what’s the deal with the pain score? - infinityrehab.com€™s-the-deal-with-pain.pdf ·...
TRANSCRIPT

What’s the deal with Pain?
Useful Pain Management in
the post-acute setting.
Mary Kofstad, APRN, MSN, FNP-BC
Vice President Clinical Operations Signature Home Health, Hospice &
NP2U

Objectives
Review pathophysiology, mechanism of action and
classifications of pain.
Discuss pharmacologic and non- pharmacologic
interventions.
Describe multimodal pain management including
evidence based tools and assessments for use in the
post-acute setting.
Case Study: you are consulted for
pain management
43 year old male status post lumbar discectomy
On Dilaudid, Fentanyl, Soma & Ativan
Not ambulating
Skipping therapy- has PT & OT
Describes pain with ambulation- shooting down left leg some foot drop bilateral leg weakness
Has been on chronic opioids for 18 months
Vital signs stable, no new or worsening complaints or symptoms.
CLINICAL QUESTIONS:
What can we do to get him moving with therapy?
Non-medication strategies?
What more do you want to know about assessment and history?

Case Study # 2 Consulted for pain
management 86 year old female C6 fracture- quadriplegic after fall
Pain in neck and shoulders, describes as shooting, aching.
Participating in Therapy, PT, OT, Speech
Has been inpatient rehab for 4 weeks
Has Tylenol ordered, takes BID, has morphine not using nurse told her “it
effects your breathing.”
Interested in stopping therapy
CLINICAL QUESTIONS:
What non medication therapies could we consider?
What other issues may be effecting decision making?
What other information and history do you need on this case?

Definitions of Pain:
An unpleasant sensory and emotional experience
associated with actual or potential tissue damage or
described in terms of such damage
IASP 1979
Whatever the experiencing person says it is existing
whenever he says it does
Margo McCaffery
1968

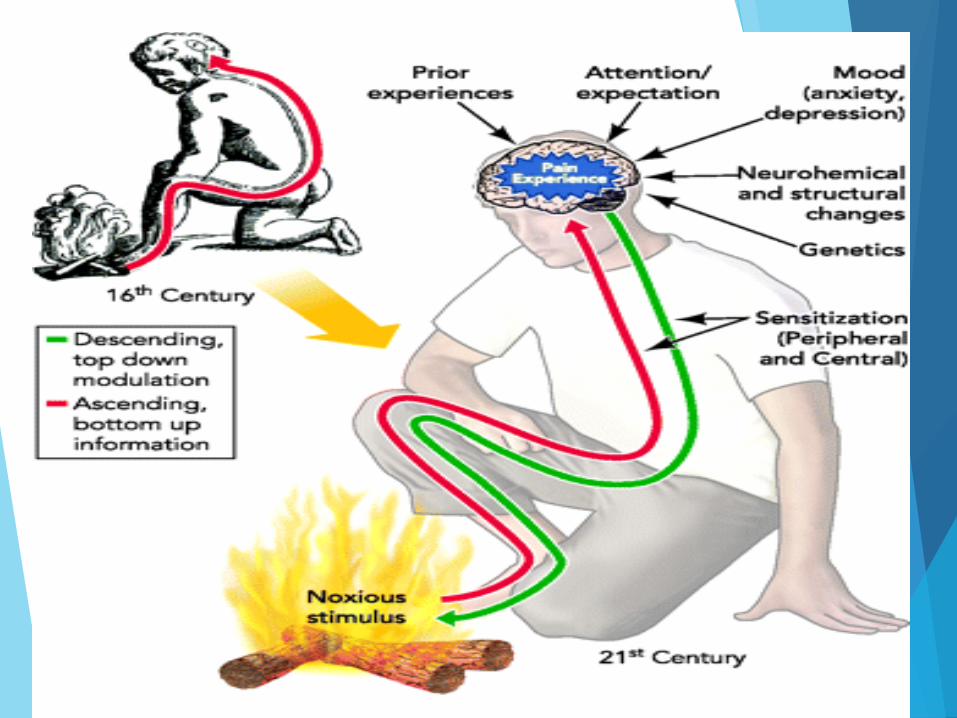
Pathophysiology of Pain:
Mechanism of Action
Nociception
-perception of pain
Nociceptors
-bare nerve endings in skin, muscle, joints, arteries, and the
viscera that respond to chemical, mechanical, and thermal
stimuli
-detect a wide range of stimuli

