wed. 11.31.12 download: –2012 skeletal ppt. and bone structure word doc. hw: read p. 135-145...
TRANSCRIPT

Wed. 11.31.12
• Download:– 2012 skeletal ppt. And Bone Structure word doc.
• HW: Read p. 135-145 answer “Did you Get It Questions” #1-10.
• Did you turn in your Tissue SXM work and Practical?
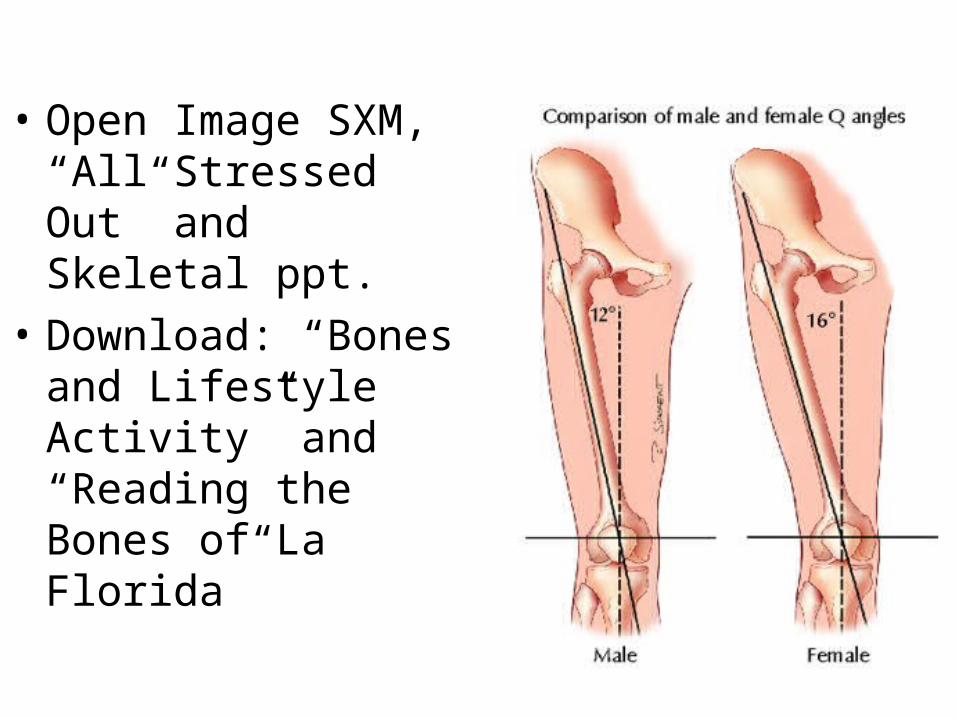
• Open Image SXM, “All Stressed Out” and Skeletal ppt.
• Download: “Bones and Lifestyle Activity” and “Reading the Bones of La Florida”

The Skeletal SystemThe Skeletal System Consists of: Bones (skeleton); Joints; Cartilages; Ligaments(bone-bone);tendons (muscle-bone)
Divided into two divisions: Axial skeleton (trunk/head); Appendicular skeleton (limbs)
Functions of Bones:Functions of Bones:
Support of the body; Protection of soft organs; Movement due to attached skeletal muscles; Storage of minerals and fats; Blood cell formation
The skeleton has 206 bones composed of living tissue: minerals (Ca, P hydroxyapatite crystals) deposited in intercellular matrix provide rigidity and hardness, compressional strength - endures squeezing(60% wt); proteins(esp. collagen) --> flexibility,toughness, tensile strength - endures stretching.
----> structure similar to reinforced concrete! (but weak torsional strength - does not endure twisting)
Two basic types of bone tissue:
Compact bone: homogeneous, dense
Spongy bone: small needle-like (spicules) pieces of bone; many open spaces
Classification of Bones:Classification of Bones: Long bones
Typically longer than wide; have a shaft with heads at both ends; contain mostly compact bone Examples: Femur, humerus
Short bones:
Generally cube-shape; contain mostly spongy bone; Examples: Carpals, tarsals
Flat bones
Thin and flattened; usually curved; thin layers of compact bone around a layer of spongy bone Examples: Skull, ribs, sternum
Irregular bones
Irregular shape; do not fit into other bone classification categories Example: Vertebrae and hip
http://depts.washington.edu/bonebio/ASBMRed/matrix.html

