when the world is turned upside down - trauma … · when the world is turned upside down accident...
TRANSCRIPT

WHEN THE WORLD IS TURNED UPSIDE DOWN
ACCIDENT RESEARCH CENTRE
Charles Darwin University, 17 August 2017
Eva Alisic

www.trauma-recovery.net
@EvaAlisic

Picture of floodsPicture of a firePicture of refugeesPicture of an injured childPicture of a funeral?


Picture of floodsPicture of a firePicture of refugeesPicture of an injured childPicture of a funeral?

Children & Trauma: What we know
67%
Children & Trauma: What we know
15%
Children & Trauma: What we know
Social support
Life threat appraisal
First responders
Caregivers
Teachers
Friends
Mental health pros
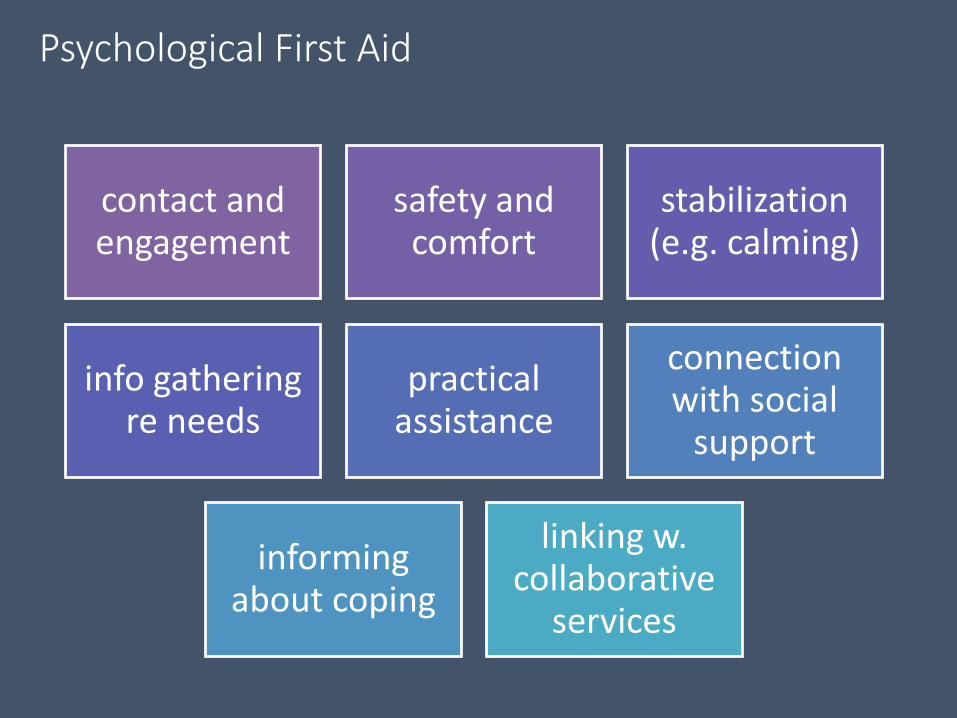
Psychological First Aid
contact and engagement
safety and comfort
stabilization (e.g. calming)
info gathering re needs
practical assistance
connection with social
support
informing about coping
linking w. collaborative
services
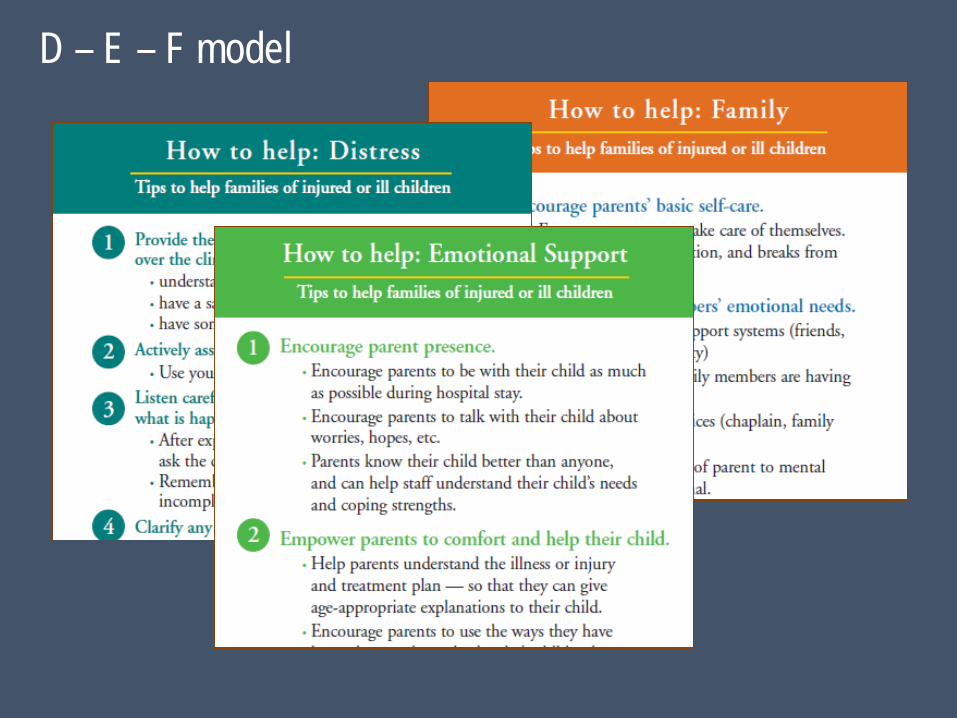
D – E – F model

