weighing the options for anticoagulation in obesity the options for anticoagulation in obesity...
TRANSCRIPT
Weighing the Options for Anticoagulation in ObesityCaitlin S. Brown, PharmD
Pharmacy Grand RoundsMay 24, 2016
Objectives• Review pharmacokinetic changes in obesity
• Discuss dosing and monitoring strategies when using low molecular weight heparin
• Outline evidence and recommendations for utilization of direct oral anticoagulants
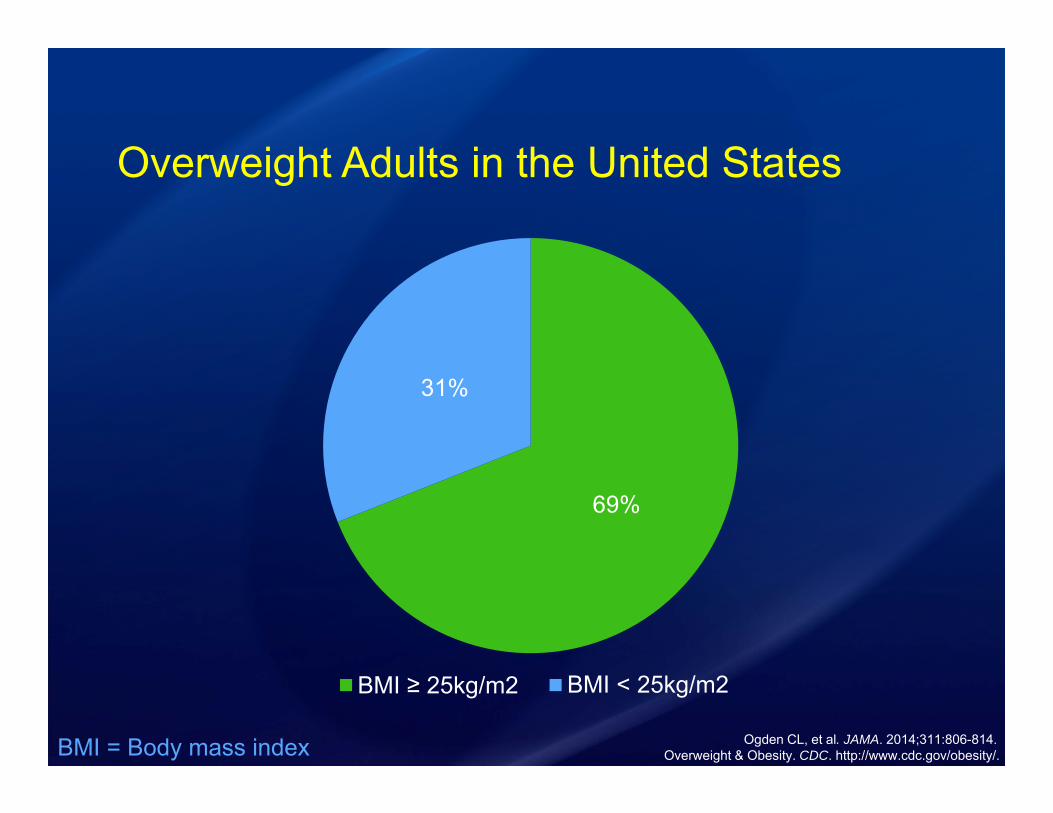
Overweight Adults in the United States
69%
31%
BMI ≥ 25kg/m2 BMI < 25kg/m2
Ogden CL, et al. JAMA. 2014;311:806-814.Overweight & Obesity. CDC. http://www.cdc.gov/obesity/. BMI = Body mass index
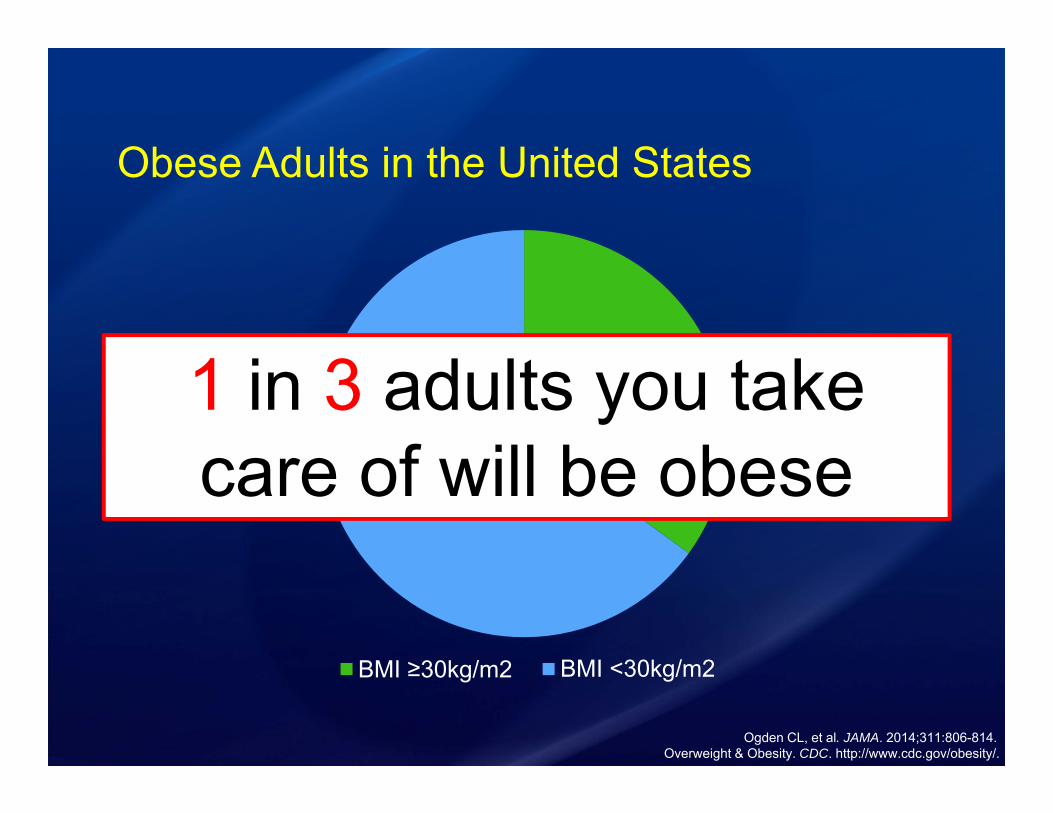
Obese Adults in the United States
35%
65%
BMI ≥30kg/m2 BMI <30kg/m2
Ogden CL, et al. JAMA. 2014;311:806-814.
1 in 3 adults you take care of will be obese
Overweight & Obesity. CDC. http://www.cdc.gov/obesity/.
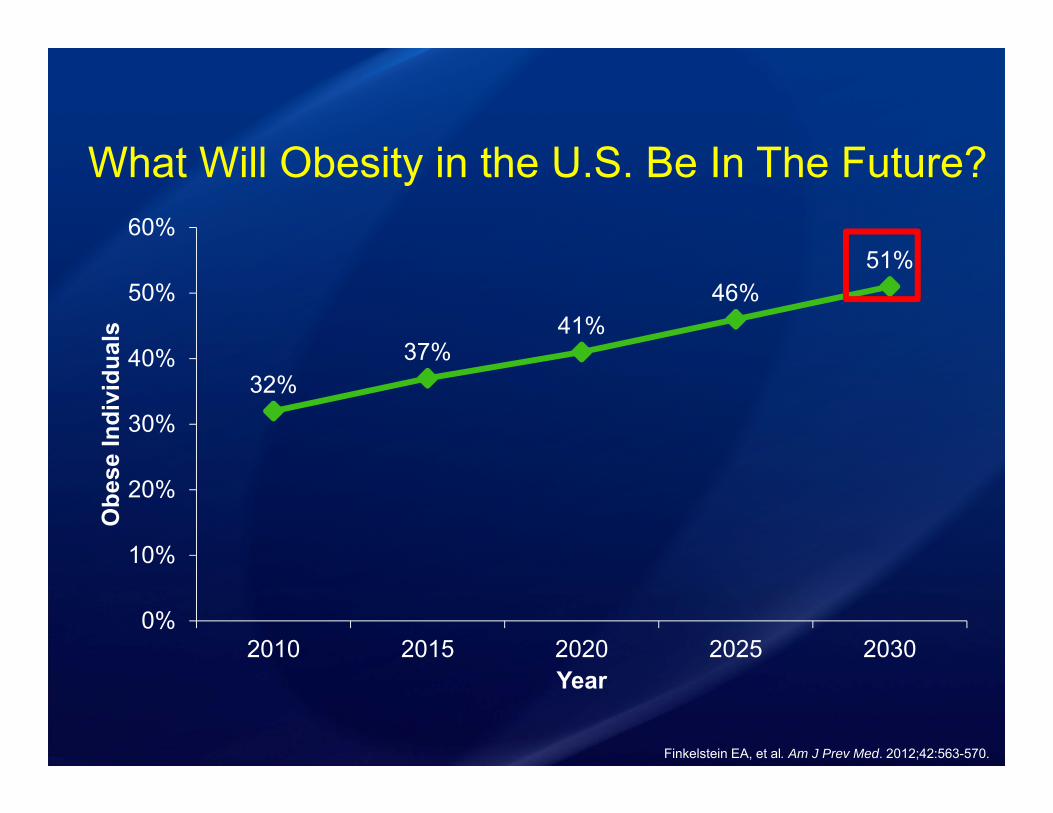
What Will Obesity in the U.S. Be In The Future?
