weight reduction medications and programs
TRANSCRIPT

Weight Reduction Medications and Programs
Clinical Policy Bulletin:
Weight Reduction Medications and Programs
Number:Â 0039Policy
Note: Many Aetna plan benefit descriptions specifically exclude services and supplies for or relatedto treatment of obesity or for diet and weight control. Under these plans, claims for weight reductionmedications and for physician supervision of weight reduction programs will be denied based on thatexclusion. Please check benefit plan descriptions for details.
Aetna considers the following medically necessary treatment of obesity when criteria are met:
Weight reduction medications, and
Clinician supervision of weight reduction programs.
Weight Reduction Medications:
Note: Many Aetna benefit plans specifically exclude coverage of weight reduction medications underthe pharmacy benefit and/or under the health benefits plan. The medical necessity criteria set forthbelow do not apply to health plans that specifically exclude services and supplies for or related totreatment of obesity or for diet or weight control. Under these plans, claims for weight loss drugswill be denied based on this exclusion. For members whose medical policies do not exclude weightreduction medications or services and supplies for or related to weight reduction programs, Aetnacovers these drugs under the medical benefit, not the pharmacy benefit. Please check benefit plandescriptions for details.
Weight reduction medications are considered medically necessary for members who have failed tolose at least one pound per week after at least 6 months on a weight loss regimen that includes a lowcalorie diet, increased physical activity, and behavioral therapy, and who meet either of thefollowing selection criteria below:
Member has a body mass index** (BMI) greater than or equal to 30 kg/m²; or
Member has a BMI greater than or equal to 27 kg/m² with any of the following obesity-related riskfactors considered serious enough to warrant pharmacotherapy:
Coronary heart disease

Dyslipidemia:
Â
HDL cholesterol less than 35 mg/dL, or
LDL cholesterol greater than or equal to 160 mg/dL, or
Triglycerides greater than or equal to 400 mg/dL
Â
Hypertension (systolic blood pressure [SBP] higher than 140 mm Hg or diastolic blood pressure[DBP] higher than 90 mm Hg on more than one occasion)
Obstructive sleep apnea
Type 2 diabetes mellitus.
Weight reduction medications are considered experimental and investigational when these criteriaare not met.
**BMI = weight (kg) ¸ [height (m)]² http://www.nhlbi.nih.gov/guidelines/obesity/BMI/bmicalc.htm
The following medications have been approved by the FDA for weight reduction:
Benzphetamine [Didrex],
Diethylpropion [Tenuate],
Lorcaserin [Belviq],
Orlistat [Xenical, Alli],
Phendimetrazine [Bontril]Â
Phentermine [Adipex-P], and
Phentermine and topiramate [Qsymia].
For Aetna's clinical policy on surgical management of obesity, see CPB 0157 - Obesity Surgery.
Clinician Supervision of Weight Reduction Programs:
Up to a combined limit of 26 individual or group visits by any recognized provider per 12-monthperiod are considered medically necessary for weight reduction counseling in adults who are obese(as defined by BMI >= 30 kg/m2**). The number of medically necessary visits for obese childrenare left to the discretion of the member's physician.
** For a simple and rapid calculation of BMI, please click below and it will take you to the Obesity

Education Initiative:
BMI = weight (kg) ¸ [height (m)]² http://www.nhlbi.nih.gov/guidelines/obesity/BMI/bmicalc.htm
The following services are considered medically necessary for the evaluation of overweight orobese individuals:
Complete blood count
Comprehensive history and physical examination
Dexamethasone suppression test and 24-hour urinary free cortisol measures if symptoms suggestCushing's syndrome.
Electrocardiogram (EKG) -- adult
Glucose tolerance test (GTT)
Hand x-ray for bone age -- child
Lipid profile (total cholesterol, HDL-C, LDL-C, triglycerides)
Metabolic and chemistry profile (serum chemistries, liver tests, uric acid) (SMA 20)
Thyroid function tests (T3, T4, TSH)
Urinalysis
Very Low Calorie Diets (VLCD):
For obese members who have been prescribed a very low calorie diet (VLCD) (less than 799Kcal/day) (e.g., Optifast, Medifast), the following services are considered medically necessary for upto 16 weeks after initiation of the VLCD:
EKG after 50 lbs of weight loss; and
Lipid profile at the beginning and end of the VLCD program; and
Serum chemistries and liver function tests (SMA 20)Â weekly during the rapid weight loss phase ofthe VLCD, then every 2 weeks thereafter up to 16 weeks.
Note: VLCDs extending beyond 16 weeks are subject to medical review to determine if additionalservices are medically necessary.
Notes: Prepackaged food supplements or substitutes and grocery items are generally excluded fromcoverage under most benefit plans. Diagnostic tests required by, for or as a result of non-coveredweight loss programs (e.g., those not requiring physician supervision) are not covered. Pleasecheck benefit plan descriptions for details.
Excluded Services:

