welcome busco, inc – arrow stage lines annual enrollment january 1, 2014
TRANSCRIPT
Welcome
Busco, Inc – Arrow Stage Lines Annual EnrollmentJanuary 1, 2014
Agenda - What we will cover
Review your Medical Plan Options for 2014 – UHC is updating their Certificate of Coverage.
2014 Updated Contribution limits for Health Savings Account (HSA)
Quick summary of other benefitsTimeline for enrollment changes

Medical Plans – Two options
Traditional Plan – Co-pay planQualified High Deductible Health Plan (QHDHP) with a Health Savings Account (HSA) – HSA Plan
Both are PPO plans – You save when you see a participating provider.
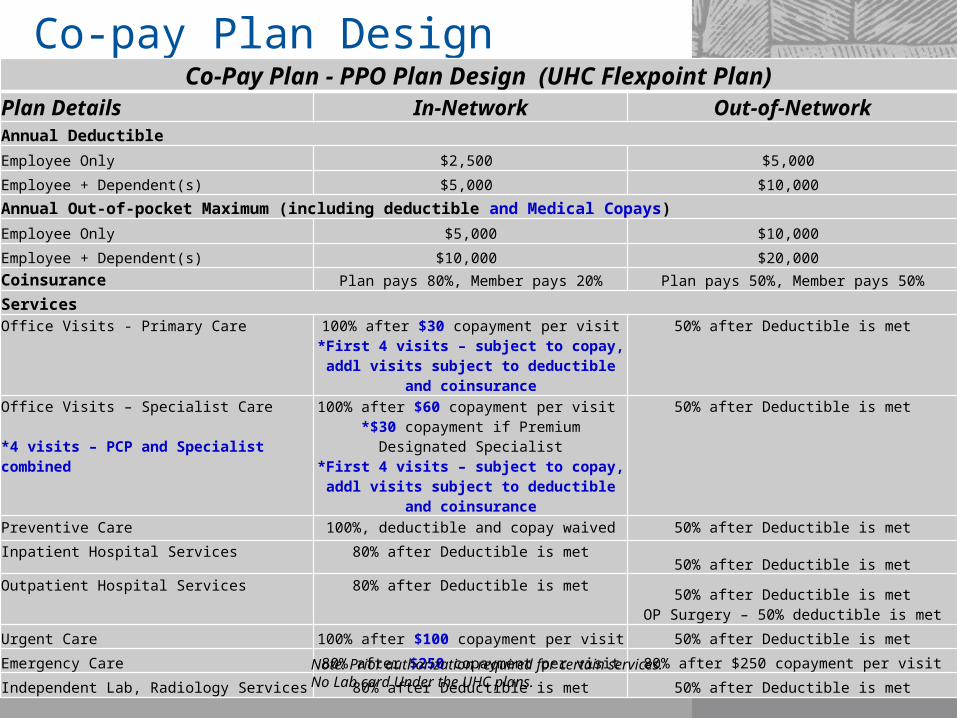
Co-pay Plan DesignCo-Pay Plan - PPO Plan Design (UHC Flexpoint Plan)
Plan Details In-Network Out-of-NetworkAnnual Deductible
Employee Only $2,500 $5,000
Employee + Dependent(s) $5,000 $10,000
Annual Out-of-pocket Maximum (including deductible and Medical Copays)
Employee Only $5,000 $10,000
Employee + Dependent(s) $10,000 $20,000 Coinsurance Plan pays 80%, Member pays 20% Plan pays 50%, Member pays 50%
ServicesOffice Visits - Primary Care 100% after $30 copayment per visit
*First 4 visits – subject to copay, addl visits subject to deductible and coinsurance
50% after Deductible is met
Office Visits – Specialist Care
*4 visits – PCP and Specialist combined
