what’s new in hv and hv 2019 (and beyond) · • patients with base line resistance usually still...
TRANSCRIPT

1
What’s new in HCV and HBV 2019 (and beyond)
St Gallen 5/12/2019
Thanks to Jane Collier and Ellie Barnes
NIHR Biomedical Research Centre, Oxford MRC STOP-HCV programme
Wellcome Trust ….and all the patients
Shared issues in viral hepatitis
Virus persistence mechanisms Host immune mechanisms

2
HCV is not going away Messina et al Hepatology 2015 Data from 1200 papers since hep C was discovered.
• WHO data 2017: HCV Prevalence -approximately 75 million RNA +
• New infections fuel the global epidemic 1.7 million new infections in 2015
Changes in HCV prevalence 2016-17
Personal communication: data 2017-2018 also dismal
Hill AM J Virus Erad. 2017 Jul 1;3(3):117-123

3
Genotypes and sub-genotypes
• HCV has an error-prone RNA-dependent RNA polymerase.
• The mutation rate is very high: 2.5 mutations per genome replication1.
• There are 7 genotypes, G1 to G7, which differ by 30-35%2.
• Within these genotypes, there are 67+ subtypes that differ by up to 20%2.
1 Ribeiro et al, (2012). Quantifying the diversification of Hepatitis C Virus (HCV) during primary infection: estimates of the in vivo mutation rate. PLoS Pathogens doi: 10.1371/journal.ppat.1002881 2 Smith, Bukh, Kuiken, Muerhoff, Rice, Stapleton and Simmonds (2014). Expanded classification of hepatitis C virus into 7 genotypes and 67 subtypes: updated criteria and genotype assignment Web resource. Hepatology 59:318-327
G4
G3
G1
G6
G2 G7
G5
SNPs in the Interferon lambda 3 locus uncover a new cytokine - Interferon lambda 4
Laidlaw and Dustin, 2014

4
GWAS results: HLA and IFNL4 regions impact on the evolution of HCV
virus proteins
human chromosomes
IFNL3/4 MHC
Ansari et al Nat Genetics 2017

5
Acute disease
Usually
asymptomatic
Persistent
infection
>80%
Progressive
disease
mild disease
Resolved
infection
<20%
E. coli expression of influenza hemagglutinin DR1 tetramer HCV Clinical Course
T Cell Immunity vs HCV - the evidence
• HLA association studies and GWAS (Class I and Class II HLA
with clearance) (Neumann C, et al. Hepatology 2006;Duggal et al, Ann Int
Med 2013 )
• Chimpanzee CD4+ and CD8+ T cell depletion experiments (Shoukry N J Ex Med 2003)
• Association of breadth and magnitude of T cell response with
viral clearance (Lauer et al Gastro 2004)
• IFN- HCV specific CD8+ T cell responses are temporally
correlated with reduced viremia after infection (Lechner F J Exp Med
2000; Thimme et al J Exp Med 2001)
• Prophylactic vaccine data (Adeno/DNA) in a chimp challenge
model. (Folgori et al Nat med 2008)
• BUT…NO ONE CORRELATE OF PROTECTION
(BIG,BROAD,SUSTAINED, FUNCTIONAL etc)
6
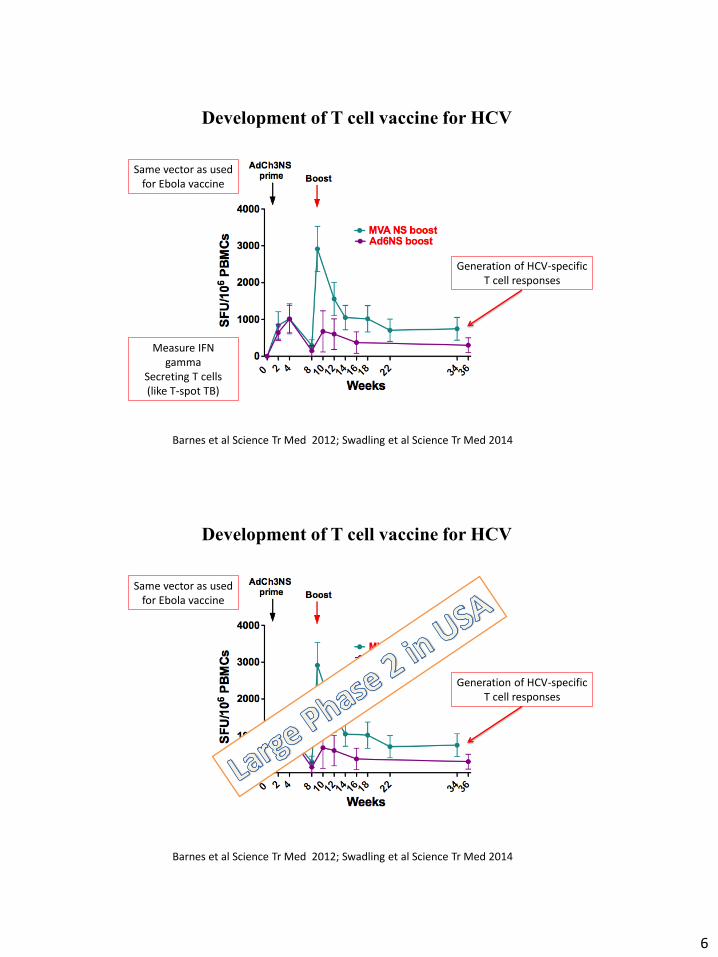
Development of T cell vaccine for HCV
Barnes et al Science Tr Med 2012; Swadling et al Science Tr Med 2014
Generation of HCV-specific T cell responses
Same vector as used for Ebola vaccine
Measure IFN gamma
Secreting T cells (like T-spot TB)
Development of T cell vaccine for HCV
Barnes et al Science Tr Med 2012; Swadling et al Science Tr Med 2014
Generation of HCV-specific T cell responses
Same vector as used for Ebola vaccine