The following interventions are considered experimental and investigational for weight reduction:
Acupuncture for weight loss
Body plethysmography (diagnostic study)
Dual-energy X-ray (DEXA) body composition (diagnostic study)
Gastric electrical stimulation (see CPB 0678 - Gastric Pacing and Gastric Electrical Stimulation)
Human chorionic gonadotropin (HCG) or vitamin injections for weight loss
Indirect calorimetry (e.g., ReeVue Indirect Calorimeter) (diagnostic study)
Whole body calorimetry and composition is considered experimental and investigational for weightreduction and other indications.
Hospital confinement is considered not medically necessary for a weight reduction program.
Note: Under most benefit plans, the following services and supplies for weight reduction arespecifically excluded from coverage (please check benefit plan descriptions for details)
Exercise programs or use of exercise equipment
Rice diet or other special diet supplements (e.g., amino acid supplements, Optifast liquid proteinmeals, NutriSystem pre-packaged foods, or phytotherapy), see CPB 0061 - Nutritional SupportÂ
Weight Watchers, Jenny Craig, Diet Center, Zone diet, or similar programs.
Background
This policy is supported by NHLBI Guidelines on Diagnosis and Management of Obesity.
Weight reduction medications should be used as an adjunct to caloric restriction, exercise, andbehavioral modification, when these measures alone have not resulted in adequate weight loss.Factors influencing successful weight loss are: weight loss during dieting alone, adherence to diet,eating habits, motivation and personality.
Weight loss due to weight reduction medication use is generally temporary. In addition, the potentialfor development of physical dependence and addiction is high. Because of this, their use to aid inweight loss is not regarded as therapeutic, but rather involves a risk/benefit ratio, which makes itmedically inappropriate in most cases.
Individuals who cannot maintain weight loss through behavioral weight loss therapy and are at riskof medical complications of obesity are an exception to this; for these persons, the risk of physicaldependence or other adverse effects may present less of a risk than continued obesity. For suchindividuals, use of weight reduction medication may need to be chronic.
Tests with weight loss drugs have shown that initial responders tend to continue to respond, whileinitial non-responders are less likely to respond even with an increase in dosage. If a person does notlose 2 kg (4.4 lb) in the first four weeks after initiating therapy, the likelihood of long-term response

is very low. If weight is lost in the initial 6 months of therapy or is maintained after the initial weightloss phase, this should be considered a success and the drug may be continued.
Other than orlistat (Xenical), which is approved for use in adolescents aged 12 years or older, weightreduction medications have not been proven to be safe and effective for treatment of obesity inchildren and adolescents.  Orlistat (Xenical) is contraindicated in persons with chronicmalabsorption syndromes and cholestasis. Qsymia is contraindicated in pregnancy, glaucoma,hyperthyroidism, hypersensitivity to sympathomimetic amines, and within 14 days oftaking monoamine oxidase inhibitors. Belviq is contraindicated in pregnancy. Other drugs listedin this policy are contraindicated in the following conditions: hypertension, atherosclerosis,coronary artery disease, and stroke.
Ioannides-Demos et al (2006) stated that there is limited safety and effectiveness data foramfepramone (diethylpropion) and phentermine and their approvals for the management of obesityare limited to short-term use.  The authors stated that, although the benefit-risk profiles ofsibutramine and orlistat appear positive, sibutramine continues to be monitored because of long-term safety concerns. The safety and effectiveness of currently approved drug therapies have notbeen evaluated in children and elderly patient populations.
On October 8, 2010, Abbott Laboratories announced that that it was withdrawing its diet drugMeridia (sibutramine) from the United States, Australian and Canadian markets as a consequence ofheightened concerns that the medication can trigger heart attack or stroke, especially in patientswith underlying cardiovascular disease.
Dual-energy X-ray (DEXA) was developed for the diagnosis of osteoporosis and was employedoriginally to clinically significant locations of the forearm, femoral neck, and lumbar spine. Withbody composition measurements by means of DEXA, a controlled x-ray beam scans the entirebody to ascertain bone mineral content, body fat and lean tissue mass. The comprehensive viewof body composition provided by DEXA is thought to be the method of choice for evaluating bodycomposition by its advocates because of its speed, ease of application as well as relatively low-doseof ionizing radiation. Its purported uses entail determining appropriate nutritional supportduring disease progression and monitoring response to therapeutic interventions.
Available evidence does not support the use of whole body DEXA for managing obesity. There is alack of reliable evidence demonstrating that whole body DEXA measurement improves themanagement of persons with obesity over simpler methods of measuring body composition(including BMI and anthropomorphic measures), such that clinical outcomes are significantlyimproved. Published data have focused on the level of agreement between whole body DEXA andvarious other methods of measuring body composition, and on the use of DEXA as an endpoint inresearch studies. Well-designed studies are needed to assess the clinical value of whole bodyDEXA scanning (Ball and Altena, 2004; Williams et al, 2006; Ritz et al, 2007; Pineau et al, 2007;Pineau et al, 2009).
Balázs (2010) stated that the rapidly increasing prevalence of over-weight and diabetes mellitus is aserious global threat to healthcare. Nowadays, medicinal plants and natural treatments arebecoming more and more popular. Diabetes has historically been treated with plants or plant-derived formulations in different cultures, mainly in China, Asia and India. Different mechanisms forthe anti-diabetic effect of plants have been proposed: increased release of insulin, reduction ofintestinal glucose absorption, as well as enhancement of glycogen synthesis. The scientific evidencesfor most of these plants are still incomplete. The large market for plant remedies has resulted in anarray of unauthorized products or marketed as dietary supplements and, at the same time, no