Emergency professionals
Knowledge Attitudes Confidence Training wishes
2648 emergency department staff812 paramedics

Knowledge of child traumatic stress (% correct)
All injury severities are at risk for traumatic stress 60.4%
All age groups are at risk for traumatic stress 38.6%
The child, parents, and siblings are at risk for tr stress 71.2%
Various behaviors (e.g. calm, frantic) can precede tr stress 31.1%
Subjective life threat is a risk factor 58.8%
Pain experience is a risk factor 43.0%
> 50% of children report stress symptoms in 1st month 7.0%
• …• …• …• …• …
Significant predictors
• Experience (years)• …• …
Non-significant
Knowledge of child traumatic stress

How confident are you that you can….
Respond calmly and without judgment to a child’s or family’s strong emotional distress
(1) not at all (2) a little (3) moderately (4) very
How confident are you that you can….
Assess and manage pain in children
(1) not at all (2) a little (3) moderately (4) very
How confident are you that you can….
Educate children & parents about traumatic stress reactions
(1) not at all (2) a little (3) moderately (4) very
Staff were moderately confident (M = 3)
Explaining procedures to children and parents
Educating children and parents about traumatic stress

• …• …• Experience (years)• …
Significant predictors
• …• …• …
Non-significant
Confidence re psychosocial care

Appetite for training
93%

Thanks to a wonderful team & great supporters
Many, many young people, families, and colleagues who contributed and shared their experiences
Members of the team(s):Sarah Curtis, Anupam Kharbanda, Mark Lyttle, Niccolo Parri, Rachel Stanley, Franz Babl, Anna Barret, Melita Giummarra, Laura Jobson, Rolf Kleber, Juul Gouweloos, Arend Groot, Hanneke Snetselaar, Tielke Stroeken, Elise v/d Putten, Lieve Hehenkamp, Revathi Krishna, John Frederick, Shaminka Gunaratnam, Rowena Conroy, Matthias Mehl, Vicki Anderson, Helen Jowett, Roderick McClure, Cameron Palmer, Prue Dunstan, Hayley Ayton, Jasmine Loo, Caitlin Arthur, Deborah Lewis,Scott McDonald, Caitlin Bishop, Peter Bowles, Georgina Johnstone, Naile Alangor, & Maggie Lam
Financial support:The Australian National Health & Medical Research Council (NHMRC), Netherlands Organisation for Scientific Research, Monash University Larkins Program, Victorian Government’s Infrastructure Support Program, Royal Children’s Hospital Foundation, SAMSHA, Netherlands Ministry of Security & Justice; Prof. Weijersstichting, et al.
First responders
Caregivers
Teachers
Friends
Mental health pros