32%37%
41%46%
51%
0%
10%
20%
30%
40%
50%
60%
2010 2015 2020 2025 2030
Obe
se In
divi
dual
s
Year
Finkelstein EA, et al. Am J Prev Med. 2012;42:563-570.
Pharmacokinetics in Obesity
Volume of Distribution
(Vd)
Elimination Half-Life
(T1/2)
Clearance(CL)
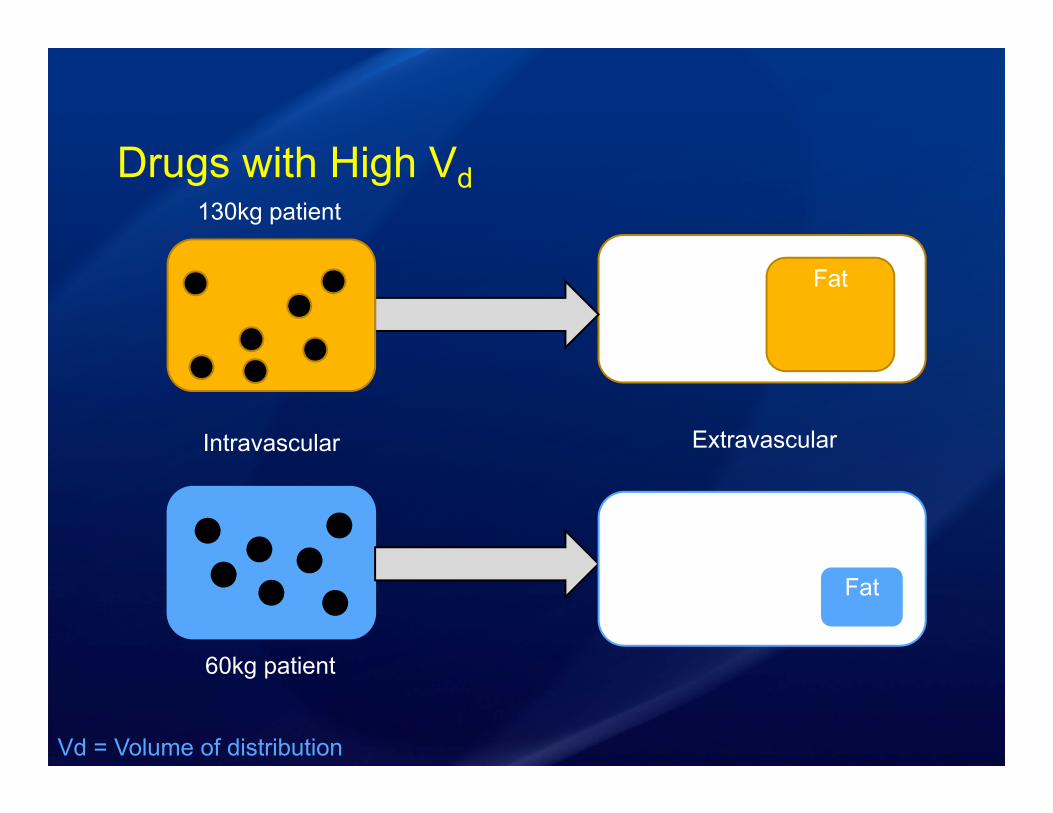
Drugs with High Vd
60kg patient
130kg patient
Intravascular Extravascular
Fat
Fat
Vd = Volume of distribution
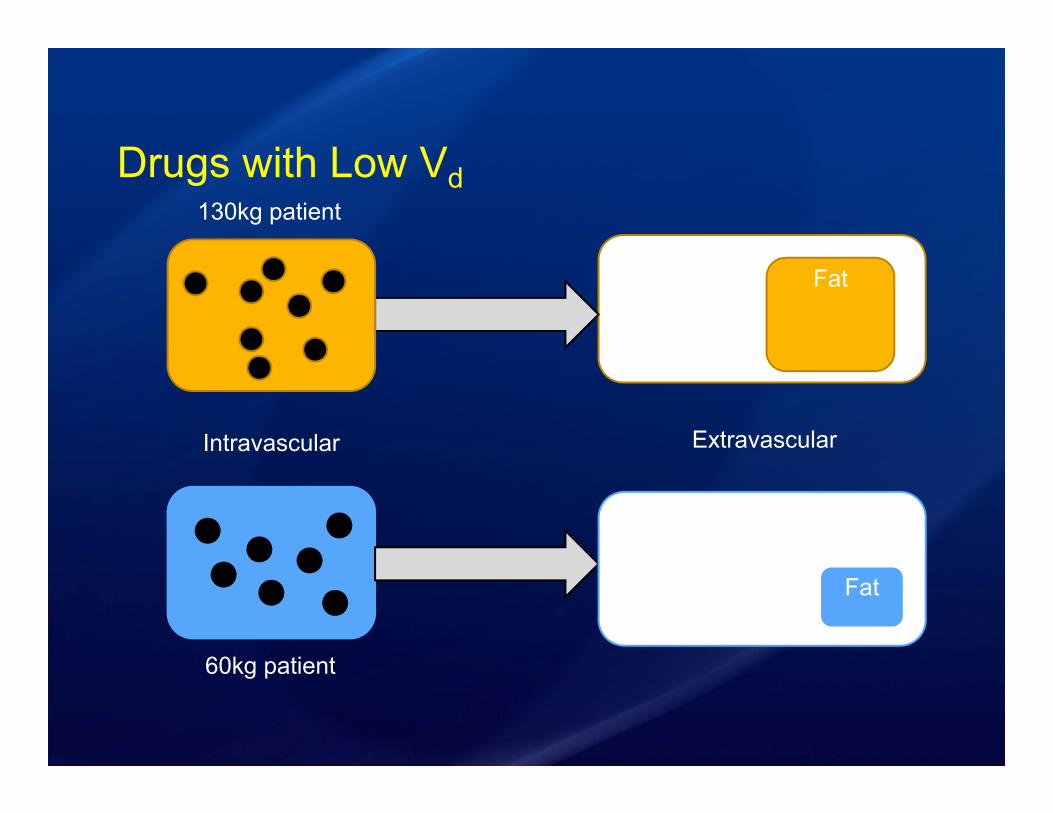
Drugs with Low Vd
60kg patient
130kg patient
Intravascular Extravascular
Fat
Fat
Clearance• Defined as the volume of blood cleared of drug
in a given time
• In obese patients:• Altered hepatic blood flow• Higher absolute clearance
Hanley MJ, et al. Clin Pharmacokinet. 2010;49:71-87.

Elimination Half-Life• Defined as time it takes for concentration to fall
to half its original concentration
Hanley MJ, et al. Clin Pharmacokinet. 2010;49:71-87.
T½ = (ln 2 x Vd) / CL
CL = Clearance
Which of the following statements is true?A. Obese and non-obese patients have similar
PK profilesB. Vd is increased in obese patientsC. T1/2 is equivalent in obese and non-obese
patientsD. Compared to non-obese patients, obese
patients have equivalent CL
Venous Thromboembolism Prophylaxis

What Does the Package Insert Say?
Indication eCrCl ≥ 30mL/min eCrCl < 30mL/min
Prophylaxis of VTE 40mg daily 30mg daily
Treatment of VTE 1mg/kg Q12H 1mg/kg daily
Enoxaparin [package insert]. Sanofi-adventis. 2013.
