when the last days are spent at home - csss bcstl · when the last days are spent at home practical...
TRANSCRIPT

When the last daysare spent at homePractical intervention guide

Published byCentre de santé et de services sociaux de Bordeaux-Cartierville–Saint-Laurent
Page layout, production and printingRobert Julien, Communications Department
Legal DepositBibliothèque nationale du QuébecISBN : 978-2-9809808-3-1 978-2-9809808 (pdf format) www.csssbordeauxcartiervillesaintlaurent.ca Under : Publications du CSSS

When the last days are spent at home
Practical intervention guide
By Lorie Lord Fontaine, Nurse, B.Sc., CSIO
Francine Lajeunesse, Nurse, B.Sc.
From the Department of Services for Persons Experiencing a Loss of Autonomy
With the participation of Karine Girard, Project Officeras part of the Program Support Service
of the Quality and University Mission Department
June 2007

“ In the fresh twilight of the evening,
life advances toward a new day… ”

When the last days are spent at home
Practical Intervention Guide Approaching death 7
Physical care 8
1. Oral care and hydration 8
2. Eye care 10 3. Skin care 10 a. Positioning 11 b. Urinary/fecal incontinence 13
4. Injectable medication 14
Death and after 16
References 18

When the last days are spent at home
Practical Intervention Guide
After having lived through the many emotions life brings, the time has come to experience the ultimate step: death. This step is a turning point for the relatives and accompanying a dying person can be very demanding.
Like snowflakes, each person is unique so, naturally, each death will also be distinct.
This practical intervention guide has been prepared to support natural caregivers who want to respect their loved one’s wish to die at home.
6

Approach ing death
As death becomes imminent, there are certain signs or physical manifestations that may occur :
eyes half-closed or glassya change in facial colourthe chin may dropdroolingirregular and difficult breathing accompanied by gargling sounds in the throat or chest (referred to as the death rattle) as the patient becomes too weak to coughweak or rapid pulsethe blood pressure may dropincreased agitation and anxietyrecovery of energygradual cooling of the bodyrosy colouring at the elbows, knees and ankles which can spread to the inside of the legs, thighs and backpurplish colouring of the hands and feetlittle urinationsemi-comatose or comatose state with no response to stimulation
▶▶▶▶▶
▶▶▶▶▶▶
▶▶▶
Even when your loved one does not appear to be conscious, your presence is comforting. Since hearing is the last sense to be lost, you should continue to speak to him.
7

Phys ica l care
1. Oral care and hydration
As long as your loved one is conscious and has a swallowing reflex, you can give him ice cubes, water or sparkling beverages, provided he is as close to a sitting position as possible. It is a good idea to help him brush his teeth or clean his dental prosthesis once or twice a day.
If the person is agitated, unconscious or semi-conscious, it is preferable to remove his dental prostheses. If he no longer has the swallowing reflex, do not force him to drink since it may cause complications, such as aspirating the fluid into the lungs.
Keep in mind that dehydration is not painful. If the mouth is kept moist, the person will not feel the sensation of thirst. A person who is dying often breathes through his mouth which makes it dry. When this occurs oral care should be provided approximately every two hours or when you change the patient’s position.
8

The following recipes may be applied with toothettes (little swabs with a sponge tip), a soft toothbrush or a facecloth :
begin by delicately rubbing the teeth, tongue, inside the cheeks, then the gums.if nystatin or magic mouthwash has been prescribed, you can continue to use it with a toothette.
If the mucous membrane is very dry : add a little mineral oil to the basic recipe
If there are scabs or deposits : add 1/3 cup of 3% hydrogen peroxide to the basic recipe, apply to the mouth and allow the effervescent effect to act for a few minutes, then rinse with a toothette imbibed with water
If the lips are dry : use a glaxal and/or vitamin E base cream (also good for the entire body)
▶
▶
1 cup of water½ teaspoon of sodium bicarbonate (baking soda)A pinch of salt
Avoid glycerine and lemon swabs as well as commercial mouthwashes containing alcohol that will dry the mouth.
Basic recipe
9

2. Eye care
Clean with eyes with a facecloth, wiping from the nose to the outside and using another corner of the facecloth for the other eye. If there are secretions, apply lukewarm compresses for a few minutes, then rub very gently to remo-ve them. You can also use no-tears baby shampoo or soap.
At the end of life, patients will often sleep with their eyes half-open due to weakness or simply because the eyelids no longer close completely. In this case it is important to keep the eyes humid with artificial tear drops which should be applied every two hours.
3. Skin care
a. Positioning It is important to change the patient’s position every two hours during the day and every four hours at night. Changing position helps to prevent bedsores and congestion in the lungs. If the mobilization seems to be painful, provide a painkiller approximately 30 minutes before changing the patient’s position.
It is important to monitor the bone pressure points (see Figure A). It is a good idea to gently massage the back and pressure points with a hydrating lotion or cream of your choice approximately three times a day when changing the patient’s position.
To avoid the too heavy and too tight covers on the level of the feet
Figure A
10