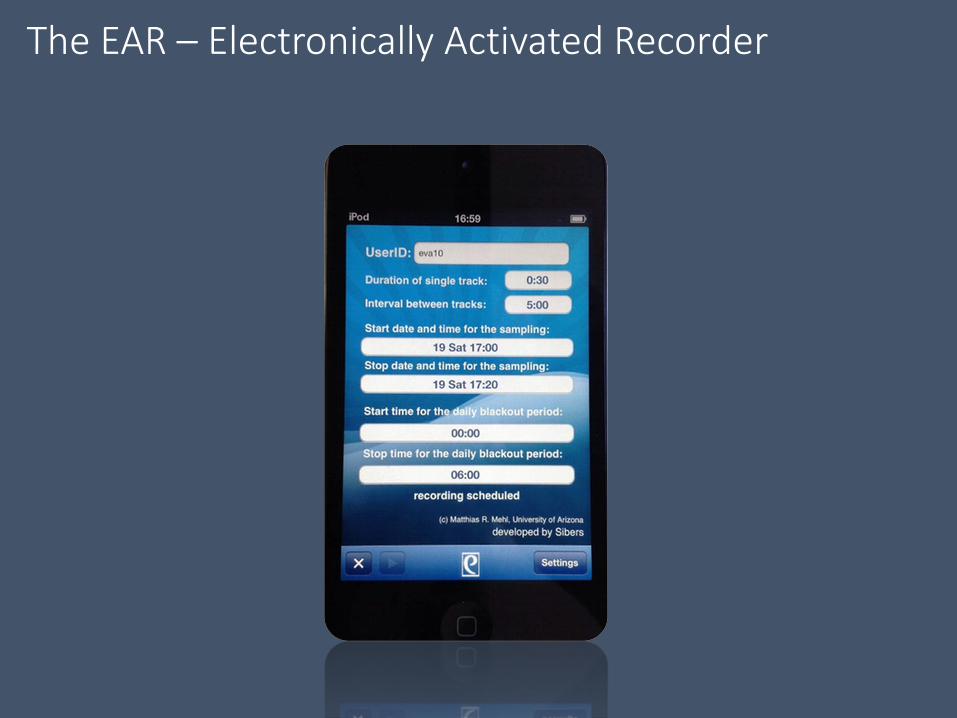
The EAR – Electronically Activated Recorder

EAR for Recovery study
Prospective cohort study of 71 children aged 3-16 (hospitalized ≥ 24hrs)
Children wore the EAR for 2 days after discharge,30-second snippets every 5 mins
Phone follow-up at 6 weeks & 3 months re child mental health (sub-sample)
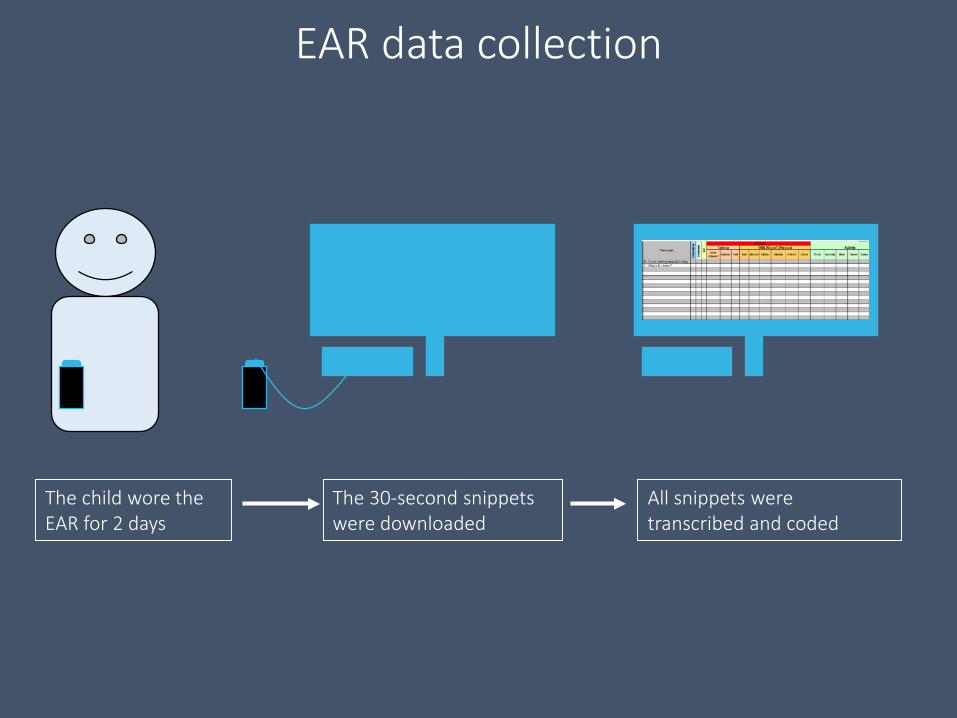
EAR data collection
The child wore the EAR for 2 days
The 30-second snippets were downloaded
All snippets were transcribed and coded

≈20,000
Adult male: Oh my goodness oh what have you done?
Child: Had to go to hospital … because I fell over the top of my horse’s head…
Father: Face planted….
Adult male: Goodness me.
Father: Ended up a couple of days at the Children's. About a week off school.
Child: Two nights, three days.
Injury talk
• How much time do children spend interacting with others?
• How much of their interactions are about the injury?
• How much of their injury interactions are about emotions?
What’s your guess?

