welcome to pedscases’ video on an approach to ...pedscases.com/sites/default/files/approach to...
TRANSCRIPT

WelcometoPedsCases’videoonanapproachtointerpreting pediatricchestx-rays.MynameisColinSiuandI’mamedicalstudentattheUniversityofAlberta.ThispodcastwasdevelopedwithDr.MelissaChan,apediatricemergencyphysicianandClinicalLecturerattheUniversityofAlbertaandStolleryChildren’sHospitalinEdmonton,Alberta,Canada
1
Theapproachthatwillbeexploredinthisvideoisthatofatoptobottomapproach.Wewillbeginbylookingatthethymus,followedbythemediastinum,heart,lungfields,diaphragmandendoffwithlookingatthebonystructures.
Thelearningobjectivesforthisvideoisto1)Demonstrateanapproachtointerpretingpediatricchestx-raysand2)Describedexpectedradiographicfindingsofcommonpediatricconditionsincludingcardiomegaly,pneumothorax,pleuraleffusion,pneumonia,asthma,cysticfibrosis,andnon-accidentalinjuries.
2

Thisvideoisaseriesofcasesthatwilltakeyoustepbystepthroughhowtointerpretapediatricchestx-ray.Wewillbeginbyunderstandingthecomponentsthatmakeupanadequatequalityfilmandthenmoveontotheactual interpretationofpediatricchestx-rays,movingthrougheachorgansystemwithatop-downapproach.Pleasefeelfreetopausethevideoatanypointifyouwouldliketotakeastabat interpretingthex-rayorcomingupwithadiagnosispriortothebigreveal.
Now,let’s jumprightintoit.Themostcommonlyorderedpediatricx-rayistheposterior-anteriorfilm.Aposterior-anteriororPAfilmispreferabletoananterior-posteriorfilmasthelattermayresultinamagnifiedheartshadow.APfilmsarereservedforsituationswherethepatientistoounstabletomoveandaportablemachine,whichcanonlyproduceAPfilms,isrequired.Firstly,checkthatthecorrectx-rayviewshavebeenobtainedandthatthefilmisthatofyourpatient.Beforeanalyzingthefilm,youmustensurethatthefilmisofadequatequality.Youcandothisbyexaminingforthreefactorswhichare:penetration,inspiration,androtation.Firstly,penetration.Youshouldbeabletoappreciatethethoracicspinethroughtheheart.(1)Ifthefilmisunderpenetrated,thelefthemidiaphragmwillnotbevisible.(2)Secondly,inspiration.Anadequatefilmwillshow9to10posteriorribs.(3)Pediatricchestx-raysmustbetakenwithasufficientinspiratoryeffortfromthepatientasafilmtakenonexpirationorwithminimalinspiratoryeffortmayexaggeratetheheartsizeandbronchovascularmarkings.Thirdly,rotation.Thespinousprocessofthevertebralbodyshouldbeequidistantfromthemedialendsof
3

theclavicle.(4)Additionally,ensurethatyouordertwoviewswhenorderinganypediatricchestx-raysuchasa lateralviewinadditiontoaPAview.Lastly,beawarethatlinesandtubesoftenappearonchestfilms– thoughtheywillnotbecoveredinthisvideo,it isimportanttorecognizewhattheyareandtonotmistakethemaspathologicalfeatures.
3

Soherewehaveourfirstcase(1):a6montholdboycomesinwithcough, feverandincreasedworkofbreathing.Achestx-rayisorderedforthispatient. Youascertainthatthisfilmisthatofyourpatient’s.Younotethatpenetrationandinspirationareadequateasthevertebralbodiesarevisiblethroughtheheartandthatapproximately8-9posteriorribsarevisible.Youconcludethattherotationisnormalastheclaviclesareequidistantfromthespine.Now,youcanbegininterpretingthefilmusingthetoptobottomapproach.Youstartatthetopandnotethatthereseemstobeincreasedopacityattherightupperlobeofthelung.Whatdoyouthinkthisrepresents?(2)
(3)This areaofincreasedopacityrepresentsthenormalthymusinapediatricpatient.Thethymusinapediatricpatientishighlyvariableinsizeandshape – itcanshrinkinsizefollowingillnessorincreasefollowingchemotherapy.Thethymusisnormallynotappreciableonfilmaftertheageof8.Inapediatricpatient,youmayappreciatethethymicsailsign– thisisanormalfinding.Thethymicsailsignisusuallyseenontherightmediastinum– therightthymusisseenasatrianglewithahorizontalfissureasthebaseofthetriangle,andthetwosidesofthetriangleconsistingofthetracheaandalineparallelingthechestwall. Incontrast,theSpinmakersailsignisanabnormalfindingindicativeofapneumomediastinum.(4)IntheSpinnakersailsign,thelobesofthethymusarelaterallydisplacedfromitspositionnearthetrachea.
4

