J Clin Pharmacol 1979; Aug-Sep: 476-86
55. Miller RR, Olson HG, Amsterdam EA, et al. Propranolol withdrawal rebound phenomenon. Exacerbation of coronary events after abrupt discontinuation of anti-anginal therapy. New Engl J Med 1975; 295: 416-8
© Adls International Limited. All rights reserved.
Fotherby
56. Olsson G, Hjemdahl P, Rehnqvist N. Rebound phenomena following gradual withdrawal of chronic metoprolol treatment in patients with ischaemic heart disease. Am Heart J 1984; 108: 454-62
57. Webster J, Hawksworth GM, Barber HE, et al. Withdrawal of long-term therapy with atenolol in hypertensive patients. Br J Clin Pharmacol1981; 12: 211-4
58. Straand J, Fugelli P, Laake AK. Withdrawing long term diuretic treatment among elderly patients in general practice. Fam Pract 1993; 10: 38-42
59. Cooper WD, Glover DR, Hormbrey JM. Symptoms in hypertensive patients: the effect of treatment withdrawal. J Hypertens 1988; 6 Suppl. 4: S629-30
Correspondence and reprints: Dr Martin D. Fotherby, Division of Medicine for the Elderly, Department of Medicine, University of Leicester, The Glenfield Hospital, Groby Road, Leicester LE3 9QP, England.
Drugs & Aging 6 (6) 1995