• How much time do children spend interacting with others?
• How much of their interactions are about the injury?
• How much of their injury interactions are about emotions?
What’s your guess?
47% (wake time)
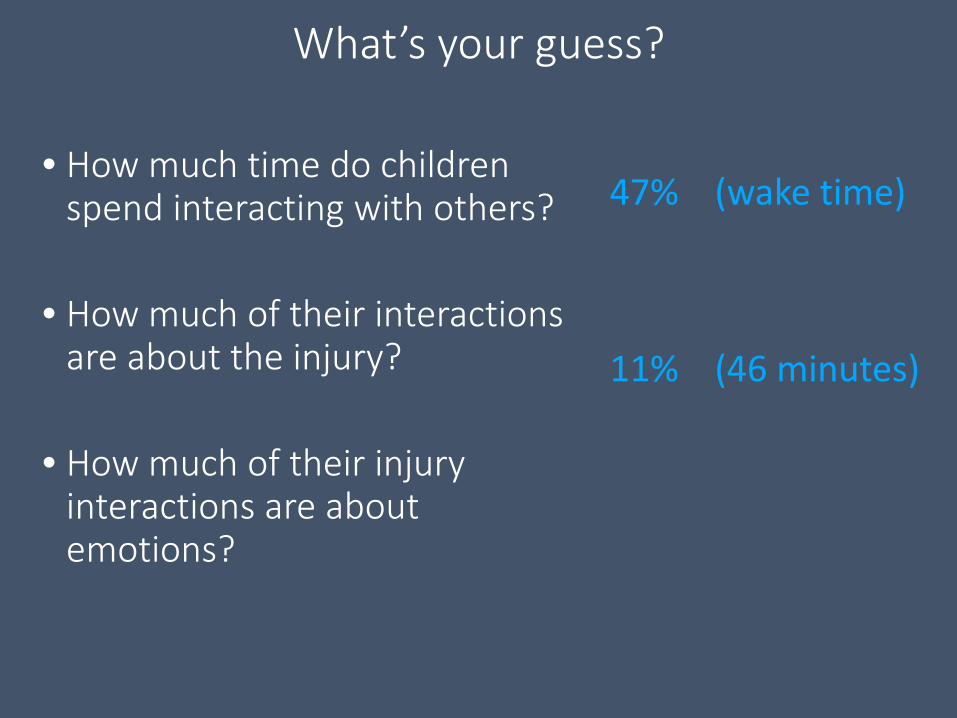
• How much time do children spend interacting with others?
• How much of their interactions are about the injury?
• How much of their injury interactions are about emotions?
What’s your guess?
47% (wake time)
11% (46 minutes)
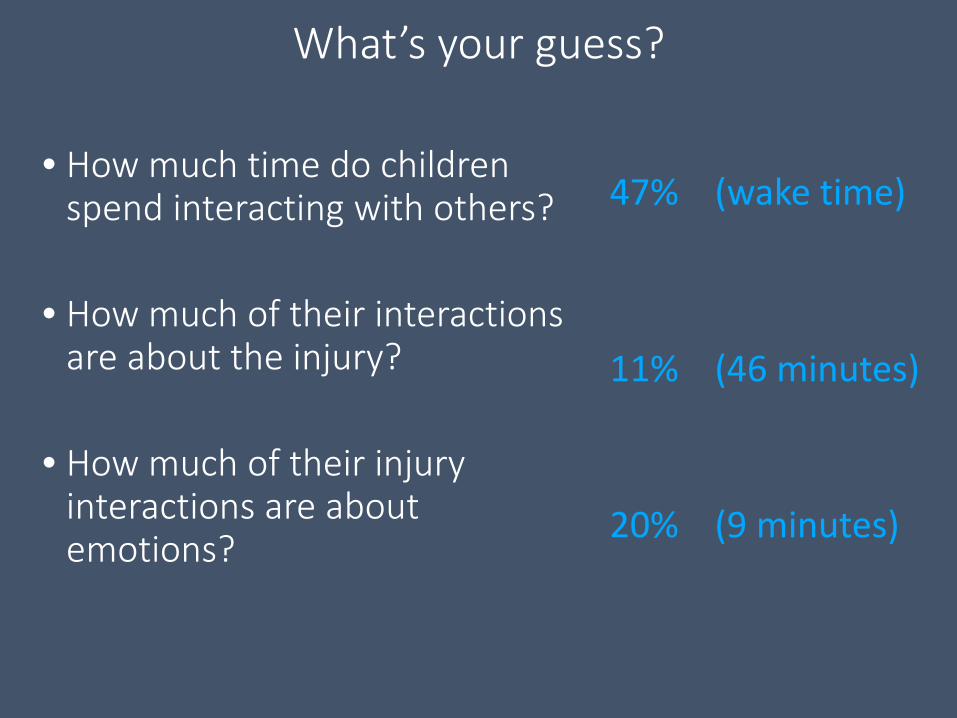
