when laughing is no longer funny - amazon s3laughing+is+no+long… · when laughing is no longer...
TRANSCRIPT

NICHE Online Connect Webinars | 2016 1
When Laughing is No Longer Funny Managing Transient Urinary Incontinence in
Hospitalized Elderly Women
Grace Umejei, BSN, RN, CWOC.
Texas Health Presbyterian Hospital Dallas

NICHE Online Connect Webinars | 2016 2
Objectives
• Identify Transient Urinary Incontinence (TUI) and discuss outcomes on the Healthcare System
• Discuss the effectiveness of behavioral modification therapy (BMT) in reducing TUI episodes
• Review the outcome of management of TUI in elderly female patients.
Mechanism of Urination
• bladder, the muscular wall
• nerve
• the brain
• urethral closure muscle
Classification and Types of Incontinence
Categories of UI
• Transient Incontinence –incontinence with reversible causes.
• Established Incontinence – when transient cause have been addressed and incontinence persists

NICHE Online Connect Webinars | 2016 3
Urinary Incontinence (UI)
• Stress – Occurs with increased abdominal pressure.
• Urge – sudden overwhelming need to urinate without ability to control
urine flow, when urinary sphincter fails as a result of pelvic floor weakness to support uterus, bladder, and other pelvic organs.
• Overflow – involuntary leakage of urine small amounts, associated with incomplete bladder emptying mechanical forces on distended bladder
• Functional – contributing factors outside urinary system not
characterized by bladder dysfunction. Inability to get to the bathroom, cognition impairment.
Facts About Urinary Incontinence
• People > 65 years are the reason for a growing hospital population.
• This segment of the population have the greatest need for health care.
• Acute hospital settings 20% to 42% of older adult patients are affected by UI
• 42.5% of UI patients have some type of skin injury.
TUI Background
• Involuntary urine loss with reversible causes.
• Negatively impacts patient outcomes, e.g.
independence, mood, falls, and skin integrity
• Affects 80% of hospitalized patients and
75% of females >60 years of age
• Cost of managing TUI is $26 billion annually

NICHE Online Connect Webinars | 2016 4
Gertrude’s Story
Literature ReviewEvidence based practice (EBP) TUI interventions
include:
• BMT, i.e. bladder training and lifestyle
modifications based on TUI assessments and
causation
• Daily bladder diary (BD) to track
continence/incontinence episodes/toileting
behaviors
• Staff education on use of BD and BMT strategy
• Patient education and counseling
PICOT Question
Is BMT (including a BD) more effective than
passive TUI care in reducing TUI episodes
in elderly hospitalized female patients on a
rehabilitation unit?

NICHE Online Connect Webinars | 2016 5
Change Strategy
• Inter-professional team formed
• Educated inter-professional team on treatment plan and management strategies
• Inter-professional team used the BD to establish toileting schedule/assess BMT effectiveness
• Incontinence episodes tracked with use of BD
• Patients queried prior to discharge on BMT satisfaction and use of incontinence protection (i.e. adult briefs)
Inter-Professional Team
• Nurses
• Patient Care Technician
• Chaplain
• Occupational Therapist (OT), Physical Therapist (PT)
• Wound Ostomy and Continence Nurse
• Physicians
• Dietary Staff
Behavioral Modification Therapy
Foundation for behavioral intervention
• Bladder Training – Skills to control symptoms of bladder dysfunction.
• Lifestyle Modification– Healthy bladder habits that will alleviate bladder symptom, enhance
function and promote bladder health

