who drug informationwho.int/medicinedocs/index/assoc/s14170e/s14170e.pdfsouth centre 215 health...
TRANSCRIPT
WHO DRUG
INFORMATION V O L U M E 12 • N U M B E R 4 • 1 9 9 8
P R O P O S E D I N N L I S T 8 0 I N T E R N A T I O N A L N O N P R O P R I E T A R Y N A M E S F O R P H A R M A C E U T I C A L S U B S T A N C E S
W O R L D H E A L T H O R G A N I Z A T I O N • G E N E V A

Volume 12, Number 4, 1998 World Health Organization, Geneva
WHO Drug Information
i
Contents
General Policy IssuesWHO's Revised Drug Strategy 209The World Intellectual Property Organization 209Pharmaceutical patents and the TRIPS
Agreement 211WTO Agreement on Technical Barriers
to Trade 213South Centre 215Health Action International 216International Federation of Pharmaceutical
Manufacturers Associations 219International Generic Pharmaceutical Alliance 220
Reports on Individual DrugsThe life-threatening risks of therapy
substitution 222Revision of HIV treatment guidelines 222Levonorgestrel for emergency contraception 223Cancer risk in women exposed to
diethylstilbestrol in utero 224Zidovudine for mother-to-child transmission
of HIV 225
General InformationRecommendations from the Expert Committee
on Drug Dependence 227Insulin: availability, affordability,
and harmonization 230
Regulatory MattersBruising and bleeding with new
antidepressants 235Reports of death in sildenafil users 235Lipodystrophy and HIV protease inhibitors 235Cisapride: new contraindications 236Cisapride: risk of arrhythmias 236Mibefradil: instructions for therapy substitution 237Mibefradil suspended in Germany 237
Isotretinoin: adverse reaction profile 237Depression with isotretinoin 238Orlistat sold illegally 238Trastuzumab: approved for breast cancer 238Ritonavir and ecstasy — a fatal combination 238WHO recommendations for influenza virus
vaccines — 1999 238Rhabdomyolysis and ritodrine 239Flutamide: severe hepatic dysfunction 239Ebrotidine: liver toxicity 239Meloxicam: gastrointestinal and skin
reactions 239Vaccine-associated thrombocytopenic purpura 240Abortifacients on free sale 240Illegal and counterfeit sildenafil on sale 240Current standards for over-the-counter
analgesics 240Safety of leukotriene antagonists 241Reformulation of flunitrazepam tablets to
prevent misuse 241Nicergoline re-evaluated 241Entacapone for Parkinson disease 242Chinese herbal medicines and adverse
reactions 242
Essential DrugsWHO Model Formulary:Ophthalmological preparationsAnti-infective agents 243
Gentamicin 243Idoxuridine 244Silver Nitrate 244Tetracycline 244
Anti-inflammatory agents 244Prednisolone 245
Local anaesthetics 245Tetracaine 245
Miotics and antiglaucoma drugs 245Acetazolamide 246Pilocarpine 246Timolol 246
Mydriatics 246Atropine 247Epinephrine 247
.../...
243

WHO Drug Information Vol. 12, No. 4, 1998
40
World Health Organization, Geneva
Contents (continued)
ii
251
Antiparkinsonism drugsLevodopa/carbidopa 248Biperiden 248
Recent Publications and DocumentsGuidelines for HIV and infant feeding 249Symptom relief in terminal illness 249Guidance modules on antiretroviral treatments 249Re-evaluating the safety profile of marketed
drugs 250Interventions to improve antimalarial use 250
Proposed InternationalNonproprietary Names: List 80

209
WHO Drug Information Vol. 12, No. 4, 1998
General Policy Issues
WHO's Revised Drug Strategy
WHO's Revised Drug Strategy was conceived in the mid-1980s to foster unity among governments,industry, consumers, academia, nongovernmental organizations, and specialized agencies. Its aim is toensure equity of access to safe drugs of proven quality by all peoples of the world and to promote theirrational use. At the same time, it seeks to remind each party of its responsibilities in the manufacture andprovision of drugs.
In compliance with the terms of the Strategy, WHO has supported governments in the formulation andimplementation of national drug policies and essential drugs programmes, expanded its normativeactivities, intensified the dissemination of information, conducted operational research on key drug issues,developed innovative training materials and programmes, and promoted collaboration. Since the originaldrafting of the Strategy, various World Health Assembly resolutions have addressed related topics suchas access to essential drugs, quality assurance, drug safety, medicinal drug promotion, drug donations,provison of independent drug information and consumer education and protection. WHO has also beenrequested to report on the impact of the work of the World Trade Organization (WTO) with respect tonational drug policies and essential drugs and make recommendations for collaboration between WTO andWHO.
In May 1998, the World Health Assembly considered a Resolution on the Revised Drug Strategy* whichled to extensive debate among members of the Assembly. It was agreed that an open-ended ad hocworking group should be established to review the complex issues raised by the Resolution, particularlyin relation to the public health implications of trade agreements and access to essential drugs.
A summary of the presentations made by panelists at the meeting of the ad hoc Working Group on theRevised Drug Strategy held from 13–16 October 1998 is set out below. The presentations represent thepolicy and views of the World Intellectual Property Organization (WIPO), the World Trade Organization(WTO), the South Centre, Health Action International (HAI), the International Federation of PharmaceuticalManufacturers Associations (IFPMA), and the International Generic Pharmaceutical Alliance (IGPA).
* Resolution EB101.R24.
The World IntellectualProperty Organization
Mr Richard Wilder, Director-Advisor, Office ofLegal and Organization Affairs, WorldIntellectual Property Organization, Geneva
The World Intellectual Property Organization(WIPO) is an intergovernmental organization withheadquarters in Geneva, Switzerland. It is one ofthe 16 specialized agencies of the United Nationssystem. As of 21 September 1998, there are 171States members of the Convention establishingWIPO. Through cooperation among States, WIPOis responsible for the promotion of protection ofintellectual property throughout the world and for
the administration of various multilateral treatiesdealing with the legal and administrative aspects ofintellectual property. Its principal activities are theprogressive development of norms in intellectualproperty, and the administration of certain treatiesfor global protection of intellectual property, inparticular for patents, trademarks, industrial designsand development cooperation.
One of the main tasks of WIPO is to cooperate withdeveloping countries in their efforts to developintellectual property. Its main objectives in thisregard are:
• To encourage and increase, in quantity andimportance, the creation of patentable inventions

210
WHO Drug Information Vol. 12, No. 4, 1998General Policy Issues
by nationals and national enterprises in develop-ing countries in order to enhance their technologi-cal self-reliance and competitiveness in interna-tional markets.
• To improve the conditions of acquisition of foreignpatented technology, making these conditionsmore favourable than they are today.
• To increase the competitiveness of developingcountries in international trade through betterprotection and more effective use of trademarksand service marks in such trade and in commerce.
• To facilitate access to technological informationcontained in patent documents and disseminatesuch information to users.
If these objectives are to be met, most developingcountries will need to do one or more of the follow-ing: enact or modernize national legislation, streng-then governmental institutions, accede to interna-tional treaties, acquire more specialists in govern-ment, industry and the legal profession, and acquirebetter access to and make better use of industrialproperty information including patent documents.WIPO provides training and technical assistance todeveloping countries in all of these areas and hasbeen doing so for many years. Recently, theseactivities have been expanded to include mattersrelating to implementation of the TRIPS Agreement.
Patent protection and proceduresfor application and legal effectIn respect to patent protection, there are severalkey points to be borne in mind in gauging theeconomic impact of the patent system. Thesepoints apply equally to patent protection for phar-maceutical processes and products. Firstly, thepatent system encourages people to invent. Be-cause they are granted exclusive rights to an inven-tion, for a limited period of time, individuals orcommercial enterprises are more willing to invest inthe resources necessary to make and commercial-ize the invention. The patent system also encour-ages people to disclose inventions rather thanretain them as trade secrets.
An application for patent protection must be filed inevery country, or region, where protection is de-sired. The decision to file or not is a businessdecision based upon the cost of obtaining protec-tion versus the value of that protection in a givencountry. It is rare that a person or company will filefor patent protection in every country having a
patent system. Furthermore, many patent systemsrequire the payment of fees to keep both applica-tions and granted patents in force.
A patent, to be valid, must meet certain conditions.First, it must relate to subject matter that is notexcluded from patent protection. A diminishingnumber of countries still exclude pharmaceuticalproducts from patent protection. WIPO advice is notto exclude such subject matter. Furthermore, theinvention for which protection is sought must benovel and involve an inventive step. That is, it mustnot be an invention that is obvious to persons whoare skilled in that area of technology. The inventionmust be useful or be applicable in some area ofindustry. In addition, the patent application mustdisclose the invention in such a way that personsskilled in the relevant area of technology can alsomake and use the invention.
Many offices require that a patent application, oncefiled, be subject to search and examination todetermine if it meets the requirements for patent-ability. A search involves looking for "prior art", i.e.prior patent documents or other literature that maybe relevant to the invention. Following the search,the invention is examined to compare it with theprior art to determine if it meets the requirementsfor patentability. If these conditions are met, thepatent is granted and will have effect for a limitedperiod of time — at least 20 years from the filingdate. There is no requirement that every patentoffice should do such a search and examinationitself. For example, many offices rely on the workthat has already been done in respect of the sameinvention by other offices. Moreover, some officesgrant protection without a search and examinationhaving been performed. It should be noted thatWIPO administers an assistance programmewhereby searches and examinations can be per-formed for patent offices that do not have thefacilities to do so themselves.
The patentee has the right to prevent others fromusing the invention without his permission. This is anegative right. The grant of a patent does not givethe patentee a positive right to use the patentedinvention. Thus, other laws, such as those for theprotection of the environment or human or animalhealth may constrain the use to which the patenteemay put the invention. Such constraints include, forexample, the requirement in many countries toobtain marketing approval for pharmaceuticalproducts from a health ministry. In respect of pre-venting others from using the invention, the paten-

211
WHO Drug Information Vol. 12, No. 4, 1998
tee is limited to the scope of the claim contained inthe patent. The claim is a formal part of the patentwhich clearly indicates the scope of the patent. It isthe claim against which the patentability of aninvention is judged and against which infringementby others of the patent is determined.
The exercise of the right to exclude others fromusing a patented invention may be subject to limita-tions in some countries, including the right of thegovernment to use the invention or by the grant ofcompulsory licenses. Moreover, countries may putin place legislation that specifies practices in thelicensing of patents that have an anti-competitiveeffect.
A patent system, to function properly, should bebalanced. On the one hand, the patentee must begranted effective protection for an invention toinduce further research and encourage the disclo-sure of inventions to the public. On the other hand,national law may take cognizance of the con-straints, as noted above, that may be imposed onthe grant and exercise of the patent right.
Pharmaceutical patentsand the TRIPS Agreement
Mr A. Otten, Director, Intellectual Property andInvestment, World Trade Organization,Geneva
The purpose of this note is to describe provisions ofthe Agreement on Trade-Related Aspects of Intel-lectual Property Rights (TRIPS Agreement) thatrelate to the standards of patent protection to beaccorded to inventions in the area of pharmaceuti-cals. To set this discussion in context, it is useful torecall three basic features of the TRIPS Agreement:
1. The TRIPS Agreement, together with some 25other legal texts, is an integral part of the Agree-ment Establishing the World Trade Organization(WTO) (and is therefore subject to the WTO disputesettlement system).
2. It covers not only patents but all the other mainareas of intellectual property rights.
3. It lays down not only the minimum substantivestandards of protection that should be provided forin each of these areas of intellectual property butalso the procedures and remedies that should be
available so that rights holders can enforce theirrights effectively.
What pharmaceutical inventions must bepatentable under the TRIPS Agreement?The main rule relating to patentability is that patentsshall be available for any invention, whether aproduct or process, in all fields of technology with-out discrimination, where those inventions meet thestandard substantive criteria for patentability —namely, novelty, inventive step and industrialapplicability. In addition, Members are required tomake grant of a patent dependent on adequatedisclosure of the invention and may require infor-mation on the best mode for carrying it out. Dis-closure is a key part of the social contract that thegrant of a patent constitutes, since it makes publiclyavailable important technical information which maybe of use to others in advancing technology in thearea, even during the patent term, and ensuresthat, after expiry of the patent term, the inventiontruly falls into the public domain because othershave the necessary information to carry it out.
Three types of exception to the above rule onpatentable subject-matter are allowed. These maybe of interest from a public health perspective.
• Inventions the prevention of whose commercialexploitation is necessary to protect public order ormorality, including to protect animal or plant life orhealth.
• Diagnostic, therapeutic and surgical methods forthe treatment of humans or animals.
• Certain plant and animal inventions.
What are the rights conferred by a patentunder the TRIPS Agreement?The minimum rights that must be conferred by apatent under the TRIPS Agreement follow closelythose that were to be found in most patent laws,namely the right for the patent owner to preventunauthorized persons from using the patentedprocess and from making, using, offering for sale,or importing the patented product or a productobtained directly by the patented process.
Term of protectionUnder the TRIPS Agreement, the term of protectionmust be at least 20 years from the date of filing thepatent application. It should be noted that, althoughthe issue of patent term extension to compensate
General Policy Issues

212
WHO Drug Information Vol. 12, No. 4, 1998
for regulatory delays in the marketing of new phar-maceutical products was raised in the negotiations,the TRIPS Agreement does not contain an obliga-tion to introduce such a system1.
Limitations/exceptions to these rightsUnder the TRIPS Agreement, patent rights are notabsolute but can be subject to limitations or excep-tions. These can be put into three categories.
• The Agreement allows limited exceptions to bemade by Members provided that such exceptionsdo not unreasonably conflict with a normal exploi-tation of the patent and do not unreasonablyprejudice the legitimate interests of the patentowner, taking account of the legitimate interest ofthird parties. Thus, for example, many countriesallow third parties to use a patented invention forresearch purposes where the aim is to understandmore fully the invention as a basis for advancingscience and technology.
• The Agreement also allows Members to authorizeuse by third parties (compulsory licences) or forpublic non-commercial use (government use)without the authorization of the patent owner.Contrary to the desire of some countries in thenegotiations, the grounds on which this can bedone are not limited by the Agreement but theAgreement contains a number of conditions thathave to be met in order to safeguard the legiti-mate interests of the patent owner. There is notspace to discuss all of these here, but two of themain such conditions are that, as a general rule,an effort must first have been made to obtain avoluntary licence on reasonable commercial termsand conditions and that the remuneration paid tothe rights holder shall be adequate in the circum-stances of each case, taking into account theeconomic value of the licence.
• The Agreement recognizes the right of Membersto take measures, consistent with its provisions,against anti-competitive practices and providesmore flexible conditions for the grant of compul-
sory licences where a practice has been deter-mined after due process of law to be anti-competi-tive. For example, each of the conditions specifi-cally referred to above for the grant of compulsorylicences may be relaxed in these circumstances.The Agreement also provides for consultation andcooperation between Members in taking actionagainst anti-competitive practices.
Transition provisionsThe TRIPS Agreement lays down some rathercomplicated transition provisions which give coun-tries time to adapt their legislation and practices totheir TRIPS obligations. These periods differ ac-cording to the type of obligation in question and thestage of development of the country concerned.Here we will limit the discussion to those transitionprovisions which relate to the application of theobligations on substantive standards for the protec-tion of pharmaceutical inventions. For these pur-poses, the obligations should be divided into twocategories:
(i) The obligations relating to the introduction ofproduct patent protection for pharmaceuticalproducts in those developing and least devel-oped countries which do not yet grant it. Sincemost developing and least developed countryMembers of the WTO already provide for prod-uct patent protection for pharmaceuticals, arelatively small number of countries are con-cerned. 2
(ii) Obligations regarding process patents for thisgroup of countries and all patent protectionobligations for other developing and least devel-oped countries.
With respect to the second category above, thebasic rule is that developing and least developedcountries have until 1 January 2000 and 1 January2006 respectively to meet the obligations in ques-tion. At that time, the rules of the TRIPS Agreementwill apply not only to new patent applications but topatents still under protection in their territories.
2. Thirteen WTO Members (Argentina, Brazil, Cuba,Egypt, India, Kuwait, Morocco, Pakistan, Paraguay,Tunisia, Turkey, United Arab Emirates and Uruguay)have notified "mailbox "systems to the TRIPS Council,thus indicating that they do not yet grant patent protectionto pharmaceutical products. (It cannot be excluded thatthere are a few other WTO Members who should havenotified this but have not done so).
General Policy Issues
1. The effective period of patent protection for inventionsof new chemical entities is much less than the full 20years, because a large part of that period will haveexpired before marketing approval is obtained from thepublic health regulatory bodies. For this reason, most ofthe major developed countries have introduced systemswhereby a prolonged period of protection can be obtainedto compensate, at least in part, for this loss of theeffective period of protection.

213
WHO Drug Information Vol. 12, No. 4, 1998
With respect to the first category of situationsreferred to above, the developing countries inquestion have until 1 January 2005 to apply productpatent protection to pharmaceutical products andthe least developed countries until 1 January 2006.Notwithstanding proposals to the contrary, theTRIPS Agreement does not require the bringingunder protection of pharmaceutical inventions thatwere in the "pipeline" in these countries on 1 Janu-ary 1995 — the time of entry into force of theWTO.3 However, with effect from the entry intoforce of the WTO (1 January 1995), these countrieshave been under an obligation to provide a systemwhereby applications for patents for pharmaceuticalproduct inventions can be filed (often referred to asthe "mailbox" system). These applications do nothave to be examined until after 1 January 2005 (or1 January 2006 in the case of least developedcountries). If found to be patentable by reference totheir filing (or priority) date, a patent would have tobe granted for the remainder of the patent termcounted from the date of filing. In the event that apharmaceutical product that is the subject of a"mailbox" application obtains marketing approvalprior to the decision on the grant of a patent, anexclusive marketing right of up to five years willhave to be granted provided that certain conditionsare met.
Concluding remarksIt will be noted that most developing and leastdeveloped countries already grant patent protectionfor pharmaceutical products. In these countries, theTRIPS Agreement will therefore not lead to funda-mental changes in this regard, although a certainamount of adjustment in legislation, for example inrespect of patent term and compulsory licensing,may be necessary. With respect to the fairly limitednumber of countries that did not provide patentprotection for pharmaceutical products at the timeof entry into force of the WTO Agreement, some,including Brazil and Argentina, have decided tobring such protection into effect more quickly thanis required under the TRIPS Agreement.
It will also be noted that the TRIPS Agreement paysconsiderable attention to the need to find an appro-priate balance between the interests of rightsholders and users and that this was an importanttheme in the negotiations. This is not only reflected
in the basic underlying balance related to disclosureand providing an incentive for research and devel-opment (R & D), but also in the limitations andexceptions to rights that are permitted in the transi-tion provisions.
It should also be appreciated that the protection ofpharmaceutical inventions is one aspect of a muchwider agreement, covering not only the protectionof intellectual property in general in a coherent andnon-discriminatory way, but also further liberaliza-tion and strengthening of the multilateral tradingsystem as a whole. While it is true that some coun-tries put particular emphasis on TRIPS matters inthe Uruguay Round negotiations, it is also true thatother countries attached great importance to otherareas, for example textiles and agriculture.
It is our belief, and a belief shared by all WTOMembers, that a strong and vibrant multilateraltrading system is essential for creating conditions ofeconomic growth and development worldwide. This,in turn, will generate the resources required toaddress health care needs.
WTO Agreement onTechnical Barriers to Trade
Doaa Abdel MotaalWorld Trade Organization, Geneva
The World Trade Organization's Agreement onTechnical Barriers to Trade (TBT) entered into forcein 1995, with the establishment of the WTO. It wasdeveloped in response to the proliferation of non-tariff barriers to trade and focuses on producttechnical requirements.
The TBT Agreement acknowledges the right ofWTO Members to develop technical requirementsas long as these do not create unnecessary obsta-cles to international trade. It lays out a number ofprinciples which technical requirements mustrespect, including the principles of nondiscrimina-tion, harmonization, equivalence, mutual recogni-tion and transparency. It also delineates a numberof legitimate objectives for which mandatory techni-cal requirements may be developed. The scope ofthe Agreement extends to central and local govern-mental as well as nongovernmental standardizationbodies.
Coverage and definitionsThe TBT Agreement divides technical requirementsinto either technical regulations or standards.
General Policy Issues
3 The pipeline refers to the backlog of inventions of newpharmaceutical products that were no longer patentable onthat date, because disclosed, but not yet on the marketbecause they are awaiting marketing approval.

214
WHO Drug Information Vol. 12, No. 4, 1998
According to the Agreement a technical regulationis a "document which lays down product character-istics or their related processes and productionmethods, including the applicable administrativeprovisions with which compliance is mandatory. Itmay also include or deal exclusively with terminol-ogy, symbols, packaging, marking or labellingrequirements as they apply to a product, process orproduction methods."
A standard is defined as a "document approved bya recognized body, that provides for common andrepeated use, rules, guidelines or characteristics ofproducts or related processes and productionmethods, with which compliance is mandatory. Itmay also include or deal exclusively with terminol-ogy, symbols, packaging, marking or labellingrequirements as they apply to a product, process orproduction method."
Compliance with technical regulations is manda-tory, while compliance with standards is voluntary.While technical regulations are addressed throughthe main body of the Agreement, standards areaddressed separately through a Code of GoodPractice contained in an annex to the Agreement.Many of the principles applied by the Agreement totechnical regulations apply to standards through thecode. The code is open to acceptance by central,local and nongovernmental (whether national orregional) standardization bodies. The Agreementalso covers conformity assessment procedures,which it defines as "any procedure used, directly orindirectly, to determine if relevant requirements intechnical regulations or standards are fulfilled".
Legitimate objectivesUnder the Agreement, technical regulations mayonly be developed for one or more of the objectivesconsidered legitimate by the Agreement. Legitimateobjectives include inter alia, national security re-quirements, the prevention of deceptive practices,or protection of human health or safety, animal orplant life or health, or the environment. The risksassociated with legitimate objectives are assessedagainst a number of factors, including, inter alia,available scientific and technical information, re-lated processing technology or intended end-usersof products.
NondiscriminationThe principle of nondiscrimination constitutes thebackbone of the international trading system. Ingeneral, it is a principle which outlaws discrimina-tion among the products of WTO Members, and
between imported and locally produced products. Inaccordance with GATT Article I — the most-favoured nation "MFN" clause — WTO Membersare bound to grant to the products of other Mem-bers treatment which is no less favourable than thataccorded to the products of any other country.Thus, no country is to give special trading advan-tage to another, or to discriminate against it. Ac-cording to GATT Article III — the national treatmentNT clause — Members must treat imported prod-ucts no less favourably than domestically producedproducts. The TBT Agreement embraces the GATTprinciple of nondiscrimination. It states that techni-cal regulations, standards and conformity assess-ment procedures must be prepared, adopted andapplied without discrimination.
Avoidance of unnecessary obstacles tointernational tradeThe avoidance of unnecessary obstacles to interna-tional trade is the principal objective of the TBTAgreement. The Agreement states that technicalregulations, standards and conformity assessmentprocedures must not be prepared, adopted orapplied with a view to or with the effect of creatingunnecessary obstacles to trade. Technical regula-tions and conformity assessment procedures mustnot be more trade-restrictive than necessary to fulfila legitimate objective, taking into account the risksthat non-fulfilment or non-conformity would create.
HarmonizationThe TBT Agreement encourages WTO Members tobase their technical regulations, standards, andconformity assessment procedures on internationalstandards, guides and recommendations whenthese exist, and when they are deemed to beappropriate and effective. The call for harmoniza-tion is designed to avoid the emergence of unduelayers of technical requirements and assessmentprocedures, and to encourage the use of thoseadopted by the international community. To com-plement this requirement, the Agreement calls uponMembers to participate in the work of internationalstandardizing and conformity assessment bodies.However, it recognizes that there may be instancesin which Members would need to derogate from thisobligation and, for certain specific instances, allowsthem to do so.
Equivalence and mutual recognitionThe TBT Agreement calls upon Members to recog-nize other Members' technical regulations as equi-valent to their own, even when they differ, provided
General Policy Issues

215
WHO Drug Information Vol. 12, No. 4, 1998
they are satisfied that they adequately fulfil theirobjectives. As international harmonization is a time-consuming process, and is sometimes difficult toachieve, the Agreement encourages Members toaccept each other's regulations as equivalent totheir own until full-fledged international harmoniza-tion becomes possible. The Agreement also en-courages Members to mutually recognize theresults of each other's conformity assessmentprocedures.
TransparencyTransparency is a central feature of the TBT Agree-ment, and is achieved through notification obliga-tions, the establishment of enquiry points, and thecreation of the WTO TBT Committee. Notificationmeans the circulation of information by a WTOMember to other Members on matters relating tothe Agreement. Notification obligations includenotifying the measures taken to implement theprovisions of the TBT Agreement nationally, suchas how its provisions have been incorporated intodomestic legislation, notifying draft technical regula-tions, conformity assessment procedures andstandards, and providing other Members withsufficient time to comment on them — with theobligation of taking these comments into account.Draft technical regulations and conformity assess-ment procedures only have to be notified when aninternational standard, guide or recommendationdoes not exist, of they are not in accordance withexisting ones, or if they may have a significanteffect on the trade of other WTO Members. Thisincludes notifying entry into any bilateral or multilat-eral agreements regarding technical regulations,standards or conformity assessment procedures.
The TBT Agreement stipulates that each WTOMember must establish an enquiry point that canrespond to questions on technical regulations,standards and conformity assessment procedures,whether proposed or adopted, and supply relevantdocuments. The Agreement has also established aTBT Committee in the WTO which is a standingbody that acts as a forum for consultations on allissues pertaining to the Agreement. Participation inthe Committee is open to all WTO Members.
Developing countriesUnder the TBT Agreement, special and differentialtreatment for developing countries is authorized,and developed countries are encouraged to providedeveloping countries with technical assistance onall matters pertaining to the Agreement.
South Centre
Mr Carlos M. Correa, University of BuenosAires, Argentina
The TRIPS Agreement contains a number of provi-sions that are likely to affect access to medicines indeveloping countries. This is particularly the case incountries under the obligation to introduce patentprotection for pharmaceuticals. However, theeffects may also be felt in countries that alreadyoffer patent protection.
The TRIPS Agreement includes several provisionsthat are bound to strengthen the protection con-ferred on pharmaceutical products and processes,such as the provisions relating to the duration ofpatent protection (minimum 20 years from theapplication date); extension of the protection to theproducts directly obtained by a protected process;reversal of the burden of proof in the case of civilprocedures relating to process patents; and protec-tion of confidential data submitted in applications forthe approval of pharmaceuticals.
However, the TRIPS Agreement does not constitutea uniform law and WTO Members have someflexibility in their implementation of the provisions atnational level. In particular, Article 8 makes aspecific reference to the protection of public healthas one of the elements to be considered whenformulating or amending national laws. In addition,Article 27 contains two health-related possibleexceptions to patentability : "Members may excludefrom patentability inventions, the prevention withintheir territory of the commercial exploitation ofwhich is necessary to protect ... health". This mayalso exclude diagnostic, therapeutic and surgicalmethods for the treatment of humans.
Likewise, under Article 30, Member countries mayprovide several exceptions (such as the so-calledBolar exception), and under Article 31 may estab-lish compulsory licences, for example, based onhealth-related grounds. Under Article 6, parallelimports may also be admitted on the basis of theprinciple of exhaustion of rights.
The possible effects of the changes in pharmaceuti-cal patent protection in the health sector may beseen from different perspectives. The likely impactof the new rules on the prices of medicines hasbeen addressed by a number of studies, under-taken before and after the adoption of the TRIPSAgreement.
General Policy Issues

216
WHO Drug Information Vol. 12, No. 4, 1998
For instance, in the pre-TRIPS period, Nogués (aWorld Bank economist) estimated consumermisallocation in developing countries and found thatthe introduction of pharmaceutical patents wouldentail significant welfare losses for consumers andincome gains for patent owners.
After the adoption of the TRIPS Agreement,Subramanian, an International Monetary Fundeconomist, examined the likely impact of introduc-ing pharmaceutical product patents in small andlarge countries, in cases where either a perfectlycompetitive market or a Nash-Cournot duopolisticmarket becomes a monopoly under patents. Thesame author later applied this model to the particu-lar case of Asian countries, such as India, Indone-sia, Pakistan, the Philippines and Thailand. Heinvestigated annual price, welfare and profit effectsfor these countries consequent upon the TRIPSAgreement. Welfare and price effects were found tobe negative for these countries, though given thetransitional periods provided for by the Agreementand the extensive time required for the approval ofnew medicines, the effects would not be felt imme-diately. The same methodology, when applied toArgentina, also indicated a significant price in-crease of 71% and a fall in consumption of 50%when monopoly follows a competitive situation, and16% and –25% respectively in the duopolistic-monopoly scenario.
There are several methodological problems inestimating the likely impact of changes in patentlaw on pharmaceuticals as a result of the imple-mentation of the TRIPS Agreement since — amongother reasons — there are important differencesfrom country to country in respect to patent laws,the characteristics of the local pharmaceuticalindustry, income levels and patterns of consump-tion. In addition, it is difficult to estimate the marketshare that would be covered by patented products,and estimates on price increases and welfareeffects require assumptions on price elasticity forwhich only scant evidence is available.
Although the results of the various studies under-taken on possible price increases for medicinesvary significantly, there is no doubt that patentslead to prices higher than those prevailing withoutprotection. The generation of monopolistic rents is,in fact, the very purpose and essence of the patentsystem. Hence, while introducing or strengtheningpatent protection, in conformity with the TRIPSAgreement, its possible social effects, particularlyon a low-income population, should be explicitlyand carefully considered.
Finally, from a public policy perspective, the possi-ble effects of changes in patent protection on otheraspects, such as local innovation, foreign directinvestment and transfer of technology, should alsobe assessed. So far, the available evidence indi-cates that, in general, a reinforced and expandedprotection is not likely to increase the local rate ofpharmaceutical research and development or theflow of technology and investments to developingcountries.
Following the adoption of the TRIPS Agreement,the likely impact of introducing pharmaceuticalproduct patents into small and large countries wasexamined by a World Bank economist. Welfare andprice effects were found to be negative in a marketintroducing patent monopoly — such as India,Indonesia, Pakistan, the Philippines or Thailand —although the effects would not be felt immediately.Of course, estimating the likely impact of changesis methodologically problematic since there areimportant differences from country to country and itis difficult to estimate the market share that wouldbe covered by patented products. However, thereis no doubt that patents lead to prices higher thanthose prevailing when patent protection is notenforced.
Health Action International
Dr Zafar Mirza, Association for Rational Use ofMedicines in Pakistan, Islamabad
Health Action International (HAI) believes thatglobal trade liberalization can and does have anegative impact on public health, especially indeveloping countries. Globalization is promoted andprotected by a range of international trade agree-ments, most notably the Uruguay Round of theGeneral Agreement on Tariffs and Trade (GATT)being implemented within the World Trade Organi-zation (WTO). Most, if not all, countries are ex-pected to join the WTO in the coming years. Theadoption of the TRIPS Agreement has significantimplications for pharmaceuticals.
Certainly, the commercial interests of pharmaceuti-cal corporations can complement public healthgoals. But just as importantly, they can conflict. HAIbelieves that national governments must maintainthe ability to regulate trade in the public interest.HAI also believes that WHO has an important rolein assisting countries to comply with trade agree-ments, while protecting public health, and in provid-ing health expertise to the WTO, particularly in thesettlement of trade disputes.
General Policy Issues