• How much time do children spend interacting with others?
• How much of their interactions are about the injury?
• How much of their injury interactions are about emotions?
What’s your guess?
47% (wake time)
11% (46 minutes)
20% (9 minutes)
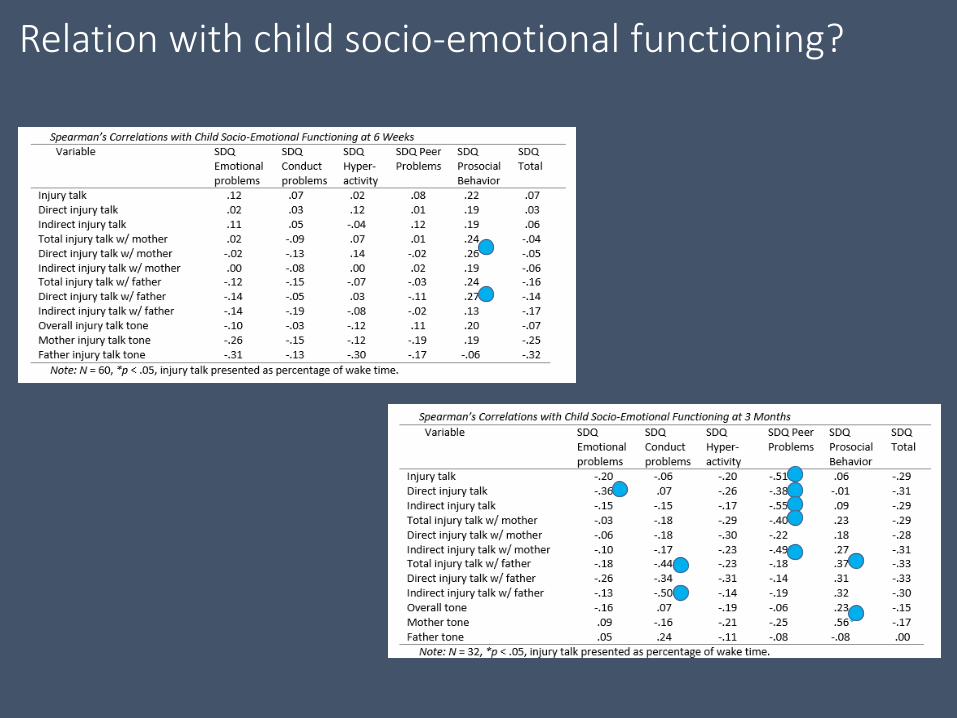
Relation with child socio-emotional functioning?
• More specific analyses and coding• Databank for future research• Use as a clinical tool
Follow the action via www.trauma-recovery.net
Next steps

