what nephrologists need to know about gadolinium
TRANSCRIPT

reviewwww.nature.com/clinicalpractice/neph
review
What nephrologists need to know about gadoliniumJeffrey G Penfield* and Robert F Reilly Jr
Continuing Medical Education onlineMedscape, LLC is pleased to provide online continuing medical education (CME) for this journal article, allowing clinicians the opportunity to earn CME credit. Medscape, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide CME for physicians. Medscape, LLC designates this educational activity for a maximum of 1.0 AMA PRA Category 1 CreditsTM. Physicians should only claim credit commensurate with the extent of their participation in the activity. All other clinicians completing this activity will be issued a certificate of participation. To receive credit, please go to http://www.medscape.com/cme/ncp and complete the post-test.
Learning objectivesUpon completion of this activity, participants should be able to: 1 Describe the metabolism and properties of gadolinium.2 Identify the connection between gadolinium and
renal disease and its mechanism.3 Specify laboratory abnormalities associated with
the use of gadolinium.4 Describe the clinical presentation and treatment of
nephrogenic systemic fibrosis.5 List recommendations for the use of gadolinium.
IntroduCtIonMRI has become an essential part of current medical practice on the basis of the high quality of the images the method is able to produce. Vascular enhancement with a gadolinium-based contrast agent further improves the results of MRI. Clinical trials and extensive clinical experi-ence have proven that gadolinium-based contrast agents are safe in patients with normal kidney function. As renal function deteriorates, however, the safety of these agents diminishes. Nephrogenic systemic fibrosis (NSF) is associated with gado-linium chelates and occurs exclusively in patients with decreased renal function. The nephrotoxicity of these agents also becomes more pronounced as renal function declines. Derangement of labora-tory measurements as a result of administration of gadolinium chelates is observed in patients with normal renal function, but the effect is greater and its duration longer in patients with renal insuf-ficiency. This Review discusses the adverse effects of gadolinium-based contrast agents in patients with decreased renal function.
Gadolinium chelates are commonly used to improve tissue contrast in MRI. Until recently the use of gadolinium was thought to be risk-free compared with alternative contrast agents. Recent studies, however, have raised serious concerns regarding the safety of gadolinium chelates. Although safe in patients with normal kidney function, administration of these agents in people with renal dysfunction can result in up to three clinical problems that the nephrologist should be familiar with. The first is nephrogenic systemic fibrosis (NSF), which was initially observed in 1997. Although manifesting primarily in skin, NSF can also cause systemic fibrosis, leading to disabling contractures and even death. Gadodiamide is the agent that has been most frequently associated with NSF, but other chelates might also pose a risk. The second clinical problem is that gadolinium chelates cause acute kidney injury, especially at high doses required for angiography. The third problem is that several laboratory artifacts are associated with gadolinium administration, with pseudohypocalcemia being the most important. The risk of a patient experiencing all three of these complications increases as renal function declines. In light of these problems, nephrologists need to re-evaluate the risks and benefits of gadolinium administration in patients with chronic kidney disease stage 3 or greater, as well as in those with acute kidney injury. keywords contrast-induced nephropathy, gadolinium, nephrogenic fibrosing dermopathy, nephrogenic systemic fibrosis, pseudohypocalcemia
JG Penfield is Staff Physician in the Section of Nephrology at Veterans Affairs North Texas Health Care System and Assistant Professor of Medicine in the Department of Medicine, The University of Texas Southwestern Medical Center. RF Reilly Jr is Acting Chairman of the Department of Medicine and Chief of the Section of Nephrology, at Veterans Affairs North Texas Health Care System, as well as Fredric L Coe Professor of Nephrolithiasis Research in Mineral Metabolism at the Department of Medicine, The University of Texas Southwestern Medical Center, Dallas, TX, USA.
Correspondence *Veterans Affairs North Texas Health Care System, 4500 S Lancaster Road, Dallas, TX 75216, USA [email protected]
received 10 May 2007 Accepted 17 August 2007
www.nature.com/clinicalpracticedoi:10.1038/ncpneph0660
rEvIEw CrItErIAWe searched a variety of medical literature sources, including PubMed, MEDLINE, and nephrology and basic science journals, for information on gadolinium, mechanisms of gadolinium toxicity, nephrogenic fibrosing dermopathy, nephrogenic systemic fibrosis, and pseudohypocalcemia and other laboratory artifacts. Three hundred and eleven references published between 1962 and June 2007 were selectively reviewed.
SUMMArY
654 nAtUre clinicAl prActice NEPHROLOGY dEcEmbER 2007 vOL 3 NO 12
© 2007 Nature Publishing Group
review review
dEcEmbER 2007 vOL 3 NO 12 PENFIELd ANd REILLY nAtUre clinicAl prActice NEPHROLOGY 655
www.nature.com/clinicalpractice/neph
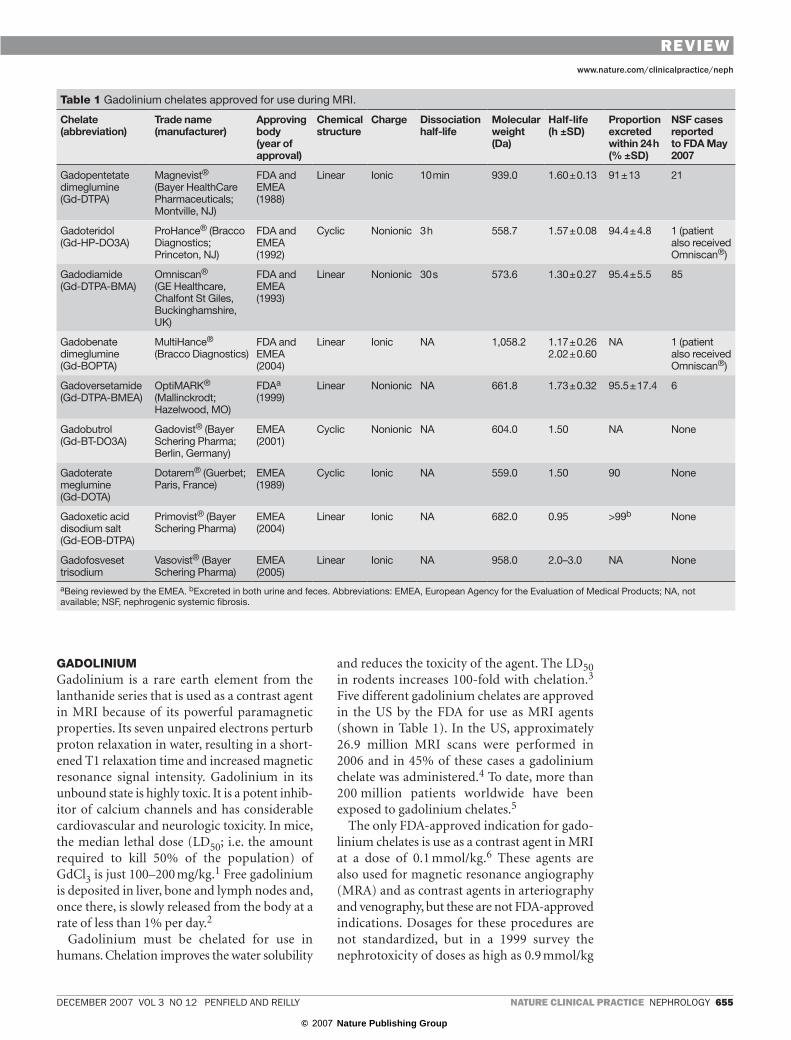
GAdoLInIuMGadolinium is a rare earth element from the lanthanide series that is used as a contrast agent in MRI because of its powerful paramagnetic properties. Its seven unpaired electrons perturb proton relaxation in water, resulting in a short-ened T1 relaxation time and increased magnetic resonance signal intensity. Gadolinium in its unbound state is highly toxic. It is a potent inhib-itor of calcium channels and has considerable cardiovascular and neurologic toxicity. In mice, the median lethal dose (LD50; i.e. the amount required to kill 50% of the population) of GdCl3 is just 100–200 mg/kg.1 Free gadolinium is deposited in liver, bone and lymph nodes and, once there, is slowly released from the body at a rate of less than 1% per day.2
Gadolinium must be chelated for use in humans. Chelation improves the water solubility
and reduces the toxicity of the agent. The LD50 in rodents increases 100-fold with chelation.3 Five different gadolinium chelates are approved in the US by the FDA for use as MRI agents (shown in Table 1). In the US, approximately 26.9 million MRI scans were performed in 2006 and in 45% of these cases a gadolinium chelate was administered.4 To date, more than 200 million patients worldwide have been exposed to gadolinium chelates.5
The only FDA-approved indication for gado-linium chelates is use as a contrast agent in MRI at a dose of 0.1 mmol/kg.6 These agents are also used for magnetic resonance angiography (MRA) and as contrast agents in arteriography and venography, but these are not FDA-approved indications. Dosages for these procedures are not standardized, but in a 1999 survey the nephrotoxicity of doses as high as 0.9 mmol/kg
table 1 Gadolinium chelates approved for use during MRI.