Pathophysiology of Pain:

Transduction of Pain
• Noxious Stimuli
– Mechanical
– Thermal
– Chemical
• Peripheral Soup
– Histamine - Antihistamines
– Substance P - Capsaicin
– Prostaglandins – Corticosteroids,
– NSAIDS
– Bradykinin
– Serotonin

Pain Classifications: ACUTE
The normal, predicted physiological response to an adverse chemical,
thermal or mechanical stimulus…
SURGERY
INFECTION
BURN
TRAUMA
ACUTE ILLNESS
TIME: Less than 1 month but can be longer than 6 months
Initiation phase: persistent nociceptive and behavioral cascade triggered by
tissue injury
This cascade has the potential to rapidly evolve into chronic pain
Acute Pain Classifications :
SOMATIC
Well localized
Aching, throbbing, gnawing
Activation of nociceptors in cutaneous
and deep tissues
Bone mets, soft tissue injuries
Acute Pain Classifications:
VISCERAL
Poorly localized
Deep aching, cramping,
pressure, referred
Activation of nociceptors
resulting from stretch,
distention or inflammation
Bowel obstruction, biliary
colic

CHRONIC PAIN
Purposeless, cyclical. Irreversible
Persists> 3-6 months
Vegetative, depressive signs
Autonomic adaption
Tissue damage may not be evident
Unpredictable

Scope of the Chronic Pain Problem
IN 2011
Chronic pain conditions affect approximately 10 million U.S. adults
Cost $560 - $635 billion annually or about $2,000 for every person living in the U.S.
Direct treatment costs $261-300 billion
Loss of productivity $297-336 billion
Medicare bears ¼ of the costs for pain or 14% of all Medicare costs
IN 2016
100 Million Americans live with Chronic Pain
IOM, 2011
Opioids: American Epidemic
OPIOIDS: 55 billion
in health and social
costs
20 billion in ED visits
78 people a day die
from an opioid
related overdose

Acute on Chronic Pain
Acute exacerbation of chronic pain condition
Preoperative assessment & formulated perioperative plan is essential.
Physical dependence means that a postoperative baseline opioid requirement is necessary to prevent withdrawal.
Postoperative opioid requirements may be more or less than preoperative levels, depending on the effect of surgery.

Consequences of Uncontrolled Pain
Delays healing
Noxious stimuli
can lead to enhanced sensitivity to subsequent noxious stimuli
(hyperalgesia)
can sensitize the pathway of previously nonpainful stimuli
(allodynia)
enhance the response of the spinal neurons
Overall result is sensitization of the central nervous system also
known as “windup”
Mayer et al., 2015; Belfer, 2013