reliable pharmaceutical-grade products are registered for this purpose.
Borel et al (2012) conducted a prospective intervention study in 104 viscerally obese men classifiedaccording to their glucose tolerance status. They were followed for one year while participating ina healthy eating-physician activity/exercise lifestyle modification program while their insulinsensitivity was tracked. The goals of the study were to evaluate glucose tolerance as well as toevaluate the respective contribution so fo changes in body fat distribution versus changes incardiorespiratory fitness (CRF) to the improvements in indices of plasma glucose/insulinhomeostasis. The results showed insulin sensitivity improved in assocication with decreases inbothvisceral (VAT) and subcutaneous adiposity (SAT) as well as improvement in CRF, regardless ofbaseline glucose tolerance. The results of this study also shoed that reduction in VAT wasassociated with an improvement in homeostasis model assessment of insulin resistance, whereasreduction in SAT was rather associated with improvement of the insulin sensitivity index ofMatsuda. The authors concluded that a one year lifestyle intervention improved plasmaglucose/insulin homeostasis in viscerally obese men, including those with normal glucose tolerancestatus at baseline.Â
Garvey et al (2012) conducted a placebo-controlled, double-blind, 52-week extension study toevaluate the long-term efficacy and safety of controlled-release phentermine/topiramate (PHEN/TPMCR) in overweight and obese subjects with cardiometabolic disease. Subjects were randomlyassigned to placebo, 7.5 mg phentermine/46 mg controlled-release topiramete, or 15 mgphentermine/92 mg controlled-release topiramate.  Of the 676 extension study participants, 84%completed the study. At week 108 PHEN/TPM-CR was associated with significant, sustainedweight loss. Significantly more PHEN/TPM CR-treated subjects at each dose achieved >= 5%, >=10%, >= 15%, and >= 20% weight loss compared with placebo (P < 0.001). The authors thereforeconcluded that PHEN/TPM CR, in conjunction with lifestyle modification, may provide a well-tolerated and effective option for the sustained treatment of obesity complicated by cardiometabolicdisease.
Mulholland et al (2012) stated that evidence from the literature supports the safe use of very-lo--energy diets (VLED) for up to 3 months in supervised conditions for patients who fail to meet atarget weight loss using a standard low-fat, reduced-energy approach.  There is, however, a needfor longer-term outcomes on obesity and associated morbidities following a VLED.  Theseresearchers investigated longer-term outcomes from studies using VLED, with a minimum durationof 12 months, published between January 2000 and December 2010.  Studies conducted in bothchildren and adults, with a mean/median BMI of greater than or equal to 28 kg/m2 were included. PubMed, Medline, Web of Science and Science Direct were searched.  Reference lists of studiesand reviews were manually searched.  Weight loss or prevention of weight gain and morbiditieswere the main outcomes assessed.  A total of 32 out of 894 articles met the inclusion criteria.  Theduration of the studies ranged from 12 months to 5 years.  Periods of VLED ranged from 25 d to 9months.  Several studies incorporated aspects of behavior therapy, exercise, low-fat diets, low-carbohydrate diets or medication.  Current evidence demonstrated significant weight loss andimprovements in blood pressure, waist circumference and lipid profile in the longer term following aVLED.  Interpretation of the results, however, was restricted and conclusions with which to guidebest practice were limited due to heterogeneity between the studies.  The authors concluded thatthe present review clearly identified the need for more evidence and standardized studies to assessthe longer-term benefits from weight loss achieved using VLED.
The ReeVue Indirect Calorimeter (KORR Medical Technologies, Salt Lake City, UT) was designed tomeasure an individual's oxygen consumption. Using this measurement, the device calculates aperson's resting energy expenditure (REE), also known as resting metabolic rate (RMR). Clinicians

