what's really behind canada's unemployed specialists?: too many
TRANSCRIPT

Findings from the Royal College’s
employment study - 2013
Too many, too few doctors?
What’s really behind Canada’sunemployed specialists?

Report Authors:
Danielle Fréchette, MPA1,2 Executive Director
Daniel Hollenberg, Ph.D.1,2 Research Associate
Arun Shrichand, BA1,2
Senior Analyst, Health System and Policies
Carole Jacob, MCS1,2
Manager, Health Policy Program Development
Indraneel Datta, MD, MSc (HEPM), FRCSC3 Clinical Assistant ProfessorGeneral Surgeon, Alberta Health Services
Research Team:
Danielle Fréchette, MPA1,2 Principal InvestigatorExecutive Director
Daniel Hollenberg, Ph.D.1, 2 Co-Principal InvestigatorResearch Associate
Carole Jacob, MCS1,2
Manager, Health Policy Program Development
Arun Shrichand, BA1,2
Senior Analyst, Health System and Policies
Galina Babitskaya, BSc1, 2
Database Analyst
Jonathan Dupré, BSc1
Data and Research Analyst, Educational Research Unit
Indraneel Datta, MD, MSc (HEPM), FRCSC3
Clinical Assistant ProfessorGeneral Surgeon, Alberta Health Services
1 Royal College of Physicians and Surgeons of Canada
2 Offi ce of Health Systems Innovation and External Relations
3 Department of Surgery, University of Calgary
Findings from the Royal College’s employment study – 2013
Suggested citation: Fréchette, D., Hollenberg, D., Shrichand, A., Jacob, C., & Datta, I. 2013. What’s really behind Canada’s unemployed specialists? Too many, too few doctors? Findings from the Royal College’s employment study. Ottawa, Ontario: The Royal College of Physicians and Surgeons of Canada.
© 2013 Royal College of Physicians and Surgeons of Canada.

Findings From The Royal College’s Employment Study - 2013
A fi rst in health system researchIn 2010, several of Canada’s national medical specialty societies reported to the Royal College that a growing
number of specialist physicians were unemployed or under-employed. The Royal College undertook research
into this highly complex problem, seeking to determine if unemployment and under-employment are the simple
and inevitable byproducts of an oversupply of physicians — or if other, more subtle factors come into play.
This report presents the fi ndings of our research to date — most notably the state of employment of new
specialists and subspecialists certifi ed in 2011 and 2012 and the key drivers and infl uencers behind their
employment challenges. (The report delves into the employment issues of specialist physicians only and does
not delve into any employment issue that may affect family physicians.)
The Royal College has unique access to specialist physicians in Canada and, as such, was able to collect
a unique set of data to inform this report. The Royal College surveyed newly certifi ed specialists and
subspecialists online for this this study, and interviewed more than 50 persons with fi rst-hand, in-depth
knowledge of the issues who provided important new insights. It is our hope that this study will spark
additional research and data collection into the phenomenon of specialist unemployment and under-
employment so that health care stakeholders can work together to identify and address the countless
factors that contribute to this growing challenge.
What our research revealed
Sixteen percent of new specialist and subspecialist physicians said they cannot fi nd work; 31 percent pursue further training to become more employable.
Data from the Royal College’s 2011 and 2012 employment surveys reveal that employment issues extend
across multiple medical specialties. Among those who responded to the surveys of new specialists and
subspecialists, 208 (16%) reported being unable to secure employment, compared to 7.1% of all Canadians
as of August 2013. Of these, 122 stated they were or would be pursuing further training and 86 reported that
they were unemployed and without a training post. Also of note is the signifi cant number of new specialists
and subspecialists — 414 (31.2%) — who chose not to enter the job market but instead pursued further
subspecialty or fellowship training because they believed such training would make them more employable.
Executive summary
EXEC
UTI
VE
SUM
MA
RY
2

Findings From The Royal College’s Employment Study - 2013
Employment challenges are increasing.
Comparison by year shows that employment challenges increased in 2012 over 2011. Those reporting
employment issues increased by four percentage points (from 13% to 17%) for specialists and by six percentage
points (from 15% to 21%) for subspecialists. Findings also show potential provincial variances, which merit
further investigation.
Locum and part-time positions are often a default option to unemployment.
Almost 22% of new graduates reported they are staying employed by combining multiple locum positions
(assuming another physician’s duties temporarily) or various part-time positions. Forty percent stated they were
not satisfi ed with their locum placement.
Employment issues are most pronounced in resource-intensive disciplines.
The survey revealed that a substantial proportion of new physicians experiencing employment issues were from
surgical and resource-intensive disciplines, including but not limited to: critical care, gastroenterology, general
surgery, hematology, medical microbiology, neurosurgery, nuclear medicine, ophthalmology, radiation oncology
and urology.
Three key drivers contribute to employment issues.
The online surveys and interviews revealed new fi ndings and confi rmed hearsay. We have clustered our
fi ndings under the following three drivers: the economy, the health system and personal factors.
1. The economy is the main factor driving new medical and surgical specialist under- and unemployment in Canada.
More physicians are competing for fewer resources
Much of specialty medical care depends on institutional health care facilities such as hospitals and their
resources, including operating rooms and hospitals beds. Access to these resources directly impacts
physician employment. While the health care needs of patients increase and the number of physicians
and surgeons continues to grow, hospital funding growth continues to slow. To control costs, resources
such as operating room time are cut. Physicians are competing for fewer resources. EXEC
UTI
VE
SUM
MA
RY
3

Findings From The Royal College’s Employment Study - 2013
Weak stock markets delay retirements
The stock market’s relatively weak performance in recent years means many medical specialists are
delaying their retirements. Long-held positions are not freeing up as expected and will not likely free
up until markets improve.
2. The way in which the health care system is organized contributes to under- and unemployment of new medical and surgical specialists.
The role of interprofessional care models
Interprofessional collaborative practice—in which multiple health workers from different professional
backgrounds provide care to patients—is increasingly taking root in Canadian healthcare. With this
development comes a new range of health professional roles and responsibilities that affect how
Canadians interact with medical services and physicians. Here is what we learned:
• Interprofessional models reduce reliance on physicians, slow job growth.
These new roles associated with interprofessional care models complement and in some cases
substitute physician services, making it possible to increase the amount of specialty medical care
that physicians and surgeons provide without increasing the number of jobs.
• Interprofessional models are reducing reliance on residents for service, enabling the
potential to better align supply of new physicians with longer-term patient needs.
Our research reveals a promising trend that some teaching facilities are adapting models of care
to include health professionals that complement or substitute for physicians. Residency programs
in these locales are therefore relying less on residents to fi ll service gaps and not taking in as
many residents. They are adjusting resident intake with what they believe will be future needs.
This is good news because the educational system will be more likely to produce the number of
specialist physicians needed rather than taking in additional residents as “boots on the ground”.
Unfortunately, this is not yet the case everywhere. This is an area that requires further research.
Workforce planning
• Determining and allocating the number of residency positions is complex and may not
always take into account societal heath needs and available resources.
Approaches for allocating residency positions can vary greatly among the provinces and territories
and decisions are broadly based on scant information about longer-term societal health needs and
health care resources. In addition, new medical graduates may not remain in the jurisdiction where
they trained, creating further imbalances in the medical supply.
EXEC
UTI
VE
SUM
MA
RY
4

Findings From The Royal College’s Employment Study - 2013
• Increasing reliance on residents can lead to overproduction.
Academic health facilities must often balance their immediate service requirements (which are
often met by residents) with the number of physicians they will need in the future. Put another
way, when additional residency positions are created to meet immediate needs, the number of
new specialists and subspecialists eventually certifi ed may exceed the number of positions needed
and available over the long term. This can happen despite the potential of better balancing service
needs through interprofessional care models (see above).
Culture of practice infl uences physicians’ willingness to share resources
Most health professions develop a personal culture of practice, which is motivated by both altruism
and self-interest. Given that the availability of clinical and practice resources is generally fi xed (this is
especially true of operating room time) established specialists can be reluctant to share resources. This
is because they wish to protect their access to clinical resources for their patients and their incomes.
Income protection is especially important for those whose retirement portfolios have been negatively
affected by the recent economic downturn.
3. Personal and context-specifi c factors drive employment challenges among new graduates.
Residents report a lack of adequate career counseling and information about jobs
The importance of career counseling for specialists cannot be overemphasized; career choices are key
to these physicians’ futures and to how they are distributed across the country. More than half of
new specialists in our study said they had not received any career counseling and more than one third
without jobs and who were not continuing training in 2012 reported that poor access to job postings
hampered their ability fi nd a job. Lack of transparency about available jobs also hindered their ability to
fi nd suitable work.
Research fi ndings reveal that a more systematic and comprehensive approach to career counseling and
job advertising than currently exists in Canada is needed to meet the needs and objectives of individual
physicians as well as the system.
Personal preferences infl uence choices
Personal factors infl uence the choices that physicians make about the type and location of practice they
will pursue. This is a byproduct of many infl uencers, including:
• the relatively late age at which new medical specialist graduates enter independent practice.
Many new graduates have family responsibilities that might make it harder to move to available
job opportunities (sandwich generation, spousal employment, etc.)
• individual career preferences such as practice location or type.
EXEC
UTI
VE
SUM
MA
RY
5

Findings From The Royal College’s Employment Study - 2013
Employment challenges are creating a new type of specialist, and contributing to “brain waste” and “brain drain”.
New specialists who lack access to hospital suitable resources, or who cannot fi nd jobs in the settings they
require, are developing ‘tailored’ or ‘morphed’ practices that allow them to work within the resources available
to them. These new practices do not embrace the full spectrum of specialists’ abilities, resulting in skill loss and
under-employment (such as when a surgeon cannot operate). This condition is called “brain waste”.
Just under 20% of recently certifi ed medical and surgical specialists who have not found positions reported
they would look for work outside Canada. The predicted physician shortages in the US may become a
market for Canada’s unemployed specialists, prompting a “brain drain”.
We need to think in new ways about medical workforce planning.
While our research has revealed many specifi c factors that contribute to specialist unemployment and under-
employment, a single, overarching message has also emerged: that a signifi cant gap appears to exist in medical
workforce planning in Canada. Most planning approaches attempt to produce the right mix and number
of physicians based on society’s health needs. But that is only part of the picture. Many specialty medical
and surgical disciplines require specifi c resources such as operating room time and hospital beds to function
effi ciently. With health care spending challenges, specialists often have limited access to such resources, which
affects the number able to practice as well as how much work each specialist can undertake.
It has become clear that medical workforce planning must consider the availability of practice resources as
well as the health needs of the population. Such an approach will help physicians do the work they have been
trained to do; to do otherwise will perpetuate physician unemployment. It will also worsen physician brain
waste and under-employment since physicians will be able to apply only a portion of their knowledge and skills
based on the resources available to them.
EXEC
UTI
VE
SUM
MA
RY
6

Findings From The Royal College’s Employment Study - 2013
Glossary of acronyms AA Anesthesia assistant
AAMC Association of American Medical College
AFMC Association of Faculties of Medicine of Canada
CAIR Canadian Association of Internes and Residents
CAPA Canadian Association of Physician Assistants
CIHI Canadian Institute for Health information
CNS Clinical nurse specialist
FTE Full-time equivalent
FMEC-PG Future Medical Education in Canada – Postgraduate Project
HRH Human resources for health
NSS National specialty societies
NP Nurse practitioner
OR Operating room
PA Physician assistant
PGME Postgraduate medical education
List of graphs and fi gures Table 1 Royal College Employment Survey, 2011and 2012 combined: Population and sample data, by response
rates, age and gender
Table 2 Royal College Employment Survey, 2011 and 2012: Response rates by province of postgraduate training
Table 3 Royal College Employment Survey, 2011 and 2012: Disciplines reporting the most employment diffi culties
Table 4 Royal College Employment Survey, 2011 and 2012: Number of new certifi cants pursuing further training
because they could not fi nd a position
Table 5 Royal College Employment Survey, 2011 and 2012: Most important reason why respondents stated they
could not fi nd a job
Table 6 Royal College Employment Survey, 2011 and 2012: Percentage of respondents stating they had not received
any career counseling
Table 7 Royal College Employment Survey, 2012: Type of career counseling reported by new specialists and
subspecialists
AC
RO
NY
MS,
LIS
T O
F G
RA
PHS
AN
D F
IGU
RES
7

Findings From The Royal College’s Employment Study - 2013
List of graphs and fi gures Figure 1 Royal College Employment Study Phases
Figure 2 Royal College Employment Survey, 2011 and 2012: Employment status reported by new specialists and
subspecialists, Canada
Figure 3 Royal College Employment Survey, 2011 and 2012: Employment status reported by new specialists, 2011
and 2012 comparison, Canada
Figure 4 Royal College Employment Survey, 2011 and 2012: Employment status reported by new subspecialists, 2011
and 2012 comparison, Canada
Figure 5 Royal College Employment Survey, 2011 and 2012: Employment status reported by new specialists and
subspecialists, by province of residency training, Alberta
Figure 6 Royal College Employment Survey, 2011 and 2012: Employment status reported by new specialists and
subspecialists, by province of residency training, British Columbia
Figure 7 Royal College Employment Survey, 2011 and 2012: Employment status reported by new specialists and
subspecialists, by province of residency training, Manitoba
Figure 8 Royal College Employment Survey, 2011 and 2012: Employment status reported by new specialists and
subspecialists, by province of residency training, Newfoundland and Labrador
Figure 9 Royal College Employment Survey, 2011 and 2012: Employment status reported by new specialists and
subspecialists, by province of residency training, Nova Scotia
Figure 10 Royal College Employment Survey, 2011 and 2012: Employment status reported by new specialists and
subspecialists, by province of residency training, Ontario
Figure 11 Royal College Employment Survey, 2011 and 2012: Employment status reported by new specialists and
subspecialists, by province of residency training, Québec
Figure 12 Royal College Employment Survey, 2011 and 2012: Employment status reported by new specialists and
subspecialists, by province of residency training, Saskatchewan
Figure 13 Royal College Employment Survey, 2011 and 2012: New specialists/subspecialists with a job, by type of
placement, Canada
Figure 14 Royal College Employment Survey, 2011 and 2012: New specialists with a job, by type of placement, by
province of residency training
Figure 15 Royal College Employment Survey, 2011 and 2012: “Is your locum placement satisfactory to you at this
time?”, percent response of specialists and subspecialists, Canada
Figure 16 Public sector health expenditure growth, Canada, 2002-2012
Figure 17 Resident satisfaction with employment or career counseling resources within their residency program
Figure 18 Royal College Employment Survey, 2012: No job placement and at end-point of residency training (n=49),
Why you feel you do not have a job placement?
LIST
OF
GR
APH
S A
ND
FIG
UR
ES
8

Findings From The Royal College’s Employment Study - 2013
Executive summary
> A fi rst in health system research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
> What our research revealed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
> Glossary of acronyms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
> List of graphs and fi gures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
1.0 Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.0 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
3.0 Research Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
> Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
> Research questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
> Study design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
> Data collection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
4.0 Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
> 4.1 The current landscape . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
> 4.2 Key drivers and infl uencers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
> 4.2.1. Economy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
> 4.2.2. System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
> 4.2.3. Personal context . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
5.0 What are the effects of employment challenges on new graduates? . . . . . . . . . . . . . . 52
> 5.1 Tailored and morphed practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
> 5.2 Leaving Canada . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
6.0 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
TAB
LE O
F C
ON
TEN
TS
Table of contents
9

Findings From The Royal College’s Employment Study - 2013
Preface 1.0
PREF
AC
E
10
After many years of talk of physician shortages, pockets of evidence have emerged in recent
years demonstrating that some medical specialists and subspecialists in some disciplines
are experiencing diffi culties fi nding employment in Canada. First experienced by cardiac
and orthopedic surgeons, this trend has been expanding to other disciplines in various
jurisdictions. With this comes talk that there may be an oversupply or surplus of physicians.
We must all avoid knee jerk reactions and quick fi xes. It is important to understand the facts and to create
meaningful solutions, not a different set of problems for Canadians.
Given the absence of any discussion of this new trend in the peer reviewed and grey literature, the Royal
College undertook and continues its comprehensive research to begin unpeeling the complex layers around
this troubling trend.
This report refl ects fi ndings from two years of research. It does not recommend solutions. These will need
to be developed by a broad group of stakeholders, including those directly affected and those who can
effect change.
Hopefully, the fi ndings presented in this report will spark others to dig deeper and to work toward solutions.
Danielle Fréchette, MPA
Executive Director, Offi ce of Health Systems Innovation and External Relations
Principal Investigator, Royal College Employment Study

Findings From The Royal College’s Employment Study - 2013
Introduction 2.0
INTR
OD
UC
TIO
N
11
As part of its preparation for the Royal College’s annual human resources for health
(HRH) conference with Canada’s national medical specialty societies (NSS) in 2010, the
Royal College’s Office of Health Policy conducted an exploratory inquiry with the NSS
to tease out HRH issues and concerns. During the inquiry phase, a number of societies,
without prompting, identified issues around physician employment (Royal College, 2010,
p. 3). This led to a consensus during that year’s conference that the Royal College should
examine this issue further given the absence of any discussion of this new trend in the
peer reviewed and grey literature (Royal College 2010 (2), p.10; Feindel 2010).
Economists theorize that a workforce surplus exists when the quantity of labour is greater than the
quantity demanded (Hall & Lieberman 2007, page 354). From this, the logical conclusion could be that Canada’s
medical schools are producing too many new specialists given that a number of them have recently been
unable to find work. Yet, wait times for medical, diagnostic and surgical services persist (Harrington 2013;
Wai et al. 2012; Tomlinson, Wong, Au & Schiller 2012, Discussion section, para. 5; CIHI 2013). Given these hard realities,
the notion that the physician labour supply exceeds the quantity demanded is difficult to reconcile.
So, the question is do we have too many physicians or are there other factors in play?
The state of physician employment and what lies behind it is a complex matter that could be examined
in a number of ways. To keep the research agenda manageable, the research undertaken to date and
presented in this report focuses on a high level, national picture of specialists who are newly certified by
the Royal College of Physicians and Surgeons of Canada. As such, family physicians are not addressed
in our research. We understand that additional research and analysis – which is not restricted to new
practitioners and depicts the medical workforce at large – is needed to develop a more comprehensive
picture of the physician employment situation. This must include granular investigations at the age, sex,
specialty/subspecialty, and jurisdiction-specific levels. We will continue our work and encourage others
to delve into the subject matter.
For now, we have a much clearer picture of the state of employment of new specialists and subspecialists,
and the main drivers behind the employment challenges experienced by new medical specialty certificants
– the economy, the system, and their personal context – which are explored in greater detail in the next
sections of this report. These main drivers and associated factors are often interconnected. We are
exploring them separately so as not to overly complicate what is already complex.