Chelate (abbreviation)
Trade name (manufacturer)
Approving body (year of approval)
Chemical structure
Charge dissociation half-life
Molecular weight (da)
Half-life (h ±sd)
Proportion excreted within 24 h (% ±sd)
NsF cases reportedto FdA May 2007
Gadopentetate dimeglumine (Gd-DTPA)
Magnevist® (Bayer HealthCare Pharmaceuticals; Montville, NJ)
FDA and EMEA (1988)
Linear Ionic 10 min 939.0 1.60 ± 0.13 91 ± 13 21
Gadoteridol (Gd-HP-DO3A)
ProHance® (Bracco Diagnostics; Princeton, NJ)
FDA and EMEA (1992)
Cyclic Nonionic 3 h 558.7 1.57 ± 0.08 94.4 ± 4.8 1 (patient also received Omniscan®)
Gadodiamide (Gd-DTPA-BMA)
Omniscan® (GE Healthcare, Chalfont St Giles, Buckinghamshire, UK)
FDA and EMEA (1993)
Linear Nonionic 30 s 573.6 1.30 ± 0.27 95.4 ± 5.5 85
Gadobenate dimeglumine (Gd-BOPTA)
MultiHance® (Bracco Diagnostics)
FDA and EMEA (2004)
Linear Ionic NA 1,058.2 1.17 ± 0.262.02 ± 0.60
NA 1 (patient also received Omniscan®)
Gadoversetamide (Gd-DTPA-BMEA)
OptiMARK® (Mallinckrodt; Hazelwood, MO)
FDAa
(1999)Linear Nonionic NA 661.8 1.73 ± 0.32 95.5 ± 17.4 6
Gadobutrol (Gd-BT-DO3A)
Gadovist® (Bayer Schering Pharma; Berlin, Germany)
EMEA (2001)
Cyclic Nonionic NA 604.0 1.50 NA None
Gadoterate meglumine (Gd-DOTA)
Dotarem® (Guerbet; Paris, France)
EMEA (1989)
Cyclic Ionic NA 559.0 1.50 90 None
Gadoxetic acid disodium salt (Gd-EOB-DTPA)
Primovist® (Bayer Schering Pharma)
EMEA (2004)
Linear Ionic NA 682.0 0.95 >99b None
Gadofosveset trisodium
Vasovist® (Bayer Schering Pharma)
EMEA (2005)
Linear Ionic NA 958.0 2.0–3.0 NA None
aBeing reviewed by the EMEA. bExcreted in both urine and feces. Abbreviations: EMEA, European Agency for the Evaluation of Medical Products; NA, not available; NSF, nephrogenic systemic fibrosis.
© 2007 Nature Publishing Group

review
656 nAtUre clinicAl prActice NEPHROLOGY PENFIELd ANd REILLY dEcEmbER 2007 vOL 3 NO 12
www.nature.com/clinicalpractice/neph
review
was not considered to be important by the majority of practitioners.7
The pharmacokinetic properties of most gado-linium chelates are similar. The compounds are water soluble, excreted unchanged by glomerular filtration, do not undergo biotransformation, and are distributed in extracellular fluid. Notable exceptions to these rules include gadoxetic acid (Primovist®; Bayer Schering Pharma, Berlin, Germany), gadofosveset trisodium (Vasovist®; Bayer Schering Pharma) and gadobenate dimeg-lumine (MultiHance®; Bracco Diagnostics, Princeton, NJ). Gadoxetic acid is taken up by hepatocytes; up to 50% of the agent is excreted in feces and 50% in urine. The chelate is used for enhanced imaging of the liver.8 Between 80–96% of circulating gadofosveset trisodium is bound to plasma proteins, and the compound has been used as a blood pool agent.9 Only a small proportion of circulating gadobenate dimeglumine is protein bound; it is taken up by hepatocytes and has a fecal excretion rate of 4%.10 Other gadolinium chelates are not bound by proteins or eliminated in feces. Molecular weights of the compounds range from 558 to 1,058 daltons. The half-life of gadolinium chelates in patients with normal renal function is approximately 1.5 hours, and more than 90% of a dose is excreted in 24 hours (Table 1).
The differences in the effects of various gadolinium preparations are attributable to gadolinium’s capacity to dissociate from chelates. The LD50s in rodents for various gadolinium chelates were found to vary up to 50-fold, but all were lethally toxic when the same amount of gadolinium was released from the chelate.11 Gadodiamide (Omniscan®; GE Healthcare, Chalfont St Giles, Buckinghamshire, UK) has the shortest dissocia-tion constant—30 seconds compared with 10 minutes and with 3 hours for gadopentetate dimeglumine (Magnevist®; Bayer HealthCare Pharmaceuticals, Montville, NJ) and gado-teridol (ProHance®, Bracco Diagnostics), respectively. The longer dissociation constant of gadoteridol is probably a function of its cyclic structure; most other gadolinium chelates have a linear structure. Release of gadolinium from a cyclic chelate requires all four cova-lent bonds to be broken simultaneously. The more flexible structure of linear chelates more readily facilitates gadolinium release. This fact might account for the higher incidence of NSF associated with gadodiamide and gadopentetate
dimeglumine. These two agents are the gado-linium preparations most frequently used in the US, which could account for a proportion of the increased incidence of NSF associated with these chelates. Market share alone does not, however, explain the disparity in the number of cases reported to be caused by these two agents.
The propensity of gadolinium chelates to undergo transmetalation might influence their toxicity. Transmetalation refers to the capacity of other cations in the body (e.g. zinc, copper and calcium) to displace gadolinium from its chelate.12 Copper has high affinity for the chelates, but is not present in the body at suffi-cient concentrations to displace large amounts of gadolinium. The concentration of calcium in serum is high, but the affinity of calcium for chelates is low. Zinc has moderate affinity and a sufficiently high serum concentration to displace gadolinium.11 In humans and experimental models, the extent of transmetalation can be evaluated in vivo as urinary zinc excretion. If gadolinium is displaced from its chelate by zinc, zinc binds the chelate and is subsequently excreted in urine. There are marked differences among the gadolinium chelates in the rates of short-term (within 3 hours) urinary zinc excretion after administration of 0.1 mmol/kg of chelate. Interestingly, these differences corre-spond to the kinetic stability of these agents. In a study in humans, urinary zinc excretion was highest with gadodiamide (27.4 μmol) and intermediate with gadopentetate dimeglumine (5.9 μmol), both of which are linear chelates.13 By contrast, in the same study, urinary zinc excretion was lowest with the cyclic chelate gadoteridol (1.2 μmol).
Similarly, in vitro studies have shown that linear chelates (i.e. gadodiamide, gadopentetate dimeglumine and gadobenate dimeglumine) are susceptible to transmetalation, but cyclic chelates (i.e. gadoteridol, gadobutrol [Gadovist®; Bayer Schering Pharma] and gadoterate meglumine [Dotarem®; Guerbet, Paris, France]) are resistant to this process.14
nEphrotoxICIty of GAdoLInIuM ChELAtEsMRI and/or MRA with gadolinium enhance-ment is often used instead of iodinated-contrast radiographic methods. MRI provides superior image quality to iodinated contrast methods, and methods that use iodinated contrast are
© 2007 Nature Publishing Group

review review
dEcEmbER 2007 vOL 3 NO 12 PENFIELd ANd REILLY nAtUre clinicAl prActice NEPHROLOGY 657
www.nature.com/clinicalpractice/neph
associated with a risk of acute kidney injury (AKI); for many years, gadolinium chelates were thought to be risk-free. Gadolinium is used in X-ray angiography in place of iodinated contrast, particularly in patients with chronic kidney disease (CKD). Early investigations reported that gadolinium chelates were not associated with AKI in patients with CKD (Table 2).15–24 The limitations of these reports include small sample size, lack of control groups, poor uniformity of pretreatment regimens, variable gadolinium doses and routes of administration, and different definitions of contrast-induced nephropathy (CIN). Higher than recommended doses of gadolinium chelates (>0.2 mmol/kg) were used in several of the studies. In response to these early reports and the desire to avoid CIN, gadolinium chelates were frequently used for standard venography and arteriography, and higher doses than those approved by the FDA were administered.
Subsequent reports (Table 3) detected an increased risk of AKI associated with gado-linium chelates in patients with CKD.25–28 These studies included more patients, one study was prospective, and the doses used were, on average, higher than those used in earlier series. There is at least one biopsy-documented case report of gadolinium-induced AKI; histological examination of the sample showed acute tubular necrosis, similar to that associated with CIN caused by iodinated contrast.29 One case report describes a patient with CKD who received iodinated contrast for coronary angiography but suffered no nephrotoxic effects.5 Three years later he developed AKI after receiving just 0.14 mmol/kg of gadodiamide for an MRA, indicating that gadolinium could be more nephrotoxic than iodinated contrast even at doses less than 0.2 mmol/kg.
It is not known whether the cause of nephro-toxicity associated with gadolinium chelates is the chelate itself or free gadolinium. As both gadolinium chelates and iodinated contrast cause acute tubular necrosis, it is reasonable to recommend avoiding high doses of gadolinium and maintaining adequate hydration in patients with CKD. In a 2000 position paper, the Contrast Media Safety Committee of the European Society of Urogenital Radiology recommended, on the basis of nephrotoxicity data, that gadolinium chelates should not be used in place of iodinated contrast media for radiographic examinations in patients with CKD.30
nEphroGEnIC systEMIC fIbrosIsNSF was first observed in 1997 and the initial case series published in 2000.31 The condition was originally known as ‘nephrogenic fibrosing dermopathy’ because it manifested primarily in skin. Later cases revealed more-diffuse involve-ment including subcutaneous tissue, striated muscle, the diaphragm and pleurae, the peri-cardium, and the myocardium. The name of the disorder was changed to NSF in 2005.32
Potential etiological agents for NSF remained elusive for many years, but the condition was known to occur exclusively in patients with decreased renal function.33 The association with gadolinium chelates was first described in January 2006 in an Austrian study by Grobner.34 Five of nine patients who received gadodiamide developed NSF within 2–4 weeks of exposure. These patients had metabolic acidosis whereas the four patients without NSF did not, but this association was not confirmed in later reports. In May 2006, the Danish Medicines Agency reported 25 cases of NSF that had occurred after gadodiamide exposure.35 Five of these cases had been reported previously by Grobner, and twenty were newly reported cases from Denmark. The FDA issued a black box warning in June 2006 that was updated in December 2006 and again in May 2007. The warning reiterated the association of gadolinium chelates with NSF.