NICHE Online Connect Webinars | 2016 6
Behavioral Modification Therapy
Detection
• Identify transient causes of UI and individual patient risk factors.
• Determine the actual or potential effect of incontinence on patient’s quality of life and functional statues.
• Anticipate and address potential complications based on established causes.
• Develop a set of interventions that target the risk factors and causes for each patient through consistent approach to evaluation. May Utilize Urinary Incontinence Assessment for Older Adults (Hartford Institute for Geriatric
Nursing, New York University, College of Nursing)
Bladder Diary
Key:
D –Diaper BSC-Bedside Commode
P- Bed Pad BP-Bed pan
PU- Pull Ups
T- Toilet
DIAPPERS Tools for Determining TUI
D Delirium Acute confusion alters one’s ability to
anticipate and meet own needs. Delirium
may occur from drugs, surgery, or acute
illness.
I Infection Urinary tract infection
A Atrophy Thin dry, friable vaginal and urethral
mucosa due to Hypo-estrogenization in
older female is associated with irritating
symptoms (burning on urination, urgency,
frequency)
P Pharmaceuticals Drugs including sedatives, hypnotics,
alcohol, anticholinergic, antihistamine,
narcotics, loop diuretics.
P Psychological
condition
Depression impairs one’s motivation and
desire to manage self-care or be
concerned about incontinence.
Fear of odor, embarrassment, obvious
leakage, and unpredictable urine leakages
can lead to marked alternation in social
activities, relationships with others, and
loss of social support.
E Excess urine
output
Excess urine output resulting large fluid
intake, caffeinated beverages endocrine
problems CHF, Peripheral edema
R Restricted mobility Poor mobility, arthritic pain, poor use of
assistive device
S Stool Impaction Narcotic use can lead to severe
constipation and fecal impaction that
obstruct the bladder neck, leading to urine
retention and/or overflow incontinence
Transient Causes of
Urinary Incontinence
and other contributing
factors

NICHE Online Connect Webinars | 2016 7
Incontinence Training-NursingAssessment
• Focused Assessment
• Determine Cause
Intervention• Develop individualized plan of care using data obtained from the history and
physical examination, and in collaboration with other team members
Evaluation of Outcome• Bladder Diary
• Follow up assessment
Nursing Education
Patient assessment.• Perform Comprehensive Assessment
• Focused Urinary Incontinence assessment
• Determine Neurological Status
• Identify Mobility and Activity Level
Incontinence Training-Patient
Counseling
Intervention
• BMT
Evaluation
• Follow up patient questionnaire

NICHE Online Connect Webinars | 2016 8
Bladder Re -Training
• Progressive voiding schedule, using relaxation and distraction techniques together with multicomponent behavioral training which patient has to learn.
• Positively affects mobility, behavior, skin integrity, urinary tract infection and bowel function.
Goal• Increase amount of time between emptying your urinary bladder and amount of
urine your bladder can hold.• Diminish leakage and sense of urgency associated with incontinence
• Determine fixed voiding schedule that corresponds to patients’ assessment
Bladder Re-Training
Prompted Voiding• Neurologically Intact
• Responsibility of RN/PCT/Patient and interdisciplinary team
• Description– Prompt patient on a schedule of every three hours during the day and every
four hours at night as time allows.
– Report continence status and to assist to the toilet
– Provide positive feedback for maintenance of continence.
• Goal– To keep the patient dry and to increase the patient’s awareness of
incontinence status and participation in bladder program
Bladder Re- Training Cont.
Scheduled Voiding
• Patients with Cognitive Impairment• unable to accurately determine wetness or dryness
• unable to take responsibility for self-toileting but able to follow instructions
with assistance.
• Responsibility - RN/PCT/Patient and interdisciplinary team
• Description• Every two hours while awake – every four hours at night the patient is taken
to the toilet (or bedside commode) on schedule and cued to void
• Goal• Prevent over-distention of bladder and keep the patient dry by toileting
frequently enough to prevent incontinence.