Findings From The Royal College’s Employment Study - 2013
Research methodology 3.0
RES
EAR
CH
MET
HO
DO
LOG
Y
12
Background
The impetus for this study stems from an exploratory inquiry conducted by the Royal College in 2010
with the national specialty societies (NSS)*, as part of preparations for its annual human resources for
health conference. The inquiry consisted of an online survey and semi-structured interviews of 39 NSS,
and was aimed at gaining general insights on the workforce challenges facing specialty medicine. One of
the findings of this inquiry was that select specialties were experiencing difficulties finding employment
in Canada, including those in: neurosurgery, cardiac surgery, plastic surgery, public health and preventive
medicine (previously community medicine), otolaryngology, nephrology, and radiation oncology (Royal
College 2010, p. 3).
These findings were subsequently presented to NSS at the 2010 Royal College/NSS human resources for
health conference. During the course of the conference, participants encouraged the Royal College to
examine the issue of physician employment in a more systematic way (Royal College, 2010 (2), p. 10).
Research questions
Given the complexity of systems research, an attempt at identifying perceived barriers to physician
employment is foundational to any further research. Therefore, the following central question and
subquestions (Creswell & Plano Clark 2010) were proposed:
What factors contribute to new specialist physicians having difficulties finding employment in Canada?
• Are there too many physicians in their specialty to meet population health care
needs (oversupply or overproduction)?
• Are employment difficulties a byproduct of other factors (e.g., social construct,
economics or policy driven)?
* Professional groups of physicians organized around a particular medical, surgical, or laboratory specialty or subspecialty.

Findings From The Royal College’s Employment Study - 2013
Qualitative: Key informant
interviews
Quantitative: Online survey
data collection and analysis
Interpretationof findings
Qualitative: Key informant
interviews (2nd phase) Data collection and analysis
Quantitative: Online survey
content developmentPhase 1
Phase 2
Phase 3
RES
EAR
CH
MET
HO
DO
LOG
Y
13
Study design This study utilized a mixed-method research approach that combined key informant interviews and
an online survey. This research design was thought to be most appropriate given the exploratory nature
of the work and the lack of available data pertaining to the area of inquiry (Creswell 1994; Greene, Caracelli
& Graham 1989).
In terms of pacing and implementation of the qualitative (key informant interviews) and quantitative (online
survey) strands of the study, a multiphase combination timing approach was adopted (Creswell et al. 2010).
As illustrated in Figure 1 below, an initial phase of key informant interviews was fi rst conducted to help
identify key themes that would inform the development of the online survey. Following the development
and dissemination of the fi rst iteration of the online survey (in 2011), the two data instruments have been
implemented concurrently. Findings from the online survey and key informant interviews were compared,
integrated and interpreted – as presented in this report.
FIGURE 1 Royal College Employment Study Phases

Findings From The Royal College’s Employment Study - 2013
RES
EAR
CH
MET
HO
DO
LOG
Y
14
Data collection
Interviews with key informants
Semi-structured, face-to-face and telephone interviews were conducted in a sample of individuals
perceived as ‘insiders’ (those with fi rst-hand, in-depth knowledge of the subject matter). The fi rst phase
of interviews was conducted with the Royal College’s specialty committee chairs (which helped inform
the online survey) and the subsequent second phase of interviews included other specialty committee
chairs, select program directors, resident associations, senior hospital administrators, postgraduate deans,
residents and other representative groups.
An interview guide was developed a priori and outlined questions intended to prompt discussion and
refl ection. Interviews ranged from 30 to 45 minutes, and delved into areas of inquiry that included (but
were not limited to) exploring the
• National picture at specialty-specifi c level,
• Post-certifi cation training trends,
• Employment patterns among new graduates,
• Enablers, barriers, future plans related to employment, and
• Perceived system issues
Under the guidance of The Ottawa Hospital Research Ethics Board, participants were approached and
asked to confi rm consent to participate in the study. All participants were informed of their rights
(voluntary participation) and clear explanations were provided on study risks, benefi ts, confi dentiality,
anonymity and conservation of data.
In all, 50 interviews were carried out. It is important to note that only trends and factors that had been
reported by a notable number of key informants and on-line survey respondents or that could be verifi ed
in the peer or grey literature are described in this report. Isolated impressions and opinions have not been
included. Although they may signal issues or trends worthy of further attention, additional validation was
deemed necessary to ensure that these are simply not a refl ection of individual issues or personal opinion.
Online survey of new Royal College certifi cants
In 2011 and 2012, the Royal College Employment Survey was forwarded to successful candidates of the
specialty and subspecialty Royal College certifi cation exams, which are held in the spring and fall respectively.
The short online survey was designed based on a branching technique, where skip patterns were utilized
to ensure that respondents answered questions relevant to them. Therefore, depending on the respondent,
questions ranged from fi ve to 18 questions. All questions are comprised of pre-categorized answers, along
with select questions that provide the option for write-ins.

Findings From The Royal College’s Employment Study - 2013
RES
EAR
CH
MET
HO
DO
LOG
Y
15
As highlighted above, the fi rst phase of key informant interviews with Royal College specialty committee
chairs assisted content development of the survey. These interviews provided intimate knowledge
of the employment situation of residents within Canadian specialty training programs, which helped
formulate survey questions that would gauge what new physicians’ plans are post certifi cation.
Employment-related questions were directed to 1) those seeking or have secured employment and 2) those
pursuing further training (subspecialty/fellowship). Other areas of inquiry included the following:
• Province of post-graduate training
• Career counseling provided during training
• Reasons for continuing training (e.g., no jobs available, passion for discipline etc.)
• Perceived reasons for why they may not have had a job placement (e.g., waiting to hear back,
no positions, unwilling to relocate, etc.)
• Type of job placement (e.g., full time, part-time, locum) and level of satisfaction.
Invitations to participate in the online survey were sent via e-mail to new certifi cants between 10-12 weeks
following the fi nal Royal College certifi cation examination. Over two years of examinations, this invitation
was sent to a total 4233 specialty and subspecialty certifi cants, of whom 1371 certifi cants (32.4%)
volunteered to participate in the survey. In 2012, a survey invitation was not forwarded to one certifi cant
because a valid email address was not available in the Royal College’s database at the time. Additionally,
there were 44 incomplete surveys over two years of the study that have been excluded from the analysis.
Under the guidance of the Ottawa Hospital Research Ethics Board, protecting participant confi dentiality
is considered tantamount. In keeping with standard ethical procedures the authors have ensured all study
information, including survey responses and transcripts of interviews, are kept in a securely locked location
onsite at the Royal College. Access to the electronic survey data and key informant interview transcripts
is password protected and only accessible by the authors at the Royal College. Following publication, all
hard copy data will be securely kept for fi ve years, after which time they will be destroyed. Electronic data
collected from the online survey will be maintained indefi nitely and used for both comparative and time
trend analysis.

Findings From The Royal College’s Employment Study - 2013
Findings 4.0
This report primarily seeks to identify high level, national factors around the state of
employment among new specialty physicians in the country and what lies behind their inability
to find work. It is understood from the outset that the findings from the first phase of our
research only scratches the surface of this complex topic. Our key informants and survey results
however are beginning to paint a clearer picture to fuel further research and discussions.
FIn
dIn
gs
16
4.1. The current landscapeHow many are securing employment after medical specialty certification?
Key findings
The survey data reveals that
employment issues are not isolated
to a few individuals in a few
specialties. Out of the 1325 new
certificants from 2011 and 2012
(31% of the cohort), 208 (16%)
reported being unable to secure
employment, compared to 7.1% of
all Canadians as of August 2013.
New graduates reported they are combining
multiple locum positions rather than longer-
term types of employment. Based on currently
available data on the topic, it is not possible to
determine if this is a result of the job market
or individual job preference. More research will
be needed to get a clearer picture. That said,
four out of ten respondents stated they were
not satisfied with their locum placement. This
finding is important given that job satisfaction
can affect retention as well as physician
wellbeing and performance.
The survey did reveal that a substantial
proportion of new physicians experiencing
employment issues were from surgical and
resource-intensive disciplines.
Employment challenges appeared
to increase over 2011 and 2012.
Those who reported having
employment issues increased by
4% points (from 13% to 17%) for
specialists from 2011 to 2012 and
by 6% points for subspecialists
(from 15% to 21%).
There may be indications of provincial variances
which merit further investigation.

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
17
It has been long established that new medical specialty certifi cants who chose not to pursue additional
training had a secure job prospect pending successful completion of their specialty certifi cation requirements,
including the certifi cation exams. So, once certifi ed, new medical and surgical specialists could seamlessly
move from being residents to independent consultants if that was their chosen career path.
Early signs that the notion of secured employment prospects was crumbling became evident with disconcerting
developments in orthopedic and cardiac surgery. A survey of orthopedic surgeons who graduated from
2006 to 2011 conducted by the Canadian Orthopedic Residents’ Association showed grim prospects for
orthopedic surgeons trying to enter practice. The survey revealed that 56% of the 176 Canadian respondents
had secured employment, 35% were completing a fellowship or graduate degree and 9% had not found
a job. Of those who had not been
able to secure a position, 69% were
taking on-call shifts and 31% had no
work at all. Slightly fewer than half
of the new orthopedic specialists had
full-time work (Taggart 2012). A study
of cardiac surgeons who graduated
between 2002 and 2008 also revealed
employment diffi culties with 98% of the
estimated 62 recent graduates stating
that fi nding employment for a new
graduate in cardiac surgery was diffi cult
or extremely diffi cult. The study also
revealed that 27% reported they had
extended their training because of a lack
of jobs and 34% considered themselves
underemployed (Ouzounian et al 2010).
To get a more comprehensive picture of
this new trend and its effects on other
disciplines, an on-line survey was sent
to new Royal College certifi cants who
were successful at the specialty and
subspecialty Royal College exams during
2011 and 2012. Overall response rates
are summarized in Table 1 and at the
provincial level in Table 2.
TABLE 1 Royal College Employment Survey
2011 and 2012 combined
Population and sample data, by response rates, age and gender
Population NResponses n
(Rate = n/N%)
Specialists 33631116
(33.2%)
Subspecialists 870255
(29.3%)
Total 42331371
(32.4%)
Population (N) and Sample (n) Characteristics
Population N Sample n
SpecialistsAGE<35
35-3940-4445+
Missing
GENDERMale
FemaleMissing
2448 (72.8%)554 (16.5%)205 (6.1%)120 (3.6%)36 (1.0%)
1712 (51.0%)1650 (49.07%)
1 (0.03%)
781 (70.0%)165 (14.8%)64 (5.7%)39 (3.5%)67(6.0%)
530 (47.5%)526 (47.1%)60 (5.4%)
SubspecialistsAGE<35
35-3940-4445+
Missing
GENDERMale
FemaleMissing
628 (72.2%)170 (19.5%)53 (6.1%)15 (1.7%)4 (0.5%)
430 (49.4%)440 (50.6%)
0 (0.0%)
186 (72.9%)42 (16.5%)16 (6.3%)6 (2.4%)5 (2.0%)
132 (51.7%)118 (46.3%)
5 (2.0%)

Findings From The Royal College’s Employment Study - 2013
TABLE 2 Royal College Employment Survey, 2011 and 2012
Response rates, by province of postgraduate training*
Province ofPost Grad Training
AB BC MB NL NS ON QC SK
Specialists2011/2012
Cohort
Responses 140 129 53 25 47 393 260 20
Population 392 286 145 63 132 1196 851 56
Response Rate 35.7% 45.1% 36.6% 39.7% 35.6% 32.9% 30.6% 35.7%
Subspecialists2011/2012
Cohort
Responses 38 32 11 3 11 94 55 1
Population 120 90 27 ** 29 365 192 5
Response Rate 31.7% 35.6% 40.7% – 37.9% 25.8% 28.6% 20%
ALL2011/2012
Cohort
Responses 178 161 64 28 58 487 315 21
Population 512 376 172 ** 161 1561 1043 61
Response Rate 34.7% 42.8% 37.2% – 36.0% 31.2% 30.2% 34.4%
* Province of educational institution that certifi cants reported where their residency training was completed ** Population data missing for subspecialties
FIN
DIN
GS
18
As outlined in Figure 2, two years of survey data reveal that employment issues are not isolated to a few individuals in a few specialties. From 2011 and 2012, 208 new certifi cants or 16% of respondents reported being unable to secure employment at the time they completed the survey from among the 1325 new certifi cants who provided responses, compared to 7.1% of all Canadians as of August 2013 (Statistics Canada
2013). Of the 208 respondents who reported not fi nding a job placement, 122 new physicians stated they will pursue further training whereas 86 reported that they were unemployed and without a training post.
Experts from the Canadian Institute of Health Information noted that these fi ndings are certainly not an over-estimate and likely an under-estimate among the cohort of new certifi cants who received the survey since
non-responders may also be experiencing employment challenges (Personal communication, January 15, 2013).
656(49%)
208(16%)
86(41%)
122(59%)
410(31%)
51(4%)
Responses: n=1325 (out of N=4233)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
n: number of responses N: total number of new certificants
Source: Royal College Job Placement Survey 2011, 2012.
FIGURE 2 Royal College Employment Survey, 2011 and 2012
Employment status reported by new specialists and subspecialists, Canada

Findings From The Royal College’s Employment Study - 2013
the perspective that some individuals were continuing
training without attempting to enter the job market,
although eligible to do so, given their perception of lack
of employment opportunities. Additionally, 51 (4%)
respondents stated they had not applied for a position at the
time of the survey for varying reasons including needing time
to rest after the rigours of training and certifi cation process.
Given the focus of our study, the remainder of this
section will focus on the cohort of new specialists and
subspecialists who were unable to fi nd a job placement
(208 in total) and those able to secure employment (410
respondents in total).
Two year trends
While further iterations of the survey will certainly
strengthen longitudinal analysis, it is noteworthy that
fi ndings by year shows that employment challenges
appeared to increase in 2012 over 2011.
As illustrated in the Figures 3 and 4, there were, overall,
more new specialists and subspecialists in 2012 compared
to 2011 who reported they did not have a job, up 4%
points for specialists (from 13% to 17%) and 6% points
for subspecialists (from 15% to 21%). Furthermore:
FIN
DIN
GS
19
Not everyone was in the active job market at the time of the surveys in 2011 and 2012. Of the 1325 new
specialty physicians who participated in the survey, 656 (49%) stated they planned to continue training post-
certifi cation. Of these 656, 414 indicated that they believed that pursuing further subspecialty or fellowship
training would make them more employable. As such, they had not intended to enter the job market,
favoring additional training instead. That said, additional write-ins by respondents and key informants added
Two years of the Royal College’s Employment Survey fi ndings disconcertingly reveal that over 200 new certifi cants, who spent at least eight years training to be medical specialists with the full desire to practice in their specialty, were not able to follow their planned professional aspirations.
• There was a notable increase among new specialists who reported continuing training because they
could not fi nd a job, with 39 in 2011, rising to 64 in 2012.
• In contrast, the number of subspecialists unable to fi nd a job stating they were continuing training
remained relatively unchanged between 2011 and 2012 (9 and 10 respectively), but there were
many more stating they had no job placement and at the end point of their training, rising from
10 in 2011 to 16 in 2012. It is not possible to determine from available data if this is owing to a lack
of fellowship and other subspecialization training opportunities or because respondents chose not to
pursue further training.
These fi ndings will warrant special, ongoing monitoring to better determine if these are developing trends
or more isolated phenomena.
Employment challenges have appeared to increase since the survey was released in 2011. It is too early, however, to determine from only two years of data collection if employment challenges will continue to worsen over time.