Although there is good evidence that only three of the five FDA-approved gadolinium chelates are associated with NSF, the FDA warned that all gadolinium chelates had the potential to cause NSF. The FDA recommended that gadolinium chelates be used in patients with advanced kidney failure (i.e. those on dialysis or with an estimated glomerular filtration rate [GFR] <15 ml/min per 1.73 m2) only if absolutely necessary, and that it might be prudent to initiate hemodialysis promptly after gadolinium administration in these patients. This recommendation was formulated on the basis of studies by Okada and colleagues36 that showed gadolinium excretion rates of 78.2%, 95.6%, 98.7% and 99.5% in the first, second, third and fourth post-gadolinium dialysis sessions, respectively.
LInk bEtwEEn GAdoLInIuM And nEphroGEnIC systEMIC fIbrosIs Several groups have examined the potential link between gadolinium administration and NSF. Deo et al.37 studied a group of patients treated in a dialysis practice in Bridgeport, CT. Three cases of
© 2007 Nature Publishing Group

review
658 nAtUre clinicAl prActice NEPHROLOGY PENFIELd ANd REILLY dEcEmbER 2007 vOL 3 NO 12
www.nature.com/clinicalpractice/neph
review
table 2 Summary of the results of studies that showed that gadolinium did not cause acute kidney injury.
study design sample size (mean age)
Agent(s) used
dose used (mmol/kg)
renal status renal outcome Preventive treatment used
Rofsky et al. (1991)20
Workup of renal mass
5 (69 years) Magnevist® 0.1 Creatinine >2.0 mg/dl (range 2.2–6.0 mg/dl)
No increase in creatinine concentration
NA
Bellin et al. (1992)15
Prospective study of consecutive patients; intravenous gadolinium (n = 10) vs no contrast (n = 10)
20 Dotarem® 0.1 GFR (Cockroft–Gault) <60 ml/min (mean 21.1 ± 3.2 ml/min)
No >25% increase in creatinine concentration; creatinine concentration increased >10% in 5 controls and 3 gadolinium-exposed patients
None
Prince et al. (1996)18
Retrospective study of iodinated contrast vs gadolinium
64 Magnevist® (n = 21), Omniscan® (n = 37) or ProHance® (n = 6)
0.2–0.4 Creatinine >1.5 mg/dl
CIN (defined as ≥0.5 mg/dl increase in creatinine concentration) occurred in 29% (9 of 31 patients) exposed to iodinated contrast and 0% exposed to gadolinium
NA
Kaufman et al. (1999)17
Digital subtraction vena cavogram
14 (66.7 years)
Omniscan® or Magnevist®
≤0.4 Creatinine ≥1.5 mg/dl (mean 2.8 ± 1.1 mg/dl)
CIN (defined as ≥0.5 mg/dl increase in creatinine concentration at 48 h) did not occur; creatinine concentration of 3 patients increased as a result of causes other than gadolinium exposure
NA
Spinosa et al. (1999)23
Renal arteriogram
25 (59 years)
Omniscan® <0.3 Creatinine >1.5 mg/dl (mean 3.1 mg/dl)
CIN (defined as >0.5 mg/dl increase in creatinine concentration at 48 h) did not occur; creatinine concentration of 2 patients increased as a result of causes other than gadolinium exposure
Hydration
Hammer et al. (1999)16
Arterial digital subtraction angiography
34 (53.1 years)
Magnevist® 0.4 Creatinine >1.5 mg/dl
CIN (defined as >0.5 mg/dl increase in creatinine concentration) occurred in 3% (1 of 34 patients)
NA
Spinosa et al. (2000)22
Retrospective study of iodinated contrast and CO2 (n = 15), gadolinium and CO2 (n = 20) and CO2 alone (n = 7)
42 Omniscan® ≤ 0.4 Creatinine >1.5 mg/dl (mean 2.2 mg/dl, range 1.6–3.6 mg/dl)
CIN (defined as ≥0.5 mg/dl increase in creatinine concentration) occurred in 40% (6 of 15 patients) exposed to iodinated contrast and 5% (1 of 20 patients) exposed to gadolinium
300–500 ml normal saline before procedure
Townsend et al. (2000)24
Prospective study of gadolinium vs normal saline infusion only (no imaging performed)
32 Omniscan® 0.2 Creatinine clearance 20–29 ml/min (n = 9), 30–60 ml/min (n = 11)
CIN (defined as >0.5 mg/dl increase in creatinine concentration) did not occur
Normal saline after bolus
Sancak et al. (2002)21
Upper extremity or superior vena cava venography
16 (53 years)
Omniscan® 0.3 Mean creatinine 1.5 mg/dl (range 1.2–1.8 mg/dl)
Largest increase in creatinine concentration was 0.2 mg/dl
NA
Rieger et al. (2002)19
Prospective procedures (arterial and intravenous )
32 Magnevist® 0.34 ± 0.06 Creatinine >1.5 mg/dl (mean 3.6 ± 1.4 mg/dl)
CIN (defined as >0.5 mg/dl increase in creatinine concentration at 72 h) did not occur; creatinine concentration of 1 patient increased as a result of cholesterol emboli
Normal saline
To convert mg/dl to μmol/l, multiply by 88.4. Abbreviations: CIN, contrast-induced nephropathy; GFR, glomerular filtration rate; NA, not available.
© 2007 Nature Publishing Group

review review
dEcEmbER 2007 vOL 3 NO 12 PENFIELd ANd REILLY nAtUre clinicAl prActice NEPHROLOGY 659
www.nature.com/clinicalpractice/neph
NSF were identified during an 18 month period that ended 1 July 2006; two of these patients had received gadodiamide and one had received gado-pentetate dimeglumine. The incidence of NSF among all hemodialysis patients in this study was 4.3 cases per 1,000 patient years. The risk of devel-oping NSF was 2.4% per gadolinium exposure.37 In another study, 33 cases of NSF were reported in the St Louis, MO, area. Nineteen confirmed cases were evaluated in more detail in a case-controlled study.38 Four patients had been exposed to gado-linium more than 1 year before diagnosis of NSF and one individual had no known exposure. The remainder had received gadolinium within a year of diagnosis. Two patients had AKI and the remainder were chronic dialysis patients. In multivariate analysis, the only statistically
significant risk factor for NSF was gadolinium exposure within 12 months of diagnosis (odds ratio 8.97). The attack rate for peritoneal dialysis patients was 4.6 per 100 patients and was 0.61 per 100 for hemodialysis patients. The number of peritoneal dialysis patients in this study was small, but evidence from a study by Joffe et al. of poor clearance of gadolinium chelates during peritoneal dialysis supports this finding.39
Khurana and co-workers40 reviewed the case records of six patients who had developed NSF between 19 days and 2 months after gado-diamide exposure. One patient had AKI, one patient had AKI superimposed on advanced CKD, another was on hemodialysis, and three had stage 5 CKD but were not yet on dialysis. This report emphasizes that NSF occurs in
table 3 Summary of the results of studies that showed that gadolinium is nephrotoxic.
study design sample size
Agent(s) used dose used (mmol/kg)
renal status renal outcome Preventive treatment used
Sam et al. (2003)28
Retrospective, uncontrolled study of patients with CKD (January 1999 to January 2001)
195 Magnevist® (n = 195)
0.28 Creatinine clearance <80 ml/min (Cockroft–Gault); mean 38.2 ± 16 ml/min
CIN (defined as >1.0 mg/dl increase in creatinine concentration at 48 h plus oligoanuria) occurred in 3.5% (7 of 195 patients); 1.9% (3 of 153) of magnetic resonance angiography group and 9.5% (4 of 42) of digital subtraction angiography group were affected
NA
Erley et al. (2004)27
Prospective, randomized study
21 Gadovist® (n = 10) or iohexol (n = 11)
0.57 ± 0.17 Creatinine >1.5 mg/dl or GFR <50 ml/min
CIN (defined as >50% decrease in GFR) occurred in 50% (5 of 10 patients) exposed to gadolinium and 45% (5 of 11) exposed to iohexol
Intravenous hydration
Briguori (2006)25
Retrospective study of consecutive patients who had undergone coronary procedures, compared with historical controls
25 Omniscan® (n = 8) or Gadovist® (n = 17); three parts agent mixed with one part iodinated contrast vs iodinated contrast alone
0.6 ± 0.3 (range 0.28–1.23)
Creatinine >2 mg/dl or creatinine clearance <40 ml/min
CIN (defined as ≥0.5 mg/dl increase in creatinine concentration within 48 h or need for dialysis within 5 days) occurred in 28% (7 of 25 patients) exposed to gadolinium plus iodinated contrast and 6.5% (2 of 32) exposed to iodinated contrast only
Normal saline plus N-acetylcysteine
Ergun et al. (2006)26
Retrospective, uncontrolled study (February 1999 to March 2005); creatinine concentration measured before, and 1, 3, 7 and approximately 30 days after, exposure to gadolinium
91 Magnevist®, Omniscan® or Dotarem®
0.2 Stage 3 and 4 CKD; mean estimated GFR 33 ml/min (range 15–58 ml/min)
CIN (defined as ≥0.5 mg/dl increase in creatinine concentration within 72 h) occurred in 12% (11 of 91 patients)
NA
To convert mg/dl to μmol/l, multiply by 88.4. Abbreviations: CIN, contrast-induced nephropathy; CKD, chronic kidney disease; GFR, glomerular filtration rate; NA, not available.