Intimate Partner Homicides
• More than 1/3 of female homicides• Often children involved• Professionals with little experience• Far-reaching consequences of decisions

Study to understand children’s and families’…
1. Characteristics
2. Experiences
3. Well-being and mental health outcomes
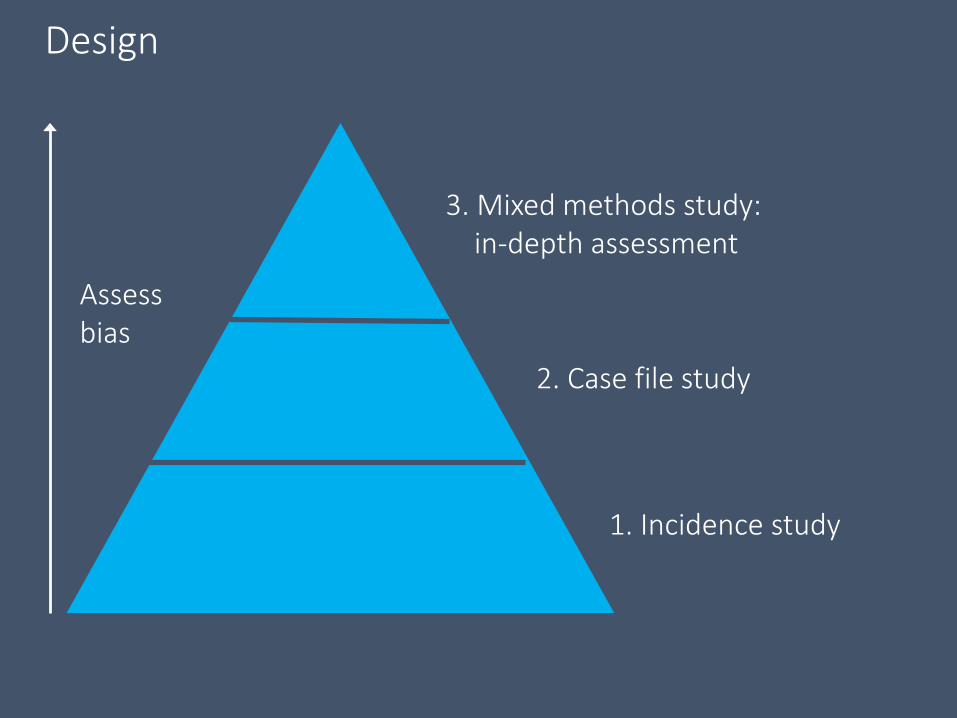
Design
3. Mixed methods study: in-depth assessment
2. Case file study
1. Incidence study
Assessbias

Child & family characteristics
7.4 years old

Child & family characteristics
Child & family characteristics
83%
Child & family characteristics
43% (16% unclear)
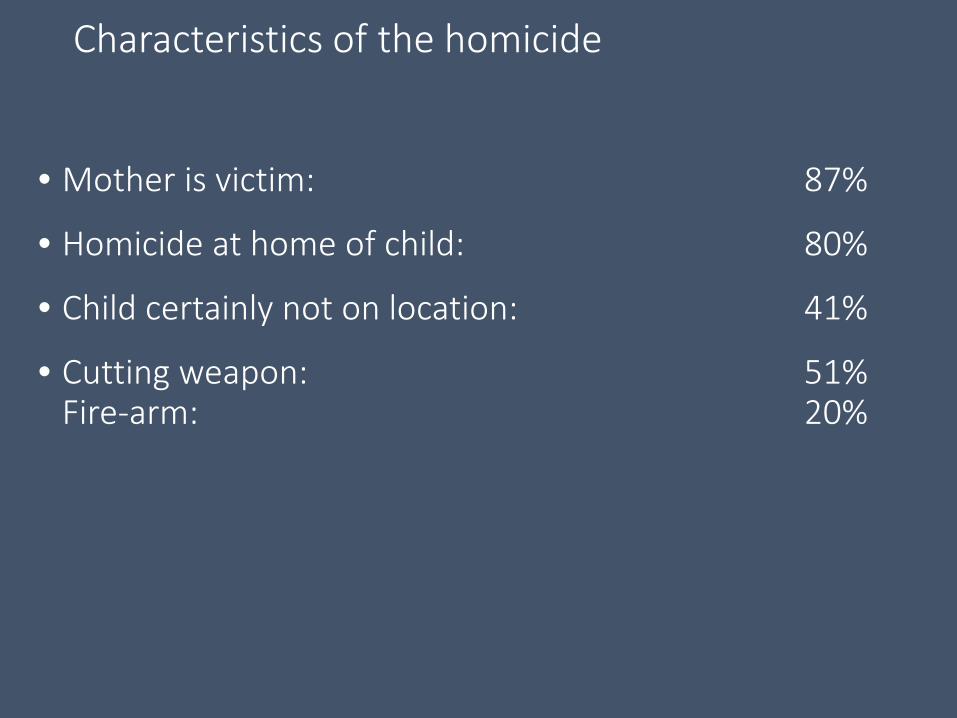
Characteristics of the homicide
• Mother is victim: 87%
• Homicide at home of child: 80%
• Child certainly not on location: 41%
• Cutting weapon: 51% Fire-arm: 20%
Insights from the interviews (re 40 youth)
Contributors to wellbeing:• Placement with trusted family members• Continuity of professional support, open communication • Good contact with both sides of family