“The safety and efficacy of prophylactic doses of Lovenox in obese patients (BMI >30 kg/m2) has not been fully determined and there is no consensus for
dose adjustment”
VTE = Venous thromboembolism
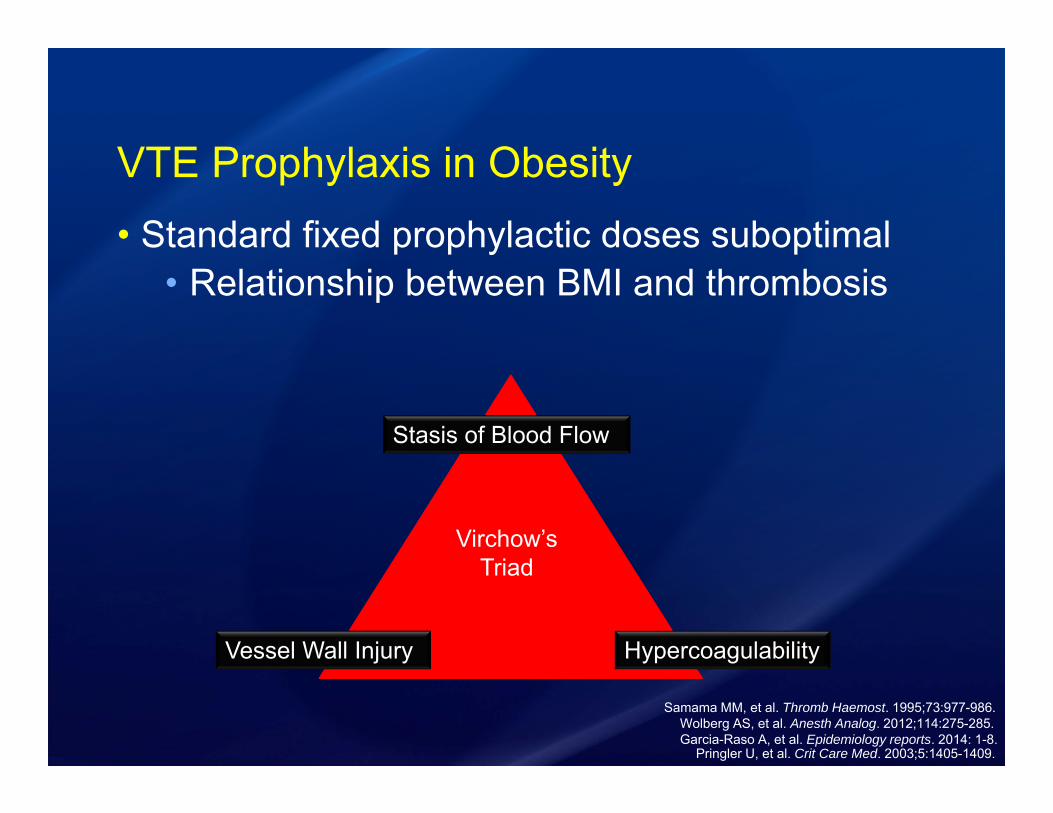
VTE Prophylaxis in Obesity• Standard fixed prophylactic doses suboptimal
• Relationship between BMI and thrombosis
Garcia-Raso A, et al. Epidemiology reports. 2014: 1-8. Wolberg AS, et al. Anesth Analog. 2012;114:275-285.
Pringler U, et al. Crit Care Med. 2003;5:1405-1409.
Stasis of Blood Flow
HypercoagulabilityVessel Wall Injury
Virchow’s Triad
Samama MM, et al. Thromb Haemost. 1995;73:977-986.
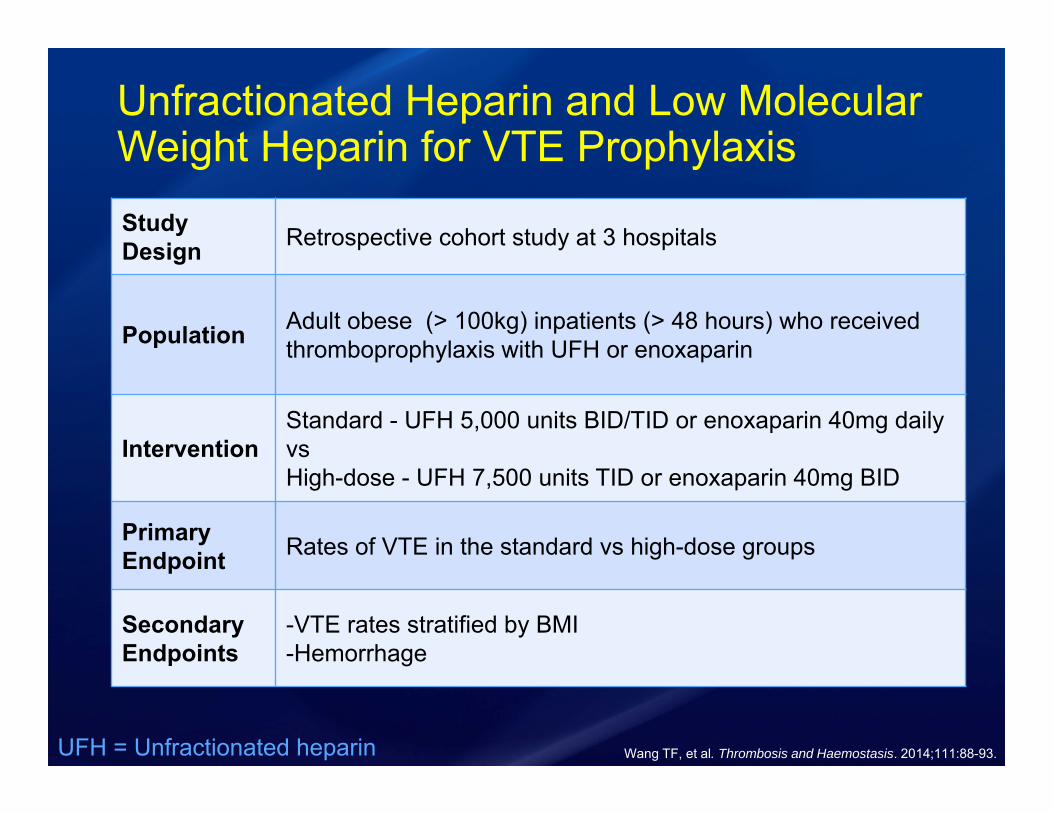
Unfractionated Heparin and Low Molecular Weight Heparin for VTE Prophylaxis
Wang TF, et al. Thrombosis and Haemostasis. 2014;111:88-93.
Study Design Retrospective cohort study at 3 hospitals
Population Adult obese (> 100kg) inpatients (> 48 hours) who received thromboprophylaxis with UFH or enoxaparin
InterventionStandard - UFH 5,000 units BID/TID or enoxaparin 40mg daily vsHigh-dose - UFH 7,500 units TID or enoxaparin 40mg BID
PrimaryEndpoint Rates of VTE in the standard vs high-dose groups
SecondaryEndpoints
-VTE rates stratified by BMI-Hemorrhage
UFH = Unfractionated heparin

Did High-Dose Prophylaxis Reduce VTE?
1.5%
0.8%
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
1.4%
1.6%
Standard High-dose
Rat
es o
f VTE
Dosing Regimen
p = 0.05
Wang TF, et al. Thrombosis and Haemostasis. 2014;111:88-93.
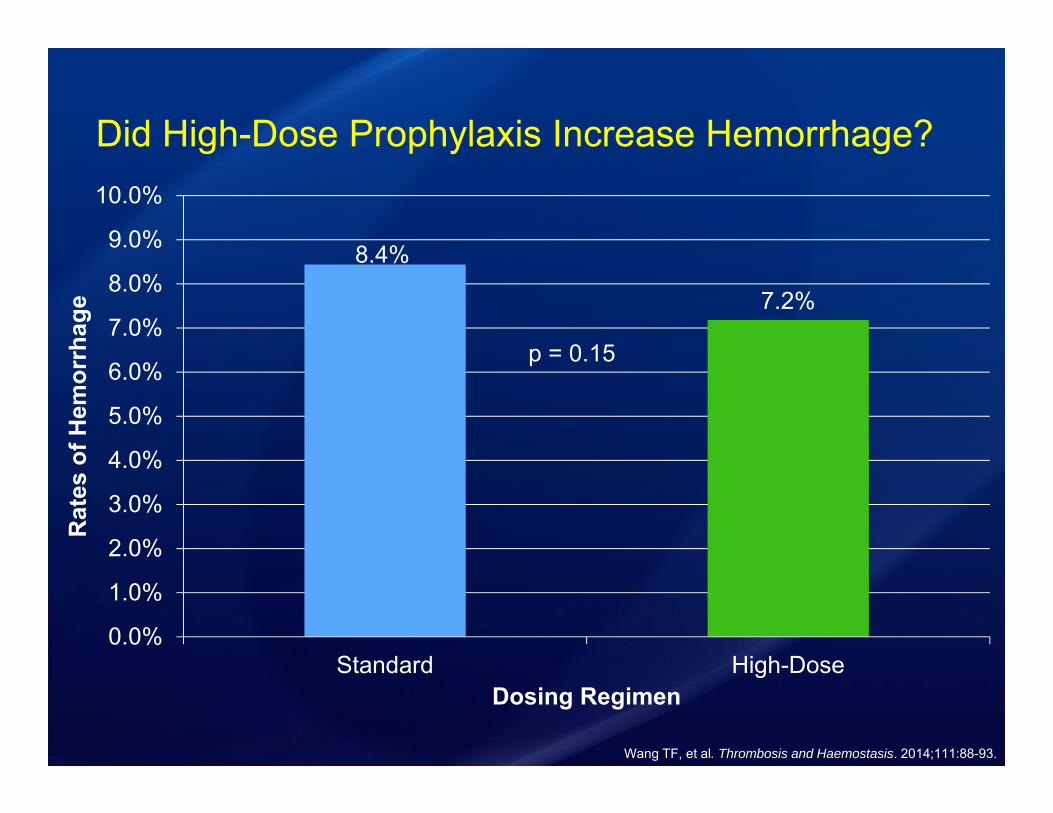
Did High-Dose Prophylaxis Increase Hemorrhage?
