who europe and antimicrobial medicines consumption. hanne bak pedersen (who/europe)
TRANSCRIPT

Hanne Bak Pedersen, Programme Manager
Health Technologies and Pharmaceuticals (HTP)
WHO Regional Office for Europe
Stockholm, 13 February 2015
Antimicrobial Medicines
Consumption (AMC)
Challenges of AMC data collection on national and
regional level in Europe
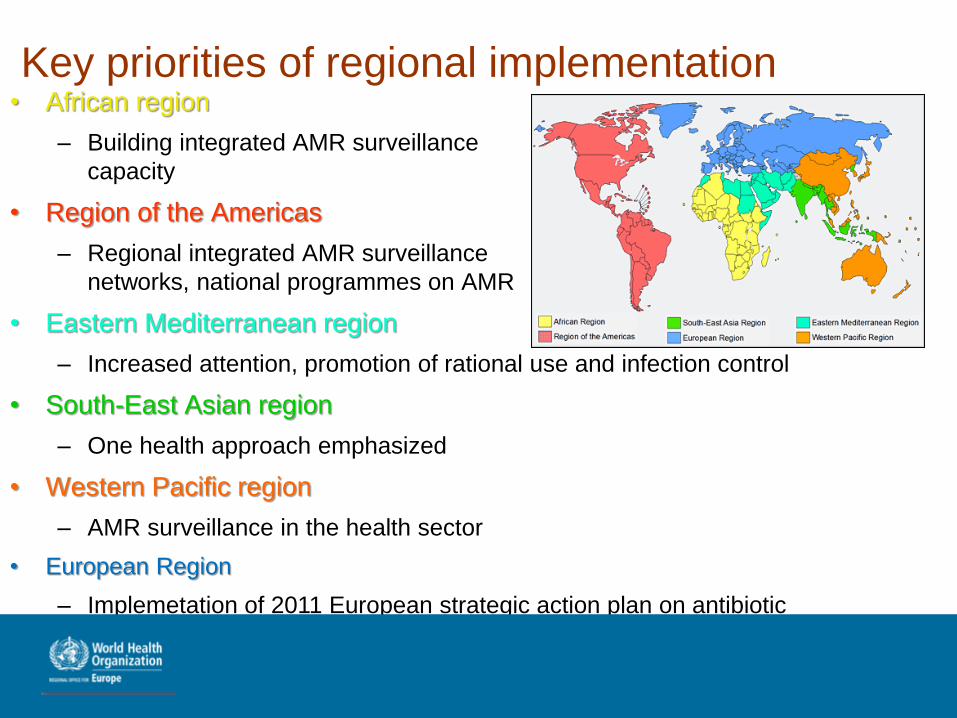
Key priorities of regional implementation• African region
– Building integrated AMR surveillance
capacity
• Region of the Americas
– Regional integrated AMR surveillance
networks, national programmes on AMR
• Eastern Mediterranean region
– Increased attention, promotion of rational use and infection control
• South-East Asian region
– One health approach emphasized
• Western Pacific region
– AMR surveillance in the health sector
• European Region
– Implemetation of 2011 European strategic action plan on antibiotic
resistance
Registers and drug utilisation studies in
Europe
• ATC/DDD - “International language for drug utilization research” -serve as a tool for presenting drug utilization research in order to improve quality of drug use
