what does the future hold for new tracking and assessment tools in multiple sclerosis
TRANSCRIPT

What does the future hold for new tracking and assessment tools in MS?
Gavin Giovannoni
Barts and The London School of Medicine and Dentistry
London, UK

Disclosures
Professor Giovannoni has received personal compensation for participating onAdvisory Boards in relation to clinical trial design, trial steering committees and dataand safety monitoring committees from: Abbvie, Bayer-Schering Healthcare, Biogen-Idec, Canbex, Eisai, Elan, Fiveprime, Genzyme, Genentech, GSK, GW Pharma,Ironwood, Merck-Serono, Novartis, Pfizer, Roche, Sanofi-Aventis, Synthon BV, Teva,UCB Pharma and Vertex Pharmaceuticals.
Regarding www.ms-res.org survey results in this presentation: please note that nopersonal identifiers were collected as part of these surveys and that by completing thesurveys participants consented for their anonymous data to be analysed andpresented by Professor Giovannoni.
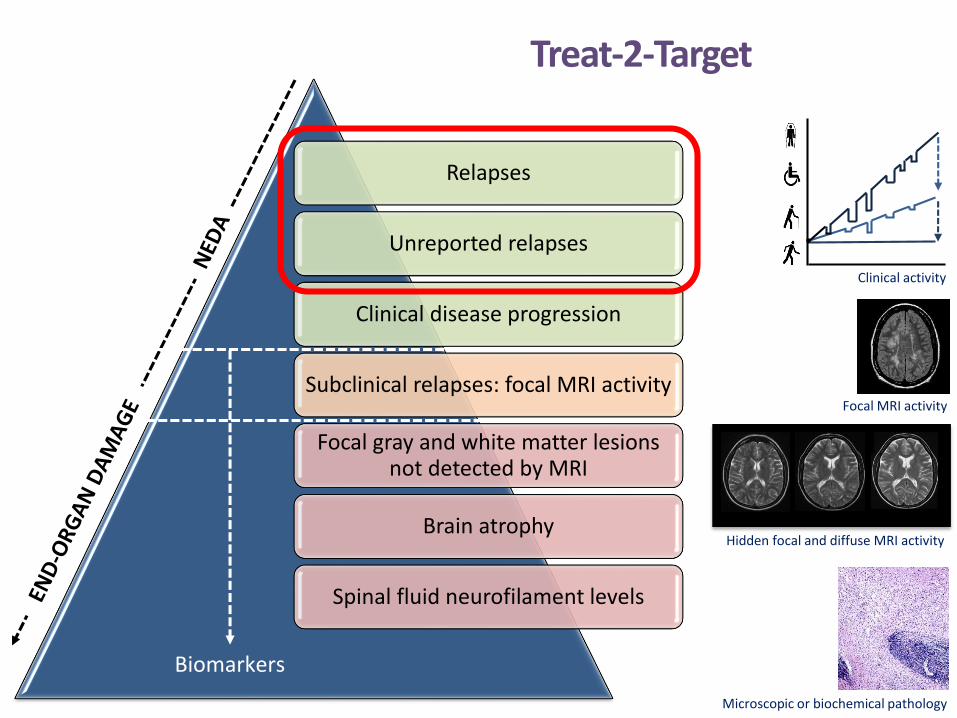
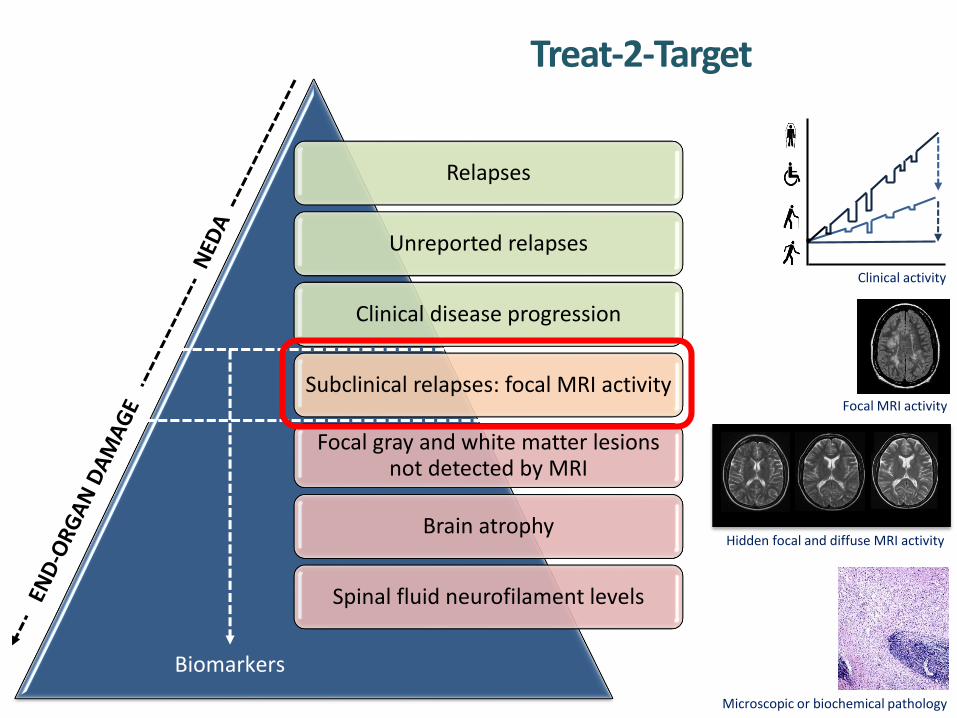
Relapses
Unreported relapses
Clinical disease progression
Subclinical relapses: focal MRI activity
Focal gray and white matter lesions not detected by MRI
Brain atrophy
Spinal fluid neurofilament levels
Treat-2-Target
Clinical activity
Focal MRI activity
Hidden focal and diffuse MRI activity
Microscopic or biochemical pathology
Biomarkers

