west nile virus surveillance ingrid garrison, dvm, mph, dacvpm state public health veterinarian...
TRANSCRIPT

West Nile Virus Surveillance
Ingrid Garrison, DVM, MPH, DACVPMState Public Health Veterinarian
September 16, 2015
West Nile Virus
Arthropod-borne virus (arbovirus) spread by infected mosquitoes
Culex species are the primary vector for West Nile virus (WNV) although it has been detected in 9 other species
Rarely transmitted by blood transfusion All blood donors now screened for WNV

West Nile Virus the Disease
Incubation period – 3-15 days Symptoms can include fever, headache, body
aches, joint pains, vomiting, diarrhea, or rash Most recover completely but fatigue and
weakness can last for weeks or months Less than 1% develop encephalitis or
meningitis 10% of patients with serious neurological illness
will die


West Nile Virus History
First isolated from a febrile patient from the West Nile district of Northern Uganda in 1937
WNV was first characterized in detail in the early 1950s and 1960s
First recognized epidemic of WNV occurred in Israel, 1951
Several large outbreaks in Egypt between 1951 and 1954

West Nile Virus History
In 1957, an outbreak in Israel was the first with severe neurologic manifestations
Between 1960 and mid 1970s, large outbreaks occurred in France, South Africa, Russia, Spain and India
Large outbreaks of WNV were very infrequent throughout the late 1970s and 1980s
West Nile Virus History
WNV was first identified in North America in New York City in 1999
An epizootic among birds associated with a high fatality rate was first noted; assessments did not detect common avian pathogens
NYC birds, infected mosquitoes, and human brain tissue from a fatal case of encephalitis identified WNV as the etiologic agenthttp://www.timesunion.com/news/article/Stone-role-raises-doubt-559620.php

Year of First Reported Human West Nile Virus Disease Case, By State – U.S., 1999-2008
Map Courtesy of CDC

West Nile Virus History
During the summer of 2002, North America had the largest outbreak of West Nile meningoencephalitits ever recorded
Factors contributing to outbreak remain unclear
KDHE began surveillance for WNV, 2001 First human case in Kansas, 2002

Mosquito Surveillance - Kansas
• In the early 2000s mosquito surveillance enjoyed robust funding
• Mosquito traps placed in all preparedness regions of Kansas
• Kansas State University trapped, identified, and tested mosquitoes for WNV

Mosquito Surveillance - Kansas
• As funding decreased the number of traps decreased
• Evaluation of the Kansas mosquito surveillance system (2001-2009)– Profound delay between mosquito collection,
identification, WNV testing, and report to KDHE– Human cases of WNV occurred BEFORE WNV
positive mosquitoes were identified– Not an ‘early warning’ system

Mosquito Surveillance - Kansas
• In 2011 Kansas Biological Survey new mosquito surveillance partner (collection, i.d.)
• Kansas Health and Environmental Lab performed WNV testing
• New methodology was established in 2013– Concentrated mosquito surveillance in county
with highest number of WNV cases (Sedgwick)

Methods

Mosquito Surveillance
Conducted weekly from June 13 to October 24, 2013 in Sedgwick County (24 weeks)
Kansas Biological Survey placed traps where mosquito transmission was most likely to occur
9 traps were set each week

Mosquito Surveillance
Encephalitis Vector Survey (EVS) traps were used
Emit carbon dioxide by using dry ice
http://www.mosquitoturlock.com/surveillance.shtm
Mosquito Surveillance
Mosquitoes transported to Kansas Biological Survey for enumeration and identification
Culex spp. mosquitoes were tested for WNV
http://i.usatoday.net/news/_photos/2012/08/30/Maryland-reports-1st-West-Nile-virus-death-PF267HV9-x-large.jpg

Human Surveillance
Reportable disease in Kansas Cases entered in EpiTrax
Investigation conducted by local health department Disease investigation guideline
Cases classified based on 2011 CDC case definition Need clinical and laboratory data Probable and confirmed cases reported
American Red Cross reports presumptive viremic blood donors for further investigation

ArboNet
KDHE reports human and mosquito surveillance data to ArboNet
National arboviral surveillance system managed by CDC and state health departments
Maintains data on: Human disease (including presumptive viremic blood donors) Veterinary disease cases Mosquitoes Dead birds Sentinel animals