217
WHO Drug Information Vol. 12, No. 4, 1998
HAI's public health principles concerning intellectualproperty protection (IPP) are as follows:
• IPP is granted for developing a product or processto provide incentives to make that product orprocess available to the public.
• A patent is not an absolute right or an end in itself;public health is an end in itself.
• IPP for pharmaceuticals should always promoteand be consistent with public health goals.
• Public health goals and commercial interests ofcompanies sometimes coincide and sometimesdiverge. They are not identical. When they con-flict, government should always have the ability tochoose public health as a legitimate reason forlimiting or conditioning commercial interests andrights.
Patents lead to higher drugprices and restrictivenessPatent protection increases the likelihood thatprices for a patented product will be higher, espe-cially if competition is limited. Price data also sug-gest that pharmaceutical corporations often setprices according to what the market can bear, not inorder to recuperate development costs with reason-able profits. Finally, pricing data clearly show thatprices of a patented drug drop quickly and dramati-cally (30%) when the patent expires and a genericequivalent comes onto the market. Moreover, priceis an important determinant of access to necessarydrugs. Whenever patents allow companies to priceany drug out of the reach of those who need it,public health suffers.
Trade agreements do not promote researchand development on diseases prevalent indeveloping countriesOne of the main arguments for strong patents isthat they are necessary for research and develop-ment. However, 75% of the world's population indeveloping countries consume only 14% of theworld's drug supply. Free trade policies and tradeagreements are not addressing the obvious marketfailure to develop and make available affordabledrugs for diseases most prevalent in poorer re-gions, such as tuberculosis, malaria and HIV/AIDS.
Trade agreements dismantle localpharmaceutical industry and limittransfer of technologyThe majority of developing countries have a rela-tively weak pharmaceutical industrial base. After
providing national treatment (NT) to the pharma-ceutical transnational companies, it is doubtful thatthere will be fair competition between local andforeign companies. Furthermore, there is no evi-dence to date documenting a positive impact of theTRIPS Agreement concerning the transfer of tech-nology and foreign direct investment in developingcountries in the pharmaceutical area.
Trade agreements reinforce justificationsfor commercial secrecy to the detriment oftransparency and drug regulationThe positive connection between the rational use ofdrugs and public health is clear, as is the connec-tion between access to adequate drug informationand rational drug use. Therefore, it is disturbing tonote that TRIPS has been used recently to arguethat access to the full clinical trial data wouldbreach the intellectual property rights of an appli-cant for a marketing licence in Europe.
Strategies for complying with tradeagreements while protecting public healthIn debates on trade and public health, it is veryimportant not to lose sight of the realities that (i)countries do have alternatives on how they chooseto comply with agreements and (ii) they have theright to pursue them in their best interests, whichmay conflict with the interests of other countries orcorporations without being illegal under WTO, and(iii) WHO has a mandate to provide Member Stateswith technical assistance, information and adviceon how best to protect and promote health for all,which includes addressing the public health implica-tions of trade policies, legislation, regulations andagreements.
Furthermore, the WTO is only three years old.Countries are still in the process of joining, includ-ing many developing countries. Countries shouldhave impartial technical advice about deciding oncompliance with TRIPS. The number of disputesinvolving public health issues is still limited. In suchcases, the WTO needs to have impartial advicefrom public health experts.
Recommendations at national levelDevelop an effective national drug policy andpromote the adoption of an essential drugs listA noteworthy study of international drug pricingdone in the 1980s showed that the presence ofsuccessful national drug policies was a major factorin lowering drug prices. Furthermore, countries thatadopt essential drugs lists will have a mechanismfor determining what drugs are needed according to
General Policy Issues

218
WHO Drug Information Vol. 12, No. 4, 1998
the disease patterns in their own countries and canbase approvals or government procurement onneed, efficacy and price.
Use compulsory licencesto achieve public health goalsUnder TRIPS, Member Countries have the right toissue compulsory licences on patents based onvarious public health grounds, such as makingessential drugs available at lower cost, subject toseveral safeguards and limitations.
Permit parallel imports of pharmaceuticalsGlobal free trade should include the right to shopglobally for the best prices. Parallel imports areparticularly important for smaller economies thatsuffer from inadequate competition. Where allowed,parallel imports have been shown to be effective inlowering drug prices. A study of the price of anti-HIV drugs in the United Kingdom showed thatparallel imports offer an average saving of 41%from the list price and 30% savings over the bestcontract price.
Ensure that trademark protection does notinterfere with public health policiesProtection of trademark rights should not interferewith sound public health policies to promote thegreater use of generic drugs or to regulate market-ing. It should be clear that countries can requiregeneric drug substitution, substitution by genericname or the printing of the generic name on thepackaging of the product.
Promote the productionand use of generic drugsBioequivalence testing, allowed close to the expira-tion of a patented drug does not violate a patent.Preventing testing until the end of the patent hasthe same effect as granting an extension on thepatent by forcing a delay in the introduction of ageneric, which means extended higher prices forconsumers.
Promote access to drug informationIPP in national legislation or through internationaltrade agreements should not be used to unjustifi-ably maintain corporate control over drug informa-tion. Specifically, access to clinical trial data isnecessary for the public and health care profession-als to make rational decisions on drugs.
Focus on alternatives that promote researchand development for drugs needed locallyPatents are not the only means for promotingresearch and development nor do they ensure thatneeded drugs are brought to market. Trade agree-
ments must be negotiated and interpreted in waysthat will permit the adequate redress of that marketfailure.
Recommendations for WHOPromote WHO input into understanding TRIPSand other trade agreementsWHO, as a UN Agency, is well placed to be anhonest broker in offering guidance, information andadvice to Member States on how to best protectpublic health while implementing trade agreements.For example, WHO has produced a clear andinformative document entitled Globalization andAccess to Drugs: Implications of the WHO/TRIPSAgreement (WHO/DAP/98.9)*, which gives usefulguidance for implementing WTO obligations. Thedocument should be made widely available.
Secure a role in providingexpertise in WTO trade disputesWTO panels are comprised of trade experts thatcan and should benefit from WHO opinion onissues of public health. A few years ago, the UnitedStates challenged Thailand's import restrictionsand strict tobacco advertising ban. In weighing itsdecision, the WTO relied heavily on submissionsfrom WHO and on World Health Assembly resolu-tions.
Public health firstNational governments have a vital role to play inensuring the protection and promotion of publichealth. Although trade agreements limit how theycan regulate trade, governments retain a range ofalternatives they can pursue to maximize publichealth goals in a globalized economy. WHO is wellplaced to advise Member States in these matters.Likewise, WHO is well placed to provide expertiseto the WTO, particularly in the settlement of dis-putes involving health issues.
International Federation ofPharmaceutical ManufacturersAssociations
Dr Harvey Bale, Director-General,International Federation of PharmaceuticalManufacturers Associations (IFPMA),Geneva, Switzerland
The International Federation of PharmaceuticalManufacturers Association (IFPMA) representsover 55 national industry associations from both
* Ed. note: See footnote page 221.
General Policy Issues

219
WHO Drug Information Vol. 12, No. 4, 1998
developed and developing countries. Membercompanies of the IFPMA are major global research-based pharmaceutical companies and companiesproducing a large volume of both generic and non-prescription drugs. We appreciate the efforts of thisworking group and the dedication of WHO and itsstaff to evidence-based decision-making. This is thefirst time that a meeting has taken place whichinvolves WHO Member States, experts and inter-ested parties in a discussion on the health aspectsof trade issues. We trust that our discussions willhave value not only in consideration of the subjectof the debate, but also in establishing a basis forfuture dialogue on the evolving link between publichealth policy and international cooperation on tradeand related matters.
One of the most profound effects of globalization asfar as pharmaceuticals are concerned is that moreresearch will be carried out on a global basis than isthe case today. This is a result of internationalagreements, including TRIPS. Ironically, while thethreat and burden of many diseases have beenglobal, pharmaceutical research efforts have, untilnow, been concentrated in relatively few countries.In the future, TRIPS rules can be expected tospread the burden of research more globally andinvolve local companies and countries which havethus far not been part of the process to discovernew treatments, cures and preventive vaccines.International companies can be expected to in-crease investment and partnership with local com-panies where this has not been possible until nowdue to the lack of patent protection and prevalenceof counterfeiting.
The majority of new medicines are discovered anddeveloped by the research industry. This meansthat industry takes the risk of carrying out multi-yeartests on dose-finding, proper indications and safetyprofile of new chemical and biological compounds,and designing quality assurance systems for themanufacture of the product. All of this takes placebefore the medicine is either approved or rejectedby regulatory authorities. The failure rate is high:only one medicine receives marketing approval outof thousands of compounds screened for therapeu-tic benefit. Only one in five entering clinical trials isapproved for patient use. Given this situation, andthe fact that it takes, on average, ten years fromdiscovery of a compound to delivery to patients, thedrug research and de-velopment process is notonly risky but expensive. In developed countries,the average cost of a new drug today is in theneighbourhood of $500 million. Only a minority of
new drugs are profitable, and it is impossible toknow whether a given compound will be successful.
Because many drugs are relatively inexpensive tocopy, and counterfeiting is even cheaper, it isimportant that strong intellectual property rightsapply to pharmaceuticals and vaccines in bothdeveloped and developing countries. The TRIPSAgreement goes far to assure that new medicineswill be forthcoming to patients in both developedand developing countries. Patient access to effec-tive therapies is lacking today in countless diseasecategories, and new diseases are constantly ap-pearing — twenty or so have been documentedover the past two decades. Meanwhile, resistanceto drugs for older diseases, such as malaria andtuberculosis, is rising. Stronger worldwide patent,trademark and trade secret protection promises toincrease access to new therapies which will ad-dress the incurable diseases of today.
Stronger intellectual property protection applied tothe products of pharmaceutical research should,when applied with vigour at the national level,increase research efforts by local companies whichhave thus far been engaged in copying drugs.There is evidence of this happening where lawshave changed or are anticipated. Further, withpatents protected, global companies will have moreincentives to do research in diseases prevalent indeveloping countries and to license technology.This is not feasible where new compounds arecopied or where counterfeiting prevails. Also,stronger worldwide patent protection will increasethe already strong competitive pressures on com-panies. Patents do not create 20-year "monopo-lies". Instead, companies face old and new com-petition in therapeutic categories and have far lessthan 20 years to exploit their patents.
Beyond these factors, individual companies withnew research capabilities, and which have beenfounded on the patent system, often enter intodiscussion with WHO and governments to providedonations and other collaborative programmes toassist specialized problems such as the recentinitiatives with UNAIDS, or with onchocerciasis,filariasis and trachoma. Objectively, companies withan inclination for these kinds of programmes wouldhave much less incentive to dedicate their re-sources to such programmes if medicines areinternationally diverted through parallel trade —which is a windfall benefit for traders, but a hiddentax on poor countries as well as a regulatory night-mare which can lead to the introduction of sub-
General Policy Issues

220
WHO Drug Information Vol. 12, No. 4, 1998
standard and counterfeit medicines into the drugchain. Common sense dictates that a company willnot want to offer a major concession to a countrythat wishes cheaper drugs, if those drugs are goingto be diverted to wealthier countries through paralleltrade. Parallel trade is inconsistent with publichealth.
What effect will new international agreements haveon local companies and on prices of pharmaceuti-cals? No generalization can ever apply to everysituation but it can be stated that potential concernshere are often not matched by reality. In addition tothe benefits that can be expected from increasedresearch at local level, evidence and the experi-ence of developing countries which have adoptedstronger patent protection over the past decadeindicate that local industry is not made redundant. Astrong local or international generic company needsgood manufacturing quality assurance programmesand the flow of new products coming from strongpatent protection. Local industry needs to worrymore about good manufacturing practices thanpatent protection, because patient safety and globalcompetition dictate higher standards.
Regarding price effect of patent changes, there isempirical evidence that this is very low for a numberof reasons. These relate to the lack of retroactiveapplication of patents, therapeutic competition frompatented and off-patent drugs, the low proportion ofpatented products on the WHO Model List of Es-sential Drugs and in consumption patterns. Accessto medicines is, however, greatly restricted in manycountries by the poor level of public expenditure onhealth care and the lack of adequate infrastructure.
In conclusion, there is much misunderstanding.However, we hope that dialogue with experts andinterested parties will continue over the comingyears. Without decisions based on dialogue, bothindustry's ability to service public health and publichealth itself, could suffer.
International GenericPharmaceutical Alliance
Mr G. Perry, Director, European GenericMedicines Association, Brussels, Belgium
The International Generic Pharmaceutical Alliance(IGPA) was established in 1997 and representsgeneric industry associations from Europe, theUnited States and Canada. The Organization isalso considering granting observer status to local
associations and companies from Africa, Asia andLatin America.
IGPA's principal objective is to promote affordablequality pharmaceutical care for all consumers. Morespecifically it:
• Supports the development of the international andregional policies which seek to ensure access tomedicinal care for all consumers.
• Promotes balanced and generic-friendly intellec-tual property laws in the pharmaceutical sectorthat ensure timely access to the market forgeneric products.
• Encourages the scientific development and pro-fessional awareness and general knowledge ofgeneric medicines.
• Promotes the global harmonization of regulationsrelated to generic products.
• Provides guidance to international organizationsand national governments in improving regulatoryand legal expertise relating to the regulation andmarketing of generic products.
• Promotes uniform and effective GMP standardsand quality control for generic pharmaceuticalsand APIs.
• Seeks strict and effective control to prevent theproduction and trade of counterfeit versions oforiginal and generic products.
• Supports the development of competition in thepharmaceutical sector.
IGPA believes that all pharmaceutical and healthlegislation worldwide should have the protection ofpublic health as its primary aim. However, this doesnot mean that this is the only aim of a global phar-maceutical policy. Encouraging innovation, ensur-ing affordability and access to medicines, andreducing barriers to trade in pharmaceuticals arealso aims that need to be promoted to ensureeffective care for patients. In order to promote theseaims, there needs to be a balanced approach,which takes into account various, and often conflict-ing, interests. The need for a balanced approach isparticularly important in the area of intellectualproperty of pharmaceuticals.
Intellectual property rights clearly contribute to thedevelopment of new pharmaceutical products. The
General Policy Issues

221
WHO Drug Information Vol. 12, No. 4, 1998
TRIPS Agreement will enable innovators of phar-maceuticals to benefit from substantial improve-ments in protection. The increased financial stabilityand rewards should lead to new revenues for newinnovations in the future.
However, one of the basic principles of intellectualproperty protection is that patents are limited innature and that the invention, after a period ofmarket protection, is placed in the public domain. Inthe pharmaceutical sector, the end of patent protec-tion leads to the development and marketing ofgeneric or multi-source versions of the originalbrand. This is important for (i) ensuring lower-pricedmedicines, (ii) encouraging competition in thepharmaceutical sector, and (iii) providing room innational or personal budgets to pay for more expen-sive new products.
Even in advanced countries, generic medicines canaccount for up to 40–60% of the pharmaceuticalmarket in volume. In the case of developing coun-tries, the creation of an off-patent market alsoopens opportunities for the development of localpharmaceutical industries that can help reduceeconomic dependence on advanced countries.
To date, however, most of the discussion on TRIPShas focused on how the provisions must be imple-mented to support intellectual property rights. Therehas been little guidance concerning the agreedlimitations of TRIPS. Similarly, there has been littleemphasis given to the balance of interests and therights of third parties which the TRIPS agreement isexpected to embrace.
The development of generic medicines is one of theimportant balances to be ensured in any analysis ofpharmaceutical intellectual property policy. Twomajor instruments exist within TRIPS to promotethis: (i) a system of compulsory licences, and (ii) asystem that permits development and registration ofgeneric products in advance of patent expiry so asto enable the products to enter the market immedi-ately after the end of patent expiry. Within theTRIPS Agreement, provision is made for thesepolicies. For example, Article 30 provides for theadvance development and registration of genericmedicines. Legislation in Australia, Canada, Hun-gary, Israel and the United States of Americaprovides for these activities. The situation in theEuropean Union is currently under discussion.
There is clearly a need for greater guidance anddiscussion on the limitations of TRIPS. The WHOinitiative in this area is therefore welcome. Thedocument entitled Globalization and Access toDrugs: Implications of the WHO/TRIPS Agreement(WHO/DAP/98.9)* is an example of how WHO canassist its Member States. In particular, the docu-ment highlights the importance of Article 30.
* Ed. note: Globalization and Access to Drugs – Implica-tions of the WHO/TRIPS Agreement", is classified as atechnical document in the general distribution category. Itis not a formal publication of WHO.
In the light of views expressed subsequent to thedocument being issued, it has been decided to revise andre-issue it. The target release date is December 1998,subject to final review being completed, and will beavailable from the Action Programme on Essential Drugs,World Health Organization, 1211 Geneva 27, Switzerland.
General Policy Issues

222
WHO Drug Information Vol. 12, No. 4, 1998
Reports on Individual Drugs
The life-threatening risksof therapy substitutionWhen a pharmaceutical product is withdrawn fromthe market for safety reasons, it is normal topropose a replacement therapy and to give adviceand instructions on substitution of a similarproduct. However, as recently demonstrated follow-ing the withdrawal of mibefradil (Posicor®), achange in treatment can sometimes prove to belife-threatening.
In mid-1997, mibefradil was introduced as a newnondihydropyridine calcium channel blocker for themanagement of hypertension and chronic stableangina. The drug was long-acting, with a half-life ofbetween 17 and 25 hours, blocking both the T-type(transient) and the L-type (long-acting) calciumchannels (1, 2). Because other available calciumchannel blockers acted upon the L-type channelonly, mibefradil was unique in terms of mechanismof action, although the rationale for this character-istic remains less well documented (3). As a resultof this selective T-type calcium channel blockeractivity, mibefradil was classified as a new categoryof calcium antagonist in the expectation that itwould hold advantage over older calcium channelblockers.
In June 1998, following reports of serious interac-tions with some 25 commonly used drugs, themanufacturer voluntarily withdrew mibefradil fromsome 38 countries worldwide (4). Since mibefradilwas not demonstrated to offer specific benefits overother drugs in the same therapeutic category, itscomplicated drug interaction profile was assessedto be an unreasonable risk to patients. The manu-facturer urged physicians to contact patients,discontinue treatment and arrange an alternativetherapy (5).
However, upon introduction of alternative therapy,some new and unexpected life-threatening reac-tions occurred (2). Four cases of cardiogenic shockin patients previously taking mibefradil and beta-adrenoreceptor antagonists were reported after achange to substitute dihydropyridine calcium chan-nel blockers (nifedipine, felodipine or nisoldipine).
One case resulted in death, and the other threecases required intensive care.
The long half-life of mibefradil may explain thesesevere reactions (2). It has been proposed that aprolonged wash-out period lasting from three daysto two weeks after mibefradil discontinuation maybe necessary before other hypertensives such asbeta-adrenoreceptor antagonists and other calciumchannel blockers can be introduced. The manufac-turer has now issued amended instructions forinitiating substitution therapy (see page 237).
It is often the case that postmarketing surveillanceof a new drug will disclose previously unexpectedadverse drug reactions or interactions. However,any subsequent withdrawal of the product andrecommendations for substitution therapy alsorequire careful and considerable reflection.
References
1. Mibefradil: a new calcium channel blocker. MedicalLetter, 39: 103–105 (1997).
2. Mullins, M.E., Horowitz, Z., Linden, D.H.J. et al. Life-threatening interaction of mibefradil and beta-blockerswith dihydropyridine calcium channel blockers. Journal ofthe American Medical Association, 280: 157–158 (1998).
3. Po, A.L.W, Zhang, W.Y. What lessons can be learntfrom withdrawal of mibefradil from the market? Lancet,351: 1829–1830 (1998).
4. WHO Drug Information, 12(3): 145 (1998)
5. Dear Doctor letter from Roche Laboratories, 8 June1998.
Revision of HIV treatmentguidelinesWhen the British HIV-1 Association (BHIVA) guide-lines on antiretroviral treatment of HIV-positiveindividuals were first published in April 1997 (1), itwas already acknowledged that they would requireupdating on a regular basis given the rapid devel-opment of HIV therapies.

223
WHO Drug Information Vol. 12, No. 4, 1998
As more experience is gained and newly docu-mented evidence becomes available, treatmentregimens undergo modification. In this respect, datafrom two large clinical endpoint studies have re-cently been presented which demonstrate superiorclinical benefit in the use of triple combinationtherapy compared to dual combination therapy inHIV-positive individuals who have either beentreated with zidovudine or are treatment naive.
The revised criteria for initiation of antiretroviraltherapy in HIV-infected adults, as presented in thelatest BHIVA guidelines (2) are the following:
Therapy should be initiated:When the patient agrees to treatment;When benefit outweights the possible risks oftherapy;When the CD4 count is >350 cells/ml;When the viral load value is associated with risk ofdisease progression.
Therapy should consist of:<50 000 RNA copies/ml: two nucleoside analoguesplus a non-nucleoside reverse transcriptase inhibi-tor or HIV protease inhibitor.>50 000 RNA copies/ml: two nucleoside analoguesplus one or two HIV protease inhibitors.
The aim of therapy in treatment-naive patientswill be:To reduce plasma viral load to less than 400–500copies/ml (and preferably <50 copies/ml) by 24weeks of therapy.To improve and extend the length and quality of life.
In July 1998, the International AIDS Society — USAPanel has also updated its recommendations forantiretroviral therapy in HIV infection to bring themin line with currently available information (3). ThePanel reviewed clinical and basic scientific studies,information from phase III clinical trials, and clinical,virological and immunological endpoint data. It alsoevaluated presentations made at research confer-ences. The Panel concluded that, overall, thesedata continue to support early introduction of potentantiretroviral therapy in patients with HIV infection.The variety of combination regimens which nowdemonstrate potency will allow a wider choice wheninitiating therapy.
The Panel recognized the important contribution ofplasma HIV RNA assays of increased sensitivity inmonitoring the therapeutic response. However,more data are needed to determine precisely theHIV RNA levels that indicate treatment failure.
With sustained monitoring, it will be possible toevaluate the long-term implications and prolongeduse of HIV regimens and determine future dosages.Adverse reactions to HIV protease inhibitors re-ported so far include hyperglycaemia, hyperlipidae-mia, peripheral fat redistribution (lipodystrophy) andvisceral fat accumulation. Thus, the optimal long-term treatment approaches to management of HIVstill need to be defined.
References
1. WHO Drug Information, 11(3): 134 (1997).
2. 1998 revision to the British HIV Association guidelinesfor antiretroviral treatment of HIV seropositive individuals.Lancet, 352: 314–316 (1998).
3. Antiretroviral therapy for HIV infection in 1998. Journalof the American Medical Association, 280: 78–86 (1998).
Levonorgestrel foremergency contraceptionThe most commonly used emergency contraceptionuntil now, the Yuzpe method, was developed in theearly 1980s. It is based on a modified regimen ofcombined oral contraceptive pills containingethinylestradiol 100 µg plus levonorgestrel 0.5 mgor dl-norgestrel 1.0 mg, repeated 12 hours later.This regimen prevents about 75% of pregnanciesthat would have occurred without this treatment.However, about 50% of treated women reportnausea and more than 20% vomiting. There is thusa need for a more effective and better toleratedmethod.
Researchers working with the UNDP/UNFPA/WHO/World Bank Special Programme of Research,Development and Research Training in HumanReproduction (HRP) confirm that the use of levo-norgestrel alone for emergency contraception ismore effective and produces side effects in consid-erably fewer users than the Yuzpe regimen (1)
Levonorgestrel is a synthetic derivative of thehormone progesterone. It is one of two activecompounds present in combined oral contraceptivepills. In the regimen proposed for emergency con-traception, two pills each containing 0.75 mg oflevonorgestrel were administered at an interval of12 hours. In a single WHO-supported study carriedout in Hong Kong, levonorgestrel was slightly butnot significantly more effective than the Yuzperegimen in preventing pregnancy. In particular, the
Reports on Individual Drugs

224
WHO Drug Information Vol. 12, No. 4, 1998
proportion of women experiencing vomiting was2.7% with levonorgestrel compared to 22.4% withthe Yuzpe regimen.
A double-blind randomized trial in 21 centres world-wide was subsequently designed to compare thetwo regimens in women, administered within 72hours of unprotected sexual intercourse. Among the1998 women who took part in the double-blindrandomized trial, the crude pregnancy rate was1.1% (95% CI: 0.6–2.0) in the levonorgestrel groupcompared to 3.2% (95% CI: 2.2–4.5) in the Yuzperegimen group. The proportion of pregnanciesprevented compared to the expected numberwithout treatment was 85% with the levonorgestrelregimen and 57% with the Yuzpe regimen. Theefficacy of both treatments was significantly andinversely related to time since unprotected coitus(p=0.01). The sooner treatment is initiated, thebetter it works.
The levonorgestrel regimen was more efficaciousand better tolerated than the Yuzpe regimen.Women in both groups reported the same sideeffects: nausea, vomiting, dizziness, fatigue, head-ache, breast tenderness and lower abdominal pain.However, for each of these side effects, women inthe levonorgestrel group reported them less fre-quently (2).
Replacement of the Yuzpe method with levonor-gestrel should improve the acceptability and effi-cacy of hormonal emergency contraception. Familyplanning programmes may wish to consider makinga change based on these findings.
References
1. Task Force on Postovulatory Methods of FertilityRegulation. Randomized controlled trial of levonorgestrelversus the Yuzpe regimen of combined oral contracep-tives for emergency contraception. Lancet, 352: 428–433(1998).
2. WHO Press Release, WHO/58, 7 August 1998.
Cancer risk in women exposed todiethylstilbestrol in uteroDiethylstilbestrol (DES) was commonly used before1970 for the prevention of spontaneous abortionand premature delivery. Several million pregnantwomen in the United States of America and Europewere exposed to DES before a strong associationwas reported in 1971 between use of the drug in
pregnancy and the occurrence of clear cell adeno-carcinoma in exposed female offspring (1).
In the mid-1970s, several cohorts of DES-exposeddaughters and unexposed comparison groups werefollowed for the occurrence of cancer, precursorlesions and reproductive side effects. The result ofDES exposure on male offspring is still unknown.Animal studies have suggested an increased risk oftesticular cancer, but results in case-control studieshave been inconsistent (2).
Some 30% of girls exposed in utero to DES presenta cervical vaginal adenosis and concern has arisenthat DES may also result in a higher risk of breastcancer (3). A study has been carried out of breastand other cancers in women exposed in utero toDES by combining the previously identified cohortsand extending the follow-up from 1978 to 1994.A total of 4536 DES-exposed daughters (68110person years) and 1544 nonexposed women(22 599 person years) were identified. The rateratio for breast cancer was 1.18 (95% CI, 0.56–2.49) and adjustment for known risk factors did notalter this result. Similarly, there was no increasedrisk for all cancers or for individual cancer sites,except for clear cell adenocarcinoma of the vaginaand cervix.
Three cases of vaginal clear cell adenocarcinomaoccurred among the exposed daughters, resultingin a standardized incidence ratio of 40.7 (95% CI,13.1–126.2) in comparison with population-basedincidence rates. All these cases occurred among29 111 person years accumulated by the cohort upto 29 years of age. The authors of this study con-cluded that since the majority of women werecurrently under 50 years of age, it is still importantto continue to monitor cancer risk as the cohortages into the menopausal years.
References
1. Herbst, A.L., Ulfelder, H., Poskanzer, D.C. et al.Adenocarcinoma of the vagina: association of maternalstilbestrol therapy with tumor appearance in youngwomen. New England Journal of Medicine, 284: 878–881(1971).
2. Guisti, R.M., Iwamoto, K. Hatch, E.E. et al. Diethyl-stilbestrol revisited: a review of the long-term healtheffects. Annals of Internal Medicine, 122: 778–788 (1995).
3. Hatch, E.E., Palmer, J.R., Titus-Ernstoff, L. et al.Cancer risk in women exposed to diethylstilbestrol inutero. Journal of the American Medical Association, 280:630–634 (1998).
Reports on Individual Drugs