supposedly can screen for abnormally low metabolic rates, teach energy balance, and identify theprecise caloric intake needed for weight loss. Clinical applications of the ReeVue IndirectCalorimeter include obesity treatment, as well as treating obesity related diseases such as diabetes,dysmetabolic syndrome X, hypothyroidism, hyperthyroidism, hypertension, cardiovascular disease,as well as sleep apnea. Under strict laboratory protocol, the ReeVue can also be used to measurebasal metabolic rate.
Fioravante et al (2012) evaluated nutritional status, body composition, and (REE in patients withchronic hepatitis C before and during treatment with pegylated interferon and ribavirin. This wasa prospective study with the evaluation of patients with hepatitis C virus before and after 12 weeksof treatment with pegylated interferon and ribavirin. The evaluation consisted of anthropometry(weight, height, BMI, and waist circumference), and body composition was determined bybioelectrical impedance analysis. The REE of each individual was obtained by indirectcalorimetry. To compare the 2 phases of treatment, the Wilcoxon test was used. The significancelevel was 5 %. Subjects had significant weight loss during treatment with a consequent decreasein BMI. This weight decrease was accompanied by a significant decrease in body fat and nodecrease in fat-free mass. There was a significant decrease in energy intake as assessed by 24-hour recall. However, there was no change in REE and in REE corrected for fat-free mass. Theauthors concluded that patients with hepatitis C treatment had significant weight loss and this wasnot associated with changes in energy expenditure.
Furthermore, an UpToDate review on "Palliative care: Assessment and management of anorexia andcachexia" (Bruera and Dev, 2013) states that "Handheld indirect calorimetry, which is more accuratethan equations at estimating basal energy needs but less precise than traditional devices used in theresearch setting, may be useful in the outpatient setting. Close to one-half of cancer patients beingevaluated in an outpatient cachexia clinic are noted to be hypermetabolic by indirect calorimetry. These assessments are appropriate in the research setting, but have little if any utility in the clinic".
Appendix
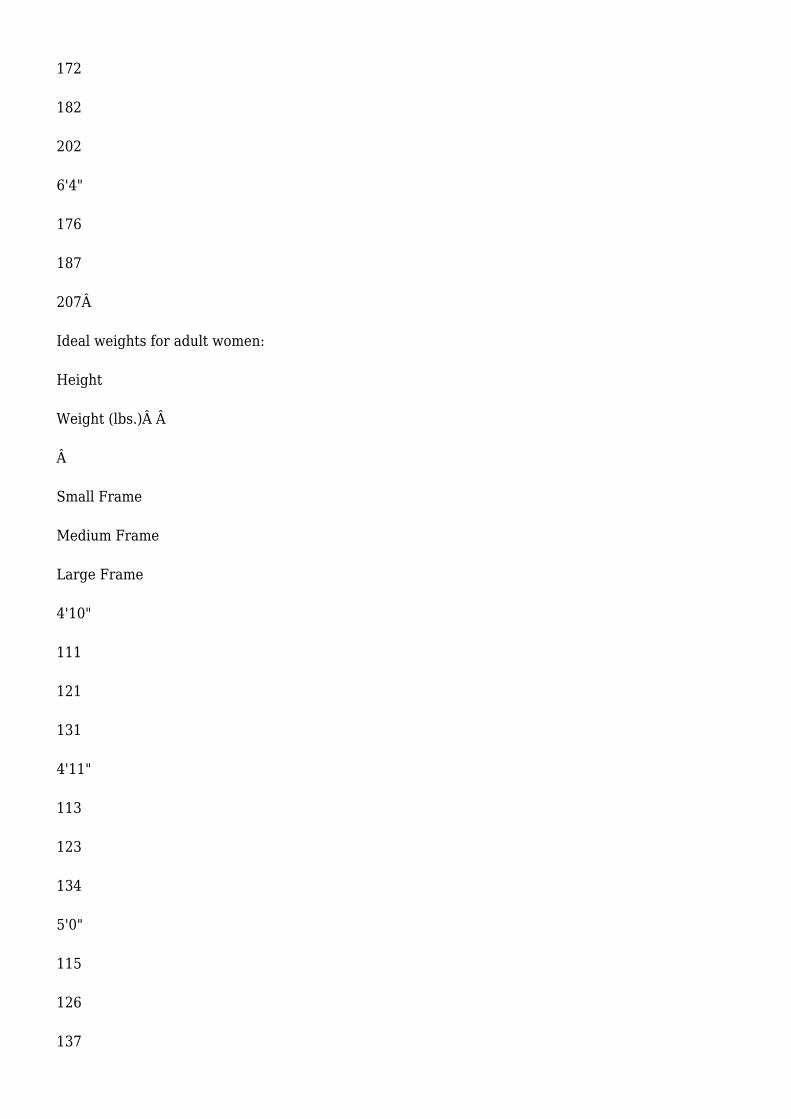
Ideal Weight Chart:
The following indicates maximum ideal weight in shoes with one-inch heels based on body frame andheight:
Ideal weights for adult men:
Height
Weight (lbs.)
Â
Small Frame
Medium Frame
Large Frame
5'2"

134
141
150
5'3"
136
143
153
5'4"
138
145
156
5'5"
140
148
160
5'6"
142
151
164
5'7"
145
154
168Â
5'8"
148
157

172
5'9"
151
160
176Â
5'10"
154
163
180
5'11"
157
166
184
6'0"
160
170
188
6'1"
164
174
192Â
6'2"
168
178
197
6'3"
172
182
202
6'4"
176
187
207Â
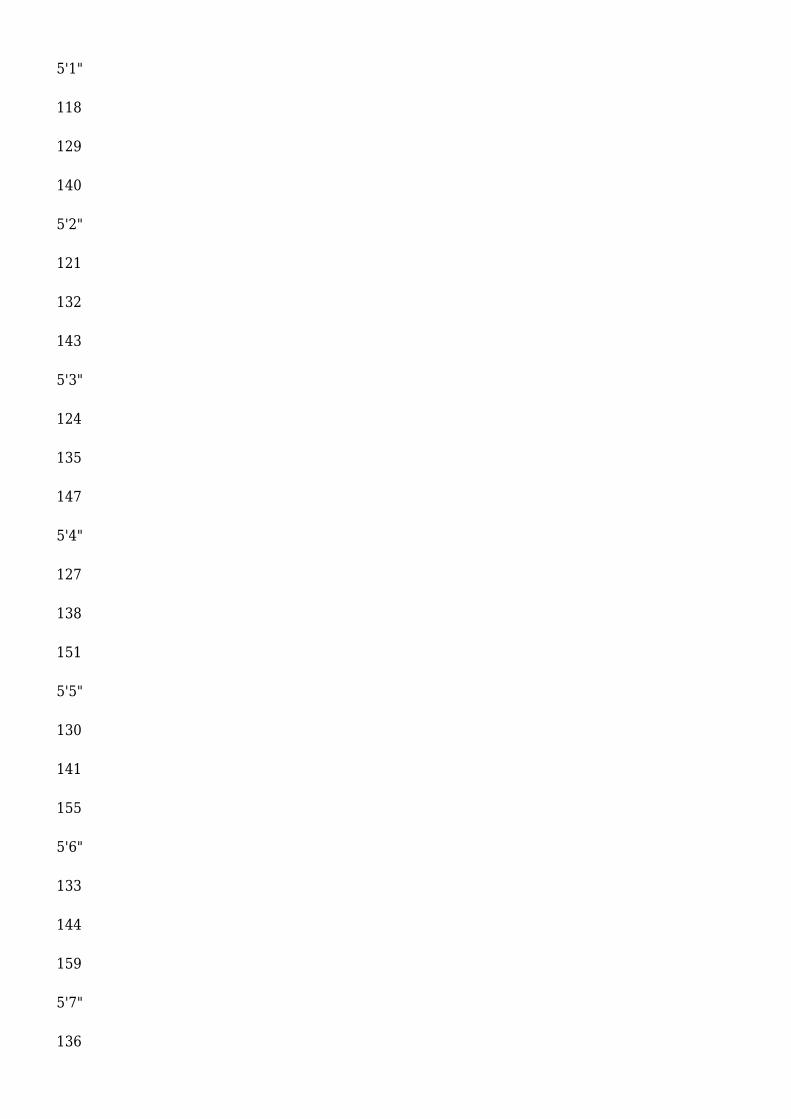
Ideal weights for adult women:
Height
Weight (lbs.)Â Â
Â
Small Frame
Medium Frame
Large Frame
4'10"
111
121
131
4'11"
113
123
134
5'0"
115
126
137
5'1"
118
129
140
5'2"
121
132
143
5'3"
124
135
147
5'4"
127
138
151
5'5"
130
141
155
5'6"
133
144
159
5'7"
136