Surveillance Results

Results
• Mosquito enumeration and identification data from KBS to KDHE within 1 business day
• Mosquito WNV test data available within 7-10 business days
• Mosquito and human surveillance data posted weekly on KDHE’s website
• Data shared with Sedgwick County Health Department
Mosquito Abundance
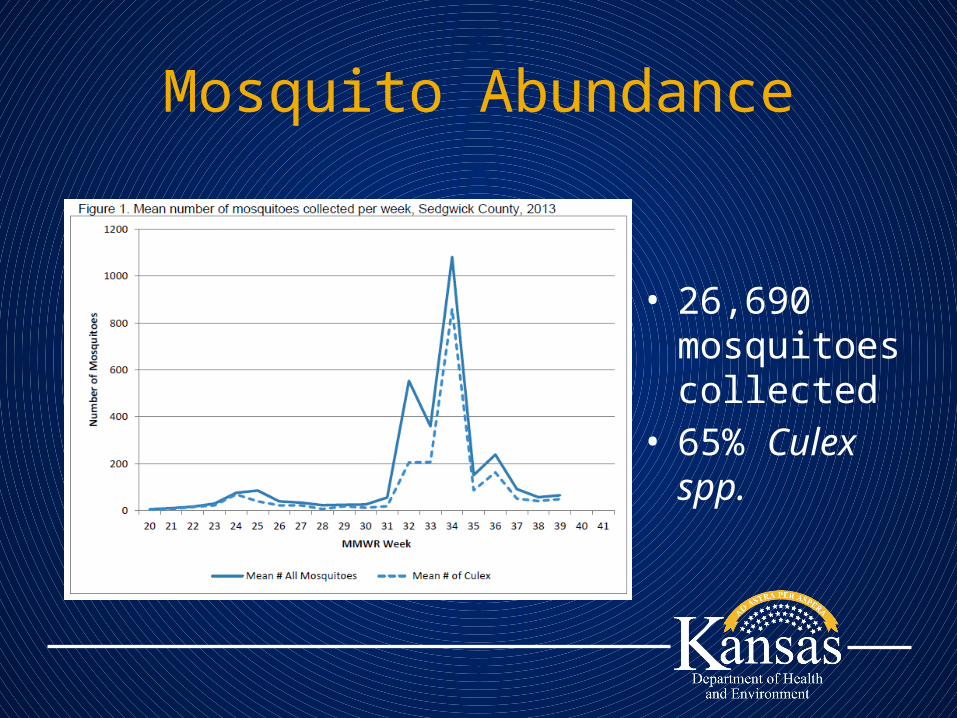
• 26,690 mosquitoes collected
• 65% Culex spp.

• 286 vials tested• 10.5% positive for WNV



Measures to Predict WNV Cases
• Vector Index (VI)– Quantify potential risk of transmission of WNV from
mosquitoes to humans– Requires three values to calculate
• Female mosquito vector presence• Vector species density• Vector species infection rate (need WNV lab data)
• Vector density– # female mosquito vectors/ # trap nights each week
• Vector density x infection rate = VI

Measures to Predict WNV Cases
• Need a measure that can be calculated quickly with the most current data
• We calculated 2 and 3 week prevalence estimates of Culex spp. and Vector Index (2013)
• Compared the number of human cases (Sedgwick County and the entire state) to the prevalence estimates

Average Number Culex spp. and Human Cases of WNV
• Strong correlation (R=0.82, 0.78) between the 2 & 3 week average number Culex and human cases that occur 2 weeks later among residents of Sedgwick County
• Strong correlation between the 2 week average number Culex and human cases occurring throughout the entire state 2,3, and 4 weeks later

Vector Index and Human Cases of WNV
• Weak correlation between VI and human cases of WNV in Sedgwick County
• Strong correlation (R=0.93) between VI and human cases of WNV throughout the entire state 3 & 4 weeks later
Results Translated
• We compared the average number of Culex mosquitoes using the 2 & 3 week prevalence estimates to determine an ‘action level’
• When the 3 week average number of Culex mosquitoes was above 44, human cases occurred 2 weeks later in Sedgwick County
• Therefore when the 3 week average approaches 44 some form of mitigation should take place
Limitations
• Unable to compare data before 2012 because of change in surveillance methodologies
• Difficult to make conclusions based on one year of data regarding a disease that has many factors that influence the number of cases (e.g. environmental factors, human behavior)
• Delay in reporting of human cases

Surveillance to Action
Mosquito Mitigation and Education
• Sedgwick County Health Department– Communicated mosquito surveillance data to
City of Wichita– Mosquito surveillance results used to determine
location of larvicide application• No adulticide used
– Fight the Bite Campaign• 210 posters• 1, 080 palm cards



• 2012-13 WNV neuroinvasive cases • Decreased 83% in U.S.• Increased 70% in Kansas• Decreased 60% in Sedgwick County

2014Count Rate
Sedgwick County 0 N/AKansas 18 0.62West North Central 104 0.50United States 1,347 0.42

What You Can Do…
• Review mosquito surveillance data– When Culex spp. > 40, issue press release
• Remind people to perform the 3 D’s
• Contact City Works Department– Determine what, if any, mosquito mitigation are
performed• Local mosquito surveillance ideal
– Larval surveillance?