Findings From The Royal College’s Employment Study - 2013
Fin
din
gs
20
Provincial trends
Given the fact that employment challenges of specialists and subspecialists is a relatively new phenomenon
in many jurisdictions, and specialties and subspecialties, our survey also collected provincial level data from
new certificants on what their intentions are in regards to employment, ongoing education and their job
search status.
However, readers need to be conscious of the data limitations in both iterations of the survey. For instance:
• The data below reports provincial counts based on the location of the educational institution where
certificants reported they had completed their postgraduate (residency) training. It should not be
assumed that certificants are seeking employment in the same province.
• There were significant differences in the response rate of certificants based on their province of
postgraduate training (Table 2).
• Due to the smaller response sample, it is not possible to determine what kind of statistical bias exists
in these results since “participants and non-participants are systematically different, … validity may
be compromised” (Wison, Orme & Combs-Orme 2004, page 19).
• Canada’s 17 medical schools are situated in eight provinces, but provide the supply of physicians for
all 10 provinces and three territories in the country.
Responses: 495 Responses: 581
Responses: 125
2011 2012
2011 2012
Responses: 124
279(57%)
296(51%)
43(35%)7
(6%)
19(15%)
6(5%)
26(21%)
18(3%)
20(4%)
66(13%)
97(17%)39
(59%)
27(41%)
33(34%)
64(66%)
10(38%)
16(62%)
10(53%)
9(47%)
49(39%)
61(48%)
38(30%)
130(26%)
170(29%)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
Responses: 495 Responses: 581
Responses: 125
2011 2012
2011 2012
Responses: 124
279(57%)
296(51%)
43(35%)7
(6%)
19(15%)
6(5%)
26(21%)
18(3%)
20(4%)
66(13%)
97(17%)39
(59%)
27(41%)
33(34%)
64(66%)
10(38%)
16(62%)
10(53%)
9(47%)
49(39%)
61(48%)
38(30%)
130(26%)
170(29%)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
FIGURE 3
Royal College Employment survey, 2011 and 2012
Employment status reported by new specialists, 2011 and 2012 comparison, Canada
FIGURE 4 Royal College Employment survey, 2011 and 2012
Employment status reported by new subspecialists, 2011 and 2012 comparison, Canada

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
21
These fi ndings must not only be reviewed with the limitations outlined above but also recognize that other
factors, such as personal preferences described further in this report, may also be in play. For instance,
there were no respondents from Saskatchewan, and Newfoundland and Labrador reporting employment
challenges compared to Alberta where 23.2% stated they had experienced problems.
Therefore, the data below should not be read as a precise refl ection of the job market in each province,
but instead as an indication of the status of the respondents when they participated in the study; although
self-reported, some variations may merit further regional-level investigation. Not only must we develop
better data, we must also gain a better understanding of the conditions and measures instituted at
the jurisdictional level that may enable or hinder employment so that we can better interpret variations
observed between provinces.
3(1.7%)
Response rate: 35% (177 of 512)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
17(41.5%)
24(58.5%)72
(40.7%)
61(34.5%)
41(23.2%)
Source: Royal College Employment Survey 2011, 2012.
Royal College Employment Survey, 2011 and 2012Employment status reported by new specialists and subspecialists, by province of residency training, Alberta
FIGURE 5
13(8.2%)
Response rate: 42% (158 of 376)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
12(46.2%)
14(53.8%)73
(46.2%)
46(29.1%)
26(16.5%)
Source: Royal College Employment Survey 2011, 2012.
Royal College Employment Survey, 2011 and 2012Employment status reported by new specialists and subspecialists, by province of residency training, British Columbia
FIGURE 6

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
22
Response rate: 37% (63 of 172)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
4(40%)
6(60%)34
(54%)
19(30.2%)
10(15.8%)
Source: Royal College Employment Survey 2011, 2012.
Royal College Employment Survey, 2011 and 2012Employment status reported by new specialists and subspecialists, by province of residency training, Manitoba
FIGURE 7
2(3.5%)
Response rate: 35% (57 of 161)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
3(30%)
7(70%)28
(49.1%)
17(29.8%)
10(17.6%)
Source: Royal College Employment Survey 2011, 2012.
Royal College Employment Survey, 2011 and 2012Employment status reported by new specialists and subspecialists, by province of residency training, Nova Scotia
FIGURE 9
Response rate: 40% (25 of 63)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
15(60%)
10(40%)
* Subspecialty population missing
Source: Royal College Employment Survey 2011, 2012.
Royal College Employment Survey, 2011 and 2012Employment status reported by new specialists and subspecialists, by province of residency training, Newfoundland & Labrador (Specialists only*)
FIGURE 8
Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
23
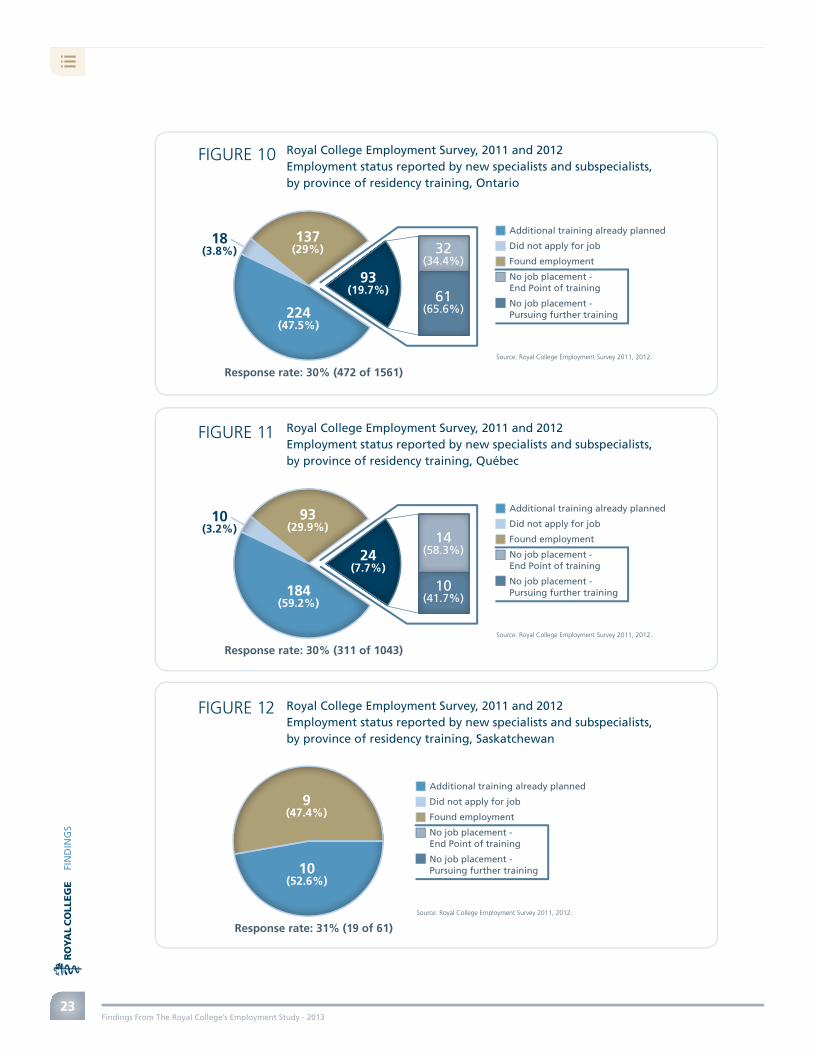
18(3.8%)
Response rate: 30% (472 of 1561)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
32(34.4%)
61(65.6%)224
(47.5%)
137(29%)
93(19.7%)
Source: Royal College Employment Survey 2011, 2012.
Royal College Employment Survey, 2011 and 2012Employment status reported by new specialists and subspecialists, by province of residency training, Ontario
FIGURE 10
10(3.2%)
Response rate: 30% (311 of 1043)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training
14(58.3%)
10(41.7%)184
(59.2%)
93(29.9%)
24(7.7%)
Source: Royal College Employment Survey 2011, 2012.
Royal College Employment Survey, 2011 and 2012Employment status reported by new specialists and subspecialists, by province of residency training, Québec
FIGURE 11
Response rate: 31% (19 of 61)
Additional training already planned
Did not apply for job
Found employment
No job placement - End Point of training
No job placement - Pursuing further training10
(52.6%)
9(47.4%)
Source: Royal College Employment Survey 2011, 2012.
Royal College Employment Survey, 2011 and 2012Employment status reported by new specialists and subspecialists, by province of residency training, Saskatchewan
FIGURE 12

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
24
Reliance on locum and part-time work
Over two years of the survey, 410 (30.9%) out of 1325 specialists and subspecialists who responded to
the surveys indicated that they have, or will soon have, a job placement.
Breaking down the data further, 225 (75.0%) of specialists and 91 (82.7%) of subspecialists indicated
they had secured full time employment. Conversely during the same period, 70 new specialists (23.3%)
and 18 new subspecialists (16.4%) revealed they were working on a locum (assuming another physician’s
duties temporarily) or part-time basis (refer to Figure 13).
SUBSPECIALISTSSPECIALISTS
Royal College Employment Survey, 2011 and 2012
New specialists/subspecialists with a job, by type of placement, CanadaFIGURE 13
The dependency on locum work and part time work has
been recently highlighted in the media as well, where
Priest (2011) noted many orthopedic surgeons are working
primarily as “locums” as they cannot gain permanent
fulltime work.
The survey’s fi ndings may be pertinent in a number of
ways. For instance, it may be an indicator of:
88 out of 410 (21.5%) specialists
and subspecialists with a job
placement in 2011 and 2012
indicated they were or will be
working on a locum or part-
time basis.
• Type of job placements reported by respondents, by province: As explained in the section titled
“Provincial Trends,” signifi cant variances in the response rate of certifi cants based on their province of
postgraduate training (Table 2) limits the Employment Survey’s validity as statistical indicator of provincial
job markets. It also remains to be determined if a physician’s province of postgraduate training is an
indicator of future retention given the paucity of pan-Canadian information in this regard.
Full time, 91,
82.7%
Part time, 28, 9.3%
NR, 5, 1.7%NR, 1, 0.9%
Locum, 6, 5.5%
Source: Royal CollegeEmployment Surveys 2011 and 2012.
Part time 12,10.9%
Locum 42, 14.0%
Full time, 225,
75.0%

Findings From The Royal College’s Employment Study - 2013
Fin
din
gs
25
These issues notwithstanding, as Figure 14 shows, new specialists who reported they had a job
placement did record interesting provincial variations that likely merit further examination. Just under
half of new specialists who completed their postgraduate training in British Columbia and half of
those in Manitoba indicated their job placement would consist of locum or part time work – higher
proportions than those reported by specialist certificants graduating from other parts of the country.
Full time
Part time
Locum
100%
80%
70%
60%
50%
40%
30%20%
10%
0%Alta. B.C. Man. N.L. N.S. On. Que. Sask. Total
90%
Source: Royal College Employment Survey, 2011 and 2012.Subspecialist data excluded given the limited number of responses to this survey question.
32
10
2
16
4
11
7
5
2
9
1
8
1
2
68
11
13
70
7 225
28
4223
3
Royal College Employment survey, 2011 and 2012
new specialists with a job, by type of placement, by province of residency training
FIgure 14
• Personal preference of physicians: Our research has collected differing perspectives from new
physicians on whether locum work is a reflection of their perception of jobs that are currently available,
or a matter of personal preference.
For some, locum work has been pursued out of pressure. For instance,
- a new certificant in pediatrics stated: “[I am] hoping for a full time permanent position.
But there are no local clinics hiring full time.” (royal College employment Survey 2012)
- a new anesthesiologist stated “I’m forced to travel the province for short term locums with no
guarantee for the coming month and regularity provided the assignments no one else wants both in
terms lower pay and lower clinical interests [and] complexity.” (royal College employment Survey 2012)
Conversely, some certificants favored locum work. For instance:
- a certificant in obstetrics and gynecology stated: “My husband is a ... resident, and there aren’t any
jobs in the area. I’ve got locum positions lined up and we plan to look for permanent jobs together
when he is finished.” (royal College employment Survey 2012)

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
26
Yes, 26(62%)
No, 16(38%)
Source: Royal College Employment Survey, 2011 and 2012.
- a plastic surgeon observed that the “locum position [is] a transition phase over the summer months.” (Royal College Employment Survey 2011)
- an anesthesiologist pointed out plans to “locum for a few months and try to decide which province I want to practice in, Ontario or BC.” (Royal College Employment Survey 2012)
While our research does not provide a clear indication as to whether or not locum positions are the ultimate
career choice or simply any available position, four of ten respondents stated they were not satisfi ed with
their current locum placement (see Figure 15 below). Lack of job satisfaction can have wide-sweeping
effects beyond retaining workers; it can also impact performance and wellbeing, among other elements
(Judge & Bono 2001).
Concrete data would assist provincial workforce
planners further and additionally, this knowledge
would help inform career seekers on the types of
placements currently available.
Despite limited data, our fi ndings to date are beginning
to paint an early picture of how successful new
specialists and subspecialists have been at securing a
job. The bottom line remains, however, that there is
great uncertainty among Canada’s future doctors about
their job prospects.
The realities of the job market and the evolving
nature of physician work preferences are two of
many different factors that may correlate with the
employment study’s data on new certifi cants attaining
locum positions.
The lack of comprehensive information and reporting
about part-time and locum work carried out in
Canada has been found to muddle the country’s
medical workforce data. This limitation provoked a
public reaction in January 2013 by Prince Edward
Island’s Health Minister who took issue with full-time
equivalency data published by CIHI given their omission
of locums who are an integral part of the contingent
of front line physicians in the province (Wright 2013).
Although new graduates reported
they are taking on locum positions,
at times as an alternative to
unemployment, 38% of respondents
stated they were not satisfi ed with
their placement. This can impact
physician performance and well-
being among other factors.
FIGURE 15 Royal College Employment Survey,
2011 and 2012
“Is your locum placement satisfactory to you at this time?”, percent response of specialists and subspecialists, Canada

Findings From The Royal College’s Employment Study - 2013
FIn
dIn
gs
27
4.2. Key drivers and influencers
Depicted here is the list of key drivers and influencers behind the employment challenges of new medical
specialists. They are grouped under three broad themes including some of the effects resulting from these
drivers. The following sections will examine each of these in more detail.
• Hospital funding• Stock market
• Career counseling• Personal factors/preferences
• Morphed practice• Underemployment• Brain drain
• Interprofessional practice
• Workforce planning
• Culture of practice
Employmentproblemmain drivers
Effect
Personal context
System
Economy

Findings From The Royal College’s Employment Study - 201328
4.2.1. Economy: Why is the state of the economy the main factor driving new medical and surgical specialist under/unemployment in Canada?
• Hospital funding- Reduced resources = more physicians competing
for fewer resources (e.g., OR time, staff, beds)- Reduced hiring
• Stock market- Delayed retirements or semi-retirements
EconomyEmploymentproblemmain drivers
There was widespread consensus among key informants that economic constraint was chief among
the many drivers behind under-employment and unemployment of new medical and surgical specialists
in Canada. This view was also echoed in the work done by the Future of Medical Education in Canada
– Postgraduate Project: “The long-term nature of physician planning cycles creates vulnerabilities for
governments and medical schools, such as sudden changes in the economy or in technology” (Glover
Takahashi et al. 2011, page 26).
Key finding
Since delivery of much of specialty medical care is dependent on institutional health care facilities,
including hospitals with their associated resources such as operating rooms and hospitals beds,
availability of and access to these resources directly impacts physician employment.

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
29
Hospital funding
Since much of the work of medical and surgical specialists occurs in hospital settings, which make up the
largest component of all health care spending, it follows that changes in hospital resourcing levels and
demand for services will impact the medical workforce. In 2012, hospital expenditures accounted for 29.2%
of total health care spending in Canada, including both public and private spending. The Canadian Institute
for Health Information (CIHI) forecasts that public sector spending on hospitals will see the lowest rates of
growth since the late 1990s, increasing by 4% and 2.9% in 2011 and 2012 respectively (CIHI, 2012a).
Slowed hospital budget growth is not surprising. A 2001 parliamentary committee report observes that “…without a new vision of what the future health care system should be, there is a risk that new money will be reinvested only in traditional, publicly funded, sectors of health care (e.g. hospitals and institutional
care)” (Parliament of Canada, 2001, p. 96).
Am
ou
nt
in b
illio
ns
$54.66 billion$79.9 billion
$30.3 billion
$144.6 billion200.0
150.0
100.0
50.0
0.02002 2003 2004 2005 2006 2007 2008 2009 2010
All public sector healthHospital expenditure
2011f/p
2012f/p
Source: CIHI, 2012a.
Public sector health expenditure growth, Canada, 2002-2012FIGURE 16
Key fi ndings s
Given decreased hospital funding growth in recent years and continuously increasing patient
health care needs, OR time and other hospital resources are constrained to control costs. As
such, there are more physicians competing for fewer resources, contributing to physician under-
employment and unemployment.
Given budgetary pressures, health care facilities are often reducing or slowing the number
of recruits they bring on board to control costs and, in so doing, reducing employment
opportunities for new graduates.
Longer-term economic forecasts and policies are not routinely taken into account by those who
determine intake into residency programs. This is particularly important since:
- access to many resources, which are required to practice and impact employment prospects,
are susceptible to changes with ever-shifting fi nancial allocations and economic policies
- it takes at least eight years from the time a trainee starts medical school before achieving
medical specialty certifi cation.