Reminder for positioning in the bed:
Align the head and trunkAllow a little flexion at the neck, wrist and fingersAvoid turning the legs to the outside when the patient is lying on his back
▶▶▶
Semi-lateral dorsal position
Semi-sitting position in bed
Here are two examples of positions:
11

Two methods for changing the patient’s position in bed
Method for raising the patient
Method for turning the patient
Position yourself at the top of the bed with one knee against the bed, keeping your back straight without twistingExtend your arms, take the drawsheet and roll it up to the trunkHold the drawsheet firmly in both hands and, pushing your foot on the ground, transfer your weight backwards as though you were going to sit on your heel. The patient will slide toward the top of the bed
1.
2.3.
Bend the patient’s legsBring the arm furthest away from you over his abdomenTurn his head to the side to which you are going to turn himRoll the edge of the drawsheet so that you can grip it firmlyTurn the person toward you, transferring the weight from one leg to the other
1.2.3.4.5.
12

b. Urinary/fecal incontinence
At the end of life, incontinence panties are often required. You must be sure to change them whenever they become soiled. At each change, wash and thoroughly dry the skin.
We recommend using protective creams such as Ihles paste. When the oint-ment becomes soiled, you will need to remove the surface and replace it with a fresh coat of paste. Avoid removing all the paste and rubbing the skin but, if you need to do so, use oil to clean the area (vegetable, mineral or baby).
If the patient suffers from urinary retention, or sometimes for other reasons, the nurse will install a urinary catheter. In this case, the following care proce-dure is required :
wash your hands before and after any manipulationplace the bag lower than the patient’s bladder to prevent refluxsake sure there are no knots in the tubing and that the cathe-ter drains wellempty the collection bag using the drainage valve every eight hours, or more often if necessary. A receptacle designed to receive urine must be used. Do not forget to reclose the valve to prevent spillsif the catheter becomes detached from the tubing. Use an alcohol swab to disinfect the outside of the catheter and the tubing, then put them back together
▶▶
▶
▶
▶
13
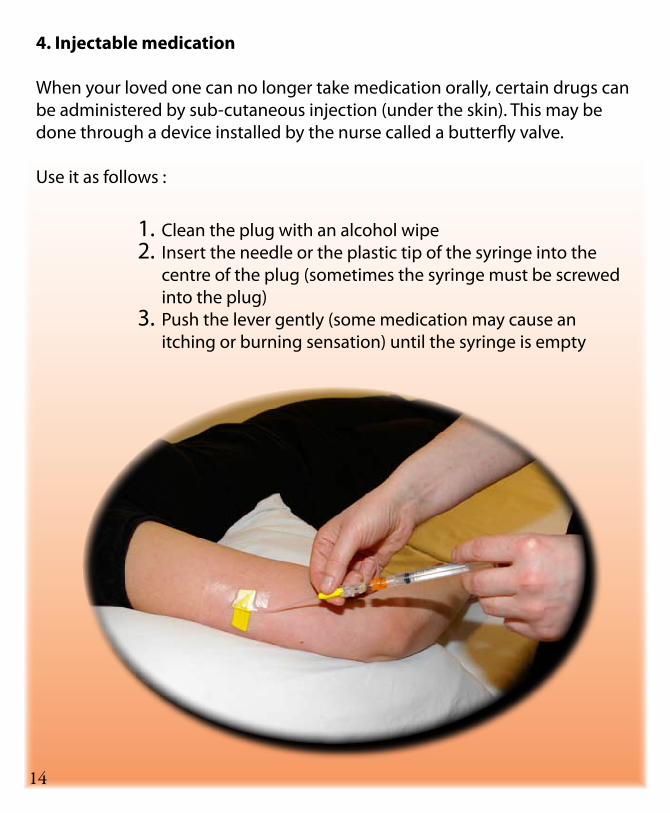
Clean the plug with an alcohol wipeInsert the needle or the plastic tip of the syringe into the centre of the plug (sometimes the syringe must be screwed into the plug)Push the lever gently (some medication may cause an itching or burning sensation) until the syringe is empty
1.2.
3.
4. Injectable medication
When your loved one can no longer take medication orally, certain drugs can be administered by sub-cutaneous injection (under the skin). This may be done through a device installed by the nurse called a butterfly valve.
Use it as follows :
14

Pain :morphine, dilaudid (hydromorphone)
Agitation/anxiety : ativan (lorazempam), versed (midazolam), nozinan (methotrimeprazine), haldol (haloperidol)
Rattling (secretions) :scopolamine (hyoscine), atropine, robinul (glycopyrrolate)
Difficulty in breathing :medication for pain and/or anxiety
Nausea or vomiting :gravol (dimenhydrinate), haldol (haloperidol), stemetil (prochlorperazine), decadron (dexamethasone)
▶
▶
▶
▶
▶
Do not hesitate to contact the nurse if you have a question or there is something you do not understand.
When certain symptoms occur, medication may be prescribed by the physi-cian to make your loved one more comfortable. They may be administered alone or as a combination. It is important to keep track of them using a table as illustrated below.
The following is a list of symptoms and the medication that is usually pres-cribed to relieve them :
15
TimeMedication Date 01 02 03 04 05 06 07 08 09 10 11 12Ex : Gravol 12/01/07 X X X