225
WHO Drug Information Vol. 12, No. 4, 1998
Zidovudine for mother-to-childtransmission of HIVMother-to-child transmission of HIV infection is amajor factor in child health and survival. The aver-age rate of vertical HIV transmission is around25%, but rates differ significantly between coun-tries. These may vary from 14% in Europe to 45%in sub-Saharan Africa. Breastfeeding may beresponsible for the higher rates in developingcountries.
Many antiretroviral drugs have been developed totreat HIV infection and the use of zidovudine toreduce vertical transmission is now standard prac-tice in many countries, with a consequent reductionin perinatally acquired HIV. A clinical trial in Thai-
Table 1. WHO recommended short course zidovudine (ZDV) regimento reduce mother-to-child transmission – possible schedule
Action 1st visit 2nd visit 3rd visit 4th visit delivery and16 weeks 24–28 weeks 34–36 weeks antenatal care postnatal care
Screen for observe, Assess Assess Assessrisk factors score
Screen and anaemia, blood anaemia anaemia anaemiatreat/HIV pressure, rapid blood pressure blood pressure blood pressuretesting plasma reagin HIV testing
HIV pretest/counsel
Prophylaxis *mebendazole *antimalarial *antimalarial *antimalarial intensive treat-*iron + folate * iron + folate * iron + folate * iron + folate ment with oral*tetanus toxoid *tetanus toxoid zidovudine,
oral zidovudine 300 mg twice a 300 mg everyday from 36 weeks until delivery 3 h of labour-
delivery
Individual where to give birth test results and infant feeding birth plan support forcounselling results of rapid counselling - if HIV positive, decision on infant decision on
plasma reagin refer to support consent for feeding infant feedinginform of voluntary groups/services ZDV therapy compliance withconfidential testing regimen
Inform obtain clean how to prepare if home delivery receive clean refer HIV+delivery kit for birth and plan plan steps delivery kit mothers forhow to seek care for emergency care/support
Plan for next visit/routine next visit/routine follow-up after family planningfollow up * bring partner birth. child *partner
immunization counselling
* as necessary
land using zidovudine twice daily from 36 weeksgestation until delivery in women who did notbreastfeed showed a 51% reduction in transmissionrisk (1). WHO recommends the regimen used inthis study for settings where practical and budget-ary considerations preclude the use of zidovudineor other therapies for longer periods.
The following important issues should be consid-ered before implementing antiretroviral therapy forprevention of vertical transmission (2):
• It is important to improve access to and quality ofservices and to assure adequate and functioningantenatal care. Health care workers will requireadditional training in the administration of anti-HIVtherapies.
Reports on Individual Drugs
226
WHO Drug Information Vol. 12, No. 4, 1998
• Voluntary confidential counselling and testing arethe cornerstones of an HIV care service. When-ever possible, partners should also be counselledand offered voluntary confidential testing.
• A system for distribution and supply of antiretro-viral therapy and breastmilk substitutes must beorganized. Regular supply, secure storage,distribution and accounting need to be organized.Zidovudine (ZDV) is now included in the WHOModel List of Essential Drugs. The regimen is setout in table 1.
• Upon introduction of antiretroviral therapy, moni-toring and evaluation of safety and efficacy shouldbe in place. Factors of operation and efficacyshould also be addressed.
The successful implementation of an antiretroviralregimen and a decrease in vertical transmission will
depend on the number of women consenting totesting and returning for the results, on the simplic-ity of the regimen, and the ease with which they canreturn for follow-up. Further information concerningthe implementation of anti-HIV therapy is availablefrom WHO and UNAIDS.
References
1. Centers for Disease Control and Prevention. Adminis-tration of zidovudine during late pregnancy to preventperinatal HIV transmission — Thailand 1996–1998.Morbidity and Mortality Weekly Report, 47: 151–153(1998).
2. World Health Organization. Recommendations on thesafe and effective use of short-course ZDV for preventionof mother-to-child transmission of HIV. Weekly Epidemio-logical Record, 73: 313-320 (1998).
Reports on Individual Drugs
Malaria Researchers!
Letters of interest are invited from researchers conducting projectson the discovery and development of drugs against malaria
Pleast contact:MMV/TDR
World Health OrganizationCH 1211 Geneva 27, Switzerland
e-mail: [email protected]: 41 22 791 4854
227
WHO Drug Information Vol. 12, No. 4, 1998
General Information
Recommendations from the ExpertCommittee on Drug DependenceEfforts to provide an international legal frameworkfor the control of psychoactive drugs have resultedin the formulation of the 1961 Single Convention onNarcotic Drugs and the 1971 Convention on Psy-chotropic Substances. Both are major achieve-ments in the development of coordinated interna-tional control of dependence-producing drugs. Theinternational drug control treaties are instrumentswhich provide a framework for the regulation of anumber of defined narcotic drugs and psychotropicsubstances, the most dangerous of which areeliminated from use. Those that are potentiallybeneficial are subjected to controls in production,manufacture, trade and distribution so that their usecan be limited exclusively to scientific or medicalpurposes. Details of the scheduling are set out inthe table on page 228.
Each Convention embodies a policy and indicatesthe type of legislation and drug regulatory control tobe administered. These controls are intended toensure the availability for legitimate use of thecontrolled substances and prevent their abuse. TheConventions assign to WHO the responsibility forrecommending their placement in the appropriateschedules for control purposes and proposingamendments to such schedules. The WHO ExpertCommittee on Drug Dependence is charged withassessing the dependence liability and therapeuticusefulness of each substance. Following evaluationof the seriousness of the public health and socialproblems related to possible abuse, WHO makes arecommendation to the Commission on NarcoticDrugs.
At the thirty-first meeting of the WHO Expert Com-mittee on Drug Dependence held in June 1998 anumber of dependence-producing psychoactivesubstances were reviewed in order to decide ontheir public health impact and status in relation tothe Conventions. The following substances wererecommended for scheduling or review.
Dihydroetorphine is a potent µ-opioid receptoragonist. Approved for marketing in China for therelief of acute severe pain, it is currently a con-
trolled drug in that country. Based on its pharmaco-logical properties and high dependence potential,the Expert Committee estimates that it is equivalentin abuse potential and effects to other drugs al-ready placed in Schedule I of the 1961 SingleConvention on Narcotic Drugs.
Remifentanil is a selective µ-opioid receptor ago-nist with an ultra-short duration of action which hasbeen approved for marketing in 17 countries. It isused medically as an analgesic for induction andmaintenance of general anaesthesia, for continua-tion of anaesthesia into the immediate postopera-tive period under the direct supervision of ananaesthetist or in an intensive care setting, or as ananalgesic component of monitored anaesthesiacare.
In terms of review criteria under the 1961 Conven-tion, opioids are calibrated and ranked againstmorphine to determine abuse potential. Based onthe pharmacological properties and dependencepotential of remifentanil, the Committee agreed thatabuse liability and the ill-effects profile are similar tothose of drugs placed on Schedule I of the Conven-tion. It was therefore recommended thatremifentanil be placed in Schedule I.
With regard to recommendations for schedulingunder the 1971 Convention on Psychotropic Sub-stances, the Committee reviewed the current statusof ephedrine use and abuse. The public health andsocial problems associated with the abuse ofephedrine appear to be significant, particularly incertain African countries. It was therefore recom-mended that l-ephedrine and the racemate beplaced in Schedule IV of the 1971 Convention.The d-isomer is significantly less potent than thel-isomer.
In making this recommendation, the Committeenoted that combination products containing ephe-drine may be eligible for exemption from schedulingunder the terms of the 1971 Convention.
A proposal was submitted to the Committee con-cerning the scheduling of isomers, esters, ethersand pharmacological analogues of the psychotropicsubstances currently controlled in Schedules I andII of the 1971 Convention. With regard to the sched-

228
WHO Drug Information Vol. 12, No. 4, 1998
Conventions, schedules and controlled substances*
The 1961 Single Convention on Narcotic Drugs
Schedule I Common opioid analgesics, coca all specified controls on manufacture,alkaloids, cannabis trade, distribution, storage, record-
keeping and reporting
Schedule II Codeine and similar drugs less addictive less strict controls on tradethan in Schedule I and retail distribution
Schedule III Specified preparations containing limited exempt from some controlquantities of drugs in Schedule I and II measures such as
prescription requirements
Schedule IV Some Schedule I drugs which are in addition to all specified controls,particularly addictive, e.g. heroin prohibition recommended
Special Opium and opium poppy, poppy straw, cultivation controls and otherMeasures coca bush and cannabis plant special measures
The 1971 Convention on Psychotropic Substances
Schedule I Hallucinogens and stimulants with no very strict controls, e.g. specialmedical use, e.g. LSD, Ecstasy authorization for research use
Schedule II Addictive psychotropic drugs with limited similar controls to narcoticmedical use, e.g. amphetamines. drugs in Schedule I
Schedule III Addictive psychotropic drugs in common less strict controls on manufacture,medical use, e.g. barbiturates trade, distribution, storage,
record-keeping and reporting
Schedule IV Less addictive psychotropic drugs, less strict controls than Schedule IIIe.g. benzodiazepines, anorectic drugs re trade and record-keeping. Pre-
scription still required unless specificallyexempted by national authorities.
uling of analogues, which are understood as "anymodified chemical compounds producing effectssimilar to those produced by the original sub-stances", the Committee agreed that extendingcontrols to these groups could contradict the sched-uling procedure stipulated in the 1971 Conventionwhich requires WHO to evaluate substances indi-vidually.
Furthermore, the lack of specificity of such groupdesignations may lead to disagreement among theparties concerning the precise scope of the controlprocedures. The same concerns apply to estersand ethers: though difficult to evaluate, their controlcould have a negative impact on legitimate indus-
trial and research activities. The Committee pro-posed that criminal activities involving analoguesshould be controlled at country level by applyingselective controls.
With regard to the scheduling of isomers, it wasrecommended that the addition of the prefix"stereo" should be made in the following phraseregarding the substances to be included in Sched-ule I of the 1971 Convention.
"The stereo-isomers, except where expresslyexcluded, of psychotropic substances in this Sched-ule whenever the existence of such stereo-isomersis possible within the specific chemical nomencla-ture in this Schedule."
* Scheduling criteria for the Single Convention on Narcotic Drugs, 1961 and the Convention on Psychotropic Substances,1971 are given in the 29th Report of the Expert Committee on Drug Dependence, WHO Technical Report Series, No. 856,World Health Organization, Geneva. Information concerning obligations of the parties, controls and exceptions relatingto the Conventions is available in: Single Convention on Narcotic Drugs, 1961. United Nations, V.93-88216 (1993) andConvention on Psychotropic Substances, 1971. United Nations, V.93-88220 (1993).
General Information

229
WHO Drug Information Vol. 12, No. 4, 1998
This addition will render the proposal more consist-ent with the current interpretation of the Schedules,and clarify the scope of controlled isomers includingracemates. Nonetheless, interpretation guidelinesmay need to be developed by an appropriateinternational body such as the INCB in collaborationwith WHO for those stereo-isomers appearing inSchedules II, III and IV.
The Committee also discussed the following sub-stances to determine the need for their futurereview. Recent literature suggests that somesubstances in the benzodiazepine group may bemore liable to abuse than others. This has beendocumented, in particular, with flunitrazepam,diazepam and the injectable dosage forms oftemazepam. Diazepam has been shown to have anabuse liability comparable to that of pentobarbitalwhich is currently in Schedule III. Of the threebenzodiazepines, flunitrazepam has already beenplaced in Schedule III and, in the case oftemazepam, the higher abuse liability will only applyto the injectable preparation, which is not easilyavailable. Thus diazepam alone meets the criterionfor critical review.
Smoking tobacco is dependence-producing andcauses grave public health consequences. It has nomedical use. Although new information indicatesthat health risks are greater than previouslythought, tobacco would not meet the schedulingcriteria under the existing international drug controltreaties. Furthermore, once it is scheduled, totalprohibition would be the only control measureapplicable to tobacco because the regulated supplyof controlled substances is not allowed for non-medical and non-scientific purposes. A new con-vention such as the International Framework Con-vention for Tobacco Control would thus have to bedeveloped.
Gamma hydroxybutyric acid (GHB) is a metabo-lite of gamma aminobutyric acid (GABA) which isfound in the human brain. GHB is used in severalcountries in Europe as an anaesthetic and haspotential usefulness for the treatment of narcolepsyand drug abuse disorders. GHB is manufacturedusing a relatively simple synthesis and inexpensivestarting materials.
Although GHB gained early favour with healthenthusiasts in the USA as a natural food supple-ment, the medical community reported cases ofoverdosage and abuse. GHB has been reported tocause drowsiness, dizziness, nausea, visual distur-
bances, unconsciousness, hypotension, brady-cardia, seizures, severe respiratory depression andcoma. A withdrawal syndrome has been describedfollowing discontinuation after long-term use.Severe cases of overdosage have required emer-gency treatment, including intensive care. Althoughresults from preclinical studies did not predict highabuse liability, this seems to be increasing in theUSA and some European countries. Similarly, achemical derivative, gamma butyrolactone (GBL),is also being abused. The Expert Committee rec-ommended that more information on abuse of GHBand GBL should be gathered and that a criticalreview should be made.
4-bromo-2,5-dimethoxyphenethylamine (2C-B) isa centrally active hallucinogenic substance. It isstructurally and pharmacologically similar tophenethylamine hallucinogens. Although it is foundin circulation in several countries, it is not registeredfor marketing in any. The ease of clandestinesynthesis and popularity as a claimed sexual en-hancer are likely to encourage its production andabuse. For this reason, the Expert Committeerecommended 2C-B for critical review.
Although no data exists indicating significant abuseof N-methyl-1-(3,4-methylenedioxyphenyl)-2-butanamine (MBDB), it is structurally and pharma-cologically similar to MDMA and N-ethyl-MDA.MBDB has been found in circulation in more than10 countries in Europe, Asia and America. There isthus a strong likelihood that MBDB will become asubstance of abuse and will lead to similar publichealth problems as MDMA. The Expert Committeerecommended that a review should be carried out.
Although rodent data would suggest that zolpidemmay have less abuse potential than benzodi-azepines, human studies do not support this. Ingeneral, when contradictory findings exist betweenanimal and human studies, the latter should takeprecedence. There have been no reports of illicitactivities concerning zolpidem, and spontaneousreports from countries within Europe have includedfew adverse effects. Although cases of a discon-tinuation syndrome have also been reported, thesedo not appear serious enough to justify internationalcontrol. However, these cases, which were very fewat the time of the previous meeting of the ExpertCommittee in 1996, have increased significantlyand the Committee recommended that data shouldbe gathered for appraisal at the next meeting.Critical review of zolpidem was recommended.
General Information

230
WHO Drug Information Vol. 12, No. 4, 1998
Insulin: availability, affordability,and harmonization
Hilary KingNoncommunicable Diseases,World Health Organization, Geneva
Insulin is a hormone produced by the beta-cells ofthe pancreas. In subjects with diabetes mellitus,insulin production is partly or wholly interrupted, asa result of beta-cell destruction (the type-1 proc-ess), or one or several defects in insulin secretion—almost always with a major contribution frominsulin resistance (the type-2 process) (1). In theformer case, a continuous supply of insulin isusually required for survival. In the latter, it may berequired for adequate metabolic control. This willprevent or delay the long-term complications ofdiabetes, such as blindness, kidney failure, neu-ropathy, and infection and gangrene of the lowerlimbs.
Patients who require insulin must take it by injec-tion, which is normally self-administered one ormore times each day. Traditionally, porcine orbovine insulin has been used for human patients.Today, recombinant DNA techniques are used toproduce biosynthetic human insulin. Insulin isavailable in a variety of strengths, of which IU100(100 international units per ml) and IU40 (40 inter-national units per ml) are the most frequently used.
A brief examination of the use of insulin in the worldreveals a marked disparity between developed anddeveloping countries, with a more than fourfolddifference in the percentage of diabetic subjectswho are treated with insulin (Table 1). This may notentirely be accounted for by differences in the
incidence and prevalence of type-1 diabetes (Table2). This article examines some of the factors whichhave brought about this inequity, most of whichcould be overcome by appropriate interventions, aswell as some other issues relating to insulin use.
AvailabilityIt is useful to distinguish between acute and chronicshortages of insulin, since these have differentcauses, and potential remedies (2).
Acute shortagesThese can occur in any country as a result of civilunrest or natural disasters such as earthquakes,floods, or fire, as well as the financial crises experi-enced by countries in economic transition. Therehave been recent examples in which the availabilityof insulin and other aspects of diabetic care havebeen studied and reported.
During the war in Croatia, local industry was ableto maintain adequate supplies of insulin, but equip-ment for monitoring metabolic control — withoutwhich insulin treatment may be ineffective — was inshort supply (3). Fortunately, the WHO collaborat-ing centre for diabetes in Zagreb had numerousinternational contacts and these provided thenecessary assistance.
Following the 1996 earthquake in Kobe, Japan, theneeds of people with diabetes received the atten-tion of the rescuing authorities once emergencytreatment of trauma victims was accomplished (4).Despite this, poor metabolic control due to suspen-sion of treatment caused by the destruction oftreatment facilities and lack of drugs and equipmentwas frequently reported and the incidence of dia-betic complications rose.
Table 1. Worldwide use of insulin (8, 23)
Region Population Insulin used Insulin/ Number Number % treated(million) (units/year) person/year diabetic treated with with insulin
(million) insulin (million)
Developed 900 105 000 120 55 7 13 countriesDeveloping 4600 45 000 10 100 3 3 countries
World 5500 150 000 30 155 10 6
General Information

231
WHO Drug Information Vol. 12, No. 4, 1998
The most effective way of dealing with acute short-ages is to be prepared. Similar supplies to thosewhich are normally used in the community shouldbe provided in terms of insulin species andstrength. Provision of ancillary equipment, such asappropriate syringes and needles, needed toensure effective insulin delivery should not beoverlooked. Major insulin manufacturers, in col-laboration with the International Diabetes Federa-tion, are natural partners in combating such acuteshortages. They have developed a plan for deliver-ing insulin supplies in emergency situations,whereby the manufacturer will provide up to threemonths supply, if the existing distribution networksare operational (5).
Chronic shortagesIn terms of the number of persons affected, chronicshortages are the most widespread and serious.They are mainly confined to the world’s poor coun-tries. Table 2 illustrates the great disparity in insulinuse between countries, and suggests a strongassociation with the level of socioeconomic devel-opment. The 400-fold difference between Indone-sia and the USA is striking, and would suggest thatfew of those who need insulin in Indonesia arereceiving it.
Chronic shortages of insulin may arise due tofailure of procurement, ineffective distribution,inadequate storage systems or simply lack offinance in the health sector. In many developingcountries, insulin may be found in urban centres,albeit at a high price, but not at all in rural areas,due to the absence of a distribution system. Philan-thropic organizations, as well as the major manu-facturers, have helped alleviate shortages in somecountries (6). Such donations can save lives, but
they represent temporary solutions. In order toachieve self-sufficiency, reorganization of the healthcare system and revised prioritization is required.Bearing in mind the rapid rise in the number ofpersons affected by diabetes in the developingworld (7), there is an urgent need to develop na-tional diabetes programmes, whereby insulin andother essential supplies are provided to all those inneed (8). At present, many thousands, perhapsmillions, of people still suffer because of an inad-equate supply of insulin.
AffordabilityThe cost of insulin is not uniform around the world.In general, it is most cheaply available in the largestmarkets, because of economies of scale and thepower of negotiation of the authorities when offeringlarge tenders. Some countries impose taxes oninsulin, which are passed on to the consumer andmay serve to raise the cost substantially. If ad-equate supplies are not available through thegovernment health sector, patients may be forcedto seek insulin though commercial retailers. Inaddition, there is variability in the price demandedby the major manufacturers. Recently, four compa-nies were asked to quote for the supply of 10-mlvials of IU40 bovine and porcine insulin to threedestinations — Jakarta, Indonesia, Ndjamena,Chad, and La Paz, Bolivia. Three companies of-fered prices in the range US$ 2.10–US$3.80 forbovine insulin and US$ 3.00–US$ 4.57 for porcineinsulin, whilst a fourth company quoted US$5.00 ineach case (9).
Furthermore, per capita income is much lower indeveloping countries, so that those who can leastafford medication are often faced with the highestexpense. Ensuring an adequate supply of insulin
Table 2. Estimated prevalence of type-1 diabetesand use of insulin in selected countries (24–25)
Country Estimated prevalence Units of insulin used(in order of prevalence) of type-1 diabetes per inhabitant per year
per 100 000 population
Bangladesh 2 1China 6 1–2Indonesia 10 0.5Japan 31 40Malaysia 46 20India 65 4United States of America 301 200Australia 370 100
General Information

232
WHO Drug Information Vol. 12, No. 4, 1998
can consume a large proportion of a family incomein such circumstances. Difficult decisions regardingfamily expenditure inevitably arise. Some patientsresort to buying a vial of insulin, or even a singleinjection, only when they feel particularly unwell.Such treatment is obviously of very little benefit interms of long-term outcome. Ignorance may alsolead to the unnecessary prescription of insulin tothose who might be adequately controlled by otherand cheaper means, such as oral agents, or dietand exercise regimes. Thus, the insulin which isavailable may not go to those who need it most. Inthis case, education of the health care provider isrequired.
The direct, annual cost of diabetes care at theMuhimbili Medical Centre in Dar es Salaam, UnitedRepublic of Tanzania in 1989–1990 was estimatedat US$ 287 for a person requiring insulin andUS$ 103 for a person not requiring insulin (10).Purchases of insulin accounted for US$ 156, or68% of average annual outpatient costs. Whencompared to the Tanzanian per capita GNP of US$240 at that time, the financial burden of diabetes,especially the insulin-requiring form, becomesobvious. The total outpatient costs of diabetes inTanzania in the same year were estimated at US$2.7 million, out of a total health care budget of US$47.4 million, of which insulin supply accounted forUS$ 800 000. Thus, outpatient usage of insulin,alone, amounted to 2% of the entire national healthcare budget.
A questionnaire survey via two medical journals,Practical Diabetes Digest and Tropical Doctor, bothwidely circulated in Africa, indicated that in mostcases patients were required to pay for their insulin(11). Prices quoted for 1990–1991 ranged fromUS$ 1.50 to US$ 20 for a 10-ml vial. The samereport estimated the total annual cost of insulintreatment in sub-Saharan Africa at US$ 25 million.
StorageTo retain its potency, insulin should be stored at atemperature of 4–8 °C. In tropical countries, thiscan only be achieved in a refrigerator. Recently,several investigators in Africa have reported pa-tients’ insulin storage practices, which appear toreflect both underlying socioeconomic conditionsand level of diabetic education. Use of a refrigeratorwas recorded in 77% of cases in Tripoli, LibyanArab Jamahiriya (12), 69% in Soweto, South Africa(13), 37% in Blantyre, Malawi (14) and only 26% inAddis Ababa, Ethiopia (15). The refrigerator did notalways belong to the patient concerned; reported
facilities included those of butchers’ shops and, inan enterprising Nigerian example, a beer parlour(16).
It has been known for some time that in the ab-sence of refrigerator facilities, insulin may be storedin porous clay pots filled with water and a bed ofsand. Thirty-eight per cent of diabetic patients inMalawi and 18% of those in Ethiopia used clay potsfor storage. When considered in the light of somevery inappropriate storage choices (freezer, car, topof television, in bed), the opportunity for betterinformation to improve patients’ insulin storagepractices is clear.
Social and cultural barriersIn some communities, widespread misconceptionsexist concerning insulin. Because it is injected,many believe it is a drug of addiction, and areunwilling to use it even if it is freely available.Others associate it with a worsening of diseasestatus, and refuse to accept it on that account. Yetothers consider it a sign of terminal illness. As withthe simple recourse to clay pot storage, a smallamount of accurate information from a respectedhealth care worker is often all that is required toovercome these problems.
Monitoring metabolic controlRecent research has clearly demonstrated theimportance of good metabolic control in preventingand delaying the progression of long-term diabeticcomplications (17). However, in most of the world’spoor countries the possibility of home blood glucosemonitoring — the most effective form — is remoteindeed. Even a weekly blood glucose estimationmay be considered a luxury in such circumstancesand measures of longer-term control, such as theHbA1c estimation, are rarely available in routinecare. Thus, the insulin which is provided or pur-chased may be ineffective and will not achieve thefundamental aim of maintaining the quality of life ofthe user. Under such circumstances, urine testing isa useful and more affordable option which shouldbe encouraged, notwithstanding its lower precision.
HarmonizationInsulin is not only available in a variety of forms, it isalso manufactured in several strengths, rangingfrom 20 international units/ml (IU20) to 100 interna-tional units/ml (IU100). For the treatment of diabe-tes the current WHO Model List of Essential Drugsrecognizes IU40 and IU100 soluble and intermedi-ate-acting insulins, in addition to the oral agentsglibenclamide and metformin (18).
General Information

233
WHO Drug Information Vol. 12, No. 4, 1998
In different countries, different forms and strengthspredominate. This is especially confusing for thetraveller, who may inadvertently use the wrongdose by drawing up their usual quantity of thewrong strength. It also requires an array of deliverysystems. For this reason, there have been calls, ledby the International Diabetes Federation, for theharmonization of insulin in all countries to IU100(19).
While such harmonization has much to recommendit, there are some difficulties to overcome beforesuch a plan would be universally acceptable.Firstly, a 10-ml vial of IU100 insulin is more expen-sive than its IU40 counterpart, and thus, its pur-chase may cause greater short-term financialhardship. Secondly, the IU100 vial lasts corre-spondingly longer, augmenting storage problems inthe absence of adequate refrigeration.
The manufacture of smaller vials might addressboth of these issues, but since the cost of the vialwould remain much the same, extra expense perunit of insulin would arise. Thus, these matters areyet to be satisfactorily resolved.
Human versus animal insulinSince the arrival of biosynthetic human insulin onthe market in the 1980s, there has been a certainamount of controversy about the relative merits ofhuman and animal insulins. Clearly, human insulinrepresents the ideal, in terms of potential antigenic-ity, and most “affluent” countries rely on it almostentirely. However, antigenic reactions to either formof animal insulin appear to be relatively rare, andanimal insulin is generally cheaper than humaninsulin. Therefore, at present, bovine or porcineinsulin still represents a cost-effective way ofachieving metabolic control for many patients,especially in developing countries.
A rather greater controversy was created by areport that use of human insulin may be associatedwith a reduced awareness of hypoglycaemia, with aconsequent risk of coma, or even death (20). Themajority of studies which subsequently addressedthis issue failed to replicate the findings of theoriginal report (21) and almost all experts nowdiscount the theory that human insulin is an impor-tant cause of hypoglycaemia unawareness. How-ever, the possibility of this association in a smallnumber of susceptible subjects is acknowledged,and no patient should be denied the opportunity touse animal insulin if prefered.
The futureAlthough it is the minority of diabetic patients whorequire regular treatment with insulin, the inconven-ience and discomfort of daily insulin injections hascome to be almost symbolic of the disease itself,causing fear and anxiety about diabetes in thepublic at large. Therefore, there has beenlongstanding interest in delivering insulin in lessinvasive ways.
Recent technological advances are making alterna-tive approaches appear more feasible. Good con-trol of both type-1 and type-2 diabetes has beenreported using inhaled insulin and at least twomultinational companies are seriously involved inproduct development. There is also interest in oralinsulin. However, all such methods are currently inthe research phase and they will not be available tothe large majority of patients for some time.
ConclusionsFor a variety of reasons, insulin remains unavail-able or unaffordable to many who need it in devel-oping countries. Consideration of insulin supply isan important ingredient of any national diabetesprogramme, but particularly in developing countries.Many of the barriers may be overcome by meas-ures which are within the means of even the world’spoorer nations.
References
1. Alberti, K.G.M.M., Zimmet, P.Z. for the WHOConsultation: Definition, diagnosis and classification ofdiabetes mellitus and its complications. Part 1: Diagnosisand classification of diabetes mellitus. Diabetic Medicine,15: 539–553 (1998).
2.. Tan, M.-H. Insulin unavailability – problems andsolutions. International Diabetes Federation Bulletin, 41:8–11 (1996).
3. Metelko, Z., Roglic, G., Skrabalo, Z. Diabetes in time ofarmed conflict: the Croatian experience. World HealthStatistics Quarterly, 45(4): 328–333 (1992).
4. Baba, S., Taniguchi, H., Nambu, S., Tsuboi, S.,Ishihara, K., Osato, S. The Great Hanshin Earthquake.Lancet, 347: 307–309 (1996).
5. Access to insulin, a report on the IDF task force oninsulin 1994–1997. Brussels, International DiabetesFederation, 1998.
6. Raab R. New developments in a practical programmeto help provide insulin and diabetes supplies to nations inurgent need. International Diabetes Digest, 6(1): 8–10(1995).
General Information