• Experiences and use vary and WHO/Europe am supporting countries with establishing medicines registers that build on the ATC/DDD methodology to facilitate retrieval, compare data and use evidence for policy action
• AMC is in target but with time the registers can expand and be used to support appropriate use of medicines broadly
• Support from WHO Collaborating Centre for Drug Statistics Methodology at the Norwegian Institute of Public Health
WHO/Europe AMC project
Initial findings: 2011 data in collaboration
with Antwerp University
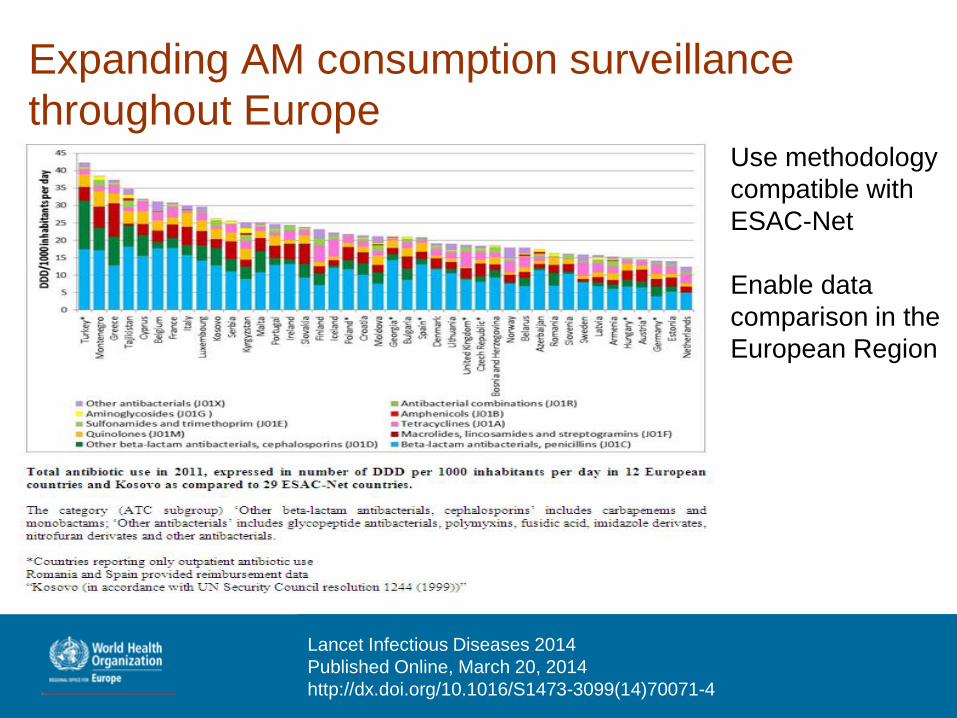
Expanding AM consumption surveillance
throughout EuropeUse methodology
compatible with
ESAC-Net
Enable data
comparison in the
European Region
Lancet Infectious Diseases 2014
Published Online, March 20, 2014
http://dx.doi.org/10.1016/S1473-3099(14)70071-4
WHO/Europe AMC project
Preliminary 2013 results in collaboration with
Arno Muller
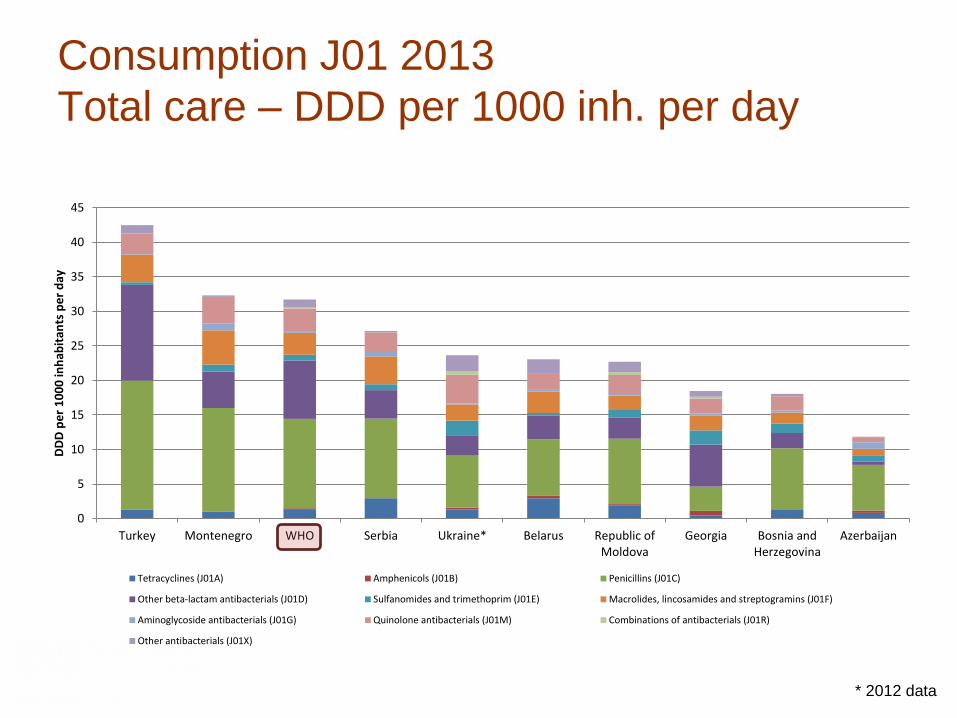
Consumption J01 2013
Total care – DDD per 1000 inh. per day
0
5
10
15
20
25
30
35
40
45
Turkey Montenegro WHO Serbia Ukraine* Belarus Republic ofMoldova
Georgia Bosnia andHerzegovina
Azerbaijan
DD