Findings From The Royal College’s Employment Study - 2013
Fin
din
gs
30
That needed vision is still evolving while Canada’s population continues to grow and physicians report
increasing complexity of their patients’ needs (National Physician Survey 2010, question 23). The 2008 global
economic crisis has also prompted some rethinking about government spending overall (Fowlie, 2013).
Commenting on the impact of the lack of available health care resources, key informants explained that
new graduates struggled to find employment across Canada despite ongoing and growing patient need.
Key informants also reported two factors associated with hospital budgetary constraints driving both
unemployment and under-employment:
• Fewer positions being advertised and filled.
• Reduced access to needed resources such as beds, operating room (OR) time and associated
hospital personnel.
Physicians are “primarily responsible for determining the number of patients who require care in hospital and
further diagnostic tests” (CIHI 2011, page vii). According to the most recent CIHI data, the volume of physician
services continues to increase. For example, surgical services and diagnostic/therapeutic services by surgeons
increased by 26.8 and 28.4% respectively between 1998-1999 and 2008-2009 (CIHI 2012b, Figure 18). Yet, key
informant interviews and survey findings reveal that the surgical and more resource intensive specialties and
subspecialties, which are highly dependent on OR and other hospital resources for their clinical practice, were
those where there are the greatest employment challenges, as shown in Table 3 below.
Royal College Employment survey, 2011 and 2012
disciplines reporting the most employment difficulties
TABLE 3
Discipline Unable to find a job placement Number (and %) of new certificants
who responded to the survey
Critical Care 5/22 (22.7%) 23/84 (27.4%)
gastroenterology 9/27 (33.3%) 27/92 (29.4%)
general surgery 13/46 (28.3%) 50/197 (25.4%)
Hematology 7/24 (29.2%) 25/68 (36.8%)
Medical Microbiology 3/13 (23.1%) 14/29 (48%)
neurosurgery 8/21 (38.1%) 22/50 (44%)
nuclear Medicine 4/7 (57.1%) 7/21 (33.3%)
Ophthalmology 13/30 (43.3%) 30/84 (35.7%)
Orthopedic surgery 15/60 (25%) 61/168 (36.3%)
Otolaryngology 5/17 (29.4%) 17/55 (30.9%)
Radiation Oncology 14/27 (51.9%) 29/60 (48.3%)
Urology 6/15 (40%) 16/61 (26.2%)
** Cardiac surgery 5/5 (100%) 5/16 (31.2%)
* includes those who stated they had not secured a position when they responded to the survey and were either continuing training or were not in a training program.
** cardiac surgeons who responded to the 2011 and 2012 surveys reported that they had not tried to apply for a position and were continuing training because they believe it will make them more employable.

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
31
Key informants commented that,
because of the high cost of running
operating rooms, one of the fi rst areas
that Canadian hospitals will “cut”
when experiencing budget constraints
is available OR time.
Within the lay press, it has been
suggested that funding restrictions
in Alberta have had many effects on
hospitals, including: limiting amount of
overtime worked by nurses and access
to certain services, and closure of
For, … fi ve or six cardiac surgeons, you’d
require a ten-bed intensive care, three operating
rooms, about 40 in-hospital fl oor beds … So last
year, we had 20% to 25% of our cases cancelled
due to a lack of beds. … the biggest cost to the
system is when I operate …. The fi rst couple
days of that patient’s stay are hugely expensive.
So if … [hospitals] can get us to do less work,
they save money.” [KII-29]
“
operating rooms and hospital beds (CBCnews 2013). It was also reported that ORs were closed or decreased in
order to stay within hospital operating budgets, which resulted in delaying or reducing surgeries and having
a direct effect on specialist services (CBCnews). Between January and March 2013, one hospital closed 20 OR
days to accommodate budget constraints and another was reported as having cancelled eight surgeries at
the end of January 2013 because of lack of access to the OR (CBCnews).
Recent reports in Ontario also note frozen funding, impending cuts and lower annual increases to hospital
operating budgets, impacting specialty medicine (Boyle 2013). To avoid defi cits, hospitals are considering or
implementing measures similar to those implemented in Alberta, such as: closing operating rooms, hospital
wings and outpatient clinics (Boyle). Other jurisdictions such as New Brunswick are also implementing
measures to contain health expenditures. In this jurisdiction, however, plans are to seek fi ndings by cuts to
non-clinical staff and services (Government of New Brunswick 2013). Despite these reassurances, there remains
some disagreement and uncertainty that cuts will not impact care or the public (Bisset 2013; New Brunswick
Medical Society 2013).
A key informant from the discipline of otolaryngology further explained how, in Canada, surgical specialties,
including otolaryngology are, in essence, viewed as a liability to the hospital because surgeons are “taking
money away” from the capital budget of the hospital when patients are brought in for surgeries.
“ It’s expensive to open up operating rooms … in the Unites States, people … are viewed as an
asset to the hospital because they bring in money and they bring in patients whose insurance
companies pay … whereas in Canada, a hospital views you as an expense because you’re bringing
in patients that are going to take money away from the capital budget of the hospital. … So we’re
not looked upon as “Oh great! You’re bringing in more patients!” It’s … like, “Oh, please, don’t bring
more.” [KII 32, emphasis added]
“
Another key informant noted that this growing dearth of health system resources left many new specialists
pursuing multiple fellowships since they could not fi nd employment.

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
32
Findings from the Royal College employment surveys clearly corroborate with these observations – over
two iterations of the survey, further subspecialisation due to a lack of employment was particularly
prevalent among new surgical certifi cants.
““… even though there’s a huge need for … [otolaryngologists], there … [are] really no resources
being offered to the point where our new graduates are struggling to get jobs and, as a result,
many of them are going off and doing fellowships in subspecialties instead of starting a practice,
hoping that that will give them a leg up or an ability to get a job after they’re fi nished … ” [KII-1] “
Royal College Employment Survey, 2011 and 2012
Number a of new certifi cants pursuing further training because they could not fi nd a position
Royal College Employment Survey, 2011 and 2012
Most important reason why respondents stated they could not fi nd a job
TABLE 4
TABLE 5
2011 2012
Surgical disciplines23/85
(27.1%)34/107
(31.78%)
Specialists and subspecialists overall
48/365 (13.2%)
74/413 (17%)
Source: Royal College Employment Survey, 2011 and 2012.
Too few available positions for my specialty in Canada
Not enough funding for my position
2011 2012 2011 2012
No job and at end of training
Specialists 22.7% 42.4% Specialists 25.9% 24.2%
Subspecialists 40% 56.2% Subspecialists 30% 12.5%
No job and continuing
training
Specialists 29.7% 69.4% Specialists 18.8% 12.9%
Subspecialists 11.1% 30% Subspecialists 44.4% 50%
Source: Royal College Employment Survey, 2011 and 2012.
New graduates also perceived that economic constraint was impacting the job market. In both the 2011
and 2012 employment surveys, respondents identifi ed “too few available positions for my specialty in
Canada” and “not enough funding for my position” among the most important reasons why they did not
have a job. Both new graduates continuing training and those who were at the endpoint of training held
this view (see Table 5 below).

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
33
• Survey fi ndings reveal that all new physicians and surgeons who had not found a job, whether
they were continuing training or not, increasingly believe that there are too few available positions
for their specialty in Canada.
• The feeling that there was not enough funding for their position varied in terms of relative
importance among new physicians and surgeons without a job, ranging from 18.9% to 44% in
2011, and 12.9% to 50% in 2012.
Stock market performance – delayed retirements
Most physicians in Canada are generally viewed as “self-employed entrepreneurs” (Canadian Foundation for
Health Improvement 2010). As such, they are usually responsible for planning and providing for their retirement
and, much like many other Canadians, the stock market plays prominently in retirement fi nancial plans.
The stock market crashes of 2001 (Mishkin & White 2002) and 2008 (Barro & Ursúa 2009) certainly left their mark
on the wealth of Canadians.
Key informants explained that the decline in investment portfolios affected physicians’ retirement patterns
and by default, not freeing up anticipated openings for new specialty graduates in Canada. Delayed
retirements owing to poor performance of physicians’ investment portfolios is not a new phenomenon.
A 2009 article in the publication “Benefi ts Canada”, for example, discussed the effects of the 2008 market
crash on retirement patterns, including how physicians were delaying their plans to exit the workforce
(Sylvain 2009). The article also refers to shifting work patterns toward semi-retirement compared to full
retirement to protect investment holdings until the market’s performance improves.
Anticipated retirement patterns were quite different not that long ago. In 2007, for example, there were
references of “raised ... anxiety level about mass physician retirement” that would further exacerbate
physician shortages (Pong, Lemire & Tepper 2007). These predictions have clearly not materialized. An analysis
of the 2007 and 2010 National Physician Survey results showed that although 6-7% of all physician
respondents stated they planned to retire from clinical practice within the next two years, that same analysis
observed that, despite methodological challenges and data limitations, it was possible to conclude that far
fewer had followed through on their stated intentions (Buske 2012).
Key fi nding
The stock market’s relatively weak performance in recent years has reduced many physicians’
retirement savings and delaying their retirement plans. Long-held positions are not freeing up as
expected and will not likely free up until markets improve.

Findings From The Royal College’s Employment Study - 2013
Much more work needs to be done to measure
the impact of physician retirement patterns on
the medical workforce, including newly certified
physicians and surgeons. This will not be an easy task.
To begin, there is “not a universally accepted officially
sanctioned definition of retirement in Canada”,
which for example can range from complete removal
from the labour market to reductions in income
or time worked (Pong 2011, page 5). In his detailed
study, Pong also notes that little is known about
physician retirements, adding that The World Health
Report 2006 recognizes that “information about
the retirement rate of health workers is very scarce”
(5). Thus, not only do we have scarce information
about the medical workforce in Canada, little can be
gleaned from international sources as well.
FIn
dIn
gs
34
Information about the
retirement rate of health workers
is very scarce” (WHO Report, 2006)
As such, it is very difficult to
systematically measure and assess
the impact of retirement patterns
on the medical job market. For
now, we must rely on verbal
reports of job opportunities that
have not opened up because of
delayed retirements prompted by
the economic downturn.
“
4.2.2. System: What elements in the health system contribute to the under-employment and unemployment of new medical and surgical specialists?
• Interprofessional practice- < reliance on physicians- < reliance on residents to cover service
• Workforce planning- Variable across Canada- Insensitive to workforce movement- Resident core to short-term service needs vs.
longer-term needs
• Culture of practice- Hospital resources (e.g., OR) not shared with new
specialists to protect own wait times and income
SystemEmploymentproblemmain drivers

Findings From The Royal College’s Employment Study - 2013
Key fi nding
Interprofessional collaborative practice is increasingly taking root in Canadian health care. With this
development come new health professional roles and responsibilities that directly impact reliance
on medical services and physician employment. Yet, there is little data and research on how these
changes in health care organization and delivery impact medical workforce requirements.
FIN
DIN
GS
35
Interprofessional care models
Delivery of modern health care is complex, labour intensive and increasingly relies on inter-professional,
collaborative teams. Health care managers and policy makers alike strive to develop and implement the
most effi cient and effective staff mixes, based on available local priorities and resources (Buchan & Dal
Modern health care is
increasingly complex and
delivered in teams, where roles
are constantly evolving, with
some substituting physicians’
services, others complementing
or doing both.
Poz 2002; Macdonald-Rencz & Bard 2010). There are many
drivers underlying the development of new roles and
interprofessional teams such as physician shortages,
rising chronic illness and economic constraints
(MacDonald-Rencz & Bard 2010). “New ways of delivering
care are required, and the expansion of interprofessional
teams” may help meet increased patient needs
(Ducharme, Adler, Pelletier, Murray & Tepper 2009, Discussion
section). As such, the role and types of various health
professionals is constantly evolving.
The changing roles of health professionals can either substitute and/or be complementary to those of
physicians and surgeons.
Advanced practice nurses, which encompass nurse practitioners (NPs) and clinical nurse specialists (CNSs),
have existed in Canada since about the early 1970s (DiCenso et al. 2010). A blended CNS/NP role that emerged
in the late 1980s was fi rst introduced in Ontario in tertiary-level neonatal intensive care units to help offset
cutbacks in pediatric residents (Hunsberger et al. 1992; Pringle 2007). Other categories of NPs were also soon
after introduced into other specialty areas within hospitals because of the perceived shortage of medical
residents and an observed lack of continuity of care for seriously ill patients (Pringle 2007; Kaasalainen et al. 2010).
Physician assistants (PA), which complement the work of physicians, have formally been a part of Canada’s
military health care system since 1984. They were fi rst legislated in the Canadian public system in Manitoba
in 1999 under the name ‘clinical assistant’ and subsequently renamed PA in 2009 (CAPA 2013a; Government
of Manitoba 2013). Since then, this new health profession has been integrated into many provinces including
Ontario, New Brunswick, Alberta and Nova Scotia (CAPA 2013a; CPSNS 2013).

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
36
Interprofessional models reducing reliance on physicians – slowing need for job growth
The new advanced practice nurses’ roles that have emerged, which substitute and complement the work of
physicians, address various types of health care needs such as (MacDonald-Rencz & Bard 2010; DiCenso et al. 2010;
Fulton & Baldwin 2004; Alcock 1996) :
• Nurse practitioners who, in addition to various primary care roles, are practicing in acute care
settings in hospitals or in specialized outpatient settings and assuming a wide range of roles such as
providing care for acutely, critically or chronically ill patients with complex conditions.
• Clinical nurse specialists, who also work in hospitals, are conducting research, providing leadership
and also promoting high standards of care and patient safety, have been associated with reductions
in hospital length of stay, readmissions, emergency room visits, costs as well as patient satisfaction
among other factors.
• Advanced practice nurses can also specialize their focus within a particular disease or medical
subspecialty and coordinate the care of high-need patients who often have complex co-morbidities,
alongside other medical specialists, in areas such as neonatology, nephrology, cardiology, psychiatry,
gerontology, palliative care and oncology.
Unlike other health professionals, the PA’s scope of practice not only depends on their own training, it
is also directly related to the tasks that the supervising physician chooses to delegate within their own
approved scope of practice (Mikhael, Ozon & Rhule 2007). Since PAs can undertake any number of clinical
activities delegated by their supervising physician, their scope of practice can be wide-ranging, such as
(McMaster University 2013; Alberta Health Services 2013; CAPA 2013b):
• Taking medical histories, conducting comprehensive physical assessments and interpreting fi ndings,
ordering and interpreting tests, and performing selected diagnostic and therapeutic interventions or
procedures including assisting in surgery.
• They are trained in many aspects of general clinical medicine in all systems, including:
cardiovascular, endocrine, musculoskeletal, pulmonary, gastrointestinal, eye, ear, nose, throat,
reproductive, neurological, psychiatry/behavioral science, genitourinary (GU), dermatology,
hematology, infectious disease.
• A PA’s scope of practice may also include patient education, research and administrative services.
Key fi nding
With the increasing prevalence of interprofessional care models comes a corresponding evolution
of health professional roles. These new roles complement and in some cases substitute physician
services, making it possible to increase the amount of specialty medical care that physicians and
surgeons provide without necessarily increasing the number of medical jobs.