7
No overall benefit seen from this vaccine…..
No overall benefit seen from this vaccine…..

8
Vaccine induces strong T cell help (like spontaneous clearance) but DAA therapy does not restore immunity
Hartnell et al in review 2019
Hepatitis C therapy pipeline 2013/14
Phase I
Phase II
Phase III
Phase IV
NS5A inhibitors
Protease inhibitors
ABT072
(Abbott)
ABT333
(Abbott)
MK3291
(Merck)
ACH-2684
(Achillon)
ACH-2928
(Achillon)
ACH-3102
(Achillon)
AZD-7295
(AstraZeneca)
IDX719
(Idenix) PPI-461
(Presidio) PPI-688
(Presidio)
ITX-5061
Entry Inhibitor
(iTherX) Telaprevir/VX-222
(Vertex)
ABT-450
(Abbott/Enanta)
ACH-1625
(Achillion) ALS-2200
(Alios/Vertex)
ANA598
(Anadys/Genentech)
BI 207127
(Boehringer)
BIT225
(Biotron)
BMS-650032
(BMS)
BMS-791325
(BMS)
Filibuvir
(Pfizer)
GS 9190
(Gilead)
GS-9256
(Gilead)
IDX184
(Idenix)
MK-5172
(Merck)
GS-938
(Gilead)
RG7128
(Gilead/Genentech) RG7227
(InterMune/Genentech)
Vaniprevir
(Merck)
VX-222
(Vertex)
VX-759
(Vertex)
Faldaprevir
(Boehringer)
asuneprevir
(BMS)
Sofosbuvir
(Gilead)
Simeprevir
(Medivir/Tibotec)
Boceprevir
(Merck) Telaprevir
(Vertex)
RG7128/RG7227
(Genentech)
GS-7977/TMC435
(Gilead/Tibotec)
GS-9256/GS-9190
(Gilead)
Boceprevir/Mericitabine
(Merck/Genentech)
BMS-790052/TMC435
(BMS/Tibotec)
BMS-790052/GS-7977
(BMS/Gilead)
BI 201335/BI 207127
(Boehringer)
ABT-450/ABT-333
(Abbot/Enanta)
ABT-450/ABT-267
(Abbot/Enanta)
ABT-450/ABT-072
(Abbot/Enanta)
ABT-450/ABT-267 and/or ABT-333
(Abbot/Enanta)
BMS-790052/BMS-650032
(BMS)
TMC435/TMC647055
(Medivir/Tibotec)
DAA combinations
Polymerase inhibitors

9
NS5A inhibitors Protease inhibitors Polymerase
inhibitors
Sofosbuvir
Ledipasvir
(Gilead)
GT1, 4, 5, 6
Sofosbuvir
Velpatisvir
(Gilead)
GT3
Granzoprevir/
Elbasvir/ (Merck)
GT1,4
Daclatasvir
Sofosbuvir
(BMS &Gilead)
GT1,3
Approved
Phase II
Phase III
The pipe line is “resolved”
Glecapravir
Pibrentasavir
(AbbVie)
Pan-GT
Sofosbuvir
Velpatisvir
Voxilaprevir
(Gilead)
Pan-GT
Pan-GT
SVR rates now 95%
Role of resistance testing • Role of resistance reported partially in phase-3 studies
• Patients with base line resistance usually still respond to therapy
– Q80T mutation in gt 1a infection linked to resistance to Simeprevir
• Resistance testing will be required in treatment failures
– whilst PI RAV revert to wild type, NS5A RAV persist for years….implications for retreatment strategies.
• So far little resistance reported in treatment failures in phase-III studies
– but in the real world difficult to treat, adherence and prescription mistakes, means potentially more likely…

