why can’t my patient hear me? james m. sosman, md
TRANSCRIPT

Why Can’t My Patient Hear Me?
James M. Sosman, MD

ID: The patient is a 57 year-old healthy Caucasian man who presented with
intermittent headaches with sudden hearing loss.
History of Present Illness:
• He noted a one month history of intermittent, throbbing occipital headaches that were not associated with photophobia, nausea, or vomiting.
• There was no response to Ibuprofen and a moderate response to Tramadol.
• He was admitted to a local hospital when the headaches began to be associated with jaw pain

HPI (continued)…:
• At the local hospital, he complained of a left-sided earache with hearing loss, left-sided facial pain, severe rotational vertigo, nausea, vomiting, and visual “floaters”
• A head CT scan was negative
• He was transferred to UWHC for further evaluation.

Past Medical History:
• History of “elevated liver enzymes” found incidentally 6 months agowhen he applied for life insurance; no further evaluation had been done
• Pinning of an open fracture of 5th digit at MCP joint on left arm
• Inguinal hernia repair in the 1960s
Family/Social History:
• Works as a farmer
• No tobacco, alcohol, or illicit drug use.
• Family history was negative for cancer and liver disease.

Medications:
• None, besides occasional Ibuprofen and Tramadol for his recent headaches
Allergies:
• Iodine contrast (nausea, vomiting, and diaphoresis)
ROS:
• Low back pain for which he was treated with Valdecoxib • History of oral ulcers shortly after starting the Valdecoxib, this medication
was then stopped• No fevers, chills , night sweats , weight loss• No abdominal pain , diarrhea , constipation , melena , BRBPR• No rashes

Physical Examination:
Vitals – T 36.2 HR 64 BP 150/84 RR 16 SaO2 93% on RA
- His sclera were anicteric.
- The pupils were normal size with normal reaction to accommodation and light. Fundus without lesions.
- Visual acuity was normal and extra-ocular muscles were intact.
- Mild horizontal nystagmus.
- Otoscopic exam was normal.
- The oropharynx was normal without any oral lesions
- The temporal arteries were not tender to palpation
- The neck was supple. There was no lymphadenopathy

Physical Examination:
- The lungs had no wheezes, rhonchi, or crackles.
- There were no murmurs, rubs, or extra sounds on cardiovascular
exam.
- The abdomen was soft, non-tender, and non-distended. There were no masses and no hepatosplenomegaly.
- The extremities were warm and there were no rashes or edema.
- He had 2+ peripheral pulses in all extremities
- The musculoskeletal exam was normal.
- The cranial nerves were normal. Sound lateralized to the right with the Weber test. In both ears, air conduction was greater than bone conduction with the Rinne test

Possible diagnosis?Possible diagnosis?

Conductive Vs Sensorineural hearing loss?


DDx: Unilateral Sensorineural Hearing Loss with or without Headache• meningitis
• Meniere’s Disease
• mastoiditis
• viral infection – VZV (Ramsay Hunt), HSV 1, mumps, measles, rubella, influenza
• Syphilis, Lyme disease
• multiple sclerosis
• autoimmune – RA, SLE, Sjögren’s, Antiphospholipid syndrome
• vasculitis – Wegener’s, PAN, GCA
• medication (drug toxicity) – Aminoglycosides, Furosemide, ASA Vincristine, Cisplatin, Vancomycin, Erythromycin, Quinine,

Laboratory Tests:
• CBC WBC 11.1K Hct 35.5 MCV 80 Plts 440K
• Chem 7 Na 137 K 3.8 Chl 101 CO2 21 BUN 12 Cr 1 Glu 86
• Liver Function Tests Tbili 0.5 Alk Phos 523 GGT 1231 AST 23 ALT 37
INR 1.0 Albumin 3.7
• TSH Normal
• VDRL Non-reactive
• Lumbar Puncture WBC 0-1 RBC 65 Glu 61 Pro 63 Culture Neg
• ANA 1:160, speckled
• Rheumatoid Factor 1:160
• ESR/CRP 116 / 5.3

Further Diagnostic Workup:
• MRI/MRA of head was normal
• Temporal Artery biopsy was negative for inflammation and negative for multinucleated giant cells
• Workup of abnormal liver function tests:
• Hepatitis A/B/C serologies were negative• Ceruloplasmin was negative• alpha-1 anti-trypsin level was normal• anti-smooth muscle antibody was negative• c-ANCA was negative• p-ANCA was positive

Further diagnostic workup continued:
• Liver biopsy was performed
Pathologic evaluation revealed a lymphoplasmocytic portal infiltrate with focal inflammation of the bile ducts, but no actual loss of the bile ducts.