(1)Oursecondcaseinvolvesa12yearoldchildthatpresentswithweight lossoverthelast6months.Thechestfilmisslightlyunderexposedasthevertebralbodiesarenotvisiblethroughtheheart.9-10posteriorribsarevisible,andtheclaviclesareequidistantfromthespine.Let’s takeastabatinterpretingthischestx-ray.Arethereanyabnormalitiespresentonthefilmandwhatisyourdiagnosis?
Firstly,werememberthatbecausethispatientis12yearsold,wedonotexpecttoseethethymusonthischestfilmandindeeditisnotvisible.Onthefilm,itseemsasthoughthere’sanopacityattherightlowerlobeofthelungandthehilarvesselsalsoseemmoreprominentaswell.Whatisthepathologybehindthis?Let’s findout!(2)
(3)Thissectionwillgoovertheidentificationofmassesinthemediastinum.First,weneedtoascertainthatthemassisindeedintra-mediastinal.Intra-mediastinalmassesdonotcontainairbronchograms,andhaveobtusemarginswiththelungs.Incontrast,alunglesionwillcreateacuteangleswiththelung.
Themediastinumisdividedintotheanterior,middleandposteriorsections.Themiddlesectioniscomprisedofthegreatvessels,tracheaandesophagus.Certaincluesareimportanttorememberinordertolocalizeamediastinalmasstooneofthesethreesections.Posteriordeviationofthetrachea,obliteratedcostophrenicangles,effacement oftheascendingaorta,andvisualizationofthehilarvesselsthroughthemass,suchasinourpatient,areindicativeofananteriormediastinal
5

mass.Withtheanteriormediastinum,amnemoniccalledtheterribleT’scanbeusedtorememberthedifferentialdiagnosis.ThefiveT’sconsistofthethymustumours,teratomaandgermcelltumours,thyroidtumours,thoracicaortaandterriblelymphoma.Furtherinvestigationsdoneforourpatientshowedthattheyhadlymphoma.(4)Lateraldeviationofthetracheaandwideningoftheparavertebrallineareindicativeofamiddlemediastinalmass.Lastly,thesplayingordestructionoftheposteriorribsandextensionofthemassabovethesuperiorclavicleareindicativeofaposteriormediastinalmass.(5)IncaseswherethelocationofthemassisuncertainafterthereviewofPAfilms,alateralfilmwillhelptofurtherdelineatethelocationofthemass.
5

(1)Ournextpatientisa3montholdcominginwithrespiratorydistress,coughandfailuretothrive.Onx-ray,thespinalvertebraearevisible,9-10posteriorribsareseen,andtheclaviclesareequallyspacedfromthespine.Thoughthethymusmaybeseeninachestx-rayfilmfora3monthold,it isnotseenhere.Therearenoopacitiesvisibleinthelungfieldsthatpointtowardsamass.However,theheartlooksa littlebitabnormal,doesn’tit?(2)
(3)Inapediatricpatient,theheart’swidthmayoccupyupto60%ofthemediastinum.However,ourpatient’sheart’swidthisdefinitelymorethan60%ofthediameterofthemediastinum,thusindicatingcardiomegaly.Commonpediatriccausesofcardiomegalyincludecongenitalheartdisease,cardiomyopathy,congestiveheartdiseaseandpericardialeffusions.Anecho-cardiogramisoftenorderedasafollow-updiagnostictoolifcardiomegalyisappreciated.
6

(1)The nextpatientisurgent:aweekoldinfantwithworseningcyanosis.Astatx-rayisorderedforhim.Youquicklyascertainthatthechest isadequatebycheckingpenetration,inspirationandrotation,allofwhicharenormalinthisfilm.Thethymusisnotpresentandtherearenoabnormalmassespresentinthefilm.Theheartseemsalittle largerthan60%ofthemediastinum’sdiameterbutmoreimportantly,younoticethattheshapeoftheheartlooksalittlebitoff.Whatisyourworkingdiagnosisatthispoint?(2)
(3)Therearealsosome congenitalcardiacconditionsthatarereadilyrecognizableonchestfilmsandthatstudentsshouldcommittomemory.Thefirstisthatfoundinourpatient:theboot-shapedheart,asignsynonymouswithadiagnosisoftetralogyofFallot.TetralogyofFallotreferstothefourdefiningcharacteristicsoftheconditionincludingaventricularseptaldefect,pulmonarystenosis,overridingaorta,andrightventricularhypertrophy.Next,isthetranspositionofthegreatarteries,aconditionthatresultsintheeggonastringsign.(4)Transpositionofthegreatarteries,isthemostcommoncyanoticcongenitalconditionfoundinnewbornsandischaracterizedbyapulmonaryarterythatarisesfromtheleftventricleandanaortathatarisesfromtherightventricle.Theenlargedheartappearsasaneggthathasbeenlaidonitssidewhilethestringisthemediastinumthathasbeennarrowedbythymicatrophyandlunghyperinflation.
7