Classification of Bones on the Classification of Bones on the Basis of ShapeBasis of Shape

Artificial biomaterial scaffolds designed to support cell and tissue growth have traditionally aimed on a macroscopic level to match the properties of the organs they are to replace without recreating the nanoscale detail observed in real organs. In the body, the nanoscale structure of the ECM provides a natural web of intricate nanofibers to support cells and present an instructive background to guide their behavior. Unwinding the fibers of the ECM reveals a level of detail unmatched outside the biological world. Each fiber hides clues that pave the way for cells to form tissues as complex as bone, liver, heart, and kidney. The ability to engineer materials to a similar level of complexity is becoming a reality.
Cells are inherently sensitive to their surroundings. Typically between 10 and 100 µm in diameter, cells respond to environmental features at all length scales from the macro down to the molecular. The outer membrane of a typical cell is covered by specific carbohydrate structures and a forest of at least six different receptor systems that can be activated by interactions with adjacent cells, ligands in the surrounding ECM, and secreted signaling molecules. Hundreds of different proteins play a role in the composite stimulation of cell receptors, which in turn determine a plethora of responses, including cell migration in the early embryo, coordinated organogenesis, and wound repair throughout adult life. Collectively, these extrinsic factors make up a highly defined and specialized cell microenvironment, which is essential for correct tissue development and continued function.
Fig. 1. Hierarchical organization of bone over different length scales. Bone has a strong calcified outer compact layer (A), which comprises many cylindrical Haversian systems, or osteons (B). The resident cells are coated in a forest of cell membrane receptors that respond to specific binding sites (C) and the well-defined nanoarchitecture of the surrounding extracellular matrix (D).

Gross Anatomy of a Long BoneGross Anatomy of a Long BoneDiaphysis: shaft; composed of compact bone
Epiphysis: ends of the bone; composed mostly of spongy bone; contains red marow
Structures of a Long BoneStructures of a Long BonePeriosteum: outside covering of the diaphysis; fibrous connective tissue membrane; contains osteoprogenitor cells, osteoblasts, osteoclasts
Sharpey’s fibers: secure periosteum to underlying bone
Arteries: supply bone cells with nutrients
Articular cartilage: covers the external surface of the epiphyses; made of hyaline cartilage; decreases friction at joint surfaces
Medullary cavity: cavity of the shaft; contains yellow marrow (mostly fat) in adults; contains red marrow (for blood cell formation) in infants
Endosteum- connective tissue lining of medullary cavity; contains osteoprogenitor cells, osteoblasts, osteoclasts
Bone MarkingsBone Markings
Sites of attachments for muscles, tendons, and ligaments
Passages for nerves and blood vessels
Categories of bone markings: projections and processes; depressions or cavities
Microscopic Anatomy of BoneMicroscopic Anatomy of BoneOsteon (Haversian System): a unit of bone
Central (Haversian) canal: opening in the center of an osteon; carries blood vessels and nerves
Perforating (Volkman’s) canal: canal perpendicular to the central canal; carries blood vessels and nerves
Lacunae: cavities containing bone cells (osteocytes); arranged in concentric rings
Lamellae: rings around the central canal; sites of lacunae
Canaliculi: tiny canals; radiate from the central canal to lacunae; form a transport system

