what matters most: it’s all about me
TRANSCRIPT

8/27/2020
1
What Matters Most: It’s ALL ABOUT ME
Arlene Stoller MS, RN-BC, ACNS-BC, GCNS, CDP
Objectives
• State the purpose of the 4Ms as they relate to care for older adults.
• Discuss the importance of knowing What Matters Most to older adults.
• Describe the association between Advance Care Planning and What Matters Most.
• List two resources available to help aid nurses in identifying What Matters Most when providing Person Centered Care.
Arlene Stoller MS, RN-BC, ACNS-BC, GCNS, CDP
NICHE Program leader/ Geriatric Clinical Nurse SpecialistLahey Hospital & Medical CenterBurlington, MAEmail: [email protected]: 617-460-2222
Why This Work Matters to Me
Based on Ihi.org. (2019). [online] Available at: http://www.ihi.org/Engage/Initiatives/Age-Friendly-Health-Systems/Documents/IHI_Age_Friendly_What_Matters_to_Older_Adults_Toolkit.pdf [Accessed 31 Aug. 2019].
Age-Friendly Health Systems
• Created by The John A. Hartford Foundation and Institute of Healthcare Improvement partnered with
• American Hospital Association
• Catholic Health Association of the United States
• Vision- To build a social movement so that all care with older adults is age-friendly care
• Follows an essential set of evidence-based practices
• Causes no harm
• Aligns with What Matters to the older adult and their family caregivers
• Birth of the 4Ms: What Matters, Medication, Mentation & Mobility

8/27/2020
2
But Why?
• Demography• Projected double in size
• Complexity• 80% have 1 chronic condition
• 77% have ≥ 2 chronic conditions
• Disproportionate Harm• ↑ rates of harm, delay & discoordination
https://www.aarp.org/livable-communities/about/info-2018/aarp-livable-communities-preparing-for-an-aging-nation.html
The 4Ms Framework
The 4Ms Framework: Medication
• Review for use of high risk
medications
• Benzodiazepines
• Opioids
• Anticholinergic meds
• Sleep meds including OTC
• Muscle relaxers
• Antipsychotics
• Deprescribe and/or avoid high
risk medications & communicate
The 4Ms Framework: Mentation
• Screen for delirium Q12 hours and
document
• Ensure sufficient oral hydration
• Orient to time, place & situation
• Support nonpharmacological sleep
• Assess
• UB-2, CAM/CAM ICU, bCam, 3D
Cam, NuDESK
• Mini-cog, MOCA
• PHQ, GDS
The 4Ms Framework: Mobility
• Screen for mobility limitations
• Ensure early, frequent and
safe movement / mobility
• Assess
• TUG
• Tethering devices
• Physical Therapy
The 4Ms Framework

8/27/2020
3
The First M: What Matters Most
• Basis for age friendly care
• Person Centered Care• Respectful of and responsive to individual patient preferences, needs and
values, and ensuring that patient values guide all clinical decisions (IOM, 2011)
• Integrates care decisions across the care team and care setting• Regular and annual wellness visits
• New diagnosis or change in health status
• Life-stage change
• Chronic disease management
• Inpatient visits (hospital, nursing home, skilled nursing facility)
Why What Matters Most Matters Most
• For older adults
• Vary in What Matters Most
• Feel more engaged, listened to
• Avoid unwanted care & receive wanted care
• For health systems
• Better patient experience scores & retention
• Avoid unnecessary utilization
• For everyone (patients, caregivers, providers, health system)
• Everyone on same page
• Improved relationships
• It is the basis of everything else
How to Reliably Ask What Matters Most
• Purpose: General getting to know person & what’s important• Agree on what information is important
• Feasible (time, training, format, method for sharing information)
• Purpose: Inform care decisions• Feasible (time, training, format, method for sharing information)
• Reliable, specific, actionable• Depends on setting & patient population
• Setting: Immediate decision (e.g. hospital, ED) or ongoing care (e.g., 1º care, ambulatory)
• Population: People with chronic conditions or serious illness and/or end of life
• Age-Friendly Health System What Matters toolkit
Essential Ingredients- Ask What Matters
• Who?• When?• Using what question(s)?
• Who?• What?• Where?
• Who?• How do we know if that
has happened?
Ask What Matters
Document What Matters
Align the Care Plan with What Matters
It’s a Conversation!
• Who can do this?
• Everyone- it is a conversation
• When should this be done?
• Ongoing
• What do I do with the information?
• Document (EHR vs Written)
Culturally Competent Conversations
• Consider the impact of race, ethnicity, language, religion, culture and identity
• Issues of trust affect “What Matters” conversations
• Be aware of unconscious biases• Verbal
• Nonverbal
Department of health and Human Services, 2013