(1)Youpreceptorasksyoutoseethenextpatientandtellsyouthattheyhaveadiagnosedmedicalcondition.However,shewantstoseeifyoucanfigureoutwhattheirmedicalconditionisbylookingattheirchestx-ray.Lookingatthex-ray,younotethatthefilmmaybealittlebitunderpenetratedasthevertebralbodiesareinvisible.Atthesametime,thelungfieldsalsolookdarkerthannormalandyouwonderifthereareanyelementsofover-penetrationhere.However,youmovealongandfindthattheinspirationandrotationarenormalforthisfilmbutfindthatthelungsfieldslooktallerthannormal.Youdonotseeathymus,noranymassesandtheheartseemstobeofregularsizeandshape.Yourevisityourpreviousfindingsofahyperlucentlungwithenlargedlungfields.Whatdoyouthinkisthepatient’smedicalcondition?
Allexaminationsofthelungsonchestx-raysshouldstartbyfirstlylookingatareasofdifferinglucency.(2)Thelungsshouldappearblackonmostfilms.Normallungsshouldincludethinwhitelungmarkingsthatextendalmosttotheperipheryofthelungfields.Diffuse bithoracicincreasedtranslucencymaybepresentinawellpatientwhohastakenabiggerbreathorwithover-exposureofthefilmbutmayalsobeobservedinpatientswithasthma,bronchiolitis,cysticfibrosisoranupperairwayobstruction.Inourpatient’scase,thediffusebithoracichyperlucencyisaradiologicfindingoftheirdiagnosedcysticfibrosis.Anotherfeatureofcysticfibrosisthatmaybeappreciatedinourpatient’sfilmisthatofanincreaseinbronchovascularmarkingsintheperihilarregion.Furthermore,bronchiectasisisalsoseeninchestfilmsofpatients
8

withcysticfibrosis.Ahypolucentlungmayresultfromatelectasis orobstructionofthebronchus.Thepresenceofunequaltranslucencybetweenthethoraceswarrantsseriousinvestigation.Patientrotationisthemostcommonreasonforunequaltranslucency,inwhichcase,astraightradiographshouldberedone.Withunequaltranslucencies,thesidethatisabnormalisthesidewithdecreasedpulmonaryvascularity,thesidewhichchangesmoreonexpiration,orthesidewithasmallcompletelyopaquehemithorax.
8

(1)Thefollowingpatientisa3dayoldneonatethatpresentswithworseningrespiratorydistressandnormalbloodpressurewhileoncontinuouspositiveairwaypressureorCPAP.Achestfilmisordered.ThePAuprightfilmiswell-penetratedasthevertebraearevisible,9-10posteriorribsarevisibleandtheclaviclesareequidistantfromthespinousprocess.Thethymusisnotvisibleinthisfilmandnoobviousmassesarevisible.Theheart’swidthislessthan60%ofthemediastinumandhasanormalshape.Now,let’s lookatthelucencyofthelungs.Thereseems tobeanareaofhyperlucencyintherightupperlungandtherealsoseemstobeatubeofsortsinsertingintoapproximatelythesameregion.TherealsoseemstobeasmallerareaofhyperlucencyintherightlowerlungneartheR.hemidiaphragm.Asidefromthat,thechestx-raylooksprettynormal.Whatisyourworkingdiagnosisatthispoint?(2)
(3)Our3dayoldpatienthasapneumothorax.Apneumothoraxcanoccurasaresultoftraumainjurytothechest,asacomplicationofalong-standinglungcondition,orasaspontaneousidiopathicentity.Tallandthinadolescentmalesareatahigherriskofdevelopingspontaneouspneumothoracices.Pneumothoracicesinneonatesareoftenidiopathicinnaturebutarealsoassociatedwithcomplicationsofventilatortherapy.Aswithourpatient,apneumothoraxisvisualizedasanareaofradiolucencybetweenthechestwallandthelung;inotherwords,thisareaappearsdarkerwithnoapparentlungmarkings.Ourpatientalsohasachesttubethathasbeeninsertedinordertohelpdraintheair.Onasupinefilm,theairaccumulatesintheposterior
9