Insights from the interviews (re 40 youth)
Fragile balance:• Functioning but still major influence on daily life• Grief symptoms among caregivers• Variation & pressure regarding contact with perpetrator;
stress due to legal procedures

Preliminary conclusions
• Cliche but true: each case is unique
• Burden is exceptionally high
• Continuity of support & mediation are important
• Need for culture-sensitive support
• Need to give children a voice re their wishes
First responders
Caregivers
Teachers
Friends
Mental health pros
In conclusion…
Gaps in knowledge & desire for training
In conclusion…
46 minutes & counting…
In conclusion…
Improving detection & providing more care
Thank you!

Key references (I)Children & Trauma – exposure, PTSD, predictors• Copeland WE, Keeler G, Angold A, Costello EJ. Traumatic events and posttraumatic stress in
childhood. Arch Gen Psychiatry. 2007;64:577-84.• Trickey, D., Siddaway, A.P., Meiser-Stedman, R., Serpell, L., & Field, A.P. (2012). A meta-analysis
of risk factors for post-traumatic stress disorder in children and adolescents. Clinical Psychology Review, 32, 122-138
• Marsac, M.L., Kassam-Adams, N., Delahunty, D.L., Widaman, K.F., & Barakat, L.P., (2014). Posttraumatic stress following acute medical trauma in children: A proposed model of bio-psycho-social processes during the peri-trauma period. Clinical Child and Family Psychology Review, 17, 399-411
• Alisic , E., Boeije, H.R., Jongmans, M.J., & Kleber, R.J. (2011) ‘Children's perspectives on dealing with traumatic events, Journal of Loss and Trauma, 16, 477-496.
• Alisic, E, Boeije, HR, Jongmans, MJ & Kleber, RJ 2012, ‘Supporting children after single-incident trauma parents’ views’, Clinical Pediatrics, vol. 51, pp. 274-282.
• Alisic, E, Jongmans, MJ, van Wesel, F & Kleber, RJ 2011b, ‘Building child trauma theory from longitudinal studies: a meta-analysis’, Clinical Psychology Review, vol. 31, pp. 736-747.
• Alisic, E., Zalta, A.K., Van Wesel, F., Larsen, S.E., Hafstad, G.S., Hassanpour, K., & Smid, G.E. (2014). Rates of post-traumatic stress disorder in trauma-exposed children and adolescents: meta-analysis. British Journal of Psychiatry, 204, 335-340.
• Gunaratnam, S. & Alisic, E. (2017). Epidemiology of trauma and trauma-related disorders in children and adolescents. In Landolt, Schnyder & Cloitre (Eds.) Evidence Based Treatments for Trauma-Related Disorders in Children and Adolescents, Springer