© 2007 Nature Publishing Group

review
660 nAtUre clinicAl prActice NEPHROLOGY PENFIELd ANd REILLY dEcEmbER 2007 vOL 3 NO 12
www.nature.com/clinicalpractice/neph
review
patients with reduced renal function and is not confined to the dialysis population. In a study in Denmark, 13 people developed NSF between 2 and 75 days after exposure to gadodiamide.41 The odds ratio for exposure was 32.5 in these patients compared with patients with end-stage renal disease (ESRD) who had not been exposed. No association of NSF with acidosis was detected. The same authors reported no new cases of NSF at their institution since the use of gadodiamide was discontinued in March 2006.42 The total number of NSF cases related to gadodiamide that they have observed has now increased to 24. The extra cases are the result of delayed diagnosis of NSF that was caused by exposure to gadodiamide before its use was discontinued at their institution (P Marckmann, personal communication).
Broome et al.43 reported 12 patients who developed NSF after gadodiamide exposure. A total of 559 MRI exams were performed on 168 dialysis patients. The 12 patients who devel-oped NSF (301 gadodiamide exposures) were compared with those who were not exposed to gadodiamide (258 MRI exams). Four of the twelve patients were liver transplant recipients with AKI secondary to hepatorenal syndrome. The odds ratio for exposure to gadodiamide was again high, at 22.3, and the prevalence of NSF among gadodiamide-exposed dialysis patients was 4%. Patients receiving gadodiamide doses of 0.1 mmol/kg and those receiving doses of 0.2 mmol/kg were compared. The odds ratio for developing NSF for those on the higher dose was 12.1, indicating that the risk of developing the condition is dose dependent. Daily dialysis, starting on the day of gadolinium administration, for 3 days did not prevent NSF in three patients.
In another series, thirteen patients devel-oped NSF after being exposed to gadolinium; all received gadodiamide, and one was exposed to both gadobenate dimeglumine and gado-diamide.44 These patients were compared with a group of 4,236 individuals who received gado-linium but did not develop NSF. Affected patients had higher serum creatinine concentrations and had undergone a greater number of contrast-enhanced magnetic resonance exams than those who did not develop NSF. Those with NSF were also affected by more proinflammatory events (defined as surgery, thromboembolic vascular events, or systemic infections), emphasizing the potential contribution of inflammation to the development of NSF. This series of patients also
included two individuals with CKD stage 3 plus AKI. One was a liver transplant recipient, the other a renal transplant recipient. The authors empha-sized that AKI in the setting of a proinflammatory event could have contributed to the development of NSF in these two patients.
Marckmann et al.45 reviewed 19 cases of gadodiamide-induced NSF to identify potential cofactors. The primary risk factor for NSF was an increasing cumulative dose of gadodiamide. The investigators also observed a statistically signifi-cant correlation between NSF and elevated serum calcium and phosphorus concentrations, and between NSF and higher doses of epoetin beta. There was no correlation of NSF with acidosis, use of angiotensin-converting-enzyme (ACE) inhibitors, or serum parathyroid levels.
At least 96 reported cases of NSF have been associated with gadolinium-containing contrast media. The type of gadolinium chelate used was reported for 63 cases; all but one patient received gadodiamide (this individual received gadopentetate dimeglumine) and one patient received both gadodiamide and gadobenate dimeglumine. There are no published case reports linking gadoversetamide (OptiMARK®; Mallinckrodt, Hazelwood, MO) with NSF, although six cases have been reported to MedWatch, the FDA safety information and adverse event reporting program. MedWatch reports are generated by volunteer clinicians and are not peer-reviewed. As of 17 January 2007, 85 cases of NSF associated with gado-diamide, 21 cases associated with gadopentetate dimeglumine, and 6 cases associated with gado-versetamide, had been reported to the FDA. NSF has also been reported to develop after sequential administration of gadodiamide and gadobenate dimeglumine, as well as after sequential administration of gadodiamide and gadoteridol.6 Only two patients who devel-oped NSF without any known exposure to gadolinium are reported in the literature.38,46
tIssuE dEposItIon of GAdoLInIuMGadolinium can be deposited in the bone tissue of normal individuals. Deposition in bone was examined in patients with normal kidney function undergoing hip replacement after gadolinium-enhanced MRI.47 Gadolinium was administered 3–8 days before surgery and levels in operative bone fragments were measured. The concentration of gadolinium was four times higher (1.77 ppm) in patients who received
© 2007 Nature Publishing Group

review review
dEcEmbER 2007 vOL 3 NO 12 PENFIELd ANd REILLY nAtUre clinicAl prActice NEPHROLOGY 661
www.nature.com/clinicalpractice/neph
gadodiamide than in those who received gado-teridol (0.477 ppm). This difference was attributed to the increased stability of cyclic gadoteridol compared with linear gadodiamide.47,48
There are two published reports of gadolinium deposition being detected in skin affected by NSF. High et al. analyzed thirteen affected skin samples from seven patients.49 Gadolinium had been deposited in four of thirteen samples (four of the seven patients with NSF) at an average concentration of 70 ppm. A sample of uninvolved skin (with actinic keratosis) from a patient with NSF had a gadolinium concen-tration of only 5 ppm. In patients with detectable levels of gadolinium, a tissue residence time of 4–11 months was postulated on the basis of exposure history.49,50 There has been one report of a patient with NSF whose affected skin was examined using scanning electron microscopy and energy-dispersive X-ray spectroscopy.51 Interestingly, gadolinium was detected only in areas at which calcium phosphate had been deposited in blood vessels.
On the basis of the above findings, the proposed etiology for NSF is the deposition of free gadolinium in tissue, secondary to prolonged gadolinium clearance time in patients with decreased renal function. Once deposited in tissue, free gadolinium is not readily cleared by the kidney because of the poor water solubility of the agent. The most consistent improvement in NSF occurs in patients whose renal dysfunction reverses. Taken together, these findings indi-cate that gadolinium deposition alone cannot be the sole cause of NSF. The pathophysiologic interaction between gadolinium deposition and reduced GFR remains to be determined.
CLInICAL fEAturEs of nEphroGEnIC systEMIC fIbrosIsNSF has been reported to affect people across a broad range of ages (8–86 years). The condition has no gender predilection. In a study by Jain and co-workers, all patients affected with NSF had a decreased GFR; 90% were on dialysis as a result of ESRD or AKI.52 Seven patients were reported to have CKD stage 3 or 4, and a disproportionate number of these individuals were renal or liver transplant recipients. The GFR of these patients was estimated using serum creatinine measure-ments. The true GFR of both liver and renal transplant recipients is usually lower than the esti-mated GFR,53,54 so it is possible that these patients had more severe CKD than was reported.
Skin involvement in NSF is symmetrical, with extensive waxy thickening and hardening of the extremities and torso. Skin can become hyperpigmented and take on a ‘woody’ texture with plaques and subcutaneous nodules. Unlike scleromyxedema, NSF tends to spare the skin of the head and neck, and is not associated with paraproteinemia.31 A review of published cases by Mendoza et al. showed that skin of the lower extremities was affected in 97% of cases, and the distribution was from ankle to mid thigh.55 The upper extremities were involved in 77% of cases, most commonly from the wrist to mid upper arm. Truncal involvement was reported in 30% of cases,55 and there have been reports of yellow scleral plaques in the eye.56 Joint contrac-tures are a common result of progressive skin, as well as muscle and fascia, fibrosis, and lead to severe immobility.57,58 Progression is rapid in a subset of patients, who can become bed or wheelchair bound as a result of contractures.