chestbutmaybepresentatthediaphragminearlystages,whileonanuprightfilm,suchaswithourcase,theairaccumulateinthelungapices. Inaddition,aneonatalpneumothoraxmayalsopresentwithamoresharplydefinedmediastinumanddiaphragmwhencomparedtothecontralateralside,thisisknownasanetchedheartbordersign.Theairinapneumothoraxmayalsoelevatethethymusfromthemediastinum,resultinginanangelwingappearance.(4)Thepresenceofahyperlucentordarkcostophrenicangleinapneumothoraxisknownasthedeepsulcussign.
If a pneumothoraxissuspected, alateraldecubitusfilmshouldbeobtainedwiththesideinquestionbeingthesidethatisfacingupwards.
9

(1)Phew,it’sbeenalongday!It’s abouttimeforlunchinyourclinicsofeelfreetochowdownonsomefoodwhilewegooverthenextpatient’schestfilm.We’reapproximatelyatthehalfwaymark!Whileyougrababite,let’s lookatournextpatient.Ournextpatientisa3yearoldthatcomesincomplainingofchestpainoninspirationaswellastachypnea,hehaspreviouslyhadahistoryofcoughandfeverforthelast10days.Let’s takealookatthex-ray!Thevertebraearevisiblethroughtheheart,9-10ribsarevisibleandtheclaviclesareapproximatelyequidistantfromthespine.Thethymusisnotvisualizedandnoobviousmassesarepresent.It ishardtocommentontheheartsizeandshapebecauseofthehypolucencyobscuringtheleftheartmargin.Upongrossexaminationofthefilm,themostremarkablefindingistheunilateralhypolucencypresentdiffuselyintheLlung.Moreso,theRlungfieldseemstobedecreasedandtheheartseems tobeshiftedtowardstherightside.Whatisyourworkingdiagnosis?(2)
(3)Ourpatientherehasapleuraleffusionasaresultofacomplicationofapreviouspneumonia.Asseenonourpatient’sfilm,ahemithoraxonsupinefilmthatisdiffuselyhazyorhasincreasedopacitymaybeindicativeofapleuraleffusion.Largepleuraleffusionsmayshiftthemediastinumtothecontralateralside.Ifapleuraleffusionissuspected,anultrasoundofthechestshouldbecarriedouttodeterminewhetherthefluidisconfinedtooneareaorfree-moving,thelatterofwhichlendsitselftopercutaneousdrainage.Anultrasoundwillalsohelpdeterminethequantityandqualityoftheeffusion.Effusionspresentinthepleuralcavitymaybean
10

empyema,collectionsofpus,ahemothoraxresultingfromchesttrauma,oranexudativeeffusionfromadiseasednearbystructure,whichincludessubdiaphragmaticabscesses,pericarditis,andpancreatitis.Theonlyrealisticwaytodifferentiatethesedifferenttypesofeffusionsistoconductathoracocentesisandpleuralfluidanalysis.
10

(1)Next,wehavean8yearoldboythatpresentedwithfever,coughandlethargy.Youstartoffbycheckingthatthefilmisfortherightpatient.Thenascertainthatthefilmisofadequatequalitybycheckingthepenetration,inspiration,androtation.Allofthesethreecomponentsarefinewiththisfilm.Youstartanalyzingthefilmwithatop-downapproachstartingwiththethymuswhichisnotvisualized,themediastinumandtheheart,allofwhicharenormal.Nowlet’s takealookatthelungs.Thepulmonaryvesselsareclearlydemarcatedandtapergradually,butyounoticeanareaofhypolucencyintherightupperlungfield.Therearenoassociatedsignsofpneumothoraxorappreciablepleuraleffusion.Nowlet’stakeacloser lookatourareaofhypolucency.Theopacityiswell-circumscribedwithnocentralcavity.Whatisyourworkingdiagnosishere?(2)
(3)Pulmonarynodulesarediscreteareasofopacitywithinthelung.Ofthese,theroundpneumoniaisthemostcommontypeofsolitarylesioninthepediatricpopulation.Ourpatientdoesindeedhavearoundpneumoniabutyourdifferentialforapulmonarynodulemayalsoincludeabronchogeniccyst,apleuralfibromaorafungalinfection.Thepresenceofanairbronchogramwithinanopacitylendsitselftothediagnosisofabacterialpneumonia.Anairbronchogramiswhenanormallydarkair-filledbronchiismadevisiblebytheopacificationofsurroundingalveoli.Roundpneumoniaismostcommonlypresentinthoseunder8,islocatedinthelowerlobe,andispresentwithoutanyotherchestwallabnormalities.Pneumococcal infectionistheculpritinthemajorityofroundpneumoniacases.(4)Thefilmontherighthand
11