8/27/2020
4
What Do I Ask? Life Priorities
Guiding Questions: Understanding Life Context and Priorities
• What is important to you today?
• What brings you joy? What makes you happy? What makes life worth living?
• What do you worry about?
• What are some goals you hope to achieve in the next six months or before your next birthday?
• What would make tomorrow a really great day for you?
• What else would you like us to know about you?
• How do you learn best? For example, listening to someone, reading materials, watching a video.
What Do I Ask? Treatment Goals
Guiding Questions: Anchoring Treatment in Goals and Preferences
• What is the one thing about your health care you most want to focus on so that you can do [fill in desired
activity] more often or more easily?
• What are your most important goals now and as you think about the future with your health?
• What concerns you most when you think about your health and health care in the future?
• What are your fears or concerns for your family?
• What are your most important goals if your health situation worsens?
• What things about your health care do you think aren’t helping you and you find too bothersome or difficult?
• Is there anyone who should be part of this conversation with us?
During the Conversation
• Invite the older adult
• Ask one or more questions- limit scripts/checkboxes
• Listen and ask questions
• Consider health literacy
• Affirm the conversation• Acknowledge thoughts and feelings
• Confirm understanding of communication
• Ask for clarification
How Do I Know “What Matters Most” if My Patient is Confused?
• Assess cognition
• Responsibility to know and engage the person
• Best times of the day for conversations
• If cognitive impairment severe• Identify who the older adult relies upon for decisions
Guiding Principle: Maximize autonomy of cognitively impaired and not diminish their self-image
Practice Recommendations for Person-Centered Care with Dementia
• Know the person living with dementia
• Recognize and accept the person’s reality
• Identify and support ongoing opportunities for meaningful engagement
• Build and nurture authentic, caring relationships
• Create and maintain a supportive community for individuals, families and staff
• Evaluate care practices regularly and make appropriate changes
Sam Fazio, Douglas Pace, Janice Flinner, Beth Kallmyer, The Fundamentals of Person-Centered Care for Individuals With Dementia, The Gerontologist, Volume 58, Issue suppl_1, February 2018, Pages S10–S19, https://doi.org/10.1093/geront/gnx122 Retrieved from https://academic.oup.com/gerontologist/article/58/suppl_1/S10/4816735
Essential Ingredients- Document What Matters
• Who?• When?• Using what question(s)?
• Who?• What?• Where?
• Who?• How do we know if that
has happened?
Ask What Matters
Document What Matters
Align the Care Plan with What Matters
8/27/2020
5
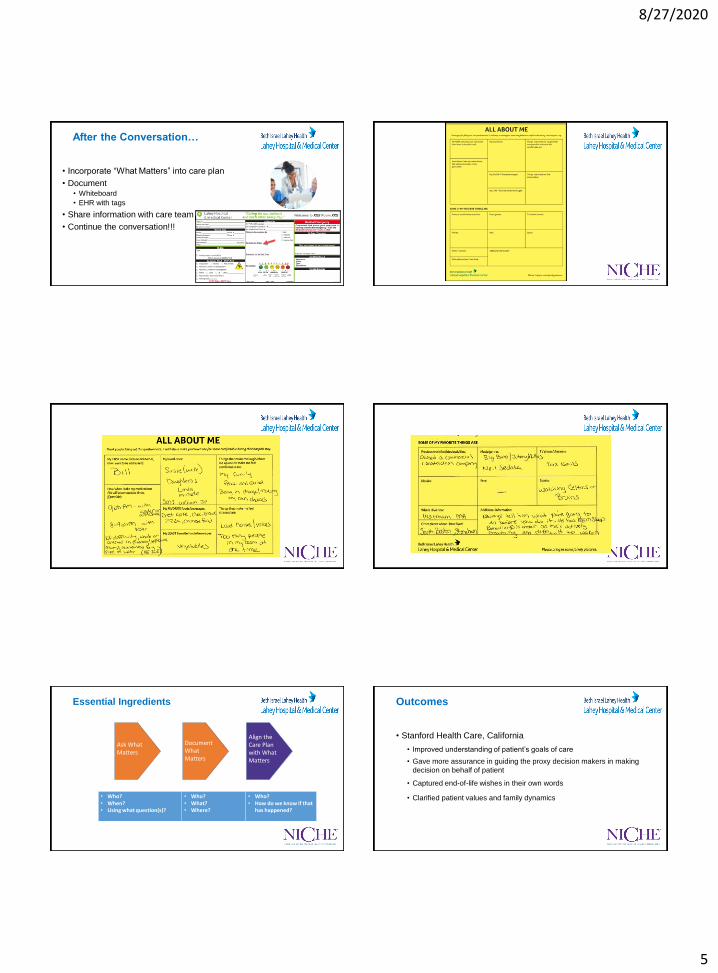
After the Conversation…
• Incorporate “What Matters” into care plan
• Document• Whiteboard
• EHR with tags
• Share information with care team
• Continue the conversation!!!
Essential Ingredients
• Who?• When?• Using what question(s)?
• Who?• What?• Where?
• Who?• How do we know if that
has happened?
Ask What Matters
Document What Matters
Align the Care Plan with What Matters
Outcomes
• Stanford Health Care, California
• Improved understanding of patient’s goals of care
• Gave more assurance in guiding the proxy decision makers in making
decision on behalf of patient
• Captured end-of-life wishes in their own words
• Clarified patient values and family dynamics