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
37
The following examples are not intended to be a comprehensive review but rather to illustrate some of
studies and reports demonstrating the benefi ts of the changing roles of other health professionals in
interprofessional collaborative health care teams, which complement and substitute physicians:
• A 2010 study on the effect of PAs
working with orthopedic surgeons
in an arthroplasty (joint repair/
replacement) practice in Winnipeg
revealed that they were not only
considered as important members of
the health care team by surgeons,
nurses, orthopedic residents and
patients, they also helped reduce wait
times and increase the number of
surgeries orthopedic surgeons could
do (Bohm, Dunbar, Pitman, Rhule and Araneta 2010). PAs were found to save their supervising physician,
on average, 204 hours per year (2010). The number of primary joint procedures also increased by
42 per cent because orthopedic surgeons were able to implement a double operating room model
facilitated by PAs which reduced average wait times from 44 weeks to 30 weeks compared with the
preceding year (2010).
• In a 2009 study on the effects of PAs and NPs in six Ontario emergency departments, it was found
that they had a direct role in reducing wait times for patients, how long they stayed in the emergency
departments and the rate of patients who left without being seen (Ducharme, et al. 2009). This study
showed that PAs will help increase the output of emergency physicians without necessarily having
to increase the number of physicians, to help better meet patient health care needs.
• A study released in 2006 examined the use of PAs and anesthesia assistants (AA) in operating rooms
in Halifax to determine, among other objectives, the types of clinical activities that could be delegated
to PAs and AAs. The study also sought to determine the effect on physicians’ time, revealing that they
decreased reliance on physicians while increasing surgical output (Sigurdson 2006):
- Of the 806 patients seen in 13 clinics for rechecks, which accounted for 69.5% of patient
volume, it was concluded that 53.5% could have safely been addressed by a PA (pages 43-44).
- In the operating room, a detailed review of 979 events showed that PAs could reduce reliance
on surgeons’ time by carrying out activities that do not tap into the skill sets unique to surgeons
(e.g., preparing/draping patients, sewing and applying dressings). As such, it was concluded that
PAs could safely perform 48.8% of minor procedures, 28.6% of elective procedures and 20.5%
of waitlist procedures (pages 44-47).
- “Considering the weekly mix of activities, a PA could increase surgical productivity by 36.7%”
(page iv).
- It was also observed that addition of PAs could allow two operating rooms to run simultaneously
thereby greatly increasing surgical productivity (page 50).
There is a growing body of evidence
about the many benefi ts of the evolving
roles of other health professionals,
working in interprofessional teams,
including reducing reliance on physicians
to increase the amount of health care
provided to patients.

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
38
- AAs permitted “individual anesthetists to run two ophthalmology rooms simultaneously. Thus
far, the rooms involve low acuity cases under conscious sedation only. With further experience,
it may be possible to run two general anesthesia rooms under the supervision of a single
anesthetist” (page 36).
• NPs have long demonstrated benefi ts for patient outcomes, reduced length of stay in hospital and
optimal use of health professionals in interprofessional teams. A 1999 program introducing acute care
NPs to improve outcomes of hip fracture care in a tertiary teaching hospital in British Columbia clearly
shows how NPs contribute to interprofessional collaborative practice (Faith 2012). In this program, “the
NP collaborated with the hospital Clinical Path Consultant and the multidisciplinary team to plan and
develop a hip fracture clinical pathway. Through this collaboration an approach to hip fracture care
evolved which incorporated the NP as a key caregiver for hip fracture patients” (page 217). This study
concludes that care by NPs for hip facture patients:
- “is well suited to the needs of hip fracture patients since it originates from an expanded scope
of nursing practice that blends medical, behavioral and social science expertise into a systematic
process of patient care” (page 216).
- “is contingent on the NP forming collaborative practices with members of the multidisciplinary
team including a strong NP/physician collaborative that ensures the comprehensive care required
by hip fracture patients” (page 216).
Despite being viewed by some as a more progressive approach to a balanced health care system in Canada,
key informants did acknowledge new interprofessional care models and evolving scopes of practice of other
health professionals could have a deleterious effect on the availability of specialist positions.
One hospital leader commented about how other health professionals were “poised” to assume signifi cant
aspects of medical specialty scopes of practice. This particular hospital leader indicated that, in his
opinion, certain non-physician providers such as advanced practice nurses, physician assistants, respiratory
therapists, anesthesia assistants and physiotherapists were at “the brink” of assuming signifi cant portions
of specialty scopes of practice.
““… we have advanced practice nurses in virtually every specialty now who can run a clinic, who
can do a lot under the direction of a consultant. We have hospitalists, … physician assistants,
... and physiotherapists picking up what orthopedic surgeons used to do. … You can’t look at
a profession that hasn’t increased its credentials and increased its training and has spread out.
… Our hospital is paying for 16 anesthesia assistants. …and anesthesia specialists want more
[anesthesia assistants]. … So even if I just put one anesthesiologist with two anesthesia assistants,
I now need half as many anesthesiologists. That’s huge! ” [KII C58, emphasis added]
“

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
39
Interprofessional models reducing reliance on residents for service – potential to better align new physician supply with longer-term needs
Certain key informants believed that new
interprofessional collaborative models, many
of which have proven to be a more progressive
approach to health care in Canada, could reduce
the need for a growing number of medical
specialist positions. Others also observed that such
new models could have the potential to improve
the job situation for unemployed specialists in
the longer term by more appropriately matching
the available mix of health professions, including
physicians, to service needs within hospitals.
Since residents or “physicians in training have a dual role of a learner and clinical care provider” (National
Steering Committee on Resident Duty Hours 2013, page 10), they are an integral component of the team providing
care to patients in teaching sites. The challenge in most teaching facilities is to ensure that residents’
education is a proper balance between: “The act of professional and clinical interactions with patients, and
the provision of clinical care, including indirect care, … [and] the application of knowledge, collaboration,
and discovery leading to the development of skills and attitudes necessary for residents to become caring,
competent physicians capable of serving patients and the society in which they function” (page 25).
Key informants confi rmed that the integration of PAs, APNs and other health professionals into new
interprofessional practice models not only improved patient care, they also had a positive impact on the
residency education by reducing reliance of residents as service providers.
New roles and interprofessional teams are not only having a positive effect on patient care, access, and patient and physician satisfaction, they are also reducing reliance on residents for shorter-term service needs which will help balance physician supply with
patient needs for the longer term.
Key fi nding
Teaching programs that include a mix of health professionals, who complement or substitute
physicians, can be less reliant on residents to fi ll patient care requirements. This development is
promising on two fronts:
- residents can pursue higher-value learning in their areas of specialty because they do less
work that can be done by others
- residency positions are not simply created to generate more “boots on the ground” to
fi ll service needs. This may help mitigate the likelihood that new specialists will be under- or
unemployed when they graduate because the educational system is not producing more
specialists than needed.

Findings From The Royal College’s Employment Study - 201340
Neurosurgery, which is among the disciplines
experiencing the greatest employment challenges,
was a prime example of the encouraging development
of integrating other health professionals to reduce
reliance on residents. Key informants in two different
provincial jurisdictions described how neurosurgery,
for example, was integrating NPs and PAs to create
new inter-professional care models. These new models
were believed to have a potential positive counter-
effect on the increasing need for high numbers of
residents by creating a “buffer zone” that could
impact the saturated job market of new graduates.
One program director for neurosurgery explained
how PAs are drawn upon to assist neurosurgery
residents, which was signifi cantly changing and
modifying both the educational and clinical service
models of neurosurgery within that jurisdiction. It was
reported that PAs may perform similar duties as of
neurosurgery residents, such as patient care on the
ward and in intensive care units, or emergency room
calls and related consults during the night. Although
PAs were not directly fi lling the extensive role of a
neurosurgeon, it was thought that the subtle changes
that the addition of PAs were making to neurosurgical
practice could ultimately lead to the requirement for
less residents within the hospital to fi ll service needs
that might otherwise not be met.
Changing neurosurgical models of care were not only restricted to the inclusion of PAs within a single
provincial jurisdiction, but were also occurring elsewhere with NPs. This development was similarly thought to
be contributing to a new model of care where NPs decreased the reliance on residents that, in turn, enhances
both patient care and the resident learning experience.
One new neurosurgery graduate observed that, with the role of NPs and PAs within new interprofessional models:
So you decrease the number of residency positions—how do you sustain neurosurgery that up until now has been dependent on the residents who take calls in the hospital and to provide that buffer so that the attending neurosurgeon can work for 30 years in the fi eld and not get burned out and quit? And my answer to that is that I do see a new model emerging where the hospitals, instead of paying for residents, will probably have to pay for nurse practitioners or physicians’ assistants to take on the role of the resident in the hospital and to help close that gap. So then it’s a more transparent model where you’re actually hiring a person for what you want them to do, rather than putting it under the guise of education.” [KII 15, emphasis added]
“
““the nurse practitioners really take care of a lot of … the day-to-day. This did free up residents
to spend less time doing …the day-to-day work that had to be done that didn’t have as much
educational value perhaps but still needed to be done. They [residents] had to do much less of
that so they were really free to go to the operating room and focus on more specifi c neurosurgical
issues as opposed to looking after some of the general medical issues, You would actually end up
training fewer neurosurgeons which may allow you [residency programs] to match the number of
graduating neurosurgeons to the number of jobs available.” [KII NG, emphasis added]
“
FIN
DIN
GS

Findings From The Royal College’s Employment Study - 201341
Medical workforce planning
Supply and organization: How is workforce planning and organization affecting residency program intake and, ultimately, the number of new specialty graduates produced against the job market?
Canada’s postgraduate medical education (PGME) system “is an essential component of physician supply in
this country” (Glover Takahashi et al. 2011, page 25). Almost all interviewees consulted in the preparation of the
Governance Paper for the Future Medical Education in Canada – Postgraduate Project (FMEC-PG) stated that
“one area of concern was the number of stakeholder organizations involved in PGME” (Pardhan & Saad 2011, page
11), which “include regulatory authorities, governments, affi liated university programs, and certifi cation bodies”
(Glover Takahashiet al., page 29).
The FMEG-PG governance paper further observes that, in addition to there being a number of stakeholders,
each may have different responsibilities such as “… an individual postgraduate offi ce has a number of lines
of accountability which include: … [a]s most academic hospitals require residents to function, PG offi ces and
individual programs must ensure adequate staffi ng by housestaff to provide clinical service functions” (Pardhan
& Saad 2011, page 12). Finally, this paper observes that: “One of the larger challenges that faces PGME in Canada
is the current state of governance. The multiple organizations and stakeholders result in different agendas and
priorities with no clear overarching strategy or plan” (page 14). Canada, in effect, does not have one single health
care system. It is “a mosaic of 14 systems, comprised of the federal government, and the country’s ten provinces
and three territories” (Fréchette & Shrichand 2011, page 1).
Thus, the process to determine the number and type of residency positions allocated in Canadian medical
schools varies greatly across the country. It is also somewhat of a mystery given the lack of public transparency,
despite informal mechanisms that might be developing. In fact, in preparing a background paper on health
workforce planning approaches in Canada for the 2011 International Health Workforce Collaborative
Conference, the authors were required to conduct key informant interviews with various members of the
Committee on Health Workforce (previously named Advisory Committee on Health Delivery and Human Resources) given lack
of comprehensive information readily available in the public domain (Fréchette & Shrichand 2011, page 11).
FIN
DIN
GS
Key fi ndings s
Approaches for allocating residency positions generally vary greatly from one province and
medical school to the next. In most cases, there are many organizations and stakeholders involved
in determining the number of residency positions that will be allocated. Often, these decision-
makers have competing priorities. Also, their decisions are broadly based on scant readily available
information about longer-term societal health needs and health care resources.
Further, because decisions around the number of residency positions are generally based on
“local” needs, the fact that new medical graduates may not necessarily stay in the jurisdiction
where they trained further contributes to imbalances in the medical supply.

Findings From The Royal College’s Employment Study - 201342
Some jurisdictions such as “Alberta and
British Columbia have adopted shared/
network planning models between a unit with
responsibility for HRH planning and a wide
network of collaborators… other provinces,
such as New Brunswick and Ontario have
established predominantly centralized planning
models in a dedicated unit or division within
their respective ministries of health” (Fréchette &
Shrichand 2011, page 11). The units contributing
to health workforce planning within the various
ministries of health “vary in size, from a handful
of persons to more than 70 and have been in
existence for varying periods of time, from a
few years to decades” (page 11).
The variability of methods becomes more
obvious by briefl y reviewing a few jurisdictions.
• Québec’s Ministry of Health and Social Services plays a greater role in determining the number
of training positions available in each specialty. The province has established a plan that sets out
targets for the types of doctors and specialists needed in that province, and follows regional
physicians resource plans knows as “PREMS” and physician resource plans commonly referred to
as “PEMs” (Fédération des médecins résidents du Québec 2013). These health workforce plans are reviewed
each year in light of discrepancies observed between available resources and hospital and regional
health system needs. The Quebec model also takes into account attrition of practicing physicians
and anticipated numbers of new doctors (2013).
• In the neighboring province of Ontario, the Ministry of Health and Long-Term Care provides funds
for an overall number of training positions, but it plays a much smaller role in determining specifi cally
how these positions are allocated among the various specialties and training programs. These are
determined in consultation with the medical schools and their Council of Faculties of Medicine of
Ontario with further insights gleaned from various sources notably the province’s “Population Needs-
Based Physician Model “ (Born & Dhalla 2012; Fréchette & Shrichand 2011).
• British Columbia’s health workforce planning is based on a complex network. While the province has
also developed its own modeling/forecasting tool, it is held in the ministry’s Health System Strategic
Planning Division, separate from the Health Human Resources Planning branch. Planning involves a
number of areas within the ministry and various committees. Based on the last information collected
in 2011, this network includes: the Strategic Policy, Information Management and Data Stewardship
area which provides data, the HHR Strategy Council which is comprised of vice-presidents of the
province’s health authorities, and the BC Academic Health Council which is the intersection of health
delivery and education. The network also includes the Medical Health Human Resources Planning
Task Force comprised of vice-presidents of medicine of the health authorities, academic leads, and
representatives from the public, the Ministry of Health and the Ministry of Education. The Task Force
The manner in which residency
positions are allocated across the
country varies greatly. Notwithstanding
the need to balance immediate service
requirements which residents often
fulfi ll, some attention is paid to longer-
term societal health care need. That
said, attempts to factor health care
needs tend to focus on more local
or jurisdictional requirements. These
approaches are insensitive to the fact
that residents do not always stay in
the area where they trained. This is
increasingly the case as the physician
job market becomes more diffi cult.
FIN
DIN
GS

Findings From The Royal College’s Employment Study - 201343
informs the allocation of residency positions by maintaining a current understanding of population
health needs. The recommendations from the network within the Ministry of Health are discussed
between the ministries of health and advanced education to match the desired slate of positions
with available educational capacity. The ultimate decisions on the number of training positions to be
funded rest with the Ministry of Advanced Education, the fund holding agency for health professions’
education (Fréchette and Shrichand 2011, pages 11-12).
These approaches are generally insensitive to the fact that residents do not always stay in the area where they
trained. This may increasingly be the case as the physician job market becomes more diffi cult. This factor will
need to be further investigated to determine how important it will be in the future.
Increased reliance on residents: Despite the promise of interprofessional care models, is the practice in many programs to increase reliance on residents for service leading to potential overproduction compared to the number of available jobs?
FIN
DIN
GS
Key fi nding
The promise of reduced reliance on residents for service with the introduction of interprofessional
models has not been realized in all residency programs. As such, many clinical departments are
still very reliant on residents to cover required services. Thus, the number of new specialists and
subspecialists produced from Canada’s faculties of medicine may exceed the number needed in
the future and available positions.
There are many reasons why medical training programs continue to rely or have increased their
reliance on residence for service coverage, regardless of future needs and jobs, such as:
- Academic health facilities are often faced with the challenge of balancing more immediate
service requirements, the number of physicians that will be needed in the future, the number
of physicians working in the facility and their work patterns. The tension between teaching
institutions’ short-term service needs - often supported by residents – frequently results in the
creation of additional residency positions irrespective of predictions of future needs and jobs.
- Despite the benefi ts of interprofessional care models, additional residency positions are
needed to fi ll gaps in patient care because of the existing supply of physicians and surgeons
in teaching hospitals, and residents provide certain services that other health professionals
cannot offer.
- Some academic physicians stipulate that they need residents to maintain their current
levels of activity. These additional residents are often used to alleviate call requirements and
patient care needs.

Findings From The Royal College’s Employment Study - 2013
The reason that a residency program will increase the number of spots is typically because … they can, because they have the money and because they need the extra service to help look after their inpatient population.” [KII 15, emphasis added]
“
44
There was wide consensus among specialty committee
chairs, program directors and senior residents alike who
were experiencing employment problems, that hospitals
were increasingly relying on residents to perform varying
aspects of “call service” and patient care. It was thought
by key informants in our study that increasing the numbers
of residency training spots for particular specialties across
Canada, notably to ensure coverage of patient service,
would in effect “fl ood” the employment market once
those residents graduated and have a dramatic effect on
employment opportunities for new graduates.
Our study also documented the fi rst “live observations” of residents actually noting during their residency
training increasing numbers of residents on the clinic fl oor. As one senior resident from otolaryngology
aptly observed:
FIN
DIN
GS
““The diffi culty is that in the training centres [hospitals] we’re now used to having so many recruits
[residents] a year to help out with the activities that occur in the hospital to support our staff,
and that’s something that’s driving more training but it’s not necessarily helpful for us when we
get to the end of this training cycle … I have directly observed increasing numbers of residents
required to perform call service in the hospital. In addition, there’s the requirement for post-
operative care of patients, and also, just looking after the patients who are already operated on
by our faculty. They [our faculty] need certain support so that they can continue on with their
level of activity, and we are it. ” [KII 41, emphasis added]
““… some of the programs are taking residents not so much because they need to train that many
residents, as they need to fi ll spots on the call schedule. And I understand that, but at the end of
the day that means we have, …, X number of residents being trained and not necessarily
enough jobs for them when they fi nish. ” [KII 28, emphasis added] “
“
Concerns about producing more specialists than available jobs was also reported in neurosurgery where
covering service needs by residents is increasingly required when interprofessional models have not properly
taken root:
The tension between teaching institutions’ shorter-term service needs and properly planning medical
resources to meet longer-term societal health needs is an important driver behind new specialists’ job
challenges. This is particularly problematic since a shorter-term view does not take into consideration that it
currently takes at least four years to produce a specialist after completion of the MD degree. Our research
has revealed, especially in certain specialties, a concerning mismatch between the supply of new graduates
and available jobs because of the misalignment between models of health workforce planning, health care
delivery models and residency intake quotas.