8.4%
7.2%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
10.0%
Standard High-Dose
Rat
es o
f Hem
orrh
age
Dosing Regimen
Wang TF, et al. Thrombosis and Haemostasis. 2014;111:88-93.
p = 0.15
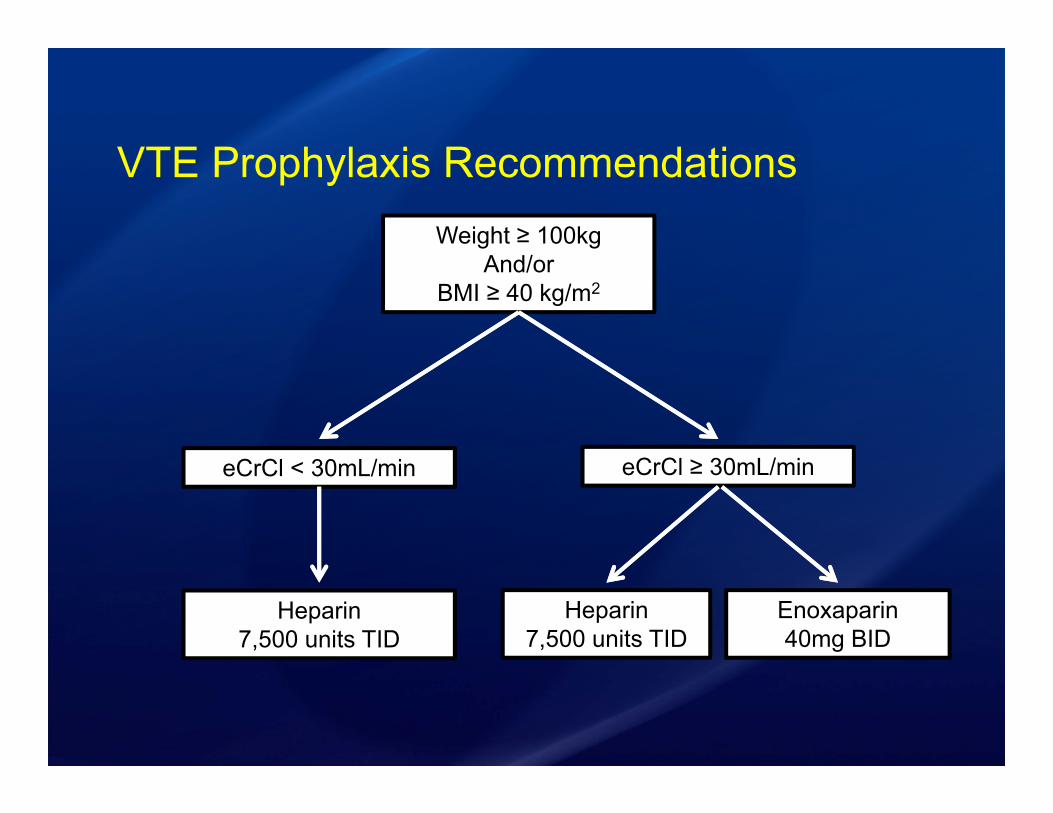
VTE Prophylaxis RecommendationsWeight ≥ 100kg
And/orBMI ≥ 40 kg/m2
eCrCl < 30mL/min eCrCl ≥ 30mL/min
Heparin 7,500 units TID
Enoxaparin 40mg BID
Heparin 7,500 units TID
Treatment Dosing of Low Molecular Weight Heparin
46F admitted with unilateral LLE swelling and redness, found to have a DVT on ultrasound. Initiated on enoxaparin for bridging to warfarin treatment.
LLE = Left lower extremity DVT = Deep vein thrombosiseCrCl = Estimated creatinine clearance
Hgb:11g/dLPlatelets: 368 x 109 LINR: 1.2 Wt: 200 kgBMI: 39.1 kg/m2
eCrCl = 96 mL/min

Which dosing strategy would you chose for this patient?
200kg, eCrCl=96mL/min
A. 150mg BIDB. 150mg BID and check anti-XaC. 200mg BIDD. 200mg BID and check anti-Xa
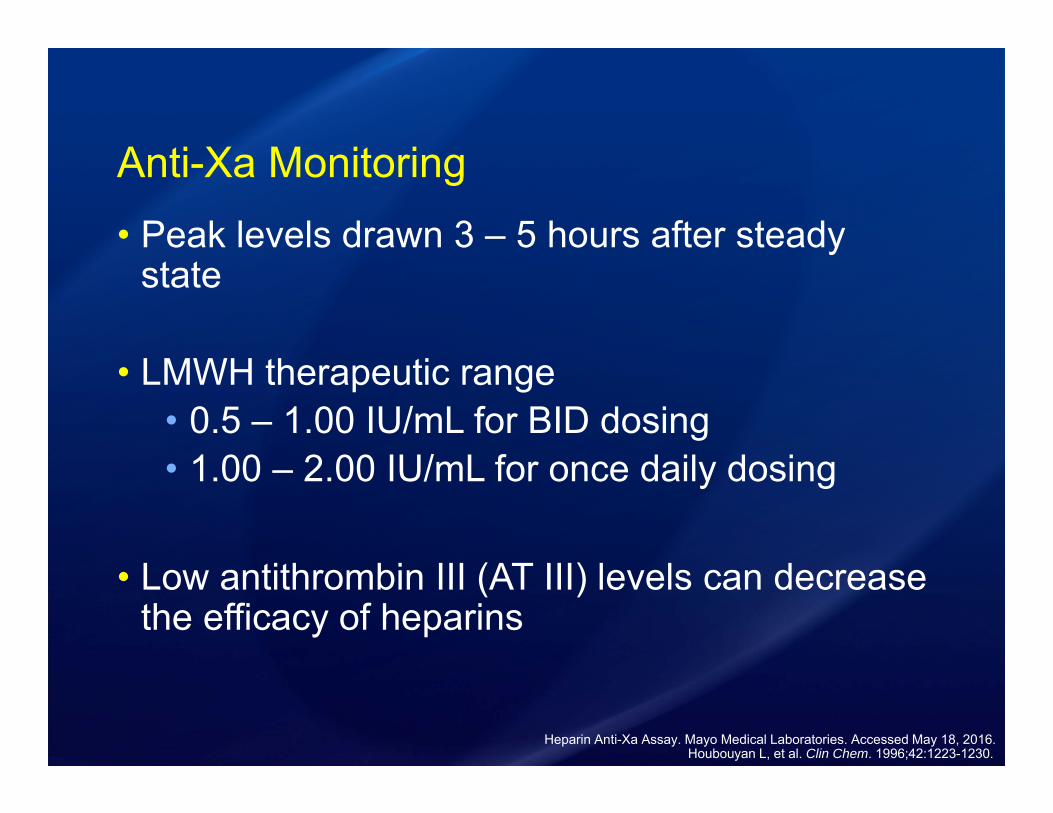
Anti-Xa Monitoring• Peak levels drawn 3 – 5 hours after steady
state
• LMWH therapeutic range• 0.5 – 1.00 IU/mL for BID dosing• 1.00 – 2.00 IU/mL for once daily dosing
• Low antithrombin III (AT III) levels can decrease the efficacy of heparins
Heparin Anti-Xa Assay. Mayo Medical Laboratories. Accessed May 18, 2016.Houbouyan L, et al. Clin Chem. 1996;42:1223-1230.
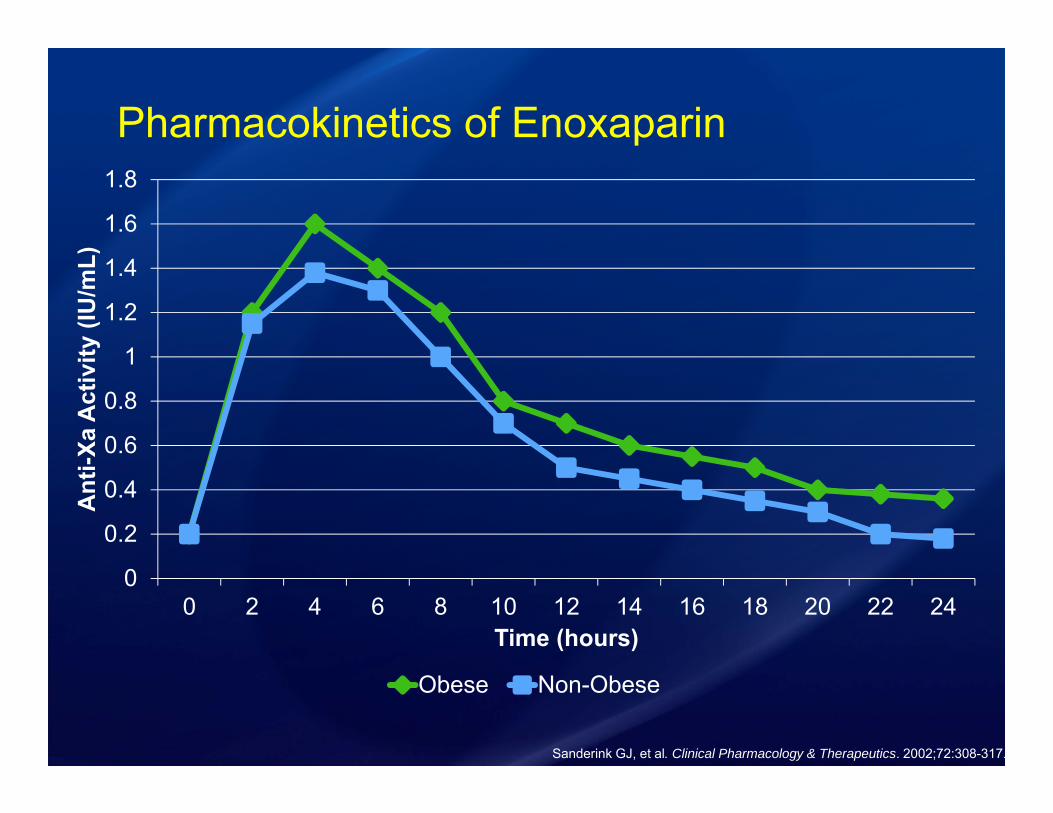
Pharmacokinetics of Enoxaparin
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
0 2 4 6 8 10 12 14 16 18 20 22 24
Ant
i-Xa
Act
ivity
(IU
/mL)
Time (hours)
Obese Non-Obese
Sanderink GJ, et al. Clinical Pharmacology & Therapeutics. 2002;72:308-317.