D p
er
10
00
inh
abit
ants
pe
r d
ay
Tetracyclines (J01A) Amphenicols (J01B) Penicillins (J01C)
Other beta-lactam antibacterials (J01D) Sulfanomides and trimethoprim (J01E) Macrolides, lincosamides and streptogramins (J01F)
Aminoglycoside antibacterials (J01G) Quinolone antibacterials (J01M) Combinations of antibacterials (J01R)
Other antibacterials (J01X)
* 2012 data
0
5
10
15
20
25
30
35
40
45
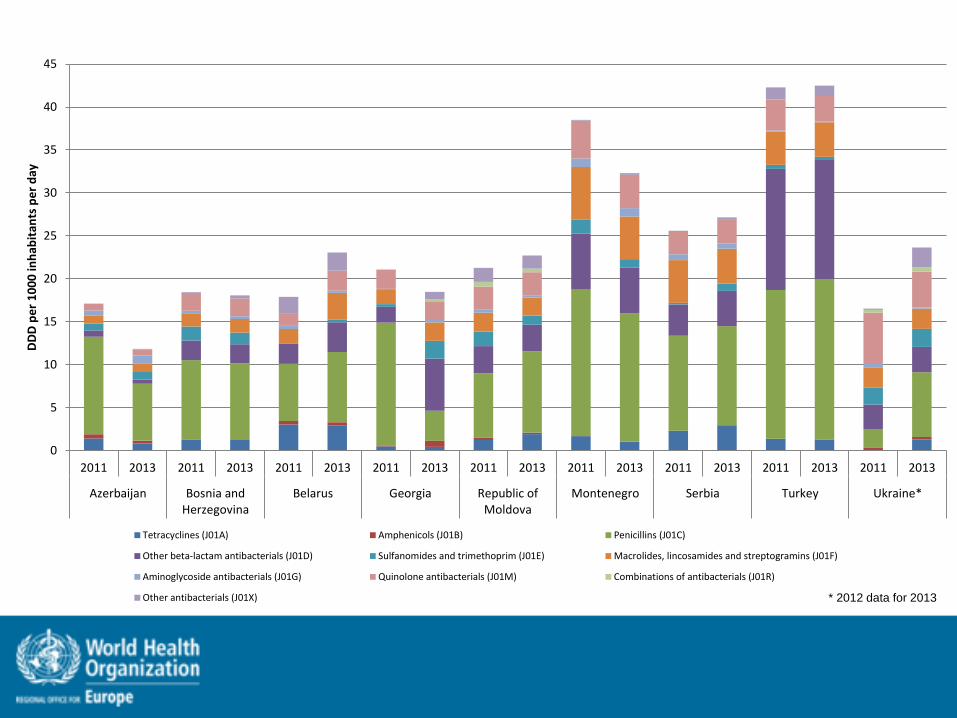
2011 2013 2011 2013 2011 2013 2011 2013 2011 2013 2011 2013 2011 2013 2011 2013 2011 2013
Azerbaijan Bosnia andHerzegovina
Belarus Georgia Republic ofMoldova
Montenegro Serbia Turkey Ukraine*
DD
D p
er
10
00
inh
abit
ants
pe
r d
ay
Tetracyclines (J01A) Amphenicols (J01B) Penicillins (J01C)
Other beta-lactam antibacterials (J01D) Sulfanomides and trimethoprim (J01E) Macrolides, lincosamides and streptogramins (J01F)
Aminoglycoside antibacterials (J01G) Quinolone antibacterials (J01M) Combinations of antibacterials (J01R)
Other antibacterials (J01X) * 2012 data for 2013
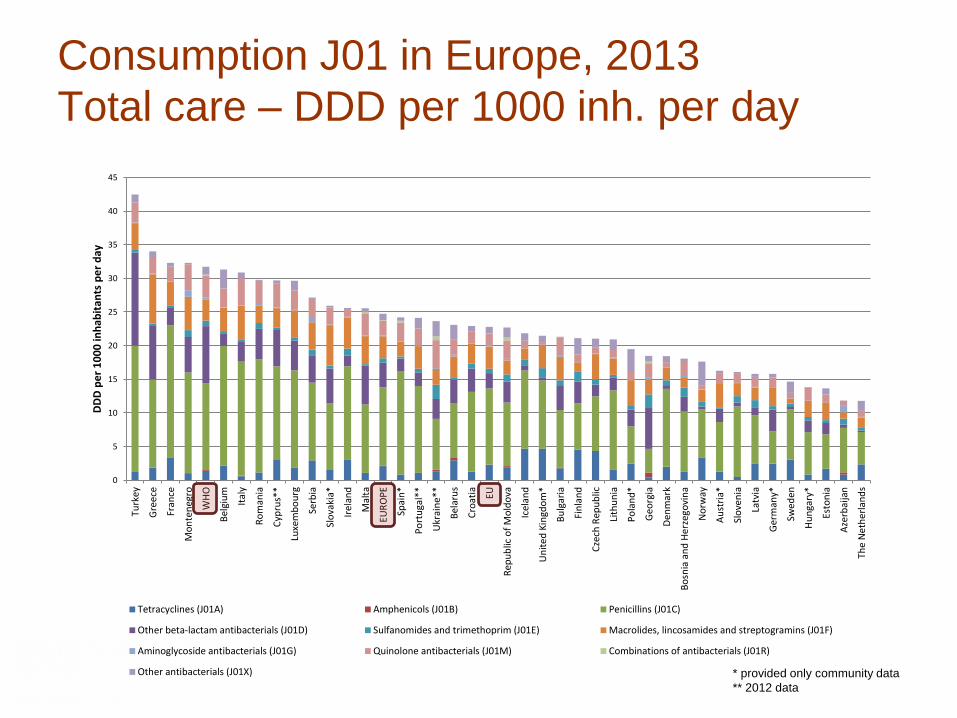
Consumption J01 in Europe, 2013
Total care – DDD per 1000 inh. per day
0
5
10
15
20
25
30
35