Why So Much Pain?
AGING
Cancer
Traumatic Injury
Autoimmune
Disease
RA
Lupus
Scleroderma
MS
Fibromyalgia
Chronic Disease
Diabetes
Osteoarthritis
Obesity
HIV
Headaches
Muscle tension
Migraine
Cluster
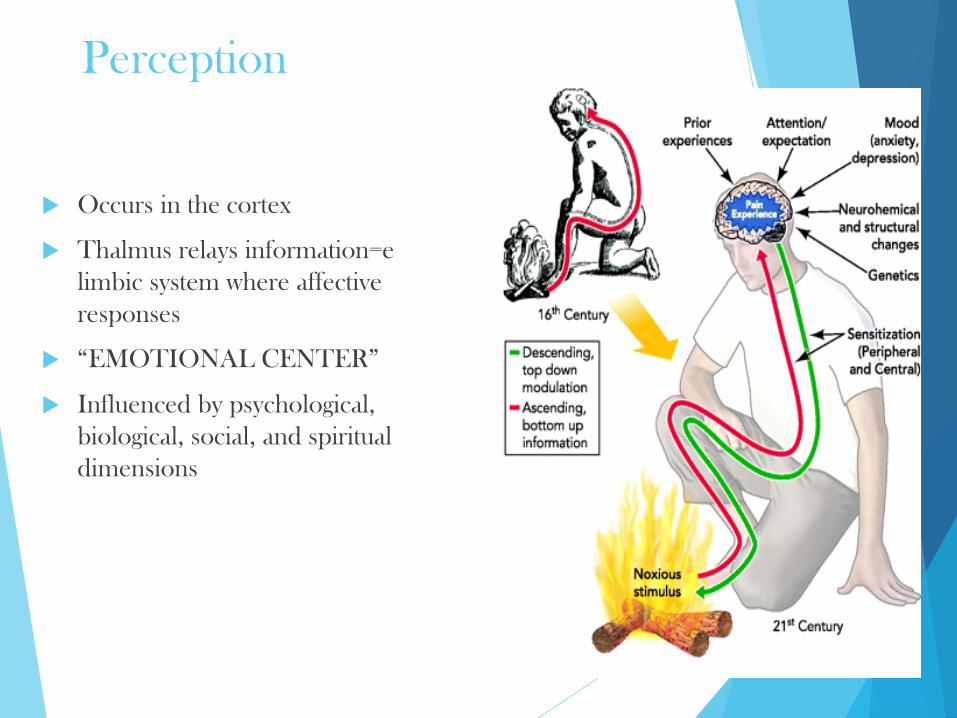
Perception
Occurs in the cortex
Thalmus relays information=e
limbic system where affective
responses
“EMOTIONAL CENTER”
Influenced by psychological,
biological, social, and spiritual
dimensions

The Brain Shows Pain
Neurologic brain
signature for pain
Standard map can be
employed for patients
experiencing pain
Yellow areas predictive
of higher levels of pain
Blue areas predict lower
levels of pain
NEJM, 2013.

Individual Response to Pain: Biology
Extent of illness or injury
whether the person has other
illnesses, is under stress,
specific genes
Predisposing factors that
affect pain:
TOLERANCE
THRESHOLDS

Individual Response to Pain: Psychological
Anxiety,
Fear,
Guilt,
Anger,
Depression,
Thinking pain represents
something worse helpless
to manage.

Individual Response to Pain: Social
Response of significant other
or family
Support, criticism, enabling
behavior or
Withdrawal—the demands of
the work environment,
Access to medical care,
culture family attitudes &
beliefs.
Stress

Comprehensive Assessment of Pain
Location
Duration
Intensity
Quality
Timing
Aggravating and alleviating factors
Nonverbal cues
Objective findings: changes in
Pulse, BP, Gait
Other symptoms
Current therapies
Prior treatment and response
Functional changes
Risk of substance abuse
Risk of diversion
NCCN Guidelines, 2012
4 A’s
• Analgesia
• ADLs
• Adverse Events
• Aberrant
Behaviors

Pain Assessment tools
One-dimensional
Verbal descriptor scale (VDS)
Numerical rating scale (NRS)
Visual analog scale (VAS)
Multidimensional
McGill Pain Questionnaire (MPQ)
Brief Pain Inventory (BPI)
Neuropathic Pain Questionnaire (NPQ)