Further diagnostic workup continued:
• Workup of sensorineural hearing loss:
• Pure tone audiometry testing showed normal hearing on the right and a severe to profound sensorineural hearing loss on the left with no word recognition.
• Vestibular testing revealed a unilateral vestibulopathy in addition to the sensoirneural hearing loss diagnosed with audiometry.
• Workup of visual “floaters”:
• Slit-lamp exam revealed a mild cell reaction in the anterior chambers consistent with a mild bilateral anterior uveitis

Further diagnostic workup continued:
• Workup of microcytic anemia (Hct 35.5, MCV 80) :
• Iron Studies
Iron 43 (50-150 µg/dL)TIBC 419 (250-370 µg/dL)Ferritin 69.6 (15-400 ng/mL)
• Stool guaiacs were positive
•Further diagnostic tests?
Further diagnostic workup continued:
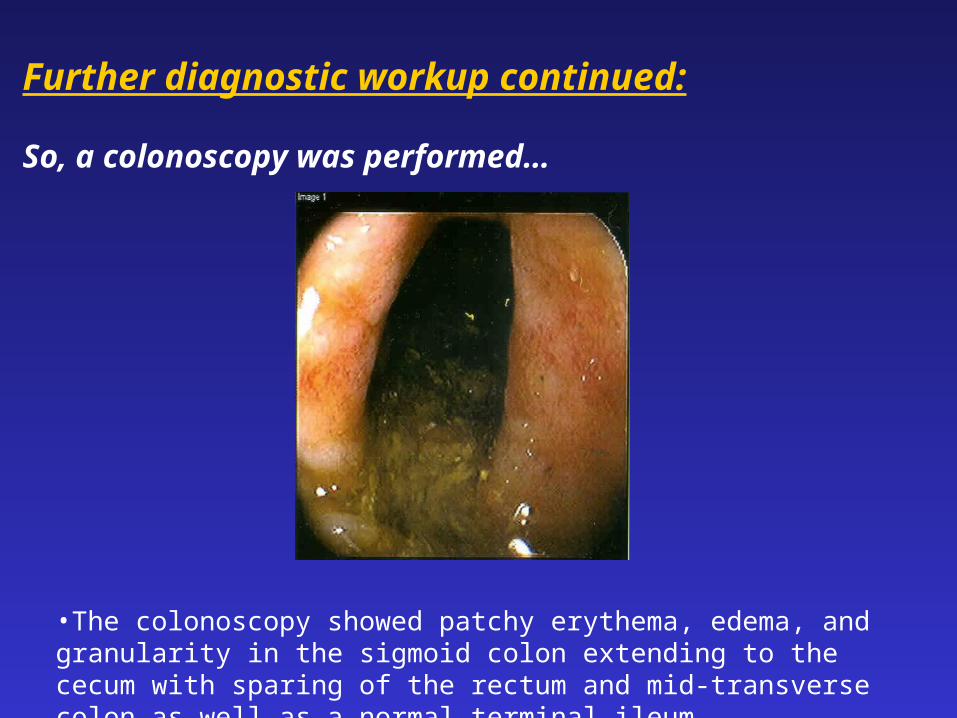
So, a colonoscopy was performed…
•The colonoscopy showed patchy erythema, edema, and granularity in the sigmoid colon extending to the cecum with sparing of the rectum and mid-transverse colon as well as a normal terminal ileum

Further diagnostic workup continued:
• Biopsy of the right colon revealed glandular architectural distortion anda diffuse lymphocytic inflammatory infiltrate consistent withchronic colitis

Differential Diagnosis:
• Colonscopy revealed chronic colitis
• Ophthalmology exam revealed anterior uveitis
• Neuro-Otologic exam identified a senorineural hearing loss
• The abnormal liver function tests were thought to be secondary to an autoimmune cholangitis (based on the histopathology of the liver biopsy and the response to steroid treatment)
Presumptive Diagnosis: subclinical inflammatory bowel disease (UC) with extra-intestinal manifestations including autoimmune
sensorineural hearing loss.