VTE Treatment Dosing with Enoxaparin
Deal EN, et al. J Thromb Thrombolysis. 2011;32:188-194.
Study Design Retrospective case series
Population
Received enoxaparin with a corresponding anti-Xa and BMI ≥40kg/m2
• 26 patients• Median weight 162kg (58% > 150kg)• 27% ICU patients
PrimaryEndpoint Achievement of goal anti-Xa level (0.5-1 IU/mL)
SecondaryEndpoints Bleeding events

Anti-Xa Levels
15%
46%
38%
0%5%
10%15%20%25%30%35%40%45%50%
Perc
enta
ge o
f Pat
ient
s
Anti-Xa Level
• No patient had subtherapeutic levels
• No thrombotic events occurred in the study
• 40% of patients with a supratherapeutic level had bleeding events
• Median starting dose was 0.8mg/kg
• Doses ranged from 80mg – 150mg BID
Deal EN, et al. J Thromb Thrombolysis. 2011;32:188-194.
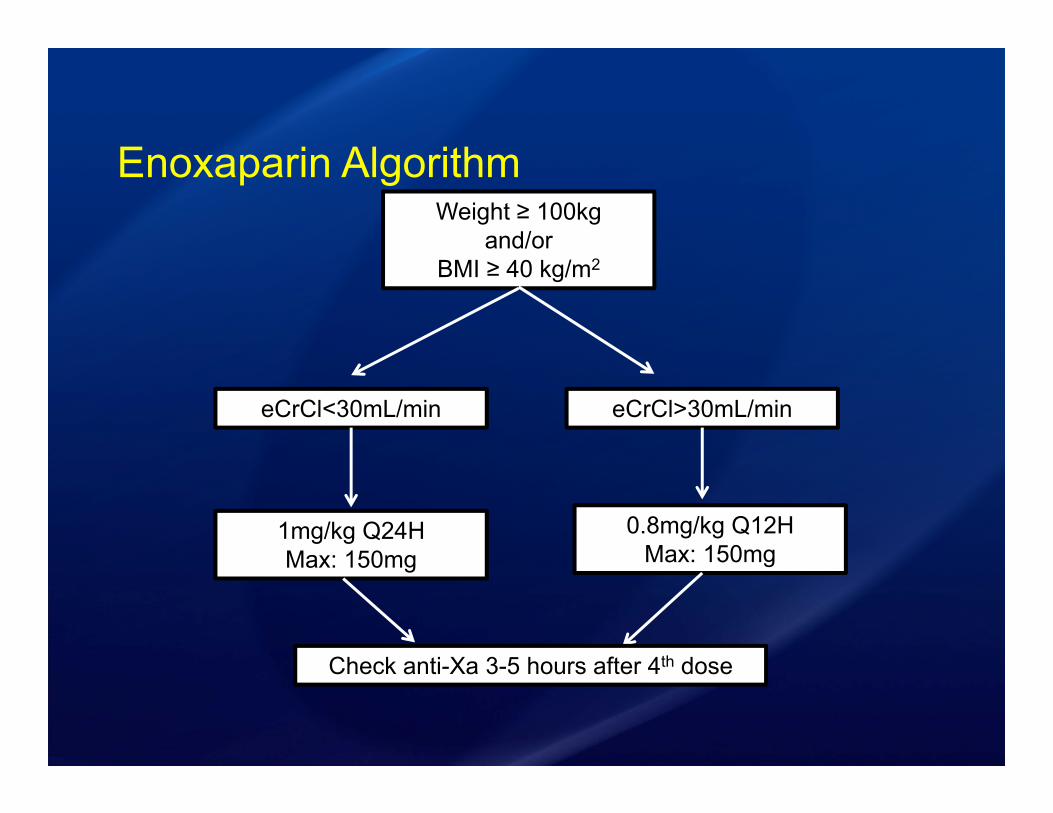
Enoxaparin AlgorithmWeight ≥ 100kg
and/orBMI ≥ 40 kg/m2
eCrCl<30mL/min eCrCl>30mL/min
1mg/kg Q24HMax: 150mg
0.8mg/kg Q12HMax: 150mg
Check anti-Xa 3-5 hours after 4th dose
46F admitted with unilateral LLE swelling and redness, found to have a DVT on ultrasound. Initiated on enoxaparin for bridging to warfarin treatment.
Hgb:11g/dLPlatelets: 368 x 109 LINR: 1.2 Wt: 200 kgBMI: 39.1 kg/m2
eCrCl = 96 mL/min
Which dosing strategy would you chose for this patient?
200kg, eCrCl=96mL/min
A. 150mg BIDB. 150mg BID and check anti-XaC. 200mg BIDD. 200mg BID and check anti-Xa
Direct Oral Anticoagulants (DOACS)
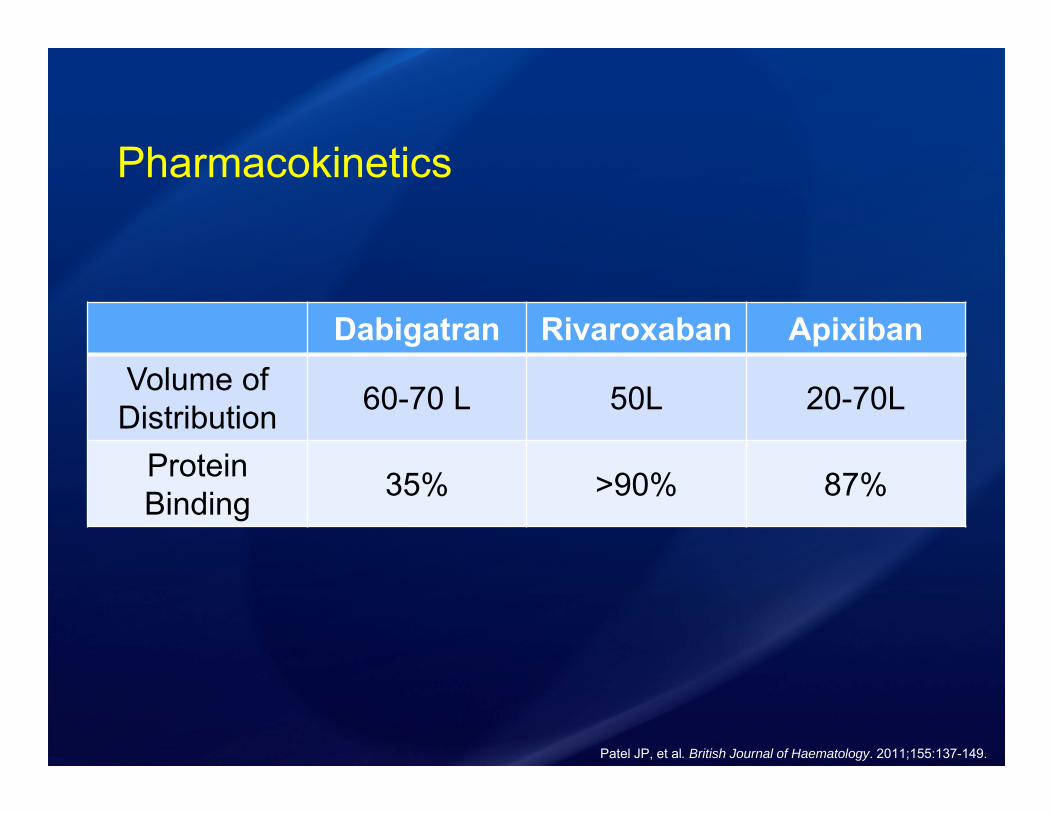
Pharmacokinetics
Dabigatran Rivaroxaban ApixibanVolume of Distribution 60-70 L 50L 20-70L
Protein Binding 35% >90% 87%
Patel JP, et al. British Journal of Haematology. 2011;155:137-149.

Obese Patients in Dabigatran StudiesStudy Intervention Weight
(kg) BMI* Number (%)≥100kg
RE-LYAtrial Fibrillation
Dabigatran110mg BID
Dabigatran150mg BID
Warfarin
82.0±19.9*
82.5±19.4*
82.7±19.7*
N/A 3,099 patients(17%)
RE-COVERVTE
Heparin/ dabigatran150mg BID
Heparin/warfarin
84 (38-175)**
82 (39-161)**
28.9±5.7
28.4±5.5
438 patients (17.1%)
394 patients(15.4%)
RE-COVER IIVTE
Heparin/ dabigatran150mg BID
Heparin/warfarin
80 (36-184)**
81 (35-210)**
28.4±5.8
28.4±5.8
Guler E, et al. Anatol J Cardiol. 2015;15:1020-1029.Connolly SJ et al. NEJM. 2009;361:1139-1151Schulman S et al. NEJM. 2009;361:2342-2352.*mean±standard deviation
**median (range)
Di Minno MND et al. Ann Med. 2015;47:61-68.