Points for clarification
Rate your pain
Concerns about saying a high number-
Addresses a true barrier in pain management
Describe your pain- OUCH
This all comes down to:
COMMUNICATION
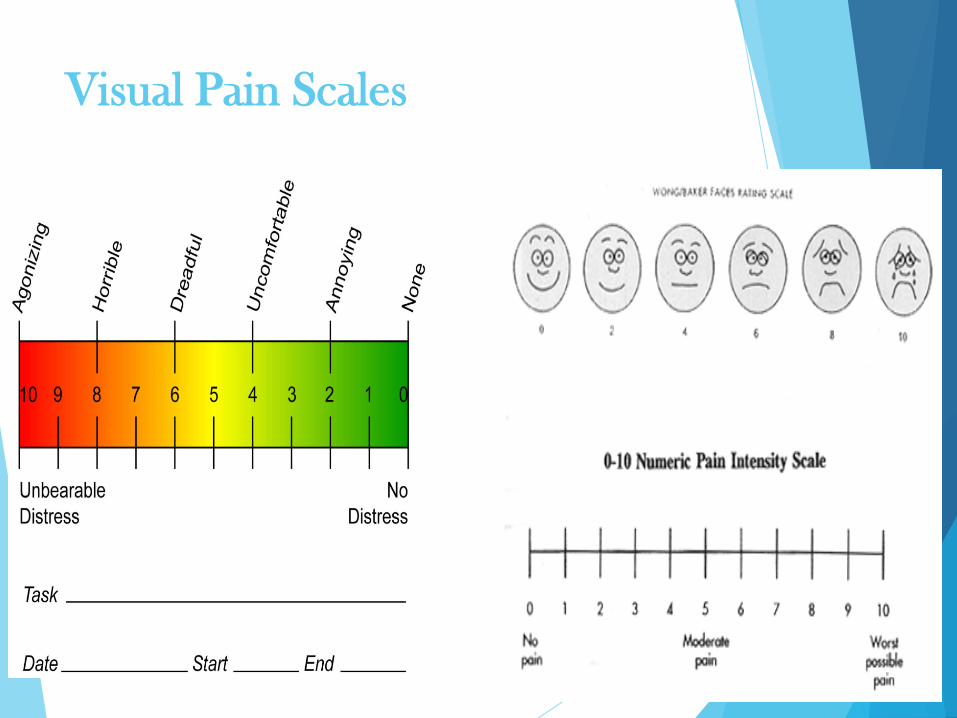
Visual Pain Scales

Pain Scales for Assessment:
CNPI-used for patients that are nonverbal
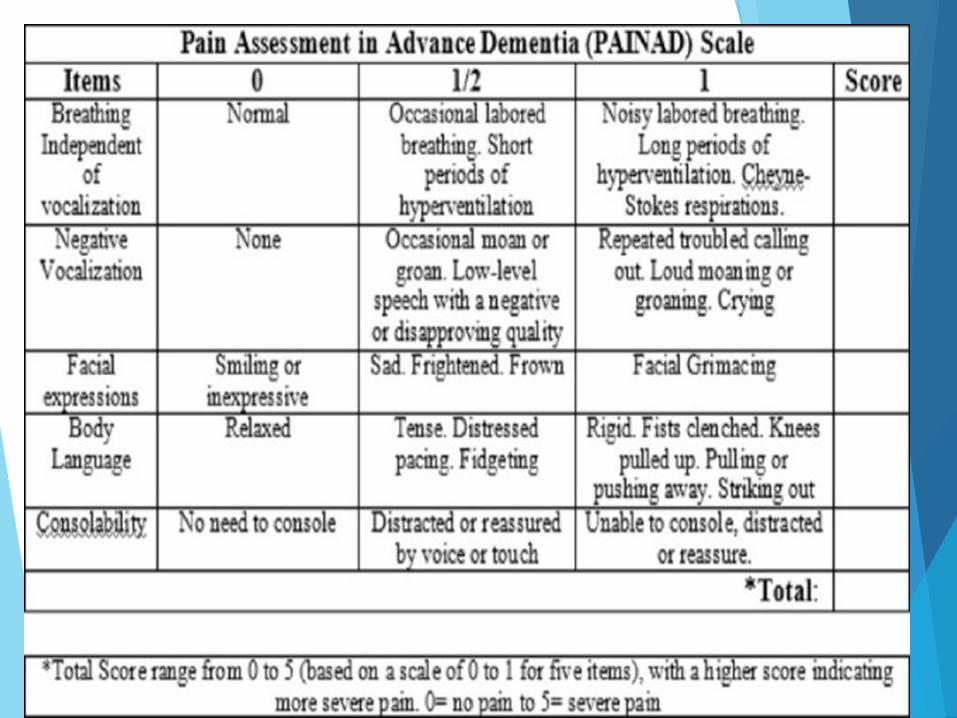
Pain Scales for Assessment:
PAINAD-used for advanced dementia or cognitive
impairment