10
HCV Genotype
3a
3b
3g
3i
Presence ofRAS
Non−RAS
RAS
A30
K
L31M
Y93
H
Daclatasvir Velpatasvir Elbasvir Pibrentasvir
A30
K +
L31
M
A30
K +
Y93
H
A30
K +
L31
M +
Y93
H
A30
K +
L31
M
A30
K +
Y93
H
A30
K +
L31
M +
Y93
H
A30
K +
L31
M
A30
K +
Y93
H
A30
K +
L31
M +
Y93
H
A30
K +
L31
M
A30
K +
Y93
H
A30
K +
L31
M +
Y93
H
100
102
104
106
108
1010
1012
Substitutions
Me
an
EC
50 F
old−
Ch
an
ge
(L
og
Sca
le)
Identified “rare subtypes” ? Resistant to new DAAs
Resistance analysis of genotype 3 hepatitis C virus
indicates subtypes inherently resistant to
nonstructural protein 5A inhibitors
Hepatology, Volume: 69, Issue: 5, Pages: 1861-1872,
First published: 09 February 2018, DOI: (10.1002/hep.29837)

11
Wei, L. et al. Sofosbuvir–velpatasvir for treatment of chronic hepatitis C virus infection in Asia: a single-arm, open-label, phase 3 trial. Lancet Gastroenterol. Hepatol. (2019)
Slides from AASLD 2018 : Safety and Efficacy of Sofosbuvir/Velpatasvir in Genotype 1-6 HCV-Infected Patients in China: Results From a Phase 3 Clinical Trial
Rare subtypes show drug resistance in real life
Retreatment options…if the drugs don’t work

12
Case 60yr old man – cirrhotic and complications
• 2009 – Hepatitis C antibody positive; HCV RNA negative
• 2012 – Hepatitis C RNA positive; genotype 3 – Still intermittent IVDU
• 2013 – Seen liver clinic – Panic attacks, anxiety, methadone 20mls, mirtazapine 30mg – Clinically cirrhotic (large spleen on ultrasound and low platelets) – Felt not tolerate interferon therapy
• 2015 – Seen in Drug and Alcohol Service by Community Hepatitis Nurse – Last injected heroin 6 weeks ago, anxiety. Hearing voices when used crack
cocaine, occ cannabis – No alcohol 6 months; previous 4-6 cans strong lager/day – Olanzapine. Methadone 30mg, mirtazapine – Clinically cirrhotic
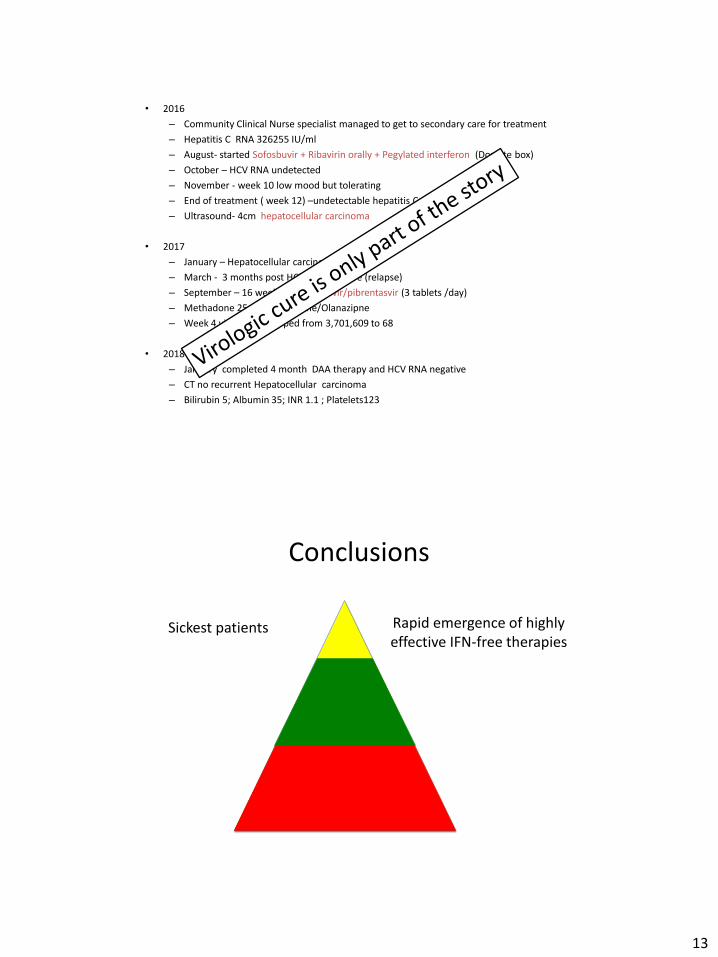
• 2016
– Community Clinical Nurse specialist managed to get to secondary care for treatment
– Hepatitis C RNA 326255 IU/ml
– August- started Sofosbuvir + Ribavirin orally + Pegylated interferon (Dosette box)
– October – HCV RNA undetected
– November - week 10 low mood but tolerating
– End of treatment ( week 12) –undetectable hepatitis C
– Ultrasound- 4cm hepatocellular carcinoma
• 2017
– January – Hepatocellular carcinoma resected
– March - 3 months post HCV RNA positive (relapse)
– September – 16 weeks of glecaprevir/pibrentasvir (3 tablets /day)
– Methadone 25mg/mirtazapine/Olanazipne
– Week 4 viral load dropped from 3,701,609 to 68
• 2018
– January completed 4 month DAA therapy and HCV RNA negative
– CT no recurrent Hepatocellular carcinoma
– Bilirubin 5; Albumin 35; INR 1.1 ; Platelets123
13
• 2016
– Community Clinical Nurse specialist managed to get to secondary care for treatment
– Hepatitis C RNA 326255 IU/ml
– August- started Sofosbuvir + Ribavirin orally + Pegylated interferon (Dosette box)
– October – HCV RNA undetected
– November - week 10 low mood but tolerating
– End of treatment ( week 12) –undetectable hepatitis C
– Ultrasound- 4cm hepatocellular carcinoma
• 2017
– January – Hepatocellular carcinoma resected
– March - 3 months post HCV RNA positive (relapse)
– September – 16 weeks of glecaprevir/pibrentasvir (3 tablets /day)
– Methadone 25mg/mirtazapine/Olanazipne
– Week 4 viral load dropped from 3,701,609 to 68
• 2018
– January completed 4 month DAA therapy and HCV RNA negative
– CT no recurrent Hepatocellular carcinoma
– Bilirubin 5; Albumin 35; INR 1.1 ; Platelets123
Conclusions
Rapid emergence of highly effective IFN-free therapies
Sickest patients