40
45
Turk
ey
Gre
ece
Fran
ce
Mo
nte
neg
ro
WH
O
Bel
giu
m
Ital
y
Ro
man
ia
Cyp
rus*
*
Luxe
mb
ou
rg
Serb
ia
Slo
vaki
a*
Irel
and
Mal
ta
EUR
OP
E
Spai
n*
Po
rtu
gal*
*
Ukr
ain
e**
Bel
aru
s
Cro
atia EU
Rep
ub
lic o
f M
old
ova
Icel
and
Un
ite
d K
ingd
om
*
Bu
lgar
ia
Fin
lan
d
Cze
ch R
epu
blic
Lith
un
ia
Po
lan
d*
Geo
rgia
Den
mar
k
Bo
snia
an
d H
erz
ego
vin
a
No
rway
Au
stri
a*
Slo
ven
ia
Latv
ia
Ger
man
y*
Swed
en
Hu
nga
ry*
Esto
nia
Aze
rbai
jan
The
Net
he
rlan
ds
DD
D p
er
10
00
inh
abit
ants
pe
r d
ay
Tetracyclines (J01A) Amphenicols (J01B) Penicillins (J01C)
Other beta-lactam antibacterials (J01D) Sulfanomides and trimethoprim (J01E) Macrolides, lincosamides and streptogramins (J01F)
Aminoglycoside antibacterials (J01G) Quinolone antibacterials (J01M) Combinations of antibacterials (J01R)
Other antibacterials (J01X) * provided only community data
** 2012 data
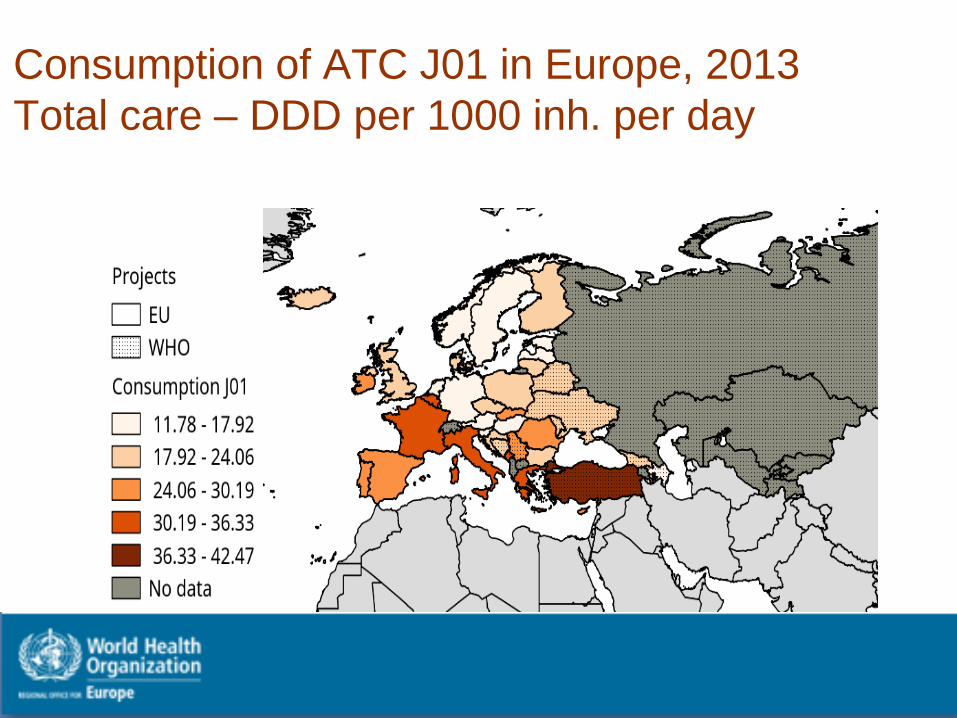
Consumption of ATC J01 in Europe, 2013
Total care – DDD per 1000 inh. per day
Similarities/Differences between EU and
WHO methodologies• Both methodologies are very similar
• Management of combined products is slightly different.