Dabigatran• RE-LY subgroup analysis
• Case reports of stroke in obese patients • 153kg (BMI 44.7kg/m2) peak level was less
than the 25th percentile of therapeutic trough
Guler E, et al. Anatol J Cardiol. 2015;15:1020-1029.Bruer L, et al. NEJM. 2013;25:2440-2442.
Connolly SJ et al. NEJM. 2009;361:1139-1151.

Dabigatran Pharmacokinetics in Obesity
020406080
100120140160180200220240260280
8 a.m. 10 a.m. Noon 2 p.m. 4 p.m. 6 p.m. 8 p.m.
Plas
ma
Leve
l of D
abig
atra
n (n
g/m
L)
Daytime Hours
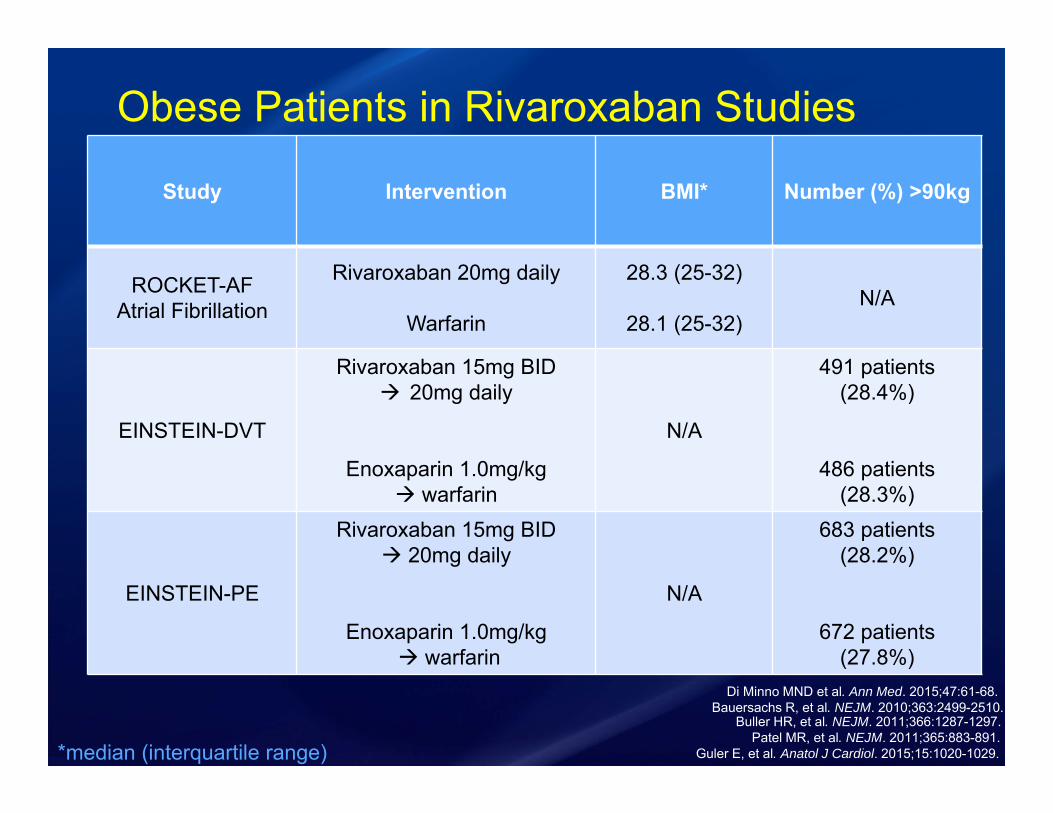
Obese Patients in Rivaroxaban Studies
Study Intervention BMI* Number (%) >90kg
ROCKET-AFAtrial Fibrillation
Rivaroxaban 20mg daily
Warfarin
28.3 (25-32)
28.1 (25-32)N/A
EINSTEIN-DVT
Rivaroxaban 15mg BID 20mg daily
Enoxaparin 1.0mg/kg warfarin
N/A
491 patients(28.4%)
486 patients(28.3%)
EINSTEIN-PE
Rivaroxaban 15mg BID 20mg daily
Enoxaparin 1.0mg/kg warfarin
N/A
683 patients(28.2%)
672 patients(27.8%)
Guler E, et al. Anatol J Cardiol. 2015;15:1020-1029.Patel MR, et al. NEJM. 2011;365:883-891.
Buller HR, et al. NEJM. 2011;366:1287-1297.Bauersachs R, et al. NEJM. 2010;363:2499-2510.
Di Minno MND et al. Ann Med. 2015;47:61-68.
*median (interquartile range)
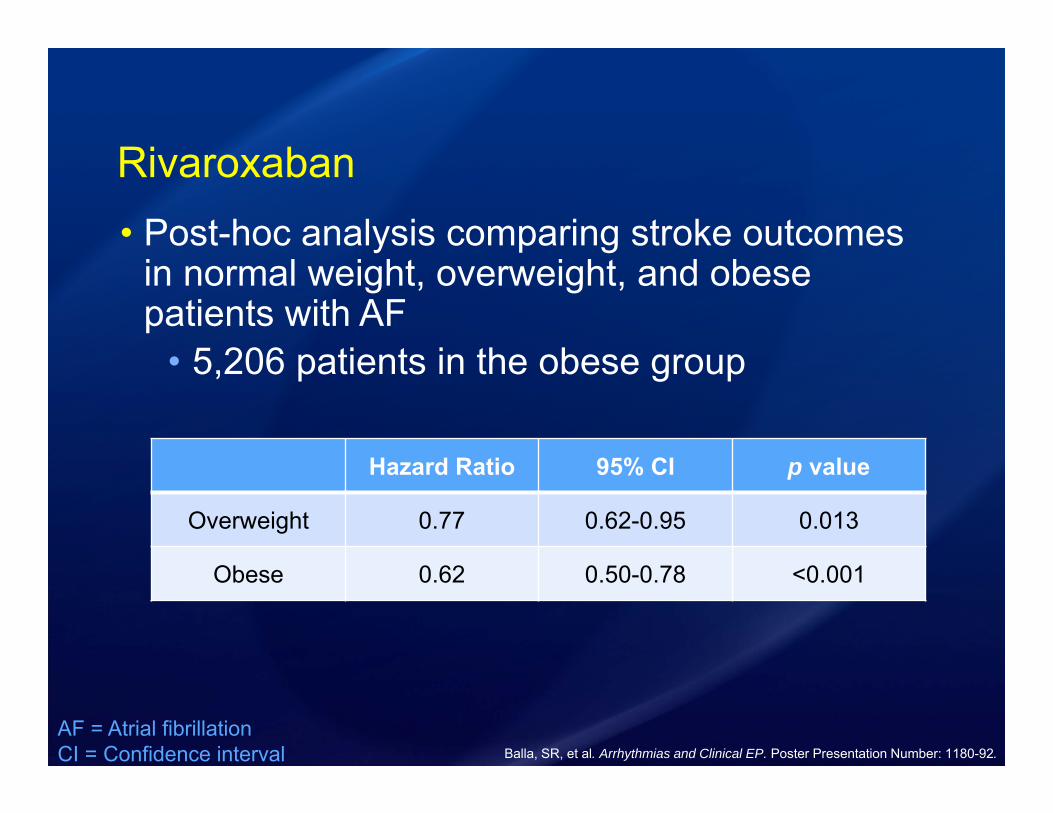
Rivaroxaban• Post-hoc analysis comparing stroke outcomes
in normal weight, overweight, and obese patients with AF
• 5,206 patients in the obese group
AF = Atrial fibrillationCI = Confidence interval Balla, SR, et al. Arrhythmias and Clinical EP. Poster Presentation Number: 1180-92.