100% after $60 copayment per visit *$30 copayment if Premium Designated Specialist
*First 4 visits – subject to copay, addl visits subject to deductible and coinsurance
50% after Deductible is met
Preventive Care 100%, deductible and copay waived 50% after Deductible is met
Inpatient Hospital Services 80% after Deductible is met50% after Deductible is met
Outpatient Hospital Services 80% after Deductible is met50% after Deductible is met
OP Surgery – 50% deductible is met
Urgent Care 100% after $100 copayment per visit 50% after Deductible is met
Emergency Care 80% after $250 copayment per visit 80% after $250 copayment per visit
Independent Lab, Radiology Services 80% after Deductible is met 50% after Deductible is met
Note: Prior authorization required for certain services. No Lab card Under the UHC plans.
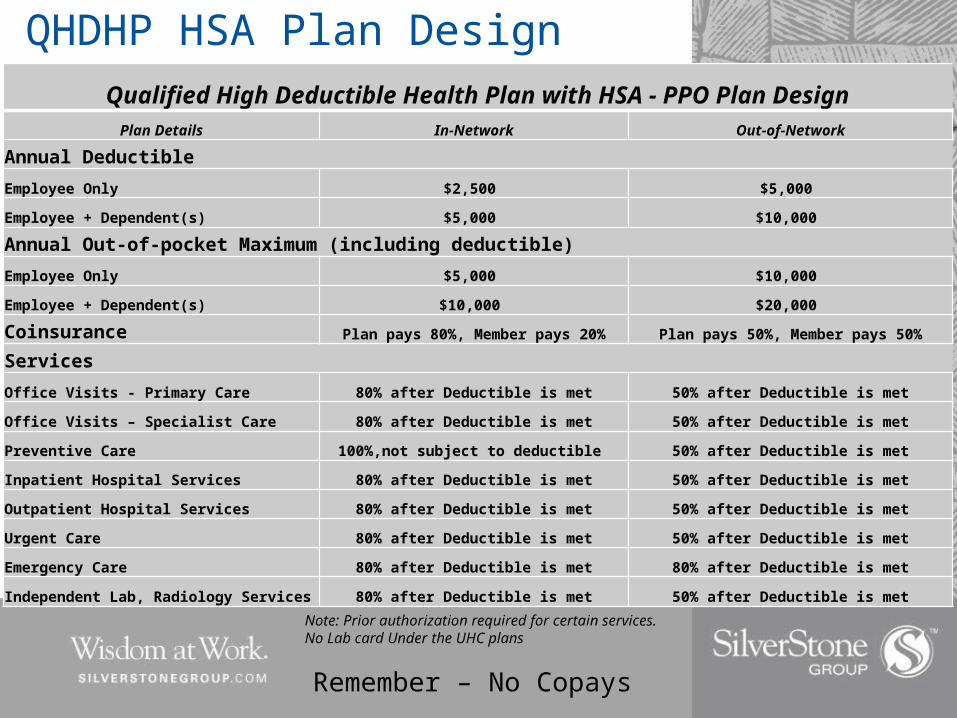
QHDHP HSA Plan Design
Qualified High Deductible Health Plan with HSA - PPO Plan DesignPlan Details In-Network Out-of-Network
Annual Deductible
Employee Only $2,500 $5,000
Employee + Dependent(s) $5,000 $10,000
Annual Out-of-pocket Maximum (including deductible)
Employee Only $5,000 $10,000
Employee + Dependent(s) $10,000 $20,000
Coinsurance Plan pays 80%, Member pays 20% Plan pays 50%, Member pays 50%
Services
Office Visits - Primary Care 80% after Deductible is met 50% after Deductible is met