Yes, 72
No, 28
Relapse reporting
• Most common reasons for not reporting their most recent relapse to a specialist MS team were: • ‘Mild relapse so not felt necessary’ 5/28 (18%)• ‘Saw or spoke to their GP’ 4/28 (14%)
• Most common reasons for not seeking healthcare support were:• ‘Felt I could manage’/mild relapse 18/42 (43%) • ‘Nothing that they can do to help’ 8/42 (19%)
Duddy M, et al. ECTRIMS 2013. P590.
N = 101
Yes, 46
No, 54
N = 102
Patients who have everexperienced an MS relapse and
not contacted a healthcare professional
Patients reporting most recentrelapse to a specialist MS team






Relapses
Unreported relapses
Clinical disease progression
Subclinical relapses: focal MRI activity
Focal gray and white matter lesions not detected by MRI
Brain atrophy
Spinal fluid neurofilament levels
Treat-2-Target
Clinical activity
Focal MRI activity
Hidden focal and diffuse MRI activity
Microscopic or biochemical pathology
Biomarkers

Yes – I do an EDSS whenever I see a patient 14 25%
Yes – I do an EDSS annually 10 18%
Yes – I occasionally do an EDSS 20 36%
No – I never do an EDSS 3 5%
Other 9 16%Yes – I do an EDSS whenever I see a
patient [14]Yes – I do an EDSS
annually [10]
Yes – I occasionally do an EDSS [20]
No – I never do an EDSS [3]
Other [9]
Survey of UK MSologists
Schmierer K, et al. ABN 2014; Unpublished.
Clinical – In your routine MS clinical practice, do you use the EDSS?
Clinical – If you do an EDSS in your routine clinical practice, do you walk the patients to assess their walking distance?
Yes [9]
No [20]
Sometimes [22]
Other [5] Yes 9 16%
No 20 36%
Sometimes 22 39%
Other 5 9%

Validating a novel web-based method to capture disease progression outcomes in MS
P-EDSS, physician or actual EDSS.The midpoint of the diamonds is the mean difference between the two EDSS scores, the upper and lower lines within the diamonds are the 95% CI. The width of the diamond indicates the sample size, the dots the actual values. The horizontal line at 0.46 indicates the mean difference between the two scores. The graph indicates the greater variation at lower EDSS scores, with greater agreement at scores > 5. Leddy S, et al. J Neurol 2013; 260:2505–2510.
ORIGINAL COMMUNICATION
we
b-
EDSS
–P
-ED
SS s
core
P-EDSS score
–4
–3
–2
–1
0
1
2
3
4
0 1 1.5 2 2.5 3 3.5 4 4.5 5.5 6 6.5 7 8

Cli
nic
Sp
eak
www.clinicspeak.com

Unmet Needs remain from both the MSer and HCP perspectives
UNMET NEEDSHCP Perspective
UNMET NEEDSPatient Perspective