Hazard Ratio 95% CI p value
Overweight 0.77 0.62-0.95 0.013
Obese 0.62 0.50-0.78 <0.001
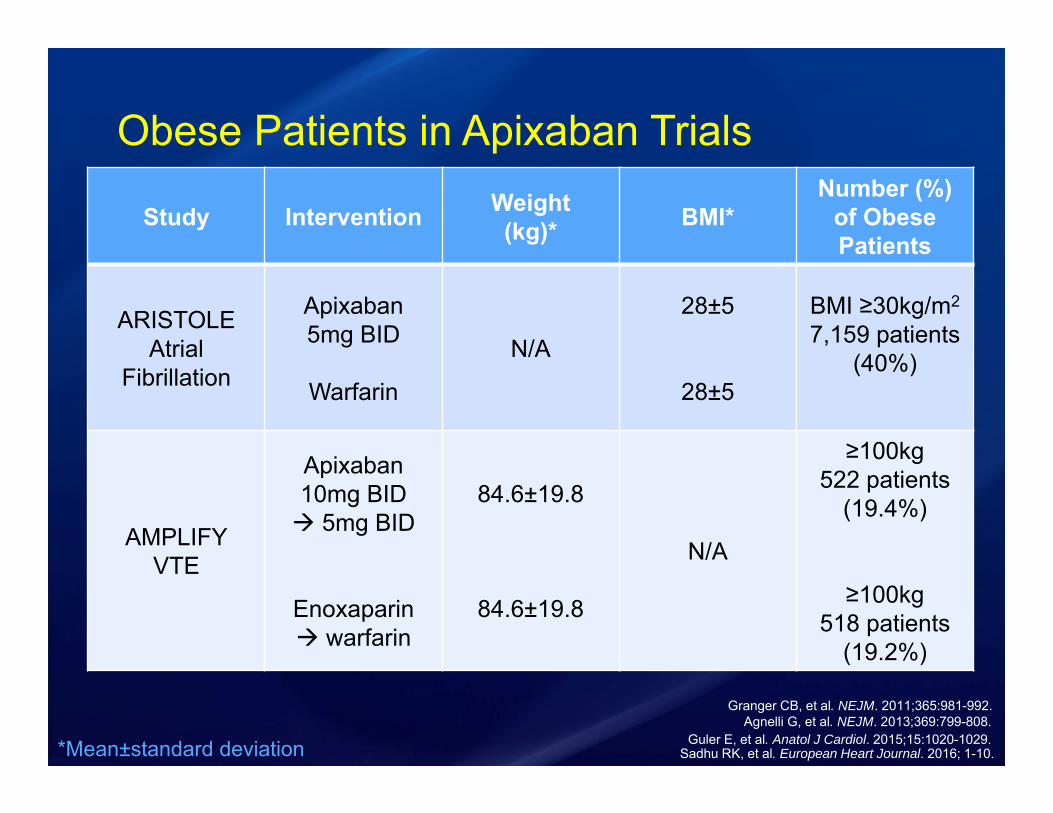
Obese Patients in Apixaban Trials
Guler E, et al. Anatol J Cardiol. 2015;15:1020-1029.
Study Intervention Weight(kg)* BMI*
Number (%) of ObesePatients
ARISTOLEAtrial
Fibrillation
Apixaban5mg BID
Warfarin
N/A
28±5
28±5
BMI ≥30kg/m2
7,159 patients(40%)
AMPLIFYVTE
Apixaban 10mg BID 5mg BID
Enoxaparin warfarin
84.6±19.8
84.6±19.8
N/A
≥100kg522 patients
(19.4%)
≥100kg518 patients
(19.2%)
Agnelli G, et al. NEJM. 2013;369:799-808.Granger CB, et al. NEJM. 2011;365:981-992.
*Mean±standard deviation Sadhu RK, et al. European Heart Journal. 2016; 1-10.
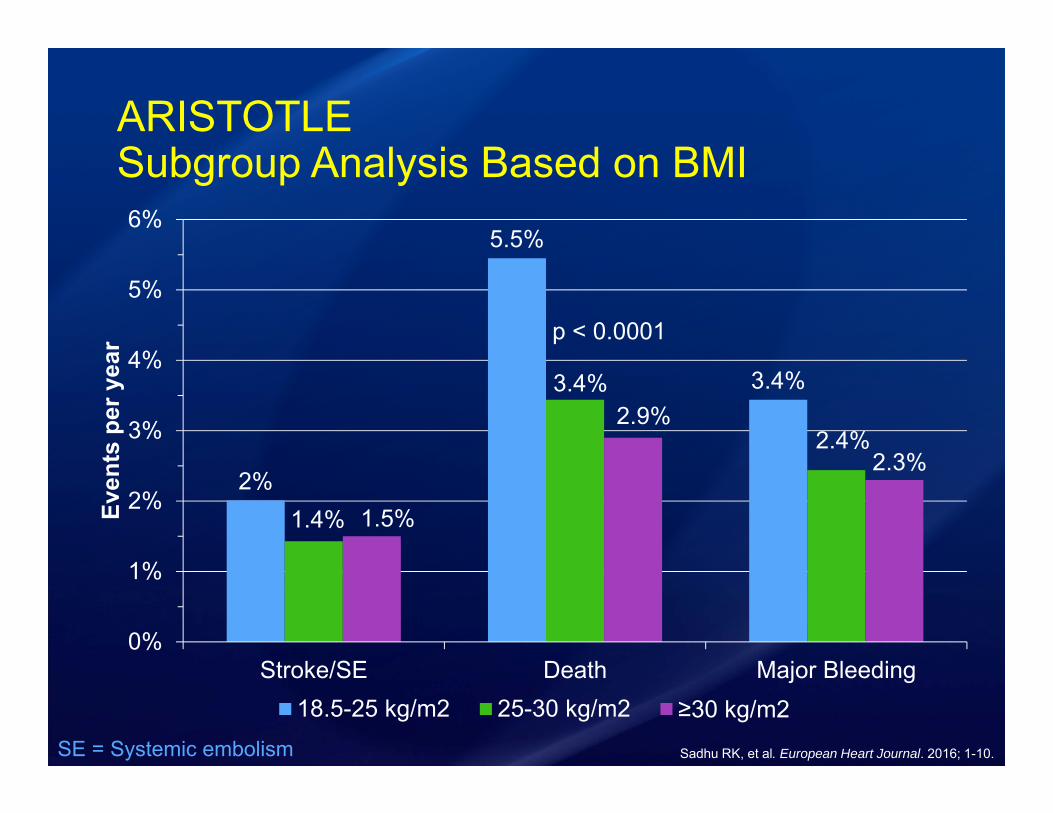
ARISTOTLESubgroup Analysis Based on BMI
2%
5.5%
3.4%
1.4%
3.4%
2.4%
1.5%
2.9%
2.3%
0%
1%
2%
3%
4%
5%
6%
Stroke/SE Death Major Bleeding
Even
ts p
er y
ear
18.5-25 kg/m2 25-30 kg/m2 ≥30 kg/m2
p < 0.0001
SE = Systemic embolism Sadhu RK, et al. European Heart Journal. 2016; 1-10.
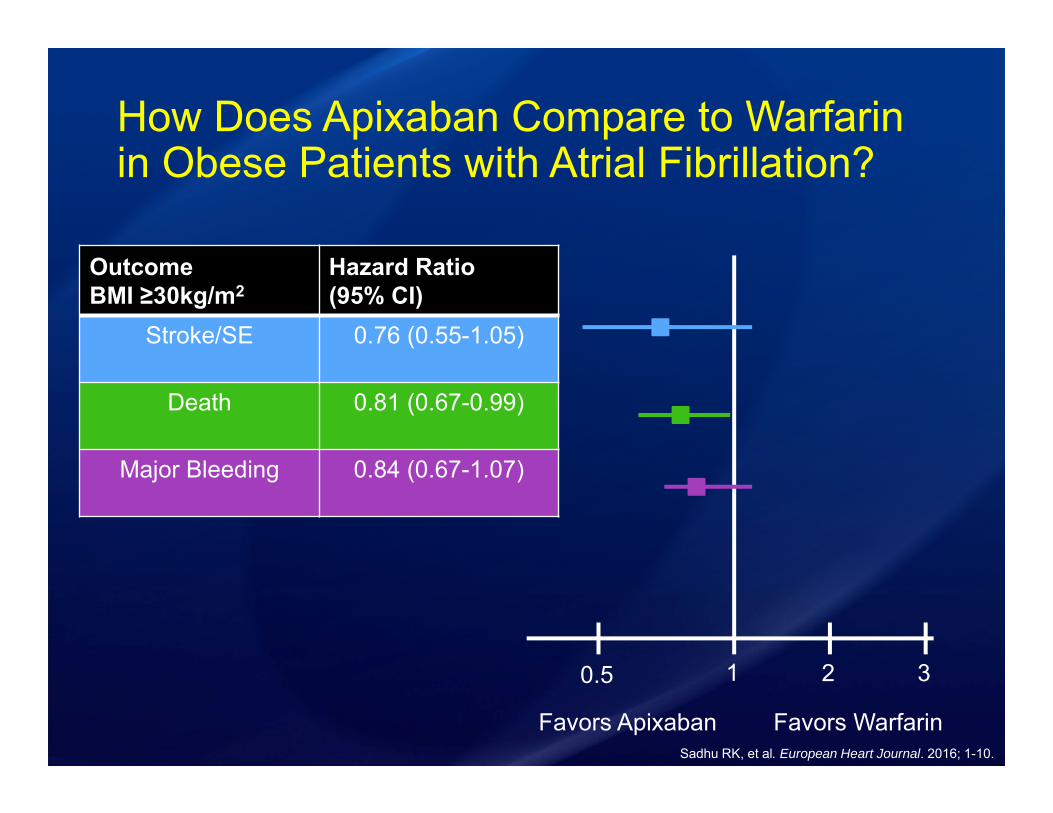
How Does Apixaban Compare to Warfarin in Obese Patients with Atrial Fibrillation?