Barriers to Pain Assessment:
PATIENT BARRIERS
Lack of knowledge about pain
and pain relief.
Cultural differences
Language barriers
Socioeconomic status
Physical and psychological
condition of patient
Age
COMMUNICATION- Health
literacy levels, diseases, age
Professional

BIAS/PROFESSIONAL BARRIERS
Lack of knowledge
Low priority
Values & beliefs
TIME
SYSTEM BARRIERS
Lack of systemic approach to pain
Lack of accountability


Points for clarification
Non verbal- hand in the
face
Not my patient
Timing
Emotions
Communication


Communication
Therapeutic communication, the sender, or nurse seeks to illicit a
response from the receiver, or patient that is beneficial to the patients
mental and physical health.
Some of the emotions associated with therapeutic communication
include but are not limited to the following: Professionalism,
Confidentiality, Courtesy, Trust, Availability, Empathy, and
Sympathy.
The process of learning is active , open and honest.
Promotes mutual understanding
RESPECT
Likely to influence human behavior

Factors influencing communication:
Perceptions
Values
Emotions
Socio-cultural background
Knowledge
Role and relationships
Environment
Gender

Physical dependence: body relies on a external
source to prevent withdrawal. Physical dependence is
predictable, easily managed with medication, and is
ultimately resolved with a slow taper off
Tolerance: body’s adaption over time to a substance
resulting in a decrease effects over time
Pseudoaddiction- under treatment of pain,
manifested by behaviors similar to addiction (clock
watching, focus on obtaining drug, aberrant
behaviors), behaviors resolve once the pain is
effectively managed
A Neurobiological Disease
ADDICTION
Involves the brain’s reward (limbic) center
An area of the brain that is associated with the affective responses
to pain
Involves dopamine
Susceptible individuals may have an alteration of the limbic or
related system that causes sensitization to the reinforcing effects of
drugs

Treatments


MEDICATIONS
Opioid Agonists
Codeine
Hydromorphone
Propoxyphene
Morphine
Oxycodone
Oxymorphone
Hydromorphone
Fentanyl
Methadone
NSAIDS NON- OPIOIDS
Aspirin
Acetaminophen
Ibuprofen (Advil®, Motrin, Nuprin)
Naproxen (Anaprox, Naprosyn)
Etodolac (Lodine)
Ketorolac (Toradol)
Nambumetone (Relafen)
Celecoxib (Celebrex)
Meloxicam (Mobic)

Treatment Tailored to Quality
Somatic
• Dull
• Aching
• Well-localized
Direct stimulation of nociceptors
• Bone metastases
• Arthritis
• Musculoskeletal pain
• Acetaminophen
• NSAIDS
• Opioids
Visceral
• Cramping
• Diffuse
• Poorly localized
Diffuse pain
• Bowel
• Lymphedema
• Ascites
• NSAIDS
• Corticosteroids
• Opioids
Neuropathic
• Burning
• Lancinating
• Shooting
Changes in the peripheral or
central nervous system
• Brachial plexopathy
• CIPN
• Opioids
• Antiepileptics
• Antidepressants
• Corticosteroids
• Local anesthetics
• NMDA antagonists

Multimodal Pain Therapy
Opioids, non opioids, NSAIDs, Regional anesthesia or Local peripheral nerve block,
ICE, HEAT, MASSAGE
POSITIVE EFFECTS: with different mechanisms of action
Improved pain relief with reduced side effects
DECREASES OPIOID USE(30%–50%)
Continuous coverage with LESS sedation
Improved patient outcomes: SHORTER LOS, REHAB; may allow earlier discharge
Potential drawbacks
Multimodal techniques can be technical and labor-intensive: TIME
Increased number of drugs increases the number of potential adverse effects