147
163
5'8"
139
150
167
5'9"
142
153
170
5'10"
145
156
173
5'11"
148
159
176
6'0"
151
162
179
Â
CPT codes covered if selection criteria are met:
97802
97803

97804
CPT codes not covered for indications listed in the CPB:
94690
94726
97810
+ 97811
97813
+ 97814
Other CPT codes related to the CPB:
77072
80048
80053
80076
80418
80420
81000
81001
81050
82465
82530
82533
82951
82952
83718
83719
83721
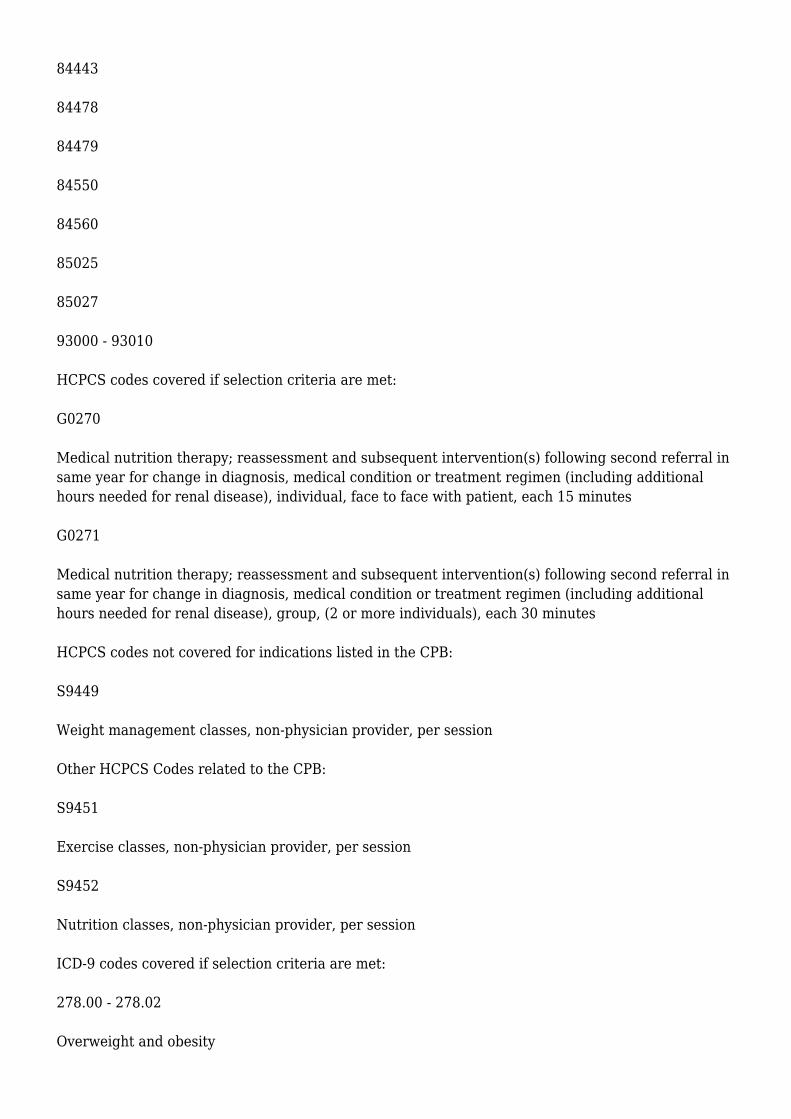
84443
84478
84479
84550
84560
85025
85027
93000 - 93010
HCPCS codes covered if selection criteria are met:
G0270
Medical nutrition therapy; reassessment and subsequent intervention(s) following second referral insame year for change in diagnosis, medical condition or treatment regimen (including additionalhours needed for renal disease), individual, face to face with patient, each 15 minutes
G0271
Medical nutrition therapy; reassessment and subsequent intervention(s) following second referral insame year for change in diagnosis, medical condition or treatment regimen (including additionalhours needed for renal disease), group, (2 or more individuals), each 30 minutes
HCPCS codes not covered for indications listed in the CPB:
S9449
Weight management classes, non-physician provider, per session
Other HCPCS Codes related to the CPB:
S9451
Exercise classes, non-physician provider, per session
S9452
Nutrition classes, non-physician provider, per session
ICD-9 codes covered if selection criteria are met:
278.00 - 278.02
Overweight and obesity