234
WHO Drug Information Vol. 12, No. 4, 1998
7. King, H., Aubert, R., Herman W.H. Global burden ofdiabetes, 1995–2025: Prevalence, numerical estimatesand projections. Diabetes Care, 21: 1414–1431 (1998).
8. World Health Organization. Reiber G., King H.Guidelines for the development of a national programmefor diabetes mellitus, WHO/DBO/DM/91.1 (1991).
9. Krosbein, P., Jörgens, V., Berger, M. The price ofinsulin. International Diabetes Federation Bulletin, 42(3): 8(1997).
10. Chale, S.S., Swai, A.B.M., Mujinja, P.G.M., McLarty,D.G. Must insulin be a fatal disease in Africa? Study ofcosts of treatment. British Medical Journal, 304: 1215–1218 (1992).
11. McLarty, D.G., Swai, A.B.M., Alberti, K.G.M.M. Insulinavailability in Africa: an insoluble problem? InternationalDiabetes Digest, 5(1): 15–17 (1994).
12. Bosseri, S. Insulin storage by diabetic patients inTripoli, Libya. International Diabetes Digest, 7(2):44(1996).
13. Gill, G., Ngubane, T. Insulin storage by diabeticpatients in Soweto, South Africa. International DiabetesDigest, 6(4):89 (1995).
14. Harries, A.D., Maher, D. Home insulin storage bypatients with diabetes mellitus in Blantyre, Malawi.International Diabetes Digest, 5(4):104 (1994).
15. Seyoum, B., Abdulkadir, J., Feleke, Y., Worku, Y.Insulin storage by diabetic patients in Ethiopia.International Diabetes Digest, 9(2):43-44 (1998).
16. Gill, G. Insulin storage by diabetic patients in tropicalcountries. International Diabetes Digest, 7(2): 25 (1996).
17. Diabetes Control and Complications Trial ResearchGroup. The effect of intensive treatment of diabetes on thedevelopment and progression of long-term complicationsin insulin-dependent diabetes mellitus. New EnglandJournal of Medicine, 329: 977–986 (1993).
18. WHO Model List of Essential Drugs (revised inDecember 1997). WHO Drug Information, 12(1): 22–35(1998).
19. Towards one strength of insulin (IU100). WHO DrugInformation, 9(3): 163 (1995).
20. Teuscher, A., Berger, W. Hypoglycaemia unaware-ness in diabetics transferred from beef/porcine insulin tohuman insulin. Lancet, 2, 382–385 (1987).
21. Jørgensen, L.N., Dejgaard, A., Pramming, S.K.Human insulin and hypoglycaemia: a literature survey.Diabetic Medicine, 11, 925–934 (1994).
22. Jervell, J. Variations in utilization and cost ofinsulin.The insulin issue. International DiabetesFederation Bulletin, 41: 1–2 (1996).
23. Amos, A., McCarty, D.J., Zimmet, P. The rising globalburden of diabetes and its complications: Estimates andprojections to the year 2010. Diabetic Medicine, 14,Supplement 5 (1997).
24. Gruber et al. (Eds). The Economics of Diabetes andDiabetes Care. A Report of the Diabetes HealthEconomics Study Group. Brussels, International DiabetesFederation (n.d.).
General Information
235
WHO Drug Information Vol. 12, No. 4, 1998
Bruising and bleeding withnew antidepressantsAustralia — Use of selective serotonin re-uptakeinhibitors (SSRIs) has increased considerably overthe past years and the Adverse Drug Reactions Ad-visory Committee has published a comprehensiveadverse effect profile concerning the new SSRIs,fluoxetine, paroxetine and sertraline.
Bruising and bleeding appeared to be importantadverse reactions to SSRIs. The most commonbleeding sites were vaginal (24 cases), and com-mon bleeding episodes involved epistaxis (19),haematuria (10), and rectal haemorrhage (8).
fluoxetine paroxetine sertraline
Total reports 919 1036 2023
Purpura/bruising 20 38 16Bleeding 10 16 41Thrombocytopenia 9 10 5Platelet dysfunction 5 5 4
Paroxetine was most commonly cited as a cause ofpurpura. Of the 14 reported platelet abnormalities,11 occurred in association with purpura or bleed-ing. Five of the reports documented abnormalplatelet aggregation, supporting the hypothesis thatfluoxetine may diminish granular storage of sero-tonin in platelets creating a haemostatic defect withbleeding.
Reference: Australian Adverse Drug Reactions Bulletin,17: 10 (1998)
Reports of death in sildenafil usersUnited States of America — The Food and DrugAdministration has summarized data on 123patients who died after having been prescribedsildenafil (Viagra®). Since introduction onto themarket in March 1998, more than 3.6 million out-patient prescriptions have been dispensed. Of the123 deaths reported in the USA, 12 were patientsfrom overseas and 42 could not be verified, leaving69 fatal cases. Of these, the cause of death couldnot be determined in 21 patients. Two deaths were
Regulatory Matters
due to stroke, 46 to cardiovascular events, 3 tocoronary artery disease and one to severe hypoten-sion and cardiac arrest.
In the 69 patients, the median age was 64, rangingfrom 29 to 87 years of age. Twenty-six patients hadtaken the 50 mg dose and 3 the 100 mg dose.Twelve patients had been using a concomitantnitrate medication that is contraindicated with silde-nafil. In all, 51 patients had one or more cardio-vascular risk factors or cerebrovascular disease.Twenty-five patients died or had symptoms leadingto death within 4–5 hours of use of sildenafil. Threedied or developed symptoms later the same day, 7the next day and 2 three or four days later.
The Food and Drug Administration will continue toevaluate adverse events and will monitor the needfor regulatory action.
Reference: FDA Viagra postmarketing report, 24 August1998.
Lipodystrophy andHIV protease inhibitorsUnited Kingdom — Since marketing, spontaneousreporting of suspected adverse effects has shownthat hyperlipidaemia, glucose intolerance, and dia-betes mellitus can occur with the HIV protease in-hibitors, ritonavir, indinavir, saquinavir and nelfina-vir. More recently, 33 case reports have suggestedthat HIV protease inhibitors may also cause periph-eral lipodystrophy, increased abdominal fat, buffalohumps and breast hypertrophy.
Although HIV protease inhibitors are a likely cause,this syndrome of reactions has also occurred in pa-tients treated with a combination of other antiretro-viral drugs for HIV which do not include protease in-hibitors. The reports are being evaluated to assesshow product information can be updated to reflectthe reactions. This will assist physicians and pa-tients in choosing appropriate treatment regimens.
Reference: Current Problems in Pharmacovigilance, Vol-ume 24, August 1998.
236
WHO Drug Information Vol. 12, No. 4, 1998
Australia — The Adverse Drug Reactions AdvisoryCommittee has received reports of adverse reac-tions to HIV protease inhibitors, including lipodys-trophy (94), hyperglycaemia, development or ag-gravation of diabetes (14) and nephrolithiasis.
The most commonly reported adverse effect is lipo-dystrophy, which involves a mobilization of the lipidstores in the face, arms and legs. Cases have beenreported involving indinavir (92), ritonavir (4) andsaquinavir (5). Onset began between 5 days andone year after commencement of treatment, with amean of 6 months.
Adverse effects are estimated to affect about 60%of patients taking HIV protease inhibitors.
Reference: Australian Adverse Drug Reactions Bulletin,17: 6 (1998).
Cisapride: new contraindicationsUnited Kingdom — The Medicines Control Agencyhas alerted prescribers to an interaction betweencisapride, a drug for reflux oesophagitis, and otherdrugs metabolized by the cytochrome P4503A4liver enzyme system. Raised blood levels of cis-apride may cause QT interval prolongation andventricular arrhythmias leading to direct electro-physiological effects on the heart.
Serious cardiac arrhythmias such as ventriculartachycardia, ventricular fibrillation and torsades depointes, resulting in sudden death, have been re-ported in patients taking cisapride. Many of thesepatients had also taken other drugs suspected of in-creasing cisapride levels in blood by inhibiting liverenzyme metabolism. However, reactions have alsooccurred in the absence of interacting drugs.
It is therefore recommended that cisapride shouldnot be used in the following circumstances:
• With CYP3A4-inhibiting drugs, including macrolideantibiotics such as erythromycin or clarithromycin,azole antifungals such as fluconazole, itracona-zole, or ketoconazole, HIV protease inhibitorssuch as ritonavir or indinavir, and nefazadone.
• With drugs known to prolong the QT interval suchas quinine, halofantrine, terfenadine, astemizole,amiodarone, quinidine, amitriptyline, pheno-thiazines and sertindole.
• In patients with a personal or family history of QTinterval prolongation.
• In patients with a previous history of ventricular ar-rhythmias or torsades de pointes.
• In patients with risk factors for arrhythmia such assecond or third degree atrioventricular block, clini-cally significant heart disease, uncorrected elec-trolyte disturbances, renal or respiratory failure.
Concern has also been expressed about use of cis-apride in children for infantile gastro-oesophagealreflux disease following reports of QT interval pro-longation in neonates. The pharmacokinetic actionof cisapride in premature neonates is unpredictableand may lead to potentially cardiotoxic blood levels.Cisapride is therefore contraindicated in prematureinfants and for up to 3 months after birth. Further-more, insufficient data are available to support cis-apride use in children under 12 years of age.
Reference: Current Problems in Pharmacovigilance, Vol-ume 24, August 1998.
Cisapride: risk of arrhythmiasUnited States of America — The Food and DrugAdministration has warned physicians of the car-diac risks associated with the use of the night-timeheartburn drug, cisapride. Between 1993 and 1998there have been 38 reports of death including heartrhythm disorders, death in patients with particularunderlying medical conditions, and patients takingother medications.
The drug should not be used in patients takingcertain antibiotics, antidepressants, antifungals, orprotease inhibitors. Contraindications now includecongestive heart failure, multiple organ failure,chronic obstructive pulmonary disease and ad-vanced cancer, electrolyte disorders – hypokalae-mia or hypomagnesaemia — severe dehydration,vomiting, diarrhoea, malnutrition, those takingpotassium-wasting diuretics and /or insulin, orthose who may experience rapid reduction ofplasma potassium.
It is recommended that drugs other than cisapride,including lifestyle modification, should be used forthe primary treatment of night-time heartburn due toreflux oesophagitis.
Reference: FDA Talk Paper, T98–39, 1998.
Regulatory Matters

237
WHO Drug Information Vol. 12, No. 4, 1998
Mibefradil: instructions fortherapy substitutionUnited States of America — Following the world-wide withdrawal of mibefradil (Posicor®) (1) themanufacturer has issued instructions to physiciansconcerning substitute therapy. Unfortunately, asmall number of patients have experienced life-threatening drug interactions caused by the changeto alternative therapy. The following precautionsshould be taken to avoid drug-drug interactions (2):
1. If either amlodipine or atenolol is to be substi-tuted, the medication should be started two or threedays prior to mibefradil discontinuation.
2. If another calcium channel blocker (exceptfelodipine) or a beta adrenoreceptor blocker (excepttimolol) is substituted, it should be started 7 daysafter mibefradil discontinuation.
3. If felodipine or timolol is chosen, it should bestarted 14 days after mibefradil discontinuation.
4. No special precautions regarding the timing arenecessary for other antihypertensive or anti-anginalmedications such as ACE inhibitors, angiotensin IIantagonists, diuretics, or nitrates.
References
1. WHO Drug Information, 12(3): 145 (1998).
2. Communication to the Food and Drug Administration'sMedwatch from Roche Laboratories, dated June 12 1998.
Mibefradil suspendedin GermanyGermany — In June 1998, Roche withdrew mibe-fradil (Posicor 50/100®, Cerate 100®) worldwidefor safety reasons. However, mibefradil was stillmarketed in Germany by Asta Medica under thebrand name Cerate 50. Asta Medica has refused tofollow Roche's decision. It has none the less agreednot to continue selling the drug without the agree-ment of the German drug regulatory authority,BfArM.
At the end of August 1998, BfArM ordered a three-month suspension of Asta Medica's marketing au-thorization for mibefradil and recall of the product.Asta Medica does not agree with the reasons forthe withdrawal and has a month in which to appeal.
This case demonstrates the problem of disharmonyin regulatory action between countries and amongpharmaceutical companies concerning severesafety problems involving the same product.
Reference: Communication to WHO from the FederalInstitute for Drugs and Medical Devices, Germany,4 November 1998.
Isotretinoin: adversereaction profileUnited Kingdom — The Medicines Control Agencyhas received 841 reports of adverse reactions as-sociated with use of isotretinoin since the drug wasapproved for marketing in 1982.
Most frequently reported reactions were skin disor-ders such as rash, dry skin and photosensitivity(18%), musculoskeletal disorders such as myalgiaand arthralgia (11%), gastrointestinal disorderssuch as cheilitis, abdominal pain and dry mouth(10%), eye disorders such as conjunctivitis, dryeyes and blurred vision (7%), neurological disor-ders such as migraine and convulsions (7%), andpsychiatric reactions, including depression, suicideand attempted suicide (5%).
Physicians are reminded that isotretinoin is a tera-togen and is contraindicated in women of childbear-ing age unless the following criteria are respected:
• Isotretinoin is only for use in severe, disfiguringcystic acne resistant to standard therapy.
• Pregnancy must be excluded before startingtherapy and a negative pregnancy test must beobtained within two weeks prior to therapy.
• Effective contraception must be practised for atleast 4 weeks before treatment, during the treat-ment period and for at least four weeks followingcessation.
Isotretinoin should only be given by, or under thesupervision of, a specialized physician or derma-tologist and should not be prescribed by a non-specialist. The physician must clearly explain theprecautions, ensure that the patient understandsthe risks, and confirm that the warnings have beenunderstood.
Reference: Current Problems in Pharmacovigilance, Vol-ume 24, August 1998.
Regulatory Matters

238
WHO Drug Information Vol. 12, No. 4, 1998
Depression with isotretinoinAustralia — A total of 129 reports of adverse reac-tions associated with the use of isotretinoin havebeen received by the Adverse Drug Reaction Ad-visory Committee between 1985 and 1998. Ofthese, 12 described depression in patients aged15–40 years. The median age was 19 years, and allpatients were taking the drug for acne. In 10 re-ports, this was the first episode of depression: 2cases were severe and 4 cases presented psy-chotic features. Three patients had suicidalthoughts, and 2 attempted suicide, with one fataloutcome.
Physicians are advised to be alert for any moodchanges in patients taking isotretinoin and to with-draw the drug if this occurs.
Reference: Australian Adverse Drug Reactions Bulletin,17: 11 (1998).
Orlistat sold illegallySwitzerland — The authorities in the canton of Zu-rich have seized several hundred packs of the anti-obesity drug orlistat (Xenical®: Roche) from phar-macies and doctors' surgeries. The product has notyet received marketing authorization and was beingprescribed and dispensed illegally.
Advertisements announcing that the product wasavailable for sale appeared in local newspapersshortly after it had received marketing authorizationfrom the European Union Commission earlier thisyear.
Meanwhile, the Intercantonal Office for the Controlof Medicines is currently assessing a marketing ap-plication for orlistat and has requested the companyto provide additional information on the possiblerisks of breast cancer.
Reference: SCRIP, No. 2361, 14 August 1998.
Trastuzumab: approved forbreast cancerUnited States of America — The Food and DrugAdministration has approved a monoclonal antibodyas a new biological treatment for metastatic breastcancer, or cancer that has spread beyond thebreast and underarm lymph nodes. Trastuzumabinhibits tumour cell growth by the binding action of
the HER2 protein. In the case of metastatic breastcancer cells, approximately 30% of tumours pro-duce excess amounts of HER2. Only patients whohave tumours with this characteristic have beenshown to benefit from the new targeted approach.
Trastuzumab (Herceptin®) is used alone intra-venously for patients where chemotherapy hasbeen abandoned, or as treatment for metastaticdisease in combination with paclitaxel in treatment-naive patients.
Trastuzumab is the second monoclonal antibody tobe approved for cancer. The first was approved in1997 for patients with non-Hodgkin lymphoma.
Reference: HHS News, P98-27, September 1998.
Ritonavir and ecstasy —a fatal combinationSweden — The Medical Products Agency has is-sued a warning concerning the potentially fatal out-come of using the HIV protease inhibitor, ritonavir,with the illicit amphetamine-type drug, ecstasy. Intwo fatal cases, the concentration of 3,4-methylendioxymetamfetamin in plasma was morethan ten times higher than that normally detected inusers. Ritonavir is one of the most potent inhibitorsof cytochrome P450, including both CYP2D6 andCYP3A4 liver enzymes. Ecstasy is metabolized byCYP2D6 enzymes and it is possible that ritonavirslows down ecstasy elimination, resulting in highlytoxic levels in plasma.
Many opiates such as dextromethorphan, codeine,hydrocodon, oxycodon, dihydrocodeine andetylmorphine are similarly metabolized by the P450enzymes mentioned above. Thus, concomitant useof ritonavir with these opiates can result in a poten-tiated narcotic effect and risk of toxicity.
Reference: Information from the Medical ProductsAgency, 9: 5 (1998).
WHO recommendations forinfluenza virus vaccines — 1999World Health Organization — Epidemics of influ-enza occur at different times of the year in differentparts of the world and the influenza virus is con-stantly changing. It is therefore appropriate forWHO to review recommendations twice a year.
Regulatory Matters

239
WHO Drug Information Vol. 12, No. 4, 1998
A recommendation will continue to be made eachFebruary relating to the composition of vaccines in-tended for use for the following winter in the north-ern hemisphere and a second recommendation willbe made each September relating to vaccines foruse the following winter in the Southern hemi-sphere.
Consequently, vaccines for use in the 1999 seasonin the southern hemisphere should contain the fol-lowing:
• an A/Sydney/5/97 (H3N2)-like virus;
• an A/Beijing/262/95 (H1N1)-like virus;
• a B/Beijing/184/93-like virus. (The most widelyused vaccine virus is B/Harbin/7/94.)
Reference: Weekly Epidemiological Record, 73: 305–308(1998).
Rhabdomyolysis and ritodrineJapan — The Pharmaceutical and Medical SafetyBureau has received nine reports of rhabdomyoly-sis associated with ritodrine, used to avoid miscar-riage and premature birth.
Three of the patients received both tablets and in-jections. Symptoms included myalgia, enervationand elevated creatine phosphokinase levels. Theproduct information has been revised accordingly.
Reference: Pharma Japan, 1604, 29 June 1998.
Flutamide: severe hepaticdysfunctionJapan — The Pharmaceutical and Medical SafetyBureau has instructed the manufacturer offlutamide, an anti-androgen treatment for prostatecancer, to revise the information leaflet and to circu-late a letter to health care professionals indicatingthat 5 fatal cases of hepatic dysfunction have beenassociated with use of flutamide this year. Elevatedlevels of hepatic enzymes have been reported anddeaths occurred during 1995 and 1996.
The revised information leaflet now includes hepaticdysfunction as a contraindication and a warning hasbeen added as follows:
• Liver function to be monitored at least everymonth.
• If elevated levels of hepatic enzymes or othersymptoms of hepatic dysfunction are observed,stop medication.
• Prior to taking this medication, patients should beinformed of the possibility of hepatic dysfunctionand should be instructed to stop the medicationand to consult their physician immediately if signsof hepatic dysfunction are observed.
References
1. Communication from the Ministry of Health and Wel-fare, Japan, to WHO dated 20 August 1998.
Ebrotidine: liver toxicitySpain — The Medical Products Agency has sus-pended the marketing authorization of ebrotidine,an anti-ulcer H
2 receptor blocker, following reportsof serious liver damage.
No cases of liver injury were reported during clinicaltrials, but several reports have been received sub-sequent to marketing in 1997. Most cases occurredin patients using the drug for more than 6 weeks orbecause of concomitant use of other medicationsknown to cause hepatotoxic reactions.
Given the availability of other remedies of equaltherapeutic value, the company has agreed to with-draw the drug from the Spanish market.
Two other countries, Mauritius and Paraguay, havegranted a marketing authorization for this product.
Reference: Communication from the Ministerio deSanidad y Consumo, Spain, to WHO dated 27 July 1998.
Meloxicam: gastrointestinaland skin reactionsUnited Kingdom — A total of 773 reports were re-ceived by the Medicines Control Agency between1996 and 1998 describing 1339 suspected adversereactions to meloxicam, a nonsteroidal anti-inflam-matory drug for osteoarthritis, rheumatoid arthritisand ankylosing spondylitis.
The most frequently reported reactions were gas-trointestinal (41%), dermatological, neurological,
Regulatory Matters
240
WHO Drug Information Vol. 12, No. 4, 1998
and cardiovascular, including dizziness, flushingand fatigue. Although most patients recovered aftermeloxicam withdrawal, 5 deaths were reported.
Of the 193 reports involving skin reactions, themost common were pruritus, rash and urticaria.Angioedema was reported in 25 patients, photosen-sitivity in 12, and bullous dermatoses, including ery-thema multiforme and Stevens-Johnson syndromein 5 patients.
Reference: Current Problems in Pharmacovigilance, Vol-ume 24, August 1998.
Vaccine-associatedthrombocytopenic purpuraJapan — Since 1994, the Pharmaceutical andMedical Safety Bureau has received 13 reports ofacute thrombocytopenic purpuras associated withvaccination. These include 8 cases following rubellavaccine, 3 with measles vaccine and 1 followingboth diphtheria-tetanus-pertussis (DTP) andmumps vaccine. The rubella, measles and mumpsvaccines were freeze-dried, live attenuated vac-cines and the DTP was purified combined.
Reference: Pharma Japan, 1604, June 1998.
Abortifacients on free saleBrazil— Physicians and health authorities are call-ing for new public health measures to reduce therisk of birth defects associated with the misuse ofmisoprostol, a drug marketed for gastric ulcer, asan abortifacient (1). A recently published study re-ports 42 cases of infants exposed in utero to miso-prostol during the first trimester of pregnancy andborn with abnormalities, mostly limb defects (2).The defects may be caused by vascular disruptiondue to misoprostol-induced uterine contractions.
The authorities are also investigating reports of theillegal sale in pharmacies of an "abortion kit" com-posed of misoprostol and the anticancer drug,methotrexate.
References
1. SCRIP No. 2342, 10 June 1998.
2. Gonzalez, C.H., Marques-Dias, M.J., Chong, A.K. et al.Congenital abnormalities in Brazilian children associatedwith misoprostol misuse in first trimester of pregnancy.Lancet, 351: 1624–1627 (1998).
Illegal and counterfeitsildenafil on saleEarly in 1998, before sildenafil (Viagra®) was au-thorized for marketing, several drug regulatory au-thorities investigated its promotion and illegal sale(1). In the United Kingdom, faxed messages weresent to private individuals offering details of howand where Viagra could be obtained, either throughthe internet or by telephone (2). In July, the UKMedicines Control Agency seized 14 boxes of unli-censed sildenafil openly on sale in London (3).
Sildenafil can be obtained via the internet. Illegalsales have also been reported from Austria,France, Germany, Hong Kong (Special Administra-tive Region), Republic of Korea, the Russian Fed-eration, Spain and Sweden. (4). In addition to this,counterfeits originating in Mexico, Israel and Indiahave also appeared on the market in the RussianFederation (5).
These situations not only challenge regulatory con-trol and legislation on promotional activities, butpoint to the need for appropriate resources for en-forcement to combat the illegal cross-border sale ofmedical products.
References:
1. Viagra's licence and the internet. Lancet, 352: 751(1998).
2. SCRIP, No. 2363, 21 August 1998.
3. Pharmaceutical Journal, 261: 185 (1998).
4. SCRIP, No. 2347, 26 June 1998.
5. SCRIP, No. 2360, 12 August 1998.
Current standards forover-the-counter analgesicsFinland — The National Agency for Medicines hasreviewed the safety, efficacy and rationale of fixed-dose combinations of analgesics available over-the-counter. The review also assesses the validity ofsummary product characteristics and package infor-mation for the consumer.
It was concluded that the following combinationsare irrational, unsafe or insufficiently documented inclinical trials:
Regulatory Matters

241
WHO Drug Information Vol. 12, No. 4, 1998
• Products containing two or more salicylic acid de-rivatives.
• Products containing acetylsalicylic acid plusphenazone or phenazone salicylate.
• Codeine in combination with caffeine.
The Agency recommends the following single-component products for the symptomatic relief ofpain, fever and the common cold: acetylsalicylicacid, ibuprofen, ketoprofen or paracetamol. Re-moval of the above-mentioned inappropriate combi-nations will improve the efficacy and safety of selfmedication.
Reference: Drug Information from the National Agency forMedicines (TABU), 6: 39–41 (1998).
Safety of leukotriene antagonistsUnited Kingdom — The Medicines Control Agencyhas published a review of adverse drug reactions toa new class of asthma drugs, leukotriene antago-nists. Zafirlukast and moltelukast, competitive cys-teinyl leukotriene type-1 receptor antagonists, wereboth marketed for the first time in 1998.
Cysteinyl leukotrienes are inflammatory mediatorsand potent constrictors of bronchial smooth musclethat attract human eosinophils and cause airwayoedema, mucus hypersecretion and reducedmucociliary clearance. By blocking this action, leu-kotriene antagonists can improve respiratory func-tion and lessen symptoms in patients with asthma.
The pharmacological action of leukotrienes is quitecomplex and varying side effects have beenreported. Zafirlukast inhibits the hepatic cytochromeP4502C9, and interacts with warfarin, theophyllin,terfenadine, acetylsalicylic acid and erythromycin.Montelukast is metabolized by hepatic cytochromeP450CYP3A4 and co-administration of such drugsas phenytoin, phenobarbitone and rifampicin, whichinduce this enzyme, result in a marked reduction inplasma levels.
Side-effects identified during clinical trials wereheadache, abdominal pain, nausea, diarrhoea,gastro-enteritis, influenza, pharyngitis, sinusitis,cough, nasal congestion, dizziness, fatigue and in-somnia. Since marketing of montelukast, 173 re-ports of 317 suspected adverse drug reactionshave been received in the United Kingdom. Theseinclude oedema (50), psychiatric reactions, includ-
ing agitation/restlessness (15), allergy, includinganaphylaxis, angioedema and urticaria (10), chestpain (7), tremor (5), mouth dryness (5), vertigo (4)and arthralgia (3).
Reference: Current Problems in Pharmacovigi-lance, Volume 24, August 1998.
Reformulation of flunitrazepamtablets to prevent misuseSweden — The Medical Products Agency has is-sued information concerning the reformulation ofRohypnol® tablets containing the benzodiazepine,flunitrazepam.
Since the drug has been subject to misuse, the newtablet is harder and film coated to make it difficult todissolve in injections or to smoke. Additionally, thenew tablet is green, with a core of indigo that will in-stantly colour any liquid it is placed in. This will alertthe consumer that flunitrazepam has been added tothe drink.
Reference: Information from the Medical ProductsAgency, 9: 6 (1998).
Nicergoline re-evaluatedJapan —The Ministry of Health and Welfare haslimited the indications for nicergoline based on adecision by the Committee on New Drug Re-examination and Re-evaluation. Nicergoline hasbeen used for the improvement of cerebral circula-tion and metabolism with indications that it will "im-prove hyperbulia and emotional disorders due tochronic cerebral circulatory disorders associatedwith sequelae of cerebral infarction and cerebralhaemorrhage".
The Ministry has cancelled the marketing authoriza-tion of nicergoline and ordered the 18 genericmanufacturers to discontinue production and sale of23 nicergoline products and recall all batches frommedical institutions and pharmacies within twoweeks.
Following the re-evaluation of new clinical trials car-ried out independently by the company, on the onehand, and the generics manufacturers on the other,the original product, Sermion® was re-granted mar-keting approval. However, all generics were de-listed as a result of insufficiently demonstrated effi-cacy. The revised indication is "improvement of
Regulatory Matters

242
WHO Drug Information Vol. 12, No. 4, 1998
hyperbulia due to chronic cerebral circulatory dis-orders associated with the sequelae of cerebralinfarction".
This unusual case involving the refusal of an origi-nal product manufacturer to cooperate in clinicaltrials with generic manufacturers may make the re-evaluation of generics a major issue for discussionin health care reform.
Reference: Pharma Japan, Number 1604, June1998.
Entacapone for Parkinson diseaseEuropean Union — The Committee for ProprietaryMedicinal Products has given a positive opinion formarketing of entacapone, a catechol-O-methyltransferase (COMT) inhibitor. Entacapone preventsthe peripheral breakdown of levodopa and in-creases the amount of dopamine transmitted to thebrain (1). This is the second COMT inhibitor ap-proved for Parkinson disease. The first wastolcapone (2).
References
1. CPMP Press Release, 28 May 1998, CPMP/1150/98.
2. WHO Drug Information, 11: 251 (1997).
Chinese herbal medicinesand adverse reactionsUnited Kingdom — In analyses carried out byKing's College Hospital in London, 7 out of 10creams prescribed to children and adults by herbalpractitioners were found to contain dexamethasone,a corticosteroid.
The creams were prescribed for eczema, eczemaherpeticum, and scaly scalp. Children had receivedhigher doses than adults. In one case application ofthe cream resulted in severe eczema herpeticumrequiring hospitalization.
Reference: The Pharmaceutical Journal, Volume 261, 8August 1998.
Regulatory Matters

243
WHO Drug Information Vol. 12, No. 4, 1998
Essential Drugs
As described in previous issues of this journal, work is now under way on the WHO ModelFormulary, and draft texts will be published regularly to obtain comments on the materialproposed for publication. Observations concerning the following sections should be addressedto: Drug Selection and Information (DSI), Division of Drug Management & Policies, WorldHealth Organization, 1211 Geneva 27, Switzerland.
WHO Model Formulary
Ophthalmological preparations
Anti-infective agentsBlepharitis, conjunctivitis, keratitis and endophthal-mitis are common acute infections of the eye, andcan be treated topically. However, in some cases— for example gonococcal conjunctivitis — bothtopical and systemic anti-infective treatment may benecessary. Blepharitis and conjunctivitis are oftencaused by staphylococcus, while keratitis and en-dophthalmitis may be bacterial, viral or fungal.
Bacterial blepharitis is treated with an antibacterialeye ointment or drops to the conjunctival sac or tothe edges of the eyelid. Although most cases ofacute bacterial conjunctivitis may resolve spontane-ously, anti-infective treatment shortens the infec-tious process and prevents complications. Acute in-fective conjunctivitis is treated with antibacterial eyedrops by day and eye ointment at night. A poor re-sponse may indicate viral or allergic conjunctivitis.Keratitis requires immediate specialist treatment.
Gentamicin is a broad-spectrum bactericidal anti-biotic with particular activity against Pseudomonasaeruginosa, Neisseria gonorrhoeae and other bac-teria that may be implicated in blepharitis or con-junctivitis. Topical application can however lead tosystemic absorption, and possible adverse effects.
Idoxuridine is used in the treatment of keratitis dueto herpes simplex virus. Idoxuridine is effectiveagainst initial epithelial infections. These mayrespond to treatment within a week and resolvecompletely in 1–2 weeks. Eye drops must be ap-plied frequently to keep the concentration high andachieve a successful therapeutic outcome.
Silver nitrate is a topical anti-infective. Its germicidalactivity is attributed to precipitation of bacterial pro-teins by silver ions. It is available in a 1% ophthal-mic solution and is used for prophylaxis of gono-coccal ophthalmia neonatorum.
Tetracycline is a broad-spectrum antibiotic with ac-tivity against Gram-positive and Gram-negativebacteria including N. gonorrhoeae, and mostchlamydia, rickettsia, mycoplasma andspirochaetes. Ophthalmic tetracycline is used inblepharitis, conjunctivitis, and keratitis produced bysusceptible bacteria. It is also used in the treatmentof trachoma caused by Chlamydia trachomatis andin the prophylaxis of ophthalmia neonatorumcaused by N. gonorrhoeae and C. trachomatis.
GENTAMICINSolution (eye drops): 0.3%
Uses: Blepharitis, conjunctivitis
Dosage:Mild to moderate infectionApply 1 drop to the affected eye every 2 hours untilinfection is under control. Thereafter, apply less fre-quently, but continuing for 48 hours after infectionhas cleared.
Severe infection1 drop every hour.
Contraindications: Hypersensitivity to gentamicinand to any related antibiotic.
Precautions: Prolonged use may result in over-growth of non-susceptible organisms includingfungi. Discontinue if there is purulent discharge, in-flammation or exacerbation of pain.
244
WHO Drug Information Vol. 12, No. 4, 1998
Adverse effects: Burning or stinging sensation.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
IDOXURIDINESolution (eye drops): 0.1%Eye ointment: 0.2%
Uses: Keratitis or keratoconjunctivitis caused byherpes simplex virus.
Dosage:Ophthalmic solution: Initially, apply 1 drop to eacheye every hour and every two hours at night untilthere is significant improvement. Thereafter, apply1 drop every two hours during the day and everyfour hours at night. Treatment should be continuedfor up to 5 days after complete healing.
Ophthalmic ointment: 1 application to the conjunc-tival sac every 4 hours and at bedtime (5 applica-tions daily). Treatment should be continued for upto 5 days after complete healing.
Contraindications: Hypersensitivity to idoxuridineor any of its components. Concurrent use of corti-costeroids.
Precautions: Do not exceed the frequency and du-ration of treatment. If there is no relief after 7 days,discontinue treatment.
Adverse effects: Burning, pain, inflammation anditching occur occasionally, and allergic reactionsrarely. Photophobia may occur.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
SILVER NITRATESolution (eye drops): 1%
Uses: Prophylaxis of gonococcal ophthalmia neo-natorum.
Dosage: The neonate’s eyes should be cleanedwith sterile gauze before applying 2 drops of thesolution to the lower conjunctival sac. Excess solu-tion around the eye should be removed to avoidstaining.
Contraindications: Hypersensitivity.
Precautions: Avoid contact with the skin to preventstaining. Avoid use of old solutions: the concentra-tion will increase as a result of solvent evaporation.
Adverse effects: Mild conjunctivitis. Repeated ad-ministration may cause corneal cauterization andblindness. Skin and mucous membrane irritationsmay occur.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
TETRACYCLINEOintment: 1% (hydrochloride)
Uses: Superficial ocular bacterial infections, pro-phylaxis of ophthalmia neonatorum due to N.gonorrhoeae or C. trachomatis. Mass treatment oftrachoma in endemic areas.
Dosage:Adults: Ointment should be applied to the affectedeye 3–4 times daily. In the case of C. trachomatisinfection, treatment should continue for at least 3weeks.
Ophthalmia neonatorumApply a thin layer of the ointment to the conjunctivalsac. Lower the neonate’s eyelids and massagegently to spread the ointment. Treatment should beundertaken within one hour of delivery to achievemaximum effect.
Contraindications: Hypersensitivity to tetra-cyclines.
Precautions: Prolonged use may result in over-growth of non-susceptible organisms includingfungi.
Adverse effects: Dermatitis, transient stinging orburning sensation occur rarely and increased lacri-mation has been reported.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
Anti-inflammatory agentsTopical ophthalmic corticosteroids such as pred-nisolone are useful in inflammatory conditions suchas uveitis and scleritis. They are also used for post-operative ocular inflammation. The duration of treat-
Essential Drugs