sidewas takenafter10daysandshowsresolutionoftheconsolidationafterempiricAmoxicillintreatment.
11

Thesubsequentpatientisa5yearoldpatientagaincominginwithafeverandacough.However,thisx-raylooksalittlebitdifferentfromourpreviousone.Let’swalkthroughthestepsagain.Thisfilmisagainwell-penetrated,8-9posteriorribsarevisualizedandtheclaviclesareequidistantfromthespinousprocess.Thethymusisnotvisualizedinthisfilmandtherearenoobviousmassespresent.Theheartseemstobeofnormalshapeandsize.Thereisnoassociatedsignsofpneumothoraxorpleuraleffusion.(1)Youdonoticehoweverthattheleftlowerlobeofthelungseemstobemorehypolucentthantherightandthereseems tobeabubble-likehyperlucencystructureamidsttheopacityintheleftlowerlung.Whatisyourworkingdiagnosisatthispoint?
Ourpatienthasanecrotizingpneumonia,characterizedbythepresenceofacavitywithinanopacity.Let’s quicklylookatanothercase.Herewehavea6yearoldsimilarlypresentingwithafeverandcough.(2)However,lookingattheirx-ray,wecanseethatthere’sbilateraldiffuseopacity.Viralpneumonia,suchasaRSVpneumonia,oftenpresentwithamoreill-definedorgroundglasspatternandareoftenbilateral.Asyoucansee,pneumoniamaypresentinmanydifferentshapesandforms.
12

Nowthatwe’vegoneoversomecasesofpneumonia.Let’s workonfindingswaytolocalizethepneumoniaonachestfilm.(1)TheSilhouettesignisveryhelpfulindeterminingthelocationoftheinfiltrate.TheSilhouettesignpointstothelossofthesilhouetteofkeystructuresnormallyseenonx-rayfilms.Thelossoftherightparatrachealstripesilhouettepointstoaninfiltrateintherightupperlobeofthelung,thelossoftherightheartborderpointstoaninfiltrateintherightmiddlelobeormedialrightlowerlobe,andthelossoftherighthemidiaphragmpointstoaninfiltrateintherightlowerlobe.(2)Thelossoftheaorticknucklecorrelateswithaninfiltrateintheleftupperlung,andlossoftheleftheartbordercorrelateswiththelingulasegmentsoftheleftupperlobe.Lastly,asvisualizedinthisfilm,lossofthelefthemi-diaphragmordescendingaortasilhouettecorrelateswithaleftlowerlobeinfiltrate.
Nowaquicktest.Canyoulocalizetheinfiltratethat ispresentonthischestx-ray?
Thispatienthasaleftlingulasegmentalpneumoniaasindicatedbythelefthypolucencyandlossoftheleftheartborder.
13

(1)Holdontight,we’reapproachingthehomestretch!Ournextpatientisa13yearoldthatcomesinwithshortnessofbreathandincreasedworkofbreathing.Let’stakeaquicklookathisx-ray.Thevertebraearevisiblethroughtheheartandtheclaviclesareequidistantfromthespine.However,inspirationseemstobeabitabnormalas11to12ribsarevisibleonthefilm.Holdontothisthought,we’llrevisitthisinabit.Asexpected,thethymusisnotvisualizedinthis13yearold.Therearenomassesapparentinthemediastinumandtheheartisofnormalshapeandsize. Inlookingatthelucencyofthefilm,itisabithardtoappreciateinthephotographbutthereisanareaofdecreasedlungmarkingsintherightapical lungthatwasdeterminedtobeasmallpneumothorax.Therearenosignsofapleuraleffusionorpulmonarynodules.Let’s gobacktoourearlierfindingregardingthepresenceof11-12ribsonthefilm.Furthermore,younoticethatbothhemi-diaphragmsseemabitmoreflattenedthannormal.Whatmedicalconditioncanresultinthispresentation?(2)
(3)Aflatteneddiaphragmismostoftenduetoanoverinflatedlung,asseenwithourpatient.Ourpatientactuallyhasunderlyingchronicasthmathathasresultedinhyperinflationofthelungsandflatteningofthediaphragm.Anotherfeaturethatmaybepresentinx-rayfilmsofasthmaticpatientsisthatofperibronchialcuffingorthickeningofthebronchialwalls.Youmaybeabletoappreciateonourpatient’sfilmthatthebronchialwallsaremoreapparentthanonanormalfilm.
14