There is an increased risk of thrombosis manifesting as deep venous thrombosis, a pulmonary embolus, thrombosed arterio-venous access, or an atrial thrombus, in patients with NSF. Elevated levels of antiphospholipid and anticardiolipin antibodies, deficiencies of protein C, protein S and antithrombin III, and presence of factor V Leiden, have all been observed in such patients.52,59–62 Patients with liver disease and those who have under-gone liver transplantation seem to be at increased risk of developing NSF. Originally thought to be confined to skin, it is now known that the fibrosis can be systemic and involve fascia, subcutaneous tissue, and other organs, including lungs, heart, muscle, kidneys, dura mater, and testes.63–66 In one case of NSF, progressive fibrosis of the diaphragm eventually led to death from respiratory failure.65
Examination of skin biopsy samples from patients with NSF reveals haphazardly-arranged thickened dermal collagen bundles interspersed with increased numbers of plump fibroblasts and mucin deposition.31,67 The skin of some patients harbors osteoclast-like giant cells with focal areas of calcification68 and ossification.69 The histology resembles that of a healing wound. Fibrocytes positive for CD34 and procollagen-1 are found in affected tissue. These fibrocytes originate in bone marrow and are drawn to the dermis by an unknown stimulus (possibly gadolinium deposition). After migrating to the dermis, the fibrocytes differentiate into cells
© 2007 Nature Publishing Group

review
662 nAtUre clinicAl prActice NEPHROLOGY PENFIELd ANd REILLY dEcEmbER 2007 vOL 3 NO 12
www.nature.com/clinicalpractice/neph
review
that resemble normal fibroblasts and could be responsible for the excessive fibrosis.64,70,71
trEAtMEnt of nEphroGEnIC systEMIC fIbrosIsTreatment of NSF is often unsuccessful. Most therapies have only been tested informally and the results published as case reports. NSF can improve with recovery of renal function after, for example, successful kidney transplantation or resolution of AKI. Published reports of treatments are often of limited value as they do not comment on the course of renal dysfunction. Disease regression must be interpreted in light of GFR; improve-ment of NSF in the setting of a rising GFR might result from reversal of the renal lesion and not from therapy for NSF per se. Ultraviolet A1 treat-ment was reported to be successful in one patient, but reversal of AKI might have been the true cause of improvement.72 Plasmapheresis was reportedly effective in another patient, but, again, improve-ment of renal function could have been the actual cause of recovery.67 Extracorporeal photo-pheresis was beneficial in three patients whose kidney function did not improve.57 Sodium thio-sulfate was reported to improve symptoms in a patient with ESRD on chronic hemodialysis.73 The mobility of one peritoneal dialysis patient partially improved after the first, but not subse-quent, courses of intravenous immunoglobulin.74 Physical therapy is recommended to prevent and treat joint contractures.
GAdoLInIuM CLEArAnCE And rEnAL dIsEAsEThe half-life and clearance of gadolinium chelates have been examined in patients with CKD or ESRD who are on hemodialysis or peritoneal dialysis.36,39,75–82 Swan et al.81 measured concen-trations of gadolinium in serum, urine and stool after a single dose of gadobenate dimeglumine (0.2 mmol/kg) in patients with varying degrees of renal function. In people with a normal GFR, the half-life of gadolinium was 1.96 hours. It increased to 6.11 ± 2.95 hours in those with a GFR of 31–60 ml/min per 1.73 m2 and to 9.48 ± 3.08 hours in those with a GFR of 10–30 ml/min per 1.73 m2. Other studies of the half-life of gadobenate dimeg-lumine and gadoversetamide in patients with CKD yielded similar results.79,80 In nine patients with stage 5 CKD (GFR 2–10 ml/min per 1.73 m2) who received a single dose of gadodiamide (0.1 mmol/kg), Joffe and co-workers found that the half-life of gadolinium was prolonged to 34.3 ± 22.9 hours.39
There have been several studies of gadolinium pharmacokinetics in hemodialysis patients; data from peritoneal dialysis patients are limited. Published reports have several limitations. For example, conclusions are often drawn on the basis of decay curves of serum gadolinium concen-tration. During formulation of these curves, it is assumed that gadolinium is removed from serum solely by dialysis. This might not be the case; sequestration of gadolinium in interstitial or intracellular compartments would be errone-ously interpreted as dialytic removal. Joffe et al.39 noted that the half-life of gadolinium (gado-diamide; 0.1 mmol/kg) during hemodialysis was 2.6 ± 0.4 hours when a low-flux biocompatible dialyzer was used for 4 hours three times per week. The authors reported that one hemodialysis session removed 65% of gadolinium; however, gadolinium levels in dialysate were not measured. Saitoh and colleagues78 reported a gadolinium half-life of 1.93 hours during hemodialysis in 13 patients dialyzed with a 1.5 m2 synthetic-polymer dialyzer at low dialysate flow rates (200 ml/min). Gadodiamide was the administered chelate (0.1 mmol/kg), and dialysis was carried out on days 1, 3, and 5 after exposure to gadolinium. The estimated proportion of gadolinium removed after each of these three dialysis sessions was 73.8%, 92.4%, and 98.9%, respectively; however, dialysate was only collected during the first hemodialysis session. Okada and co-workers36 studied 70 hemo-dialysis patients who received a 0.1 mmol/kg dose of gadopentetate dimeglumine, and estimated the proportions of gadolinium removed after four 4-hour dialysis sessions to be 72.8%, 95.6%, 98.7%, and 99.5%. Dialysate samples were not collected—percentage gadolinium removal was estimated on the basis of serum concentration decay curves. The first dialysis session occurred at variable intervals after gadolinium administration (same day in 16 patients, next day in 34 patients, 2 days later in 14 patients, and 3 days later in 6 patients). The type of dialyzer used in the study was not reported.
Data from the largest series of peritoneal dialysis patients who had received a gadolinium chelate were reported by Joffe et al.39 Nine patients underwent continuous ambulatory peritoneal dialysis with four exchanges per day. Dialysate was collected and gadolinium half-life was estimated to be 52.7 ± 6.2 hours. Only 69% of gadolinium had been removed after 22 days of peritoneal dialysis. In a case report of another peritoneal dialysis patient, who had received gadoversetamide (0.1 mmol/kg),
© 2007 Nature Publishing Group

review review
dEcEmbER 2007 vOL 3 NO 12 PENFIELd ANd REILLY nAtUre clinicAl prActice NEPHROLOGY 663
www.nature.com/clinicalpractice/neph
the gadolinium half-life was reported to be 9 hours.76 The patient, however, was producing 3 liters of residual urine per day. The rate of removal of gadolinium by peritoneal clearance was low in both studies, at 3.8 ± 0.6 ml/min and 5.13 ml/min, respectively.
We will not review in vitro studies in detail in this article, but some useful insights can be gained from them. First-order kinetic modeling showed that 12.2–14.7 hours of dialysis were required to remove 97% of an injected gado-linium dose.75 Gadolinium clearance during dialysis is more efficient when membranes with a large pore size are used,83 and nonionic gadolinium chelates are more easily removed via positively-charged dialysis membranes than ionic gadolinium chelates (see Table 1 for charge status of gadolinium chelates).77
LAborAtory AbnorMALItIEs AssoCIAtEd wIth GAdoLInIuMGadolinium chelates interfere with a wide variety of assays. The most widely reported laboratory artifact associated with gadolinium is pseudo-hypocalcemia.84–89 Gadolinium can also reduce ACE levels, alter serum iron concentration (reduce or elevate, depending on the assay), increase total iron-binding capacity, and lower serum zinc levels.89
Pseudohypocalcemia was first reported to be associated with gadolinium in 1995.90 It is most common for gadolinium to affect colorimetric assays that employ orthocresolphthalein (OCP), the agent most frequently used to measure calcium concentration. Pseudohypocalcemia does not occur when assays that employ atomic emission spectroscopy or ion-selective elec-trodes are used. Artifactual reduction of calcium concentration is thought to result either from binding of gadolinium to OCP, which prevents OCP from binding calcium, or from binding of calcium to the excess chelate that is included in some (but not all) gadolinium chelate prepara-tions. Gadodiamide has 0.025 mmol/ml of excess chelate and gadopentetate dimeglumine 0.001 mmol/ml; gadoterate meglumine contains no excess chelate. The purpose of including excess chelate in gadolinium preparations is to maintain gadolinium binding during storage.
In a study by Prince et al. of 896 patients whose serum calcium level was measured within 24 hours of gadodiamide administration, 165 developed pseudohypocalcemia.88 Calcium concentration declined by more than 0.5 mmol/l
(2 mg/dl) in 42 patients, and in 25 patients was less than 1.5 mmol/l (6 mg/dl). Oral or intravenous calcium was administered to 18 patients for what was mistakenly interpreted as ‘true’ hypocalcemia, even though the patients had no clinical symp-toms of the disorder. The pseudohypocalcemic effect persisted for up to 4.5 days in patients with CKD, and was more pronounced at high doses of gadodiamide. In patients with a normal GFR who had received low-dose gadodiamide, pseudo-hypocalcemia lasted 4–6 hours. In those whose GFR was reduced, the artifact persisted for more than 24 hours. Recommended minimum waiting times from administration of contrast medium to collection of plasma sample have been established for the Roche OCP assay (Hitachi 747 analyzer; Roche Diagnostics, Indianapolis, IN) on the basis of GFR (Table 4).91
Kang et al.91 also examined the effect of several different gadolinium chelates on in vitro calcium concentrations. Gadodiamide and gado-versetamide both reduced calcium levels, whereas gadoteridol and gadopentetate dimeglumine did not. Interestingly, both the gadolinium chelates that cause pseudohypocalcemia in vitro are packaged with higher concentrations of excess chelate—331 mg/ml for gadoversetamide and 12 mg/ml for gadodiamide versus 0.2 mg/ml for gadoteridol and 0.4 mg/ml for gadopentetate dimeglumine. This fact indicates that pseudohypocalcemia might be the result of calcium binding to excess infused chelate, rather than of dissociation of gadolinium from chelate in vivo.40
table 4 Recommended minimum waiting time from administration of contrast medium to collection of plasma sample for the measurement of calcium.
estimated glomerular filtration rate (ml/min per 1.73m2)
waiting time (h)
20 50
30 18
40 11
50 8
60 6
75 5
90 4
130 3
Permission obtained from the American Association for Clinical Chemistry © Kang HP et al. (2004) Clin Chem 50: 741–746.