Acknowledgements
KDHE• Amie Worthington, BEPHI • Brian Hart, KHEL• Alyssa Bigler, KHEL
KBS• Dr. Christopher Rogers
Sedgwick County Health Dept• Christine Steward• Adrienne Byrne-Lutz
City of Wichita• Scott Lindeback• Code Enforcement Staff• Citizens• Media

www.kdheks.govAmie Worthington, Medical Investigator
Ingrid Garrison, State Public Health VeterinarianBureau of Epidemiology and Public Health Informatics
Kansas Department of Health and Environment785-296-2898 [email protected]
785-296-2501 [email protected]
Healthy Kansans living in safe and sustainable environments.

References
• Selvar, MD, James M. "West Nile Virus: An Historical Overview." The Ochsner Journal 5.3 (2003): 6-10. Web.
• Centers for Disease Control and Prevention, Division of Vector-Borne Diseases. West Nile Virus in the United States: Guidelines for Surveillance, Prevention, and Control. 4th Revision June 14, 2003. Accessed October 22, 2014. http://www.cdc.gov/westnile/resourcepages/pubs.html
• "Anopheles Mosquitoes." Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. Web. 29 Oct. 2014.

WNV Clinical Criteria (2011)
• Neuroinvasive disease – Fever (≥100.4°F or 38°C) as reported by the patient or a health-
care provider, AND– Meningitis, encephalitis, acute flaccid paralysis, or other acute
signs of central or peripheral neurologic dysfunction, as documented by a physician, AND
– Absence of a more likely clinical explanation.• Non-neuroinvasive disease
– Fever (≥100.4°F or 38°C) as reported by the patient or a health-care provider, AND
– Absence of neuroinvasive disease, AND– Absence of a more likely clinical explanation

WNV Lab Criteria (2011)
• Isolation of virus from, or demonstration of specific viral antigen or nucleic acid in, tissue, blood, CSF, or other body fluid, OR
• Four-fold or greater change in virus-specific quantitative antibody titers in paired sera, OR
• Virus-specific IgM antibodies in serum with confirmatory virus-specific neutralizing antibodies in the same or a later specimen, OR
• Virus-specific IgM antibodies in CSF and a negative result for other IgM antibodies in CSF for arboviruses endemic to the region where exposure occurred, OR
• Virus-specific IgM antibodies in CSF or serum.

Case Classification - Probable
• Neuroinvasive diseaseA case that meets the clinical criteria for neuroinvasive disease and the following laboratory criteria: Virus-specific IgM antibodies in CSF or serum but with no other testing.
• Non-neuroinvasive diseaseA case that meets the clinical criteria for non-neuroinvasive disease and the laboratory criteria for a probable case: Virus-specific IgM antibodies in CSF or serum but with no other testing.
Case Classification - Confirmed
Neuroinvasive disease• Meets clinical criteria for neuroinvasive disease and one or more
the following laboratory criteria : Isolation of virus from, or demonstration of specific viral antigen or nucleic acid in, tissue, blood, CSF, or other body fluid, OR
• Four-fold or greater change in virus-specific quantitative antibody titers in paired sera, OR
• Virus-specific IgM antibodies in serum with confirmatory virus-specific neutralizing antibodies in the same or a later specimen, OR
• Virus-specific IgM antibodies in CSF and a negative result for other IgM antibodies in CSF for arboviruses endemic to the region where exposure occurred.

Case Classification - Confirmed
Non-neuroinvasive disease• Meets clinical criteria for non-neuroinvasive disease and one or
more of the following laboratory criteria for a confirmed case: Isolation of virus from, or demonstration of specific viral antigen or nucleic acid in, tissue, blood, CSF, or other body fluid, OR
• Four-fold or greater change in virus-specific quantitative antibody titers in paired sera, OR
• Virus-specific IgM antibodies in serum with confirmatory virus-specific neutralizing antibodies in the same or a later specimen, OR
• Virus-specific IgM antibodies in CSF and a negative result for other IgM antibodies in CSF for arboviruses endemic to the region where exposure occurred.