Your Task: Identify the parts of the bone:-Use the post its and tape to label:-Epiphysis (proximal and distal) and Diaphysis (and bone tissue types)-Articular cartilage (+ function)-Periosteum, Perforating Fibers (+ functions). -Epiphyseal line (+ define)
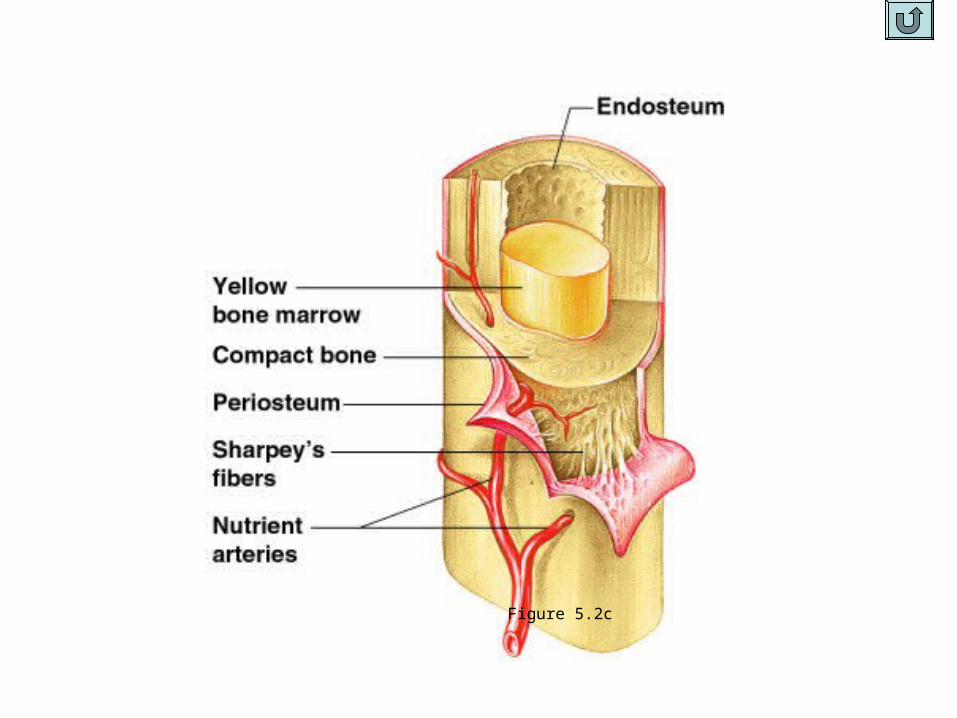
Figure 5.2c


Microscopic Anatomy of BoneMicroscopic Anatomy of Bone
Figure 5.3

Types of Bone Cells Types of Bone Cells (derive from 2 different types bone marrow cells)(derive from 2 different types bone marrow cells)Osteoblasts:
*Gap junctions with neighboring osteoblasts allow cells to communicate with each other.
*They come from bone marrow precursor cells. These precursors are capable of turning into either osteoblasts or fat cells, and various factors determine which kind of cells will be made. One of the factors is called Cbfa 1, which will cause the cell to differentiate into an osteoblast.
*The job of osteoblasts is to make the proteins that will form the organic matrix of bone and to control mineralization of the bone
*They have receptors for hormones such as vitamin D, estrogen, and parathyroid hormone.
*They secrete factors that activate osteoclasts (RANK-ligand) and other factors which communicate with other cells.
*They secrete PHEX, a protein that helps to regulate the amount of phosphate excreted by the kidney.
*When the team of osteoblasts has finished making new bone, some become surrounded with matrix and differentiate into osteocytes. Others will remain on the surface of the new bone and differentiate into lining cells. The rest undergo apoptosis (cell suicide) and disintegrate.
Osteocytes:*live inside the bone and have long branches which allow them to contact each other as well as the lining cells on the bone surface.
*are in a perfect position to sense any mechanical strain on the bone.
*can secrete growth factors which activate the lining cells or stimulate the osteoblasts.
*direct bone remodeling to accommodate mechanical strain and repair fatigue damage.
Lining cells:are former osteoblasts which have become flat and pancake-shaped.
*line the entire surface of the bone.
* are responsible for immediate release of calcium from the bone if the blood calcium is too low.
* protect the bone from chemicals in the blood which dissolve crystals (such as pyrophosphate).
*have receptors for hormones and factors that initiate bone remodeling.
Osteoclasts: Bone-destroying cells; are large cells with many nuclei.
*share lineage with blood cells (especially macrophages).
*Precursors circulate in the blood and bone marrow; Mature osteoclasts are formed from fusion of the precursors.
*Recognize bone through integrins (membrane proteins connected to extracelular matrix)* Break down bone matrix using exocytosis type vacuole release of HCl to acidify environment around bone for remodeling and
release of calcium. Waste products taken up by endocytosis.
(http://depts.washington.edu/bonebio/ASBMRed/structure.htm)l