© 2007 Nature Publishing Group

review
664 nAtUre clinicAl prActice NEPHROLOGY PENFIELd ANd REILLY dEcEmbER 2007 vOL 3 NO 12
www.nature.com/clinicalpractice/neph
review
The reduction in ACE levels observed after gadolinium administration is thought to result from binding of zinc by the chelate; measurement of ACE is zinc dependent. Iron concentration is increased by gadolinium when the Vitros® 950 (Ortho-Clinical Diagnostics, Raritan, NJ) and Synchron LX® 20 (Beckman Coulter, Brea, CA) assays are used.89 Likewise total iron-binding capacity is increased by gadolinium when either the Modular P or Dimension RxL (Roche Diagnostics, Indianapolis, IN, and Dade Behring, Deerfield, IL, respectively) methods are used to quantify this parameter. The formazan dye employed in the zinc assay probably binds gado-linium, resulting in a falsely low concentration of zinc being detected.
rECoMMEndAtIons for usE of GAdoLInIuMThe FDA,6 Danish Medicines Agency (DMA),35 United Kingdom Medicines and Healthcare products Regulatory Agency (MHRA),92 and American College of Radiology (ACR),93 among other organizations, have published recom-mendations regarding gadolinium use. Selected recommendations by these agencies have been chosen to frame our discussion of some of the more-controversial issues. The MHRA has submitted a public assessment report to the European Medicines Agency, but this statement does not represent the view of all member states. The DMA report is an independent Danish publication. The ACR recommendations were derived from a ‘blue ribbon’ panel and repre-sent consensus of ACR members; they have not, however, been adopted as policy by the ACR.94
The FDA is the only agency to suggest that all gadolinium chelates are potentially linked to NSF.6 The other three organizations mentioned above specifically implicate gadodiamide as being associated with the highest risk for NSF. This assertion is based on the fact that most cases of NSF are associated with this gado-linium preparation. The DMA and MHRA view gadodiamide as being contraindicated in patients with a GFR of less than 30 ml/min per 1.73 m2,35,92 whereas the ACR recommends avoiding gadodiamide in patients with any degree of renal dysfunction.93 Although the FDA does not state that any specific preparation is contra-indicated, it does recommend that physicians carefully consider the need for any gadolinium chelate in patients with moderate kidney dysfunction to ESRD. The ACR and MHRA regard
gadoversetamide and gadopentetate dimeglumine as being associated with an increased risk of NSF, but do not specifically recommend that these agents be avoided. As gadodiamide is the agent most often associated with NSF in reported cases, we agree with the ACR and Kuo et al.95 that use of this preparation be avoided in patients with any degree of renal dysfunction. It is also prudent to avoid using gadoversetamide and gadopentetate dimeglumine until more data regarding their risk become available. These agents are reported to cause NSF and, like gadodiamide, have a linear structure and short dissociation half-lives.
The MHRA report states that serum creatinine concentration should be measured before gado-linium administration.92 By contrast, the ACR recommends relying on information regarding kidney disease provided by the referring physi-cian or by the patient via a questionnaire.93 Given that even patients with advanced CKD are often unaware of their disease, we agree with the MHRA that a serum creatinine concentration should be obtained by the referring physician if a gadolinium chelate is to be administered. If a patient has any history of kidney disease, determination of serum creatinine level should be required by the radiology department within 30 days before the imaging procedure, or sooner if there is a clinical concern about recent deterioration in GFR (e.g. a preceding iodinated contrast study). We recognize that NSF is a rare occurrence in patients with stage 3 or 4 CKD, but we feel that this recommendation is justified given the serious consequences of the disorder.
The need for a gadolinium-based contrast study should be carefully considered in a patient with CKD stage 3 or greater and alternative imaging modalities should be considered. The lowest possible dose of gadolinium should be used because development of NSF might be dose related.43 The use of gadolinium in angiographic studies as an alternative to iodinated contrast should be carefully evaluated because the dose required is often high and recent studies indicate that gadolinium is nephrotoxic (see Table 3).
Other recommendations that are consistent with those in published literature and prudent to adopt are that standard gadolinium doses should not be exceeded and repeat doses should not be given in less than 1 week, that gadodiamide should be avoided in patients with renal dysfunction who have had or are about to undergo liver transplanta-tion, and that postponing the imaging study until renal function has recovered in patients with AKI should be considered.92
© 2007 Nature Publishing Group

review review
dEcEmbER 2007 vOL 3 NO 12 PENFIELd ANd REILLY nAtUre clinicAl prActice NEPHROLOGY 665
www.nature.com/clinicalpractice/neph
Perhaps the most controversial issue is the need for post-gadolinium hemodialysis; there is a marked difference of opinion on this topic among recom-mending bodies. The FDA originally stated that it might be prudent to promptly initiate hemodialysis after administration of gadolinium chelates to patients with advanced kidney dysfunction (stage 5 CKD or ESRD). The most recent FDA update (23 May 2007) recommended consideration of prompt post-gadolinium dialysis only in patients who were already on hemodialysis (the term “prompt” is not defined in the recom-mendation).6 The FDA also stated that it is not known whether hemodialysis prevents NSF. The ACR advocates hemodialysis within 2 hours of gadolinium administration in patients already on hemodialysis.93 There is, as yet, no evidence to support this recommendation. The MHRA does not consider hemodialysis to be indicated in such instances, due to a lack of evidence regarding its effi-cacy.92 The risks associated with post-gadolinium hemodialysis are minimal for stable ESRD patients with functioning accesses; as such, the FDA recom-mendation is reasonable. The MHRA correctly asserts, however, that there is no evidence that hemodialysis will prevent NSF. Data reported by Broome and co-workers for three patients who developed NSF despite three consecutive daily hemodialysis sessions clearly show that NSF can still develop despite aggressive dialysis.43 Assumptions about gadolinium removal from the body that are made on the basis of plasma concentration decay curves might lead to overestimation of the efficiency of gadolinium clearance by hemodialysis.
The risk of developing NSF after gadolinium exposure in patients with stage 3–5 CKD is unknown, but seems to be less than the 2.5–4.0% postulated for the ESRD population.37,43 NSF has developed in two patients with stage 3 CKD;44 one patient was a renal allograft recipient, the other a liver transplant recipient, and GFR was declining in both at the time of multiple exposures to gado-linium. It is probable that the true GFR of both patients was lower than that estimated using the Modification of Diet in Renal Disease equation.96 The FDA’s original warning in June 2006 and subsequent update in December of that year stated that patients with a GFR of less than 60 ml/min per 1.73 m2 were at risk of developing NSF after exposure to gadolinium. In the most recent update (23 May 2007), the GFR cutoff had been changed to less than 30 ml/min per 1.73 m2.6 Five patients with stage 4 CKD have developed NSF after gadolinium administration.43,44 All had been exposed to
gadolinium several times. One patient had under-gone renal transplantation, two had undergone liver transplantation, and two had advanced stage 4 CKD (estimated GFR 17–18 ml/min per 1.73 m2).
Taken together, these findings indicate that subgroups of patients with CKD stage 3 or 4 might be at increased risk of developing NSF after gado-linium administration. These subgroups include those exposed to gadolinium more than once, liver graft recipients, and patients for whom the Modification of Diet in Renal Disease equation might overestimate true GFR (e.g. organ trans-plant recipients and those with AKI superimposed on CKD). The risk of developing NSF increases as GFR declines through CKD stages 3, 4 and 5 to ESRD, with a very low risk in CKD stage 3 and a 2.5% risk per exposure for patients with ESRD. We agree with the MHRA that the evidence to date does not justify the risks that are associated with acute access placement and hemodialysis after gadolinium exposure. Every effort should be made to postpone any gadolinium-enhanced imaging procedures in patients with AKI. At our institution, gadoteridol was in use before the association between NSF and gadolinium chelates was recog-nized. We will continue to use gadoteridol in preference to other FDA-approved gadolinium chelates because patients receiving gadoteridol have the lowest reported incidence of NSF.
Decisions regarding the benefit of hemodialysis for gadolinium clearance are also difficult when managing peritoneal dialysis patients. Peritoneal dialysis seems to be an inefficient means of removing gadolinium. It should be pointed out, however, that this opinion is based on data derived from patients maintained on older chronic ambu-latory peritoneal dialysis regimens. Improved clearance might be possible with more-aggressive cycler-based regimens, and this possibility warrants further study. That said, data from the Morbidity and Mortality Weekly Report indicating that the incidence of NSF in gadolinium-exposed peritoneal dialysis patients is 7.5 times higher than that in hemodialysis patients is alarming.38 It seems prudent to avoid exposing peritoneal dialysis patients to gadolinium if possible, until the risk is further clarified. If gadolinium must be used, gadoteridol should be considered as the first choice of chelate. Initiating post-exposure hemo-dialysis should be considered, especially if the patient has a functioning access. Alternatively, the peritoneal dialysis prescription could be increased. It should be emphasized, however, that
© 2007 Nature Publishing Group

review
666 nAtUre clinicAl prActice NEPHROLOGY PENFIELd ANd REILLY dEcEmbER 2007 vOL 3 NO 12
www.nature.com/clinicalpractice/neph
review
these approaches might not prevent NSF and there are no data to support them.