V85.23 - V85.44
Body mass index 27.0-70 and over, adult
Other ICD-9 Codes related to the CPB:
250.00, 250.02, 250.10, 250.12, 250.20, 250.22, 250.30, 250.32, 250.40, 250.42, 250.50, 250.52,250.60, 250.62, 250.70, 250.72, 250.80, 280.82, 250.90, 250.92
Diabetes
255.0
Cushing's syndrome
259.8 - 259.9
Other and unspecified endocrine disorders
272.0
Pure hypercholesterolemia
327.23
Obstructive sleep apnea (adult) (pediatric)
401.0 - 405.99
Hypertensive disease
414.00 - 414.9
Coronary atherosclerosis
783.1
Abnormal weight gain
783.6
Polyphagia
V85.0 - V85.22
Body mass index less than 19-26.9, adult
The above policy is based on the following references:
American Obesity Association, C. Everett Koop Foundation, and Shape Up America! Guidance fortreatment of adult obesity. Bethesda, MD: Shape Up America!; October 1996. Available at:

http://www.shapeup.org/sua. Accessed March 16, 2000.
Bra GA, Gray DS. Obesity. Part I. Pathogenesis. West J Med. 1988;149:429-441.
National Task Force on the Prevention and Treatment of Obesity, National Institutes ofHealth. Very low-calorie diets. JAMA. 1993;270:967-974.
National Task Force on the Prevention and Treatment of Obesity, National Institutes ofHealth. Long-term pharmacotherapy in the management of obesity.JAMA. 1996;276:1907-1915.
Foster DW. Gain and loss in weight. In: Harrison's Principles of Internal Medicine. 14th ed. ASFauci, E Braunwald, KJ Isselbacher, et al., eds. New York, NY: McGraw-Hill; 1998:244-246.
U.S. Department of Agriculture and U.S. Department of Health and Human Services. Nutrition andyour health: Dietary guidelines for Americans. 3rd ed. Home and Garden Bulletin. No. 232.Washington, DC: U.S. Government Printing Office; 1990.
Goldstein DJ, Potvin JH. Long-term weight loss: The effect of pharmacologic agents. Am J Clin Nutr.1994;60(5):647-657.
Silverstone T. Appetite suppressants: A review. Drugs. 1992;43(6):820-836.
United States Pharmacopeial Convention, Inc. Appetite suppressants (systemic). In: USP DI: DrugInformation for the Health Care Professional. 19th ed. Rockville, MD: United States PharmacopeialConvention; 1999: 452-459.
No author listed. Weight control. In: Introductory Nutrition and Diet Therapy. 2nd ed. MMEschleman, ed. Philadelphia, PA: J.B. Lippincott Co. ;1991;368.
No author listed. Metabolic drugs: Drugs used in obesity. In: AMA Drug Evaluations Subscription.DR Bennett, ed. Chicago, IL: American Medical Association (AMA); 1992: III/MET 6:7.
Scheen AJ, Desaive C, Lefebvre PJ. Therapy for obesity--today and tomorrow. Baillieres ClinEndocrinol Metab. 1994;8(3):705-727.
Bjorntorp P. Treatment of obesity. Int J Obes Relat Metab Disord. 1992;16(suppl 3):S81-S84.
Bray GA. Use and abuse of appetite-suppressant drugs in the treatment of obesity. Ann Intern Med.1993;119(7 pt 2):707-713.

Mosby-Year Book, Inc. Mosby's GenRx: TheComplete Reference for Generic and Brand Drugs.8th ed. St. Louis, MO: Mosby; 1998.
American Society of Health-System Pharmacists,Inc. American Hospital Formulary Service DrugInformation 98. Bethesda, MD: American Societyof Health-System Pharmacists; 1998.
U.S. Department of Health and Human Services,National Institutes of Health (NIH). Clinicalguidelines on the identification, evaluation, andtreatment of overweight and obesity in adults. National Heart, Lung, and Blood Institute andNational Institute of Diabetes and Digestive and Kidney Diseases. Bethesda, MD: NIH; June 1998.
Jarvis M, McNaughton L, Seddon A, Thompson D. The acute 1-week effects of the Zone diet onbody composition, blood lipid levels, and performance in recreational endurance athletes. JStrength Cond Res. 2002;16(1):50-57.
Haller C, Schwartz JB. Pharmacologic agents for weight reduction. J Gend SpecifMed. 2002;5(5):16-21.
Shepherd TM. Effective management of obesity. J Fam Pract. 2003;52(1):34-42.
Heshka S, Anderson JW, Atkinson RL, et al. Weight loss with self-help compared with a structuredcommercial program: A randomized trial. JAMA. 2003;289(14):1792-1798.
Institute for Clinical Systems Improvement (ICSI). Pharmacological approaches to weight loss inadults. Technology Assessment Report No. 71. Bloomington, MN: ICSI; February 2003.
Asp N G, Bjorntorp P, Britton M, et al. Obesity - problems and interventions. SBU Report No. 160.Stockholm, Sweden: Swedish Council on Technology Assessment in Health Care (SBU); 2002.
O'Meara S, Riemsma R, Shirran L, et al. A rapid and systematic review of the clinical effectivenessand cost-effectiveness of orlistat in the management of obesity. Health TechnolAssess. 2001;5(18):1-81.
NHS Centre for Reviews and Dissemination (CRD). The prevention and treatment of childhoodobesity. Effective Health Care. York, UK: CRD; 2002; 7(6).
U.S. Preventive Services Task Force. Screening for obesity in adults: Recommendations andrationale. Ann Intern Med. 2003;139(11):930-932.
U.S. Preventive Services Task Force. Behavioral counseling in primary care to promote a healthydiet: Recommendations and rationale. Am J Prev Med. 2003;24(1):93-100.
U.S. Preventive Services Task Force. Behavioral counseling in primary care to promote physicalactivity: Recommendation and rationale. Ann Intern Med. 2002;137(3):205-207.