Let’s takeafurtherlookatotherpathologiesthatmayaffectthediaphragm.Whenexaminingthediaphragm,firstlooktoseeifbothsidesareequal,thoughtherightdiaphragmmaybeslightlyhigherthantheleftduetothepresenceoftheliver.Thediaphragmisusuallyvisibleatthelevelofthe9th or10th rib.Curvingofthediaphragmmayresultfromphrenicnerveparalysis,liverenlargementoranabdominaltumour.Lossofclarityintheareaofthediaphragmismostlikelyduetopulmonarycollapseoraconsolidationobscuringthediaphragm.Alsoexamineforthepresenceoffreeairunderneaththediaphragm.Amarkedelevationofthediaphragmmaybeduetoalossoflungvolume,paralysisofthephrenicnerve,replacementofdiaphragmaticmuscleswithfibroelastic tissues,acongenitaldiaphragmaticherniaorsubpulmonaryeffusion.
14

(1)Phew,thatwasalongday.Herecomesyourlastpatientoftheday:aninfantcomesintoEmergencyandtheparenttellsyouthathefelloffthecouch,hithisheadandhadaseizureathome.Younoticesomebruisesonhisanteriorthoraxinyourphysicalexamandyoudecidetoorderachestx-ray.Thevertebraeareclearlyvisiblethroughtheheart,8-9ribsarevisibleandtheclaviclesareequi-distantfromthespine.Pleasenotethatthisfilmhasbeendarkenedinordertoenhancethepathology.Thethymusisnotvisualizedandnomassesareseen.Theheartisanormalsizeandshape.Therearenoareasofhypo- orhyperlucencyandnosignsofapneumothorax,pleuraleffusionorpneumonia.Thediaphragmsdonotseemtobeflattenedorelevated.Let’s nowtakeacloserlookattheribs.Whatabnormalitiesdoyouseeandwhatisyourworkingdiagnosis?(2)
(3)Whenlookingattheribs,usually10-12ribsshouldbeappreciated.Theribsareimportantindicatorsforpossiblechildabuse,morecorrectlytermednon-accidentalinjuries.Postero-medialribfractures,whicharepresentinourpatient’sfilm,especiallyhavehighspecificityfornon-accidentalinjuriesinchildrenunder3.Otherlesscommoncausesofribfracturesincludetraumaduringbirthdeliveryorinamotorvehicleaccidentortraumaininfantswithfragilebones.Fracturesofthescapula,spinousprocessandsternumarealsospecificfornon-accidentalinjuriesbutlesscommon.Ifthesesignsareseenonachestfilm,lookforothersignsthatarehighlycorrelatedwithnon-accidentalinjuriesincludingmultiplefractureselsewhereinthebody,fracturesindifferentstagesofhealing,delayinseekingmedical
15

treatment,andothercoexistinginjuries.Thoughhospitalprotocolsmayvaryinregardstoreportingnon-accidentalinjuries,itisquintessentialthatanysuspicionsbereportedtochildprotectionservicesoranequivalentagencyatyourhealthcarecentre.
Otherribanomalies includebifidribsthatareoftenpickedupinthepediatricpopulationandpresentasanasymptomatichardmass.(4)Additionally,lookforexpandedanterioredgesintheribs– amarkerofrickets.Destructivebonelesionsmaypointtothepresenceofinfectionsormalignancies.
15

Let’s endwithaquickreviewofthesystemsthatwerecoveredinthisvideo.Firstlyremember tochecktheadequacyofthefilmbycheckinginspiration,penetration,androtation.Then,approachthefilmusingatopdownformat.TheappearanceofthethymusonachestfilmisnormalinpatientsuptoeightyearsofagebutthepresenceoftheSpinnakersignindicatesapneumomediastinum.Rememberthemediastinumcanbeseparatedintotheanterior,middleandposteriorcompartments;pathologyassociatedwitheachcompartmentwillappeardifferentlyonachestfilm.Torememberthedifferentialdiagnosisforananteriormediastinalmass,remembertheterribleT’s.Thenormalheartshouldbelessthan60%thewidthofthemediastinum.TetralogyofFallotisvisualizedasaboot-shapedheartwhiletransposition ofthegreatarteriesisvisualizedasaneggonastring.
16