Office Visits – Specialist Care 80% after Deductible is met 50% after Deductible is met
Preventive Care 100%,not subject to deductible 50% after Deductible is met
Inpatient Hospital Services 80% after Deductible is met 50% after Deductible is met
Outpatient Hospital Services 80% after Deductible is met 50% after Deductible is met
Urgent Care 80% after Deductible is met 50% after Deductible is met
Emergency Care 80% after Deductible is met 80% after Deductible is met
Independent Lab, Radiology Services 80% after Deductible is met 50% after Deductible is met
Remember – No Copays
Note: Prior authorization required for certain services. No Lab card Under the UHC plans
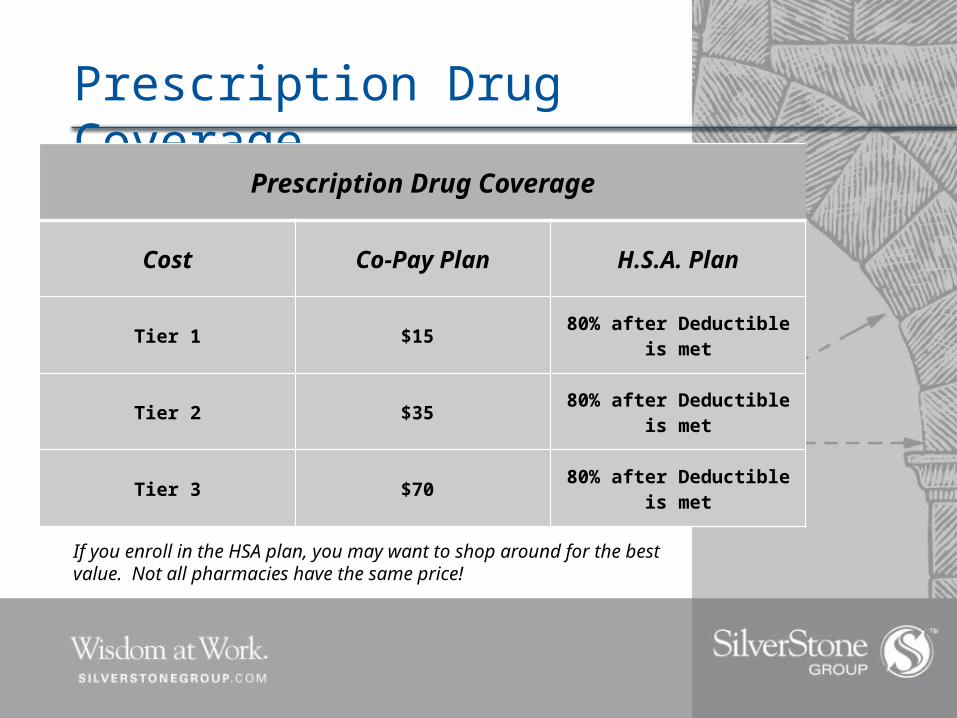
Prescription Drug Coverage
Prescription Drug Coverage
Cost Co-Pay Plan H.S.A. Plan
Tier 1 $15 80% after Deductible is met
Tier 2 $35 80% after Deductible is met
Tier 3 $70 80% after Deductible is met
If you enroll in the HSA plan, you may want to shop around for the best value. Not all pharmacies have the same price!
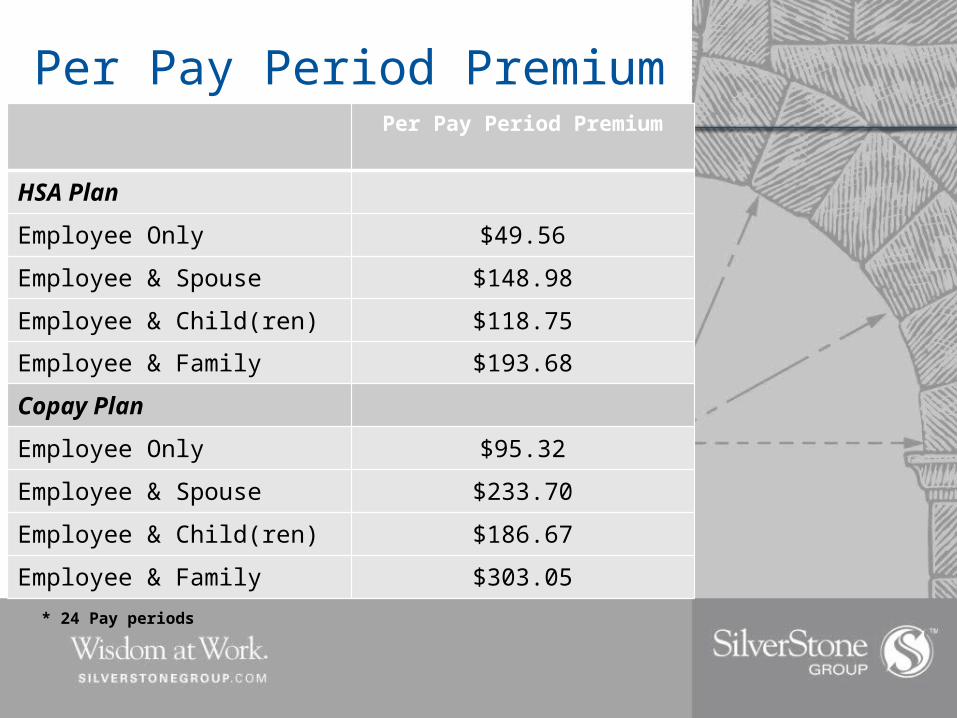
Per Pay Period Premium CostsPer Pay Period Premium
HSA Plan
Employee Only $49.56
Employee & Spouse $148.98
Employee & Child(ren) $118.75
Employee & Family $193.68
Copay Plan
Employee Only $95.32
Employee & Spouse $233.70
Employee & Child(ren) $186.67
Employee & Family $303.05
* 24 Pay periods