Findings From The Royal College’s Employment Study - 201345
FIN
DIN
GS
A “culture of professional practice” refers to how health professions create and implement certain socio-
cultural norms that are part of the context or setting from which professions interact. “Each healthcare
profession has a different culture, including values, beliefs, attitudes, customs and behaviours” (Hall
2005, page 188). A culture of professional practice also delineates and/or sets forth boundaries for how
professional practice patterns will emerge, alongside the technical aspects or patterns occurring within a
clinical health care setting. Put differently, the practice of any profession, including medicine, has long been
known to be shaped and informed by the socio-cultural context (Ginsburg & Tregunno 2005; Hall 2005). Within
the health professions literature, professions have been recognized to exhibit and demonstrate various
aspects of “closure” whereby a given health profession “limits the number and type of entrants into its
fold, thus enhancing the market value of the service” (Hall 2005, page 189; Witz 1992).
Several ways were identifi ed from the research in which a culture of professional practice infl uenced and
defi ned professional practice patterns amongst specialists and, ultimately, had a signifi cant effect on
employment opportunities for new graduates. Key informants commented that, in addition to other driving
factors infl uencing physician employment, specialists themselves within certain hospital divisions were
implementing a culture of practice akin to “turf protectionism” (Gieryn 1983), where there was a distinct
unwillingness to share hospital resources such as OR with other incoming specialists.
Key fi nding
Most professions develop their own culture, which is motivated by both a greater altruistic
purpose for patients and self-interest.
Given that the availability of clinical and practice resources is generally fi xed, (this is especially the
case for OR time) established physicians and surgeons are reluctant to share resources to protect:
- their access to clinical resources to avoid cancelled surgeries that would further increase
their patients’ wait times
- their income as many wish to continue to practice at the same or increased level of intensity.
Income protection is particularly important for those whose retirement portfolios have been
negatively affected by the recent economic downturn.
Sharing available resources,
such as OR time, with new
colleagues was seen as having
a negative impact both on
individual surgeons’ existing
wait lists and income.
One senior hospital leader described scenarios within
his hospital units where specialist physicians appeared
unwilling to share OR time that became available when a
specialist position was vacated. Instead of allowing for a
new specialist to join the clinical team, the available OR
time was absorbed by the remaining group of specialists.
Referred to repeatedly as “sharing the pie”, this senior
hospital leader stated:
Culture of practice

Findings From The Royal College’s Employment Study - 201346
FIN
DIN
GS
Because OR time is generally not expanding for many surgical disciplines in Canada, surgeons must weigh
the need of including another associate within their surgical team against losing additional OR time,
ultimately contributing to an increased patient wait list, cancelled surgeries and, at times, loss of staff.
As one program director described:
Additional clinical and/or surgical procedures with extra OR time can also increase surgeons’ annual
income. The substantial increase in numbers of residents now in various training sites is also contributing
to income growth as the staff or attending surgeon can bill for surgeries conducted with residents. Thus,
some key informants stated there are few incentives for specialists to include a new specialist on their
hospital team nor is there a disincentive to have fewer residents practicing within the hospital.
““… We allow our department heads to decide how they’re going to divvy it up [operating room
time]…, so if you have a practice with 10 general surgeons but you have enough resources for
12, they’re quite enjoying the fact of having 10 share the pie instead of 12. … We have 15 ORs
and we could have 15 surgeons except that the 12 here want to have a day and a half as opposed
to a day, … When I saw a good person, I would say, ‘Let’s everybody spread a little bit and take a
little bit less of the pie so that we can keep this good person.’ ” [KII 24]
“
““… the number of OR days you have is the same and so if you want to bring someone else in you
have to cut the pie tighter. ... and there becomes a point where as surgeons, your practice
becomes very unwieldy and very diffi cult if you don’t have enough operating time because
you’re waiting list just grows longer and longer and longer. And then you just, you’re constantly …
fi ghting the battle and cancelling patients because something more urgent walks in the door and
your staff gets frustrated and they quit, and it just—it’s a diffi cult situation.” [KII 27, emphasis added]
“
What has happened in an unprecedented
way in the last ten years is the remaining three
urologists - who by the way have just lost half
their retirement in the stock market … they say,
“Geez, why don’t we not hire another urologist?
Let’s assume this person’s OR time and split it
amongst the three of us. … And this is what’s
really killing the people who are just coming out.
We [new graduates] are not being allowed in.”
[KII UR Grad B59, emphasis added]
“There are concerns that what amounts
to a confl ict among certain senior
specialists is not only having a negative
effect on hiring practices toward new
graduates by their not advertising
for new hospital positions, they are
also preferring to hire new graduates
on only a part-time or “associate”
basis which pays less than if they
were hired as full partners (Dempsey
2012), thus contributing to physician
underemployment.

Findings From The Royal College’s Employment Study - 201347
Fin
din
gs
4.2.3. Personal context: What are the personal factors driving employment challenges among new graduates?
The ability of new medical and surgical specialists to find and secure employment can also be influenced by
their individual experiences around career counseling, and their personal choices and needs.
• Career counseling- Generally poorly rated
- Poor understanding of job market
- Difficulty locating information about jobs
• Personal factors/preferences- Not going to where jobs are: - Issues with practice location or job type - Family obligations prevent move
Personal contextEmploymentproblemmain drivers
Career counseling
Key findings In addition to poor access
to job postings, lack of
transparency about available
jobs was reported as hindering
unemployed specialists find
suitable work.
The importance of career counseling cannot be
overemphasized, given that career choices by new
medical and surgical specialists are not only important
for physicians at the individual level, the individual
choices they make also impact the overall number, mix
and distribution of specialists across the country.
Yet, new specialists reported concerns:
- five out of ten who participating in our study in
2012 stated they had not received any career
counseling and;
- more than 1/3 without jobs and not continuing
training in 2012 reported that poor access to job
postings hampered their ability find a job.
A more systematic and
comprehensive approach to
career counseling and job
advertising than currently exists
in Canada is desirable to meet
both individual physician and
system needs and objectives.
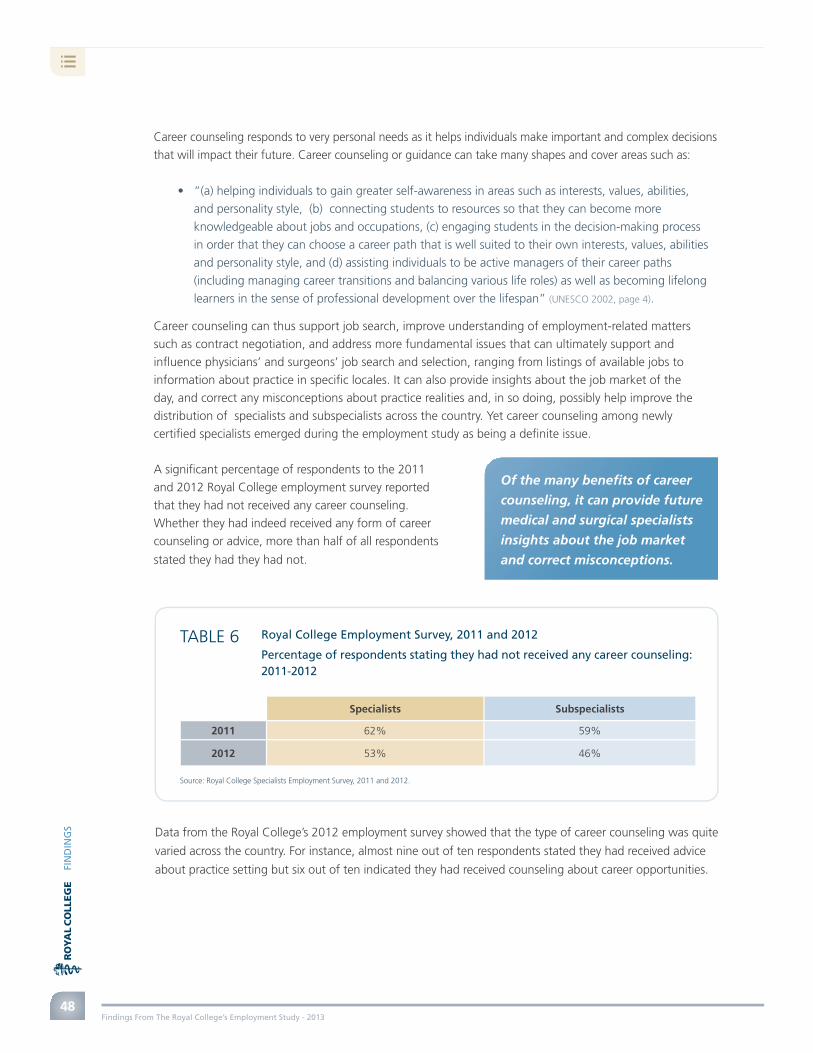
Findings From The Royal College’s Employment Study - 201348
FIN
DIN
GS
Career counseling responds to very personal needs as it helps individuals make important and complex decisions
that will impact their future. Career counseling or guidance can take many shapes and cover areas such as:
• “(a) helping individuals to gain greater self-awareness in areas such as interests, values, abilities,
and personality style, (b) connecting students to resources so that they can become more
knowledgeable about jobs and occupations, (c) engaging students in the decision-making process
in order that they can choose a career path that is well suited to their own interests, values, abilities
and personality style, and (d) assisting individuals to be active managers of their career paths
(including managing career transitions and balancing various life roles) as well as becoming lifelong
learners in the sense of professional development over the lifespan” (UNESCO 2002, page 4).
Career counseling can thus support job search, improve understanding of employment-related matters
such as contract negotiation, and address more fundamental issues that can ultimately support and
infl uence physicians’ and surgeons’ job search and selection, ranging from listings of available jobs to
information about practice in specifi c locales. It can also provide insights about the job market of the
day, and correct any misconceptions about practice realities and, in so doing, possibly help improve the
distribution of specialists and subspecialists across the country. Yet career counseling among newly
certifi ed specialists emerged during the employment study as being a defi nite issue.
Of the many benefi ts of career
counseling, it can provide future
medical and surgical specialists
insights about the job market
and correct misconceptions.
A signifi cant percentage of respondents to the 2011
and 2012 Royal College employment survey reported
that they had not received any career counseling.
Whether they had indeed received any form of career
counseling or advice, more than half of all respondents
stated they had they had not.
Data from the Royal College’s 2012 employment survey showed that the type of career counseling was quite
varied across the country. For instance, almost nine out of ten respondents stated they had received advice
about practice setting but six out of ten indicated they had received counseling about career opportunities.
Royal College Employment Survey, 2011 and 2012
Percentage of respondents stating they had not received any career counseling: 2011-2012
TABLE 6
Specialists Subspecialists
2011 62% 59%
2012 53% 46%
Source: Royal College Specialists Employment Survey, 2011 and 2012.

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
49
There is not only great variability reported about the type of career counseling received, so is there around
the opinions of residents about how satisfi ed they are with the employment or career counseling resources
within their residency program. Data from the CAIR 2012 National Resident Survey (refer to Figure 17)
showed that only 9% of those surveyed stated they were satisfi ed and 26% were somewhat satisfi ed with
the resources in their program (Dufour 2012).
Royal College Employment Survey, 2012
Type of career counseling reported by new specialists and subspecialists
Total exceeds 100% since question allowed multiple responses.
Source: 2012 Royal College Employment Survey.
TABLE 7
Advice about practice setting (academic vs. community)298 respondents (86.4%)
Work conditions (remuneration, benefi ts, and research/training oppurtunities)226 respondents (65.5%)
Career opportunities221 respondents (64.1%)
Other (eg., staff mentorship, getting fellowship, the advantages of academic medicine, paths to apply for job)
14 respondents (4.1%)
21%Unsatisfied
22%Somewhatunsatisfied22%
Had not usedthese resources
9%Satisfied
26%Somewhat
satisfied
Source: 2012 National Resident Survey. Canadian Association of Internes and Residents.
In the 2012 Royal College employment study,
over one third (34.7%) of all respondents who
had not secured a position and who were not
continuing training when they completed the
survey stated that poor access to job postings
was another factor contributing to their inability
to fi nd a job. This was reported as being more
problematic by subspecialists with 62.5%
identifying this factor, compared to 21.2% of
specialists who responded to this question.
FIGURE 17Resident satisfaction with employment or career counseling resources within
their residency program
More than 1/3 of new specialists
without jobs and not continuing
training in 2012 reported that poor
access to job postings hampered
their ability fi nd a job.

Findings From The Royal College’s Employment Study - 2013
FIN
DIN
GS
50
Although the internet is increasingly the tool of choice for job seekers to locate employment opportunities, it
does have its limitations: “While the Internet has opened up many new opportunities, many job seekers face the
challenge of fi nding, navigating, prioritizing and evaluating this material effectively. …” (de Raaff et al 2012, p. 4).
Our research not only revealed that some job seekers found sifting
through available information daunting, some key informants who
reported they had not been able to secure a job expressed frustration
about the lack of openness about available positions. Some felt that
better access to and transparency about available jobs was key to
helping unemployed specialists fi nd suitable work. In short, access
to comprehensive job postings might facilitate matching personal
choices and needs with the job market.
The fi nal report of the Future of Medical Education in Canada Project acknowledged the strategic importance
to “[e]ncourage ongoing mentorship programs (student-student and faculty-student) to provide guidance
for learners in such activities as choosing electives, engaging in research, getting involved in the community,
and making career choices” (AFMC 2010, page 11). Some informants in our study stated that a more systematic
and comprehensive approach than currently exists in Canada is desirable to meet both individual physician
and system needs and objectives.
…there are no job
posting nowadays, it’s
all hidden.” 2012 Royal
College Employment Survey
“
Personal factors and preferences
Personal factors infl uence the choices that physicians make about the type and location of practice.
UK research affi rms that “[m]otivation and values that underpin it are major factors in determining career
choices” (Jackson, Ball, Hirsh & Kidd 2003, page 13).
Key fi ndings
Personal factors infl uence the choices that physicians make about the type and location of
practice they can and will pursue. This is a byproduct of many infl uencers, including;
- the later age at which new graduates enter independent practice. Many new graduates
have family responsibilities that might make it less easy to move to available job
opportunities (sandwich generation, spousal employment, etc.)
- personal career preference such as practice location or type.
Key informants stated that access to comprehensive job postings might facilitate matching
personal choices and needs with the job market.

Findings From The Royal College’s Employment Study - 2013
wish to stay near family
hiring hospital doesn’t have the resourcesI have been trained to use
don’t like living in a rural/remote setting
can’t/won’t move
don’t like working in a community hospital
Column totals may exceed 100% as this question allowed for multiple responses. Source: Royal College Employment Survey, 2011 and 2012
20.4%
28.6%
8.2%
6.1%
38.8%
51
FIN
DIN
GS
Royal College Employment Survey, 2012
No job placement and at end-point of residency training (n=49), Why you feel you do not have a job placement?
FIGURE 18
Our research shows that various personal motivations and needs impact job and career choices. While
data collected to date is relatively limited, fi ndings show that personal reasons merit ongoing examination
(refer to Figure 18).
Despite a tight job market, new graduates often have families and associated obligations that might make
it more diffi cult for them to follow available openings. This is particularly so since most medical specialists
start independent practice at a later age because of the length of their training. As such, they may be
experiencing many of the challenges of others in the “sandwich generation” which is “caught between
the often confl icting demands of caring for children and caring for seniors” (Williams 2005, page 16).
It has also been observed “that spousal opportunities, educational opportunities for all members of the
family, cultural, recreation and religious activities, community orientation, special funding for locum support,
assistance with practice establishment costs, and paid vacation time, to name a few, have a positive impact
on recruitment and retention” (Task Force Two 2006, page 24).
Few interesting locations
and practice type combinations.
Looking at options.” 2012 Royal
College Employment Survey
I could not get any clinic
time at a hospital in Ottawa
despite there being such a need.
My husband works in Ottawa,
making a move not an option.”
2012 Royal College Employment Survey
“ … after having trained in neurosurgery, with a Master’s from a fairly prestigious institution in the United States, plus a fellowship from also a fairly prestigious location in the United States, I don’t think I should go to a small community hospital to do straightforward general neurosurgery procedures… I would [prefer] go to a larger centre in the United States, where I could have a better lifestyle and do the practice that I wanted .” 2011 Royal College Employment Survey
“
“

Findings From The Royal College’s Employment Study - 2013
What are the effects of employment challenges on new graduates?
5.0
• Morphed practice- Work only within available resources- Don’t practice specialty as taught- Underemployment: for ex., surgeons that
don’t or rarely operate- Fear of skill loss
• Brain drain- 27.3% of those in 2012 reporting
no job and not training plan to seek employment outside of Canada
Employmentproblemmain drivers
5.1. Tailored and morphed practices
Effect
52
WH
aT
aR
E TH
E EF
FEC
Ts?
Because some new specialists have only
been able to secure limited access to hospital
resources such as OR time or have not been
able to secure a job in a hospital setting
required to practice their discipline, they are
developing tailored or morphed practices.
These tailored or morphed practices allow
new medical and surgical specialists to work
within the resources available to them.
Key findings These morphed practices do not embrace
the full spectrum of the discipline in
which they were certified, resulting in a
form of under-employment or brain waste
(such as a surgeon who does not or rarely
does operations).
New physicians and surgeons who have
developed morphed practices tailored to
available resources are in effect evolving
into a new type of specialist. While this
new breed of specialists may be providing
much needed services, concerns remain
that these new practice models are a
waste of the talent and competencies
these specialists spent years to develop.
There are also concerns about skills
loss that may result in poorer patient
outcomes if these morphed specialists
secure jobs that require the full spectrum
of the discipline taught during residency.