245
WHO Drug Information Vol. 12, No. 4, 1998
ment depends on the type and severity of infectionand may range from a few days to several weeks.However, long-term use should be avoided. Cessa-tion should be gradual to avoid exacerbation of thecondition.
Topical corticosteroids should only be prescribed byqualified ophthalmologists as they may aggravateocular inflammation due to underlying herpes sim-plex or open-angle glaucoma.
PREDNISOLONEEye drops: 0.5%
Uses: Short-term treatment of ocular inflammation.
Dosage: Apply 1–2 drops to the eye every 1–2hours until inflammation subsides.
Contraindications: Hypersensitivity to cortico-steroids. Pre-existing glaucoma.
Precautions: Use with caution in patients withcataract, diabetes, corneal thinning disease or in-fections of the cornea or conjunctiva.
Adverse effects: Corneal thinning, which mayimpair corneal healing. Increased intra-ocular pres-sure, which may precipitate glaucoma, optic nervedamage, or cataract. Secondary ocular infections.Burning or stinging sensations may occur rarely
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
Local anaestheticsTopical local anaesthetics are employed for simpleophthalmological procedures and for short opera-tive procedures involving the cornea and conjunc-tiva. Tetracaine, available in 0.5% ophthalmic solu-tion, provides a rapid local anaesthesia which lastsfor 15 minutes or more. Prolonged or unsuperviseduse of tetracaine is not recommended.
TETRACAINESolution (eye drops): 0.5 % (hydrochloride)
Uses: Short-acting local anaesthesia of the corneaand conjunctiva.
Dosage:One to two drops instilled into the conjunctival sac.
Contraindications: Hypersensitivity to tetracaineand other ester-type local anaesthetics. Ocular in-flammation or infection.
Precautions: Prolonged use may result in severekeratitis, permanent corneal opacification, scarringand delayed corneal healing. The anaesthetizedeye should be protected from dust and bacterio-logical contamination until sensation is fullyrestored.
Adverse effects: Burning sensation, stinging, andredness occur frequently. Allergic reactions are re-ported rarely.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
Miotics and antiglaucoma drugsGlaucoma is often associated with abnormallyhigh intra-ocular pressure and may result in blind-ness. The rise in pressure is almost always due toreduced outflow of aqueous humour, the inflow re-maining constant. It can be treated by applicationof eye drops containing beta adrenoreceptor an-tagonist, miotics or epinephrine.
The commonest condition is chronic, simple glau-coma where the obstruction is in the trabecularmeshwork. This is treated initially with a topicalbeta adrenoreceptor antagonist. Epinephrine orpilocarpine is added to control the intra-ocularpressure as necessary.
Miotics, through their parasympathomimetic action,contract the iris sphincter and the ciliary muscleand widen the trabecular meshwork, thereby facili-tating outflow of the aqueous humour and loweringintra-ocular pressure. However, systemic absorp-tion may occur, producing muscarine-like toxicity.
Acetazolamide, a carbonic anhydrase inhibitor,reduces intra-ocular pressure by reducing the pro-duction of aqueous humour. Carbonic anhydraseinhibitors are used as adjuncts for prolongedtherapy in patients with open-angle glaucoma notresponsive to miotics alone. They should be admin-istered concurrently with pilocarpine or epine-phrine, to enhance their antiglaucoma effects.
Timolol is a non-selective beta adrenoreceptor an-tagonist with an intra-ocular pressure lowering ef-fect. However, since systemic absorption may oc-
Essential Drugs

246
WHO Drug Information Vol. 12, No. 4, 1998
cur, ophthalmic beta adrenoreceptor antagonistsshould be used with caution in certain individuals.
ACETAZOLAMIDETablet: 250 mg
Uses: As an adjunct to other agents in the treat-ment of open-angle glaucoma and secondary glau-coma resulting from anterior uveitis, iritis, herpeszoster infections, trauma or the granulomatocycliticcrisis syndrome. Closed-angle glaucoma.Pre-operative treatment for some types of glaucoma.
Dosage: Initially, 250 mg 4 times daily. Dosageshould be adjusted according to patient responseand may be reduced to 250 mg twice or even oncedaily.
Contraindications: Hypersensitivity to sulfona-mides. Pregnancy. Severe renal or hepatic impair-ment.
Precautions: A blood count is necessary whenused for prolonged periods. May impair mentalawareness. Use with caution in diabetic patients.
Adverse effects: Paraesthesia, hypokalaemia, lackof appetite, nausea, vomiting, diarrhoea, polyuria,metabolic imbalance, transient myopia, drowsinessand depression have been reported. Adverse ef-fects related to sulfonamide use can also occur.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
PILOCARPINESolution (eye drops): 2%, 4%(hydrochloride or nitrate).
Uses: Open-angle glaucoma or closed-angleglaucoma. Non-uveitic secondary glaucoma, miosisfollowing surgery or ophthalmoscopic examination.
Dosage:Chronic glaucomaAdults: Apply 1 drop of a 2% or 4% solution 4 timesdaily.
Acute closed-angle glaucomaApply 1 drop of a 2% solution every 10 minutes 3 to6 times, then 1 drop every 1 to 3 hours until intra-ocular pressure subsides.
Contraindications: Hypersensitivity.
Precautions: Use with caution in patients withbronchial asthma or retinal disease.
Adverse effects: Parasympathomimetic effectshave been reported following systemic absorption.Eye pain, transient blurring of vision, bradycardia,sweating, increased salivation, intestinal spasm andbronchospasm also occur.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
TIMOLOLSolution (eye drops): 0.25%, 0.5% (maleate)
Uses: Alone or in combination with other antiglau-coma agents in ocular hypertension. Open-angleglaucoma. Aphakic glaucoma. Secondary glau-coma.
Dosage:Adults: Apply one drop of 0.25% or 0.5% solution1–2 times daily.
Children: Apply 1 drop of 0.25% solution, 1–2 timesdaily.
Contraindications: Heart failure, bradycardia,heart block, asthma or obstructive airways disease.
Precautions: May precipitate myasthenia gravis insusceptible patients.
Adverse effects: Local allergic blepharitis andtransient dryness of eyes have been reported.Visual disturbances, decreased corneal sensitivity,diplopia and ptosis are rarely reported. If absorbedto a large extent systemically, allergic reactions,chest pain, difficulty in breathing, arrhythmias, dizzi-ness, confusion or mental depression, nausea,vomiting, diarrhoea and muscle weakness mayoccur.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
MydriaticsMydriatics are used to dilate the pupil and paralysethe ciliary muscle in ophthalmological procedures.
Essential Drugs

247
WHO Drug Information Vol. 12, No. 4, 1998
Atropine produces mydriasis by relaxing the sphinc-ter muscle of the iris and cycloplegia by paralysingthe ciliary muscle. It produces these effects byblocking the cholinergic effects of acetylcholine. At-ropine is also used for the treatment of iridocyclitismainly to prevent posterior synechia.
Ophthalmic atropine is useful in refraction proce-dures in children, but not in adults because of itsprolonged duration of action. Higher concentrationsof the mydriatic agents are usually required in pa-tients with dark iridic pigmentation. Care should betaken to avoid overdosing in this situation. Mydria-sis may rarely precipitate acute closed-angle glau-coma particularly in patients over 60 years of age.
Epinephrine produces mydriasis by contracting con-junctival blood vessels and the dilator muscle of thepupil. It lowers intra-ocular pressure by reducing therate of production of aqueous humour and increas-ing the outflow through the trabecular meshwork.
ATROPINESolution (eye drops): 0.1%, 0.5%, 1% (sulfate)
Uses: Cycloplegic refraction procedures in youngchildren. Treatment of uveitis.
Dosage:UveitisAdults: Apply one drop of a 1% solution to the eye1–2 times daily.
Cycloplegic refractionChildren: Apply 1 drop twice daily for 1–3 days priorto refraction. The eye drops should be applied inthe following concentrations : Infants up to 1 year ofage: 0.1%. Children 1–5 years of age: 0.1–0.5%.Children 5 years of age and above: 0.5% –1%.
Contraindications: Hypersensitivity. Closed-angleglaucoma.
Precautions: May precipitate glaucoma.
Adverse effects: Contact dermatitis, systemic anti-cholinergic effects, tachycardia, xerostomia, leth-argy, hallucination, mental confusion, blurred vision,skin rash, or dry skin may occur.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
EPINEPHRINESolution (eye drops): 2% (as hydrochloride)
Uses: Open-angle glaucoma, for use alone or incombination with miotics, beta adrenoreceptor an-tagonists or carbonic anhydrase inhibitors.
Dosage: Apply eye-drops 1–2 times daily.
Contraindications: Hypersensitivity, closed-angleglaucoma.
Precautions: Hypertension and heart disease.Hyperthyroidism. Diabetes
Adverse effects: Pigmentation of conjunctiva andreversible macular oedema in aphakia have beenreported after prolonged use. Burning, stinging,ophthalmalgia and conjunctival hyperaemia fre-quently occur and, less frequently, blurred vision,hypertension, headache, arrhythmias, or dizziness.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
Antiparkinsonism drugsThe use of pharmacotherapy will depend upon thedegree of incapacity of the patient, but is generallynot justified until symptoms compromise workingability and social relationships. Close supervision isthen needed to ensure that treatment regimens aretolerated and that appropriate changes are made tothe regimen as the disease progresses.
The most effective form of therapy is a combinationof levodopa and a peripheral dopadecarboxylaseinhibitor, carbidopa. The response to levodopa/carbidopa can be compromised both by toleranceand adverse effects. Tolerance, resulting in pro-gressive shortening of the therapeutic response, in-variably occurs within 2–5 years. Fluctuatingdyskinesias and mental changes — which are mostevident during troughs in the plasma drug concen-trations — disruption of the sleep cycle, vividdreams and hallucinations are characteristic ad-verse effects that may occur at any time. Ameliora-tion of these effects can sometimes be achieved byadministering levodopa in a sustained releasepreparation or in a greater number of fractionateddoses throughout the day. Supplementary use ofamantadine, bromocriptine or selegiline can be ofvalue either to enhance the effect of levodopa or to
Essential Drugs

248
WHO Drug Information Vol. 12, No. 4, 1998
permit dosage to be reduced to a level where ad-verse effects are no longer troublesome.
Anticholinergic drugs such as biperiden are usuallysufficient in drug-induced pseudo-parkinsonism.They are also used as adjunctive therapy in otherforms of parkinsonism where the primary need isto stimulate dopaminergic activity in the striatalsystem.
LEVODOPA/CARBIDOPATablet: 100 mg + 10 mg, 250 mg + 25 mg
Uses: All forms of parkinsonism other than drug-induced.
Dosage: Dose is expressed in terms of levodopa.The optimum daily dose must be determined foreach patient by careful clinical monitoring andshould be taken after meals.
Initial dose100 mg levodopa + 10 mg carbidopa twice daily in-creasing, as necessary, by increments of 100 mg +10 mg every few days to a maximum of 1500 mglevodopa daily.
Contraindications: Known hypersensitivity to levo-dopa or carbidopa. Concurrent use of monoamineoxidase inhibitors. Narrow-angle glaucoma. Con-firmed or suspected malignant melanoma.
Precautions: Close supervision of patients is nec-essary. Mental changes and cardiac conductivity inpatients with atrial, nodal or ventricular dysrhyth-mias, or with a history of myocardial infarction,should be monitored. A rapid increase in dosagemay cause adverse effects, particularly in the eld-erly. Levodopa/carbidopa is teratogenic in animals,and pregnant women should be treated only whenthe needs of the mother outweigh the risk to thefetus.
Adverse effects: Nausea, anorexia and vomitingare sometimes troublesome, particularly at the out-set of treatment when postural hypotension mayalso occur, particularly in elderly patients and thosereceiving antihypertensives. Psychiatric and neuro-logical disturbances are the most frequent dose-limiting adverse effects. About half of all patientstreated complain of vivid dreams, hallucinations ordelusions. Psychotic symptoms and confusionalstates are less common. Mild intermittent dys-kinesias which occur within a few months of starting
treatment often respond to reduction or fractiona-tion of dosage.
Later in the course of the disease, the scope fordose adjustment is decreased as any dose reduc-tion is increasingly likely to result in akinesia. Pain-ful dystonic spasms and short episodes of akinesia,tremor and rigidity lasting from a few minutes toseveral hours are characteristic of the later phasesof treatment. Severe generalized dyskinesias aremost likely to occur in patients who have receivedhigh doses over prolonged periods. Sudden with-drawal in these circumstances has resulted in neu-roleptic malignant syndrome.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
BIPERIDENTablet: 2 mg (hydrochloride)
Uses: Treatment of drug-induced parkinsonismand adjunctive treatment of all other forms of thecondition.
Dosage: Initially, 2 mg three times daily or 2–4 mgonce daily up to a maximum of 16 mg daily de-pending on response and tolerance.
Contraindications: Known hypersensitivity tobiperiden. Closed-angle glaucoma. Obstructiveuropathy. Myasthenia gravis.
Precautions: Elderly patients are highly suscepti-ble to dose-related adverse effects. Patients shouldbe warned that their ability to drive or operatemachinery may be impaired. Close supervisionof patients with cardiac dysryhthmias, congestivecardiac failure or coronary heart disease is impor-tant, since they are at particular risk of atrio-ventricular block due to vagal stimulation of thesinoatrial node.
Adverse effects: Drowsiness, dry mouth, consti-pation, blurred vision, postural hypotension, hesi-tancy of micturition, glaucoma, dizziness, tachycar-dia and dysrhythmias commonly occur. Confusionand psychiatric disturbances, particularly in the eld-erly, can be difficult to manage.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
Essential Drugs

249
WHO Drug Information Vol. 12, No. 4, 1998
Recent Publications and Documents
Guidelines forHIV and infant feedingIt is now recognized that if an HIV-infected motherbreastfeeds, there is an additional risk that herinfant will be infected. In many countries, personneldealing with health, nutrition and welfare are begin-ning to face a demand for information, advice andsupport from anxious mothers and families. Besidesbeing of intense personal concern, the issue of HIVtransmission through breastfeeding is also of publichealth importance — especially in countries whereboth fertility rates and HIV-infection of pregnantwomen are high. AIDS has already doubled themortality of children under 5 years of age in someareas. Although only a small proportion of thisincrease is the result of breastfeeding, there is apressing need for countries to develop and imple-ment sound public health policies on HIV and infantfeeding.
The guidelines cover policy issues and implementa-tion, monitoring and evaluation of HIV and infantfeeding strategies, and include a list of usefulresources and reference materials. They alsosummarize knowledge of HIV transmission throughbreastmilk
HIV and Infant Feeding: Guidelines for Decision-Makers.UNICEF/UNAIDS/WHO. Document WHO/FRH/NUT/CHD/98.1. Available from: World Health Organization, Geneva,Switzerland. e mail: [email protected]
Symptom relief in terminal illnessThis guide explains the management of secondarysymptoms commonly seen in patients sufferingfrom cancer, AIDS, and other terminal diseases.Practical advice is offered on how to evaluatepatients and find ways to improve their comfort andquality of life, and emphasis is placed on the needfor individual treatment plans.
Each symptom is covered according to a commonapproach which outlines possible causes, describesthe steps to follow and explains how to select andimplement the best treatment option. For drugtherapies, information includes recommendeddrugs, doses, and modes of administration, to-
gether with advice dealing with side-effects andother problems that may arise.
The book complements information contained in theWHO guide, Cancer Pain Relief: with a Guide toOpioid Availability, 2nd ed. Pain management istherefore not covered in this publication.
Symptom Relief in Terminal Illness. Available from: WorldHealth Organization, Geneva, Switzerland. ISBN 92 4154507 0. Price: Sw.fr. 25 (Sw.fr 17.50 in developingcountries). e mail: [email protected]
Guidance modules onantiretroviral treatmentsTremendous optimism has been generated by therecent development of new antiretrovirals, particu-larly the triple combination therapies, which promisea longer and better life for people living with HIV/AIDS. In response to requests for information onthese treatments and for policy and technicalguidance for health professionals and governments,nine guidance modules have been published byWHO in collaboration with UNAIDS. The modulescover the following topics:
1. Introduction to antiretroviral treatments.
2. Introducing antiretroviral treatments into nationalhealth systems: economic considerations.
3. ARV treatments: planning and integration intohealth services.
4. Safe and effective use of antiretrovirals.
5. Laboratory requirements for the safe and effec-tive use of antiretrovirals.
6. The use of antiretroviral drugs to reduce motherto child transmission of HIV.
7. Treatments following exposure to HIV.
8. Antiretrovirals: regulation, distribution and con-trol.
9. Ethical and societal issues relating to antiretro-viral treatments.
250
WHO Drug Information Vol. 12, No. 4, 1998Recent Publications and Documents
UNAIDS and WHO are committed to increasingaccess to new technologies which have beenshown to be effective in preventing and treatingHIV/AIDS, and to improving the length and qualityof life of all those in need. However, enthusiasm forthe possibilities of triple therapy is tempered byseveral concerns. These involve the long-termbenefit and safety of use and accessibility andcompliance with these expensive and complicatedtreatments. Furthermore, sophisticated laboratoryand clinical services with qualified care providersare necessary for these therapies and follow-up.
Meanwhile, UNAIDS and WHO will continue toassess progress, and guidance provided in themodules will be regularly updated.
Guidance modules on antiretroviral treatments. Availablefrom: World Health Organization, Geneva, Switzerland.WHO/ASD/98.1. e-mail: [email protected]
Re-evaluating the safety profileof marketed drugsAddressed primarily to regulatory authorities anddrug manufacturers, this publication responds tothe absence of any harmonized, systematic proce-dures for assessing newly detected hazards, bal-ancing risks against benefits, and defining theresults in terms of action.
A group of 24 representatives of government regu-latory authorities and industry offer detailed adviceon concepts and procedures for determining themagnitude of the safety problem and deciding onappropriate action. This may involve a routinechange in product information or immediate with-drawal of the drug from the market.
The publication promotes a public health approachto encourage consistent practices when a majorsafety problem is identified. Examples are used toillustrate responses when evaluating benefitthrough scoring the seriousness of different ad-verse reactions. The model standard reporting formpresented in the publication plays a central role inthe recommended procedures. It concludes with a
series of in-depth case histories for seven drugsand a model for the quantification of risks. This isaccompanied by a detailed example of how themodel works in practice.
Benefit-risk balance for marketed drugs: evaluating safetysignals. CIOMS. Available from: World HealthOrganization, Geneva, Switzerland. ISBN 92 9036 068 2.Price: Sw.fr. 15 (Sw.fr 10.50 in developing countries).e-mail: [email protected]
Interventions to improveantimalarial useA Task Force on Improved Use of Antimalarialswas set up in 1993 by the UNDP/World Bank/WHOSpecial Programme for Research and Training inTropical Diseases to identify and test ways torationalize and improve the home treatment ofmalaria using existing oral antimalarials. Researchinterventions were implemented in six South-EastAsian countries which had the highest rates ofantimalarial multidrug resistance in the world.Treatment regimens included a 5-day combinationof artesunate + mefloquine and a 7-day course ofquinine + tetracycline. The Task Force provided aforum for identifying problem areas and testing theeffect of small but potentially important changes inthe delivery of drugs in the private sector.
Several approaches were tested in Cambodia,China, Lao People's Democratic Republic,Myanmar, Thailand and Viet Nam. These includedsubsidies for certain drug combinations, improvedpackaging of doses, health education interventions,use of a pharmacological marker to measure com-pliance, and assessment of drug quality. Theresults are described in a supplement of the Bulletinof the World Health Organization. User-friendlypackaging of drugs, which included simple andclear patient information, produced the best results.
Interventions to improve antimalarial use. Bulletin of theWorld Health Organization,76 (Suppl. 1), 1998. Availablefrom: World Health Organization, Geneva, Switzerland.ISBN 92 4 068751 3. Price: Sw.fr. 20.– (Sw.fr. 14.– indeveloping countries). e-mail: [email protected]

WHO Drug Information, Vol. 12, No 4, 1998 Proposed INN: List 80
International Nonproprietary Names for Pharmaceutical Substances (INN) Notice is hereby given that, in accordance with article 3 of the Procedure for the Selection of. Recommended International Nonproprietary Names for Pharmaceutical Substances, the names given in the list on the following pages are under consideration by the World Health Organization as Proposed International Nonproprietary Names. The inclusion of a name in the lists of Proposed International Nonproprietary Names does not imply any recommendation of the use of the substance in medicine or pharmacy.
Lists of Proposed (1-73) and Recommended (1-35) International Nonproprietary Names can be found in Cumulative List No. 9, 1996. The statements indicating action and use are based largely on information supplied by the manufacturer. This information is merely meant to provide an indication of the potential use of new substances at the time they are accorded Proposed International Nonproprietary Names. WHO is not in a position either to uphold these statements or to comment on the efficacy of the action claimed. Because of their provisional nature, these descriptors will neither be revised nor included in the Cumulative Lists of INNs
Dénominations communes internationales des Substances pharmaceutiques (DCI) Il est notifié que, conformément aux dispositions de l'article 3 de la Procédure à suivre en vue du choix de Dénominations communes internationales recommandées pour les Substances pharmaceutiques les dénominations ci-dessous sont mises à l'étude par l'Organisation mondiale de la Santé en tant que dénominations communes internationales proposées. L'inclusion d'une dénomination dans les listes de DCI proposées n'implique aucune recommandation en vue de l'utilisation de la substance correspondante en médecine ou en pharmacie.
On trouvera d'autres listes de Dénominations communes internationales proposées (1-73) et recommandées (1-35) dans la Liste récapitulative No. 9, 1996. Les mentions indiquant les propriétés et les indications des substances sont fondées sur les renseignements communiqués par le fabricant. Elles ne visent qu'à donner une idée de l'utilisation potentielle des nouvelles substances au moment où elles sont l'objet de propositions de DCI. L'OMS n'est pas en mesure de confirmer ces déclarations ni de faire de commentaires sur l'efficacité du mode d'action ainsi décrit. En raison de leur caractère provisoire, ces informations ne figureront pas dans les listes récapitulatives de DCI,
Denominaciones Comunes Internacionales para las Sustancias Farmacéuticas (DCI) De conformidad con lo que dispone el párrafo 3 del "Procedimiento de Selección de Denominaciones Comunes Internacionales Recomendadas para las Sustancias Farmacéuticas", se comunica por el presente anuncio que las denominaciones detalladas en las páginas siguientes están sometidas a estudio por la Organización Mundial de La Salud como Denominaciones Comunes Internacionales Propuestas. La inclusión de una denominación en las listas de las DCI Propuestas no supone recomendación alguna en favor del empleo de la sustancia respectiva en medicina o en farmacia.
Las listas de Denominaciones Comunes Internacionales Propuestas (1-73) y Recomendadas (1-35) se encuentran reunidas en Cumulative List No. 9, 1996. Las indicaciones sobre acción y uso que aparecen se basan principalmente en la información facilitada por los fabricantes. Esta información tiene por objeto dar una idea únicamente de las posibilidades de aplicación de las nuevas sustancias a las que se asigna una DCI Propuesta. La OMS no está facultada para respaldar esas indicaciones ni para formular comentarios sobre la eficacia de la acción que se atribuye al producto. Debido a su carácter provisional, esos datos descriptivos no deben incluirse en las listas recapitulativas de DCI.
251

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
Proposed International Nonproprietary Names: List 80 Comments on, or formal objections to, the proposed names may be forwarded by any person to the INN Programme of the World Health Organization within four months of the date of their publication in WHO Drug Information, i.e., for List 80 Proposed INN not later than 15 May 1999.
Dénominations communes internationales proposées: Liste 80 Des observations ou des objections formelles à l'égard des dénominations proposées peuvent être adressées par toute personne au Programme des Dénominations communes internationales de l'Organisation mondiale de la Santé dans un délai de quatre mois à compter de la date de leur publication dans WHO Drug Information, c'est-à-dire pour la Liste 80 de DCI Proposées le 15 mai 1999 au plus tard.
Denominaciones Comunes Internacionales Propuestas: Lista 80 Cualquier persona puede dirigir observaciones u objeciones respecto de las denominaciones propuestas, al Programa de Denominaciones Comunes Internacionales de la Organización Mundial de la Salud, en un plazo de cuatro meses, contados desde la fecha de su publicación en WHO Drug Information, es decir, para la Lista 80 de DCI Propuestas el 15 de mayo de 1999 a más tardar.
Proposed INN (Latin, English, French, Spanish)
DCI Proposée
DCI Propuesta
Chemical name or description: Action and use: Molecular formula Chemical Abstracts Service (CAS) registry number: Graphic formula
Nom chimique ou description: Propriétés et indications: Formule brute Numéro dans le registre du CAS: Formule développée
Nombre químico o descripción: Acción y uso: Fórmula empírica Número de registro del CAS: Fórmula desarrollada
abaperidonum abaperidone
abapéridone
abaperidona
7-[3-[4-(6-fluoro-1,2-benzisoxazol-3-yl)piperídino]propoxy]-3-(hydroxymethyl)-4H-1 -benzopyran-4-one antipsychotic
7-[3-[4-(6-fluoro-1,2-benzisoxazol-3-yl)piperidin-1-yl]propoxy]-3-(hydroxyméthyl)-4H-chromén-4-one psychotrope
7-[3-[4-(6-fluoro-1,2-benzisoxazol-3-il)piperidino]propoxi]-3-(hidroximetil)-4H-1-benzopiran-4-ona antipsicótico
C25H25FN2O5 183849-43-6
252

WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
alitretinoinum alitretinoin
alitrétinoine
alitretinoína
(2E,4E,6Z,8E)-3,7-dimethyl-9-(2,6,6-trimethyl-1-cyclohexen-1-yl)-2,4,6,8-nonatetraenoic acid antineoplastic
acide (2E,4E,6Z,8E)-3,7-diméthyl-9-(2,6,6-triméthylcyclohex-1-ényl)nqna-2,4,6,8-tétraénoíque antinéoplasique
ácido (2E,4E,6Z,8E)-3,7-dimetil-9-(2,6,6-trimetil-1-ciclohexen-1-il)-2,4,6,8-nonatetraenoico antineoplásico
C20H28O2 5300-03-8
anecortavum anecortave
anécortave
anecortava
17,21 -dihydroxypregna-4,9(11l)-diene-3,20-dione 21-acetate steroid
21-acètate de 17-hydroxy-3,20-dioxoprégna-4,9(11)-dién-21-yle sféroïde
21-acetato de 17-hidroxi-3,20-dioxopregna-4,9(11)-dien-21-iIo esteroide
C23H30O5 7753-60-8
artemotilum artemotil
artémotil
artemotilo
(3R,5aS,6R,8aS,9R,10S,12R,12aR)-10-ethoxydecahydro-3,6,9-trimethyl-3,12-epoxy-12H-pyrano[4,3-j]-1,2-benzodioxepin antimalarial
(3R,5aS,6R,8aS,9R,10S,12R,12aR)-10-éthoxy-3,6,9-triméthyldécahydro-3,12-époxypyrano[4,3-j]-1,2-benzodioxépine antipaludique
(3R,5aS,6R,8aS,9R,10S,12R,12aR)-10-etoxidecahidro-3,6,9-trimetil-3,12-epoxi-12H-pirano[4,3-j]-1,2-benzodioxepina antipalúdico
253

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
C17H28O5
arzoxifenum arzoxifene
arzoxifène
arzoxifeno
2-(p-methoxyphenyl)-3-[p-(2-piperidinoethoxy)phenoxy]benzo[b]thiophene-6-ol antiestrogen
2-(4-méthoxyphényl)-3-[4-[2-(pipéridin-1-yl)éthoxy]phénoxy]benzo= [b]thiophén-6-ol antioetrogène
2-(p-metoxifenil)-3-[p-(2-piperidinoetoxi)fenoxi]benzo[b]tiofeno-6-ol antiestrógeno
C28H29NO4S
atorolimumabum atorolimumab
atorolimumab
atorolirnumab
immunoglobulin G3, anti-(human Rh(D) antigen) (human monoclonal clone P3x22914G4 γ3-chain), disulfide with human monoclonal P3x22914G4 κ-chain, dimer immunomodulator
immunoglobuline G3, anti-(antigène Rh(D) humain) (chaîne γ3 de l'anticorps monoclonal humain P3x22914G4), dimère du disulfure avec la chaîne Κ de l'anticorps monoclonal humain P3x22914G4 immunomodulateur
inmunoglobulina G3, anti-(antígeno Rh(D) humano) (cadena γ3 del clon monoclonal humano P3x22914G4), dímero del disulfuro con la cadena Κ del anticuerpo monoclonal humano P3x22914G4 inmunomodulador
254
75887-54-6
182133-25-1
202833-08-7