– WHO follows strictly the ATC/DDD methodology
– ECDC does not follow strictly the ATC/DDD methodology
– However both methods should give the same figuresex: J01EE01
• WHO: 1 DDD = 4 unit doses (1 unit dose = sulfa: 0.4g, trim: 80mg)
• ESAC-Net: 1 DDD = 1.92g
• Main difference is the data sources and types used by both projects.
– WHO uses mostly wholesales (one country reported reimbursement data), no clear differentiation between hospital and community sectors
– ESAC-Net uses either sales or/and reimbursement data, for most of the countries, it is possible to differentiate between both sectors
Member State actions taken examples:
Armenia: Development of national drug register ; MoH activities to increase
awareness on resistance to antibiotics; Development of
Strategy for Containment of Antimicrobial Resistance
Azerbaijan: Development of national drug register
Georgia: Lobbying for new law to stop OTC dispense of antibiotics; Activities to
increase awareness on resistance to antibiotics; Development of national AMR
action plan
Former Yugoslav Republic of Macedonia: MoH activities to increase awareness
on resistance to antibiotics; enforcement of prescription only dispensing
Kyrgyzstan: Development and adoption of national drug policy
Kosovo (in accordance with UN Security Council resolution 1244 (1999)) :Activities to increase awareness on
resistance to antibiotics incl. mass media
Serbia: Development of national drug policy; enforcement of prescription only
dispensing
Turkey: National plan on rational drug use (2013-2017); MoH activities to increase
awareness on resistance to antibiotics incl. mass media; enforcement of
prescription only dispensing
Next steps
• Multi-country AMR consultation 24-27 February
including ATC/DDD workshop, consultation on AMC
data from 2012-13 as well as on qualitative follow up
study initially carried out in Albania and Turkey
• Finalise and publish 2011/12/13 AMC data and
continue with 2014 surveillance
• The qualitative research protocol is developed with
the Institute of social pharmacy, Copenhagen
University and we plan to support that studies are
undertaken in all the AMC project group countries
Next steps: Responsible use of antimicrobial
medicines
• Regulatory mechanisms for new antibiotics
• Effective low-cost tools for diagnosis and susceptibility
testing – support appropriate use of these in the country
specific context
• Access to medicines accompanied by measures to
protect continued efficacy incl. in line with Good
Distribution Practices, prescription restrictions etc
• Codes of practice; standards for presence of
antimicrobials and antimicrobial residues in the
environment, water supply and food
Key messages for shaping and implementing
the Global Action Plan
Support country action:
• Strengthen national intersectoral and interdisciplinary
coordination
• Promote prudent use policies and enforcement
• Building surveillance capacity
• Awareness-raising among all stakeholders
Thank you for your attention !The role of pharmacist in encouraging prudent use of antibiotic medicines
and averting antimicrobial resistance – a review of current policies and
experiences in Europe
http://www.euro.who.int/en/health-topics/Health-
systems/medicines/publications2/2014/the-role-of-pharmacist-in-
encouraging-prudent-use-of-antibiotic-medicines-and-averting-
antimicrobial-resistance-a-review-of-current-policies-and-experiences-in-
europe
Health Technologies and Pharmaceutical web site:
http://www.euro.who.int/en/health-topics/Health-systems/medicines
Programme manager [email protected]