Whenexaminingthelungs,lookforareasofdifferinglucencyinthelung.Apneumothoraxisseenasanareaofradiolucencybetweenthechestwallandthelung.Thepresenceofthedeepsulcussignalsopointstowardsthediagnosisofapneumothorax.Roundpneumoniaisthemost commontypeofsolitarylesioninthepediatricpopulationandtheSilhouettesigncanbeusefulindeterminingthelocationofthislesion.Apleuraleffusionisoftenvisualizedasahemithoraxthat isdiffuselyhazyorhasincreasedopacity.Largepleuraleffusionsmaycauseacontralateralmediastinalshift.
17

Forthediaphragm,checkthatbothhemidiaphragmsareatthesamelevelandlookforfreeairunderthehemidiaphragms.Lastly,lookforanylesionsordeformitiesintheribsandbeonthelookoutforcommonsignsofnon-accidentalinjuries.
18
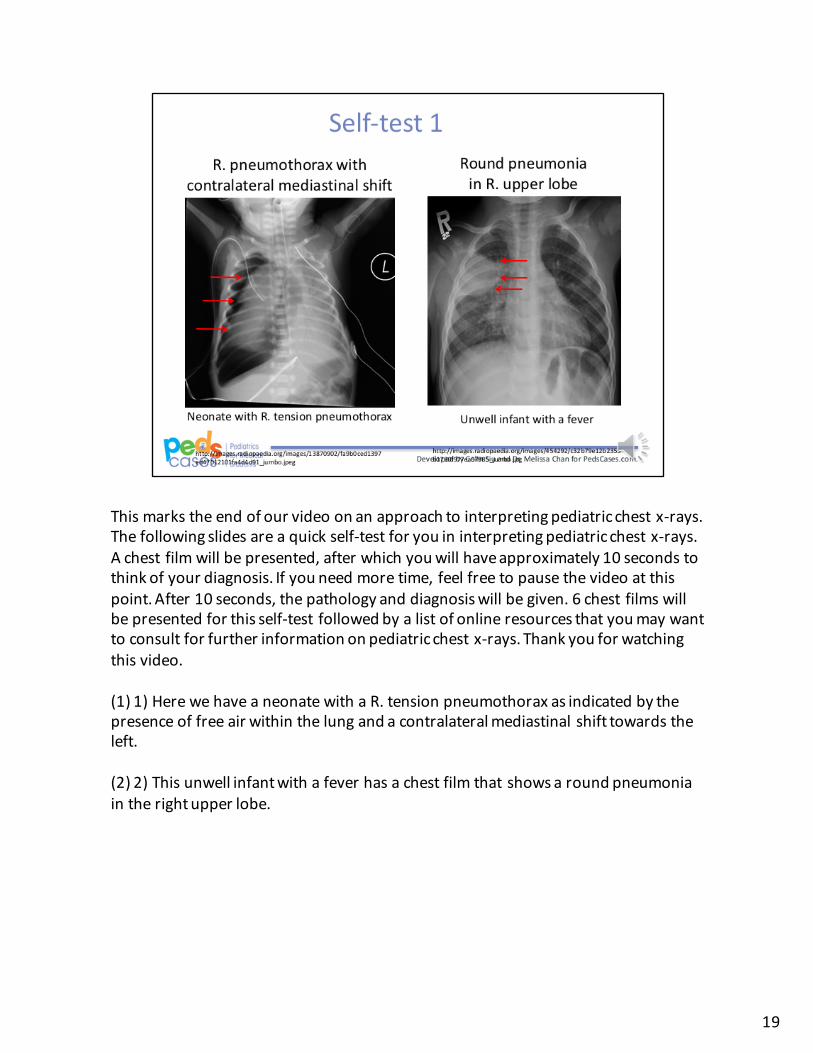
Thismarkstheendofourvideoonanapproachtointerpretingpediatricchestx-rays.Thefollowingslidesareaquickself-testforyouininterpretingpediatricchestx-rays.Achestfilmwillbepresented,afterwhichyouwillhaveapproximately10secondstothinkofyourdiagnosis.Ifyouneedmoretime,feelfreetopausethevideoatthispoint.After10seconds,thepathologyanddiagnosiswillbegiven.6chestfilmswillbepresentedforthisself-testfollowedbyalistofonlineresourcesthatyoumaywanttoconsultforfurtherinformationonpediatricchestx-rays.Thankyouforwatchingthisvideo.