WHO Drug Information, Vol. 12, No 4, 1998 Proposed INN List 80
avasimibum avasimibe
avasimibe
avasimiba
2,6-diisopropylphenyl[(2,4,6-triisopropylphenyl)acetyl]sulfamate antihyperlipidaemic
[[2,4,6-tris(1-méthyléthyl)phényl]acétyl]sulfamate de 2,6-bis-(1-méthyléthyl)phényle antihyperlipidémiant
[(2,4,6-trisopropilfenil)acetil]sulfamato de 2,6-diisopropilfenilo antihiperlipémico
166518-60-1
bexarotenum bexarotene
bexarotène
bexaroteno
p-[1-(5,6,7,8-tetrahydra-3,5,5,8,8-pentamethyl-2-naphthyl)vinyl]benzoic acid antineoplastic, antidiabetic
acide 4-[1-(3,5,5,8,8-pentaméthyl-5,6,7,8-tétrahydronaphtalén-2-yl)éthényl]= benzoïque antinéoplasique, antidiabétique
ácido p-[1-(5,6,7,8-tetrahidro-3,5,5,8,8-pentametil-2-naftil)vinil]benzoico antineoplásico, antidiabético
C24H28O2 153559-49-0
carabersatum carabersat
carabersate
carabersato
N-[(3R,4S)-6-acetyl-3-hydroxy-2,2-dimethyl-4-chromanyl]-p-fluorobenzamide anticonvulsant
N-[(3R,4S)-6-acétyl-3-hydroxy-2,2-diméthyl-3,4-dihydro-2H-chromén-4-yl]-4-fluorobenzamide anticonvulsivant
N-[(3R,4S)-6-acetil-3-hidróxi-2,2-dimetil-4-cromanil]-p-fluorobenzamida anticonvulsiveo
C29H43NO4S
255

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
C 2 0 H 2 0 F N O 4 184653-84-7
caspofunginum caspofungin
caspofungine
caspofungina
(4R,5S)-5-[(2-aminoethyl)amino]-N2-(10,12-dimethyltetradecanoyl)-4-hydroxy-L-ornithyl-L-threonyl-trans-4-hydroxy-L-prolyl-(S)-4-hydroxy-4-(p-hydroxyphenyl)-L-threonyl-threo-3-hydroxy-L-ornithy[-trans-3-hydroxy-L-proline cyclic (6→1 )-peptide antifungal
N-[(2R,6S,9S,11R,12S,14aS,15S,20S,23S,25aS)-12-[(2-aminoéthyl)amino]-20-[(1R)-3-amino-1-hydroxypropyl]-23-[(1S,2S)-1,2-dihydroxy-2-(4-hydroxyphényl)éthyl]-2,11,15-trihydroxy-6-[(1R)-1-hydroxyéthyl]-5,8,14,19,22,25-hexaoxotétracosahydro-1H-dipyrrolo[2,1-c:2',1'-/]= [1,4,7,10,13,16]hexaazacyclohénicosén-9-yl]-10,12-diméthyltétradécamide antifongique
(4R,5S)-5-[(2-aminoetil)amino]-N2-(10,12-dimetiltetradecanoil)-4-hidroxi-L-ornitil-L-treonil-trans-4-hydroxy-L-prolil-(S)-4-hidroxi-4-(p-hidroxifenil)-L-treonil-treo-3-hidroxi-L-ornitil-trans-3-hidroxi-L-prolina, péptido cíclico (6→1 ) antifùngico
C52H88N10O15 162808-62-0
256
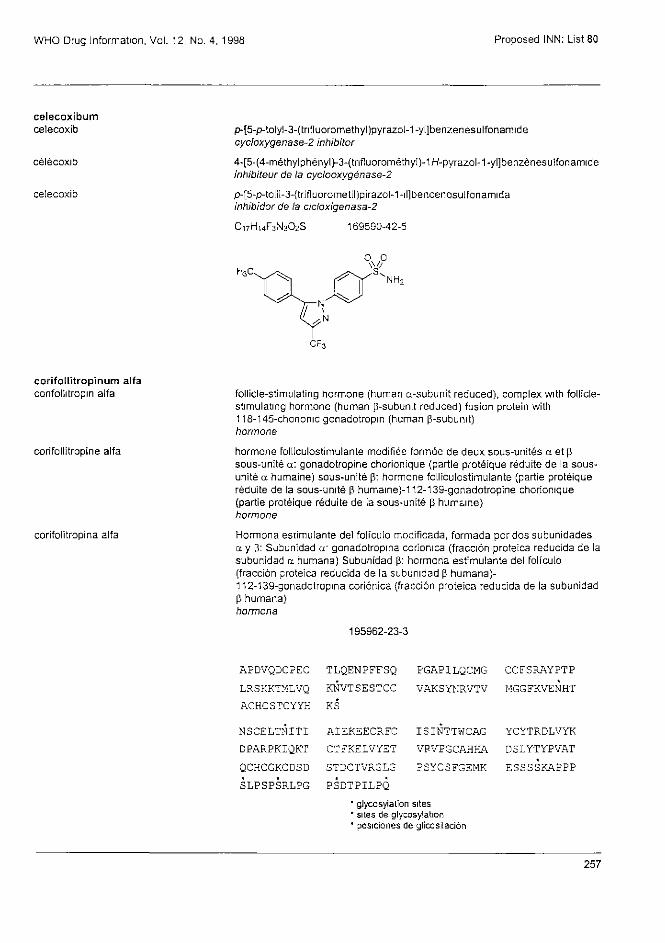
WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
celecoxibum
celecoxib
célécoxib
celecoxib
p-[5-p-tolyl-3-(trifluoromethyl)pyrazol-1-yl]benzenesulfonamide cycloxygenase-2 inhibitor
4-[5-(4-méthylphényl)-3-(trifluorométhyI)-1H-pyrazol-1-yl]benzènesulfonamide inhibiteur de la cyclooxygénase-2
p-[5-p-toliI-3-(trifluorometil)pirazol-1-il]bencenosulfonamida inhibidor de la cicloxigenasa-2
C17H14F3N3O2S 169590-42-5
corifollitropinum alfa corifollitropin alfa
corifollitropine alfa
corifolitropina alfa
follicle-stimulating hormone (human α-subunit reduced), complex with follicle-stimulating hormone (human β-subunit reduced) fusion protein with 118-145-chorionic gonadotropin (human β-subunit) hormone
hormone folliculostimulante modifiée formée de deux sous-unités α et β sous-unité α: gonadotropine chorionique (partie protéique réduite de la sous-unité α humaine) sous-unité β: hormone folliculostimulante (partie protéique réduite de la sous-unité β humaine)-112-139-gonadotropine chorionique (partie protéique réduite de la sous-unité β humaine) hormone
Hormona estimulante del folículo modificada, formada por dos subunidades α y β: Subunidad α' gonadotropina corionica (fracción proteica reducida de la subunidad α humana) Subunidad β: hormona estimulante del folículo (fracción proteica reducida de la subunidad β humana)-112-139-gonadotropina coriónica (fracción proteica reducida de la subunidad β humana) hormona
257
APDVQDCPEC TLQENPFFSQ PGAPILQCMG CCFSRAYPTP LRSKKTMLVQ KNVTSESTCC VAKSYNRVTV MGGFKVENHT ACHCSTCYYH KS
NSCELTNITI AIBKEECRFC ISINTTWCAG YCYTRDLVYF DPARPKIQKT CTFKELVYET VPVPGCAHHA DSLYTYPVAT QCHCGKCDSD STDCTVRGLG PSYCSFGEMK ESSSSKAPPP SLPSPSRLPG PSDTPILPQ
* glycosylation sites * sites de glycosylation * posiciones de glicosilación
195962-23-3

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
darbufelonum darbufelone
darbufélone
darbufelona
5-[(Z)-3,5-di-tert-butyl-4-hydroxybenzylidene]-2-imino-4-thiazolidinone anti-inflammatory agent
(Z)-5-[3,5-bis(1,1-diméthyéthyl)-4-hydroxybenzylidène]-2-iminothiazolidin-4-one anti-inflammatoire
5-[(Z)-3,5-di-terc-butil-4-hidroxibencilideno]-2-imino-4-tiazolidinona antiinflamatorio
depreotidum depreotide
dépréotide
depreotida
cyclo(L-homocysteinyl-N-methyl-L-phenylalanyl-L-tyrosyl-D-tryptophyl-L-lysyl-L-valyl),(1→1')-sulfide with 3-(2-mercaptoacetamido)-L-alanyl-L-lysyl-L-cysteinyl-L-lysinamide diagnostic agent
(1→1')-sulfure de cyclo[L-homocystéinyi-(N-méthyl-L-phénylalanyl)-L-tyrosyl-D-tryptophyl-L-lysyl-L-valyl] et de[3-[(sulfanylacétyl)amino]-L-alanyl]-L-lysyl-L-cystéinyl-L-lysinamide produit à usage diagnostique
(1→1')-sulfuro de ciclo[L-homocisteinil-(N-metil-L-fenilalanil)-L-tirosil-D-triptofil-L-lisil-L-valilo] y 3-(2-mercaptoacetamido)-L-alanil-L-lisil-L-cisteinil-L-lisinamida agente de diagnóstico
C65H96N16O12S2 161982-62-3
deracoxibum deracoxib
déracoxib
deracoxib
p-[3-(difluoromethyl)-5-(3-fluoro-4-methoxyphenyl)pyrazol-1 -yl]benzenesulfonamide cycloxygenase-2 inhibitor
4-[3-(difluorométhyl)-5-(3-fluoro-4-méthoxyphényl)-1H-pyrazol-1-yl]benzènesulfonamide inhibiteur de la cyclooxygénase-2
p-[3-(difluorometil)-5-(3-fluoro-4-metoxifenil)pirazol-1-il]bencenosulfonamida inhibidor de la cicloxigenasa-2
258
C 1 8 H 2 4 N 2 O 2 S 139226-28-1

WHO Drug Information, Vol 12, No 4, 1998 Proposed INN: List 80
C17H14F3N3O3S 169590-41-4
desloratadinum desloratadine
desloratadine
desloratadina
8-chloro-6,11-dihydro-11-(4-piperidylidene)-5H-benzo[5,6]cyclohepta-[1,2-b]pyridine histamine-H1 receptor antagonist
8-chloro-11-(pipéridin-4-ylidène)-6,11-dihydro-5H-benzo[5,6]cyclohepta-[1,2-b]pyridine antagoniste des récepteurs H1 de l'histamine
8-cloro-6,11-dihidro-11-(4-piperidilideno)-5H-benzo[5,6]ciclohepta-[1,2-b]piridina antagonista de los receptores H1 de la histamina
C19H19CIN2 100643-71-8
desmoteplasum desmoteplase
desmotéplase
desmoteplasa
plasminogen activator (Desmodus rotundus, isoform α1 protein moiety reduced) plasminogen activator
activateur du plasminogène (Desmodus rotondus, isoforme α1, partie protéique réduite) activateur du plasminogène
activador del plasminógeno (isoforma α1, fracción proteica reducida de Desmodus rotundus) activador del plasminógeno
145137-38-8
259
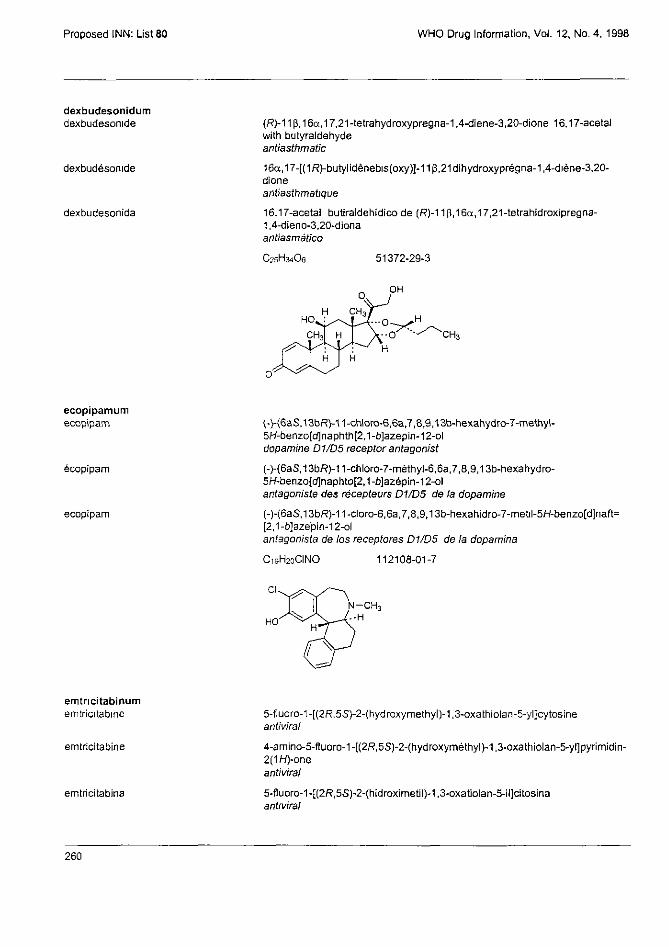
Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
dexbudesonidum dexbudesonide
dexbudésonide
dexbudesonida
(R)-11β,16α,17,21-tetrahydroxypregna-1,4-diene-3,20-dione 16,17-acetal with butyraldehyde antiasthmatic
16α,17-[(1R)-butylidènebis(oxy)]-11ββ21dihydroxyprégna-1,4-diène-3,20-dione antiasthmatique
16,17-acetal butiraldehídico de (R)-11β,16α,17,21-tetrahidroxipregna-1,4-dieno-3,20-diona antiasmático
C25H34O6
ecopipamum ecopipam
ecopipam
ecopipam
(-)-(6aS,13bR)-11-chloro-6,6a,7,8,9,13b-hexahydro-7-methyl-5H-benzo[d]naphth[2,1-b]azepin-12-ol dopamine D1/D5 receptor antagonist
(-)-(6aS,13bR)-11-chloro-7-méthyl-6,6a,7,8,9,13b-hexahydro-5H-benzo[d]naphto[2,1-b]azépin-12-ol antagoniste des récepteurs D1/D5 de la dopamine
(-)-(6aS,13bR)-11-cloro-6,6a,7,8,9,13b-hexahidro-7-metil-5H-benzo[d]naft= [2,1-b]azepin-12-ol antagonista de los receptores D1/D5 de la dopamina
C19H20ClNO 112108-01-7
emtricitabinum emtricitabine
emtricitabine
emtricitabina
5-fluoro-1-[(2R,5S)-2-(hydroxymethyl)-1,3-oxathiolan-5-yl]cytosine antiviral
4-amino-5-fluoro-1-[(2R,5S)-2-(hydroxyméthyl)-1,3-oxathiolan-5-yl]pyrimidin-2(1H)-one antiviral
5-fluoro-1-[(2R,5S)-2-(hidroximetil)-1,3-oxatiolan-5-il]citosina antiviral
260
51372-29-3
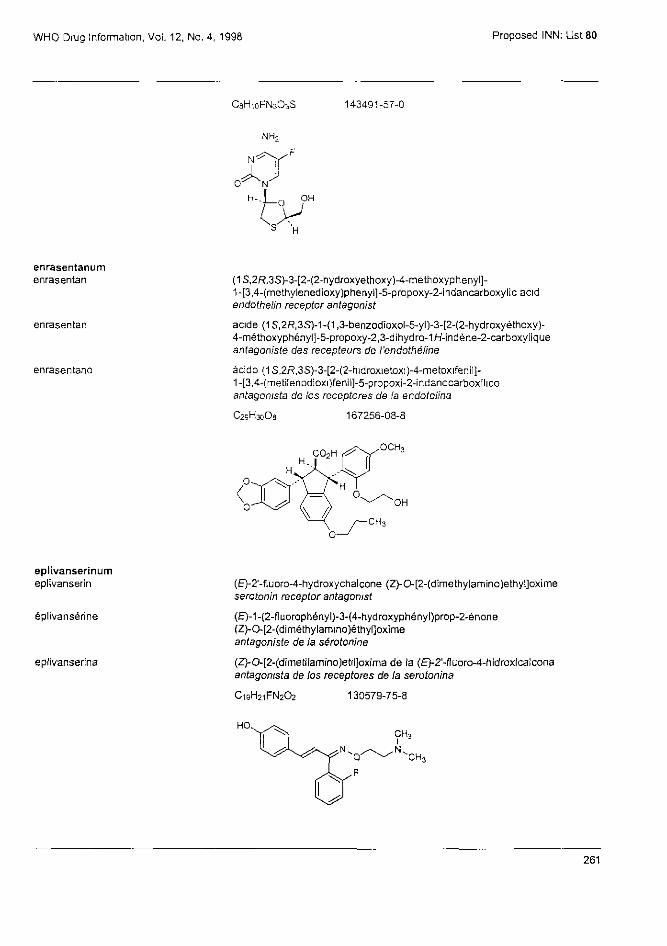
WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
C8H10FN3O3S 143491-57-0
enrasentanum enrasentan
enrasentan
enrasentano
(1S,2R,3S)-3-[2-(2-hydroxyethoxy)-4-methoxyphenyl]-1-[3,4-(methylenedioxy)phenyl]-5-propoxy-2-indancarboxylic acid endothelin receptor antagonist
acide (1S,2R,3S)-1-(1,3-benzodioxol-5-yl)-3-[2-(2-hydroxyéthoxy)-4-méthoxyphényl]-5-propoxy-2,3-dihydro-1H-indène-2-carbaxylique antagoniste des récepteurs de l'endothéline
ácido (1S,2R,3S)-3-[2-(2-hidroxietoxi)-4-metoxifenil]-1-[3,4-(metilenodioxi)fenil]-5-propoxi-2-indanocarboxilico antagonista de los receptores de la endotelina
C29H30O9 167256-08-8
eplivanserinum eplivanserin
éplivansérine
eplivanserina
(E)-2'-fluoro-4-hydroxychalcone (Z)-O-[2-(dimethylamino)ethyl]oxime serotonin receptor antagonist
(E)-1-(2-fluorophényl)-3-(4-hydroxyphényl)prop-2-énone (Z)-O-[2-(diméthylamino)éthyl]oxime antagoniste de la sérotonine
(Z)-O-[2-(dimetilamino)etil]oxima de la (E)-2'-fluoro-4-hidroxicalcona antagonista de los receptores de la serotonina
C19H21FN2O2 130579-75-8
261

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
ethylcellulosum
ethylcellulose
éthylcellulose
etilcelulosa
cellulose ethyl ether pharmaceutical aid
éther éthylique de cellulose auxiliaire pharmaceutique
éter etílico de celulosa excipiente
9004-57-3
etilevodopum
etilevodopa
étilévodopa
etilevodopa
(-)-3,4-dihydroxy-L-phenylalanine, ethyl ester antiparkinsonian
(-)-(2S)-2-amino-3-(3,4-dihydroxyphényl)propanoate d'éthyle antiparkinsonian
éster etílico de (-)-3,4-dihidroxi-L-fenilalanina antiparkinsoniano
C11H15NO4 37178-37-3
exisulindum exisulind
exisulind
exisulind
5-fluoro-2-methyl-1-[(Z)-p-(methylsulfonyl)benzylidene]indene-3-acetic acid antineoplastic
acide 2-[5-fluoro-2-méthyl-1-[(Z)-4-(méthylsulfonyl)benzylidéne]-1H-indén-3-yl]acétique antinéoplasique
ácido 5-fluoro-2-metil-1-[(Z)-p-(metilsulfonil)bencilideno]indeno-3-acético antineoplásico
C20H17FO4S
262
59973-80-7
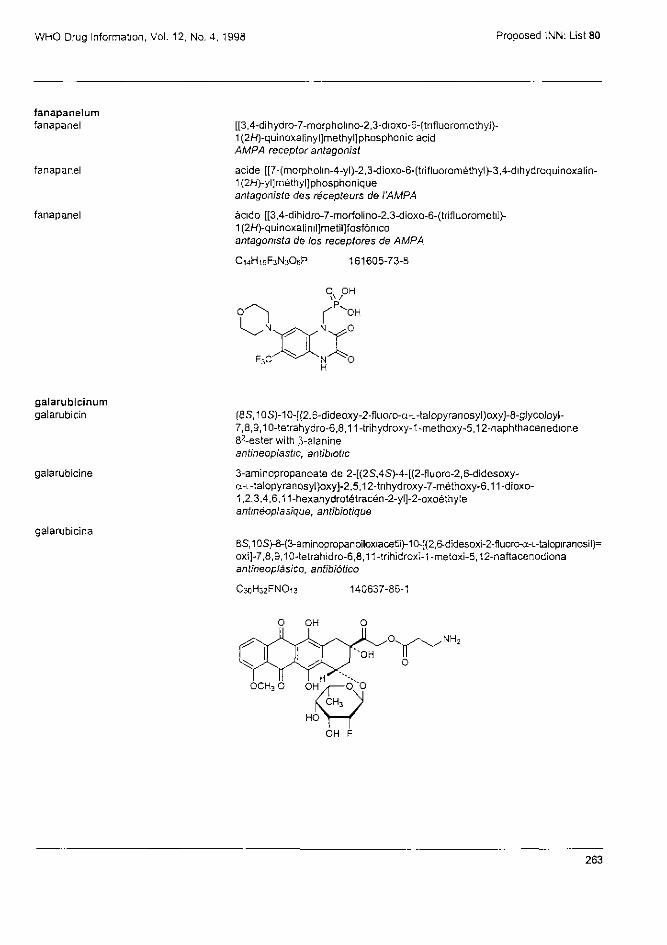
WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
fanapanelum fanapanel
fanapanel
fanapanel
[[3,4-dihydro-7-morpholino-2,3-dioxo-6-(trifluoromethyl}-1(2H)-quinoxalinyl]methyl]phosphonic acid AMPA receptor antagonist
acide [[7-(morpholin-4-yl)-2,3-dioxo-6-(trifluorométhyl)-3,4-dihydroquinoxalin-1(2H)-yl]méthyl] phosphonique antagoniste des récepteurs de l'AMPA
ácido [[3,4-dihidro-7-morfolino-2,3-dioxo-6-(trifluorometiI)-1(2H)-quinoxalinil]metil]fasfónico antagonista de los receptores de AMPA
C14H15F3N3O6P 161605-73-8
ga la rub ic inum galarubicin
galarubicine
galarubicina
(8s,10S)-10-[(2,6-dideoxy-2-fluoro-α-L-talopyranosyl)oxy]-8-glycoloyl-7,8,9,10-tetrahydro-6,8,11-trihydroxy-1-methoxy-5,12-naphthacenedione 82-ester with β-alanine antineoplastic, antibiotic
3-aminopropanoate de 2-[(2S,4S)-4-[(2-fluoro-2,6-didesoxy-α-L-talopyranosyl)oxy]-2,5,12-trihydroxy-7-méthoxy-6,11-dioxo-1,2,3,4,6,11-hexahydrotétracén-2-yl]-2-oxoéthyle antinéoplasique, antibiotique
(8S,10S)-8-(3-aminopropanoiloxiacetiI)-10-[(2,6-didesoxi-2-fluoro-α-L-talopiranosil)= oxi]-7,8,9,10-tetrahidro-6,8,11-trihidroxi-1-metoxi-5,12-naftacenodiona antineoplásico, antibiótico
C30H32FNO13 140637-86-1
263

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
gantofibanum gantofiban
gantofiban
gantofibán
4-[[(5R)-3-[p-(carboxyamidino)phenyl]-2-oxo-5-oxazolidinyl]methyl]-1-piperazineacetic acid, 1-ethyl methyl ester fibrinogen receptor antagonist
2-[4-[[(5R)-3-[4-[(méthoxycarbonyl)carbamimidoyl]phényl]-2-oxooxazolidin-5-yl]méthyl]pipérazin-1-yl]acétate d'éthyle antagoniste du récepteur du fibrinogène
4-[(5R)-3-[(4-metoxicarbonilaminoiminometil)fenil]-2-oxo-5-oxazolidinilmetil]-1-piperazinilacetato de etilo antagonista del receptor del fíbrinógeno
C21H29N5O6 183547-57-1
gimeracilum
gimeracil
giméracil
gimeracilo
5-chloro-2,4-pyridinediol adjuvant for antineoplastic
5-chloropyridine-2,4-diol adjuvant d'antinéoplasiques
5-cloro-2,4-piridinadiol coadyuvante del tratamiento con antineoplásicos
103766-25-2
OH
hemoglobinum glutamerum hemoglobin glutamer
hémoglobine glutamère
hemoglobina glutámero
hemoglobin glutamer; the species specifity should be indicated in brackets behind the name, "(bovine)"; the average mass of the polymer is given as e.g., hemoglobin glutamer-250 for 250kD oxygen carrier
produit de la réaction du pentanedial avec l'hémoglobine; l'origine de l'hémoglobine doit être indiquée, "(bovine)"; la masse moléculaire moyenne doit être donnée, par exemple: hémoglobine glutamère-250 pour 250 kD porteur d'oxygène
hemoglobina polimerizada con glutaraldehído; debe indicarse entre paréntesis el origen del material, "(bovino)"; la masa del polímero medio se da como, por ej., hemoglobina glutamero-250 para 250kD portador de oxigeno
C5H4CINO2
264

WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
hyetellosum
hyetellose
hyétellose
hietelosa
cellulose 2-hydroxyethyl ether pharmaceutical aid
éther 2-hydroxyéthylique de cellulose auxiliaire pharmaceutique
éter 2-hidroxietilico de celulosa excipiente
hymetellosum
hymetellose
hymétellose
himetelosa
cellulose 2-hydroxyethyl methyl ether pharmaceutical aid
éther 2-hydroxyéthylique et méthylique de cellulose auxiliaire pharmaceutique
éter2-hidroxilico metílico de celulosa excipiente
hyprolosum
hyprolose
hyprolose
hiprolosa
cellulose 2-hydroxypropyl ether pharmaceutical aid
éther 2-hydroxypropylique de cellulose auxiliaire pharmaceutique
éter 2-hidroxipropiIico de celulosa excipiente
insulinum detemirum
insulin determir
insuline détémir
insulina detemir
298-(N6-myristoyl-L-lysine)-308-de-L-threonineinsulin (human) antidiabetic
298-(N6-tétradécanoyl-L-lysine)-308-dès-L-thréonineinsuline humaine antidiabétique
298-(N6-miristoil-L-lisina)-308-des-L-treoninainsulina (humana) antidiabético
265
9004-64-2
9032-42-2
9004-62-0

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
C267H402N64O76S6 169148-63-4
itavastatinum itavastatin
itavastatine
itavastatina
(3R,5S,6E)-7-[2-cyclopropyl-4-(p-fluorophenyl)-3-quinolyl]-3,5-dihydroxy-6-heptenoic acid antihyperlipidaemic
acide (6E)-(3R,5S)-7-[2-cyclopropyl-4-(4-fluorophényl)quinoléin-3-yl]-3,5-dihydroxyhept-6-énoïque antihyperlipidémíant
ácido (3R,5S,6E)-7-[2-cicloclopropil-4-(p-fluorofenil)-3-quinolil]-3,5-dihidroxi-6-heptenoico antihiperlipémico
C25H24FNO4 147511-69-1
leridistimum leridistim
léridistim
leridistim
14-L-alanine-50-L-aspartic acid-14-125-interleukin 3 (human reduced) fusion protein with peptide (synthetic) linked with 17-L-serinegranulocyte colony-stimulating factor (human reduced) immunomodulator
protéine de fusion entre la [14-L-alanine-50-acide L-aspartique]-14-125-interleukine 3 (humaine, réduite) et le [17-L-sérine]facteur de stimulation des colonies de granulocytes (humain, réduit) immunomodulateur
proteína de fusión de la [14-L-alanina-50-ácido L-aspártico]-14-125-interleucina-3 (humana reducida) con el [17-L-serina]factor de estimulación de las colonias de granulocitos (humano reducido) inmunomodulador
266
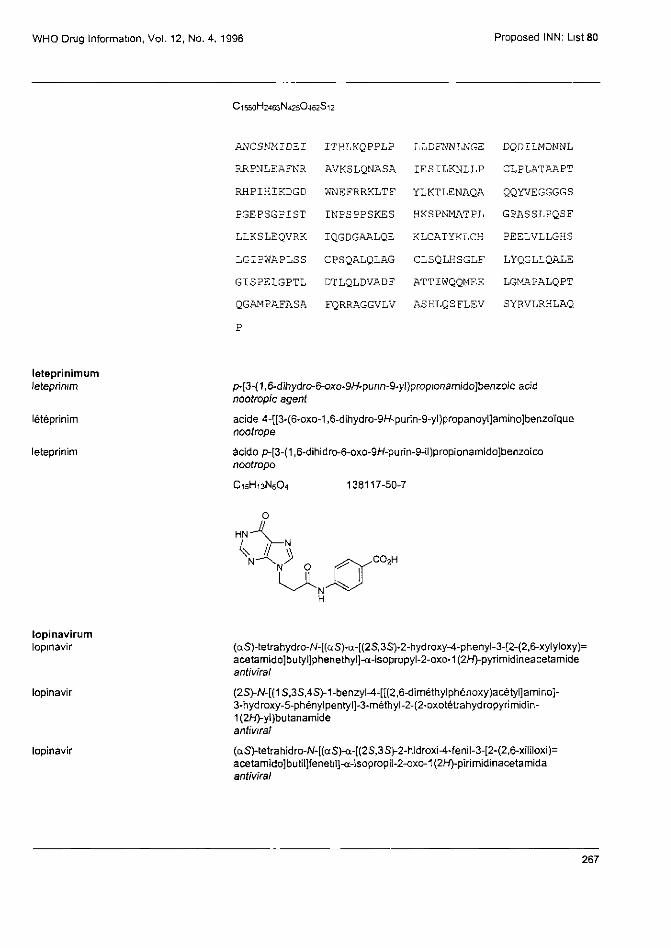
WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
C 1 5 5 0 H 2 4 6 3 N 4 2 5 O 4 6 2 S 1 2
ANCSNMIDEI ITHLKQPPLP LLDFNNLNGE DQDILMDNNL
RRPNLEAFNR AVKSLQNASA IESILKNLLP CLPLATAAPT
RHPIHIKDGD WNEFRRKLTF YLKTLENAQA QQYVEGGGGS
PGEPSGPIST INPSPPSKES HKSPNMATPL GPASSLPQSF
LLKSLEQVRK IQGDGAALQE KLCATYKLCH PEELVLLGHS
LGIPWAPLSS CPSQALQLAG CLSQLHSGLF LYQGLLQALE
GISPSLGPTL DTLQLDVADF ATTIWQQMEE LGMAPALQPT
QGAMPAFASA FQRRAGGVLV ASHLQSFLEV SYRVLRHLAQ
leteprinimum
leteprinim
leteprinim
leteprinim
p-[3-(1,6-dihydro-6-oxo-9H-purin-9-yl)propionamido]benzoic acid nootropic agent
acide 4-[[3-(6-oxo-1,6-dihydro-9H-purin-9-yl)propanoyl]amino]benzoïque nootrope
ácido p-[3-(1,6-dihidro-6-oxo-9H-purin-9-il)propionamido]benzoico nootropo
C 1 5 H 1 3 N 5 O 4 138117-50-7
lopinavirum lopinavir
lopinavir
lopinavir
(αS)-tetrahydro-N-[(αS)-α-[(2S,3S)-2-hydroxy-4-phenyl-3-[2-(2,6-xylyloxy)= acetamido]butyl]phenethyl]-α-isopropyl-2-oxo-1(2H)-pyrimidineacetamide antiviral
(2S)-N-[(1S,3S,4S)-1-benzyl-4-[[(2,6-diméthylphénoxy)acétyl]amino]-3-hydroxy-5-phénylpentyl]-3-méthyl-2-(2-oxotètrahydropyrirnidin-1(2H)-yl)butanamide antiviral
(αS)-tetrahidro-N-[(αS)-α-[(2S,3S)-2-hidroxi-4-fenil-3-[2-(2,6-xililoxi)= acetamido]butil]fenetil]-α-isopropil-2-oxo-1(2H)-pirimidinacetamida antiviral
267