Bone Growth: Bone Growth: involves replacement of connective tissue by boneinvolves replacement of connective tissue by boneIntramembranous Bone Formation- Intramembranous Bone Formation- (ex. cranium bones, clavicle)(ex. cranium bones, clavicle)
1. Membrane of fibrous connective tissue laid down during fetal development 1. Membrane of fibrous connective tissue laid down during fetal development 2. Several ossification centers develop as small spicules of bone laid down in open framework of spongy bone, 2. Several ossification centers develop as small spicules of bone laid down in open framework of spongy bone,
replacing connective tissue replacing connective tissue 3. On surface, osteoblasts lay down thin layer of compact bone. 3. On surface, osteoblasts lay down thin layer of compact bone. *Not completed in cranium for up to 2 years --> fontanelles wh/ eventually close after 2 yrs --> sutures*Not completed in cranium for up to 2 years --> fontanelles wh/ eventually close after 2 yrs --> sutures
Endochondral (Intracartilaginous) Bone FormationEndochondral (Intracartilaginous) Bone Formation1. Chondroblasts lay down cartilage model in fetus, starting wk 6 1. Chondroblasts lay down cartilage model in fetus, starting wk 6 2. Osteoblasts in periosteum lay down ring of bone around center of cartlage model to strengthen shaft as 2. Osteoblasts in periosteum lay down ring of bone around center of cartlage model to strengthen shaft as
cartilage replace by bone. (starting a month 5)cartilage replace by bone. (starting a month 5)3. Osteoblasts migrate to center of bone and lay down bone tissue on remaining fragments of calcified cartilage --3. Osteoblasts migrate to center of bone and lay down bone tissue on remaining fragments of calcified cartilage --
> primary center of ossification in diaphysis of bone- spongy bone > primary center of ossification in diaphysis of bone- spongy bone 4. Primary ossification center expands outward from center in both directions. 4. Primary ossification center expands outward from center in both directions. 5. Secondary centers of ossification develop in each epiphysis. 5. Secondary centers of ossification develop in each epiphysis. 6. Osteoclasts carve out medullary canal in diaphysis; osteoblasts lay down Haversian systems of compact bone. 6. Osteoclasts carve out medullary canal in diaphysis; osteoblasts lay down Haversian systems of compact bone. 7. 7. New cartilage is continuously formed; Older cartilage becomes ossified; Cartilage is broken down; Bone
replaces cartilage at faster rate than cartilage divides --> bone deposition overtakes cartilage growth and primary and secondary ossification centers merge; growth in length stops.
8.. Epiphyseal plates: allow for growth in length of long bone during childhood
***Bones are constantly remodeled throughout life by interaction of osteoblasts and osteoclasts; bone can continue to grow/ thicken in width, esp. with “stress”
***Cartilage remains in isolated areas: bridge of the nose, parts of ribs, joints. Max. bone growth up to 25 yrs., depending on sex, type of bone
Aging:
Loss of calcium (begins age 30 females, 50-60 males): decreased production sex hormones; bone resoprtion > bone formation ; Decreased protein production -->bones more brittle
http://depts.washington.edu/bonebio/ASBMRed/growth.html