8/27/2020
6
Meet Gloria Advance Directives
The Conversation Project. (n.d.). Retrieved from http://theconversationproject.org/
What’s in the Literature?
• Older adults overestimate the success rate of CPR (Sharma Jayathissa & Weatherall, 2016)
• Majority of patients want family present when given important information and significant decisions are being made (Friis & Forde, 2015)
• Older adults inaccurately assume their family members are knowledgeable about their end-of-life preferences (Li-Shan et al., 2015)
• Culture influences the desire to discuss ACP, with Western older adults wishing to participate directly in these discussions, while Asian cultures prefer collective family decision making and often wish their family members to make the decisions for them (Kwak & Salmon, 2007; Ko & Berkman, 2010)
• One third of individuals selected to be the healthcare agent were not the next of kin (Cheang et al., 2014)
• Patients often do not discuss AD during primary care visits with providers (Vandrvoort et al., 2014)
What’s in the Literature
• Employment transitions, such as retirement, often results in ACP conversations (Huang et al., 2015)
• 86% of adults ≥ 70 years of age admitted to a Pennsylvania Health System for an isolated hip fracture had no documented conversation of EOL care planning (Dunn, Ahn & Bernstein, 2016)
• 40% of patients entering a long term care facility as a full code, changed their
status to DNR after ACP conversations (Mukamel, Ladd, & Temkin-Greener, 2013)
• An ACP conversation about hospitalization during end-of-life resulted in a decrease in hospitalization rates during that period of time (Silveira, Wiitala, & Piette, 2014)
Forms provide structure, but conversations with the healthcare decision maker & the healthcare provider are more important than paper documents
(Lee, 2014)
Tips on Acting on What Matters Most
• Collaborative negotiations when difference in plan (agree there is no best answer & brainstorm alternatives)
• “I know you don’t like the CPAP mask, but are you willing to try it for 2 weeks to see if it helps you be less tired so you can get back to volunteering which you said was most important to you”
• Care options likely involve input from many disciplines (PT, SW, community organizations, etc.)
Tips on Acting on What Matters Most
Use patient’s preferences
• “There are several things we could do, but knowing what matters most to you, I suggest we…”
Use patient’s priorities (not just diseases) in communicating, decision-making, assessing benefit

8/27/2020
7
What Matters Most: COVID-19
• ACP is always essential, but with these new times it is critical! • Don’t wait- If patient is >60 and has one or more serious illnesses- Reach out
• Talking about goals of care and treatment preferences is not always easy. It can be uncomfortable and stressful.
• You know this virus is going around. • Have you thought about what it means for you? • What goal of care is most important to you now? • Not many older people who are sick enough to need a ventilator to breathe will survive. • If you get a bad case, would you want to go to the hospital and potentially be treated in an
ICU on a ventilator? • We will do our best to honor your preferences.
• Discuss the difference between• Prolonging Life- Focus is on living longer• Maintaining Function- Focus is on staying strong and independence• Comfort Care- Focus is on improving comfort level and QOL
Patient Care Priorities
https://patientprioritiescare.org/about/
Patient Care Priorities- Mr K.
https://patientprioritiescare.org/about/
Patient Care Priorities- What Matters Most to Mr K.
https://patientprioritiescare.org/about/
Putting the 4Ms into Practice: A “Recipe”
1. Understand your current state
2. Describe what it means to provide care consistent with the 4Ms
3. Design/adapt your workflow to deliver care consistent with 4Ms
4. Provide care consistent with the 4Ms
5. Study your performance
6. Improve and sustain care consistent with the 4Ms
Many Other Tools