HSA CONTRIBUTIONS

HSA Contribution LimitsEach year, the IRS sets contribution limitsThese limits are for the total funds contributed, including company contributions, your contributions and any other contributions
For 2014, total limits are:$3,300 for individual coverage$6,550 for family coverage (all other coverage levels)Note: IF you enroll in the QHDHP - Arrow will contribute $125 into your HSA
accounts in January 2014. If you are age 65 or over and not eligible for the HSA account, Arrow will contribute $125 to an FSA account on your behalf

HSA Contributions
HSA Contribution amounts are flexible. Amounts can be changed monthly basis--you are not locked in for the year.
2014 Minimum Per Pay Period Contribution is $10.00
HSA Plan premium is less The savings in your premium deductions
should be contributed to your HSA accounts.
HSA Contributions
You are allowed to contribute the entire year’s limit whenever you first become eligible for the HSA (even if that is in December) However, you must remain eligible for at least 12 months
after that date, or you will be subject to taxes and penalties on the amount you contributed.
When contributing lump sums outside of payroll deductions, you must claim on your tax return to take advantage of the tax savings. Section provided on tax return – after tax contributions to HSA
Catch-Up Contributions
For individuals ages 55+, the IRS allows additional “catch-up contributions”
Eligible individuals may contribute an extra $1,000 for the year 2014
This is to help save additional money for retirement

Other Important Information
Arrow will continue to offer the Flexible Spending Accounts Health Care Spending Accounts (Full and Limited) Dependent Care Spending Account
You will receive an ID Card – Includes Medical and RX information. Be sure to share a copy with your pharmacy and physician the first time you see them in 2014.

Employee – Paid by Employer
Current Life Benefit: $15,000
Current AD&D* Benefit: $15,000*Accidental Death and Dismemberment
Basic Life and AD&D - LFG

Voluntary Term Life/AD&D- LFG (Employee Paid) Employee Coverage
Increments: $10,000
Maximum: Lesser of 4X annual earnings or $500,000
Guarantee Issue: $100,000
Dependent Coverage
Spouse (Employee participation required)
Increments: $5,000
Maximum: 50% of employee amount up to $250,000
Guarantee Issue: Less than 60 - $30,000: Over 60 – No GI
Child(ren) (Employee participation required)
Increments: $2,000
Maximum: $10,000 (19 years (23 if FT Student))
Guarantee Issue: $10,000
Voluntary Life Benefit
• This is your Annual Enrollment opportunity to make changes to your coverage amount, or request to enroll for coverage under the plan.
• This is NOT an open enrollment. If you did not enroll when you were initially eligible, you may request enrollment now, but your request will be subject to Evidence of Insurability.