Long Bone Formation and GrowthLong Bone Formation and Growth

Long Bone Formation and GrowthLong Bone Formation and Growth

Calcium HomeostasisCalcium HomeostasisCalcium: muscle contraction, nerve impulses, blood clotting,
Calcitonin: secreted by thyroid gland, decreases blood calcium levels by causing its deposition on bone; inhibits osteoclasts; increases urinary Ca excretion
Parathyroid hormone (Pth) - secreted by parathyroid gland cells, which also have calcium receptors:Stimulate osterclasts to remove calcium from bone; Stimulate the kidneys and intestine to absorb more calcium (active transport); Raise calcium levels in the blood
Vitamin DVitamin D (from diet or sunlight on skin -->enzymes produce it from cholesterol) --> liver, converted to calcidiol (from diet or sunlight on skin -->enzymes produce it from cholesterol) --> liver, converted to calcidiol -->kidney, converted to calcitriol (active form):-->kidney, converted to calcitriol (active form):
+production of Ca carriers in intestinal cells+production of Ca carriers in intestinal cells+active transport Ca from kidneys to blood+active transport Ca from kidneys to blood+bone resorption+bone resorption
Other Factors Influencing Bone Growth:Other Factors Influencing Bone Growth:Stress - exercise, piezoelectric effectStress - exercise, piezoelectric effectGrowth Hormone- secreted by ant. Pituitary; regulates rate and time of ossificationGrowth Hormone- secreted by ant. Pituitary; regulates rate and time of ossification
pituitary dwarfism- hyposecretion of GH--> short stature, delayed bone growth, normal bonepituitary dwarfism- hyposecretion of GH--> short stature, delayed bone growth, normal boneachondroplastic dwarfism- more common; genetic defect in receptor for growth factors or mutations achondroplastic dwarfism- more common; genetic defect in receptor for growth factors or mutations
effecting epiphyseal plate--> normal size head and pelvis but shortened limbseffecting epiphyseal plate--> normal size head and pelvis but shortened limbsGigantism (hypersecretion before epiphyseal plate closes) vs. AcromegalyGigantism (hypersecretion before epiphyseal plate closes) vs. Acromegaly
Sex hormones-Sex hormones- Estrogen: +bone growthEstrogen: +bone growth Testosterone: rapid bone growth but also closure of epiphyseal plates -->men reach max. height fasterTestosterone: rapid bone growth but also closure of epiphyseal plates -->men reach max. height fasterNutritional deficiencies:Nutritional deficiencies: Calcium; Phosphorus--> increased liability to fractures -->osteomalaciaCalcium; Phosphorus--> increased liability to fractures -->osteomalacia Vitamin D --> decreased intestinal absorption of Ca --> poorly calcified bone --> ricketsVitamin D --> decreased intestinal absorption of Ca --> poorly calcified bone --> rickets Vitamin C --> inability to maintain intercellular matrix/collagen --> slowed growth, delayed healingVitamin C --> inability to maintain intercellular matrix/collagen --> slowed growth, delayed healing Vitamin A ---> decreased coordination between osteoblasts and osteoclasts--> decreased rate bone growthVitamin A ---> decreased coordination between osteoblasts and osteoclasts--> decreased rate bone growth
http://depts.washington.edu/bonebio/ASBMRed/hormones.html
http://depts.washington.edu/bonebio/ASBMRed/exercise.html


DISORDERS:
Osteoporosis:
Can occur to due aging (women lose 1% bone / year after 30; men .5%); lack movement/bedrest; weightlessness
50% women, 20% men affected by age 65; 1/3-1/4 white females by 65 experience fracture related to osteoporosis
150,00 hip fractures/year --> 12-20% die complications; only 25% recover fully
8X more common in females - why? Men have larger bones to start; bone loss begins earlier in women; pregnancy, breastfeeding and menstrual cycles take toll; more women diet; women live longer
Bone Density: About 80% of the bone density is determined by heredity, and 20% by lifestyle (such as diet, exercise, smoking, and various medications.)
Treatment: 1. Estrogen 2. Supplemental Ca 3. Exercise 4. Electromagnetic fields
Prevention: 1. Maximize bone mass by taking in 1200 mg/day calcium; Vitamin D 2. Increase exercise 3. Limit smoking and alcohol consumption 4. DEXA - dual energy X-ray absorptiometry: measures bone density at susceptible sites
Rickets/Osteomalacia
Osteomalacia means "soft bones". The bones are about half mineral (calcium and phosphate) and half protein matrix, which is called osteoid. Normally 98% of the osteoid is mineralized, and 2% is new osteoid that has just been made and is waiting to get mineralized. In osteomalacia, the mineral does not deposit in the osteoid normally, so extra osteoid accumulates. This happens because there is not enough mineral supplied to the bone, or because there is a problem with the osteoblasts. Collagen without mineral is soft and flexible, like your ears.
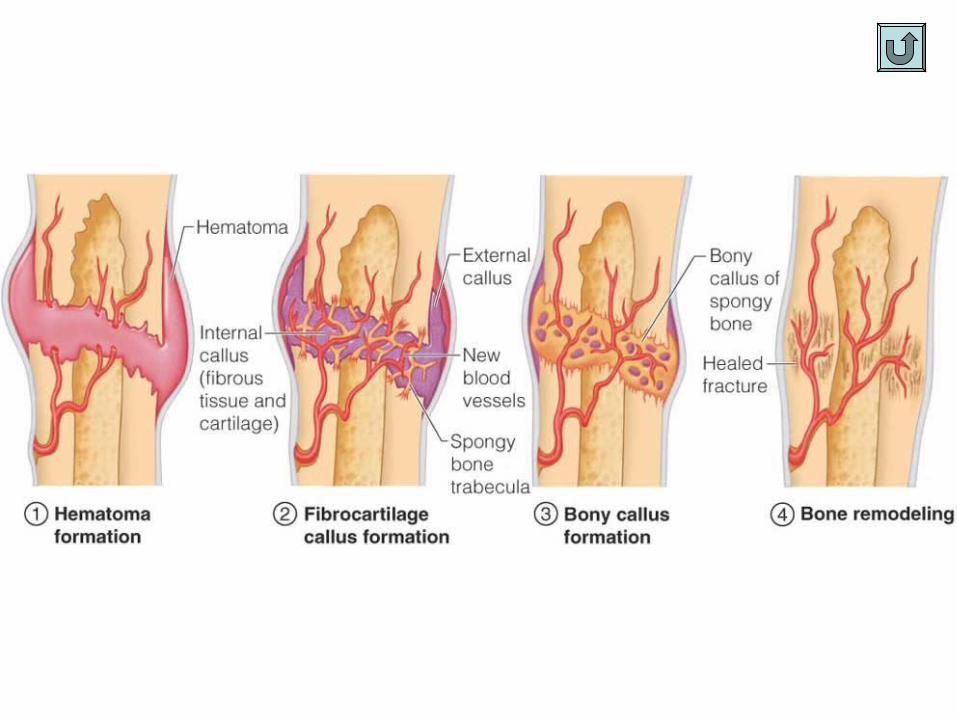
Fractures & Repairhttp://depts.washington.edu/bonebio/ASBMRed/growth.html
http://depts.washington.edu/bonebio/ASBMRed/diseases.html