ConCLusIonsOver time, the number of indications for, and doses of, gadolinium chelates have increased beyond those originally approved by the FDA. Although these increases have probably not compromised the safety of patients with normal renal function, for those with a reduced GFR the risk of devel-oping NSF is now a concern. A strong association between NSF and gadolinium-based agents has emerged from retrospective analyses. Gadolinium has been detected in affected tissue, but there is as yet no definitive proof that gadolinium is the cause of NSF. Treating an animal model such as a 5/6 nephrectomized rat with gadolinium chelates might provide some insight into causal relationships. Until more data become available, it is advisable to avoid using gadolinium chelates (particularly gadodiamide) whenever possible in people with severe kidney disease to ESRD. As gadolinium chelates can be nephrotoxic, their use should no longer be considered ‘safe’ in terms of CIN. If a gadolinium chelate is administered, the physician should be familiar with associated labora-tory artifacts so that unnecessary treatment is not initiated on the basis of erroneous values.
kEy poInts■ Originally thought to be safe contrast agents,
gadolinium chelates have recently been shown to be associated with the development of nephrogenic systemic fibrosis (NSF) in patients with impaired renal function
■ NSF, previously known as nephrogenic fibrosing dermopathy, occurs only in patients with kidney dysfunction, is characterized by waxy thickening of the skin of the extremities and torso, and commonly leads to joint contractures and immobility
■ The proposed, but not yet proven, etiology of NSF is tissue deposition of free gadolinium that is liberated from chelates, secondary to prolonged gadolinium clearance time due to impaired renal function
■ Treatments for NSF have only been tested informally; the condition has been shown to improve in response to recovery of kidney function
■ Several authorities have issued recommendations for use of gadolinium chelates; most advise caution when considering use of these agents in patients with renal dysfunction
references1 Caille JM et al. (1983) Gadolinium as a contrast agent
for NMR. AJNR Am J Neuroradiol 4: 1041–10422 Tweedle MF (1992) Physicochemical properties
of gadoteridol and other magnetic resonance contrast agents. Invest Radiol 27 (suppl 1): S2–S6
3 Bousquet JC et al. (1988) Gd-DOTA: characterization of a new paramagnetic complex. Radiology 166: 693–698
4 AuntMinnie.com (online 21 February 2007) IMV Report: MRI market growing. [http://www.auntminnie.com/index.asp?Sec=sup&Sub=bai&Pag=dis&ItemId=74472] (accessed 19 June 2007)
5 Thomsen HS (2004) Gadolinium-based contrast media may be nephrotoxic even at approved doses. Eur Radiol 14: 1654–1656
6 US Food and Drug Administration (online 23 May 2007) Healthcare professional sheet: gadolinium-containing contrast agents for magnetic resonance imaging (MRI) (marketed as Omniscan, OptiMARK, Magnevist, ProHance, and MultiHance). [http://www.fda.gov/cder/drug/InfoSheets/HCP/gccaHCP.htm] (accessed 19 June 2007)
7 Morcos SK et al. (1999) Contrast-media-induced nephrotoxicity: a consensus report. Contrast Media Safety Committee, European Society of Urogenital Radiology (ESUR). Eur Radiol 9: 1602–1613
8 Hamm B et al. (1995) Phase I clinical evaluation of Gd-EOB-DTPA as a hepatobiliary MR contrast agent: safety, pharmacokinetics, and MR imaging. Radiology 195: 785–792
9 Lauffer RB et al. (1998) MS-325: albumin-targeted contrast agent for MR angiography. Radiology 207: 529–538
10 Kirchin MA et al. (1998) Gadobenate dimeglumine (Gd-BOPTA): an overview. Invest Radiol 33: 798–809
11 Cacheris WP et al. (1990) The relationship between thermodynamics and the toxicity of gadolinium complexes. Magn Reson Imaging 8: 467–481
12 Idee JM et al. (2006) Clinical and biological consequences of transmetallation induced by contrast agents for magnetic resonance imaging: a review. Fundam Clin Pharmacol 20: 563–576
13 Puttagunta NR et al. (1996) Human in vivo comparative study of zinc and copper transmetallation after administration of magnetic resonance imaging contrast agents. Invest Radiol 31: 739–742
14 Laurent S et al. (2006) Comparative study of the physicochemical properties of six clinical low molecular weight gadolinium contrast agents. Contrast Media Mol Imaging 1: 128–137
15 Bellin MF et al. (1992) Gd-DOTA: evaluation of its renal tolerance in patients with chronic renal failure. Magn Reson Imaging 10: 115–118
16 Hammer FD et al. (1999) Gadolinium dimeglumine: an alternative contrast agent for digital subtraction angiography. Eur Radiol 9: 128–136
17 Kaufman JA et al. (1999) Gadolinium-based contrast agents as an alternative at vena cavography in patients with renal insufficiency—early experience. Radiology 212: 280–284
18 Prince MR et al. (1996) Nephrotoxicity of high-dose gadolinium compared with iodinated contrast. J Magn Reson Imaging 6: 162–166
19 Rieger J et al. (2002) Gadolinium as an alternative contrast agent for diagnostic and interventional angiographic procedures in patients with impaired renal function. Nephrol Dial Transplant 17: 824–828
20 Rofsky NM et al. (1991) Renal lesion characterization with gadolinium-enhanced MR imaging: efficacy and safety in patients with renal insufficiency. Radiology 180: 85–89
© 2007 Nature Publishing Group

review review
dEcEmbER 2007 vOL 3 NO 12 PENFIELd ANd REILLY nAtUre clinicAl prActice NEPHROLOGY 667
www.nature.com/clinicalpractice/neph
21 Sancak T et al. (2002) Gadodiamide as an alternative contrast agent in intravenous digital subtraction angiography and interventional procedures of the upper extremity veins. Cardiovasc Intervent Radiol 25: 49–52
22 Spinosa DJ et al. (2000) Lower extremity arteriography with use of iodinated contrast material or gadodiamide to supplement CO2 angiography in patients with renal insufficiency. J Vasc Interv Radiol 11: 35–43
23 Spinosa DJ et al. (1999) Renal insufficiency: usefulness of gadodiamide-enhanced renal angiography to supplement CO2-enhanced renal angiography for diagnosis and percutaneous treatment. Radiology 210: 663–672
24 Townsend RR et al. (2000) Safety of intravenous gadolinium (Gd-BOPTA) infusion in patients with renal insufficiency. Am J Kidney Dis 36: 1207–1212
25 Briguori C (2006) Gadolinium-based contrast agents and nephrotoxicity in patients undergoing coronary artery procedures. Catheter Cardiovasc Interv 67: 175–180
26 Ergun I et al. (2006) The safety of gadolinium in patients with stage 3 and 4 renal failure. Nephrol Dial Transplant 21: 697–700
27 Erley CM et al. (2004) Gadolinium-based contrast media compared with iodinated media for digital subtraction angiography in azotaemic patients. Nephrol Dial Transplant 19: 2526–2531
28 Sam AD et al. (2003) Safety of gadolinium contrast angiography in patients with chronic renal insufficiency. J Vasc Surg 38: 313–318
29 Akgun H et al. (2006) Are gadolinium-based contrast media nephrotoxic? A renal biopsy study. Arch Pathol Lab Med 130: 1354–1357
30 Thomsen HS et al. for the Contrast Media Safety Committee of the European Society of Urogenital Radiology (ESUR) (2002) Gadolinium-containing contrast media for radiographic examinations: a position paper. Eur Radiol 12: 2600–2605
31 Cowper SE et al. (2000) Scleromyxoedema-like cutaneous diseases in renal-dialysis patients. Lancet 356: 1000–1001
32 Daram SR et al. (2005) Nephrogenic fibrosing dermopathy/nephrogenic systemic fibrosis: report of a new case with literature review. Am J Kidney Dis 46: 754–759
33 Cassis TB et al. (2006) Nephrogenic fibrosing dermopathy in a patient with acute renal failure never requiring dialysis. Int J Dermatol 45: 56–59
34 Grobner T (2006) Gadolinium—a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant 21: 1104–1108
35 Danish Medicines Agency (online 29 May 2006) Investigation of the safety of MRI contrast medium Omniscan [press release]. [http://www.dkma.dk/1024/visUKLSArtikel.asp?artikelID=8931]
36 Okada S et al. (2001) Safety of gadolinium contrast agent in hemodialysis patients. Acta Radiol 42: 339–341
37 Deo A et al. (2007) Nephrogenic systemic fibrosis: a population study examining the relationship of disease development to gadolinium exposure. Clin J Am Soc Nephrol 2: 264–267
38 Centers for Disease Control and Prevention (CDC) (2007) Nephrogenic fibrosing dermopathy associated with exposure to gadolinium-containing contrast agents—St Louis, Missouri, 2002–2006. MMWR Morb Mortal Wkly Rep 56: 137–141
39 Joffe P et al. (1998) Pharmacokinetics of gadodiamide injection in patients with severe renal insufficiency and patients undergoing hemodialysis or continuous ambulatory peritoneal dialysis. Acad Radiol 5: 491–502
40 Khurana A et al. (2007) Nephrogenic systemic fibrosis: a review of 6 cases temporally related to gadodiamide injection (omniscan). Invest Radiol 42: 139–145
41 Marckmann P et al. (2006) Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. J Am Soc Nephrol 17: 2359–2362