MULTIMODAL APPROACH
Avoid multiple drugs from same
class that have the same
mechanism of action: Maximize
treatment before abandoning
Use lowest effective dose or
intervention
Discontinue if intolerable side
effect or adverse effect or if
treatment is not helpful
PATIENT: Pharmacy, Therapy,
Physician, Nurse, Aide,
Chaplain= TEAM

Nonpharmacological Interventions:
NO PILLS
Strategies other than medications
Types of non pharmacologic interventions
Basic comfort measures
Cutaneous stimulation techniques
Cognitive and behavioral strategies

Rationale for Nonpharmacologic
Treatment of Pain
Pain is more than just a sensory
experience.
Pain has affective, cognitive,
behavioral, sociocultural and
spiritual dimensions.
Most pain is best treated with a
combination of pharmacologic
and nonpharmcologic strategies
MULTIMODAL PAIN
MANAGEMENT

Primary vs Adjunctive Treatment
Type of pain
Pain intensity
Duration
Patient preference

Additional Benefits of
Nonpharmacologic Interventions
Reduced anxiety
Improved mood
Increased sense of control
over pain
Improved sleep
Decreased fatigue
Improved function
Restored hope
Improved quality of life

Barriers to Nonpharmacological
Pain Management
Lack of knowledge
Belief that nonpharmacologic interventions are
not effective
Perceptions that patients won’t be receptive
Lack of time & equipment
Lack of support from colleagues, administrators

Basic Comfort Measures
Positioning
Environmental
conditions
Lighting
Noise
Temperature
Pacing activities / rest
Supportive devices

Cutaneous stimulation
Stimulation of the skin and underlying tissues
Locations:
Directly over or around pain
Proximal to the pain (between pain and the
brain)
Distal to pain (beyond the pain)
Contralateral to pain (opposite side)

Heat/Cold
HEAT: Vasodilation
Decreases sensitivity to pain,
releases muscle tension, and
provides a competing
sensory experience
Useful for muscle tension or
spasm, neck and back pain,
arthritis, postoperative pain
NOT FOR ACUTE PAIN
OR INJURY
COLD: Vasoconstriction
Decreases sensitivity to pain,
reduces muscle spasms, and
provides a competing sensory
experience.
Useful for muscle spasms,
back pain, arthritis, headache,
trauma and surgical incision
pain
Cold may be more effective
than heat

Vibration
Changes the quality of pain sensations (e.g., sharp to dull)
Useful for muscle pain, tension headache, phantom limb pain,
postoperative pain
High frequency (fine motion) vibrations more effective than low
frequency
Duration: Up to 30 minutes, 2- 3 times / day
Contraindicated
Thrombocytopenia
Thrombophlebitis / DVT
Burned, cut, or fragile skin

Massage
Rubbing, kneading,
tapping or manipulating
soft tissue
Produces physical and
mental relaxation,
improves circulation
and may reduce edema
Useful for low back
pain, cancer pain,
fibromyalgia, headache,
musculoskeletal pain,
post-exercise pain and
soreness
Traditional massage: gentle kneading
strokes
Site of pain, back, neck, scalp, hands,
feet
Duration: 5 minutes – 1 hour
Contraindications
Thrombocytopenia
Fragile skin
Superficial thrombophlebitis or
DVT
Acute inflammation or skin
infection
Superficial tumor sites

TENS
Skin stimulation through
mild electrical current
Various modes:
conventional, brief-intense,
strong low-rate
(acupuncture-like)
Electrodes placed directly
over or near the site of pain
or at an acupuncture point
Useful for musculoskeletal
pain, low back pain,
rheumatoid arthritis,
postoperative pain,
phantom limb pain, and
headache
Requires a physician’s order
Contraindications
On-demand pacemakers
Implanted electrical
devices
Reserved for moderate –
severe pain due to cost