NICHE Online Connect Webinars | 2016 9
Bladder Re Training cont.,
• URGE Suppression Techniques – Freeze, Squeeze, Breathe or Distraction.
• If urge cannot be suppressed and you must go slowly
• DOUBLE Voiding
Lifestyle Modification
Habits that may be modified to alleviate bladder symptoms or
promote bladder health
Dietary
• Ensure adequate fluids
• Avoid caffeinated beverages
• Promote high-fiber diet for bowel regularity
• Promote a regular voiding schedule, about every 3 hours
Pharmacology
• Monitor poly-pharmacy, drug interactions
Life style Modification Cont.
Mobility• OT, PT. to assist with gait or transfer training, assistive devices, develop
toilet skills to promote independence.
• Utilize clothing that is easy to undo to promote independence in toileting.
• Monitor for transient causes of urinary incontinence and treat quickly.
Social Environment• Promote a positive approach to continence.
• Promote socialization.
• Assist with toileting if needed
• Recognize urinary incontinence as medical syndrome that is abnormal, promote the desire to maintain urinary continence.
NICHE Online Connect Webinars | 2016 10
Lifestyle Modification cont.
Environmental Modifications• Physical Environment
• Ensure good lighting in room, bathroom, call light within reach
• Obtain bedside commode, promote independence.
• Non-skid sock, non-glare floor also cord free floors
Smoking cessation• Optimal treatment outcome changes
• Adhering to these changes will require significant behavioral changes from the patient.
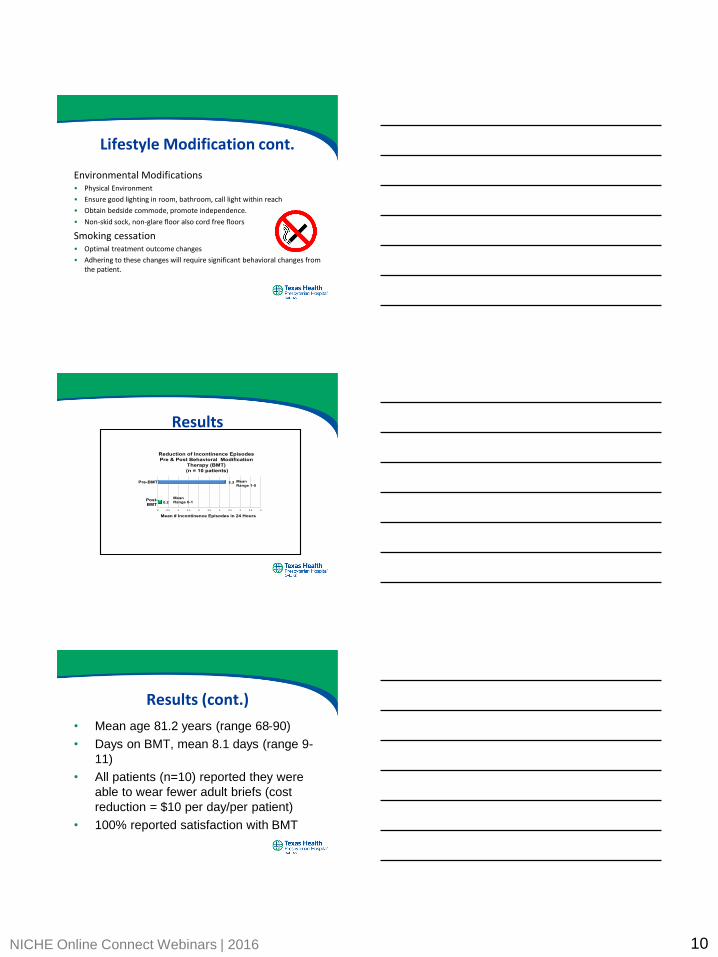
Results
0.2
3.3
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5
Post-
BMT
Pre-BMT
Mean # Incontinence Episodes in 24 Hours
Reduction of Incontinence Episodes
Pre & Post Behavioral Modification
Therapy (BMT)
(n = 10 patients)
Mean
Range 1-5
Mean
Range 0-1
Results (cont.)
• Mean age 81.2 years (range 68-90)
• Days on BMT, mean 8.1 days (range 9-
11)
• All patients (n=10) reported they were
able to wear fewer adult briefs (cost
reduction = $10 per day/per patient)
• 100% reported satisfaction with BMT

NICHE Online Connect Webinars | 2016 11
Conclusion
• BDs are effective TUI management tools;
maintaining documentation is challenging.
• BMT is a cost-effective EBP intervention
Summary
• Increase of elderly patients with UI.
• Behavioral modification interventions can significantly improve symptoms of TUI when education, counselling, support and encouragement are applied.
• Need to implement BMT in acute care setting in order to reverse the current practice of focusing TUI management on UI consequences rather than treating underlying causes of UI.
Thank you!

NICHE Online Connect Webinars | 2016 12
References
DuBeau, C. E., Kuchel, G. A., Johnson II, T., Palmer, M. H., & Wagg, A. (2010). Incontinence in the frail elderly: Report from the 4th international consultation on incontinence. Neurology and Urodynamic, 29, 165-178.
Melville, J.L., Katon, W., Delaney, K., Newton, K. (2005). Urinary incontinence in US women: A population-based study. Archive Internal Medicine, 165(5) 537-542.
Shamliyan, T., Wyman, J., Kane, R.L. (2012) Nonsurgical treatments for urinary incontinence in adult women: Diagnosis and comparative effectiveness. Agency for Healthcare Research and Quality, 36.
Wyman, J.F., Burgio, K.I., Newman, D.K. (2009). Practical aspects of lifestyle modifications and behavioral interventions in the treatment of overactive bladder and urgency urinary incontinence. International Journal of Clinical Practice, 63(8), 1177-1191.
Questions