Death and af terWhen the person stops breathing, there is no need to hurry.
Here are some suggestions and advice :
Take the time you need together as a family. Contact the people who would like to be there. You can keep your loved one’s body for several hours.
Wash the body if necessary or desired.
Position the body on the back, in an attitude of rest.
Make sure you have the terminal illness certificate ornon-reanimation form.
Contact the physician so that he can sign the death certificate. If he is not available, call 911, indicating that it concerns a death that was expected so that the Urgences-Santé physician can come and fill out the certificate.
When the death certificate has been signed, contact the funeral salon you have chosen.
Do not forget to advise the practitioners at the CLSC of the death.
Return any unused medication to the pharmacy.
16

To facilitate the various steps you will need to take in regard to government and financial institutions, the Government of Quebec has prepared a brochure entitled “What to do in the event of death” available from your CLSC, the Government’s website at :
www.gouv.qc.ca Or by telephoning Communications Quebec :
1 800 363-1363.
Mourning is an experience that is unique to each individual. It may be very painful as your daily life will be filled with emotions and reactions which will probably come and go in varying intensity. If you feel overwhelmed or would like to be accompanied in the process of this bereavement, talk to a close friend or family member. Health and social service professionals are also available to help you: your family doctor, a nurse, psychologist or social worker. To find out more about these resources, contact your CLSC.
17

ReferencesMain reference
Mainville, M-C., (2005), Mourir à domicile, Éditions Ressources, National Library of Canada, ISBN 2-923215-03-6, 130 pages.
Other sources (in alphabetic order)
Canadian Association of Nurses in Oncology (1997), Le manuel de la douleur: Principes et problèmes de la gestion de la douleur causée par le cancer, S. Lawrence Librach, Bruce P. Squires. Pegasus Healthcare International and S. Lawrence Librach, 134 pages.
Cloutier, C., Landry, G., (1995), Soins palliatifs à domicile: Guide pratique d’intervention, CLSC Verdun/Côté St-Paul, 34 pages.
CLSC Beauce-Sartigan (2001), Guide d’intervention en soins palliatifs à domicile: maintien à domicile, 399 pages.
Fontaine, L. (1992), Alors qu’une vie s’achève: Guide pratique d’accompagnement des mourants de troisième âge, Les Éditions JML Inc., Bibliothèque nationale du Québec. ISBN: 2-89234-039-X, 96 pages.
Foucault, C. et Chapados, C., (1996) L’art de soigner en soins palliatifs: Perspectives infirmières, 2ième édition, Les Presses de l’Université de Montréal, National Library of Canada, ISBN 2-7606-1626-6, 215 pages.
Léveillé, G., (2000), Guide d’intervention clinique en soins palliatifs: à l’intention des infirmières et des infirmiers, La Maison Michel Sarrazin, Éditions Anne Sigier, Quebec, 197 pages.
Regroupement des pharmaciens en établissement de santé ayant un intérêt pour les soins palliatifs, (2002), Guide pratique des soins palliatifs: gestion de la douleur et autres symptômes, 3e édition, Association des pharmaciens des établissements de santé du Quebec, Montreal, 336 pages.
Smeltzer, S. et Bare, B., Soins Infirmiers, Médecine et Chirurgie, Fonction Génito-urinaire, p.1037.
18

AcknowledgementsThis guide was produced with the financial support our CSSS within the scope of the Projets qualité initiative designed to improve the quality of client services.
A special thank you to everyone who contributed to the preparation of this Guide.
19

Centre d’hébergement Notre-Dame-de-la Merci(Administrative center)555, Gouin Blvd. West, Montreal, H3L 1K5 (514.331.3020)
Centre d’hébergement Saint-Joseph-de-la-Providence11810, Bois-de-Boulogne Ave., Montreal, H3M 2X7 (514.334.3120)
Pavillon des Bâtisseurs11844, Bois-de-Boulogne Ave., Montreal, H3M 2X6 (514.334.4817)
Centre d’hébergement de Saint-Laurent1275, Côte-Vertu Blvd, Saint-Laurent, H4L 4V2 (514.744.4981)
CLSC de Bordeaux-Cartierville11822, Bois-de-Boulogne Ave., Montreal, H3M 2X6 (514.331.2572)
CLSC de Saint-Laurent1055, Sainte-Croix Ave., Saint-Laurent, H4L 3Z2 (514.748.6381)
Centre d’hébergement de Cartierville12235, Grenet St., Montreal, H4J 2N9 (514.337.7300)
sitesOur
www.csssbordeauxcartiervillesaintlaurent.ca