8/27/2020
8
References
• Department of Health and Human Services, Centers for Medicare and Medicaid. 2016. Advance Care Planning. Retrieved from:https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/Advance CarePlanning.pdf
• Department of Health & Human Services, National Standards for CLAS in Health and Health care: A blueprint for advancing and sustaining CLAS policy and Practice, 2013. Retrieved from https://www.pcpcc.org/sites/default/files/resources/A%20Blueprint%20for%20Advancing%20and%20Sustaining%20CLAS%20Policy%20and%20Practice.pdf
• Dunn, R. H., Ahn, J. & Bernstein, J. (2016). End-of-life care planning and fragility fractures of the hip: Are we missing a valuable opportunity? Clinical Orthopaedics and Related Research, 474, 1736-1739. Doi:10.1007/s11999-015-4675-1
• Fazio, Sam, Douglas, Flinner, Janice, & Beth. (2018, January 18). Fundamentals of Person-Centered Care for Individuals With Dementia. Retrieved from https://academic.oup.com/gerontologist/article/58/suppl_1/S10/4816735
• Friis, P., Førde, R. (2015). Advance care planning discussions with geriatric patients. Tidsskr Nor Laegeforen. 10, 233-5.
• Ihi.org. (2019). [online] Available at: http://www.ihi.org/Engage/Initiatives/Age-Friendly-Health-Systems/Documents/IHI_Age_Friendly_What_Matters_to_Older_Adults_Toolkit.pdf [Accessed 31 Aug. 2019].
• It's Your Health Care. It's Your Choice. (n.d.). Retrieved April 28, 2017, from http://www.honoringchoicesmass.com/
• Huang, I.A., Neuhaus, J.N. & Chiong, W. (2015). Racial and ethnic differences in advance directive possession: Role of demographic factors, religious affiliation and personal health values in a national survey of older adults. Journal of Palliative Care, 19, 149-156. Doi:10.1089/jpm.2015.0326
References
• Kwak, J. & Salmon, J.R. (2007). Attitudes and preferences of Korean-American older adults and caregivers on end-of-life. Journal of the American Geriatrics Society, 11, 1867-72.. Doi:10.1111/j.1532-5415.2007.01394.x
• Ko, E. & Berkman, C.S. (2010). Role of children in end-of-life treatment planning among Korean American older adults. Journal of Social Work in End of Life & Palliative Care, 6, 164-84. doi: 10.1080/15524256.2010.529019
• Li-Shan, K., Huang, M. O’Connor, M. & Lee, S. (2015). Nurses’ views regarding implementing advance care planning for older people: A systematic review and synthesis of qualitative studies. Journal of Clinical Nursing, 24, 2057-2073. doi:10.1111/jocn.12853
• Lee, T. J. (2014). Discussing advance care planning with elderly patients. North Carolina medical Journal, 75, 347-351.
• Lum, H.D., Sudore, R.L. & Bekelman, D.B. (2015). Medical Clinics of North America,99, 391-403. doi:10.1016/j.mcna.2014.11.010
• Lum, H, D., Jones, J, Matlock, D.D., Glasgow, R.E., Schwartz, R.S., Sudore, R.L. & Kutner, J.S. (2016). Advance care planning meets group medical visits: The feasibility of promoting conversations. Annals of Family Medicine, 14, 125-132. doi:10.1370/afm.1906
• (n.d.). Frequently Asked Questions. Retrieved from https://patientprioritiescare.org/faqs/#1497886638837-397dd140-0de4Cheang, F., Finnegan, T., Hession, A. & Clayton, J.M. (2014). Single-centre cross-sectional analysis of advance care planning among elderly inpatients. Internal Medicine Journal, 967-974. doi:10.1111/imj.12550
• (n.d.). Vitalize 360 - Senior Health & Wellness Program. Retrieved from https://www.hebrewseniorlife.org/vitalize360
References
• (n.d.). Homepage. Retrieved from https://nicheprogram.org/
• Mukamel, D.B., Ladd, H. & Temkin-Greener, H. (2013). Stability of cardiopulmonary resuscitation and do not resuscitate orders among long-term nursing home residents. Medical Care, 51, 666-672. doi:10.1097/MLR.0b013e31829742b6
• Patient Priorities Care. (2019). Homepage - Patient Priorities Care. [online] Available at: https://patientprioritiescare.org/ [Accessed 3 Sep. 2019].
• Sharma, R., Jayathissa, S. & Weatherall, M. (2016). Cardiopulmonary resuscitation knowledge and opinions on end of life decision making of older adults admitted to an acute medical service. The New Zealand Medical Journal;129, 25-35.
• Silveira, M.J., Wiitala, W. & Piette, J. (2014). Advance directive completion by elderly Americans: A decade of change. Journal
• Stanford Medicine Bucket List Planner: Tool for reflecting on core values and goals through “bucket list” planning. Retrieved September 2019 https://med.stanford.edu/content/dam/sm/letter/documents/Bucket-list-toolkit-Periyakoil-lab.pdf of the American Geriatrics Society, 62, 706-710. doi:10.1111/jgs.12736.
• Vandervoort, A., Houttekier, D., Van den Block, L., van de Steen, J.T., Vander Stichele, R. & Deliens, L. (2014). Advance care planning and physician orders in nursing home residents with dementia: A nationwide retrospective study among professional caregivers and relatives. Journal of Pain and Symptom Management, 47, 245-256.