42 Thomsen HS et al. (2007) Enhanced computed tomography or magnetic resonance imaging: a choice between contrast medium-induced nephropathy and nephrogenic systemic fibrosis? Acta Radiol 48: 593–596
43 Broome DR et al. (2007) Gadodiamide-associated nephrogenic systemic fibrosis: why radiologists should be concerned. AJR Am J Roentgenol 188: 586–592
44 Sadowski EA et al. (2007) Nephrogenic systemic fibrosis: risk factors and incidence estimation. Radiology 243: 148–157
45 Marckmann P et al. (2007) Case-control study of gadodiamide-related nephrogenic systemic fibrosis. Nephrol Dial Transplant [doi:10.1093/ndt/gfm261]
46 Weiss AS et al. (2007) A case of nephrogenic fibrosing dermopathy/nephrogenic systemic fibrosis. Nat Clin Pract Nephrol 3: 111–115
47 Gibby WA et al. (2004) Comparison of Gd DTPA-BMA (Omniscan) versus Gd HP-DO3A (ProHance) retention in human bone tissue by inductively coupled plasma atomic emission spectroscopy. Invest Radiol 39: 138–142
48 White GW et al. (2006) Comparison of Gd(DTPA-BMA) (Omniscan) versus Gd(HP-DO3A) (ProHance) relative to gadolinium retention in human bone tissue by inductively coupled plasma mass spectroscopy. Invest Radiol 41: 272–278
49 High WA et al. (2007) Gadolinium is detectable within the tissue of patients with nephrogenic systemic fibrosis. J Am Acad Dermatol 56: 21–26
50 High WA et al. (2007) Gadolinium is quantifiable within the tissue of patients with nephrogenic systemic fibrosis. J Am Acad Dermatol 56: 710–712
51 Boyd AS et al. (2007) Gadolinium deposition in nephrogenic fibrosing dermopathy. J Am Acad Dermatol 56: 27–30
52 Jain SM et al. (2004) Nephrogenic fibrosing dermopathy in pediatric patients. Pediatr Nephrol 19: 467–470
53 Pöge U et al. (2005) MDRD equations for estimation of GFR in renal transplant recipients. Am J Transplant 5: 1306–1311
54 Cantarovich M et al. (2006) Poor prediction of the glomerular filtration rate using current formulas in de novo liver transplant patients. Transplantation 82: 433–436
55 Mendoza FA et al. (2006) Description of 12 cases of nephrogenic fibrosing dermopathy and review of the literature. Semin Arthritis Rheum 35: 238–249
56 Cowper SE (2003) Nephrogenic fibrosing dermopathy: the first 6 years. Curr Opin Rheumatol 15: 785–790
57 Gilliet M et al. (2005) Successful treatment of three cases of nephrogenic fibrosing dermopathy with extracorporeal photopheresis. Br J Dermatol 152: 531–536
58 Levine JM et al. (2004) Involvement of skeletal muscle in dialysis-associated systemic fibrosis (nephrogenic fibrosing dermopathy). Muscle Nerve 30: 569–577
59 Hubbard V et al. (2003) Scleromyxoedema-like changes in four renal dialysis patients. Br J Dermatol 148: 563–568
60 Mackay-Wiggan JM et al. (2003) Nephrogenic fibrosing dermopathy (scleromyxedema-like illness of renal disease). J Am Acad Dermatol 48: 55–60
61 Streams BN et al. (2003) Clinical and pathologic features of nephrogenic fibrosing dermopathy: a report of two cases. J Am Acad Dermatol 48: 42–47
© 2007 Nature Publishing Group

review
668 nAtUre clinicAl prActice NEPHROLOGY PENFIELd ANd REILLY dEcEmbER 2007 vOL 3 NO 12
www.nature.com/clinicalpractice/neph
62 Swartz RD et al. (2003) Nephrogenic fibrosing dermopathy: a novel cutaneous fibrosing disorder in patients with renal failure. Am J Med 114: 563–572
63 Gibson SE et al. (2006) Multiorgan involvement in nephrogenic fibrosing dermopathy: an autopsy case and review of the literature. Arch Pathol Lab Med 130: 209–212
64 Jimenez SA et al. (2004) Dialysis-associated systemic fibrosis (nephrogenic fibrosing dermopathy): study of inflammatory cells and transforming growth factor beta1 expression in affected skin. Arthritis Rheum 50: 2660–2666
65 Kucher C et al. (2006) Nephrogenic fibrosing dermopathy/nephrogenic systemic fibrosis with diaphragmatic involvement in a patient with respiratory failure. J Am Acad Dermatol 54 (suppl 2): S31–S34
66 Ting WW et al. (2003) Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol 139: 903–906
67 Baron PW et al. (2003) Nephrogenic fibrosing dermopathy after liver transplantation successfully treated with plasmapheresis. Am J Dermatopathol 25: 204–209
68 Hershko K et al. (2004) A variant of nephrogenic fibrosing dermopathy with osteoclast-like giant cells: a syndrome of dysregulated matrix remodeling? J Cutan Pathol 31: 262–265
69 Ruiz-Genao DP et al. (2005) Osseous metaplasia in the setting of nephrogenic fibrosing dermopathy. J Cutan Pathol 32: 172–175
70 Edward M et al. (2007) Cutaneous mucinosis associated with dermatomyositis and nephrogenic fibrosing dermopathy: fibroblast hyaluronan synthesis and the effect of patient serum. Br J Dermatol 156: 473–479
71 Kucher C et al. (2005) Histopathologic comparison of nephrogenic fibrosing dermopathy and scleromyxedema. J Cutan Pathol 32: 484–490
72 Kafi R et al. (2004) UV-A1 phototherapy improves nephrogenic fibrosing dermopathy. Arch Dermatol 140: 1322–1324
73 Yerram P et al. (2007) Nephrogenic systemic fibrosis: a mysterious disease in patients with renal failure—role of gadolinium-based contrast media in causation and the beneficial effect of intravenous sodium thiosulfate. Clin J Am Soc Nephrol 2: 258–263
74 Chung HJ and Chung KY (2004) Nephrogenic fibrosing dermopathy: response to high-dose intravenous immunoglobulin. Br J Dermatol 150: 596–597
75 Choyke PL et al. (1995) Clearance of gadolinium chelates by hemodialysis: an in vitro study. J Magn Reson Imaging 5: 470–472
76 Dorsam J et al. (1995) Elimination of gadolinium-DTPA by peritoneal dialysis. Nephrol Dial Transplant 10: 1228–1230
77 Okada S et al. (2003) Effect of the surface potential of the hemodialysis membrane and the electrical charge of the gadolinium contrast medium on dialyzability. J Nippon Med Sch 70: 12–15
78 Saitoh T et al. (2006) Dialyzability of gadodiamide in hemodialysis patients. Radiat Med 24: 445–451
79 Schuhmann-Giampieri G and Krestin G (1991) Pharmacokinetics of Gd-DTPA in patients with chronic renal failure. Invest Radiol 26: 975–979
80 Swan SK et al. (1999) Pharmacokinetics, safety, and tolerability of gadoversetamide injection (OptiMARK) in subjects with central nervous system or liver pathology and varying degrees of renal function. J Magn Reson Imaging 9: 317–321
81 Swan SK et al. (1999) Safety and pharmacokinetic profile of gadobenate dimeglumine in subjects with renal impairment. Invest Radiol 34: 443–448
82 Ueda J et al. (1999) Permeability of iodinated and MR contrast media through two types of hemodialysis membrane. Eur J Radiol 31: 76–80
83 Ueda J et al. (1998) Permeability of gadolinium-DTPA through two types of hemodialysis membrane. Invest Radiol 33: 734–737
84 Emerson J and Kost G (2004) Spurious hypocalcemia after Omniscan- or OptiMARK-enhanced magnetic resonance imaging: an algorithm for minimizing a false-positive laboratory value. Arch Pathol Lab Med 128: 1151–1156
85 Lin J et al. (1999) Interference of magnetic resonance imaging contrast agents with the serum calcium measurement technique using colorimetric reagents. J Pharm Biomed Anal 21: 931–943
86 Lowe A et al. (2005) Interference of gadolinium-containing contrast-enhancing agents with colorimetric calcium laboratory testing. Invest Radiol 40: 521–525
87 Moore CD et al. (2006) Spurious hypocalcemia after gadodiamide-enhanced magnetic resonance imaging: a case report and review of the literature. Rev Urol 8: 165–168
88 Prince MR et al. (2003) Gadodiamide administration causes spurious hypocalcemia. Radiology 227: 639–646
89 Proctor KA et al. (2004) Gadolinium magnetic resonance contrast agents produce analytic interference in multiple serum assays. Am J Clin Pathol 121: 282–292
90 Normann PT et al. (1995) Interference of gadodiamide injection (OMNISCAN) on the colorimetric determination of serum calcium. Scand J Clin Lab Invest 55: 421–426
91 Kang HP et al. (2004) Model for predicting the impact of gadolinium on plasma calcium measured by the o-cresolphthalein method. Clin Chem 50: 741–746
92 Medicines and Healthcare products Regulatory Agency (online 7 February 2007) Public assessment report: increased risk of nephrogenic fibrosing dermopathy/nephrogenic systemic fibrosis and gadolinium-containing MRI contrast agents. [http://www.mhra.gov.uk/home/idcplg?IdcService=SS_GET_PAGE&ssDocName=CON2030229&ssSourceNodeId=221&ssTargetNodeId=221]
93 Kanal E et al. (2007) ACR guidance document for safe MR practices: 2007. AJR Am J Roentgenol 188: 1447–1474
94 Van Moore A Jr (2007) Commentary on “ACR guidance document for safe MR practices: 2007”. AJR Am J Roentgenol 188: 1446
95 Kuo PH et al. (2007) Gadolinium-based MR contrast agents and nephrogenic systemic fibrosis. Radiology 242: 647–649
96 Levey AS et al. (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 130: 461–470
AcknowledgmentsCharles P Vega, University of California, Irvine, CA, is the author of and is solely responsible for the content of the learning objectives, questions and answers of the Medscape-accredited continuing medical education activity associated with this article.
Competing interestsThe authors declared no competing interests.
© 2007 Nature Publishing Group