Monitoring your own disease






PROMs / PROs
Generic
Outcome-specific
MS-specific
MS outcome-specific
•EQ5D
• SF36
•Barthel Index
•Berg Balance Scale
•Ambulation Index
•MSIS-29
•MusiQoL
•MSWS-12
•MSFIS
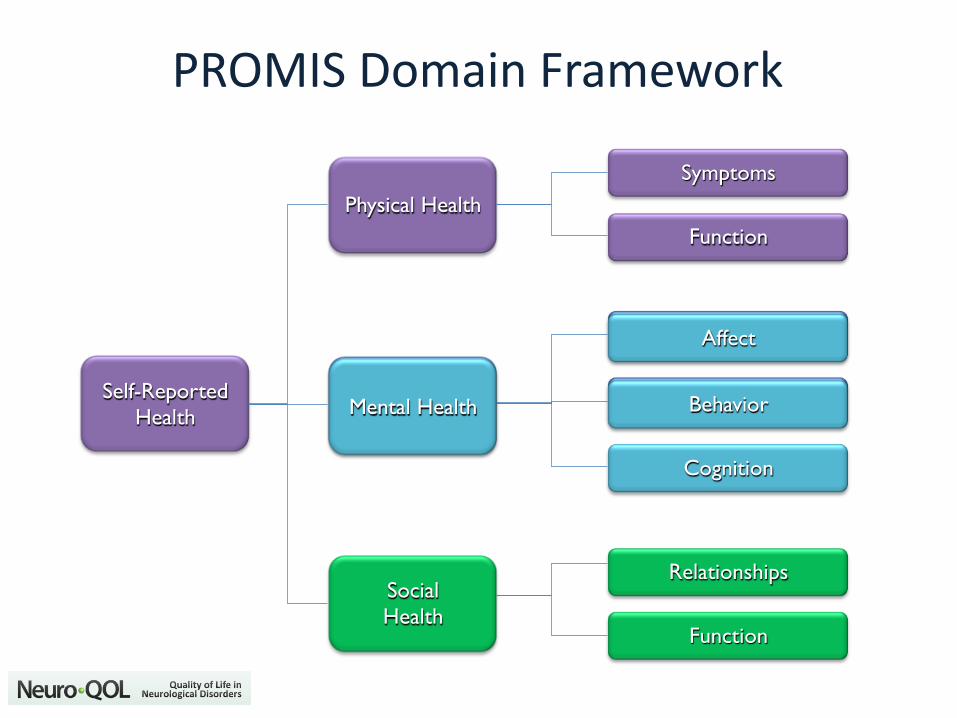
PROMIS Domain Framework
Self-Reported
Health
Social
Health
Mental Health
Physical Health
Symptoms
Function
Affect
Behavior
Cognition
Relationships
Function
Mental Health
Affect
Behavior
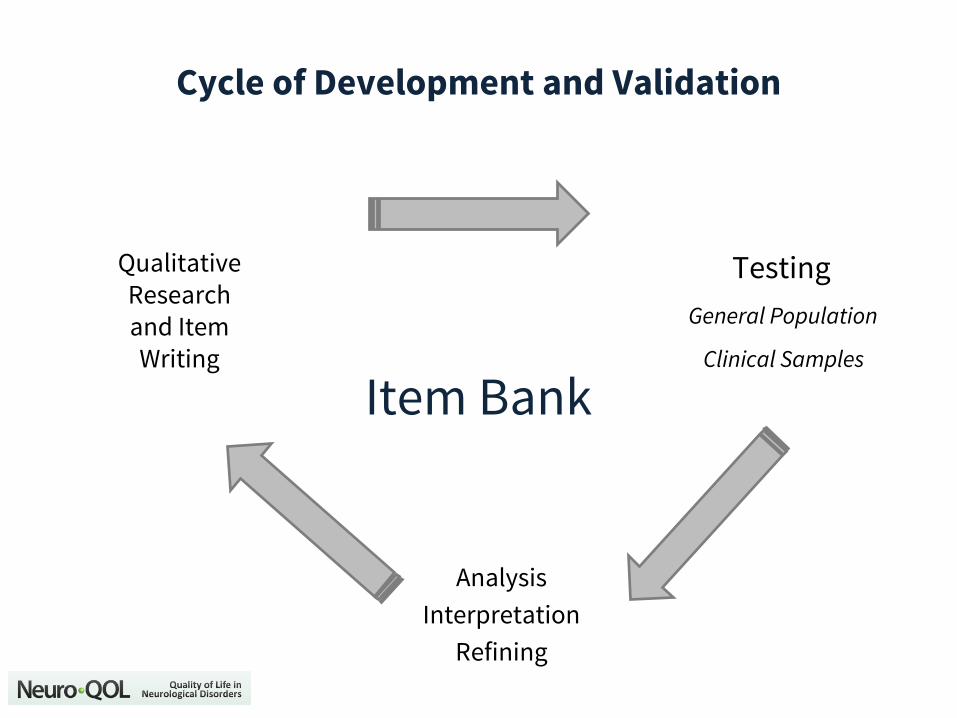
Testing
General Population
Clinical Samples
Analysis
Interpretation
Refining
Qualitative Research and Item Writing
Item Bank
Cycle of Development and Validation

Physical Functioning Item Bank
Item1
Item2
Item3
Item4
Item5
Item6
Item7
Item8
Item9
Itemn
100500
• Are you able to get in and out of bed?• Are you able to stand without losing your balance for 1 minute?• Are you able to walk from one room to another?• Are you to walk a block on flat ground?• Are you able to run or jog 2 miles?• Are you able to rund 5 miles?

Questionnaire Fatigue
Relapses
Unreported relapses
Clinical disease progression
Subclinical relapses: focal MRI activity
Focal gray and white matter lesions not detected by MRI
Brain atrophy
Spinal fluid neurofilament levels
Treat-2-Target
Clinical activity
Focal MRI activity
Hidden focal and diffuse MRI activity
Microscopic or biochemical pathology
Biomarkers










Conclusions
• eMonitoring and eHealth are here to stay
• Adoption is occurring very rapidly in some sectors
• Advantages are obvious
• Improved efficiency (cost and time effective)
• Better outcomes
• Higher satisfaction
• Hurdles to adoption are not insurmountable
• Privacy and data protection
• Medico-legal issues
• eMonitoring
• I don’t know how to do it yet
• Adoption, adherence, design, etc.
• automatic, smartphone (‘the great disruptor’)