12 yr. old boy
6’5” - gigantism
Acromegaly- thickened bones, increased soft tissue growth (bulbous nose, thickened skin)

The photograph above shows a group of children who had rickets caused by too little vitamin D.

Rickets occurs when this process takes place at the growth plates. The cartilage is mineralizing at a rapid rate. When the growth plate can't mineralize, it becomes thick, wide and irregular. The ends of the bones become weak and painful, especially at the knees which are bowed and fragile.
Children with mineralizing problems have both rickets and osteomalacia. Adults who develop the disease after they have grown will have only osteomalacia, because they no longer have growth plates. They can have painful bones which break easily. The photograph at right shows an adult who had rickets as a child. Below is an X-ray from a child with rickets, showing bowed legs; bones near the knee are fuzzy and wide.
Rickets and osteomalacia have several causes. The most common is vitamin D deficiency, seen when people do not get enough sunlight exposure and also don't have vitamin D in their diet. People with liver or kidney disease have problems with vitamin D because they can't convert it to the active form. Some people inherit problems with vitamin D or with function of the osteoblasts. Low blood phosphate also causes osteomalacia, and this can be caused by inherited problems with the kidneys, certain kidney diseases, or side effects of drugs.

Recap!• What is MNI?• Determining Age @ Death.• Geographic Ancestry--- there is no biological basis for
‘race’ but there are skeletal differences. • Determining Sex of skeleton.• Determining Height

Your task…• You are a crime scene
investigator. Work in pairs!• Take photo of crime scene.• Determine:
– MNI
– Sex
– Geographic Ancestry
– Height
– Age @ Death
– Possible Injuries
Written Crime Scene Report:• Create a GOOGLE DOC!
• Include a written response that details what information you used to identify the individual. – All of the points on the left– explain what
they are and how you used them in your identification!
• Also, theorize what may have happened at your crime scene!– Area of crime, time of day, details of
crime. – Include a photo of your crime scene.
• Dropbox completed Report by the end of class!

JointsJointsArticulations of bones
Functions of joints: hold bones together; allow for mobility. Cartilage good at resisting compression but not shearing forces (twisting, bending)
Ways joints are classified:
Functionally:
Synarthroses – immovable joints
Amphiarthroses – slightly moveable joints
Diarthroses – freely moveable joints
Structurally:
Fibrous joints: Generally immovable; bones united by fibrous tissue; Examples: Sutures; Syndesmoses: Allows more movement than sutures Example: distal end of tibia and fibula
Cartilaginous joints: Immovable or slightly moveable; bones connected by cartilage; Examples: Pubic symphysis, Intervertebral joints(discs)
Synovial joints: Freely moveable; articulating bones are separated by a joint cavity; synovial fluid is found in the joint cavity; Articular cartilage (hyaline cartilage) covers the ends of bones; Joint surfaces are enclosed by a fibrous articular capsule; Have a joint cavity filled with synovial fluid; Ligaments reinforce the joint
Structures Associated with the Synovial JointStructures Associated with the Synovial JointBursae – flattened fibrous sacs; Lined with synovial membranes; Filled with synovial fluid; Not actually part of the joint
Tendon sheath- Elongated bursa that wraps around a tendon
Classification of Synovial Joints