Dental – UCCI (Slight increase in rates - Benefits stay the same)Covered Services:
Preventive Services (Deductible Waived)
Includes oral exams, cleaning, fluoride treatments, bitewing x-rays, sealants and space maintainers
100%Exams – 1 per 6 Months
Cleanings – 1 per 6 Months
Basic Services
Includes procedures such as fillings, extractions, oral surgery, general anesthesia, palliative treatment
80% after deductible
Major Services – 6 month waiting period for new hires
Includes crowns, bridges and dentures 50% after deductible
Orthodontia (Deductible Waived)
Children only up to age 19 50%$1,000 Lifetime Max (per insured)
Deductible (Applied to Basic & Major Services)
$50 ($150 family)
Maximum Benefit per Calendar Year $1,000 per insured for Preventive, Basic & Major Services combined
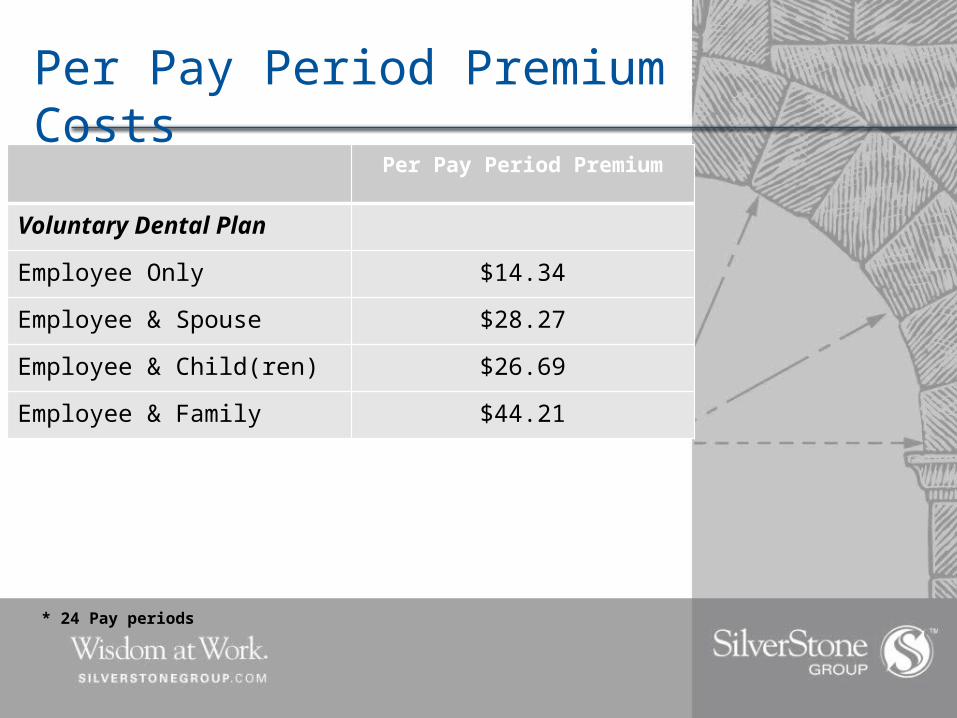
Per Pay Period Premium Costs
Per Pay Period Premium
Voluntary Dental Plan
Employee Only $14.34
Employee & Spouse $28.27
Employee & Child(ren) $26.69
Employee & Family $44.21
* 24 Pay periods
Voluntary Vision Plan - EyeMed
• Slight Rate increase and Benefits Stay the same• $10 copay for Exam with Dilation (Every 12 months)• Contacts - $115 Allowance Conventional and
Disposable• Frames - $100 Allowance (Every 24 Months)• Lens Allowances (Once every 12 Months):
• $25 copay for Single Vision • $25 copay for Bifocal• $25 Copay for Trifocal• $25 Copay plus 20% off retail less $55 allowance for
Standard Progressive
Refer to more detailed Plan Summary “Online”