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
C37H48N4O5 192725-17-0
lusupultidum lusupultide
lusupultide
lusupultida
glycyl-L-isoleucyl-L-prolyl-L-phenylalanyl-L-phenylalanyl-L-prolyl-L-valyl-L-histidyl-L-leucyl-L-lysyl-L-arginyl-L-leucyl-L-leucyl-L-isoleucyl-L-valyl-L-valyl-L-valyl-L-valyl-L-valyl-L-valyl-L-leucyl-L-isoleucyl-L-valyl-L-valyl-L-vaIyl-L-isoleucyl-L-valylglycyl-L-alanyl-L-leucyl-L-leucyl-L-isoleucylglycyl-L-leucine pulmonary surfactant
glycyl-L-isoleucyl-L-prolyl-L-phénylalanyl-L-phénylalanyl-L-proIyl-L-valyl-L-histidyl-L-leucyl-L-lysyl-L-arginyl-L-leucyl-L-leucyl-L-isoleucyl-L-valyl-L-valyl-L-valyl-L-valyl-L-valyl-L-valyl-L-leucyl-L-isoleucyl-L-valyl-L-valyl-L-valyl-L-isoleucyl-L-valyl-glycyl-L-alanyl-L-leucyl-L-leucyl-L-isoleucyl-glycyl-L-leucine surfactif pulmonaire
glycil-L-isoleucil-L-prolil-L-fenilalanil-L-fenilalanil-L-prolil-L-valil-L-histidil-L-leucil-L-lisil-L-arginil-L-leucil-L-leucil-L-isoleucil-L-valil-L-valil-L-valil-L-valil-L-valil-L-valil-L-leucil-L-isoleucil-L-valil-L-valil-L-valil-L-isoleucil-L-valilglicil-L-alanil-L-leucil-L-leucil-L-isoleucilglicil-L-leucina tensioactivo pulmonar
C182H310N40O35 200074-80-2
Gly—Ile—Pro—Phe—Phe—Pro—Val—His—Leu—Lys— 10
Arg—Leu—Leu—Ile—Val—Val—Val—Val—Val—Val — 20
Leu—Ile—Val—Val—Val—Ile—Val—Gly—Ala—Leu— 30
Leu—Ile—Gly—Leu
maribavirum maribavir
maribavir
maribavir
5,6-dichloro-2-(isopropyIamino)-1-β-L-ribofuranosylbenzimidazole antiviral
5,6-dichloro-N-(1-méthyléthyl)-1-(β-L-ribofuranosyl)-1H-benzimidazol-2-amine antiviral
5,6-dicloro-2-(isopropilamino)-1-β-L-ribofuranosilbenzimidazol antiviral
268

WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
C 1 5 H 1 9 C l 2 N 3 O 4
minopafantum minopafant
minopafant
minopafant
(+)-1-ethyl-2-[[N-[[(2R)-2-methoxy-3-[[[4-octadecylcarbamoyl)oxy]piperidino] carbonyl]oxy]propoxy]carbanyl]-o-anisamido]methyl]pyridiniurn chloride platelet activating factor antagonist
(+)-chlorure de 1-éthyl-2-[[(2-méthoxybenzoyl)[[(2R)-2-méthoxy-3-[[[4-[(octadécylcarbamoyl)oxy]pipérídin-1-yl]carbonyl]oxy]propoxy]= carbonyl]amino]méthyl]pyridinium antagoniste du facteur activant les plaquettes
(+)-1-etil-2-[[N-[[(2R)-2-metoxi-3-[[[4-[(octadecilcarbamoil)oxi]piperidino]= carbonil]oxi]propoxi]carbonil]-o-anisamido]metil]piridinio antagonista del factor de activación de plaquetas
C46H73ClN4O9 128420-61-1
minretumomabum minretumomab
minrétumomab
minretumomab
immunoglobulin G1 anti-(human tumor-associated glycoprotein 72) (mouse monoclonal Mab CC-49 γ1-chain), disulfide with mouse monoclonal Mab CC-49-chain, dimer immunomodulator
immunoglobuline G1 anti-(glycoprotéine 72 humaine associée aux turneurs) (chaîne γ1 de l'anticorps monoclonal de souris Mab CC-49), dimère du disulfure avec la chaîne Κ de l'anticorps monoclonal de souris Mab CC-49 immunomodulateur
Inmunoglobulina G1 anti-(glicoproteina 72 humana asociada a los tumores) (cadena γ1 del anticuerpo monoclonal de ratón Mab CC-49), dímero del disulfuro con la cadena Κ del anticuerpo monoclonal de ratón Mab CC-49 inmunomodulador
269
176161-24-3
195189-17-4
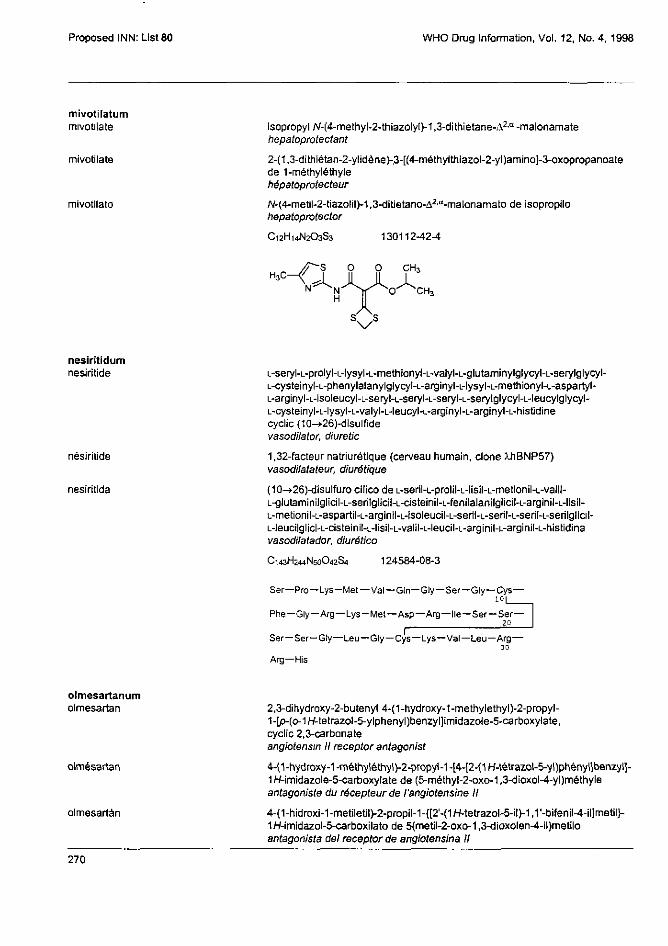
Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
mivotilatum mivotilate
mivotilate
mivotilato
isopropyl N-(4-methyl-2-thiazolyl)-1,3-dithietane-Δ2,α -malonamate hepatoprotectant
2-(1,3-dithiétan-2-ylidène)-3-[(4-métriylthiazol-2-yl)amino]-3-oxopropanoate de 1-méthyléthyle hépatoprotecteur
N-(4-metil-2-tiazolil)-1,3-ditietano-Δ2,α-malonamato de isopropilo hepatoprotector
C12H14N2O3S3 130112-42-4
nesiritidum nesiritide
nésiritide
nesiritida
L-seryl-L-prolyl-L-lysyl-L-methionyl-L-valyl-L-glutaminylglycyl-L-serylglycyl-L-cysteinyl-L-phenylalanylglycyl-L-arginyl-L-lysyl-L-methionyl-L-aspartyl-L-arginyl-L-isoleucyl-L-seryl-L-seryl-L-seryl-L-serylglycyl-L-leucylglycyl-L-cysteinyl-L-lysyl-L-valyl-L-leucyl-L-arginyl-L-arginyl-L-histidine cyclic (10→26)-disulfide vasodilator, diuretic
1,32-facteur natriurétique (cerveau humain, clone λhBNP57) vasodilatateur, diurétique
(10→26)-disulfuro cilico de L-seril-L-prolil-L-lisil-L-metionil-L-valil-L-glutaminilglicil-L-serilglicil-L-cisteinil-L-fenilalanilglicil-L-arginil-L-lisil-L-metionil-L-aspartil-L-arginil-L-isoleucil-L-seril-L-seril-L-seril-L-serilglicil-L-leucilglicl-L-cisteinil-L-lisil-L-valil-L-leucil-L-arginil-L-arginil-L-histidina vasodilatador, diurético
C 1 4 3 H 2 4 4 N 5 0 O 4 2 S 4 124584-08-3
Ser—Pro—Lys—Met—Val—Gln—Gly—Ser—Gly—Cys— 10
Phe—Gly—Arg—Lys-Met—Asp—Arg—Ile—Ser—Ser— 20
oImesartanum olmesartan
olmésartan
olmesartán
2,3-dihydroxy-2-butenyl 4-(1-hydroxy-1-methylethyl)-2-propyl-1-[p-(o-1H-tetrazol-5-ylphenyl)benzyl]imidazole-5-carboxylate, cyclic 2,3-carbonate angiotensin II receptor antagonist
4-(1-hydroxy-1-méthyléthyl)-2-propyl-1-[4-[2-(1H-tétrazol-5-yl)phényl]benzyl]-1H-imidazole-5-carboxylate de (5-méthyl-2-oxo-1,3-dioxol-4-yl)méthyle antagoniste du récepteur de l'angiotensine II
4-(1-hidroxi-1-metiletil)-2-propil-1-[[2-(1H-tetrazol-5-il)-1,1'-bifenil-4-il]metil]-1H-imidazol-5-carboxilato de 5(metil-2-oxo-1,3-dioxolen-4-il)metilo antagonista del receptor de angiotensina II
270
Ser —Ser-Gly—Leu—Gly—Cys—Lys—Val—Leu—Arg— 30
Arg—His

WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
C29H30N6O6 144689-63-4
oseltamivirum oseltamivir
oséltamivir
oseltamivir
ethyl (3R,4R,5S)-4-acetamido-5-amino-3-(1-ethylpropoxy)-1-cyclohexene-1-carboxylate antiviral
(3R,4R,5S)-4-(acétylamino)-5-amino-3-(1-éthylpropoxy)cyclohex-1-ène-1-carboxylate d'éthyle antiviral
(3R,4R,5S)-4-acetamido-5-amino-3-(1-etilpropoxi)-1-ciclohexeno-1-carboxilato de etilo antiviral
oteracilum
oteracil
otéracíl
oteracilo
1,4,5,6-tetrahydro-4,6-dioxo-s-triazine-2-carboxylic acid antineoplastic
acide 4,6-dioxo-1,4,5,6-tétrahydro-1,3,5-triazine-2-carboxylique antinéoplasique
ácido 1,4,5,6-tetrahidro-4,6-dioxo-s-triazina-2-carboxílico antineoplásico
937-13-3
271
C16H28N2O4 196618-13-0
C1H3N3O4

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1996
parecoxibum
parecoxib
parécoxib
parecoxib
N-[[p-(5-methyl-3-phenyl-4-isoxazolyl)phenyl]sulfonyl]propionamide cycloxygenase-2 inhibitor
N-[[4-(5-méthyl-3-phénylisoxazol-4-yl)phényl]sulfonyl]propanamide inhibiteur de la cyclooxygénase-2
N-[[p-(5-metil-3-fenil-4-isoxazolil)fenil]sulfonil]propionamida inhibidor de la cicloxigenasa-2
C19H18N2O4S 198470-84-7
pegacaristimum pegacaristim
pégacaristim
pegacaristim
N-(3-hydroxypropyl)-1-163-megakaryocyte growth and development factor (human), monoether with polyethylene glycol monomethyl ether colony stimulating factor
N-[3-[[méthylpoly(oxyéthylène)]oxy]propyl]-1-163-facteur de croissance et de développement de mégakaryocyte (humain) facteur stimulant de colonies de mégakaryocytes
N-(3-hidroxipropil)-1-163-factor de desarrollo y crecimiento de megacariocitos (humano), monoéter con el éter monometilico de polietilenglicol factor estimulante de colonias
* pegylation site * site de pégylation * posición de pegilación
187139-68-0
272

WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
pegnartograstimum pegnartograstim
pégnartograstim
pegnartograstim
N-L-methionyl-1-L-alanine-3-L-threonine-4-L-tyrosine-5-L-arginine-17-L-serine colony-stimulating factor (human clone 1034), reaction product with succinic anhydride, esters with polyethylene glycol monomethyl ether immunomodulator
esters entre le produit de réaction du N-L-méthionyl-[1-L-alanine-3-L-thréonine-4-L-tyrosine-5-L-arginine-17-L-serine] facteur de stimulation de colonie (clone humain 1034) avec l'anhydride succinique et le α-methyl-ω-hydroxypoly(oxyéthylène) immunomodulateur
ésteres con el éter monometilico de polietilenglicol del producto de reacción con anhidrido succinico del N-L-metionil-1 -L-alanina-3-L-treonina-4-L-tírosina-5-L-arginina-17-L-serina-factor-estimulante de colonias (clon humano 1034) inmunomodulador
* pegylation site * site de pegylation * posición de pegilación
ponazurilum ponazuril
ponazuril
ponazurilo
1-methyl-3-[4-[p-[(trifluoromethyl)sulfonyl]phenoxy]-m-tolyl]-s-triazine-2,4,6(1H,3H,5H)-trione coccidiostatic
1-méthyl-3-[3-méthyl-4-[4-[(triflorométhyl)sulfonyl]phénoxy]phényl]-1,3,5-triazine-2,4,6(1H,3H,5H)-trione coccidiostatique
1-metil-3-[4-[p-[(trifluorometil)sulfonil]fenoxi]-m-tolil]-s-triazina-2,4,6(1H,3H,5H)-triona coccidiostático
C18H14F3N3O6S 69004-04-2
273
204565-76-4
M
APTYRASSLP QSFFLKSLEQ VRKIQGDGAA LQEKLCATYK
LCHPEELVLL GHSLGIPWAP LSSCPSQALQ LAGCLSQLHS
GLFLYQGLLQ ALEGISPELG PTLDTLQLDV ADFATTIWQQ
MEELGMAPAL QPTQGAMPAF ASAFQRBAGG VLVASHLQSF
LEVSYRVLRH LAQP

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
rofecoxibum rofecoxib
rofecoxib
rofecoxib
4-[p-(methylsulfonyl)phenyl]-3-phenyl-2(5H)-furanone cycloxygenase-2 inhibitor
4-[4-(méthylsulfonyl)phényl]-3-phénylfuran-2(5H)-one inhibiteur de la cyclooxygénase-2
4-[p-(metilsulfonil)fenil]-3-fenil-2(5H)-furanona inhibidor de la cicloxigenasa-2
C17H14O4S 162011-90-7
sarizotanum sarizotan
sarizotan
sarizotán
(-)-3-[[[(R)-2-chromanylmethyl]amino]methyI]-5-(p-fluorophenyl)pyridine antipsychotic
(-)-N-[[(2R)-3,4-dihydro-2H-chromén-2-yl]méthyl][5-(4-fluoropriényl)pyridin-3-yl]méthanamine psychotrope
(-)-3-[[[(R)-2-cromanilmetil]amino]metil]-5-(p-fluorofenil)piridina antipsicótico
C22H21FN2O 177975-08-5
satraplatinum
satraplatin
satraplatine
satraplatino
(OC-6-43)-bis(acetato)amminedichloro(cyclohexylamine)platinum antineoplastic
(OC-6-43)-bis(acétato)amminedichloro(cyclohexanamine)platine antinéoplasique
(OC-6-43)-bis(acetato)aminadicloro(clclohexilamina )platino antineoplásico
129580-63-8
274
C10H22Cl2N2O4Pt

WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
semparatidum semparatide
semparatide
semparatida
L-alanyl-L-valyl-L-seryl-L-α-glutamyl-L-histidyl-L-glutaminyl-L-leucyl-L-leucyl-L-histidyl-L-α-aspartyl-L-lysylglycyl-L-lysyl-L-seryl-L-isoleucyl-L-glutaminyl-L-α-aspartyl-L-leucyl-L-arginyl-L-arginyl-L-arginyl-L-α-glutamyil-L-leucyl-L-leucyl-L-α-glutamyI-L-lysyl-L-leucyl-L-leucyl-L-α-glutamyl-L-lysyl-L-leucyl-L-histidyl-L-threonyl-L-alaninamide hormone analogue
L-alanyl-L-valyl-L-seryl-L-glutamyl-L-histidyl-L-glutaminyl-L-leucyl-L-leucyl-L-histidyl-L-aspartyl-L-lysyi-glycyl-L-lysyl-L-seryl-L-isoleucyl-L-glutaminyl-L-aspartyl-L-leucyl-L-arginyl-L-arginyl-L-arginyl-L-glutamyl-L-leucyl-L-leucyl-L-glutamyl-L-lysyl-L-leucyl-L-leucyl-L-glutamyl-L-lysyl-L-leucyl-L-histidyl-L-thréonyl-L-alaninamide analogue d'hormone
L-alanil-L-valil-L-seril-L-α-glutamil-L-histidil-L-glutaminil-L-leucil-L-leucil-L-histidil-L-α-aspartil-L-lisilglicil-L-lisil-L-seril-L-isoleucil-L-glutaminil-L-α-aspartil-L-leucil-L-arginil-L-arginil-L-arginil-L-α-glutamil-L-leucil-L-leucil-L-α-glutamil-L-lisil-L-leucil-L-leucil-L-α-glutamil-L-lisil-L-leucil-L-histidil-L-treonil-L-alaninamida análogo de hormona
C175H300N56O51 154906-40-8
Ala—Val—Ser —Glu—His—Gln—Leu—Leu—His—Asp— 10
Lys—Gly—Lys—Ser—Ile—Gln—Asp—Leu—Arg—Arg— 20
Arg—Glu—Leu—Leu—Glu—Lys—Leu—Leu—Glu—Lys —
Leu—His—Thr—Ala-NH2
simeticonum simeticone
siméticone
simeticona
α-(trimethylsilyI)-ω-methylpoly[oxy(dimethylsilylene)], mixture with silicon dioxide antiflatulent
mélange de α-(triméthylsilyl)-α-méthylpoly[oxy(diméthylsilylène)] et de dioxyde de silicium antiflatulent
α-(trimetilsilil)-ω-metilpoli[oxi(dimetilsilileno)], mezcla con dióxido de silicio antiflatulento
sitamaquinum
sitamaquine
sitamaquine
sitamaquina
8-[[6-(diethylamino)hexyl]amino]-6-methoxy-4-methyiquinoline antiprotozoal
N,N-diéthyl-N'-(6-méthoxy-4-méthylquinoléin-8-yl)hexane-1,6-diamine antiprotozoaire
8-[[6-(dietilamino)hexil]amino]-6-metoxi-4-metilquinolina antiprotozoario
275
8050-81-5
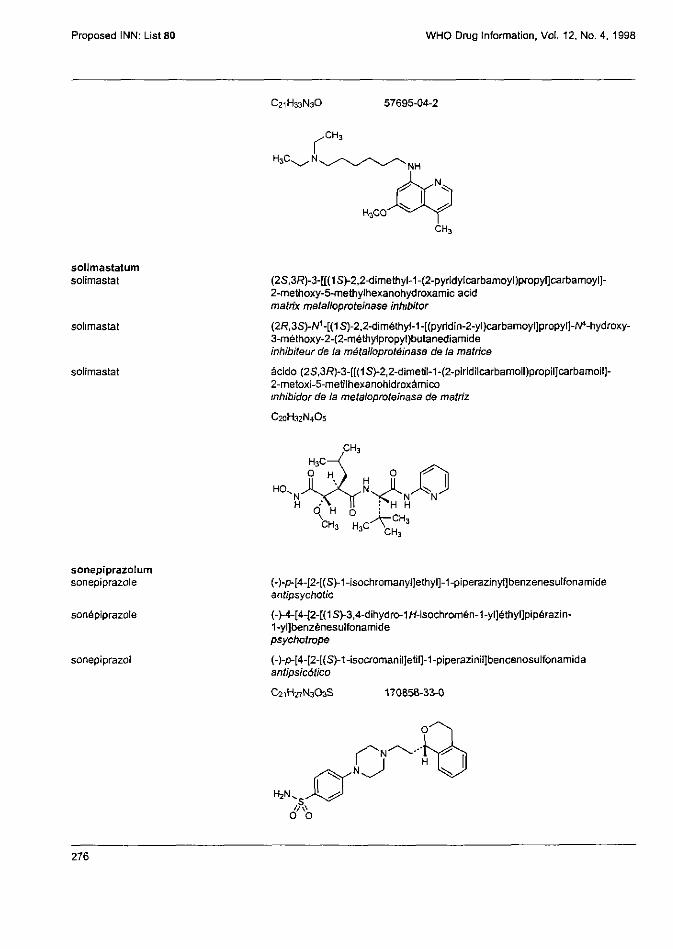
Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
solimastatum solimastat
solimastat
solimastat
(2S,3R)-3-[[(1S)-2,2-dimethyl-1-(2-pyriclylcarbamoyl)propyl]carbamoyl]-2-methoxy-5-methylhexanohydroxamic acid matrix metalloproteinase inhibitor
(2R,3S)-N1-[(1S)-2,2'-dimethyl-1-[(pyridin-2-yl]carbamoyl]propyl]-N4-hydroxy-3-méthoxy-2-(2-méthylpropyl)butanediamide inhibiteur de la métalloprotéinase de la matrice
ácido (2S,3R)-3-[[(1S)-2,2-dimetil-1-(2-piridilcarbamoil)propil]carbamoil]-2-metoxi-5-metilhexanohidroxámico inhibidor de la metaloproteinasa de matriz
C 2 0 H 3 2 N 4 O 5
sonepiprazolum sonepiprazole
sonépiprazole
sonepiprazol
(-)-p-[4-[2-[(S)-1-isochromanyl]ethyl]-1-piperazinyl]benzenesulfonamide antipsychotic
(-)-4-[4-[2-[(1S)-3,4-dihydro-1H-isochromén-1-yl]éthyl]pipérazin-1-yl]benzènesulfonamide psychotrope
(-)-p-[4-[2-[(S)-1-isocromanil]etil]-1-piperazinil]bencenosulfonamida antipsicótico
276
C21H33N3O 57695-04-2
C21H27N3O3S 170858-33-0

WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
tabimorelinum tabimorelin
tabimoréline
tabimorelina
(R)-α-[(E)-5-amino-N,5-dimethy[-2-hexenamido]-N-methyl-/V-[(R)-α-(methylcarbamoyl)phenethyl]-2-naphthalenepropionamide growth hormone release stimulating peptide
(5)-5-amino-N-[(1R)-2-[[(1R)-1-benzyl-2-(méthylamino)-2-oxoéthyl]= èthylamino]-1-(naphtalén-2-ylméthyl)-2-oxoéthyl]-N,5-diméthylhex-2-énamide peptide stimulant la libération de l'hormone de croissance
(R)-α-[(E)-5-amino-N,S-dimetil-2-hexenamido]-N-metil-N-[(R)-α-(metilcarbamoil)fenetil]-2-naftalenopropionamid péptido estimulante de la liberación de la hormona del crecimiento
C32H40N4O3 193079-69-5
tafenoquinum tafenoquine
tafénoquine
tafenoquina
(±)-8-[(4-amino-1-methylbutyl)amino]-2,6-dimethoxy-4-methyl-5-[(α,α,α-trifluoro-m-tolyl)oxy]quinoline antimalarial
(4RS)-N4-[2,6-diméthoxy-4-méthyl-5-[3-(trifluorométhy])phénoxy]quinoléin-8-yl]pentane-1,4-diamine antipaludique
(±)-8-[(4-amino-1-metilbutil)amino]-2,6-dimetoxi-4-metil-5-[(α,α,α-trifluoro-m-tolil)oxi]quinolina antipalúdico
C24H28F3N3O3 106635-80-7
and enantiomer et énantiomère y enantiómero
277

Proposed INN: List 80 WHO Drug Information. Vol. 12, No. 4, 1998
talampanelum talampanel
talampanel
talampanel
(R)-7-acetyl-5-(p-aminophenyl)-8,9-dihydro-8-methiyl-7H-1,3-dioxolo= [4,5-h] [2,3] benzodiazepine AMPA receptor antagonist
(8R)-7-acétyl-5-(4-aminophényl)-8-méthyl-8,9-dihydro-7H-1,3-dioxolo= [4,5-h][2,3]benzodiazépine antagoniste des récepteurs de l'AMPA
(R)-7-acetil-5-(p-aminofenil)-8,9-dihidro-8-metil-7H-1,3-dioxolo= [4,5-h][2,3]benzodiazepina antagonista del receptor AMPA
C19H19N3O3 161832-65-1
telithromycinum telithromycin
télithromycine
telitromicina
(3aS,4R,7R,9R,10R,11R,13R,15R,15aR)-4-ethyloctahydro-11-methoxy-3a,7,9,11,13,15-hexamethyl-1-[4-[4-(3-pyrrdyl)imidazol-1-yl]butyl]-10-[[3,4,6-trideoxy-3-(dimethylamino)-β-D-xylo-hexopyranosyl]oxy]-2H-oxacyclotetradecino[4,3-d]oxazole-2,6,8,14(1H,7H,9H)-tetrone antibiotic
(3aS,4R,7R,9R,10R,11R,13R,15R,15aR)-10-[[3-(diméthylamino)-3,4,6-tridésoxy-β-D-xylo-hexopyranosyl]oxy]-4-ethyl-11-méthoxy-3a,7,9,11,13,15-hexaméthyl-1-[4-(pyridin-3-yl)-1H-imidazol-1-yl]butyl]= octahydro-2H-oxacyclotétradécino[4,3-d]oxazole-2,6,8,14(1H,7H,9H)-tétrone antibiotique
(3aS,4R,7R,9R,10R,11R,13R,15R,15aR)-4-etiloctahidro-11-metoxi-3a,7,9,11,13,15-hexametil-1-[4-[4-(3-piridil)imidazol-1-il]butil]-10-[ [3,4,6-tridesoxy-3-(dimetilamino)-β-D-xilo-hexopiranosil]oxi]-2H-oxaciclotetradecino[4,3-d]oxazol-2,6,8,14(1H,7H,9H)-tetrona antibiótico
C43H65N5O10 173838-31-8
278

WHO Drug Information, Vol 12, No. 4, 1998 Proposed INN: List 80
tenatoprazolum tenatoprazole
ténatoprazole
tenatoprazol
(±)-5-methoxy-2-[[(4-methoxy-3,5-dimethyl-2-pyridyl)methyl]sulfinyl]-1H-imidazo[4,5-b]pyridine antiulcer agent
5-méthoxy-2-[(RS)-[(4-méthoxy-3,5-diméthylpyridin-2-yl)méthyl]sulfinyl]-1H-imidazo[4,5-b]pyridine antiulcéreux
(±)-5-metoxi-2-[[(4-metoxi-3,5-dimetil-2-piridil)metil]sulfinil]-1H-imidazol[4,5-b]piridina antiulceroso
C16H18N4O3S 113712-98-4
teriflunomidum teriflunomide
tériflunomide
teriflunomida
(Z)-2-cyano-α' α' α-trifluoro-3-hydroxy-p-crotonotoluidide antirheumatic
(Z)-2-cyano-3-hydroxy-N-[4-(trifluorométhyl)phényl]but-2-énamide antirhumatismal
(Z)-2-ciano-α' α' α-trifluoro-3-hidroxi-p-cratonotoluidida antirreumático
C12H9F3N2O3
t imcodarum timcodar
timcodar
timcodar
(S)-N-benzyl-p-chloro-α-[N-methyl-2-(3-tr imethoxyphenyl)glyoxylamido]-N-[3-(4-pyridyl)-1-[2-(4-pyridyI)etriyl]propyl]hydrocinnamamide multidrug resistance inhibitor, antineoplastic
(2S)-N-benzyl-3-(4-chlorophényl)-2-[méthyl[2-oxo-2-(3,4,5-triméthoxyphényl)acétyl]amino]-N-[3-(pyridin-4-yl)-1-[2-(pyridin-4-yl)éthyl]propyl]propanamide inhibiteur de la multirésistence aux médicaments, antinéoplasique
(S)-N-bencil-p-cloro-α-[N-metil-2-(3,4,5-trimetoxifenil)glioxilamido]= N-[3-(4-piridil)-1-[2-(4-piridil)etil]propil]hidrocinamamida inhibidor de la resistancia a multiples fármacos, antineoplástico
279
and enantiomer et énantiomère y enantiómero
108605-62-5