Fibrous JointsFibrous Joints

Cartilaginous JointsCartilaginous Joints

Synovial JointsSynovial Joints

The Synovial JointThe Synovial Joint


Types of Synovial Joints Based on Types of Synovial Joints Based on ShapeShape

Types of Synovial Joints Based on Types of Synovial Joints Based on ShapeShape

Knee- includes medial and lateral meniscus; anterior (ACL) and posterior cruciate ligaments; medial and lateral collateral ligaments; anterior patellar ligament; several bursae
***“terrible triad: (1) rupture of the medial collateral ligament, (2) damage to the medial meniscus, and (3) rupture of the anterior cruciate ligament
The anterior cruciate ligament (or ACL) is one of the four major ligaments of the knee. It connects from a posterio-lateral (back & outside) part of the femur to an anterio-medial (front & inside) part of the tibia.Damage to the ACL frequently occurs with lateral blows to the knee (as happens with a tackle from the side in football) and often is accompanied by injuries to the medial collateral ligament (MCL) and the medial meniscus, which is attached to the MCL; physicians are taught "...knee injuries come in threes - anterior cruciate, medial collateral, medial meniscus." Clinical studies, however, have noted a lateral meniscal tear to occur more commonly than the classic "terrible triad" noted previously. Non-contact tears or ruptures of the ACL often occur when athletes moving quickly in one direction make a sharp or sudden change in direction (cutting). In jump sports, ACL failure has been linked to heavy or stiff landing as well as twisting or turning the knee while landing. Studies indicate that women in jumping and cutting sports such as basketball, volleyball, cheerleading, or football (soccer), are significantly more prone to ACL injuries than men; this is generally believed to be due to differences between the sexes in training, the angle between the hip and knee called the "Q-angle", different strength-to-weight ratios, limb alignment, joint laxity, muscle recruitment patterns, size of the trochlear notch, and reaction time of muscle contraction. A new study suggests hormone-induced changes in muscle and ligament tension associated with menstrual cycles may be a factor but others have refuted this.
http://rad.usuhs.mil/medpix/medpix.html?mode=single&comebackto=mode%3Dcat_browse&recnum=5339

Shoulder -Rotator cuff tear is a common cause of pain and disability in the adult population. The rotator cuff is made up of a thickened capsule and four muscles and their tendons. These combine to form a "cuff" over the upper end of the arm (head of the humerus), providing stability but allowing maximum flexibility. The four muscles - supraspinatus, infraspinatus, subscapularis, and teres minor - originate from the "wing bone"(scapula), and together form a single tendon unit. This inserts on the greater tuberosity of the humerus. The rotator cuff helps to lift and rotate the arm and to stabilize the ball of the shoulder within the joint. Most tears occur in the supraspinatus but other parts of the tendon may be involved.
What causes the rotator cuff to tear? The rotator cuff tendons have areas of very low blood supply. The more blood supply a tissue has, the better and faster it can repair and maintain itself. The areas of poor blood supply in the rotator cuff make these tendons especially vulnerable to degeneration from aging. The degeneration of aging helps explain why the rotator cuff tear is such a common injury later in life. Rotator cuff tears usually occur in areas of the tendon that had low blood supply to begin with and then were further weakened by degeneration. This problem of degeneration may be accelerated by repeating the same types of shoulder motions. This can happen with overhand athletes, such as baseball pitchers. But even doing routine chores like cleaning windows, washing and waxing cars, or painting can cause the rotator cuff to fatigue from overuse. Excessive force can tear weak rotator cuff tendons. This force can come from trying to catch a heavy falling object or lifting an extremely heavy object with the arm extended. The force can also be from a fall directly onto the shoulder. Sometimes injuries that tear the rotator cuff are painful, but sometimes they aren't. Researchers estimate that up to 40 percent of people may have a mild rotator cuff tear without even knowing it.