American Gastroenterological Association medical position statement on obesity. Gastroenterology.2002;123(3):879-881.
National Institute for Clinical Excellence (NICE). Guidance on the use of orlistat for the treatment ofobesity in adults. Technology Appraisal Guidance No.22. London, UK: NICE; 2001.
O'Meara S, Riemsma R, Shirran L, et al. The clinical effectiveness and cost-effectiveness ofsibutramine in the management of obesity: A technology assessment. Health Technol Assess. 2002;6(6):1-97.
Shekelle P, Morton S, Maglione M. Ephedra and ephedrine for weight loss and athletic performanceenhancement: Clinical efficacy and side effects. Evidence Report/Technology Assessment 76.Rockville, MD: Agency for Healthcare Research and Quality (AHRQ); 2003.
McTigue K, Harris R, Hemphill MB, et al. Screening and interventions for overweight and obesity inadults. Preventive Services Task Force Systematic Evidence Review No. 21. Rockville, MD: Agencyfor Healthcare Research and Quality (AHRQ); 2003.
Jain A. What works for obesity? A summary of the research behind obesity interventions. London,UK: BMJ Publishing Group Ltd.; April 30, 2004.
Institute for Clinical Systems Improvement (ICSI). Diet programs for weight loss in adults. Technology Assessment ReportNo.83.Bloomington,MN:ICSI;August2004.Availableat:http://www.icsi.org/knowledge/detail.asp?catID=107&itemID=1742. Accessed September 21, 2004.
Avenell A, Broom J, Brown TJ, et al. Systematic review of the long-term effects and economicconsequences of treatments for obesity and implications for health improvement. Health TechnolAssess. 2004;8(21): iii-iv, 1-182.
O'Meara S, Riemsma R, Shirran L, et al. A systematic review of the clinical effectiveness of orlistatused for the management of obesity. Obes Rev. 2004;5(1):51-68.
Padwal R, Li SK, Lau DC. Long-term pharmacotherapy for obesity and overweight. CochraneDatabase Syst Rev. 2004;(3):CD004094.
Pittler MH, Ernst E. Dietary supplements for body-weight reduction: A systematic review. Am J ClinNutr. 2004;79(4):529-536.
Smartt P. Evidence based review of weight loss medicines:Â A report commissioned by the NewZealand Accident Compensation Corporation (ACC). NZHTA Report. Christchurch, New Zealand:New Zealand Health Technology Assessment (NZHTA); 2004;7(6).
Day P. What is the evidence for the safety and effectiveness of surgical and non-surgicalinterventions for patients with morbid obesity? NZHTA Technical Brief Series. Christchurch, NewZealand: New Zealand Health Technology Assessment (NZHTA); 2005;4(1).
Institute for Clinical Systems Improvement (ICSI). Diet programs for weight loss in adults.Technology Assessment Report No. 83. Bloomington, MN: ICSI; March 2004.Â
Institute for Clinical Systems Improvement (ICSI). Behavioral therapy programs for weight loss in
adults. Technology Assessment Report No.87. Bloomington,MN:ICSI; January2005. Available at:http://www.icsi.org/knowledge/detail.asp?catID=107&itemID=1993. Accessed February 7, 2006.
Institute for Clinical Systems Improvement (ICSI). Treatment of obesity in children andadolescents. Technology Assessment Report No.90. Bloomington,MN:ICSI;2005. Available at:http://www.icsi.org/knowledge/detail.asp?catID=107&itemID=2243. Accessed February 7, 2006.
Shekelle PG, Morton SC, Maglione MA, et al. Pharmacological and surgical treatment of obesity.Evidence Report/Technology Assessment No. 103. Prepared by the Southern California-RANDEvidence-Based Practice Center, Santa Monica, CA, under contract no. 290-02-0003. AHRQPublication No. 04-E028-2. Rockville, MD: Agency for Healthcare Research and Quality; July 2004.Available at http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat1a.chapter.19289. Accessed June13, 2005.
Snow V, Barry P, Fitterman N, et al. Pharmacologic and surgical management of obesity in primarycare: A clinical practice guideline from the American College of Physicians. Ann Intern Med.2005:142(7):525-531.
Li Z, Maglione M, Tu W, et al. Meta-analysis: Pharmacologic treatment of obesity. Ann Intern Med.2005;142(7):532-546.
Tsai AG, Wadden TA. Systematic review: An evaluation of major commercial weight loss programs inthe United States. Ann Intern Med. 2005;142(1):56-66.
Whitlock EP, Williams SB, Gold R, et al. Screening and interventions for childhood overweight: Asummary of evidence for the US Preventive Services Task Force. Pediatrics. 2005;116(1):e125-e144.
Wadden TA, Berkowitz RI, Womble LG, et al. Randomized trial of lifestyle modification andpharmacotherapy for obesity. N Engl J Med. 2005;353(20):2111-2120.
Swedish Council on Technology Assessment in Healthcare (SBU). Interventions to prevent obesity: Asystematic review. Stockholm, Sweden; SBU; 2005.
Ioannides-Demos LL, Proietto J, Tonkin AM, McNeil JJ. Safety of drug therapies used for weight lossand treatment of obesity. Drug Saf. 2006;29(4):277-302.
Abell TL, Minocha A, Abidi N. Looking to the future: Electrical stimulation for obesity. Am J Med Sci.2006;331(4):226-232.
Dixon JB. Weight loss medications--where do they fit in? Aust Fam Physician. 2006;35(8):576-579.
Blissmer B, Riebe D, Dye G, et al. Health-related quality of life following a clinical weight lossintervention among overweight and obese adults: Intervention and 24 month follow-up effects.Health Qual Life Outcomes. 2006;4:43.
Arterburn DE, DeLaet DE, Schauer DP. Obesity. In: BMJ Clinical Evidence. London, UK: BMJPublishing Group; July 2005.
National Institute for Health and Clinical Excellence (NICE). Obesity: The prevention, identification,assessment and management of overweight and obesity in adults and children. Clinical Guideline 43.London, UK: NICE; 2006.