(1)1)HerewehaveaneonatewithaR.tensionpneumothoraxasindicatedbythepresenceoffreeairwithinthelungandacontralateralmediastinalshifttowardstheleft.
(2)2)Thisunwellinfantwithafeverhasachestfilmthatshowsaroundpneumoniaintherightupperlobe.
19
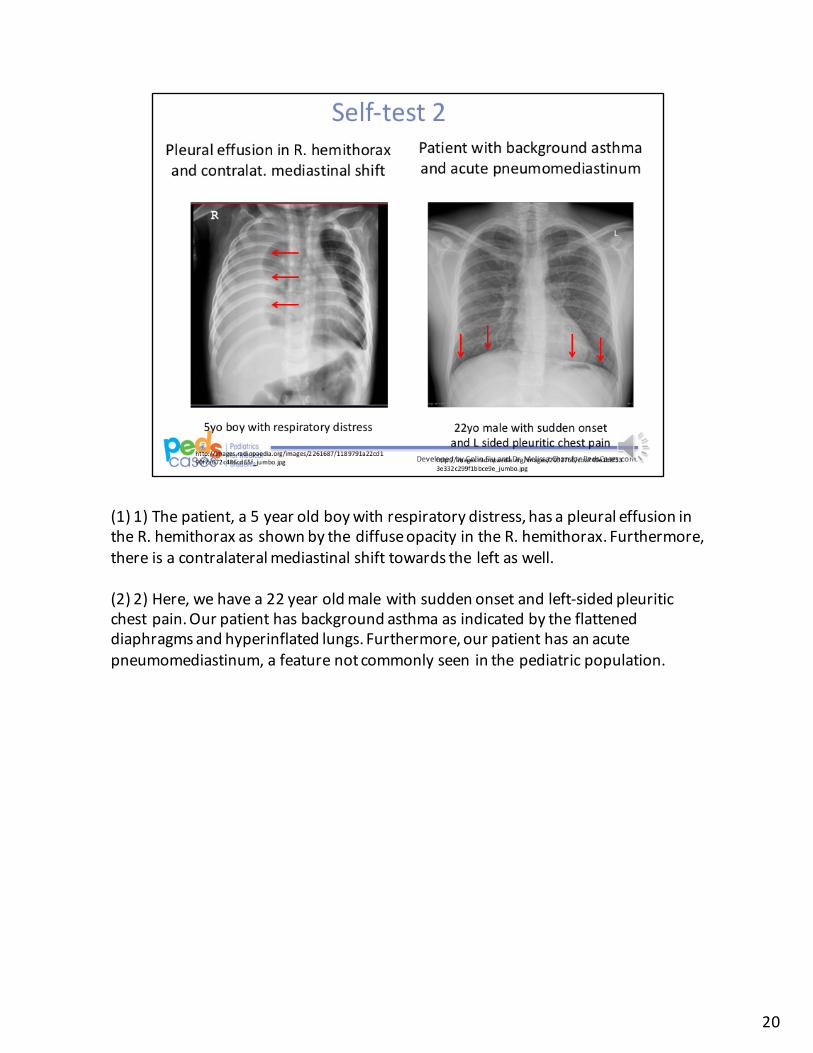
(1)1)Thepatient,a5yearoldboywithrespiratorydistress,hasapleuraleffusionintheR.hemithoraxasshownbythediffuseopacityintheR.hemithorax.Furthermore,thereisacontralateralmediastinalshifttowardstheleftaswell.
(2)2)Here,wehavea22yearoldmalewithsuddenonsetandleft-sidedpleuriticchestpain.Ourpatienthasbackgroundasthmaasindicatedbytheflatteneddiaphragmsandhyperinflatedlungs.Furthermore,ourpatienthasanacutepneumomediastinum,afeaturenotcommonlyseeninthepediatricpopulation.
20

(1)1)Thepatient,a5yearoldboy,showsaboot-shapedheartonhischestx-ray.Theboot-shapedheartispathognomonicforadiagnosisofTetralogyofFallot.Furthermore,thereisanassociatedR.sidedaorticarchvisualizedonthefilm.
(2)2)Lastly,wehaveafilmthatshowsexpansionoftheanteriorribendsatthecostophrenicjunctions.Thisispathognomonicforadiagnosisofrickets.
21
Formoreresourcesonplainradiographic films,pleasevisitradiopedia.org,theUCLAradiologywebsiteortheUniformedServicesUniversityoftheHealthSciences.
22

23

24