14
Conclusions
Rapid emergence of highly effective IFN-free therapies
Sickest patients
Patients with less advanced fibrosis
General availability
Conclusions
Rapid emergence of highly effective IFN-free therapies
Sickest patients
Patients with less advanced fibrosis
Emerging availability
Undiagnosed Awaiting ascertainment

15
• 257 million people have chronic HBV infection (WHO report, April 2017) • In 2015, 887 000 deaths – mostly from complications (liver cirrhosis and HCC) • Endemic in Sub-Sharan Africa and East Asia
Chronic HBV
Chronic HBV infection – cccDNA (Persistently infected Hepatocytes)

16
Chronic HBV – Exhaustion of HBV specific T-cell
Reference: T cell exhaustion. E John Wherry. Nature Immunology 12, 492–499 (2011) doi:10.1038/ni.2035
Nucleoside/nucleotide analogues in the treatment of chronic hepatitis B

17
Strategies to overcome chronic HBV infection
• Direct Chronic HBV infection
1. Entry inhibitors
2. cccDNA
3. siRNA – targetting viral transcripts
4. Capsid assembly modulators
5. Inhibitors of HBs release
• Restoration of Immune response
Restore Innate immunity
1. TLR agonists
2. Specific antiviral cytokine delivery
Restore Adaptive immunity
1. Therapeutic vaccines
2. Inhibitors of negative checkpoint modulators
3. Autologous transfer of engineered HBV-specific T cells
1
2
3 4
5
Aims of Immunotherapy
Vaccines (multiple antigens)
Immuno-modulators
Immunotherapy
Reference: PD-1/PD-L1 pathway and T-cell exhaustion in chronic hepatitis virus infection. Journal of Viral Hepatitis, 2010, 17, 453–458. T. Watanabe, A. Bertoletti & T. A. Tanoto.
Overcome the inhibitory mechanisms impairing the T cell function

18
Awaiting progress…
Shared issues in viral hepatitis
Virus persistence mechanisms Host immune mechanisms
Antivirals
C

19
Shared issues in viral hepatitis
Virus persistence mechanisms Host immune mechanisms
Antivirals
B
RT Other targets