0.5 1 2 3
OutcomeBMI ≥30kg/m2
Hazard Ratio(95% CI)
Stroke/SE 0.76 (0.55-1.05)
Death 0.81 (0.67-0.99)
Major Bleeding 0.84 (0.67-1.07)
Favors Apixaban Favors WarfarinSadhu RK, et al. European Heart Journal. 2016; 1-10.
DOACS for VTE
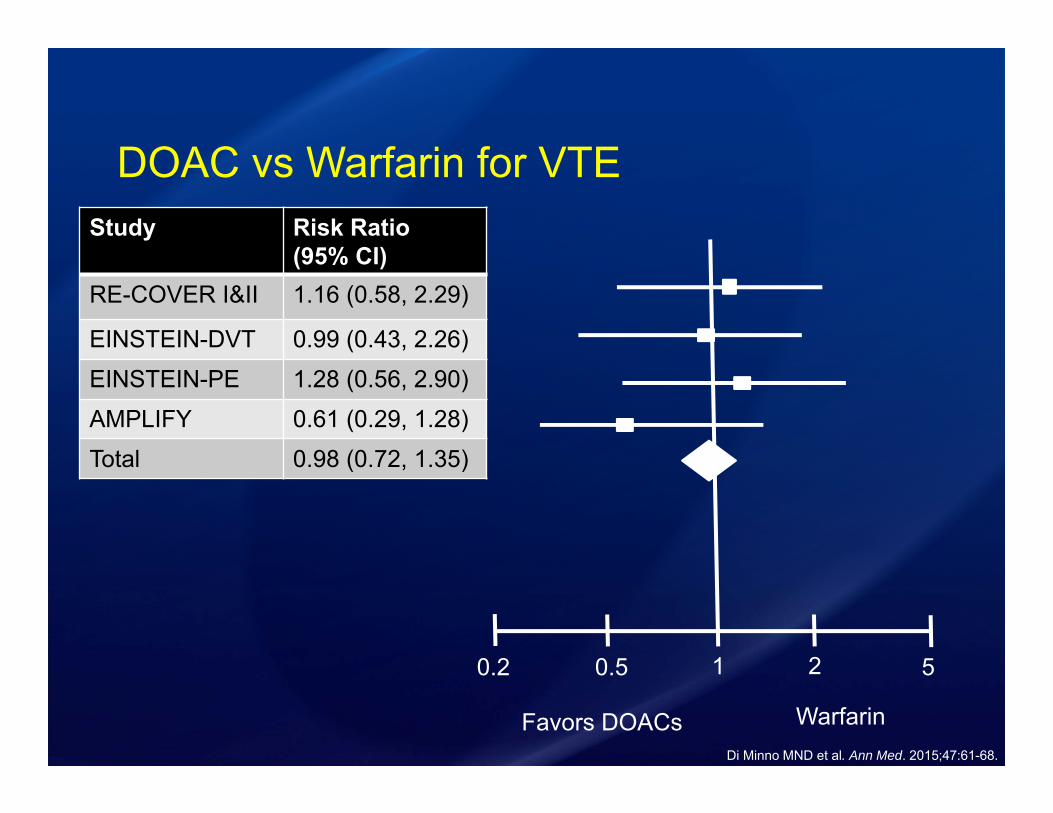
DOAC vs Warfarin for VTE
0.2 0.5 1 52
Favors DOACs WarfarinDi Minno MND et al. Ann Med. 2015;47:61-68.
Study Risk Ratio (95% CI)
RE-COVER I&II 1.16 (0.58, 2.29)
EINSTEIN-DVT 0.99 (0.43, 2.26)
EINSTEIN-PE 1.28 (0.56, 2.90)
AMPLIFY 0.61 (0.29, 1.28)
Total 0.98 (0.72, 1.35)
DOACs Recommendations in Obesity• Avoid dabigatran in obese patients
• Rivaroxaban may be considered in obese patients
• Apixaban has the best evidence for utilization of DOACs in obese patients

In a post-hoc analysis comparing apixaban vs warfarin in obese patients (BMI≥30kg/m2) with atrial fibrillation warfarin prevented more strokes and systemic embolism?A. TrueB. False
Summary• Evaluate pharmacokinetics when dosing medications in
obese patients
• For VTE prophylaxis “high-dose” heparin or LMWH is recommended for patients ≥100kg and BMI ≥40kg/m2
• For VTE treatment dose adjustments are warranted and anti-Xa levels should be monitored
• Apixiban may be considered for anticoagulation in obese patients
Questions & Discussion
Dose Capping with Unfractionated Heparin• NSTEMI
• Obese patients took longer to reach goal aPTT
• No dose cap • Higher doses achieves therapeutic
anticoagulation more rapidly
• VTE• Weight-based nomograms with no cap• Studies have shown relationship between
patients’ weight and heparin requirement
Joncas, SX, et al. Obesity Journal. 2013;21:1753-1758.Patel JP, et al. BJH. 2011;155:137-149.
Fondaparinux• Vd = 8.2L
• Largely resides in the intravascular space• >94% protein bound
• Treatment of VTE based on the MATISSE trials• 10mg if >100kg
Patel JP, et al. British Journal of Haematology. 2011;155:137-149.Fondaparinux [package insert]. GlaxoSmithKline. 2001.

Anti-Xa Monitoring Cost• Mayo Clinic Hospital – Rochester
• $207.50
• Vancomycin trough level cost $150.00

Anti-Xa Dose AdjustmentsAnti-Xa Level
(U/mL) Hold Next Dose Dosage Change Next Anti-Xa Level
<0.35 No Increase by 25% 4 hour after next dose
0.35-0.49 No Increase by 10% 4 hour after next dose
0.5-1.0 No NoNext day, then weekly, then
monthly
1.1-1.5 No Decrease by 20% Before next dose
1.6-2.0 3 hours Decrease by 30%Before next dose and 4 hour after
next dose
>2.0 Until anti-Xa <0.5 Decrease by 40%Before next dose and 4h after next
dose
Nutescu EA, et al. Ann Pharmacother. 2009;43:1064-1083.
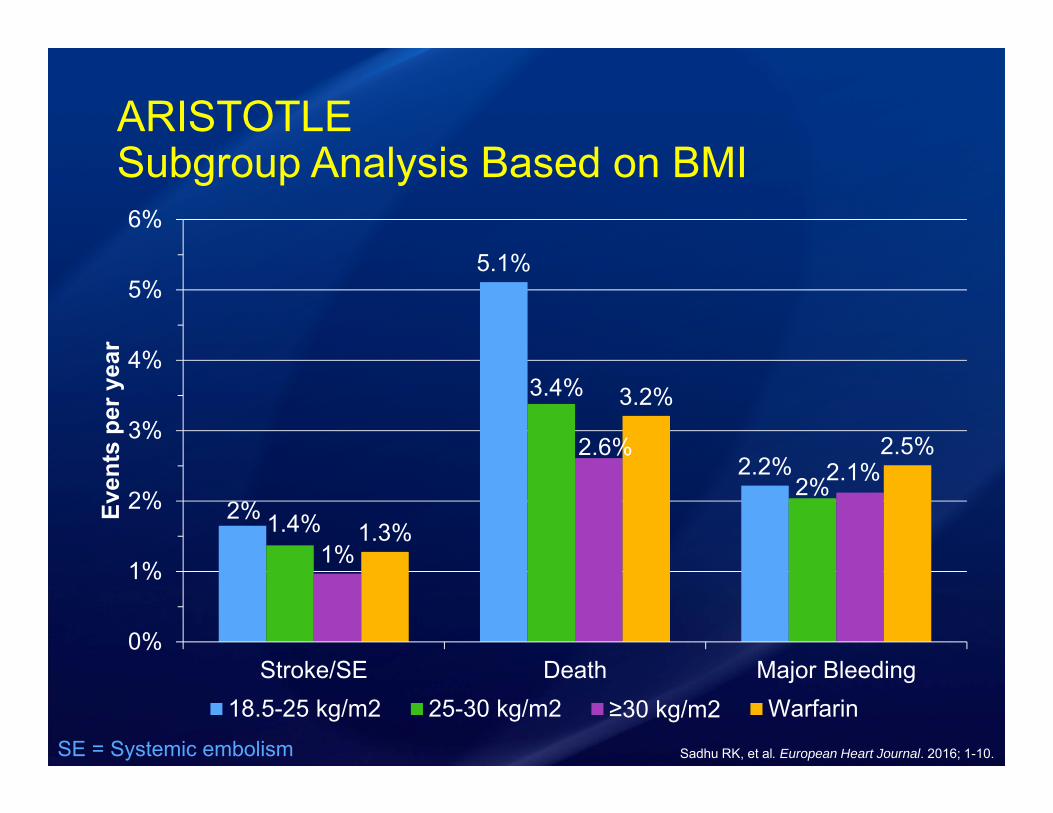
ARISTOTLESubgroup Analysis Based on BMI
2%
5.1%
2.2%
1.4%
3.4%
2%
1%
2.6%2.1%
1.3%
3.2%
2.5%
0%
1%
2%
3%
4%
5%
6%
Stroke/SE Death Major Bleeding
Even
ts p
er y
ear
18.5-25 kg/m2 25-30 kg/m2 ≥30 kg/m2 WarfarinSE = Systemic embolism Sadhu RK, et al. European Heart Journal. 2016; 1-10.