Findings From The Royal College’s Employment Study - 2013
A number of new graduates have been
unable to secure a position in hospital
settings or only able to secure limited
access to hospital resources such as OR
time needed to practice their specialty
because of hiring limits driven by both
economic constraint and established
physicians retaining access to available
resources. For instance, Comeau (2004)
has argued that due to operating room
restrictions, less than half of Canada’s
orthopedic surgeons are working at full
capacity, with many operating only one
to two days a week. In response, some
new graduates are developing tailored
or morphed practices that allow them
to practice with the resources available
to them. For example, some new
otolaryngology graduates are pursuing
a clinical practice without actually
conducting any major aspects of surgery
itself, despite their extensive training in
surgery during their residency program.
Known as an “offi ce practice”, these
practices are non-surgical or provide
limited surgical services.
A recent trend for some graduates is that
they recognize that even if they are able to
get a hospital appointment, they probably
won’t get much OR time, and so…they try
to alter their practice so they’re doing more
things that can be done in the offi ce, such as
skin cancers…certain procedures for snoring
and sleep apnea, and… outpatient type
things where you don’t require bed resources
or necessarily general anesthesia. …There
[are] a couple of people that have decided
that they’re not going to do surgery and
just do a clinical practice, which is possible
in otolaryngology as well. …we fi nd this is a
tremendous waste after the amount of time
and effort going into learning surgery…if
somebody works for fi ve years, hoping to have
at least a one-day-a-week hospital surgical
appointment, and then has an offi ce practice,
and [is] not able to use the skills that they
learned during training – I think [that] would
be a tremendous disappointment.” [KII 32]
“
These morphed or tailored practices are in fact creating a new breed of specialist and some key informants
expressed concerns about skill loss. Although there is limited literature in regards to this issue in Canada,
there is evidence in regards to volume of practice and patient outcomes. A 2003 study demonstrated that
surgical volume was inversely related to patient mortality in eight procedures including lung resections,
repair of abdominal aortic aneurysms, esophagectomies, coronary artery bypass grafting, pancreatic
resections, cystectomies, aortic valve replacements and carotid surgery (Birkmeyer, Stukel, Siewers, Goodney,
Wenneberg & Lucas 2003). The mortality was higher for patients who had low volume surgeons, irrespective of
the hospital volume (2003). Therefore, one can hypothesize that if recent Canadian graduates are not able
to have high enough procedural volumes than this may result in poorer patient outcomes in the future.
53
WH
AT
AR
E TH
E EF
FEC
TS?
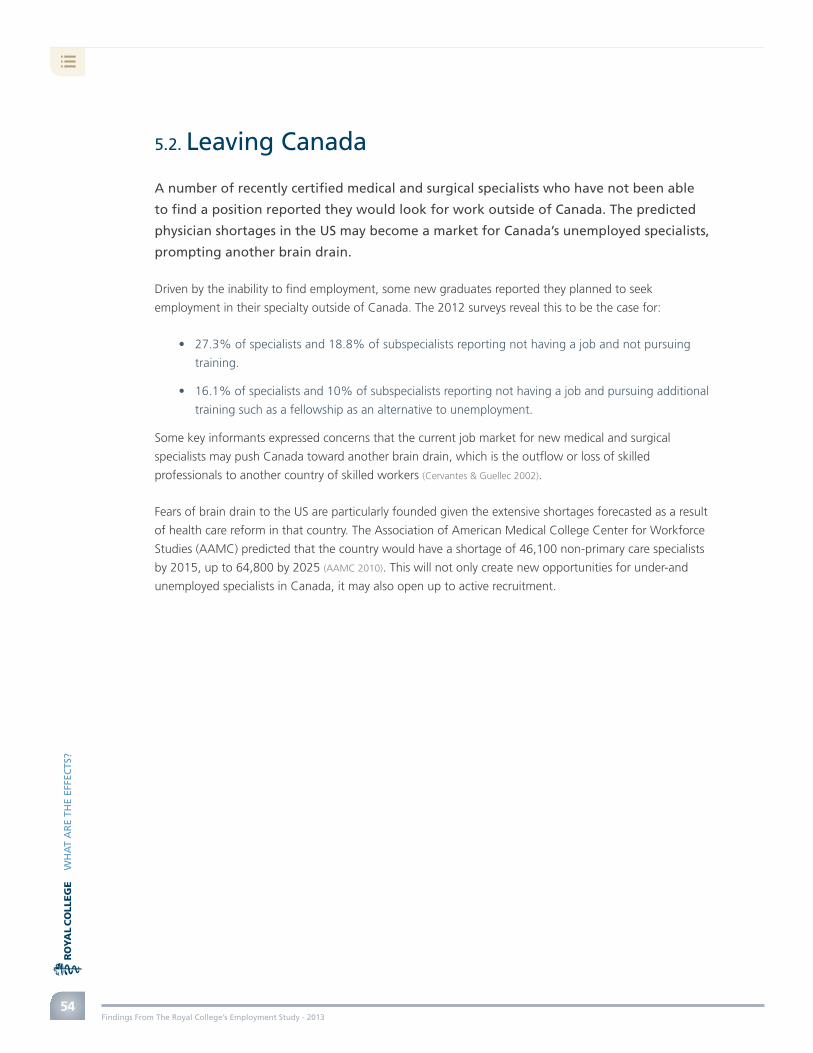
Findings From The Royal College’s Employment Study - 2013
A number of recently certifi ed medical and surgical specialists who have not been able
to fi nd a position reported they would look for work outside of Canada. The predicted
physician shortages in the US may become a market for Canada’s unemployed specialists,
prompting another brain drain.
Driven by the inability to fi nd employment, some new graduates reported they planned to seek
employment in their specialty outside of Canada. The 2012 surveys reveal this to be the case for:
• 27.3% of specialists and 18.8% of subspecialists reporting not having a job and not pursuing
training.
• 16.1% of specialists and 10% of subspecialists reporting not having a job and pursuing additional
training such as a fellowship as an alternative to unemployment.
Some key informants expressed concerns that the current job market for new medical and surgical
specialists may push Canada toward another brain drain, which is the outfl ow or loss of skilled
professionals to another country of skilled workers (Cervantes & Guellec 2002).
Fears of brain drain to the US are particularly founded given the extensive shortages forecasted as a result
of health care reform in that country. The Association of American Medical College Center for Workforce
Studies (AAMC) predicted that the country would have a shortage of 46,100 non-primary care specialists
by 2015, up to 64,800 by 2025 (AAMC 2010). This will not only create new opportunities for under-and
unemployed specialists in Canada, it may also open up to active recruitment.
5.2. Leaving Canada
54
WH
AT
AR
E TH
E EF
FEC
TS?

Findings From The Royal College’s Employment Study - 2013
Conclusion 6.0
The fi ndings presented in this report are not the fi nal answer.
This report is only a beginning.
Our research has revealed what appears to be an important gap in how medical workforce planning
has been generally visualized in Canada. Most approaches to date are based on producing the right mix
and number of physicians, based on society’s health needs. Our research revealed that is only part of the
picture. A number of specialty medical disciplines need particular resources, such as operating room time
and hospital beds. However, costs must be controlled so access to such resources is tightly controlled,
affecting how many specialists and subspecialists can practice and how much work they can do.
As such, medical workforce planning must look at both the health needs of the population and the
availability of practice resources, now and in the future. This will help physicians and surgeons do
the work they have been trained to do and what needs to be done. To do otherwise will perpetuate
physician unemployment with the associated likelihood that Canada’s unemployed physicians will fi nd
jobs elsewhere, prompting a new brain drain. Poor planning will also worsen physician brain waste or
underemployment since they will only be able to apply a portion of their knowledge and skills based
on the resources available to them.
Unpeeling the multiple layers around the complex factors impacting and driving physician employment
will take time. Our investigation continues and, hopefully, will drive others to join in the search for better
information, understanding and answers.
“For meaningful change to occur in physician distribution, changes in [postgraduate medical
education] PGME training must be part of a comprehensive package of reforms that includes
interprofessional practice models, professional and career support, and remuneration.”
[Takahashi, Bates, Verma, Meterissian, Rungta & Spadafora 2011, page 26] “
55
CO
NC
LUSI
ON
Answers to Canada’s physician unemployment problems will thus require broad input and collaboration,
and most importantly, a cohesive national strategy.

Findings From The Royal College’s Employment Study - 2013
Alberta Health Services. Physician Assistants. Retrieved from http://www.albertahealthservices.ca/8754.asp
Alock, D. S. 1996. The clinical nurse specialist, clinical nurse specialist/nurse practitioner and other titled nurse in Ontario. Canadian Journal of Nursing Administration, 9(1), 23-44.
Association of Faculties of Medicine of Canada. 2010. The Future of Medical Education in Canada (FMEC): A Collective Vision for MD Education. Ottawa, On: Association of Faculties of Medicine of Canada. Retrieved from http://www.afmc.ca/fmec/pdf/collective_vision.pdf
Association of American Medical College’s Center for Workforce Studies. 2010. Physician Shortages to Worsen Without Increases in Residency Training. Retrieved from https://www.aamc.org/download/286592/data/
Barro, R.J., & Ursúa, J.F. 2009. Stock-Market Crashes and Depressions – Working Paper 14760. Cambridge, MA: National Bureau of Economic Research. Retrieved from http://www.nber.org/papers/w14760.pdf?new_window=1
Birkmeyer, J.D., T.A. Stukel, A.E. Siewers, P.P. Goodney, D.E. Wennberg, & F.L. Lucas. 2003. Surgeon Volume and Operative Mortality in the United States. N Eng J Med, 349, 2117-2127.
Bisset, K., 2013. Job cuts in New Brunswick health system. Metro. Retrieved from http://metronews.ca/news/canada/638903/job-cuts-in-new-brunswick-health-system/
Bohm, E.R., Dunbar, M., Pitman, D., Rhule, C., & Araneta, J. 2010. Experience with physician assistants in a Canadian arthroplasty program. Canadian Journal of Surgery, 53(2), 103–108. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2845948/
Born, K., & Dhalla. I. 2012. How specialty positions are allocated for medical school graduates. Healthy Debate. Retrieved from http://healthydebate.ca/2012/01/topic/politics-of-health-care/residencymatch
Buchan, J., & Dal Poz, M.R., 2002. Skill mix in the health care workforce: reviewing the evidence. Bulletin of the World Health Organization, 80(7):, 575-580. Retrieved from http://www.who.int/bulletin/archives/80(7)575.pdf
Boyle, T. 2013. Ontario budget will see more hospital downsizing and community upsizing, health minister says. The Star. Retrieved from http://www.thestar.com/news/canada/2013/05/02/ontario_budget_will_see_more_hospital_downsizing_and_community_upsizing_health_minister_says.html
Buske, L. 2012. Best Laid Plans – Results of National Physician Survey Cohort Analysis. Canadian Collaborative Centre for Physician Resources Bulletin. Retrieved from http://nationalphysiciansurvey.ca/wp-content/uploads/2012/07/C3PR-Bulletin-Cohort-201207-EN.pdf
Canadian Association of Internes and Residents. 2012. Summary of Key Findings: 2012 National Resident Survey. Retrieved from http://cair.ca/u/elibrary/Summary%20of%20Key%20Findings%20-%20CAIR%202012%20National%20Resident%20Surve.pdf
Canadian Association of Physician Assistants (CAPA). 2013a. About PAs-History. Retrieved from http://capa-acam.ca/about-pas/history/
Canadian Association of Physician Assistants (CAPA). 2013b. Scope of practice and national competency profi le. Retrieved from http://capa-acam.ca/wp-content/uploads/2012/12/NCP_en_sept20092.pdf
Canadian Foundation for Healthcare Improvement. 2010. Myth: Most physicians prefer fee-for-service payments. Retrieved from http://www.cfhi-fcass.ca/publicationsandresources/Mythbusters/ArticleView/10-01-01/13b5e8bb-e7c2-4544-8da5-b1aa5d9e38db.aspx
Canadian Institute for Health Information (CIHI). 2011. Health Care Cost Drivers. The Facts. Ottawa, On: CIHI. Retrieved from https://secure.cihi.ca/free_products/health_care_cost_drivers_the_facts_en.pdf
Canadian Institute for Health Information (CIHI). 2012a. National Health Expenditure Trends, 1975 to 2012. Ottawa, On: CIHI. Retrieved from https://secure.cihi.ca/estore/productFamily.htm?locale=en&pf=PFC1952
Canadian Institute for Health Information (CIHI). 2012b. Health Care Cost Drivers: Physician Expenditure—Technical Report. Ottawa, on: CIHI. Retrieved from http://www.cihi.ca/CIHI-ext-portal/pdf/internet/HEALTH_COSTDRIVER_PHYS_TECH_EN
References
56
REF
EREN
CES

Findings From The Royal College’s Employment Study - 2013
Canadian Institute for Health Information. 2013. Wait Times for Priority Procedures in Canada, 2013. Ottawa, On: CIHI. Retrieved from https://secure.cihi.ca/free_products/wait_times_2013_en.pdf
Cervantes, M., & Guellec, D. 2002. “The brain drain: Old myths, new realities. OECD Observer. Retrieved from http://www.oecdobserver.org/news/archivestory.php/aid/673/The_brain_drain:_Old_myths,_new_realities.html
College of Physicians and Surgeons of Nova Scotia (CPSN). 2013. Clinical Assistant Program. Retrieved from http://www.cpsns.ns.ca/Registration/Clinicalassistantprogram.aspx
Comeau, P. 2004. Crisis in orthopedic care: surgeon and resource shortage. Canadian Medical Association Journal, 171(3), 223.
Creswell, J. W. 1994. Research design: Qualitative and quantitative approaches. London: Sage.
Creswell, J. W., & Plano Clark, V.L. 2010. Designing and Conducting Mixed Methods. Thousand Oaks: CA: Sage.
Cuddenback, G., Wilson, E., Orme, J.G., & Combs-Orme, T. 2004. Detecting and Statistically Correcting Sample Selection Bias. Journal of Social Service Research, 30(3). Retrieved from http://www.haworthpress.com/web/JSSR
de Raaf, S., Shek-wai Hui, T., & Vincent, C. 2012. CareerMotion: How Web-based technologies can improve the career choices of young people. Ottawa, On: Social Research and Demonstration Corporation. Retrieved from http://www.careermotion.ca/en/fi les/1313/2639/2243/en_cmreport.pdf
CBCnews. 2013. Edmonton hospitals cutting overtime, operating room days. Retrieved from http://www.cbc.ca/news/canada/edmonton/story/2013/01/30/edmonton-.html
Dempsey, A. 2012. Health-care checkup: Why can’t newly graduated specialist doctors in Canada fi nd jobs? The Star. Retrieved from http://www.thestar.com/news/gta/2012/11/15/healthcare_checkup_why_cant_newly_graduated_specialist_doctors_in_canada_fi nd_jobs.html
DiCenso, A., Martin-Misener, R., Bryant-Lukosius, D., Beaugeault, I., Kilpatrick, K., Donald, F., (et. al.) 2010. Advanced practice nursing in Canada: overview of a decision support synthesis. Nursing Leadership, 23 (Special Issue), 15-34.
Ducharme, J., Alder, R.J., Pelletier, C., & Tepper, J. 2009. The impact on patient fl ow after the integration of nurse practitioners and physician assistants in 6 Ontario emergency departments. Canadian Journal of Emergency Medicine, 11(5), 455-461. Retrieved from http://www.cjem-online.ca/v11/n5/p455
Dufour, M. Through the Residents’ Lens: Results from the Canadian Association of Internes and Residents 2012 National Resident Survey. PowerPoint presentation at the Royal College of Physicians and Surgeons of Canada 2012 Human Resources for Health Dialogue Conference. December 3, 2012. Retrieved from http://www.royalcollege.ca/portal/page/portal/rc/common/documents/advocacy/hhr2012_dufour_cair_e.pdf
Eakin, J., Robertson, A., Poland, B., Coburn, D., & Edwards, R. (1996). Towards a critical social science perspective on health promotion research. Health promotion international, 11(2), 157-165.
Fédération des médecins résidents du Québec. 2013. Practising In Quebec – Positions Available (PREM). Retrieved from: http://www.fmrq.qc.ca/formation-medicale/info_ang.cfm?noPageSiteInternet=142&cfgsection=pratiquerauquebec&cfgsoussection=postes-disponibles-prem
Feindel, C.M., 2010. The Current Status of Cardiac Surgery Workforce in Canada: Presentation at the 2010 Royal College-NSS Human Resources for Health Conference. December 7, 2010. Retrieved from http://www.royalcollege.ca/portal/page/portal/rc/common/documents/advocacy/hhr_attachment6_e.pdf
Forster, F. 2012. Developing a nurse practitioner role for hip fracture care: A journey of challenges International Journal of Orthopaedic and Trauma Nursing. International Journal of Orthopaedic and Trauma Nursing 16, 214–221Fowlie, J. 2013. BC Liberals postelection budget rolls out new rounds of cuts. Vancouver Sun. Retrieved from http://www.vancouversun.com/news/Liberals+post+election+budget+rolls+round+cuts/8588892/story.html
Fowlie, J. 2013. BC Liberals postelection budget rolls out new rounds of cuts. Retrieved from http://www.vancouversun.com/news/Liberals+post+election+budget+rolls+round+cuts/8588892/story.html
Fulton, J. S. & K. Baldwin. 2004. An Annotated Bibliography Refl ecting CNS Practice and Outcomes. Clinical Nurse Specialist, 18(1), 21-39.
57
REF
EREN
CES