Proposed INN; List 80 WHO Drug Information, Vol. 12, No. 4, 1998
C43H45CIN4O6 179033-51-3
tipranavirum tipranavir
tipranavir
tipranavir
3'-[(1R)-1-[(6R)-5,6-dihydro-4-hydroxy-2-oxo-6-phenethyl-5-propyl-2H-pyran-3-yl]propyl]-5-(trifluoromethyl)-2-pyridinesulfonanilide antiviral
N-[3-[(1R)-1-[(6R)-4-hydroxy-2-oxo-6-(2-phényléthyl)-6-propyl-5,6-dihydro-2H-pyran-3-yI]propyl]phényl]-5-(trifluorométhyl)pyridine-2-sulfonamide antiviral
3'-[(1R)-1-[(6R)-5,6-dihidro-4-hidroxi-2-oxo-6-fenetil-6-propil-2H-piran-3-il]propil]-5-(trifluorometil)-2-piridinasulfonanilida antiviral
C31H33F3N2O5S 174484-41-4
tonabersatum tonabersat
tonabersate
tonabersato
N-[(3S,4S)-6-acetyl-3-hydroxy-2,2-dimethyl-4-chromanyl]-3-chloro-4-fluorobenzamide anticonvulsant
N-[(3S,4S)-6-acétyl-3-hydroxy-2,2-diméthyl-3,4-dihydro-2H-chromén-4-yl]-3-chIoro-4-fluorobenzamide anticonvulsant
N-((3S,4S)-6-acetil-3-hidroxi-2,2-dimetil-4-cromanil]-3-cloro-4-fluorobenzamida anticonvulsivo
280

WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
C20H19CIFNO4 175013-84-0
tositumomabum tositumomab
tositumomab
tositumomab
immunoglobulin G2a anti-(human antigen CD 20) (mouse monoclonal clone B1R1 γ2a-chain), disulfide with mouse monoclonal clone B1R1 λx-chain, dimer immunomodulator
immunoglobuline G2a anti-(antigène CD 20 humain) (chaîne γ2a de l'anticorps monoclonal de souris B1R1), dimère du disulfure avec la chaîne λx de l'anticorps monoclonal de souris B1R1 immunomodulateur
Inmunoglobulina G2a anti-(antigeno CD 20 humano) (cadena γ2a del anticuerpo monoclonal de ratón B1R1),dímero del disulfuro con la cadena λx del anticuerpo monoclonal de ratón B1R1 inmunomodulador
travoprostum travoprost
travoprost
travoprost
isopropyl (Z)-7-[(1R,2R,3R,5S)-3,5-dihydroxy-2-[(1E,3R)-3-hydroxy-4-[(α,α,α-trifluoro-m-toiyl)oxy]-1-butenyl]cyclopentyl]-5-heptenoate prostaglandin
(5Z)-7-[(1R,2R,3R,5S)-3,5-dihydroxy-2-[(1E)-(3R)-3-hydroxy-4-[3-(trifluorométhyl)phénoxy]but-1-ényl]cycIopentyl]hept-5-énoate de 1-méthyléthyle prostaglandins
(Z)-7-[(1R,2R,3R,5S)-3,5-dihidroxi-2-[(1E,3R)-3-hidroxi-4-[(α,α,α-trifluoro-m-tolil)oxi]-1-butenil]ciclopentil]-5-heptenoato de isopropilo prostaglandina
C26H35F3O6 157283-68-6
281
192391-48-3

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
upidosinum upidosin
upidosine
upidosina
N-[3-[4-(o-methoxyphenyl)-1-piperazinyl]propyl]-3-methyl-4-oxo-2-phenyl-4H-1-benzopyran-8-carboxamide α1-adrenoreceptor antagonist
N-[3-[4-(2-méthoxyphényl)pipérazin-1-yl]propyl]-3-méthyl-4-oxo-2-phényl-4H-chromène-8-carboxamide antagoniste α1-adrénergique
N-[3-[4-(o-metoxifenil)-1-piperazinil]propil]-3-metil-4-oxo-2-fenil-4H-1 -benzopirano-8-carboxamida antagonista de los receptores α1-adrenérgicos
C31H33N3O4 152735-23-4
valdecoxibum
valdecoxib
valdécoxib
valdecoxib
p-(5-methyl-3-phenyl-4-isoxazolyl)benzenesulfonamide cycloxygenase-2 inhibitor
4-(5-méthyl-3-phénylisoxazol-4-yl)benzènesulfonamide inhibiteur de la cyclooxygénase-2
p-(5-metil-3-fenil-4-isoxazolil)bencenosulfonamida inhibidor de la cicloxigenasa-2
C16H14N2O3S 181695-72-7
vangatalcitum vangatalcite
vangatalcite
vangatalcita
dialuminum tetramagnesium carbonate dodecahydroxide trihydrate antacid
carbonate et dodécahydroxyde de dialuminium et de tétramagnésium trihydraté antiacide
dodecahidróxido carbonato de dialuminio y tetramagnesio trihidrato antiácido
282
Al2Mg4(OH)12CO3 , 3 H 2 0

WHO Drug Information, Vol. 12, No 4, 1998 Proposed INN: List 80
vepalimomabum vepalimomab
vépalimomab
vepalimomab
immunoglobulin M (mouse monoclonal 1B2 µ-chain anti-human vascular adhesion protein VAP-1), disulfide with mouse monoclonal 1B2 light chain, dimer immunomodulator
immunoglobuline M anti-(protéine d'adhésion vasculaire humaine VAP-1) (chaîne µ de l'anticorps monoclonal de souris 1B2), dimère du disulfure avec la chaîne légère de l'anticorps monoclonal de souris 1B2 immunomodulateur
inmunoglobulina M (cadena µ del anticuerpo monoclonal de ratón 1B2 dirigido contra la proteína humana de adhesión vascular VAP-1), dímero del disulfuro con la cadena ligera del anticuerpo monoclonal de ratón 1B2 inmunomodulador
vilazodonum vilazodone
vilazodone
vilazodona
5-[4-[4-(5-cyanoindol-3-yl)butyl]-1-piperazinyl]-2-benzofurancarboxamide antidepressant
5-[4-[4-(5-cyano-1H-indol-3-yl)butyl]pipérazin-1-yl]benzafurane-2-carboxamide antidépresseur
5-[4-[4-(5-cianoindol-3-il)butil]-1-piperazinil]-2-benzofurancarboxamida antidepresivo
C26H27N5O2-HCI 163521-12-8
283
195158-85-1

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
C28H37N3O7 21102-49-8
volpristinum
volpristin
volpristine
volpristina
(3R,4R,5E,105,12E,14S,26aR)-8,9,14,15,24,25,26,26a-octahydro-14-hydroxy-3-isopropyl-4,12-dimethyl-3H-21,18-nitrilo-1H,22H-pyrrolo= [2,1-c][1,8,4,19]dioxadiazacyclotetracosine-1,7,16,22(4H,17H)-tetrone antibacterial
(5E,10E,12E)-(3R,4R,14S,26aR)-14-hydroxy-4,12-diméthyl-3-(1-méthyléthyl)-3,4,8,9,14,15,24,25,26,26a-décahydro-7H-21.18-nitrilo-1H,22H-pyrrolo= [2,1-c][1,8,4,19]dioxadiazacyclotétracosène-1,7,16,22(17H)-tétrone antibactérien
(3R,4R,5E,10E,12E,14S,26aR)-8,9,14,15,24,25,26,26a-octahidro-14-hidroxi-3-isopropil-4,12-dimetil-3H-21,18-nitrilo-1H,22H-pirrolo= [2,1-c][1,8,4,19]dioxadiazaciclotetracosina-1,7,16,22(4H,17H)-tetrona antibacteriano
284

WHO Drug Information, Vol, 12, No. 4, 1998 Proposed INN: List 80
AMENDMENTS TO PREVIOUS LISTS MODIFICATIONS APPORTÉES AUX LISTES ANTÉRIEURES
MODIFICACIONES A LAS LISTAS ANTERIORES
Proposed International Nonproprietary Names (Prop. INN): List 18 (WHO Chronicle, Vol. 21, No. 11, 1967)
p. 12 hypromellosum hypromellose replace the chemical name by the following:
a mixed methyl and 2-hydroxypropyl ether of cellulose
Dénominations communes internationales proposées (DCI Prop.): Liste 18 (Chronique OMS, Vol. 21, No. 11, 1967)
p. 11 hypromellosum
hypromellose remplacer le nom chimique par le suivant:
mélange d'éthers méthyliques et 2-hydroxypropyliques de cellulose
Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 1B (Crónica de la OMS, Vol. 21, No. 11, 1967)
p. 132 hypromellosum
hipromelosa sustitúyase el nombre quimico por el siguiente:
mezcla de éteres metilicos y 2-hidroxipropilicos de celulosa
Proposed International Nonproprietary Names (Prop. INN): List 31 (WHO Chronicle, Vol. 28, No. 3, 1974)
p. 22 calcitoninum calcitonin replace the description by the following:
a polypeptide hormone that lowers the calcium concentration
(the species specificity should be indicated in brackets behind the name) e.g.
calcitonin (human) C151H226N40O45S3
Cys— Gly—Asn— Leu—Ser—Thr—Cys— Met—Leu—Gly—Thr—Tyr—Thr— 10
Gin—Asp—Phe—Asn—Lys—Phe—His—Thr-Phe—Pro—Gin—Thr—Ala — 20
Ile—Gly—Val—Gly—Ala—Pro-NH2 30
285
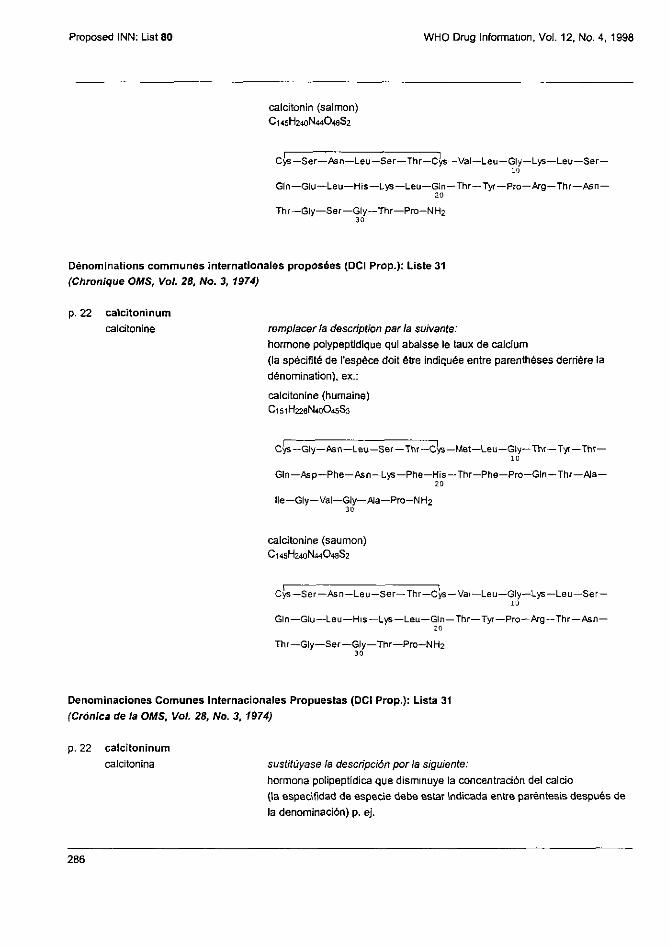
Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
calcitonin (salmon) C145H240N44O48S2
Cys— Ser—Asn—Leu—Ser—Thr—Cys—Val—Leu—Gly—Lys—Leu—Ser
Gin—Glu—Leu—His—Lys—Leu—Gin—Thr—Tyr—Pro—Arg—Thr—Asn — 20
Thr—Gly—Ser—Gly—Thr—Pro-NH2 30
Dénominations communes internationales proposées (DCI Prop.): Liste 31 (Chronique OMS, Vol. 28, No. 3, 1974)
p. 22 calcitoninum calcitonine remplacer la description par la suivante:
hormone polypeptideque qui abaisse le taux de calcium (la spécifité de l'espèce doit être indiquée entre parenthèses derrière la dénomination), ex.:
calcitonine (humaine) C151H226N40O45S3
Cys— Gly— Asn— Leu—Ser— Thr— Cys— Met—Leu— Gly— Thr— Tyr—Thr— 10
Gin—Asp—Phe—Asn—Lys—Phe—His—Thr—Phe—Pro—Gln—Thr—Ala— 20
Ile—Gly—Val—Gly—Ala—Pro-NH2 30
Cys—Ser—Asn—Leu—Ser—Thr—Cys—Val—Leu—Gly—Lys—Leu—Ser
Gin—Glu—Leu—His—Lys—Leu—Gin—Thr—Tyr—Pro—Arg—Thr—Asn— 20
Thr—Gly—Ser—Gly—Thr—Pro-NH2 30
Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 31 (Crónica de la OMS, Vol. 28, No. 3, 1974)
p. 22 calcitoninum calcitonina sustitúyase la descripción por la siguiente:
hormona polipeptídica que disminuye la concentración del calcio (la especifidad de especie debe estar indicada entre paréntesis después de la denominación) p. ej.
286
calcitonine (saumon) C145H240N44O48S2

WHO Drug Information, Vol 12, No. 4, 1998 Proposed INN: List 80
calcitonina (humana) C151H226N40O45S3
Cys—Gly—Asn—Leu—Ser—Thr—Cys—Met—Leu—Gly—Thr—Tyr—Thr— 10
Gln—Asp—Phe—Asn—Lys—Phe—His—Thr-Phe—Pro—Gln—Thr—Ala— 20
Ile—Gly—Val—Gly—Ala—Pro-NH2 30
calcitonina (salmón) C145H240N44O48S2
Proposed International Nonproprietary Names (Prop. INN): List 68 (WHO Drug Information, Vol. 6, No. 4, 1992)
p. 2 altumomabum altumomab replace the description by the following:
immunoglobulin G1, anti-(human carcinoembryonic antigen) (mouse monoclonal ZCE025 γ1-chain), disulfide with mouse monoclonal ZCE025 light chain, dimer
p. 16 satumomabum satumomab replace the description by the following:
immunoglobulin G1, anti-(human tumor-associated glycoprotein 72) (mouse monoclonal B72.3 light chain), disulfide with mouse monoclonal B72 3 light chain, dimer
Dénominations communes internationales proposées (DCI Prop.): Liste 68 (Informations Pharmaceutiques OMS, Vol. 6, No. 4, 1992)
p. 2 altumomabum altumomab remplacer la description par la suivante.
immunoglobuline G1, anti-(antigène associé aux carcinomes embryonnaires humains) (chaîne γ1 de l'anticorps monoclonal de souris ZCE025), dimère du disulfure avec la chaîne légère de l'anticorps monoclonal de souris ZCE025
287
Cys—Ser—Asn—Leu—Ser—Thr—Cys —Val—Leu—Gly—Lys—Leu—Ser
Gin—Glu—Leu—His—Lys—Leu—Gin—Thr—Tyr—Pro—Arg—Thr—Asn— 20
Thr—Gly—Ser—Gly—Thr—Pro-NH2 30

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
p. 16 satumomabum satumomab remplacer la description parla suivante:
immunoglobulins G1, anti-(glycoprotéine 72 humaine associée aux tumeurs) (chaîne légère de l'anticorps monoclonal de souris B72.3), dimère du disulfure avec la chaîne légère de l'anticorps monoclonal de souris B72.3
Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 68 (Información Farmacéutica OMS, Vol. 6, No. 4, 1992)
p. 2 altumomabum altumomab sustitúyase la descripción por la siguiente:
inmunoglobulina G1, anti-(antigeno carcinoembrionario humano) (cadena γ1 del anticuerpo monoclonal de ratón ZCE025), dimero del disulfuro con la cadena ligera del anticuerpo monoclonal de ratón ZCE025
p. 16 satumomabum satumomab sustitúyase la descripción por la siguiente:
inmunoglobulina G1, anti-(glicoproteína 72 humana asociada al tumor) (cadena ligera del anticuerpo monoclonal de ratón B72.3), dímero del disulfuro con la cadena ligera del anticuerpo monoclonal de ratón B72.3
Proposed International Nonproprietary Names (Prop. INN): List 69 (WHO Drug Information, Vol. 7, No. 2, 1993)
p. 3 edobacomabum edobacomab replace the description by the following.
immunoglobulin M, anti-(endotoxin) (mouse monoclonal XMMEN-0E5 µ-chaín), disulfide with mouse monoclonal XMMEN-0E5 light chain, pentameric dimer
p. 9 zolimomabum aritoxum zolimomab aritox replace the description by the following.
immunoglobulin G1, anti-(human CD5 (antigen) heavy chain) (mouse monoclonal H65-RTA γ1-chain), disulfide with mouse monoclonal H65-RTA light chain, dimer, disulfide with ricin (castor bean A-chain)
Dénominations communes internationales proposées (DCI Prop.): Liste 69 (Informations Pharmaceutiques OMS, Vol. 7, No. 2, 1993)
p. 3 edobacomabum édobacomab remplacer la description par la suivante:
immunoglobuline M, anti-(endotoxine) (chaîne m de l'anticorps monoclonal souris XMMEN-0E5), dimère pentamérique du disulfure avec la chaîne légère de l'anticorps monoclonal de souris XMMEN-0E5
288

WHO Drug Information, Vol 12, No. 4, 1998 Proposed INN: List 80
p. 9 zolimomabum aritoxum zolimomab aritox remplacer la description par la suivante:
immunoglobuline G1, anti-(chaîne lourde de l'antigène CD5 humain) (chaîne γ1 de l'anticorps monoclonal de souris H65-RTA), dimère du disulfure avec la chaîne légère de l'anticorps monoclonal de souris H65-RTA, disulfure avec la chaîne A de la ricine
Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 69 (Información Farmacéutica OMS, Vol. 7, No. 2, 1993)
p. 3 edobacomabum edobacomab
p. 9 zolimomabum aritoxum zolimomab aritox
sustitúyase la descripción por la siguiente: inmunoglobulina M, anti-(endotoxina) (cadena µ del anticuerpo monoclonal de ratón XMMEN-0E5), dímero pentamérico del disulfuro con la cadena ligera del anticuerpo monoclonal de ratón XMMEN-0E5
sustituyase la descripción por la siguiente: inmunoglobulina G1, anti-(cadena pesada del antígeno humano CD5) (cadena γ1 del anticuerpo monoclonal de ratón H65-RTA), dímero del disulfuro con la cadena ligera del anticuerpo monoclonal de ratón H65-RTA, disulfuro con ricina (cadena A de la judía de ricino)
Proposed International Nonproprietary Names (Prop. INN): List 70 (WHO Drug Information, Vol. 7, No, 4, 1993)
p 1 abciximabum abciximab
p. 3 capromabum capromab
p 4 detumomabum detumomab
p. 5 enlimomabum enlimomab
replace the description by the following: immunoglobulin G1, anti-(human integrin αllbβ3) Fab fragment (human-mouse monoclonal c7E3 clone p7E3VHhCγ1 γ1-chain), disulfide with human-mouse monoclonal c7E3 clone p7E3VκhCκ κ-chain
replace the description by the following: immunoglobulin G1, anti-(human prostatic carcinoma cell) (mouse monoclonal 7E11-C5.3 γ1-chain), disulfide with mouse monoclonal 7E11-C5.3 light chain, dimer
replace the description by the following: immunoglobulin G1, anti-(human B lymphoma cell) (mouse monoclonal SPECIFID heavy chain), disulfide with mouse monoclonal SPECIFID light chain, dimer
replace the description by the following: immunoglobulin G2a, anti-(human CD54 (antigen)) (mouse monoclonal BI-RR-1 γ2a-chain), disulfide with mouse monoclonal BI-RR-1 light chain, dimer
289

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1996
p. 13 votumumabum votumumab replace the description by the following:
immunoglobulin G3, anti-(human carcinoma-associated antigen) (human monoclonal 88BV59 γ3-chain), disulfide with human monoclonal 8SBV59 κ-chain, dimer
Dénominations communes internationales proposées (DCI Prop.): Liste 70 (Informations Pharmaceutiques OMS, Vol. 7, No. 4, 1993)
p. 1 abciximabum abciximab
p. 4 capromabum capromab
p. 5 detumomabum détumomab
p 5 enlimomabum enlimomab
p. 13 votumumabum votumumab
remplacer la description par la suivante: immunoglobuline G1, anti-(intégrine αllbβ3 humaine) fragment Fab (chaîne γ1 de l'anticorps monoclonal chimérique homme-souris c7E3 clone p7E3VHhCγ1), disulfure avec la chaîne K de l'anticorps monoclonal chimérique homme-souris c7E3 clone p7ESVKhCK
remplacer la description par la suivante: immunoglobuline G1, anti-(cellules du carcinome prostatique humain) (chaîne γ1 de l'anticorps monoclonal de souris 7E11-C5.3), dimère du disulfure avec la chaîne légère de l'anticorps monoclonal de souris 7E11-C5.3
remplacer la description par la suivante: immunoglobuline G1, anti-(cellules de lymphome B humain) (chaîne lourde de l'anticorps monoclonal de souris SPECIFID), dimère du disulfure avec la chaîne légère de l'anticorps monoclonal de souris SPECIFID
remplacer la description par la suivante: immunoglobuline G2a, anti-(antigène CD54 humain) (chaîne γ2a de l'anticorps monoclonal de souris BI-RR-1 ), dimère du disulfure avec la chaîne légère de l'anticorps monoclonal de souris BI-RR-1
remplacer la description par la suivante: immunoglobuline G3, anti-(antigène associé aux carcinomes humains) (chaîne γ3 de l'anticorps monoclonal humain 88BV59), dimère du disulfure avec la chaîne K de l'anticorps monoclonal humain 88BV59
290

WHO Drug Information, Vol. 12, No. 4, 1998 Proposed INN: List 80
Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 70 (Información Farmacéutica OMS, Vol. 7, No. 4, 1993)
p 1 abciximabum abciximab
p.4
p.5
capromabum capromab
detumomabum detumomab
p 5 enlimomabum enlimomab
p. 14 votumumabum votumumab
sustitúyase la descripción por la siguiente inmunoglobulina G1, anti-(integrina αllbβ3 humana) fragmento Fab (cadena γ1 del anticuerpo monoclonal hombre-ratón c7E3 clon p7E3VHhCγ1), disulfuro con la cadena Κ del anticuerpo monoclonal hombre-ratón c7E3 clon p7E3VxhCκ
sustitúyase la descripción por la siguiente inmunoglobulina G1, anti-(células de carcinoma prostático humano) (cadena Γ1 del anticuerpo monoclonal de ratón 7E11-C5.3), dímero del disulfuro con la cadena ligera del anticuerpo monoclonal de ratón 7E11-C5.3
sustitúyase la descripción por la siguiente: inmunoglobulina G1, anti-(celulas de linfoma B humano) (cadena pesada del anticuerpo monoclonal de ratón SPECIFID), dímero del disulfuro con la cadena ligera del anticuerpo monoclonal de ratón SPECIFID
sustitúyase la descripción por la siguiente: inmunoglobulina G2a, anti-((antigeno) CD54 humano) (cadena γ2a del anticuerpo monoclonal de ratón BI-RR-1), dimero del disulfuro con la cadena ligera del anticuerpo monoclonal de ratón BI-RR-1
sustituyase la descripción por la siguiente: inmunoglobulina G3 anti-(antígeno asociado a los carcinomas humanos) (cadena γ3 del anticuerpo monoclonal humano 38BV59), dímero del disulfuro con la cadena K del anticuerpo monoclonal humano 88BV59
Proposed International Nonproprietary Names (Prop. INN): List 71 Dénominations communes internationales proposées (DCI Prop.): Liste 71 Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 71 (WHO Drug Information, Vol. 8, No. 2, 1994)
p. 14 inolimomabum inolimomab replace the description by the following:
immunoglobulin G1, anti-(human interleukin 2 receptor α-chain) (mouse monoclonal B-B10 γ1-chain), disulfide with mouse monoclonal B-810 κ-chain, dimer
291
Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
inolimomab
inolimomab
remplacer la description par la suivante: immunoglobuline G1, anti-(chaîne α du récepteur de l'interleukine 2 humain) (chaîne γ1 de l'anticorps monoclonal de souris B-B10), dimère du disulfure avec la chaîne K de l'anticorps monoclonal de souris B-B10
sustitúyase la descripción por la siguiente: inmunoglobulina G1, anti-(cadena α del receptor de interleukina 2 humano) (cadena γ1 del anticuerpo monoclonal de ratón B-B10), dímero del disulfuro con la cadena K del anticuerpo monoclonal de ratón B-B10
p. 17 nacolomabum tafenatoxum nacolomab tafenatox
nacolomab tafénatox
nacolomab tafenatox
p. 19 regavirumabum regavirumab
régavirumab
regavirumab
replace the description by the following: immunoglobulin G1, anti-(human colorectal tumor antigen C242) Fab fragment (mouse monoclonal r-C242Fab-SEA clone pkP941 γ1-chain) fusion protein with enterotoxin A (Staphylococcus aureus), disulfide with mouse monoclonal r-C242Fab-SEA clone pkP941 κ-chain
remplacer la description par la suivante: protéine de fusion entre l'immunoglobuline G1, anti-(antigène C242 associé aux tumeurs colorectales humaines) fragment Fab (chaîne γ1 de l'anticorps monoclonal de souris r-C242Fab-SEA clone pkP941) et l'entérotoxine A (Staphylococcus aureus), disulfure avec la chaîne κ de l'anticorps monoclonal de souris r-C242Fab-SEA clone pkP941
sustitúyase la descripción por la siguiente: inmunoglobulina G1, anti-(antigeno C242 de tumor colorrectal humano) fragmento Fab (cadena γ1 del anticuerpo monoclonal de ratón r-C242Fab-SEA clon pkP941) proteina de fusión con la enterotoxina A (Staphylococcus aureus), disulfuro con la cadena K del anticuerpo monoclonal de ratón r-C242Fab-SEA clon pkP941
replace the description by the following: immunoglobulin G1, anti-(human herpesvirus 5 glycoprotein B) (human monoclonal γ1-chain), disulfide with human monoclonal κ-chain, dimer
remplacer la description par la suivante: immunoglobuline G1, anti-(glycoprotéine B du virus de l'herpès 5 humain) (chaîne γ1 de l'anticorps monoclonal humain), dimère du disulfure avec la chaîne K de l'anticorps monoclonal humain
sustitúyase la descripción por la siguiente: inmunoglobulina G1, anti-(glicoproteina B del virus del herpes 5 humano) (cadena γ1 del anticuerpo monoclonal humano), dímero del disulfuro con la cadena K del anticuerpo monoclonal humano
292

WHO Drug Information, Vol. 12, No 4, 1998 Proposed INN: List 80
Proposed International Nonproprietary Names (Prop. INN): List 72 Dénominations communes internationales proposées (DCI Prop.): Liste 72 Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 72 (WHO Drug Information, Vol, 8, No. 4, 1994)
p. 3 afelimomabum afelimomab
afélimomab
afelimomab
p. 27 priliximabum
priliximab
priliximab
priliximab
replace the description by the following: immunoglobulin G3, anti-(human tumor necrosis factor a) F(ab')2 fragment (mouse monoclonal LU54107 γ3-chain), disulfide with mouse monoclonal LU54107 κ-chain, dimer
remplacer la description par la suivante:
immunoglobuline G3, anti-(facteur de nécrose tumorale a humain) fragment
F(ab')2 (chaîne γ3 de l'anticorps monoclonal de souris LU54107), dimère du
disulfure avec la chaîne K de l'anticorps monoclonal de souris LU54107
sustitúyase la descripción por la siguiente:
inmunoglobulina G3, anti-(factor de necrosis tumoral a humano) fragmento
F(ab')2 (cadena γ3 del anticuerpo monoclonal de ratón LU54107), dímero del
disulfuro con la cadena K del anticuerpo monoclonal de ratón LU54107
replace the description by the following:
immunoglobulin G 1 , anti-(human CD4 (antigen)) (human-mouse monoclonal
cm-T412 γl-chain), disulfide with human-mouse monoclonal cm-T412
K-chain, dimer
remplacer la description par la suivante:
immunoglobuline G 1 , anti-(antigène CD4 humain) (chaîne γ1 de l'anticorps
monoclonal chimérique homme-souris cm-T412), dimère du disulfure avec la
chaîne K de l'anticorps monoclonal chimérique homme-souris cm-T412
sustitúyase la descripción por la siguiente:
inmunoglobulina G1 , anti-((antígeno) CD4 humano) (cadena γ1 del
anticuerpo monoclonal hombre-ratón cm-T412), dímero del disulfuro con la
cadena K del anticuerpo monoclonal hombre-ratón cm-T412
Proposed International Nonproprietary Names (Prop. INN): List 78 Dénominations communes internationales proposées (DCI Prop.): Liste 78 Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 78 (WHO Drug Information, Vol. 11, No. 4, 1997)
p. 280 delete/supprimer/suprimase nelzarabinum nelzarabine
nélzarabine nelzarabina
insert/insérer/insértese nelarabinum nelarabine
nélarabine
nelarabina
293

Proposed INN: List 80 WHO Drug Information, Vol. 12, No. 4, 1998
Proposed International Nonproprietary Names (Prop. INN): List 79 Dénominations communes internationales proposées (DCI Prop.): Liste 79 Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 79 (WHO Drug Information, Vol. 12, No. 2, 1998)
p. 105 eniporidum eniporide éniporide eniporida
add the fallowing CAS registry number: insérer le numéro dans le registre du CAS suivant: insértese el número de registro del CAS siguiente:
176644-21-6
p 106 esomeprazolum esomeprazole ésoméprazole esomeprazol
add the following CAS registry number insérer le numéro dans le registre du CAS suivant. insértese el número de registro del CAS siguiente:
119141-88-7
p. 112 stannsoporfinum stannsoporfin stannsoporfine stannsoporfina
replace the molecular formula by the following: remplacer la formule brute par: sustitúyase la fórmula molecular por:
C34H36CI2N4O4Sn
Procedure and Guiding Principles / Procédure et Directives / Procedimientos y principios generales
The text of the Procedures for the Selection of Recommended International Nonproprietary Names for Pharmaceutical Substances and General Principles for Guidance in Devising International Nonproprietary Names for Pharmaceutical Substances will be reproduced in uneven numbers of proposed INN lists only.
Les textes de la Procédure à suivre en vue de choix de dénominations communes internationales recommandées pour les substances pharmaceutiques et des Directives générales pour la formation de dénominations communes internationales applicables aux substances pharmaceutiques ont été publiés avec la liste 77 des DCI proposées et seront, à nouveau, publiés avec la prochaine liste.
El texto de los Procedimientos de selección de denominaciones comunes internacionales recomendadas para las sustancias farmacéuticas y de los Principios generales de orientación para formar denominaciones comunes internacionales para sustancias farmacéuticas aparece solamente en los números impares de las listas de DCI propuestas.
294