Physical Exercise
Aerobic exercise, resistance training
ROM, passive exercise in debilitated patients
Useful for low back pain, osteoarthritis, neck pain,
general musculoskeletal pain
Supervised by trained professional
Practiced on a regular basis
Intensity, frequency, duration should be
individualized to avoid exacerbation of pain
Active lifestyle change

Cognitive and Behavioral Strategies
Change the way pain is interpreted and experienced
Modify thoughts that prevent coping with pain effectively
Divert attention away from pain
Increase personal sense of control over pain
Relaxation
Release of stress and tension
associated with pain
Decreased autonomic
nervous system activity
Useful for:
Pain caused by muscle
tension
Arthritis, procedural pain,
postoperative pain, cancer
pain
Cognitive and affective
components of pain

Relaxation Techniques
Jaw Relaxation
Rhythmic breathing
Heartbeat breathing
Progressive muscle relaxation
Stretch-based relaxation
Meditation
Prayer

Music therapy
Distracts attention from pain,
stimulates relaxation, or
changes attitude / mood
Useful for procedural pain,
postoperative pain, cancer
pain, arthritis pain
Use patient preference for
music selection
Encourage tapping out
rhythm, singing, dancing
Give patient control over
volume and length of
intervention

Imagery/Distraction
IMAGERY
Using one’s imagination to
create sensory images that
decrease pain
Distraction / Relaxation
Imagery (pleasant scene)
Pain-focused (image of pain
itself)
Useful for back pain,
postoperative pain, arthritis
pain, headache, cancer pain
DISTRACTION
Directing attention away from pain
Requires:
Mental capacity to concentrate
Physical ability / energy to engage in
distracting activities
Useful for brief pain episodes,
procedural pain
Awareness of pain may return when
distraction ends

Complementary / Alternative
Medicine
Energy Therapies
Therapeutic Touch
Reiki
Qi Gong
Magnet Therapy
Dietary supplements
Herbal therapy
Homeopathy
Aromatherapy
Accupuncture

Caregiver Fatigue: Don’t get there

# 1 Solution: Set realistic
Expectations
If Chronic Pain establish
baseline
Okay to take meds
Okay to medicate –
especially prior to exercise

Patient satisfaction

Patient’s are informed

Time Management

Side effects matter

Case Study: you are consulted for
pain management
43 year old male status post lumbar discectomy
On Dilaudid, Fentanyl, Soma & Ativan
Not ambulating
Skipping therapy- has PT & OT
Describes pain with ambulation- shooting down left leg some foot drop bilateral leg weakness
Has been on chronic opioids for 18 months
Vital signs stable, no new or worsening complaints or symptoms.
CLINICAL QUESTIONS:
What can we do to get him moving with therapy?
Non-opioid strategies?
What more do you want to know about assessment and history?

Case Study # 2 Consulted for pain
management 86 year old female C6 fracture- quadriplegic after fall
Pain in neck and shoulders, describes as shooting, aching.
Participating in Therapy, PT, OT, Speech
Has been inpatient rehab for 4 weeks
Has Tylenol ordered, takes BID, has morphine not using nurse told her “it
effects your breathing.”
Interested in stopping therapy
CLINICAL QUESTIONS:
What non medication therapies could we consider?
What other issues may be effecting decision making?
What other information and history do you need on this case?

Take Away
Pain is Subjective
Patient Perception and communication styles matter
Patient expectations critical to our overall assessments,
treatment & management
Multimodal therapy is the best way to treat
Lots of tools exist
Patient Preference for care and treatment MATTERS

Acute Pain: Symptom
Chronic Pain: Disease

TAKE AWAYS
Multimodal- not multi medications
ASSESS- RIGHT TOOL
EDUCATE- EXPECTATIONS: TEACH BACK
EmPathy
Proactive
Patience
PARTICIPATING- TheraPy, ADL’s
COMMUNICATE

Questions??