Findings From The Royal College’s Employment Study - 2013
Ginsburg, L. & Tregunno, D. 2005. New Approaches to interprofessional education and collaborative practice: Lessons from the organizational change literature. Journal of Interprofessional Care, Supplement 1, 177-187.Government of Manitoba. 2009. The Medical Act (C.C.S.M. c. M90)-Clinical Assistants and Physician Assistants Regulation. Retrieved from http://web2.gov.mb.ca/laws/regs/pdf/m090-183.99.pdf
Government of New Brunswick. 2013. REVISED/ Renewal of New Brunswick’s health-care system: Partners take measures to ensure its sustainability-News Release. Retrieved from http://www2.gnb.ca/content/gnb/en/news/news_release.2013.04.0345.html
Glover Takahashi, S., Bates J., Verma S., Meterissian S., Rungta K., & Spadafora S., 2011 Environmental Scan Synthesis Report. Ottawa, On: Association of Faculties of Medicine of Canada. Retrieved from: http://www.afmc.ca/pdf/fmec/Synthesis-Report.pdf
Gieryn, T. F. 1983. Boundary-work and the demarcation of science from non-science: Strains and interests in professional ideologies of scientists. American Sociological Review, 48, 781-795.
Greene, J. C., Caracelli, V. J., & Graham, W. F. (1989). Toward a conceptual framework for mixed-method evaluation designs. Educational Evaluation and Policy Analysis, 11, 255-274.
Hall, P. 2005. Interprofessional teamwork: Professional cultures as barriers. Journal of Interprofessional Care, Supplement 1, 188-196
Hall, R.E., & Lieberman, M. 2007. Microeconomics: Principles and Applications. Cincinnati: South Western Education Publishing.
Harrington, D.W., Wilson, K., Rosenberg, & M. Bell, S. 2013. Access granted! barriers endure: determinants of diffi culties accessing specialist care when required in Ontario, Canada. BMC Health Services Research, 13, 146. Retrieved from http://www.biomedcentral.com/1472-6963/13/146
Hunsberger, M., Mitchell A., Blatz, S., Paes, B., Pinelli, J., Southwell, French, S., & Soluk, R. 1992. Defi nition of an advanced nursing practice role in the NICU: The clinical nurse specialist/neonatal practitioner. Clinical Nurse Specialist, 6(2), 91-96.
Jackson, C., Ball, J.E., Hirsh, W., & Kidd, J.M. 2003. Informing Career Choices: The Need for Career Advice in Medical Training. Cambridge, UK: The National Institute for Careers Education and Counseling. Retrieved from: http://www.crac.org.uk/CMS/fi les/upload/nicec_informingchoices_medicaltrainig_report.pdf
Judge, T.A., Bono, J.E. 2001. Relationship of Core Self-Evaluations Traits—Self-Esteem, Generalized Self-Effi cacy, Locus of Control, and Emotional Stability—With Job Satisfaction and Job Performance: A Meta-Analysis. Journal of Applied Psychology, 8(1), 80-92. Retrieved from: http://dtserv2.compsy.uni-jena.de/__C12579D400409087.nsf/0/9FD1ECAD14418FB4C12579E4006AC7BE/$FILE/Judge_Bono_2001.pdf
Kaasalainen, S., Martin-Misener R., Kilpatrick, K., Harbman, P. Bryant-Lukosius, D., Donald, F., Carter, N., & DiCenso, A. 2010. A historical overview of the development of advanced practice nursing roles in Canada. Canadian Journal Nursing Leadership. 23(Special Issue), 35-60.
McMaster University. Physician Assistant Education Program. 2013. Retrieved from http://fhs.mcmaster.ca/physicianassistant/
MacDonald-Rencz, S. & Bard, R. 2010. The role for advanced practice nursing in Canada. Nursing Leadership, 23(Special Issue), 8-11.
Mishkin, F.S. & White, E.N. 2002. U.S. Stock market crashes and their aftermath: implications for Monetary Policy- Working Paper 8992. Cambridge, MA: National Bureau of Economic Research. Retrieved from http://www.nber.org/papers/w8992.pdf?new_window=1
National Steering Committee on Resident Duty Hours. 2013. Fatigue, Risk and Excellence: Towards a Pan-Canadian Consensus on Resident Duty Hours. Ottawa, On: The Royal College of Physicians and Surgeons of Canada. Retrieved from: http://www.residentdutyhours.ca/documents/fatigue_risk_and_excellence.pdf
New Brunswick Medical Society. 2013. New Brunswick’s doctors seek more details on “effi ciencies” from hospitals. Retrieved from http://www.nbms.nb.ca/news/new-brunswick-s-doctors-seek-more-details-on-effi ciencies-from-hospitals/#.Ufvf11r70Vk
Ouzounian, M., Hassan, A., Teng C.J., Tang G.H., Vanderby S.A., Latham T.B., & Feindel C.M., 2010. The cardiac surgery workforce: a survey of recent graduates of Canadian training programs. Ann Thorac Surg, 90, 460-466. Retrieved from http://www.annalsthoracicsurgery.org/article/S0003-4975(10)00921-5/fulltext#sec1
58
REF
EREN
CES

Findings From The Royal College’s Employment Study - 2013
Pardhan A., & Saad N. 2011. Governance in Postgraduate Medical Education in Canada. Ottawa, On: Association of Faculties of Medicine of Canada. Retrieved from: http://www.afmc.ca/pdf/fmec/08_Pardhan_Governance.pdf
Parliament of Canada. The Health of Canadians – The Federal Role Interim Report, Volume One – The Story So Far, Chapter Six: Myths and Realities 2001. Retrieved from http://www.parl.gc.ca/Content/SEN/Committee/371/pdf/interim-soci-e.pdf
Pong, R.W., Lemire, F., & Tepper J. 2007. Physician Retirement in Canada: What Is Known and What Needs to be Done. –Paper prepared for the 10th International Medical Workforce Conference. Retrieved from http://rcpsc.medical.org/publicpolicy/imwc/10_ret&retCAN.pdf
Pong, R.W. 2011. Putting Away the Stethoscope for Good? Toward a New Perspective on Physician Retirement. Ottawa, On: Canadian Institute for Health Information. Retrieved from https://secure.cihi.ca/free_products/HHR%20Physician%20Report_En_Web.pdf
Presnell, D. 2013. Growing Rural Medicine. UBC Reports, 59(4). Retrieved from http://www.publicaffairs.ubc.ca/2013/04/03/growing-rural-medicine/
Priest, L. 2011. Canadian surgeons face flat-lining job market. The Globe And Mail. Retrieved from http://www.theglobeandmail.com/life/health-and-fitness/canadian-surgeons-face-flat-lining-job-market/article568544/
Pringle D. 2007. Nurse practitioner role: Nursing needs it. Royal College of Physicians and Surgeons of Canada. 2010. Royal College - National Specialty Societies’ Human Resources for Health Conference, Report on pre-conference consultations with NSS
Royal College of Physicians and Surgeons of Canada. 2010. Royal College - National Specialty Societies’ Human Resources for Health Conference, Report on pre-conference consultations with NSS.
Royal College of Physicians and Surgeons of Canada.2010 (2). Royal College - National Specialty Societies’ Human Resources for Health Conference, Back to basics: getting the record straight on the numbers and the story they tell. Retrieved from http://www.royalcollege.ca/portal/page/portal/rc/common/documents/advocacy/nss_hrh_conference_summary2010_e.pdf
Sylvain, M. 2009. Doctors’ Retirement Plans on Life Support. Benefits Canada. February 4, 2009. Retrieved from http://www.benefitscanada.com/investments/global-investments/doctors-retirement-plans-on-life-support-9839/2
Statistics Canada. 2013. Labour force characteristics, seasonally adjusted, by province (monthly). Retrieved from http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/lfss01a-eng.htm
Taggart, K. 2012. New orthopedic surgeons facing spectre of unemployment, meeting told. Canadian Medical Association. Retrieved from http://www.cma.ca/new-orthopedic-surgeons-unemployment
Task Force Two: A physician human resource strategy for Canada. 2006. A physician human resource strategy for Canada: Final report. Retrieved from: http://www.physicianhr.ca/reports/TF2FinalStrategicReport-e.pdf
The College of Family Physicians of Canada, Canadian Medical Association & The Royal College of Physicians and Surgeons of Canada. 2010. National Physician Survey. Retrieved from http://nationalphysiciansurvey.ca/surveys/
Tomlinson, C., Wong, C., Au, H.-J., & Schiller, D. 2012. Factors associated with delays to medical assessment and diagnosis for patients with colorectal cancer. Can Fam Physician, 58, 495-501. Retrieved from http://171.66.125.180/content/58/9/e495.full?sid=6a568ee4-cf85-4468-ae11-273fb754d891
United Nations Educational, Scientific and Cultural Organization. 2002. Handbook on career counseling: A practical manual for developing, implementing and assessing career counselling services in higher education settings. Paris: UNESCO. Retrieved from http://unesdoc.unesco.org/images/0012/001257/125740e.pdf
Wai, E.S., Mackinnon, M., Hooker, R., Moccia, P., Perry, K., & Truong, P. T. 2012. Wait Times in Diagnostic Evaluation and Treatment for Patients With Stage III Non-Small Cell Lung Cancer in British Columbia. American Journal of Clinical Oncology, 35(4), 373–377. Retrieved from http://journals.lww.com/amjclinicaloncology/Abstract/2012/08000/Wait_Times_in_Diagnostic_Evaluation_and_Treatment.13.aspx
Williams, C. 2005. The Sandwich Generation. Canadian Social Trends. Statistics Canada — Catalogue No. 11-008. Retrieved from http://www.statcan.gc.ca/pub/11-008-x/2005001/article/7033-eng.pdf
Witz, C. B. 1992. Professions and patriarchy. London: Routledge.
Wright, T. 2013. Currie challenges accuracy of the latest CIHI report. The Guardian. Retrieved from: http://www.theguardian.pe.ca/News/Local/2013-01-25/article-3164317/Currie-challenges-accuracy-of-the-latest-CIHI-report/1
59
REF
EREN
CES

Findings From The Royal College’s Employment Study - 2013
Pardhan A., & Saad N. 2011. Governance in Postgraduate Medical Education in Canada. Ottawa, On: Association of Faculties of Medicine of Canada. Retrieved from: http://www.afmc.ca/pdf/fmec/08_Pardhan_Governance.pdf
Parliament of Canada. The Health of Canadians – The Federal Role Interim Report, Volume One – The Story So Far, Chapter Six: Myths and Realities 2001. Retrieved from http://www.parl.gc.ca/Content/SEN/Committee/371/pdf/interim-soci-e.pdf
Pong, R.W., Lemire, F., & Tepper J. 2007. Physician Retirement in Canada: What Is Known and What Needs to be Done. –Paper prepared for the 10th International Medical Workforce Conference. Retrieved from http://rcpsc.medical.org/publicpolicy/imwc/10_ret&retCAN.pdf
Pong, R.W. 2011. Putting Away the Stethoscope for Good? Toward a New Perspective on Physician Retirement. Ottawa, On: Canadian Institute for Health Information. Retrieved from https://secure.cihi.ca/free_products/HHR%20Physician%20Report_En_Web.pdf
Presnell, D. 2013. Growing Rural Medicine. UBC Reports, 59(4). Retrieved from http://www.publicaffairs.ubc.ca/2013/04/03/growing-rural-medicine/
Priest, L. 2011. Canadian surgeons face flat-lining job market. The Globe And Mail. Retrieved from http://www.theglobeandmail.com/life/health-and-fitness/canadian-surgeons-face-flat-lining-job-market/article568544/
Pringle D. 2007. Nurse practitioner role: Nursing needs it. Nursing Leadership, 20(2), 1-5.
Royal College of Physicians and Surgeons of Canada. 2010. Royal College - National Specialty Societies’ Human Resources for Health Conference, Report on pre-conference consultations with NSS.
Royal College of Physicians and Surgeons of Canada.2010 (2). Royal College - National Specialty Societies’ Human Resources for Health Conference, Back to basics: getting the record straight on the numbers and the story they tell. Retrieved from http://www.royalcollege.ca/portal/page/portal/rc/common/documents/advocacy/nss_hrh_conference_summary2010_e.pdf
Sylvain, M. 2009. Doctors’ Retirement Plans on Life Support. Benefits Canada. February 4, 2009. Retrieved from http://www.benefitscanada.com/investments/global-investments/doctors-retirement-plans-on-life-support-9839/2
Statistics Canada. 2013. Labour force characteristics, seasonally adjusted, by province (monthly). Retrieved from http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/lfss01a-eng.htm
Taggart, K. 2012. New orthopedic surgeons facing spectre of unemployment, meeting told. Canadian Medical Association. Retrieved from http://www.cma.ca/new-orthopedic-surgeons-unemployment
Task Force Two: A physician human resource strategy for Canada. 2006. A physician human resource strategy for Canada: Final report. Retrieved from: http://www.physicianhr.ca/reports/TF2FinalStrategicReport-e.pdf
The College of Family Physicians of Canada, Canadian Medical Association & The Royal College of Physicians and Surgeons of Canada. 2010. National Physician Survey. Retrieved from http://nationalphysiciansurvey.ca/surveys/
Tomlinson, C., Wong, C., Au, H.-J., & Schiller, D. 2012. Factors associated with delays to medical assessment and diagnosis for patients with colorectal cancer. Can Fam Physician, 58, 495-501. Retrieved from http://171.66.125.180/content/58/9/e495.full?sid=6a568ee4-cf85-4468-ae11-273fb754d891
United Nations Educational, Scientific and Cultural Organization. 2002. Handbook on career counseling: A practical manual for developing, implementing and assessing career counselling services in higher education settings. Paris: UNESCO. Retrieved from http://unesdoc.unesco.org/images/0012/001257/125740e.pdf
Wai, E.S., Mackinnon, M., Hooker, R., Moccia, P., Perry, K., & Truong, P. T. 2012. Wait Times in Diagnostic Evaluation and Treatment for Patients With Stage III Non-Small Cell Lung Cancer in British Columbia. American Journal of Clinical Oncology, 35(4), 373–377. Retrieved from http://journals.lww.com/amjclinicaloncology/Abstract/2012/08000/Wait_Times_in_Diagnostic_Evaluation_and_Treatment.13.aspx
Williams, C. 2005. The Sandwich Generation. Canadian Social Trends. Statistics Canada — Catalogue No. 11-008. Retrieved from http://www.statcan.gc.ca/pub/11-008-x/2005001/article/7033-eng.pdf
Witz, C. B. 1992. Professions and patriarchy. London: Routledge.
Wright, T. 2013. Currie challenges accuracy of the latest CIHI report. The Guardian. Retrieved from: http://www.theguardian.pe.ca/News/Local/2013-01-25/article-3164317/Currie-challenges-accuracy-of-the-latest-CIHI-report/1
59
REF
EREN
CES