Disorders Associated with JointsDisorders Associated with JointsDislocations; Sprains; Torn Cartilage
Functional Instability Following Lateral Ankle Sprain.Injury Clinic- Sports Medicine. 29(5):361-371, 2000. Hertel, JayAbstract:Lateral ankle sprain (LAS) is an extremely common athletic injury. Despite extensive clinical and basic science research, the recurrence rate remains high. Functional instability (FI) following LAS is hypothesised to predispose individuals to reinjury because of neuromuscular deficits which result following injury. When LAS occurs, structural damage not only occurs to the ligamentous tissue, but also to the nervous and musculotendinous tissue around the ankle complex. While injury to the ligaments may result in laxity of the joints of the ankle complex, neuromuscular deficits are also likely to occur due to the injury to the nervous and musculotendinous tissue. These neuromuscular deficits may be manifested as impaired balance, reduced joint position sense, slower firing of the peroneal muscles to inversion perturbation of the ankle, slowed nerve conduction velocity, impaired cutaneous sensation, strength deficits and decreased dorsiflexion range of motion. Additionally, the abnormal formation of scar tissue after injury may lead to sinus tarsi syndrome or anterolateral impingement syndrome, which may also lead to FI of the ankle complex.Bursitis – inflammation of a bursa usually caused by a blow or friction; Tendonitis – inflammation of tendon sheaths
Arthritis – inflammatory or degenerative diseases of joints.
Osteoarthritis: Most common chronic arthritis; not always related to normal aging processes; due to genetic defect in gene for collagen II, the primary component of cartilage. Affects 15.8 million Americans
Rheumatoid arthritis: an autoimmune disease – the immune system attacks the joints; Symptoms begin with bilateral inflammation of certain joints; Often leads to deformities (1.5 million women, 600,000 men
Gouty Arthritis: Inflammation of joints is caused by a deposition of urate crystals from the blood; can usually be controlled with diet
Repair: http://www.medicallegalart.com/animation.html
Joint Replacements
Arthroscopic surgery
**let’s watch some surgeries! http://www.nlm.nih.gov/medlineplus/surgeryvideos.html
(Virtual surgery- http://www.edheads.org/activities/knee/)
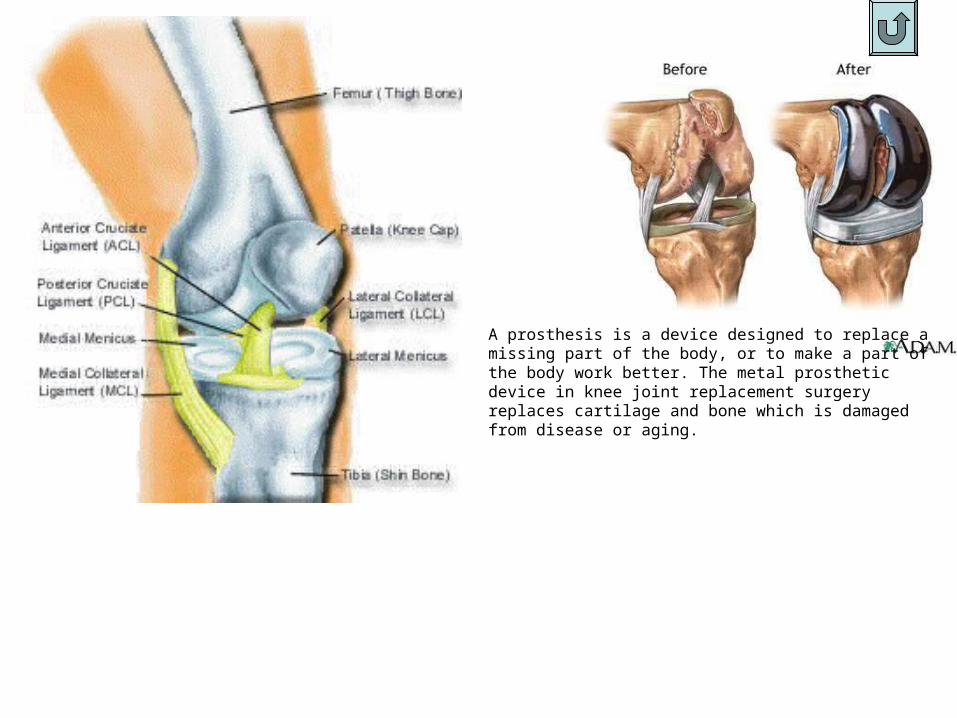
A prosthesis is a device designed to replace a missing part of the body, or to make a part of the body work better. The metal prosthetic device in knee joint replacement surgery replaces cartilage and bone which is damaged from disease or aging.