Lambert M-L, Kohn L, Vinck I, et al. Pharmacological and surgical treatment of obesity. Residentialcare for severely obese children in Belgium. KCE Reports 36. Brussels, Belgium: Belgian HealthCare Knowledge Centre (KCE); 2006.
Dansinger ML, Tatsioni A, Wong JB, et al. Meta-analysis: The effect of dietary counseling for weightloss. Ann Intern Med. 2007;147(1):41-50.
Wilfley DE, Stein RI, Saelens BE, et al. Efficacy of maintenance treatment approaches for childhoodoverweight: A randomized controlled trial. JAMA. 2007;298(14):1661-1673.
Whitlock EP, O'Connor EA, Williams SB, et al. Effectiveness of weight management programs inchildren and adolescents. Evidence Report/Technology Assessment No. 170. Prepared by the OregonEvidence-based Practice Center under Contract No. 290-02-0024. AHRQ Publication No. 08-E014.Rockville, MD: Agency for Healthcare Research and Quality (AHRQ); September 2008.
Orozco LJ, Buchleitner AM, Gimenez-Perez G, et al. Exercise or exercise and diet for preventing type2 diabetes mellitus. Cochrane Database Syst Rev. 2008;(3):CD003054.
Ball SD, Altena TS. Comparison of the BOD POD and dual energy x-ray absorptiometry in men.Physiol Meas. 2004;25(3):671-678.
Williams JE, Wells JC, Wilson CM, et al. Evaluation of Lunar Prodigy dual-energy X-rayabsorptiometry for assessing body composition in healthy persons and patients by comparison withthe criterion 4-component model. Am J Clin Nutr. 2006;83(5):1047-1054.
Ritz P, Sallé A, Audran M, Rohmer V. Comparison of different methods to assess body compositionof weight loss in obese and diabetic patients. Diabetes Res Clin Pract. 2007;77(3):405-411.
Pineau JC, Guihard-Costa AM, Bocquet M. Validation of ultrasound techniques applied to body fatmeasurement. A comparison between ultrasound techniques, air displacement plethysmography andbioelectrical impedance vs. dual-energy X-ray absorptiometry. Ann Nutr Metab. 2007;51(5):421-427.
Pineau JC, Filliard JR, Bocquet M. Ultrasound techniques applied to body fat measurement in maleand female athletes. J Athl Train. 2009;44(2):142-147.
U.S. Food and Drug Administration (FDA). Meridia (sibutramine hydrochloride) information.Postmarketing drug safety information for patients and providers. Rockville, MD: FDA; updatedOctober 8, 2010.
Rogovik AL, Chanoine JP, Goldman RD. Pharmacotherapy and weight-loss supplements for treatmentof paediatric obesity. Drugs. 2010;70(3):335-346.
Whitlock EP, O'Connor EA, Williams SB, et al. Effectiveness of weight management interventions inchildren: A targeted systematic review for the USPSTF. Pediatrics. 2010;125(2):e396-e418.
Balazs A. Role of phytotherapy in the prevention and treatment of obesity. Orv Hetil.2010;151(19):763-773.
Borel AL, Nazare JA, Smith J, et al. Improvement in insulin sensitivity following a 1-year lifestyleintervention program in viscerally obese men: Contribution of abdominal adiposity. Metabolism.2012;61(2):262-72.

Garvey WT, Ryan DH, Look M, et al. Two-year sustained weight loss and metabolic benefits withcontrolled-release phentermine/topiramate in obese and overweight adults (SEQUEL): Arandomized, placebo-controlled, phase 3 extension study. Am J Clin Nutr. 2012;95(2):297-308.
Mulholland Y, Nicokavoura E, Broom J, Rolland C. Very-low-energy diets and morbidity: A systematicreview of longer-term evidence. Br J Nutr. 2012;108(5):832-851.
Fioravante M, Alegre SM, Marin DM, et al. Weight loss and resting energy expenditure in patientswith chronic hepatitis C before and during standard treatment. Nutrition. 2012;28(6):630-634.
Bruera E, Dev R. Palliative care: Assessment and management of anorexia and cachexia. Lastreviewed October 2013. UpToDate Inc., Waltham, MA.
http://link.reuters.com/kuq24t