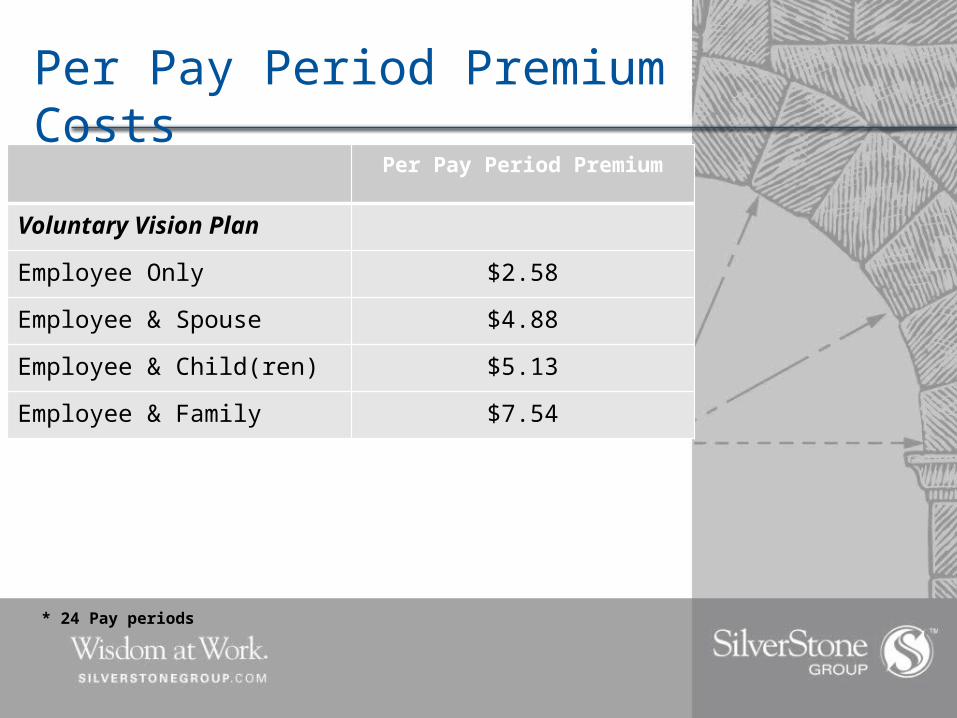
Per Pay Period Premium Costs
Per Pay Period Premium
Voluntary Vision Plan
Employee Only $2.58
Employee & Spouse $4.88
Employee & Child(ren) $5.13
Employee & Family $7.54
* 24 Pay periods

Other Benefits
myuhc.com – Your resource and access to relevant and helpful tools
Treatment Cost Estimator Provider Search Quicken Health Expense Tracker Cost & Quality Ratings Enhanced Personal Health Record Make sure you visit Health Care Lane!
Other Benefits Care24 – EAP
24/7 access to nurses or master’s level counselors
Health Education Medical Triage – 24/7
UHC’s Wellness Program – Simply Engaged (Watch for additional information)
Health Assessment (20 minute questionnaire) Online Coaching Healthy Mind, Health Body Newsletter Incentives from $75 to $350 for participating.
Other Benefits
Voluntary ProductsCancer
Hospital Supplement
Accident
Short Term Disability
Contact 1-877-282-0808 for product details and instructions how to enroll

All Employees should review and verify his or her name, address and dependent information by December 22, 2013.
Any changes in your benefit elections also need to be confirmed by December 22, 2013
REMEMBER – If you are currently enrolled in a medical option, you will default to your existing election if no benefit election is completed online.
If you are not enrolling, you must Waive coverage via the online enrollment system.
www.buscobenefits.com
ACTION ACTION
Questions?
Thank you for your attention!

Thank you!