Key references (II)Psychosocial Care / Psychological First Aid / D-E-F model• Brymer M, Jacobs A, Layne C, Pynoos R, Ruzek J, Steinberg A, et al. Psychological first aid field
operations guide, 2nd Edition. National Child Traumatic Stress Network and National Center for PTSD. 2006.
• Psychological First Aid online course. Available from: http://learn.nctsn.org/course/index.php?categoryid=11
• Stuber ML, Schneider S, Kassam-Adams N, Kazak AE, Saxe G. The medical traumatic stress toolkit. CNS Spectr 2006; 11:137-42
• Kassam-Adams, N., Marsac, M.L., Hildenbrand, A., & Winston, F. (2013). Posttraumatic stress following pediatric injury: Update on diagnosis, risk factors, and intervention. JAMA Pediatrics167, 1158-1165. doi: 10.1001/jamapediatrics.2013/2741
• Alisic, E., Hoysted, C., Kassam-Adams, N., Landolt, M.A., Curtis, S., Kharbanda, A.B., Lyttle, M.D., Parri, N., Stanley, R., & Babl, F.E. (2016). Psychosocial care for injured children: worldwide survey among hospital Emergency Department staff. Journal of Pediatrics 170: 227-33
• Alisic, E., Tyler, M.P., Giummarra, M.J., Kassam-Adams, R., Gouweloos, J., Landolt, M.A., & Kassam-Adams, N. (2017). Trauma-informed care for children in the ambulance: International survey among pre-hospital providers. European Journal of Psychotraumatology. doi: 10.1080/20008198.2016.1273587
• Hoysted, C., Babl, F.E., Kassam-Adams, N., Landolt, M.A., Jobson, L., Curtis, S., Kharbanda, A.B., Lyttle, M.D., Parri, N., Stanley, R., & Alisic, E. (in press). Perspectives of Hospital Emergency Department Staff on Trauma-informed Care for Injured Children: An Australian and New Zealand Analysis. Journal of Paediatrics and Child Health.
Key references (III)EAR & Ear for Recovery Study• Mehl, MR, Pennebaker, JW, Crow, DM, Dabbs, J & Price, JH 2001, ‘The Electronically
Activated Recorder (EAR): a device for sampling naturalistic daily activities and conversations’, Behavior Research Methods Instruments and Computers, vol. 33, pp. 517.
• Mehl, MR, Robbins, ML & Deters, Fg 2012, ‘Naturalistic observation of health-relevant social processes: the Electronically Activated Recorder methodology in psychosomatics’, Psychosomatic Medicine, vol. 74, pp. 410-417.
• Mehl, MR, Vazire, S, Ramírez-Esparza, N, Slatcher, RB & Pennebaker, JW 2007, ‘Are women really more talkative than men?’, Science, vol. 317, no. 5834, p. 82.Robbins et al
• Alisic, E, Barrett, A, Bowles, P, Conroy, R, & Mehl, MR 2016, ‘Families coping with child trauma: A naturalistic observation methodology’, Journal of Pediatric Psychology, vol. 41, pp. 117-127.
• Alisic, E, Barrett, A, Bowles, P, Babl, FE, Conroy, R, McClure, RJ, Anderson, V & Mehl, MR 2015, ‘Ear for recovery: protocol for a prospective study on parent–child communication and psychological recovery after paediatric injury,’ BMJ Open, vol. 5, e007393
• Alisic, E., Gunaratnam, S., Barrett, A., Conroy, R., Jowett, H., Bressan, S., Babl, F.E.,McClure, R.J., Anderson, V. & Mehl, M.R. (2017). Injury talk: spontaneous parent-child conversations in the aftermath of a potentially traumatic event, working paper on PsyArXiv

Key references (IV)
Intimate partner homicide & ‘Care for Children after IPH’ study • Stöckl, H., Devries, K., Rotstein, A., Abrahams, N., Campbell, J., Watts, C., & Moreno, C. G.
(2013). The global prevalence of intimate partner homicide: a systematic review. The Lancet, 382, 859-865.
• Lewandowski, L. A., McFarlane, J., Campbell, J. C., Gary, F., & Barenski, C. (2004). "He killed my mommy!" Murder or attempted murder of a child's mother. Journal of Family Violence, 19, 211-220.Alisic et al BMC Psychiatry
• Alisic, E., Krishna, R.N., Groot, A., & Frederick, J.W. (2015). Children's mental health and wellbeing after parental intimate partner homicide: a systematic review. Clinical Child and Family Psychology Review, 18, 328-345
• Alisic, E., Groot, A., Snetselaar, H., Stroeken, T., & Van de Putte, E. (2015). Parental intimate partner homicide and its consequences for children: protocol for a population-based study. BMC Psychiatry, 15, 177
• Alisic, E., Groot, A., Snetselaar, H., Stroeken, T., & Van de Putte, E.M. (in press) Children Bereaved by Fatal Intimate Partner Violence: A Population-Based Study into Demographics, Family Characteristics and Homicide Exposure. PLOS One

Pictures – in order of appearance1. By Christian Gonzalez Alfonso, CC BY-NC 2.0 https://www.flickr.com/photos/cristyanlaison/2608123006/
2. By IHH Humanitarian Relief Foundation, CC BY-NC-ND 2.0 http://bit.ly/2v3Oxaf
3. By Douglas Sprott, CC BY-NC 2.0, http://bit.ly/2u4EgGj
4. By Sylvain Pedneault,CC BY-SA 3.0 https://commons.wikimedia.org/wiki/File%3AFirePhotography.jpg
5. By TBC, CC BY-NC 2.0
6. Alex Matthews, via Cartoonstock: http://bit.ly/2fKOrON
7. Sydney Harris: http://bit.ly/2vI9dlZ
8. Eva Alisic, personal picture
8. Roberto Volterra CC BY-NC 2.0 http://bit.ly/2v16OAP
9. Arend Groot, personal picture