Autoimmune Sensorineural Hearing Loss and IBD:
• Extraintestinal manifestations of IBD are common and occur in up to25% of patients with Crohn’s and Ulcerative Colitis
• Extraintestinal manifestations include:• reactive arthropathy (up to 20% of patients)• axial arthropathy• uveitis and episcleritis• skin lesions (Erythema nodosum and Pyoderma gangrenosum)• primary sclerosing cholangitis (2-5% of patients)• sensorineural hearing loss (<5%)
• Autoimmune sensorineural hearing loss (ASNHL) was first describedin 1979 by McCabe who reported 18 patients with progressive bilateral hearing loss that responded to steroids and/or cyclophosphamide

ASNHL and IBD continued:
• ASNHL has been reported in a small number of patients with UC and
Crohn’s, it is usually bilateral and sudden in onset
• Hearing loss usually occurs during active IBD, but therehave been reports of ASNHL occurring when the disease is in remission.
• Other immune-mediated conditions associated with SNHL include:
• Rheumatoid Arthritis (30-55%)• Sjögren’s (25-40%)• Polyarteritis nodosa• SLE (21%)• Relapsing polychondritis• Giant Cell Arteritis• Wegener’s granulomatosis (8%)

ASNHL and IBD continued:
• Kumar et al. in 2000 reported results from a prospective study of 20 patients with active UC and 20 healthy age and sex-matched controls:
• pure tone audiometry revealed significant SNHL throughout all frequencies in patients with UC compared with controls
• no UC patients or controls complained of auditory symptoms
• no association was found between hearing loss and smoking history, extent of disease, coexistence of other extraintestinalmanifestations, or immunosuppressive therapy
• subclinical SNHL can be associated with UC

ASNHL:•More common in women than men
•Pathogenesis of ASNHL is unclear, hypotheses include:
• T-lymphocyte mediated cytotoxicity
• immune complex deposition
• vasculitis of the inner ear
• auto-immunity due to hidden self-antigens
• cross-reacting antibodies
• non-specific effect of systemic inflammation with increasedlevels of peripheral blood T-lymphocytes and circulating pro-inflammatory cytokines such as IL-1, IL-6, and TNF which can cause a low-grade progressive tissue injury
•Diagnosis is clinical based on presentation and response to therapy


ASNHL continued:
• Specifically, antibodies to type II collagen have been implicated as well
as an anti-68 kd autoantibody. The 68 kd antigen has in turn beenlinked to the highly inducible heat shock protein (hsp) 70. Antibodies to hsp 70 can be identified using the Otoblot Western blot assay (Sensitivity = 42%, Specificity = 90%, PPV 91%)
• hsp 70 is one of the many cross-reacting proteins against the innerear which may be linked to immune-mediated hearing loss
• Therefore, the clinical response to steroid therapy establishes the presumptive diagnosis of immune-mediated hearing loss
• In order to prevent irreversible damage and help preserve auditoryfunction immediate treatment with steroids is recommended

Hospital Course:
• The patient was started on Fluromethalone drops for his uveitis whichcompletely resolved within two weeks.
• Therapy for the patient’s sensorineural hearing loss included Prednisone 1 mg/kg with a quick taper, but repeat audiometric testing showed normalization of the vestibulopathy with only minimal improvement in his hearing. He continues to have some dysequilibrium and tinnitus.
• His liver function tests normalized after initiating oral steroids.
• Throughout his hospital stay he continued to deny any GI complaints.
• However, five months later… he is reporting 2-3 loose stoolsper day with occasional blood. A repeat colonoscopy is pending.

Learning Objectives:
1. Identify extraintestinal manifestations of IBD.
2. Recognize that there is a well-documented association between sensorineural hearing loss and IBD.
3. Learn some of the hypotheses behind the pathogenesis of autoimmunesensorineural hearing loss.
4. Recognize the importance of immediate treatment of autoimmunesensorineural hearing loss.

References:
1. Bachmeyer C, Leclerc-Landgraf N, Laurette F, Coutarel P, Cadranel JF, Medioni J,Dhote R, Mougeot-Martin M. Acute autoimmune sensorineural hearing lossassociated with Crohn’s disease. Amer Jour Gastro. Vol 93 (12): 2565-2567, 1998.
2. Kanra G, Kara A, Secmeer G, Ozen H, Gurakan F, Akcoren Z, Atas A. Sensorineural hearing loss as an extra-intestinal manifestation of ulcerative colitis in an adolescent girl with pyoderma gangrenosum. Eur J Pediatr.Vol 161: 216-218, 2002.
3. Kumar BN, Smith MSH, Walsh RM, Green JRB. Sensorineural hearing loss inulcerative colitis. Clin Otolaryngol Vol 25: 143-145, 2000.
4. McCabe BF. Autoimmune sensorineural hearing loss. Ann Otol. Vol 88: 585-9,1979.
5. Mathews J, Rao S, Kumar BN, Phil M. Autoimmune sensorineural hearingloss: is it still a clinical diagnosis? Jour Laryngology & Otology.Vol 117: 212-214,2003.